Embed Size (px)
Citation preview

Orthodontic Consultation
file:///C:/ProgramData/Nierman/DentalWriterNet/Reports/out.html
Version: ORTHOQ Orthodontic Questionnaire OFFICE USE Patient ID:
CURRENT DATE: / / -' MALE
FEMALE NAME:
DATE OF BIRTH: / /
Please tell us why you have presented for evaluation and possible treatment
-' Crowding --' My dentist found the problem
' Overbite HABITS
-' Don't like my smile J Thumb sucking
- I Appearance '-.) Tongue habit
-` Better function '-t Mouth breathing
---' Airway assessment
` Teasing at school
Other
Referring Physician: Contact ID:
Dental History 'D If the patient has ever sucked their thumb or Yes
Patient plays a musical (mouth) instrument finger, until what age?
D No
.--` Yes -1 Yes Patient has consulted an orthodontist or another dentist Does the patient have any speech problems? regarding the orthodontic or TMJ problem
No No -' -
Does the patient breathe through the mouth?
_1 during the day
_i during the night
2 during the day and night
-' Yes Has one or more parent had previous ortho
No treatment?
Other
TMD Health Questionnaire Patient Concerns and Onset
Chief concern
Date of onset
Patient Signature: Date:
1 of 4 2/24/2016 2:53 PM

TMD Health Questionnaire Pain Symptoms
YOUR PAIN SYMPTOMS
—' Headaches
JMigraine headaches
Frequent neck aches or sore neck muscles
- Chronic shoulder or back pain
J Trouble sleeping soundly
- Jaws tired on waking
D Teeth sore on waking
' 11 Wisdom teeth have been extracted
-' Headaches in right or left temple areas
Headaches in front or back of head
J Teeth clenching during day
TJTeeth clenching at night
J Teeth grind when asleep
When are your pain symptoms are the worst?
Does anything make you feel better?
How often do you take medication for relieft of pain?
Trauma
Yes Have you ever had a severe blow to the head —1 Yes
Have you ever been involved in any serious accidenst, such as
—'No or jaw? No
car accident
—' Yes Any whiplash neck injuries?
No
Other Symptoms and History
Orthodontic Consultation
file:///C:/ProgramData/Nierman/DentalWriterNet/Reports/out.html
Patient Signature: Date:
2 of 4 2/24/2016 2:53 PM

TMD Health Questionnaire
'J Yes
'D No
U Yes
No
J Yes
J No
J Yes
U No
0 Yes
0 No
0 Yes
0 No
Yes
- ' No
0 Yes
'J No
3 Yes
J No
Yes
0 No
0 Yes
0 No
JAW JIONT SYMPTOMS
Does your jaw feel tired after a big meal?
Are there any foods you avoid eating?
Do you ever get dizzy?
Do you ever feel faint?
Do you ever feel nauseated?
Is there a family history of jaw joint (TMJ) problems or headaches?
Do you feel or hear a "clicking", "popping" or "cracking" noise from either jaw joint?
Has your jaw ever locked when you were unable to open or close?
Do you have difficulty opening wide or yawning?
Have you ever had pain in either jaw joint?
Does your jaw aqche when you open wide?
Yes
No
0 Yes
0 No
0 Yes
U No
0 Yes
0 No
U Yes
0 No
Yes
- No
Do you suffer from any loss of hearing?
Do you have itchiness or stuffiness in either ear?
Do you hear ringing, hissing or buzzing noises in either ear?
Do you wear glasses or contacts
Are there times when your eyesight blurs?
Do you get pain in, around or behind either eye?
U Yes
0 No
0 Yes
0 No
0 Yes
0 No
0 Yes
0 No
0 Yes
0 No
°Yes
Cj No
BREATHING
Do you have allergies?
Do you have sinus problems?
Do you snore at night?
Is your nose stuffed when you don't have a cold?
Have you been diagnosed with Sleep Apnea?
Have you had a sleep study done at a Sleep Clinic (hospital)?
0 Yes
0 No
EAR AND EYE SYMPTOMS
Do you have pain in either ear?
Orthodontic Consultation file:///C/ProgramData/Nierman/DentalWriterNet/Reports/out.html
Patient Signature: Date:
2/24/2016 2:53 PM
MLD PAIN
1111111
MODE DATE PAIN Am\
SEVERE PAIN
B Burning O Dull N Numbing P Pressure S Sharp T Tingling R Radiating
file:///C:/ProgramData/Nierman/DentalWriterNet/Reports/out.html Orthodontic Consultation
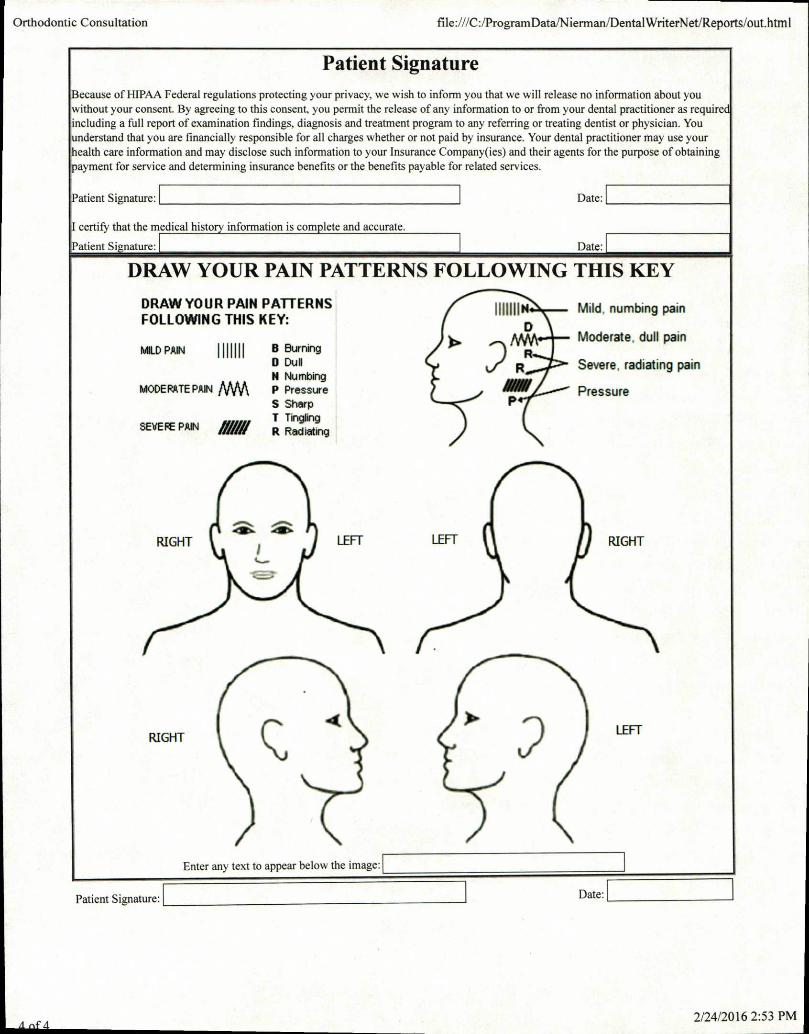
Patient Signature Because of HIPAA Federal regulations protecting your privacy, we wish to inform you that we will release no information about you without your consent. By agreeing to this consent, you permit the release of any information to or from your dental practitioner as require including a full report of examination findings, diagnosis and treatment program to any referring or treating dentist or physician. You nderstand that you are financially responsible for all charges whether or not paid by insurance. Your dental practitioner may use your
health care information and may disclose such information to your Insurance Company(ies) and their agents for the purpose of obtaining ayment for service and determining insurance benefits or the benefits payable for related services.
Date: Patient Signature:
I certify that the medical history information is complete and accurate.
anent Si nature: Date:
DRAW YOUR PAIN PATTERNS FOLLOWING THIS KEY
DRAW YOUR PAIN PATTERNS FOLLOWING THIS KEY:
1111111 Mild, numbing pain D
Moderate, dull pain
R Severe, radiating pain
Pressure
dB* RIGHT
42>I
LEFT LEFT RIGHT
RIGHT EFT
Enter any text to appear below the image:
Patient Signature:
Date:
2/24/2016 2:53 PM
BLAINE P. CUSACK, B.S., D.D.S.
Clinical Director/ General Dentist
Medical/ Dental Records Release
❑ I, the undersigned hereby authorize Dr. Cusack to release to
, any and all of my medical/ dental
information and records including office notes, medical charts, x-rays,
MRI films, and letters received while under his care.
❑ Please forward any and all medical/dental records, MRI films, x-rays,
etc. your facility has on file for me to.
Dr. Blaine P. Cusack
475 W. 55th St. Suite 207
La Grange, IL 60525
Phone: (708) 482-0300
Fax: (708) 482- 0541
• Diplomate of the American Academy of Pain Management
• Diplomate of the American Board of Orofacial Pain
• Diplomate of the Academy of Dental Sleep Medicine
• Credentialed by the Certification Board of the Academy of Dental Sleep Medicine
Patient Name (print)
Date
Address
SS#
City, State, Zip Patient's Date of Birth
x Patient Signature
Witness
Comprehensive Dental Care for Head, Neck & Facial Pain, TM Disorders and Sleep Appliance Therapy / Biological Dentistry
475 W. 55th Street • Suite 207 • LaGrange, IL 60525-3566 Phone: 708.482.0300 • Fax: 708.482.0541

BLAINE P. CUSACK, B.S., D.D.S. Clinical Director / General Dentist
PATIENT CONSENT FORM
• Diplomate of the American Academy of Pain Management
• Diplomate of the American Board of Orofacial Pain
• Diplomate of the Academy of Dental Sleep Medicine
• Credentialed by the Certification Board of the Academy of Dental Sleep Medicine
I understand that, under the Health Insurance Portability Act of 1996 (HIPAA), I
have certain rights to privacy regarding my protected health information. I
understand that this information can and will be used to:
• Conduct, plan and direct my treatment and follow-up among the
multiple health care providers who may be involved in that treatment
directly and indirectly.
• Obtain payment from third-party payers.
• Conduct normal healthcare operations such as quality assessments and
physician certification.
I have been informed by you of your notice of Privacy Practices containing a
more complete description of the uses and disclosures of my health
information. I have been given the right to review such Notice of Privacy
Practices from time to time and that I may contact this organization at any time
at the address below to obtain a current copy of the Notice of Privacy Practices.
I understand that I may request in writing that you restrict how my private
information is used or disclosed to carry out treatment, payment or health care
operations. I also understand you are not required to agree to my requested
restrictions, but if you do agree then you are bound to abide by such
restrictions. I understand that I may revoke this consent in writing at any time,
except to the extent that you have taken action relying on this consent.
Patient Name
Patient Signature
Relationship to patient
Date
Comprehensive Dental Care for Head, Neck & Facial Pain, TM Disorders and Sleep Appliance Therapy / Biological Dentistry
475 W. 55th Street • Suite 207 • LaGrange, IL 60525-3566 Phone: 708.482.0300 • Fax: 708.482.0541

• Diplomate of the American Academy of Pain Management
• Diplomate of the American Board of Orofacial Pain
• Diplomate of the Academy of Dental Sleep Medicine
• Credentialed by the Certification Board of the Academy of Dental Sleep Medicine
BLAINE P. CUSACK, B.S., D.D.S. Clinical Director / General Dentist
FINANCIAL TERMS AND CONDITIONS ■ As a condition of treatment by Dr. Cusack and his office, I
understand that financial arrangements must be in advance. The
practice depends upon reimbursement from the patients for the
costs incurred in that care and financial responsibility on the part
of each patient must be determined before treatment.
■ All emergency dental- medical services, performed without prior
financial arrangements must be made in cash at the time services
are performed. I understand that dental/ medical services
furnished to me are charged directly to me and that I am
personally responsible for payment of all dental/ medical services.
If I carry insurance forms to assist in making collections from
insurance companies. However, this office cannot and will not
render services on the assumption that charges will be paid by an
insurance company.
■ A service charge of 1 1/2% per month (18% per annum) will be
charged on the unpaid principle balance on all accounts not paid
within 60 days of the treatment date.
■ In consideration of the professional service rendered to me, or at
my request, by Dr. Cusack and/ or his staff, I agree to pay the
value of said services to the Doctor, or his assignee, at the time
the service are rendered, or within (5) days of billing if credit shall
be extended. I further agree for payment there for. Additionally, I
agree that a waiver of any further terms or condition. I further
agree that in the unlikely event that his office must institute
collection proceedings with request to amounts owed by me for
professional services rendered, this office shall be entitled to
recover all costs incurred including and not limited to reasonable
collection and or attorney fees.
■ I grant my permission to you, or your assigned to telephone me at
work to discuss any matter related to this form.
■ I have read the above conditions, understood them and agree to
their consent.
Signed Date
Relationship Witness
Comprehensive Dental Care for Head, Neck & Facial Pain, TM Disorders and Sleep Appliance Therapy Biological Dentistry
475 W. 55th Street • Suite 207 • LaGrange, IL 60525-3566 482.0300 • Fax: 708.482.0541





























