Embed Size (px)
Citation preview

VOLUME 3: NO. 1 JANUARY 2006
Race, Ethnicity, and Linguistic Isolation asDeterminants of Participation in Public
Health Surveillance Surveys
ORIGINAL RESEARCH
Suggested citation for this article: Link MW, Mokdad AH,Stackhouse HF, Flowers NT. Race, ethnicity, and linguis-tic isolation as determinants of participation in publichealth surveillance surveys. Prev Chronic Dis [serialonline] 2006 Jan [date cited]. Available from: URL:http://www.cdc.gov/pcd/issues/2006/jan/05_0055.htm.
PEER REVIEWED
Abstract
IntroductionTo plan, implement, and evaluate programs designed to
improve health conditions among racial and ethnic minor-ity populations in the United States, public health officialsand researchers require valid and reliable health surveil-lance data. Monitoring chronic disease and behavioral riskfactors among such populations, however, is challenging.This study assesses the effects of race, ethnicity, and lin-guistic isolation on rates of participation in the BehavioralRisk Factor Surveillance System (BRFSS).
MethodsCounty-level data from the 2003 BRFSS survey and
2000 U.S. census were used to examine the effects of race,ethnicity, and linguistic isolation on six measures of surveyparticipation (i.e., rates of resolution, screening, coopera-tion, response, language barriers, and refusal).
ResultsParticipation rates were significantly lower in coun-
ties with higher percentages of black people and peoplewho did not speak English. Response rates decreased by4.6% in counties with the highest concentration of black
residents compared with counties with few black resi-dents. Likewise, response rates decreased by approxi-mately 7% in counties in which a larger percentage of thepopulation spoke only Spanish or another Indo-Europeanlanguage compared with counties in which all residentsspoke English.
ConclusionThe negative relationship between the percentage of
Spanish-only–speaking households and participation ratesis troubling given that the BRFSS is conducted in bothSpanish and English. The findings also indicate that moreneeds to be done to improve participation among otherminorities. Researchers are investigating several ways ofaddressing disparities in participation rates, such as usingpostsurvey adjustments, developing more culturally appro-priate data-collection procedures, and offering surveys inmultiple languages.
Introduction
Reducing racial and ethnic disparities in health is anoverarching goal of Healthy People 2010 (1). To reach thisgoal, however, public health officials require valid and reli-able data from health surveillance to plan, implement, andevaluate programs designed to improve health conditionsamong racial and ethnic minority populations (2-4). Forinstance, health surveillance efforts have highlightedracial and ethnic disparities in health conditions such ascardiovascular disease, hypertension, diabetes, certaincancers (e.g., colon and rectal, pancreatic, stomach), andnationally notifiable diseases (e.g., chlamydia, gonorrhea,salmonelosis) and in risk factors for chronic conditionssuch as physical inactivity, excessive alcohol consumption,
The opinions expressed by authors contributing to this journal do not necessarily reflect the opinions of the U.S. Department of Health and Human Services,the Public Health Service, the Centers for Disease Control and Prevention, or the authors’ affiliated institutions. Use of trade names is for identification only
and does not imply endorsement by any of the groups named above.
www.cdc.gov/pcd/issues/2006/jan/05_0055.htm • Centers for Disease Control and Prevention 1
Michael W. Link, PhD, Ali H. Mokdad, PhD, Herbert F. Stackhouse, MA, Nicole T. Flowers, MD

VOLUME 3: NO. 1JANUARY 2006
and cigarette smoking (5-11).Despite the success of many sur-veillance efforts, monitoringchronic disease and behavioralrisk factors among minority popu-lations remains a challenge.
The proportion of racial and ethnicminorities who participate in majorhealth surveys is often lower thanthe proportion for the overall U.S.population. Some of the reasons forlower rates of participation amongracial and ethnic minorities includedisproportionate mistrust of govern-ment and the research community,cultural and language barriers,lower rates of literacy and health lit-eracy (the capacity to obtain,process, and understand basichealth information and servicesneeded to make appropriate healthdecisions), high mobility patterns,reluctance to reveal personal infor-mation, and data-collection proce-dures (e.g., characteristics of theinterviewers) (12-26). Becauseminority groups, particularly groupsof lower socioeconomic status, maybe underrepresented in publichealth statistics generated by thesesurveys, the health risks and healthproblems that they face may be inad-equately described.
The potential for such problemshas increased over the past severaldecades as the U.S. population hasgrown more diverse. From 1980 to2002, according to the U.S. CensusBureau, the proportion of minori-ties among the civilian, noninstitu-tionalized population grew from6.4% to 13.3% among Hispanics,11.7% to 13.0% among blacks, and1.5% to 4.4% among Asians (27-30). Additionally, as of2002, 11.7% of U.S. residents were reported to have beenborn in a foreign country, with 53.3% of those sayingthey had been born in Latin America, 25.0% in Asia,
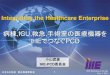
13.7% in Europe, and 8.0% in someother region of the world (31).Moreover, the various racial andethnic groups are not distributedequally across the United States(Figures 1–3). As a result, thepotential impact of race and eth-nicity on survey participation ratesvaries considerably among andwithin regions.
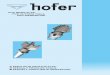
There has also been a correspon-ding growth in the percentage ofU.S. residents who primarily speaka language other than English.According to the 2000 census,47.0 million (18%) of the 262.4million people aged 5 years andolder spoke a language other thanEnglish at home (33). This per-centage increased from 14% in1990 and from 11% in 1980.Linguistic isolation is defined bythe U.S. Census Bureau as livingin a household in which all mem-bers aged 14 years and olderspeak a non-English languageand also speak English less than“very well” (i.e., have difficultywith English) (32). In 2000,approximately 4.5% of the U.S.population could have been con-sidered linguistically isolated.Among certain subpopulations,however, the percentage of peoplewho said they spoke English lessthan very well was high: 51% ofindividuals spoke an Asian orPacific Island language, 49%spoke Spanish, and 34% spokeanother Indo-European language(33). Table 1 shows the major lan-guages included in each group.Again, the types of languages spo-ken within linguistically isolated
households across the United States vary by region(Figures 4–6). Because most health surveys are typi-cally conducted in English only, linguistic isolation canbe expected to significantly increase the level of
2 Centers for Disease Control and Prevention • www.cdc.gov/pcd/issues/2006/jan/05_0055.htm
The opinions expressed by authors contributing to this journal do not necessarily reflect the opinions of the U.S. Department of Health and Human Services,the Public Health Service, the Centers for Disease Control and Prevention, or the authors’ affiliated institutions. Use of trade names is for identification only
and does not imply endorsement by any of the groups named above.
Figure 1. Percentage of Hispanic or Latino adults aged18 years and older, United States. Source: U.S.Census 2000 (32).
Figure 2. Percentage of black or African Americanadults aged 18 years and older, United States.Source: U.S. Census 2000 (32).
Figure 3. Percentage of Asian or Pacific Islander adultsaged 18 years and older, United States. Source: U.S.Census 2000 (32).

nonresponse among people who donot speak English.
As one of the world’s largest healthsurveillance systems, the BehavioralRisk Factor Surveillance System(BRFSS) has been instrumental intracking health disparities acrosspopulations in the United States(34). Yet over the past decade,BRFSS participation rates, likethose of most other surveys, havedeclined sharply (35). As part of aneffort to reverse this trend andensure the reliability and validity ofBRFSS data, we assessed the impactof race, ethnicity, and linguistic iso-lation on measures of survey partici-pation. This report includes theresults of that assessment as well asa discussion of potential means ofimproving survey participation ratesamong these groups, thus makingpopulation-based health surveys likethe BRFSS surveys more represen-tative of the entire population.
Methods
The BRFSS gathers datathrough computer-assisted tele-phone interview (CATI) surveysdesigned to collect uniform, state-specific data on preventive healthpractices and risk behaviors thatare linked to the leading causes ofmorbidity and mortality amongadults. The survey is conducted byall 50 states and the District ofColumbia, as well as by PuertoRico, Guam, and the VirginIslands with assistance from theCenters for Disease Control andPrevention (CDC). However, thethree territories are not includedin the analysis presented here. Further details on theBRFSS design, methodology, and questionnaire arepresented elsewhere (36).
Measures and variables
To examine aspects of survey participation, we calculated the fol-lowing six dependent measures ofsurvey participation at the countylevel based on final case dispositionfor telephone numbers calledbetween January 1, 2003, andDecember 31, 2003:
1. Resolution rate: the percentage ofall sampled telephone numbers forwhich household status with aworking telephone number has beendetermined
2. Screening rate: the percentage ofall known households in which thepresence or absence of an eligiblerespondent has been determined
3. Cooperation rate: the percentageof known, eligible households inwhich a completed or partially com-pleted interview has been obtained
4. Response rate: the percentage ofall confirmed and potentially eligi-ble sample members for whom aninterview has been completed,which we calculated using ResponseRate 4 recommended by theAmerican Association for PublicOpinion Research (37)
5. Language-barrier rate: the per-centage of all sampled householdsgiven a final disposition of languagebarrier. Interviewers could not com-municate with household membersbecause of the language spoken inthe home (which was presumablynot English or Spanish, the two lan-guages in which the BRFSS surveyis conducted)
6. Refusal rate: the percentage of all sampled householdsgiven a final disposition of refusal, indicating either the
VOLUME 3: NO. 1JANUARY 2006
www.cdc.gov/pcd/issues/2006/jan/05_0055.htm • Centers for Disease Control and Prevention 3
The opinions expressed by authors contributing to this journal do not necessarily reflect the opinions of the U.S. Department of Health and Human Services,the Public Health Service, the Centers for Disease Control and Prevention, or the authors’ affiliated institutions. Use of trade names is for identification only
and does not imply endorsement by any of the groups named above.
Figure 4. Percentage of linguistically isolatedSpanish-language households, United States.Source: U.S. Census 2000 (32).
Figure 5. Percentage of linguistically isolated Asian-language or Pacific Island-language households,United States. Source: U.S. Census 2000 (32).
Figure 6. Percentage of linguistically isolated Indo-European–language households, United States.Source: U.S. Census 2000 (32).

VOLUME 3: NO. 1JANUARY 2006
selected sample member’s refusal to complete the inter-view or the interviewer’s inability to recontact the house-hold because of a hang-up or other refusal by someone inthe household
We conducted the analysis at the county level because ofa lack of available information about survey nonrespon-dents at the individual or household level. Counties wereincluded in the analysis if they had 30 or more observa-tions in the denominator of each of the six participationmeasures. Our use of these criteria ensured greater stabil-ity in the measures calculated and helped us compare theimpact of independent variables across the six models esti-mated; however, it also limited the analysis to 1894 of the3141 counties in the United States.
County-level predictor variables for race, ethnicity, andlinguistic isolation were derived from 2000 U.S. censuscounts (32). We calculated the percentage of each county’spopulation that was black or African American, Asian,and Hispanic, as well as the percentage who spoke onlySpanish, only an Asian language, or only another Indo-European language. On average, the included countieshad somewhat higher percentages of blacks than did thenonincluded counties (9.0% compared with 7.1%), Asians(1.2% compared with 0.4%), Asian-language–only households (0.2% compared with 0.1%), and Indo-European–language–only households (0.4% comparedwith 0.3%) but slightly lower percentages of Hispanics(4.8% compared with 6.9%) and Spanish-language–onlyhouseholds (1.0% compared with 1.5%).
We also developed several county-level control vari-ables to account for some of the other factors that arethought to affect participation rates within certain geo-graphic areas. Socioeconomic status, often measuredthrough a combination of income and education levels, isan important mediator of racial and ethnic health dis-parities and an important predictor of survey participa-tion (2,38). Likewise, living in an urban area, being awayfrom home frequently, and screening calls with answeringmachines, caller-identification devices, or similar deviceshave been shown to reduce respondent contactability andparticipation rates (21,38,39). We used 2000 U.S. censusdata to develop four control variables based on 1) the per-centage of households in each county with incomes of$50,000 or more, 2) the percentage of adults aged 25 andolder in each county who had less than a high school edu-cation (e.g., no high school diploma or equivalency), 3) the
percentage of households in each county that were inurban areas, and 4) the percentage of households in eachcounty with heads of household who had a one-way com-mute to work of 30 minutes or more. We used BRFSS datato calculate a fifth control variable measuring the percent-age of all calls made within a county that resulted in con-tact with an answering machine, privacy manager, orsome other identifiable type of call-screening device.
Statistical analysis
Because all variables in the analysis were expressed aspercentages, we used ordinary least squares (OLS) regres-sion modeling to assess the impact of race, ethnicity, andlinguistic isolation on survey participation. In preliminaryanalyses, we found a high degree of correlation betweenAsian race and Asian-language isolation (r = 0.92; P < .001)and between Hispanic ethnicity and Spanish-language iso-lation (r = 0.93; P < .001). We used separate models todetermine which variables (race, ethnicity, or linguisticisolation) were better predictors, but we found the differ-ences between them to be marginal. Although linguisticisolation is a definite barrier to survey participation, raceand ethnicity may or may not be factors; thus, the Asian-language–only and Spanish-language–only vari-ables were retained in the final models, but the variablesAsian race and Hispanic ethnicity were not retained.Because of the strong correlation between race, ethnicity,and language-isolation variables, however, we had difficul-ty determining the proportional impact of each.
We also examined the possible effects of multi-collinearity in our analysis. Because we found thatregressing the other predictor and control variables onurbanicity explained more than 50% of the variance inthe percentage-urban variable (adjusted R2 = 0.52; F =296.7), we removed urbanicity from the final models.
The final OLS models were estimated for each of the sixparticipation measures (rates of resolution, screening,cooperation, response, language barriers, and refusal).The dependent variables used were the county-level esti-mates for percentage of black adults, percentage ofSpanish-language–only households, percentage of otherIndo-European-language–only households, and percent-age of Asian-language–only households. The control vari-ables used were the percentage of households withincomes of $50,000 or more, the percentage of adults aged25 and older with less than a high school education, the
4 Centers for Disease Control and Prevention • www.cdc.gov/pcd/issues/2006/jan/05_0055.htm
The opinions expressed by authors contributing to this journal do not necessarily reflect the opinions of the U.S. Department of Health and Human Services,the Public Health Service, the Centers for Disease Control and Prevention, or the authors’ affiliated institutions. Use of trade names is for identification only
and does not imply endorsement by any of the groups named above.

percentage of heads of household with a one-way work com-mute of 30 minutes or more per day, and the percentage ofBRFSS calls that reached an answering machine or call-screening device. Model selection was based on forced entryof all variables into the models rather than stepwise selec-tion. The models were estimated using SPSS 13.0 (SPSSInc, Chicago, Ill) with the Complex Samples module.
Finally, we used the OLS coefficients from the finalmodels and the maximum county-level populationparameters to calculate the maximum impact of race,ethnicity, and linguistic isolation on the six measures ofsurvey participation.
Results
In general, minority race and ethnicity and linguistic iso-lation had significant negative correlations with surveyparticipation rates (Table 2). The regression coefficients (ß)in these models estimate the amount of increase ordecrease in the dependent measures for every one-unit dif-ference in the independent variables. For example, forevery percentage-point increase in the black population ofa county, the county-level response rate declined by 0.06%.Counties with higher percentages of black residents tend-ed to have significantly lower rates of participation andhigher refusal rates. Statistically significant (α = .05) neg-ative relationships were noted between the percentage ofblack adults in a county and county-level resolution rates(ß = –0.03; P = .001), screening rates (ß = –0.18; P = .001),cooperation rates (ß = –0.13; P = .001), and response rates(ß = –0.06; P = .001), although a significant positive rela-tionship was seen with refusal rates (ß = 0.06; P = .001).The percentage of black residents in a county did not havea significant effect on the rate of nonparticipation attrib-uted to a language barrier.
Linguistic isolation also had a negative effect on partic-ipation rates, although the magnitude of this effect dif-fered across the three language types. Higher rates ofSpanish-language isolation led to lower resolution rates (ß= –0.11; P = .04), screening rates (ß = –0.92; P = .001), coop-eration rates (ß = –0.58; P = .001), and response rates (ß =–0.26; P = .001). The impact of Spanish-language isolationon response rates was more than four times the impact ofthe percentage of black adults in a county. Counties withhigher percentages of Spanish-language–only householdsalso had higher percentages of nonparticipation attributed
to language barriers (ß = 0.12; P = .001). Rates of Spanish-language isolation did not, however, significantly affect thepercentage of nonparticipation attributed to refusals.
The percentage of households in which only Indo-European languages were spoken did not significantlyaffect resolution rates, but it did have a significant nega-tive effect on screening rates (ß = –1.36; P = .001), coopera-tion rates (ß = –1.39; P = .001), and response rates (ß =–0.64; P = .001). Counties with higher rates of Indo-European-language–only households also had higherlanguage-barrier and refusal rates.
In contrast, Asian-language–isolated households hadless effect on survey participation rates. Counties withhigher percentages of Asian-language–only households didhave significantly lower resolution rates (ß = –0.48; P = .03)and screening rates (ß = –0.98; P = .03), but they did not havesignificantly lower cooperation or response rates. Similarly,although higher percentages of Asian-language isolation ledto a significant increase in the language-barrier rate (ß =0.14; P = .001), there was a significant decrease in therefusal rate in these counties (ß = –1.90; P = .001).
Overall, race, ethnicity, and language-isolation modelsexplained 27% to 31% of the variance in the screening,response, and language-barrier rates, but the models wereonly about half as effective in explaining variance in reso-lution, cooperation, and refusal rates.
Because the impact of race, ethnicity, and linguistic-iso-lation variables depended on the size of a county subpopu-lation, we calculated the maximum impact of these variables among the subset of 1894 counties examinedhere. Table 3 shows the amount of change we might expectin the percentage of each rate in counties with the highestconcentrations of black residents and language-isolatedhouseholds. We calculated this expected change by multi-plying the high range value for each population character-istic by its corresponding OLS coefficient from Table 2. Wefound, for example, that in counties in which slightly morethan one fourth of the households spoke only Spanish,screening rates were approximately 25% lower than incounties with no Spanish-language–only households. Wealso found that in counties in which approximately threefourths of the adult population was black, response rateswere 5% lower than in counties with no black residents.Response rates were 7% lower in counties with the highestconcentrations of households in which Spanish was the
VOLUME 3: NO. 1JANUARY 2006
www.cdc.gov/pcd/issues/2006/jan/05_0055.htm • Centers for Disease Control and Prevention 5
The opinions expressed by authors contributing to this journal do not necessarily reflect the opinions of the U.S. Department of Health and Human Services,the Public Health Service, the Centers for Disease Control and Prevention, or the authors’ affiliated institutions. Use of trade names is for identification only
and does not imply endorsement by any of the groups named above.

VOLUME 3: NO. 1JANUARY 2006
predominant language and no one in the household spokeEnglish very well. Likewise, response rates were approxi-mately 7% lower in counties with higher concentrations ofhouseholds in which other Indo-European languages werespoken rather than English.
Discussion
Our study revealed that survey participation rateswere significantly lower in areas with higher concen-trations of racial and ethnic minorities and linguisti-cally isolated households. These important findingsindicate the need to ensure adequate representation ofthese populations in large-scale health surveys such asthe BRFSS. As we examine ways of increasing BRFSSparticipation rates, these findings will help us to designand implement more effective means of involving thesehard-to-reach populations.
One particularly disturbing finding was the significantimpact of Spanish-language isolation on participationrates, given that BRFSS surveys are offered in bothSpanish and English. Education is an important mediat-ing factor in survey participation among Hispanic individ-uals because lower levels of literacy and health literacyhave been related to a greater reluctance by Hispanicindividuals to participate in health surveys (26,40). Ourstudy shows, however, that even after controls are addedfor education, areas with higher concentrations ofSpanish-only–speaking households are less likely to par-ticipate in health surveys. This may be because of ineffec-tive procedures for contacting and eliciting participationfrom predominantly Spanish-speaking households, lack ofbilingual or Spanish-speaking interviewers, or inadequatetraining of Spanish-speaking interviewers. It is also likelythat current Spanish-language survey translations do notadequately address the different Spanish dialects spokenin the United States, such as those spoken by individualsor families originating from Mexico, Puerto Rico, or Cuba(41). Moreover, it may also reflect the impact of ethnic andcultural issues. Therefore, we may have to assume thatconcepts and interpretation are culturally dependent(42,43). We were unable, however, to disentangle theinfluence of language and culture.
Our findings also indicate that more needs to be done toimprove participation among other minorities, such asAfrican Americans, Asians who are isolated by language,
and other language-isolated groups. To this end,researchers are investigating ways to address disparitiesin participation rates by postsurvey adjustments, cultural-ly appropriate data-collection procedures, and multiplelanguage use.
Standard techniques are widely used to compensate fordemographic differences between a survey sample and thegeneral population it represents (21). Postsurvey adjust-ments such as weighting and stratification represent stan-dard practices in most major health surveys. However,these techniques are often limited to a few key demo-graphic variables for which population estimates are avail-able. Moreover, they may produce larger standard errorsthat decrease the precision of estimates.
Researchers need to develop survey designs that betteraddress the increasingly complex racial, ethnic, and lin-guistic mix of the U.S. population. A U.S. Department ofHealth and Human Services report recommended that“culturally and linguistically appropriate interviewingtechniques need to be employed at all times when con-ducting surveys on racial and ethnic issues” (4). The reportfurther recommended that relevant cultural factors andlanguage requirements be incorporated into surveydesigns when feasible. Researchers need to be cognizant ofthe customs, values, and beliefs of individuals in minoritycommunities, particularly because they relate to the shar-ing of personal information, including health care practicesand health conditions (44). Focus groups and cognitiveinterviews of people from various backgrounds can helpdetermine whether respondents will interpret and respondto survey requests and questions as intended (45,46).
Some research has shown that the race, ethnicity, andsex of an interviewer can affect a respondent’s level of coop-eration (14). Because an interviewer with a backgroundand characteristics similar to those of a potential surveyparticipant may not be available, it is important that inter-viewers be trained to understand and manage multipleculturally specific issues. This understanding requires thedevelopment and implementation of cultural-sensitivitytraining programs for interviewers. Culturally specificscripts could also be made available to interviewers inanticipation of challenging situations.
Researchers also need to consider increasing the numberof languages in which a survey is offered, especially in com-munities where rates of linguistic isolation are high.
6 Centers for Disease Control and Prevention • www.cdc.gov/pcd/issues/2006/jan/05_0055.htm
The opinions expressed by authors contributing to this journal do not necessarily reflect the opinions of the U.S. Department of Health and Human Services,the Public Health Service, the Centers for Disease Control and Prevention, or the authors’ affiliated institutions. Use of trade names is for identification only
and does not imply endorsement by any of the groups named above.

Moreover, it is important to ensure that the translatedquestions are culturally equivalent in terms of coherenceand appropriateness (19,20,47,48).
Researchers have used two approaches in addressinglinguistic isolation. The first approach is to translatethe questionnaire and hire interviewers who are fluentin that language. This native-language speakerapproach is used by the California Health InterviewSurvey (CHIS), a state-based telephone survey similarin content to the BRFSS survey. The 2001 CHIS wastranslated into Spanish, Mandarin Chinese,Cantonese, Vietnamese, Korean, and Cambodian(Khmer). Approximately 10% of the completed inter-views in the state were conducted in Spanish, and 5%were conducted in one of the Asian languages (49).
The second approach is to rely upon third-party inter-preters to administer the survey. Some language-serviceproviders can provide interpreters in more than 150 lan-guages (50). Using a three-way telephone connection, forexample, an interpreter (who has access to an English ver-sion of the questionnaire but not necessarily a versiontranslated into the respondent’s language) translates theconversation between the English-speaking interviewerand the native-language–speaking respondent. Thisapproach is used for the National Immunization Survey(NIS), a telephone survey that collects immunization infor-mation on children aged 19 to 35 months living in U.S.households. In 2002, interviews conducted by this methodaccounted for 4% to 5% of the completed interviews inareas such as Boston, Newark, New York City, and KingCounty, Wash (51).
Both of these translation approaches have advan-tages and disadvantages. The use of native-lan-guage–speaking interviewers helps ensure that thesurvey questionnaire is administered in a standardizedmanner but reduces the number of languages andinterviewers available. In contrast, third-party inter-pretation allows questionnaires to be administered inmany languages, but administration of the question-naire may be less consistent. Third-party interpreta-tion also does not allow for assessment of culturalequivalence, thereby potentially leading to measure-ment error. Both approaches are also relatively costly.Additionally, neither approach provides a completesolution to the problem of increasing survey participa-tion among people isolated by language.
There are several limitations to the current study. First,sample sizes in some counties limited the analysis to 1894of 3141 counties. Second, because information on key vari-ables such as race, ethnicity, and language spoken in thehousehold was not available at the individual level of nonresponding households, the analysis was conducted atan aggregate (county) level. Although aggregate-levelapproaches to studying racial and ethnic disparities havebeen encouraged by the U.S. Department of Health andHuman Services when individual-level data are not avail-able, future studies of survey participation could bestrengthened by surveys that are designed to collect dataon key variables from nonrespondents (4). Third, the highcorrelation between the race, ethnicity, and language variables for Asian and Hispanic individuals limited ourability to disentangle the effects on survey participation ofculture and language for these two groups.
Adequately identifying racial and ethnic disparities inhealth care and developing effective strategies to eliminatethese disparities depends on the availability of valid andreliable data. Considerations of race, ethnicity, accultura-tion, and language are critical to the success of such healthsurveillance efforts. Researchers need to infuse these ele-ments into their study designs, data-collection protocols,and data-processing routines. Indeed, several pilot studiesare now being conducted in conjunction with the BRFSS totry to address these issues. These studies are using alter-native sampling frames to reach individuals who are inac-cessible by landline telephones, multiple modes of surveydata collection, prenotification techniques tailored tominority racial and ethnic populations, surveys in languages other than English and Spanish, andcase-management techniques for preassigning likely non-English–speaking households to bilingual interview-ers. Such efforts are essential for meeting the challenges tohealth surveillance posed by the growing diversity of theU.S. population.
Author Information
Corresponding Author: Michael W. Link, PhD, Centersfor Disease Control and Prevention, 4770 Buford Hwy NE,Mail Stop K-66, Atlanta, GA 30341. Telephone: 770-488-5444. E-mail: [email protected].
Author Affiliations: Ali H. Mokdad, PhD, Herbert F.Stackhouse, MA, Nicole T. Flowers, MD, Centers for
VOLUME 3: NO. 1JANUARY 2006
www.cdc.gov/pcd/issues/2006/jan/05_0055.htm • Centers for Disease Control and Prevention 7
The opinions expressed by authors contributing to this journal do not necessarily reflect the opinions of the U.S. Department of Health and Human Services,the Public Health Service, the Centers for Disease Control and Prevention, or the authors’ affiliated institutions. Use of trade names is for identification only
and does not imply endorsement by any of the groups named above.

VOLUME 3: NO. 1JANUARY 2006
Disease Control and Prevention, Atlanta, Ga.
References
1. U.S. Department of Health and Human Services. Data2010: the Healthy People 2010 database [Internet].Hyattsville (MD): U.S. Department of Health andHuman Services, Centers for Disease Control andPrevention, National Center for Health Statistics;2004. Available from: URL: http://wonder.cdc.gov/data2010/.
2. Ver Ploeg M, Perrin E, editors; National ResearchCouncil. Eliminating health disparities: measurementand data needs. Washington (DC): NationalAcademies Press; 2004.
3. Perot RT, Youdelman M. Racial, ethnic, and primarylanguage data collection in the health care system: anassessment of federal policies and practices. New York:The Commonwealth Fund; 2001.
4. U.S. Department of Health and Human Services.Improving the collection and use of racial and ethnicdata in HHS [Internet]. Washington (DC): U.S.Department of Health and Human Services, HHSData Council; 1999 Dec. Available from: URL:http://www.aspe.hhs.gov/datacncl/RaceRpt/index.htm.
5. Pearcy JN, Keppel KG. A summary measure of healthdisparity. Public Health Rep 2002; 117(3):273-80.
6. Miller B, Lolonel L, Bernstein L, Young J Jr.Racial/ethnic patterns of cancer in the United States,1988-92. Bethesda (MD): National Cancer Institute;1996.
7. Adekoya N, Hopkins RS. Racial disparities in nation-ally notifiable diseases — United States, 2002. MMWR2005;54(01):9-11.
8. Ro M. Moving forward: addressing the health of AsianAmerican and Pacific Islander women. Am J PublicHealth 2002;92:516-19.
9. Centers for Disease Control and Prevention. Healthdisparities experienced by black or African Americans— United States. MMWR 2005;54(01):1-3.
10. Board of Health Sciences Policy, Institute of Medicine.Unequal treatment: confronting racial and ethnic dis-parities in health care. Washington (DC): NationalAcademies Press; 2003.
11. Srinivasan S, Guillermo T. Toward improved health:disaggregating Asian American and NativeHawaiian/Pacific Islander data. Am J Public Health2000;90:1731-4.
12. Hoyo C, Reid ML, Godley PA, Parrish T, Smith L,Gammon M. Barriers and strategies for sustained par-ticipation of African-American men in cohort studies.Ethn Dis 2003;13:470-6.
13. Harris Y, Gorelick PB, Samuels P, Bempong I. WhyAfrican Americans may not be participating in clinicaltrials. J Natl Med Assoc 1996;88:630-4.
14. Moorman PG, Newman B, Millikan RC, Tse CK,Sandler DP. Participation rates in a case-controlstudy: the impact of age, race, and race of interviewer.Ann Epidemiol 1999;9(3):188-95.
15. Williams DR, Neighbors HW, Jackson JS. Racial/eth-nic discrimination and health: findings from communi-ty studies. Am J Public Health 2003;93:200-8.
16. Millon-Underwood S, Sanders E, Davis M.Determinants of participation in state-of-the-art can-cer prevention, early detection/screening and treat-ment trials among African Americans. Cancer Nurs1993;16:25-33.
17. Corbie-Smith G,Thomas SB, St. George DM. Distrust,race, and research. Arch Intern Med2002;162(21):2458-63.
18. Hughes GD, Sellers DB, Fraser LB Jr, Knight B,Areghan GA. Barriers and strategies for sustainedparticipation of African-American men in cohort stud-ies. Ethn Dis 2003;13:534-6.
19. Hunt SM, Bhopal R. Self report in clinical and epi-demiological studies with non-English speakers: thechallenge of language and culture. J EpidemiolCommunity Health 2004;58:618-22.
20. Hunt S, Bhopal R. Self reports in research with non-English speakers. BMJ 2003;327:352-3.
21. Groves RM, Fowler FJ, Couper MP, Lepkowski JM,Singer E, Tourangeau R. Survey methodology. NewYork: John Wiley & Sons, Inc; 2004.
22. Holmes SA. Census Bureau linked to WWII intern-ment of Japanese-Americans [Internet]. New YorkTimes 2000 Mar 17 [cited 2005 April 04]. Availablefrom: URL: http://archives.nytimes.comes/archives/search.
23. Gamble VN. A legacy of distrust: African Americansand medical research. Am J Prev Med 1993;9:35-8.
24. Bell PA. Racial/ethnic homogeneity of neighborhoodsand variation in Census coverage of African Americans[Internet]. Washington (DC): U.S. Census Bureau.Available from: URL: http://www.census.gov/srd/papers/pdf/ev93-39.pdf.
25. Gudykunst WB, Kim YY. Communicating withstrangers: an approach to intercultural communica-
8 Centers for Disease Control and Prevention • www.cdc.gov/pcd/issues/2006/jan/05_0055.htm
The opinions expressed by authors contributing to this journal do not necessarily reflect the opinions of the U.S. Department of Health and Human Services,the Public Health Service, the Centers for Disease Control and Prevention, or the authors’ affiliated institutions. Use of trade names is for identification only
and does not imply endorsement by any of the groups named above.

tion. New York: The McGraw-Hill Companies; 1997.26. Institute of Medicine. Health literacy: a prescription to
end confusion. Washington (DC): National AcademiesPress; 2004.
27. U.S. Census Bureau. Trends in the 20th century[Internet]. Washington (DC): U.S. Census Bureau;2004 [cited 2005 Apr 4]. Available from: URL:http//www.census.gov.
28. McKinnon J. The black population in the UnitedStates: March 2002 [Internet]. Washington (DC): U.S.Census Bureau; 2003 [cited 2005 Apr 4]. Availablefrom: URL: http://www.census.gov.
29. Reeves T, Bennett C. The Asian and Pacific Islanderpopulation in the United States: March 2002[Internet]. Washington (DC): U.S. Census Bureau;2003 [cited 2005 Apr 4]. Available from: URL:http://www.census.gov.
30. Ramirez RR, de la Cruz GP. The Hispanic populationin the United States: March 2002 [Internet].Washington (DC): U.S. Census Bureau; 2003 [cited2005 Apr 4]. Available from: URL: http://www.census.gov.
31. Larsen LJ. The foreign-born population in the UnitedStates: 2003 [Internet]. Washington (DC): U.S. CensusBureau; 2004 [cited 2005 Apr 4]. Available from: URL:http://www.census.gov.
32. U.S. Census Bureau. Census 2000 summary file tech-nical documentation. Washington (DC): U.S. CensusBureau; 2004.
33. Shin HB, Bruno R. Language use and English-speak-ing ability: 2000 [Internet]. Washington (DC): U.S.Census Bureau; 2003 [cited 2005 Apr 4]. Availablefrom: URL: http://www.census.gov.
34. Centers for Disease Control and Prevention.Behavioral Risk Factor Surveillance System preva-lence tables, 2002-2003 [Internet]. Atlanta (GA):Centers for Disease Control and Prevention [cited 2005 Apr 4]. Available from: URL:https://www.cdc.gov/brfss.
35. Link MW. BRFSS response rates: which way is up? St.Louis (MO): Presentation from the Behavioral RiskFactor Surveillance System annual conference; 2003Feb.
36. Centers for Disease Control and Prevention.Behavioral Risk Factor Surveillance System question-naires and survey data [Internet]. Atlanta (GA):Centers for Disease Control and Prevention [cited 2005 Apr 4]. Available from: URL:http://www.cdc.gov/brfss.
37. American Association for Public Opinion Research.Standard definitions: final dispositions of case codesand outcome rates for surveys. Ann Arbor (MI):American Association for Public Opinion Research;2004.
38. Groves RM, Couper MP. Nonresponse in householdinterview surveys. New York: John Wiley & Sons, Inc;1998.
39. Link MW, Oldendick RW. Is call screening really aproblem? Public Opin Q 2004;63:577-89.
40. Ratzan SC, Parker RM. Introduction [Internet]. In:Health literacy. Bethesda (MD): U.S. National Libraryof Medicine, National Institutes of Health; 1990 Jan–1999 Oct. Available from: URL:http://www.nlm.nih.gov/pubs/cbm/hliteracy.html#15.
41. Amastae J, Elias-Olivares L. Spanish in the UnitedStates: sociolinguistic aspects. Cambridge: CambridgeUniversity Press; 1982.
42. Herdman M, Fox-Rushby J, Badia X. A model of equiv-alence in the cultural adaptation of HRQoL instru-ments: the universalist approach. Qual Life Res1998;7:323-35.
43. Herdman M, Fox-Rushby J, Badia X. ‘Equivalence’and the translation and adaptation of health-relatedquality of life questionnaires. Qual Life Res1997;6:237-47.
44. Hilton A, Skrutkowski M. Translating instrumentsinto other languages: development and testingprocesses. Cancer Nurs 2002;25(1):1-7.
45. Chang AM, Chau JP, Holroyd E. Translation of ques-tionnaires and issues of equivalence. J Adv Nurs 1999Feb;29(2):316-22.
46. Eyton J, Neuwirth G. Cross-cultural validity: ethno-centrism in health studies with special reference to theVietnamese. Soc Sci Med 1984;18(5):447-53.
47. Geisinger KF. Cross-cultural normative assessment:translation and adaptation issues influencing the nor-mative interpretation of assessment instruments.Psychol Assess 1994;(4):304-12.
48. Nicholson NS. Translation and interpretation. AnnuRev Applied Linguistics 1995;15:42-62.
49. Brown ER. Community participation and communitybenefit in large health surveys: enhancing quality, rel-evance, and use of the California Health InterviewSurvey. In: Cohen SB, Lepkowski JM, editors. EighthConference on Health Survey Research Methods.Hyattsville (MD): National Center for HealthStatistics; 2004. p. 49-54.
50. Language Line Services. Over-the-phone language
VOLUME 3: NO. 1JANUARY 2006
www.cdc.gov/pcd/issues/2006/jan/05_0055.htm • Centers for Disease Control and Prevention 9
The opinions expressed by authors contributing to this journal do not necessarily reflect the opinions of the U.S. Department of Health and Human Services,the Public Health Service, the Centers for Disease Control and Prevention, or the authors’ affiliated institutions. Use of trade names is for identification only
and does not imply endorsement by any of the groups named above.

VOLUME 3: NO. 1JANUARY 2006
interpretation [Internet]. Monterey (CA): LanguageLine Services [cited 2005 Apr 4]. Available from: URL:http://www.languageline.com .
51. Murray MC, Battaglia M, Cardoni J. Enhancing datacollection from “other language” households. In: CohenSB, Lepkowski JM, editors. Eighth Conference onHealth Survey Research Methods. Hyattsville (MD):National Center for Health Statistics; 2004. p. 109-14.
Tables
Table 1. Major Languages Spoken by
English-Language–Isolated Groupsa
Spanish Spanish, Ladino
Other Indo-European Most languages of Europe and the Indic languages languages of India, including the Germanic languages, such
as German, Yiddish, and Dutch; the Scandinavian languages, such as Swedish and Norwegian; the Romance languages, such as French, Italian, and Portuguese; the Slavic languages, such as Russian, Polish, and Serbo-Croatian; the Indic languages, such as Hindi, Gujarathi, Punjabi, and Urdu; Celtic languages; Greek; Baltic languages; and Iranian languages.
Asian and Pacific Chinese; Korean; Japanese; Vietnamese; Hmong Island languages Khmer; Lao; Thai; Tagalog or Pilipino; the
Dravidian languages of India, such as Telegu, Tamil, and Malayalam; and other languages of Asia and the Pacific, including the Philippine, Polynesian, and Micronesian languages.
aSource: Shin and Bruno (33).
10 Centers for Disease Control and Prevention • www.cdc.gov/pcd/issues/2006/jan/05_0055.htm
The opinions expressed by authors contributing to this journal do not necessarily reflect the opinions of the U.S. Department of Health and Human Services,the Public Health Service, the Centers for Disease Control and Prevention, or the authors’ affiliated institutions. Use of trade names is for identification only
and does not imply endorsement by any of the groups named above.
Language Group Major Languages

Table 2. Effects of Race, Linguistic Isolation, and Other Variables on County-level Participation Rates (N = 1894), 2003Behavioral Risk Factor Surveillance System
% Black residents >18 y –0.03 .001 –0.18 .001 –0.13 .001 –0.06 .001 <0.01 .07 0.06 .001
(0.01) (0.02) (0.01) (0.01) (<0.01) (0.01)
% Spanish-language–only –0.11 .04 –0.92 .001 –0.58 .001 –0.26 .001 0.12 .001 –0.03 .71
households (0.05) (0.11) (0.09) (0.04) (0.01) (0.08)
% Asian-language–only –0.48 .03 –0.98 .03 –0.24 .53 –0.21 .24 0.14 .001 –1.90 .001households (0.22) (0.45) (0.38) (0.18) (0.03) (0.31)
% Indo-European- –0.12 .44 –1.36 .001 –1.39 .001 –0.64 .001 0.12 .001 0.82 .001language–only households (0.15) (0.31) (0.26) (0.12) (0.02) (0.21)
% Calls that reached 0.11 .001 –0.19 .001 0.10 .001 0.04 .001 <–0.01 .001 –0.02 .29answering machines (0.01) (0.03) (0.02) (0.01) (<0.01) (0.02)
% Households with heads –0.04 .001 –0.13 .001 –0.05 .01 –0.05 .001 <0.01 .02 0.09 .001who commute >30 (0.01) (0.02) (0.02) (0.01) (<0.01) (0.02)minutes one-way to work
% Households with income –0.18 .001 –0.30 .001 –0.18 .001 –0.17 .001 <0.01 .11 0.22 .001>$50,000 (0.01) (0.03) (0.02) (0.01) (<0.01) (0.02)
% Adults aged >25 y with –0.06 .007 –0.06 .16 –0.04 .24 –0.04 .013 <–0.01 .51 0.15 .001<high school education (0.02) (0.04) (0.04) (0.01) (<0.01) (0.03)
aResolution rate = (number of cases determined to be households/total number of cases) × 100%. Intercept: ß (SE) = 91.01 (0.81); P = .001.Adjusted R2 = 0.18.bScreening rate = (number of households where eligibility is determined/total number of households) × 100%. Intercept: (SE) = 93.65 (1.66); P =.001. Adjusted R2 = 0.30.cCooperation rate = (number of completed interviews/number of confirmed eligible households) × 100%. Intercept: ß (SE) = 83.24 (1.38); P = .001.Adjusted R2 = 0.16.dResponse rate = (number of completed interviews/estimated total number of eligible households) × 100%. Intercept: ß (SE) = 43.15 (0.64); P = .001.Adjusted R2 = 0.31.eLanguage-barrier rate = (number of cases with language-problem code/total number of cases) × 100%. Intercept: ß (SE) = 0.06 (0.09); P = .54.Adjusted R2 = 0.27.fRefusal rate = (number of cases with refusal code/total number of cases) × 100%. Intercept: ß (SE) = 7.31 (1.14); P = .001. Adjusted R2 = 0.17.gß indicates ordinary least squares regression coefficient.
VOLUME 3: NO. 1JANUARY 2006
www.cdc.gov/pcd/issues/2006/jan/05_0055.htm • Centers for Disease Control and Prevention 11
The opinions expressed by authors contributing to this journal do not necessarily reflect the opinions of the U.S. Department of Health and Human Services,the Public Health Service, the Centers for Disease Control and Prevention, or the authors’ affiliated institutions. Use of trade names is for identification only
and does not imply endorsement by any of the groups named above.
Language-Resolution Screening Cooperation Response Barrier Refusal Ratea Rateb Ratec Rated Ratee Ratef
ßg ßg ßg ßg ßg ßgCharacteristic (SE) P (SE) P (SE) P (SE) P (SE) P (SE) P

VOLUME 3: NO. 1JANUARY 2006
Table 3. Maximum Impact of Race and Linguistic Isolation on County-level Participation Rates, 2003 Behavioral Risk Factor
Surveillance Systema
% Black residents 77.4 –0.03 –2.3 –13.9 –10.1 –4.6 0.0 4.6>18 y
% Spanish- 26.8 –0.11 –2.9 –24.7 –15.5 –7.0 3.2 0.0language–only households
% Asian-language– 8.7 –0.48 –4.2 –8.5 0.0 0.0 1.2 –16.5only households
% Indo-European- 10.8 –0.12 0.0 –14.7 –15.0 –6.9 1.3 8.9language–only households
aImpact of variable = maximum county-level population parameter × ß for population characteristic (from Table 1). The impact of variables that were notstatistically significant (P > .05) in Table 2 are assumed to have no impact and are set to zero in this table. bMaximum population parameter value = maximum county-level value for population characteristic. cß indicates ordinary least squares regression coefficient.dResolution rate = (number of cases determined to be households/total number of cases) × 100%.eScreening rate = (number of households where eligibility is determined/total number of households) × 100%.fCooperation rate = (number of completed interviews/number of confirmed eligible households) × 100%.gResponse rate = (number of completed interviews/estimated total number of eligible households) × 100%.hLanguage-barrier rate = (number of cases with language-problem code/total number of cases) × 100%.iRefusal rate = (number of cases with refusal code/total number of cases) × 100%.
12 Centers for Disease Control and Prevention • www.cdc.gov/pcd/issues/2006/jan/05_0055.htm
The opinions expressed by authors contributing to this journal do not necessarily reflect the opinions of the U.S. Department of Health and Human Services,the Public Health Service, the Centers for Disease Control and Prevention, or the authors’ affiliated institutions. Use of trade names is for identification only
and does not imply endorsement by any of the groups named above.
Maximum Measures of Survey ParticipationPopulationParameter ßc for Resolution Screening Cooperation Response Language- Refusal
Valueb Population Rated Ratee Ratef Rateg Barrier Rateh RateiCharacteristic (%) Characteristic (%) (%) (%) (%) (%) (%)