Embed Size (px)
Citation preview

J Med Dent Sci 2011; 58: 89-96
Corresponding Author: Miho KusanagiGraduate School of Health Care Sciences, Tokyo Medical and Dental University 1-5-45 Yushima Bunkyo-ku, Tokyo 113-8519, JapanTel: +03-5803-5342 Fax: +03-5803-5342E-mail: [email protected] January 31;Accepted March 11, 2011
Original Article
Effect of early intervention using state modulation and cue reading on mother-infant interactions in preterm infants and their mothers in Japan
Miho Kusanagi1), Taiko Hirose1), Kumi Mikuni2) and Motoko Okamitsu1)
1) Graduate School of Health Care Sciences. Tokyo Medical and Dental University2) School of Nursing & Social Services. Health Sciences University of Hokkaido
This study examined the effects of ear ly intervention on mothers and their preterm infants. Intervention aimed to facilitate mother-infant interaction by enhancing the mother’s ability to modulate her infant’s state and to read infant cues. Specifically, the intervention consisted of a nurse researcher visiting the Neonatal Intensive Care Unit (NICU) before each infant was discharged, and conducting post-discharge home visits until the infant reached a corrected age of 60 weeks. For research design purposes, mother-infant dyads were placed into either (1) an Intensive Intervention Group (IIG) or (2) a Mild Intervention Group (MIG). The outcomes of the groups were then compared. The effects of early intervention were rated by examining mother-infant interaction and the durations of infant sleep and crying. Despite individual differences, there were more improved interaction scores at Time 1 in IIG members that had recorded lower interaction scores earlier than those of MIG. A lower frequency of night crying was also recorded from the IIG. The results implied that interventions teaching state-modulation methods and cue reading to the mothers should be started while their infants are in the NICU.
Key words: early intervention, mother-infant interaction, preterm infant, NCATS
1. Introduction
When infants and mothers both adapt their behavior to one another, a smooth and positive interaction takes place1. In this situation, the mother has the ability to read her infant’s behaviors/cues sensitively and to respond accordingly, and the infant responds to the mother; in this way, they modulate their behaviors through interaction. However, the quality of interaction is reduced when the adaptation process is hindered. In the Barnard Model 2, both mother and infant share responsibility for their interactions. Risk factors can affect the mothers’ capability for sensitivity and responsiveness. Risk factors for infants include prematurity (<37 weeks), low birth weight (<2,500 g), disabilities, and difficult temperaments. Preterm infants often demonstrate low responsiveness to their mothers2. Due to their prematurity, such infants also have difficulty interacting with their mothers. This can lead to mothers becoming less responsive and less sensitive to their infants, resulting in disrupted mother-child relationships. In the 1980s, several early intervention projects were conducted in the US. For example, some of the programs were directed at improving difficult family lives caused by poverty and other adverse factors such as adolescent pregnancy or abuse by providing early education programs and by supporting preterm infants and their families3. Early intervention studies of preterm and other at-risk infants in the US involved conducting home visits and promoting mother-infant interactions, attachment, and child development 4-7. The studies were based on the premise that nurses are the most optimal coordinators and helpers in the intervention, so they are the most appropriate assistants to facilitate the intervention and collaboration with multiple care providers to help mothers and their infants.

90 J Med Dent SciM. Kusanagi et al.
In Japan, early intervention projects for preterm infants have been conducted since the early 1990s8. However, most projects were not initiated by nurses and have seldom measured the effects of early interventions by nurses. In the literature, little research has focused on mother-infant interactions. Neonatal Intensive Care Unit (NICU) infants and mothers need more support than do healthy, full-term infants and their parents because NICU infants and their mothers develop a mother-infant relationship in an unfamiliar environment. Previous research has suggested that even mothers who had healthy preterm infants experienced parenting anxiety8. In Japan, many mothers with preterm infants strongly desire more frequent home visits than those with full-term infants do, because mothers with preterm infants tend to experience more anxiety, stress, and difficulty in parenting9. Most mothers seem to be more comfortable and receptive to receiving help if nurses visit their homes after NICU discharge. A plausible study reported positive outcomes of continuous support provided by nurses according to preterm infants’ and their mothers’ needs; this highlighted the critical role of nurses in helping mothers with parenting by focusing on building mother-infant relationships4; therefore, intervention by nurses should start in the NICU and continue after discharge. This study was designed to determine how an early intervention regimen performed by a nurse promotes (a) interactions between mothers and preterm infants, (b) parenting, and (c) infant development and reduces (d) parenting stress. Thus, 4 hypotheses (H) were proposed: H1. Mother-infant interaction in the Intensive
Intervention Group (IIG) is better than that in the Mild Intervention Group (MIG) at the corrected ages of 46 weeks (Time 1) and 60 weeks (Time 2).
H2. Mothers in the IIG can modulate their infant’s states better than mothers in the MIG can.
H3. Physical growth and cognitive development of the IIG infants are better than that of MIG infants at Times 1 and 2.
H4. Parenting stress for the IIG mothers is lower than that for MIG mothers.
2. Materials and Methods
Materials Infant cues are non-verbal, engagement/disengagement communication signs that infants and young children
use. An infant state is classified into 6 states: Quiet Sleep, Active Sleep, Drowsy, Quiet Alert, Active Alert, and Crying. The state in which the child is most attentive and most open to learning is the Quiet Alert state. This is the optimal state in which to undertake such activities and teaching. If a mother can identify the 6 states, she can easily understand whether her infant is sleeping or awake. Based on the premise that mothers can learn infant cues and state modulation, which is theorized to help smooth an infant’s transition from wake to sleep and vice versa, this can facilitate self-regulation with their infant (a competency that enables soothing of oneself when an infant is in distress or excited).
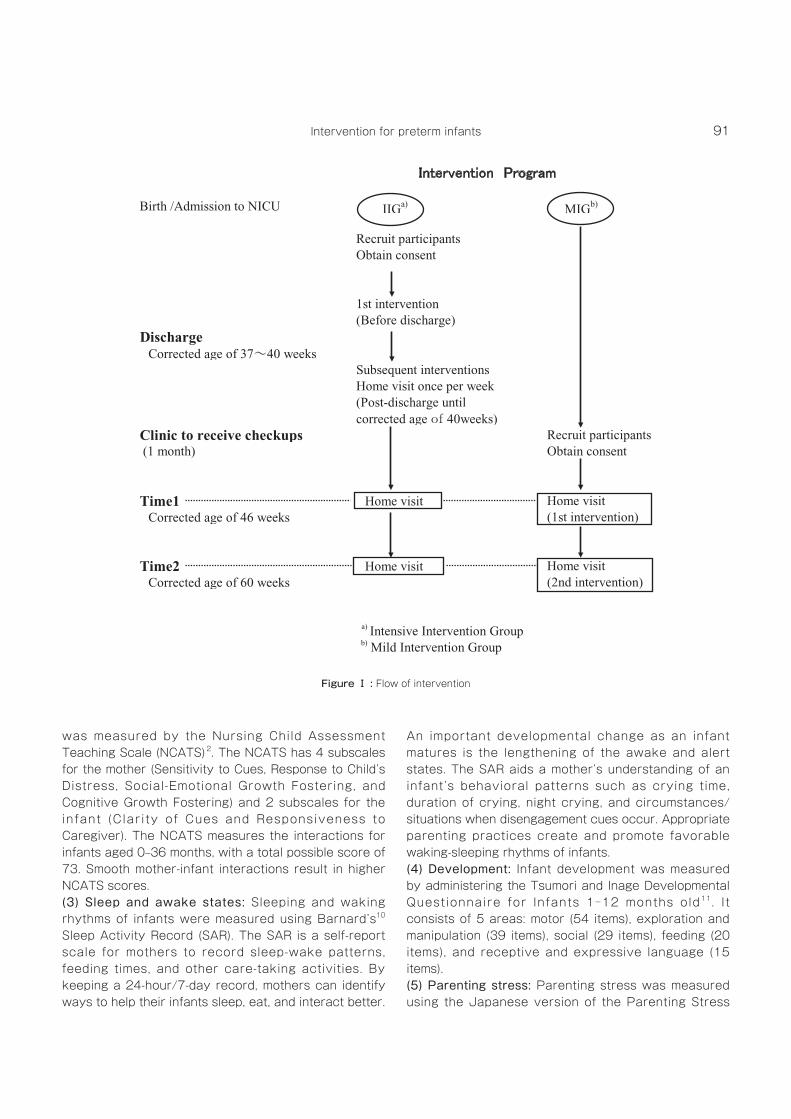
Methods Mother-infant dyads of the IIG were provided with the nurse’s service when the infant was in NICU, while mothers in the MIG received the service when their infants reached a corrected age of 46 weeks (the number of weeks of age a preterm infant would be when calculated from the expected date of delivery). In particular, a nurse researcher contacted mothers of infants in the NICU before an infant was discharged and at the outpatient clinic to carry out checkups after discharge. The nurse researcher conducted home visits after discharge until the infant reached the corrected age of 60 weeks in order to assist mothers in using state modulation and infant cue reading. Additionally, the nurse researcher worked closely with mothers to provide support and advice, as well as to listen to the mothers’ concerns about their infants and parenting.
1) Participants Participants were 51 mother-infant dyads in an urban area of Japan. Inclusion criteria for infants were (a) singleton, (b) preterm birth (<37 weeks), (c) low birth weight (<2,500 g), (d) first-born baby, (e) oral feeding, and (f) no medical complications. The Ethics Committee of Tokyo Medical and Dental University granted approval. Mothers were briefed on the study and provided written informed consent for themselves and their infant.
2) Variables and Measures(1) Demographic data: Mothers were asked to provide their age, and their infant’s gestational age and birth weight were obtained. Other information was collected from medical and nursing charts. Data collection was conducted with the mother’s consent.(2) Mother-infant interaction: Mother-infant interaction
91Intervention for preterm infants
was measured by the Nursing Child Assessment Teaching Scale (NCATS)2. The NCATS has 4 subscales for the mother (Sensitivity to Cues, Response to Child’s Distress, Social-Emotional Growth Fostering, and Cognitive Growth Fostering) and 2 subscales for the infant (Clarity of Cues and Responsiveness to Caregiver). The NCATS measures the interactions for infants aged 0–36 months, with a total possible score of 73. Smooth mother-infant interactions result in higher NCATS scores.(3) Sleep and awake states: Sleeping and waking rhythms of infants were measured using Barnard’s10 Sleep Activity Record (SAR). The SAR is a self-report scale for mothers to record sleep-wake patterns, feeding times, and other care-taking activities. By keeping a 24-hour/7-day record, mothers can identify ways to help their infants sleep, eat, and interact better.
An important developmental change as an infant matures is the lengthening of the awake and alert states. The SAR aids a mother’s understanding of an infant’s behavioral patterns such as crying time, duration of crying, night crying, and circumstances/situations when disengagement cues occur. Appropriate parenting practices create and promote favorable waking-sleeping rhythms of infants. (4) Development: Infant development was measured by administering the Tsumori and Inage Developmental Questionnaire for Infants 1‒12 months old11. It consists of 5 areas: motor (54 items), exploration and manipulation (39 items), social (29 items), feeding (20 items), and receptive and expressive language (15 items).(5) Parenting stress: Parenting stress was measured using the Japanese version of the Parenting Stress
������������ �������
Birth /Admission to NICU IIGa) MIGb)
Recruit participantsObtain consent
1st intervention(Before discharge)
Discharge Corrected age of 37~40 weeks
Subsequent interventionsHome visit once per week(Post-discharge untilcorrected age of 40weeks)
Clinic to receive checkups Recruit participants (1 month) Obtain consent
Time1 Home visit Home visit Corrected age of 46 weeks (1st intervention)
Time2 Home visit Home visit Corrected age of 60 weeks (2nd intervention)
a) Intensive Intervention Groupb) Mild Intervention Group
a)
b)
Figure Ⅰ : Flow of intervention
92 J Med Dent SciM. Kusanagi et al.
Index (PSI) 12. The Japanese version of PSI was adapted from Abidin’s PSI and has 78 items: 8 parent subscales (40 items) and 7 child subscales (38 items). The higher the reported score, the higher the level of parenting stress.
3) Procedures Group assignment: IIG subjects gave consent to be involved in the study groups when their infants were still in the NICU, whereas MIG subjects gave consent to be involved in the study when the parents and infants visited the outpatient clinic for checkups. Eighteen mothers expressed a desire to be assigned to MIG although they were recruited at the NICU, and their request was accommodated. As indicated, the IIG dyads were provided with the nurse’s services when the infant was in the NICU, while those in the MIG were provided with the service at the corrected infant age of 46 weeks. The intervention program was conducted by the nurse researcher. The intervention included (1) coaching on state modulation
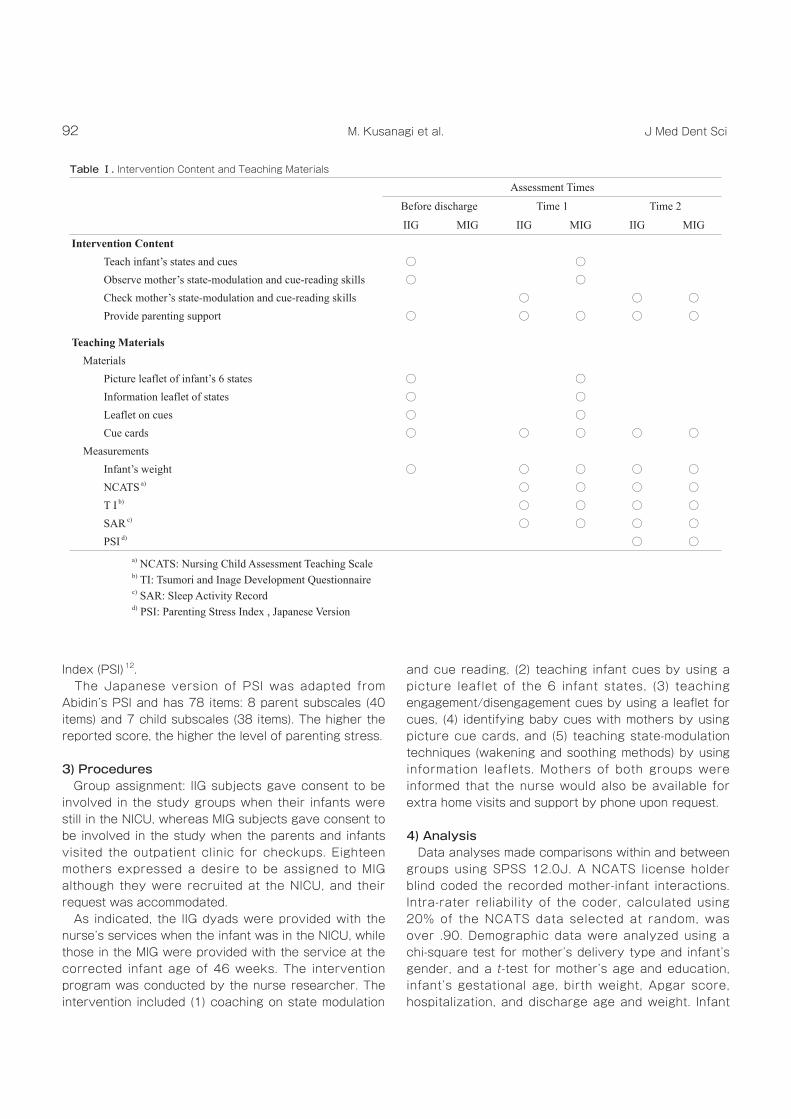
and cue reading, (2) teaching infant cues by using a picture leaflet of the 6 infant states, (3) teaching engagement/disengagement cues by using a leaflet for cues, (4) identifying baby cues with mothers by using picture cue cards, and (5) teaching state-modulation techniques (wakening and soothing methods) by using information leaflets. Mothers of both groups were informed that the nurse would also be available for extra home visits and support by phone upon request.
4) Analysis Data analyses made comparisons within and between groups using SPSS 12.0J. A NCATS license holder blind coded the recorded mother-infant interactions. Intra-rater reliability of the coder, calculated using 20% of the NCATS data selected at random, was over .90. Demographic data were analyzed using a chi-square test for mother’s delivery type and infant’s gender, and a t-test for mother’s age and education, infant’s gestational age, birth weight, Apgar score, hospitalization, and discharge age and weight. Infant
Assessment Times
Before discharge Time 1 Time 2
IIG MIG IIG MIG IIG MIGIntervention Content
Teach infant’s states and cues ○ ○Observe mother’s state-modulation and cue-reading skills ○ ○Check mother’s state-modulation and cue-reading skills ○ ○ ○Provide parenting support ○ ○ ○ ○ ○
Teaching MaterialsMaterials
Picture leaflet of infant’s 6 states ○ ○Information leaflet of states ○ ○Leaflet on cues ○ ○Cue cards ○ ○ ○ ○ ○
MeasurementsInfant’s weight ○ ○ ○ ○ ○NCATS a) ○ ○ ○ ○T I b) ○ ○ ○ ○SAR c) ○ ○ ○ ○PSI d) ○ ○
a) NCATS: Nursing Child Assessment Teaching Scaleb) TI: Tsumori and Inage Development Questionnairec) SAR: Sleep Activity Recordd) PSI: Parenting Stress Index , Japanese Version
Table Ⅰ. Intervention Content and Teaching Materials
93Intervention for preterm infants
development and Parenting Stress Scale scores were tested with the Mann-Whitney U-test. Between and within-group changes of mother-infant interactions and infant sleep and crying were compared by t-test. The F-test examined the variances in the mother‒infant interaction scores between the groups. Significance was set at 5%, and marginal tendency was indicated at 10%, although not considered significant.
3. Results
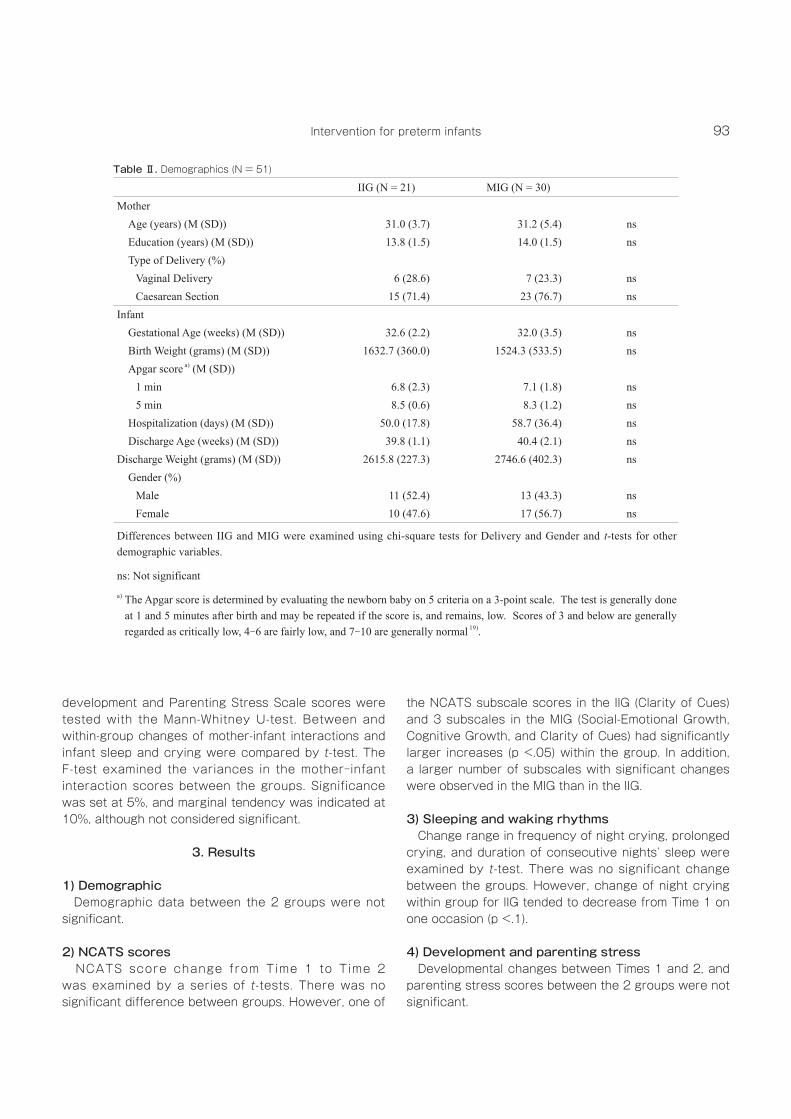
1) Demographic Demographic data between the 2 groups were not significant.
2) NCATS scores NCATS score change from Time 1 to Time 2 was examined by a series of t -tests. There was no significant difference between groups. However, one of
the NCATS subscale scores in the IIG (Clarity of Cues) and 3 subscales in the MIG (Social-Emotional Growth, Cognitive Growth, and Clarity of Cues) had significantly larger increases (p <.05) within the group. In addition, a larger number of subscales with significant changes were observed in the MIG than in the IIG.
3) Sleeping and waking rhythms Change range in frequency of night crying, prolonged crying, and duration of consecutive nights’ sleep were examined by t-test. There was no significant change between the groups. However, change of night crying within group for IIG tended to decrease from Time 1 on one occasion (p <.1).
4) Development and parenting stress Developmental changes between Times 1 and 2, and parenting stress scores between the 2 groups were not significant.
IIG (N = 21) MIG (N = 30)Mother
Age (years) (M (SD)) 31.0 (3.7) 31.2 (5.4) nsEducation (years) (M (SD)) 13.8 (1.5) 14.0 (1.5) nsType of Delivery (%)
Vaginal Delivery 6 (28.6) 7 (23.3) nsCaesarean Section 15 (71.4) 23 (76.7) ns
InfantGestational Age (weeks) (M (SD)) 32.6 (2.2) 32.0 (3.5) nsBirth Weight (grams) (M (SD)) 1632.7 (360.0) 1524.3 (533.5) nsApgar score a) (M (SD))
1 min 6.8 (2.3) 7.1 (1.8) ns5 min 8.5 (0.6) 8.3 (1.2) ns
Hospitalization (days) (M (SD)) 50.0 (17.8) 58.7 (36.4) nsDischarge Age (weeks) (M (SD)) 39.8 (1.1) 40.4 (2.1) ns
Discharge Weight (grams) (M (SD)) 2615.8 (227.3) 2746.6 (402.3) nsGender (%)
Male 11 (52.4) 13 (43.3) nsFemale 10 (47.6) 17 (56.7) ns
Differences between IIG and MIG were examined using chi-square tests for Delivery and Gender and t-tests for other demographic variables.
ns: Not significant
a) The Apgar score is determined by evaluating the newborn baby on 5 criteria on a 3-point scale. The test is generally done at 1 and 5 minutes after birth and may be repeated if the score is, and remains, low. Scores of 3 and below are generally regarded as critically low, 4-6 are fairly low, and 7-10 are generally normal 19).
Table Ⅱ. Demographics (N = 51)
94 J Med Dent SciM. Kusanagi et al.
4. Discussion
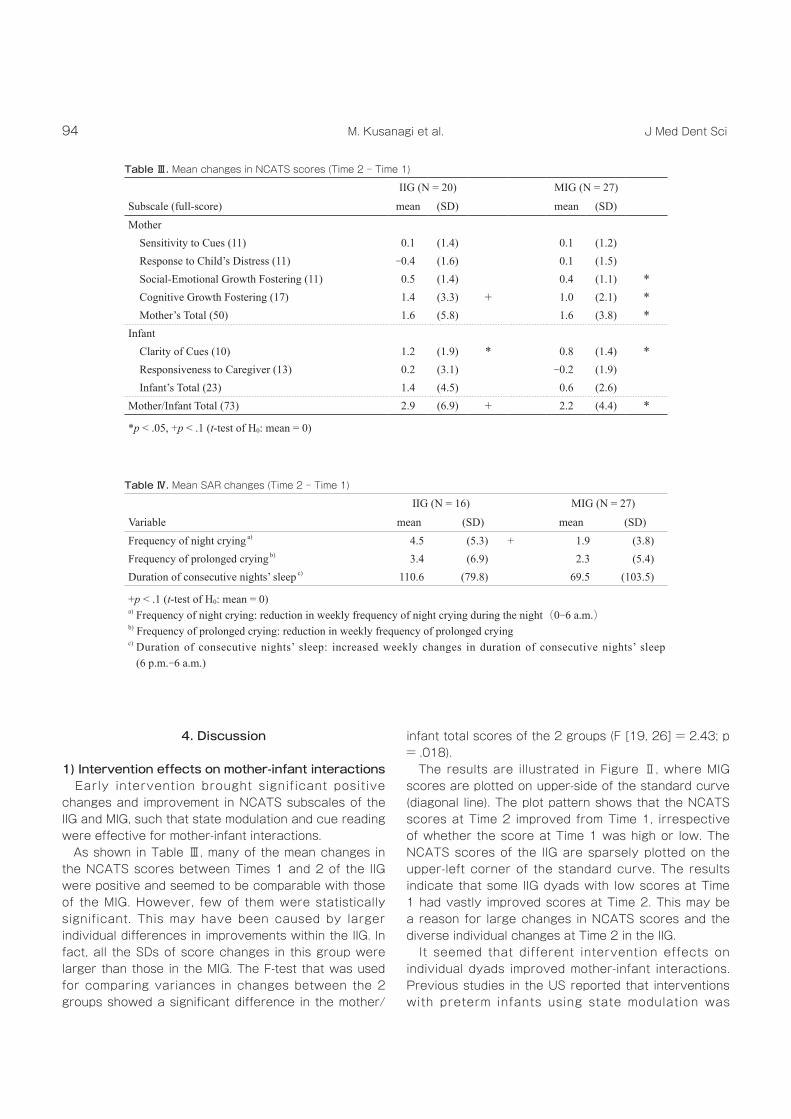
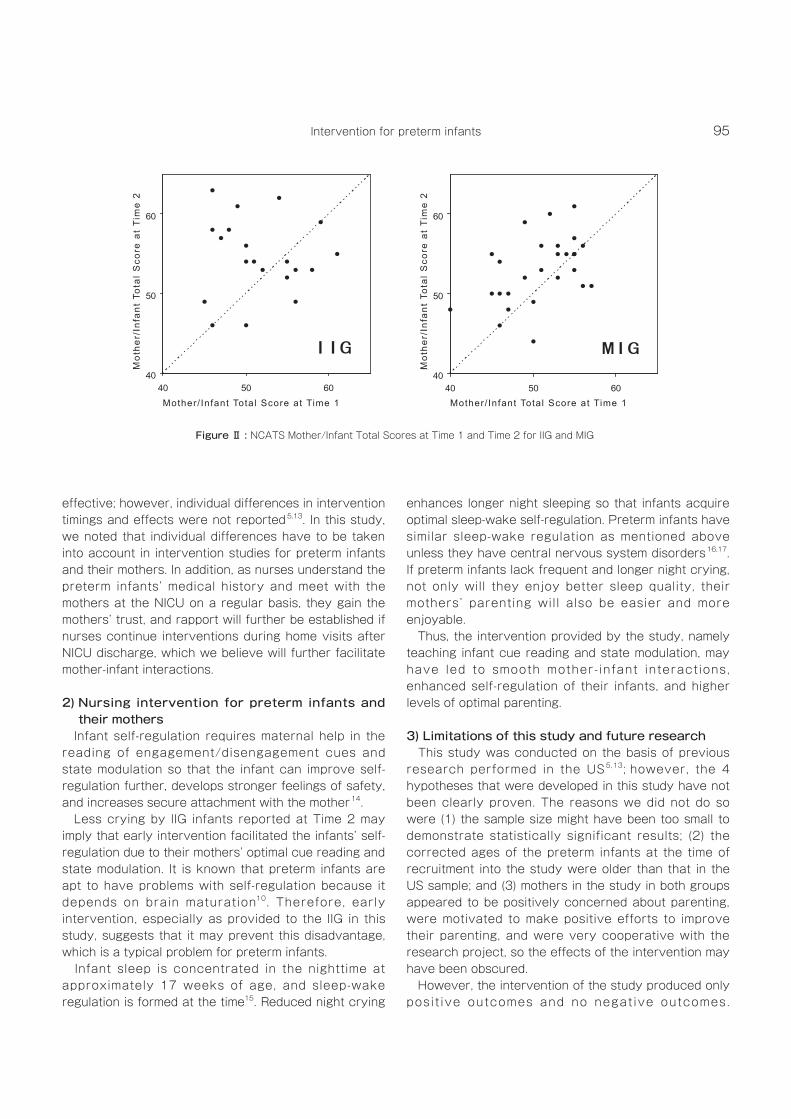
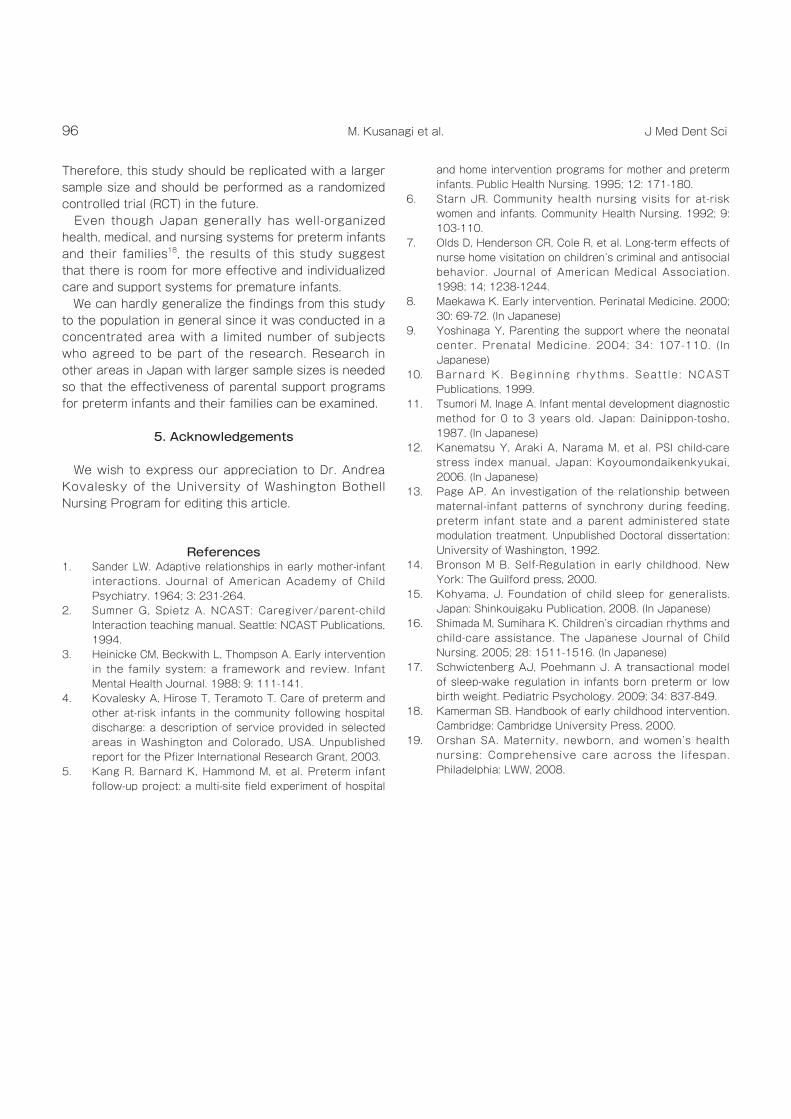
1) Intervention effects on mother-infant interactions Early intervention brought significant positive changes and improvement in NCATS subscales of the IIG and MIG, such that state modulation and cue reading were effective for mother-infant interactions. As shown in Table Ⅲ, many of the mean changes in the NCATS scores between Times 1 and 2 of the IIG were positive and seemed to be comparable with those of the MIG. However, few of them were statistically significant. This may have been caused by larger individual differences in improvements within the IIG. In fact, all the SDs of score changes in this group were larger than those in the MIG. The F-test that was used for comparing variances in changes between the 2 groups showed a significant difference in the mother/
infant total scores of the 2 groups (F [19, 26] = 2.43; p = .018). The results are illustrated in Figure Ⅱ, where MIG scores are plotted on upper-side of the standard curve (diagonal line). The plot pattern shows that the NCATS scores at Time 2 improved from Time 1, irrespective of whether the score at Time 1 was high or low. The NCATS scores of the IIG are sparsely plotted on the upper-left corner of the standard curve. The results indicate that some IIG dyads with low scores at Time 1 had vastly improved scores at Time 2. This may be a reason for large changes in NCATS scores and the diverse individual changes at Time 2 in the IIG. It seemed that different intervention effects on individual dyads improved mother-infant interactions. Previous studies in the US reported that interventions with preterm infants using state modulation was
IIG (N = 16) MIG (N = 27)
Variable mean (SD) mean (SD)Frequency of night crying a) 4.5 (5.3) + 1.9 (3.8)Frequency of prolonged crying b) 3.4 (6.9) 2.3 (5.4)Duration of consecutive nights’ sleep c) 110.6 (79.8) 69.5 (103.5)
+p < .1 (t-test of H0: mean = 0)a) Frequency of night crying: reduction in weekly frequency of night crying during the night(0-6 a.m.)b) Frequency of prolonged crying: reduction in weekly frequency of prolonged crying c) Duration of consecutive nights’ sleep: increased weekly changes in duration of consecutive nights’ sleep
(6 p.m.-6 a.m.)
IIG (N = 20) MIG (N = 27)
Subscale (full-score) mean (SD) mean (SD)Mother
Sensitivity to Cues (11) 0.1 (1.4) 0.1 (1.2)Response to Child’s Distress (11) -0.4 (1.6) 0.1 (1.5)Social-Emotional Growth Fostering (11) 0.5 (1.4) 0.4 (1.1) *Cognitive Growth Fostering (17) 1.4 (3.3) + 1.0 (2.1) *Mother’s Total (50) 1.6 (5.8) 1.6 (3.8) *
InfantClarity of Cues (10) 1.2 (1.9) * 0.8 (1.4) *Responsiveness to Caregiver (13) 0.2 (3.1) -0.2 (1.9)Infant’s Total (23) 1.4 (4.5) 0.6 (2.6)
Mother/Infant Total (73) 2.9 (6.9) + 2.2 (4.4) *
*p < .05, +p < .1 (t-test of H0: mean = 0)
Table Ⅲ. Mean changes in NCATS scores (Time 2︲Time 1)
Table Ⅳ. Mean SAR changes (Time 2︲Time 1)
95Intervention for preterm infants
effective; however, individual differences in intervention timings and effects were not reported5,13. In this study, we noted that individual differences have to be taken into account in intervention studies for preterm infants and their mothers. In addition, as nurses understand the preterm infants’ medical history and meet with the mothers at the NICU on a regular basis, they gain the mothers’ trust, and rapport will further be established if nurses continue interventions during home visits after NICU discharge, which we believe will further facilitate mother-infant interactions.
2) Nursing intervention for preterm infants and their mothers
Infant self-regulation requires maternal help in the reading of engagement/disengagement cues and state modulation so that the infant can improve self-regulation further, develops stronger feelings of safety, and increases secure attachment with the mother14. Less crying by IIG infants reported at Time 2 may imply that early intervention facilitated the infants’ self-regulation due to their mothers’ optimal cue reading and state modulation. It is known that preterm infants are apt to have problems with self-regulation because it depends on brain maturation10. Therefore, early intervention, especially as provided to the IIG in this study, suggests that it may prevent this disadvantage, which is a typical problem for preterm infants. Infant sleep is concentrated in the nighttime at approximately 17 weeks of age, and sleep-wake regulation is formed at the time15. Reduced night crying
enhances longer night sleeping so that infants acquire optimal sleep-wake self-regulation. Preterm infants have similar sleep-wake regulation as mentioned above unless they have central nervous system disorders16,17. If preterm infants lack frequent and longer night crying, not only will they enjoy better sleep quality, their mothers’ parenting will also be easier and more enjoyable. Thus, the intervention provided by the study, namely teaching infant cue reading and state modulation, may have led to smooth mother- infant interactions, enhanced self-regulation of their infants, and higher levels of optimal parenting.
3) Limitations of this study and future research This study was conducted on the basis of previous research performed in the US5,13; however, the 4 hypotheses that were developed in this study have not been clearly proven. The reasons we did not do so were (1) the sample size might have been too small to demonstrate statistically significant results; (2) the corrected ages of the preterm infants at the time of recruitment into the study were older than that in the US sample; and (3) mothers in the study in both groups appeared to be positively concerned about parenting, were motivated to make positive efforts to improve their parenting, and were very cooperative with the research project, so the effects of the intervention may have been obscured. However, the intervention of the study produced only posit ive outcomes and no negative outcomes.
40
50
60
40 50 60Mot her / I nf ant Tot al Scor e at Ti me 1
Moth
er/I
nfan
t To
tal
Scor
e at
Tim
e 2
40
50
60
40 50 60Mot her / I nf ant Tot al Scor e at Ti me 1
Moth
er/I
nfan
t To
tal
Scor
e at
Tim
e 2
Figure Ⅱ : NCATS Mother/Infant Total Scores at Time 1 and Time 2 for IIG and MIG
Mot
her/
Infa
nt T
otal
Sco
re a
t T
ime
2
Mot
her/
Infa
nt T
otal
Sco
re a
t T
ime
2
Mother/ Infant Total Score at Time 1 Mother/ Infant Total Score at Time 1
96 J Med Dent SciM. Kusanagi et al.
Therefore, this study should be replicated with a larger sample size and should be performed as a randomized controlled trial (RCT) in the future. Even though Japan generally has well-organized health, medical, and nursing systems for preterm infants and their families18, the results of this study suggest that there is room for more effective and individualized care and support systems for premature infants. We can hardly generalize the findings from this study to the population in general since it was conducted in a concentrated area with a limited number of subjects who agreed to be part of the research. Research in other areas in Japan with larger sample sizes is needed so that the effectiveness of parental support programs for preterm infants and their families can be examined.
5. Acknowledgements
We wish to express our appreciation to Dr. Andrea Kovalesky of the University of Washington Bothell Nursing Program for editing this article.
References1. Sander LW. Adaptive relationships in early mother-infant
interactions. Journal of American Academy of Child Psychiatry. 1964; 3: 231-264.
2. Sumner G, Spietz A. NCAST: Caregiver/parent-child Interaction teaching manual. Seattle: NCAST Publications, 1994.
3. Heinicke CM, Beckwith L, Thompson A. Early intervention in the family system: a framework and review. Infant Mental Health Journal. 1988; 9: 111-141.
4. Kovalesky A, Hirose T, Teramoto T. Care of preterm and other at-risk infants in the community following hospital discharge: a description of service provided in selected areas in Washington and Colorado, USA. Unpublished report for the Pfizer International Research Grant, 2003.
5. Kang R, Barnard K, Hammond M, et al. Preterm infant follow-up project: a multi-site field experiment of hospital
and home intervention programs for mother and preterm infants. Public Health Nursing. 1995; 12: 171-180.
6. Starn JR. Community health nursing visits for at-risk women and infants. Community Health Nursing. 1992; 9: 103-110.
7. Olds D, Henderson CR, Cole R, et al. Long-term effects of nurse home visitation on children’s criminal and antisocial behavior. Journal of American Medical Association. 1998; 14; 1238-1244.
8. Maekawa K. Early intervention. Perinatal Medicine. 2000; 30: 69-72. (In Japanese)
9. Yoshinaga Y, Parenting the support where the neonatal center. Prenatal Medicine. 2004; 34: 107-110. (In Japanese)
10. Barnard K. Beginning rhythms. Seatt le : NCAST Publications, 1999.
11. Tsumori M, Inage A. Infant mental development diagnostic method for 0 to 3 years old. Japan: Dainippon-tosho, 1987. (In Japanese)
12. Kanematsu Y, Araki A, Narama M, et al. PSI child-care stress index manual, Japan: Koyoumondaikenkyukai, 2006. (In Japanese)
13. Page AP. An investigation of the relationship between maternal-infant patterns of synchrony during feeding, preterm infant state and a parent administered state modulation treatment. Unpublished Doctoral dissertation: University of Washington, 1992.
14. Bronson M B. Self-Regulation in early childhood. New York: The Guilford press, 2000.
15. Kohyama, J. Foundation of child sleep for generalists. Japan: Shinkouigaku Publication, 2008. (In Japanese)
16. Shimada M, Sumihara K. Children’s circadian rhythms and child-care assistance. The Japanese Journal of Child Nursing. 2005; 28: 1511-1516. (In Japanese)
17. Schwictenberg AJ, Poehmann J. A transactional model of sleep-wake regulation in infants born preterm or low birth weight. Pediatric Psychology. 2009; 34: 837-849.
18. Kamerman SB. Handbook of early childhood intervention. Cambridge: Cambridge University Press, 2000.
19. Orshan SA. Maternity, newborn, and women’s health nursing: Comprehensive care across the lifespan. Philadelphia: LWW, 2008.





























