Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Head-to-head comparison of diagnosticaccuracy of stress-only myocardial perfusionimaging with conventional and cadmium-zinctelluride single-photon emission computedtomography in women with suspected coronaryartery disease
Teresa Mannarino, MD,a Roberta Assante, MD, PhD,a Carlo Ricciardi, MSc,a
Emilia Zampella, MD, PhD,a Carmela Nappi, MD, PhD,a Valeria Gaudieri, MD,
PhD,a Ciro Gabriele Mainolfi, MD,a Eugenio Di Vaia, MD,a
Mario Petretta, MD,b Mario Cesarelli, MSc,c Alberto Cuocolo, MD,a
and Wanda Acampa, MD, PhDa,d
a Department of Advanced Biomedical Sciences, University Federico II, Naples, Italyb Department of Translational Medical Sciences, University Federico II, Naples, Italyc Department of Electrical Engineering and Information Technology, University Federico II,
Naples, Italyd Institute of Biostructure and Bioimaging, National Council of Research, Naples, Italy
Received Apr 23, 2019; accepted Jun 11, 2019
doi:10.1007/s12350-019-01789-7
Background. Breast attenuation may impact the diagnostic accuracy of stress myocardialperfusion imaging (MPI) with single-photon emission computed tomography (SPECT). Wecompared the performance of conventional (C)-SPECT and cadmium-zinc-telluride (CZT)-SPECT systems in women with low-intermediate likelihood of coronary artery disease (CAD).
Methods andResults. A total of 109 consecutivewomenunderwent stress-optional restMPI byboth C-SPECT and CZT-SPECT. In the overall study population, a weak albeit significant cor-relation between total perfusion defect (TPD) measured by C-SPECT and CZT-SPECT wasobserved (r = 0.38, P < .001) and at Bland-Altman analysis the mean difference in TPD (C-SPECTminus CZT-SPECT) was 2.40% (P < .001). Overall concordance of semi-quantitative diagnosticperformance between C-SPECT and CZT-SPECT was observed in 52 (48%) women with a j
value of 0.09. Normalcy rate was significantly higher using CZT-SPECT compared to C-SPECT(P < .001). Machine learning analysis performed through the implementation of J48 algorithmproved that CZT-SPECT has higher sensitivity, specificity, and accuracy than C-SPECT.
Conclusions. Inwomenwith low-intermediate likelihood ofCAD, there is a poor concordanceof diagnostic performance between C-SPECT and CZT-SPECT, and CZT-SPECT allows betternormalcy rate detection compared to C-SPECT. (J Nucl Cardiol 2019)
Key Words: CAD Æ SPECT Æ MPI Æ Diagnostic application
Electronic supplementary material The online version of this
article (https://doi.org/10.1007/s12350-019-01789-7) contains sup-
plementary material, which is available to authorized users.
Teresa Mannarino and Roberta Assante are the first two authors shared
first co-authorship.
The authors of this article have provided a PowerPoint file, available
for download at SpringerLink, which summarises the contents of the
paper and is free for re-use at meetings and presentations. Search for
the article DOI on SpringerLink.com.
Reprint requests: Wanda Acampa, MD, PhD, Department of Advanced
Biomedical Sciences, University Federico II, Via Pansini 5, 80131
Naples, Italy; [email protected]
1071-3581/$34.00
Copyright � 2019 American Society of Nuclear Cardiology.

AbbreviationsSPECT Single-photon emission computed
tomography
MPI Myocardial perfusion imaging
CAD Coronary artery disease
C Conventional
CZT Cadmium-zinc-telluride
ECG Electrocardiography
SSS Summed stress score
TPD Total perfusion defect
LV Left ventricular
INTRODUCTION
Stress single-photon emission computed tomogra-
phy (SPECT) myocardial perfusion imaging (MPI)
represents the most widely used non-invasive cardiac
imaging tool for diagnosis and risk stratification of
patients with suspected or known coronary artery
disease (CAD).1,2 However, conventional (C)-SPECT
systems utilize large sodium iodide crystals, photomul-
tiplier tubes, and parallel-hole collimation, and are
therefore inherently insensitive, necessitating prolonged
imaging times and relatively large radioisotope doses.
Novel dedicated gamma cameras with semiconductor
cadmium-zinc-telluride (CZT) detectors have been
introduced in the clinical practice for cardiac imaging.3
These new CZT-SPECT cameras, characterized by
improved spatial, temporal, and energy resolution as
compared to C-SPECT cameras, provided better image
quality and shorter acquisition time, translating into
higher diagnostic accuracy.4,5 The characteristics of
heart-oriented geometry and higher energy resolution
related to CZT-SPECT are expected to reduce soft tissue
attenuation. Prior studies compared the diagnostic per-
formance of CZT-SPECT with that of C-SPECT
cameras in patients with suspected CAD and showed a
good correlation of the semi-quantitative perfusion
scores and functional parameters between the two
systems.6-8 These findings support the use of the novel
gamma cameras in clinical routine practices also con-
sidering the improvements in acquisition time and
radiation exposure reduction. A low-dose protocol with
a CZT-SPECT can be used in women with known or
suspected CAD without loss of accuracy compared to
men.9 However, no data are available comparing C-
SPECT and CZT-SPECT findings in women with
suspected CAD.
This study was designed to directly compare the
results of C-SPECT and CZT-SPECT stress-only MPI in
women with low-intermediate likelihood of CAD. In a
subgroup of women with low likelihood of CAD we also
assessed the prevalence of attenuation defects using C-
SPECT and CZT-SPECT according to semi-quantitative
analysis.
MATERIALS AND METHODS
Patients
We studied 109 consecutive women with low-intermedi-
ate likelihood of CAD submitted by referring physicians to
stress MPI for atypical angina, uninterpretable electrocardiog-
raphy (ECG) stress testing, or inability to exercise.1 Patients’
clinical history was collected, and cardiac risk factors were
assessed before testing. Atypical angina was defined as the
presence of two criteria including substernal chest pain or
discomfort, with characteristic quality and duration, provoked
by exertion or emotional stress and relieved by rest and/or
nitrates.10 The review committee of our institution approved
the study and all patients gave informed consent (Protocol
Number 110/17).
Pre-scan Likelihood of CAD
As part of the baseline examination, clinical teams
collected information on traditional cardiovascular risk factors,
including age, gender, blood pressure, smoking history, serum
cholesterol, family history of CAD, rest electrocardiographic
characteristics, diabetes and its complications (including neu-
ropathy, nephropathy, peripheral vascular disease, and
retinopathy), as well as the results of ECG stress testing.
Hypertension was defined as a known history of systolic blood
pressure[ 140 mmHg or the use of antihypertensive medica-
tion. Hypercholesterolemia was defined as a known history of
dyslipidemia or treatment with cholesterol-lowering medica-
tion. Patients were classified as having diabetes if they had a
previous diagnosis of diabetes or were receiving treatment with
oral hypoglycemic drugs or insulin. A positive family history
of CAD was defined as the presence of CAD in first-degree
relatives. These data were verified and complemented with
demographic and clinical information collected from medical
records. From these clinical variables, the pre-test CAD
likelihood was calculated for each patient by dedicated
software based on Bayesian analysis of pre-scan patients’ data
(Cadenza, version 5.04.3, Advanced Heuristics, Inc., Bain-
bridge Island, Washington).11 For patients who underwent
pharmacologic stress testing, pre-test likelihood was calculated
without using the stress test parameters. According to pre-test
likelihood of CAD, patients with a likelihood score \ 0.15
were considered at low risk of CAD, while those with a score
between 0.15 and 0.85 were considered at intermediate risk of
disease.
Study Protocol
Patients underwent stress 99mTc sestamibi gated MPI by
physical exercise or dipyridamole stress test, according to the
recommendations of the European Association of Nuclear
Mannarino et al Journal of Nuclear Cardiology�Conventional and CZT cameras in women

Medicine.12 In all patients, beta-blocking medications and
calcium antagonists were withheld for 48 hours and long-
acting nitrates for 12 hours before testing. For patient
undergoing exercise test, symptom-limited treadmill standard-
ized protocols were performed, with monitoring of heart rate
and rhythm, blood pressure, and ECG. Test endpoints were
achievement of 85% maximal predicted heart rate, horizontal
or down-sloping ST-segment depression[ 2 mm, ST-segment
elevation [1 mm, moderate to severe angina, systolic blood
pressure decrease[ 20 mm Hg, blood pressure[ 230/120 mm
Hg, dizziness, or clinically important cardiac arrhythmia. For
dipyridamole stress test, patients were instructed not to
consume products containing caffeine for 24 hours before the
test. Dipyridamole was infused at dose of 0.142 mg�kg-1 9
minute-1 intravenous over 4 minutes. A dose of 100 mg of
aminophylline was administered intravenously in the event of
chest pain or other symptoms, or after significant ST depres-
sion. At peak exercise, or 4 minutes after completion of
dipyridamole infusion, a bolus of 370 MBq of 99mTc-sestamibi
was intravenously injected. For both types of stress, heart rate,
blood pressure, and 12-lead ECG data were recorded at rest, at
the end of each stress stage, at peak stress and in the delay
phases at rest. Maximal degree of ST-segment changes at 80
ms after the J-point of the ECG was measured and assessed as
horizontal, down-sloping, or up-sloping. Horizontal or down-
sloping ST-segment depression C 0.1 mV, persisting for at
least 0.06 to 0.08 seconds after the J-point in one or more ECG
lead, were considered diagnostic for ischemia, whereas up-
sloping ST depressions C1.0 mm were considered non-
diagnostic. All ST depression \ 1.0 mm additional from
baseline was defined as negative.13
MPI
All patients underwent stress-optional rest MPI by both
C-SPECT and CZT-SPECT systems according to a random-
ized scheme in 1:1 ratio that determined which camera was
used for first acquisition. The study protocol is shown in
Figure 1.
For C-SPECT a dual-head rotating gamma Anger camera
(E.CAM, Siemens Medical Systems, Hoffman Estates, IL,
USA) equipped with a low-energy, high-resolution collimator
and connected with a dedicated computer system was used.14
No attenuation or scatter correction was used. For gating, a
cardiac cycle was divided into eight frames. Perfusion imaging
was reconstructed by summing the gated data at each projec-
tion into an ‘‘ungated’’ raw data file before low phase pre-
filtering and ramp filtered back projection.
For CZT-SPECT (D-SPECT, Spectrum Dynamics, Cae-
sarea, Israel) recordings were obtained using 9 pixilated CZT
crystal detector columns mounted vertically spanning a 90�geometry.15 Each of the columns consists of 1,024 (16 9 64)
5-mm thick CZT crystal elements (2.46 9 2.46 mm). Square-
hole tungsten collimators are fitted to each of the detectors,
which are shorter than conventional low-energy, high-resolu-
tion collimators, yielding significantly better geometric speed.
Data were acquired focusing on the heart by the detectors
rotating in synchrony and saved in list mode. Images were
obtained with the patient in a semi recumbent position. A 10-s
pre-scan acquisition was performed to identify the location of
the heart and to set the angle limits of scanning for each
detector (region of interest—centric scanning). Using the
myocardial count rate from the pre-scan acquisition, the time
per projection was set to target the recording of 1000
myocardial kcounts; the duration of the scans was less than
10 minutes for stress and 4 minutes for rest. Summed and gated
projections were reconstructed with an iterative maximum
likelihood expectation maximization algorithm using 7 and 4
iterations, respectively.
Imaging Interpretation
An automated software program (e-soft 2.5, QGS/QPS,
Cedars-Sinai Medical Center, Los Angeles, CA) was used to
calculate left ventricular (LV) volumes, ejection fraction, wall
motion, wall thickening, and the scores incorporating both the
extent and severity of perfusion defects, using standardized
segmentation of 17 myocardial regions.16 The total perfusion
defect (TPD) of the stress images was also generated,
representing the defect extent and severity and expressed as
a percentage of the LV myocardium.17 A post-stress LV
ejection fraction[ 45% and a summed stress score (SSS)\ 3
were considered normal.18 All studies were visually reviewed
and interpreted by two nuclear medicine physicians with[6
years of experience in nuclear cardiology blinded to clinical
information. A third nuclear medicine physician resolved any
discrepant readings. At reporting clinical interpretation, a
patient was defined as normal when a SSS [ 3 at semi-
quantitative analysis was associated with the preserved wall
thickening into the defect and visual over-read.19 Therefore, all
segments defined as normal at reporting but showing reduced
tracer uptake in the anterior wall at semi-quantitative analysis
at C-SPECT and/or CZT-SPECT were considered as false
defects due to breast attenuation rather than to true perfusion
abnormalities.
Statistical Analysis and Supervised MachineLearning
Statistical analysis was performed with a commercially
available software package (SPSS, version 20.0 for Windows,
SPSS Inc., Chicago, IL, USA). Continuous variables were
expressed as mean ± standard deviation and categorical data as
frequencies or percentage. Correlations between C-SPECT and
CZT-SPECT were evaluated by linear regression analysis, and
the agreement between the two SPECT systems was assessed
by Bland-Altman analysis.20 Comparison of continuous data
between groups was performed using the two-sided Student’s t
test. Concordance between the methods was also expressed as
exact agreement by the j statistics using the following grading
system: B 0.40 poor agreement, 0.41 to 0.60 moderate
agreement, 0.61 to 0.80 good agreement, and[ 0.80 excellent
agreement. Normalcy rate, defined as percentage of normal
result at semi-quantitative analysis (SSS\ 3) in the subgroup
of subjects with low (\ 0.15) likelihood of CAD, was
determined for both C-SPECT and CZT-SPECT considering
Journal of Nuclear Cardiology� Mannarino et al
Conventional and CZT cameras in women

normal MPI at reporting imaging interpretation and compared
by using McNemar Test. The effect of randomization sequence
on results was assessed by Cochran-Mantel-Haenszel test for
stratified cross-tabulations. A P value \ .05 was considered
statistically significant.
Supervised machine learning analysis was performed by
Knime analytics platform whose validity has been widely
acknowledged.21-25 In this study, J48 was implemented
through Knime analytics platform in its Java version. Cross-
validation was also implemented to exploit different combi-
nations of training and test sets.26 Parameters of global and
regional LV function and the scores incorporating both the
extent and severity of perfusion defects were employed to
conduct the analysis with J48 algorithm to assess the classi-
fications related to the two cameras. End-point for the analysis
of sensitivity, specificity, and diagnostic accuracy was the
classification of normal at reporting clinical interpretation
(including in the evaluation of semi-quantitative analysis the
presence of preserved wall thickening and the overall visual
over-read). The intraclass coefficient of correlation (ICC) was
used to assess intra- and interobserver reproducibility for
reporting clinical interpretation.27 The diagnostic perfor-
mances of the algorithm were the mean of the cycles coming
from 10 folds cross-validation. McNemar test was used to
evaluate the differences between the accuracy of the two
systems. In addition, the Matthews correlation coefficient
(MCC) was computed for each camera as it involves values of
all the four quadrants of a confusion matrix, and it is
considered a balanced measure. It is a quality indicator for
binary-class classification that ranges from - 1, when there is
perfect disagreement between actuals and prediction, to ? 1
for the perfect agreement. Receiver operating characteristics
(ROC) curve area was used to assess the goodness of a model
in distinguishing two classes ranging from 0 to 1.
RESULTS
The clinical characteristics of patient population are
shown in Table 1. Of the total 109 patients enrolled, 72
(66%) were at low and 37 (34%) at intermediate
likelihood of CAD. Sixty (55%) patients underwent
physical exercise stress test and 49 (45%) dipyridamole
stress test. Stress test results are reported in Table 2.
Comparison Between C-SPECT and CZT-SPECT in Overall Patient Population
In the overall study population, SSS (6.4 ± 4.2 vs
3.1 ± 3.2) and TPD (6.6 ± 4.9 % vs 4.2 ± 3.8 %) were
significantly higher (both P \ .0001) by C-SPECT
Figure 1. Study protocol for stress myocardial perfusion imaging. AC, Anger camera; CZT,cadmium-zinc-telluride camera.
Table 1. Clinical characteristics of 109 womenwith suspected CAD referred for stress MPI
Characteristic
Age (years) 62 ± 10
Body mass index (kg/m2) 28 ± 5
Diabetes mellitus, n (%) 26 (24)
Hypertension, n (%) 92 (84)
Smoking, n (%) 38 (35)
Hypercholesterolemia, n (%) 70 (64)
Family history of CAD, n (%) 60 (55)
Pharmacologic stress testing, n (%) 49 (45)
Values are expressed as mean value ± standard deviation oras number (percentage) of subjectsCAD, Coronary artery disease
Mannarino et al Journal of Nuclear Cardiology�Conventional and CZT cameras in women

compared to CZT-SPECT. No significant correlation
between SSS measured by C-SPECT and by CZT-
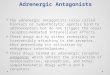
SPECT was found (r = 0.18, P = .06). At Bland-Altman
analysis, the mean difference in SSS (C-SPECT minus
CZT-SPECT) was 3.25 and the lower and upper limits
of agreement between the two SPECT systems were - 6
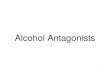
to 12 (Figure 2). Despite a weak but significant corre-
lation between TPD measured by C-SPECT and CZT-
SPECT (r = 0.38, P \ .001), the mean difference
between the two techniques was statistically significant
(2.40%, P \ .001) and at Bland-Altman analysis the
lower and upper limit of agreement between the two
SPECT systems were - 7% to 12% (Figure 3). Mean
values of post-stress LV ejection fraction were signif-
icantly higher by C-SPECT compared to CZT-SPECT
(74 ± 15% vs 66 ± 10, P\ .001). Agreement between C-
SPECT and CZT-SPECT for the classification of women
as normal or abnormal according to semi-quantitative
analysis is depicted in Figure 4. The difference between
the measurements obtained by the same examiner and
two different examiners for reporting clinical interpre-
tation was negligible with excellent intra- and
interobserver ICC (both [ 0.90). The overall concor-
dance of diagnostic performance between the two
SPECT systems was 48% with a very low j value of
0.09. Stress MPI was normal in 24 (22%) women by C-
SPECT and in 69 (63%) by CZT-SPECT and abnormal
in 85 (78%) at C-SPECT and in 40 (37%) by CZT-
SPECT. ECG stress test results were not correlated to
the presence of abnormal MPI results. Moreover, the
Cochran-Mantel-Haenszel test showed that randomiza-
tion sequence had no significant influence on the
differences between C-SPECT and CZT-SPECT (chi
square 1.76, P = .18). The 18 patients with concordant
normal results were all classified as normal at reporting
clinical interpretation. Of the 34 women with concordant
abnormal results, 13 were confirmed as abnormal at
reporting clinical interpretation and showed perfusion
defects in anterior (n = 8), lateral (n = 1) and inferior
(n = 4) walls. The remaining 21 women with concordant
abnormal results and classified as normal at reporting
clinical interpretation, all showed perfusion defects in
the anterior wall. The overall 57 patients with discordant
results showed myocardial perfusion defects in the
anterior wall associated with preserved wall thickening
and were classified as normal at reporting clinical
interpretation. Thus, 96 (88%) women were considered
normal and 13 (12%) abnormal at reporting clinical
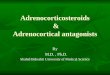
interpretation. Figure 5 shows a woman with discordant
results between C-SPECT and CZT-SPECT and classi-
fied as normal at reporting clinical interpretation.
Comparison Between C-SPECT and CZT-SPECT in Women at Low CAD Likelihood
Considering the 72 women at low CAD likelihood,
at semi-quantitative analysis 14 (20%) had normal and
58 (80%) abnormal MPI by C-SPECT and 43 (60%) had
normal and 29 (40%) abnormal MPI by CZT-SPECT.
Normalcy rate was significantly higher using CZT-
SPECT compared to C-SPECT (P\ .001).
Machine Learning Analysis
The diagnostic performances of two cameras,
according to the reporting clinical interpretation, are
summarized in Table 3. J48 showed accuracies of 91%
for C-SPECT and 96% for CZT-SPECT. CZT-SPECT
exhibited a sensitivity of 77%, a higher capacity of
detecting abnormal women than C-SPECT (61%).
Moreover, the ability to classify women according to
the clinical interpretation was proved to be better
through CZT-SPECT because of a higher specificity
(99%) than C-SPECT (95%). MCC and ROC curve area
Table 2. Stress test results according to stress type
Exercise (n = 60) Dipyridamole (n = 49) P value
Baseline heart rate (bpm) 78 ± 11 72 ± 13 \ .05
Peak heart rate (bpm) 140 ± 18 92 ± 15 \ .001
Baseline systolic blood pressure (mmHg) 132 ± 14 149 ± 22 \ .001
Peak systolic blood pressure (mmHg) 159 ± 18 133 ± 23 \ .001
Baseline diastolic blood pressure (mmHg) 82 ± 8 87 ± 10 \ .01
Peak diastolic blood pressure (mmHg) 92 ± 8 76 ± 10 \ .001
Symptoms, n (%) 3 (5%) 1 (2%) 0.36
Non-diagnostic ECG changes, n (%) 22 (37%) 12 (24%) 0.17
Values are expressed as mean value ± standard deviation or as number (percentage) of subjectsECG, Electrocardiography
Journal of Nuclear Cardiology� Mannarino et al
Conventional and CZT cameras in women

confirmed the difference that can be clearly observed
between the previous metrics. Confusion matrix of J48
for C-SPECT and CZT-SPECT are reported in Table 4.
A McNemar test was also performed, and the P value of
.017 enhanced a 95% statistically significant difference
between the accuracy of the two systems.
DISCUSSION
To our knowledge, this is the first study comparing
semi-quantitative results between C-SPECT and CZT-
SPECT in women with low-intermediate likelihood of
CAD. The results of the present investigation highlight a
poor concordance in diagnostic performance comparing
C-SPECT and CZT-SPECT. It also emerged that CZT-
SPECT leads to a better interpretation of the MPI results
in women with low likelihood of CAD. MPI with
SPECT represents a non-invasive accurate method for
the diagnostic evaluation of patients with suspected or
known CAD.1,2 However, C-SPECT using Anger cam-
era has poor energy resolution, long acquisition time,
and low spatial resolution. A high percentage of atten-
uation defect visible as reduction of tracer uptake
relative to soft tissue attenuation has been demon-
strated.28 A reverse distribution pattern, characterized by
new perfusion defect or a worsening of a pre-existing
defect on the rest images, may be frequent in patients
with a low likelihood of CAD and is frequently related
to soft tissue attenuation artifacts.29 It may be relevant in
women, where breast attenuation may adversely affect
diagnostic accuracy.30 In our study, imaging was per-
formed without attenuation correction and this might
have had an impact on the high number of perfusion
artifacts revealed by C-SPECT camera. However, it has
been reported that the diagnostic performance does not
change if comparing attenuation correction data with
non-corrected data in female patients.31 The new CZT-
SPECT are characterized by higher energy and spatial
resolution with a shorter time acquisition. In a previous
study, Liu et al.32 compared the performance of CZT-
SPECT and C-SPECT camera, by using phantoms and
water bags to simulate breasts and evaluate artifacts
Figure 2. Agreement between C-SPECT and CZT-SPECT byBland-Altman analysis for SSS measurement. The differencesbetween the two SPECT systems are plotted against the meansof the two systems. The horizontal black line indicates themean difference between the two systems and the red linesindicate the limits of agreements.
Figure 3. Agreement between C-SPECT and CZT-SPECT byBland-Altman analysis for TPD measurement. The differencesbetween the two SPECT systems are plotted against the meansof the two systems. The horizontal black line indicates themean difference between the two systems and the red linesindicate the limits of agreements.
Figure 4. Agreement between C-SPECT and CZT-SPECT forthe classification of women with normal and abnormal stressMPI. CI, confidence interval.
Mannarino et al Journal of Nuclear Cardiology�Conventional and CZT cameras in women

derived from soft tissue attenuation. In that study, the
authors demonstrated that CZT-SPECT provides better
physical performance and image quality and results in
lower artificial defects than C-SPECT. In particular,
false perfusion defect in anterior wall derived from
breast attenuation resulted less prominent with novel
CZT-SPECT.32 However, no data are available
comparing semi-quantitative results between C-SPECT
and CZT-SPECT in women. Several studies have
demonstrated a high correlation between quantitative
measure of perfusion abnormality and functional param-
eters using novel CZT-SPECT and C-SPECT systems,
with a good concordance between the two methods.8,32
A recent multicenter study evaluating a new solid-state
Figure 5. Discordant semi-quantitative analysis in a 48-year-old woman with hypertension,dyslipidemia, family history of CAD, and suspected CAD. Stress MPI shows a myocardialperfusion defect in the apical segment of the antero-septal region at C-SPECT (A) and normalmyocardial perfusion at CZT-SPECT (B).
Table 3. Machine learning analysis
Accuracy (%) Error (%) Sensitivity (%) Specificity (%) MCC ROC curve area
C-SPECT 91 9 61 95 0.56 0.763
CZT-SPECT 96 4 77 99 0.82 0.928
MCC, Matthews correlation coefficient; ROC, receiver operating characteristic
Table 4. Confusion matrix per algorithm
C-SPECT CZT-SPECT
Negative Positive Negative Positive
Negative 91 5 Negative 95 1
Positive 5 8 Positive 3 10
Journal of Nuclear Cardiology� Mannarino et al
Conventional and CZT cameras in women

cardiac camera showed diagnostic performance compa-
rable to that of C-SPECT camera, with superior image
quality and significantly shorter acquisition time.7 It has
also been demonstrated that a CZT-SPECT can be
routinely used in women with suspected or known CAD
with a good accuracy associated with lower radiation
exposure.9,33
In our study population, including only women with
suspected CAD, we found a not significant correlation in
both SSS and TPD value between conventional and
CZT-SPECT. Moreover, a poor concordance (48%) of
diagnostic performance between the two methods was
found, considering semi-quantitative results for the
classification of abnormal perfusion. These findings are
related to the presence of higher values of SSS,
indicating a larger myocardial perfusion defect in
correspondence of anterior wall in our population, when
images were acquired by C-SPECT. These counts
reduction visible at conventional images likely corre-
spond to a false myocardial defect due to the breast
attenuation. A different gantry geometry of the CZT-
SPECT in association with patient position (upright or
supine) and the position of the detectors closer to patient
body reduce attenuation artifacts, limiting the overesti-
mation of the perfusion defect scores obtained by C-
SPECT. Yet, CZT-SPECT demonstrated a significant
progressive increase in count rate related to decreasing
size of the imaged object and this can have an impact on
the evaluation of the anterior wall in women.34 To
compare semi-quantitative data between the two sys-
tems, we selected a study population including only
women with suspected CAD and low-intermediate pre-
scan likelihood of disease. Moreover, all images were
analyzed by using visual method with the addition of
examination of gated results. Using cinematic display of
wall motion and wall thickening from gated MPI has
been demonstrated to improve diagnostic certainty and
effectively differentiate artifacts from true perfusion
defects. Thus, we have a high level of confidence that
normal MPI at reporting imaging interpretation can be
considered truly negative. Indeed, it has been demon-
strated that overall diagnostic accuracy provided using
visual analysis by experts is comparable to automatic
quantitative analysis of CZT-SPECT, when compared to
coronary angiography.35 As well, it has been demon-
strated that also using semi-quantitative analysis, visual
over-read remains important in the final interpretation of
results.36 Also, prognostic information derived by using
visual analysis resulted comparable to quantitative
analysis.37 Thus, visual interpretation remains an impor-
tant tool to classify patients as normal or abnormal at
MPI.
In our study, we had a high prevalence of perfusion
artifacts by C-SPECT camera. The large majority of
defects were considered as false positive due to breast
attenuation according to reporting clinical interpretation.
The incidence of false positive results without evalua-
tion of gated images was comparable between our
investigation and prior studies.38,39 The addition of
SPECT gated imaging reduces the degree of uncertainty
in the interpretation of myocardial perfusion studies with
a significant increase in the normalcy rate in patients
with a low likelihood of CAD.39 In agreement with
published data,40 we also observed a higher value of
mean post-stress LV ejection fraction by C-SPECT
compared to CZT-SPECT. LV ejection fraction mea-
surement by CZT-SPECT is more comparable to that
obtained by cardiac magnetic resonance imaging rather
than by C-SPECT.41,42
In our study a separate analysis was performed in 72
women with low likelihood of CAD and normal MPI,
where normalcy rate was also calculated. We demon-
strated that the use CZT-SPECT improves normalcy rate
in women with a low likelihood of CAD. Finally, a
machine learning analysis was performed through the
implementation of J48 algorithm proving that CZT-
SPECT has higher values of accuracy, sensitivity, and
specificity than C-SPECT. These data suggest that CZT-
SPECT may be more appropriate than C-SPECT in
women with suspected CAD, leading to a better diag-
nostic accuracy and better discrimination between
perfusion artifacts and true perfusion defects.
In this study SPECT acquisitions with both cameras
have been performed with a high dose. Thus, it was not
possible to outline the additional potential advantage of
a lower dose in female population using a stress-only
protocol by CZT-SPECT compared to the use by C-
SPECT.
NEW KNOWLEDGE GAINED
Our study adds new information about the use of
CZT-SPECT in women with low-intermediate likeli-
hood of CAD. In particular, it indicates that CZT-
SPECT might allow a better diagnostic performance in
the identification of false positive results due to breast
attenuation defect in women.
CONCLUSION
In women with low-intermediate likelihood of
CAD, there was a poor concordance in myocardial
perfusion scores between C-SPECT and CZT-SPECT.
In particular, discordance was observed in the identifi-
cation of myocardial perfusion defects in the anterior
wall. In women with low likelihood of CAD, CZT-
SPECT allows a higher normalcy rate compared to C-
SPECT, showing a better diagnostic performance.
Mannarino et al Journal of Nuclear Cardiology�Conventional and CZT cameras in women

Disclosure
T. Mannarino, R. Assante, C. Ricciardi, E. Zampella, C.
Nappi, V. Gaudieri, C.G. Mainolfi, E. Di Vaia, M. Petretta, M.
Cesarelli, A. Cuocolo and W. Acampa declare that they have
no conflict of interest.
References
1. Hendel RC, Berman DS, Di Carli MF, Heidenreich PA, Henkin
RE, Pellikka PA, et al. ACCF/ASNC/ACR/AHA/ASE/SCCT/
SCMR/SNM 2009 appropriate use criteria for cardiac radionuclide
imaging. J Am Coll Cardiol 2009;53:2201-29.
2. Green R, Cantoni V, Petretta M, Acampa W, Panico M, Buon-
giorno P, et al. Negative predictive value of stress myocardial
perfusion imaging and coronary computed tomography angiogra-
phy: A meta-analysis. J Nucl Cardiol 2018;25:1588-97.
3. Sharir T, Ben-Haim S, Merzon K, Prochorov V, Dickman D, Ben-
Haim S, et al. High-speed myocardial perfusion imaging initial
clinical comparison with conventional dual detector anger camera
imaging. JACC Cardiovasc Imaging 2008;1:156-63.
4. Slomka PJ, Patton JA, Berman DS, Germano G. Advances in
technical aspects of myocardial perfusion SPECT imaging. J Nucl
Cardiol 2009;16:255-76.
5. Berman DS, Kang X, Tamarappoo B, Wolak A, Hayes SW,
Nakazato R, et al. Stress thallium-201/rest technetium-99 m
sequential dual isotope high-speed myocardial perfusion imaging.
JACC Cardiovasc Imaging 2009;2:273-82.
6. Esteves FP, Raggi P, Folks RD, Keidar Z, Askew JW, Rispler S,
et al. Novel solid-state-detector dedicated cardiac camera for fast
myocardial perfusion imaging: Multicenter comparison with
standard dual detector cameras. J Nucl Cardiol 2009;16:927-34.
7. Tanaka H, Chikamori T, Hida S, Uchida K, Igarashi Y, Yokoyama
T, et al. Comparison of myocardial perfusion imaging between the
new high-speed gamma camera and the standard anger camera.
Circ J 2013;77:1009-17.
8. Verger A, Djaballah W, Fourquet N, Rouzet F, Koehl G, Imbert L,
et al. Comparison between stress myocardial perfusion SPECT
recorded with cadmium-zinc-telluride and Anger cameras in var-
ious study protocols. Eur J Nucl Med Mol Imaging 2013;40:331-
40.
9. Gimelli A, Bottai M, Quaranta A, Giorgetti A, Genovesi D,
Marzullo P. Gender differences in the evaluation of coronary
artery disease with a cadmium-zinc telluride camera. Eur J Nucl
Med Mol Imaging 2013;40:1542-8.
10. Diamond GA, Forrester JS. Analysis of probability as an aid in the
clinical diagnosis of coronary-artery disease. N Engl J Med
1979;300:1350-8.
11. Diamond GA, Staniloff HM, Forrester JS, Pollock BH, Swan HJ,
et al. Computer assisted diagnosis in the noninvasive evaluation of
patients with suspected coronary artery disease. J Am Coll Cardiol
1983;1:444-55.
12. Verberne HJ, Acampa W, Anagnostopoulos C, Ballinger J, Bengel
F, De Bondt P, European Association of Nuclear Medicine
(EANM), et al. EANM procedural guidelines for radionuclide
myocardial perfusion imaging with SPECT and SPECT/CT: 2015
revision. Eur J Nucl Med Mol Imaging 2015;2015:1929-40.
13. Fletcher GF, Ades PA, Kligfield P, Arena R, Balady GJ, Bittner
VA, et al. Exercise standards for testing and training: A scientific
statement from the American Heart Association. Circulation
2013;128:873-934.
14. Acampa W, Petretta M, Daniele S, Del Prete G, Assante R,
Zampella E, et al. Incremental prognostic value of stress
myocardial perfusion imaging in asymptomatic diabetic patients.
Atherosclerosis 2013;227:307-12.
15. Gambhir SS, Berman DS, Ziffer J, Nagler M, Sandler M, Patton J,
et al. A novel high sensitivity rapid acquisition single photon
cardiac imaging camera. J Nucl Med 2009;50:635-43.
16. Germano G, Kavanagh PB, Waechter P, Areeda J, Van Kriekinge
S, Sharir T, et al. A new algorithm for the quantitation of
myocardial perfusion SPECT. I: Technical principles and repro-
ducibility. J Nucl Med 2000;41:712-9.
17. Slomka PJ, Nishina H, Berman DS, Kang X, Friedman JD, Hayes
SW, et al. Automatic quantification of myocardial perfusion stress-
rest change: A new measure of ischemia. J Nucl Med
2004;45:183-91.
18. Nappi C, Gaudieri V, Acampa W, Assante R, Zampella E,
Mainolfi CG, et al. Comparison of left ventricular shape by gated
SPECT imaging in diabetic and nondiabetic patients with normal
myocardial perfusion: A propensity score analysis. J Nucl Cardiol
2018;25:394-403.
19. Acampa W, Petretta M, Florimonte L, di Santolo MS, Cuocolo A.
Sestamibi SPECT in the detection of myocardial viability in
patients with chronic ischemic left ventricular dysfunction: Com-
parison between visual and quantitative analysis. J Nucl Cardiol
2000;7:406-13.
20. Bland JM, Altman D. Statistical methods for assessing agreement
between two methods of clinical measurement. Lancet
1986;1:307-10.
21. Sharma N, Bansal K. Comparative study of data mining tools.
JoADMS 2015;2:35-41.
22. Warr WA. Scientific workflow systems: Pipeline Pilot and
KNIME. J Comput Aided Mol Des 2012;26:801-4.
23. Dietz C, Berthold MR. KNIME for open-source bioimage analy-
sis: A tutorial. In: Focus on bio-image informatics. Berlin:
Springer; 2016. p. 179-97.
24. Rajmohan K, Paramasivam I, Sathya Narayan S. Prediction and
diagnosis of cardiovascular disease: A critical survey. In: 2014
World Congress on Computing and Communication Technologies
(WCCCT). IEEE; 2014. p. 246-51
25. Quinlan JR. C4.5: Programs for machine learning. Amsterdam:
Elsevier; 2014.
26. Kohavi R. A Study of cross-validation and bootstrap for accuracy
estimation and model selection In: IJCAI ‘95 proceedings of the
14th international joint conference on artificial intelligence
1995;2:1137-45.
27. Shrout PE, Fleiss JL. Intraclass correlations: Uses in assessing
rater reliability. Psychol Bull 1979;86:420-8.
28. Doukky R, Rahaby M, Alyousef T, Vashistha R, Chawla D, Amin
AP. Soft tissue attenuation patterns associated with supine acqui-
sition SPECT myocardial perfusion imaging: A descriptive study.
Open Cardiovasc Med J 2012;6:33-7.
29. Araujo W, DePuey EG, Kamran M, Undavia M, Friedman M.
Artifactual reverse distribution pattern in myocardial perfusion
SPECT with technetium-99m sestamibi. J Nucl Cardiol
2000;7:633-8.
30. Mieres JH, Shaw LJ, Hendel RC, Miller DD, Bonow RO, Berman
DS, et al. A report of the American Society of Nuclear Cardiology
Task Force on women and heart disease (Writing Group on per-
fusion imaging in women). J Nucl Cardiol 2003;10:95-101.
31. Wolak A, Slomka PJ, Fish MB, Lorenzo S, Berman DS, Germano
G. Quantitative diagnostic performance of myocardial perfusion
SPECT with attenuation correction in women. J Nucl Med
2008;49:915-22.
Journal of Nuclear Cardiology� Mannarino et al
Conventional and CZT cameras in women

32. Liu CJ, Cheng JS, Chen YC, Huang YH, Yen RF. A performance
comparison of novel cadmium-zinc-telluride camera and conven-
tional SPECT/CT using anthropomorphic torso phantom and water
bags to simulate soft tissue and breast attenuation. Ann Nucl Med
2015;29:342-50.
33. Sharir T, Slomka PJ, Hayes SW, DiCarli MF, Ziffer JA, Martin
WH, et al. Multicenter trial of high-speed versus conventional
single-photon emission computed tomography imaging: Quanti-
tative results of myocardial perfusion and left ventricular function.
J Am Coll Cardiol 2010;55:1965-74.
34. Bienenstock EA, Ennis M. The effect of object size on the sen-
sitivity of single photon emission computed tomography:
Comparison of two CZT cardiac cameras and an Anger scintilla-
tion camera. EJNMMI Phys 2014;1:97.
35. Duvall WL, Slomka PJ, Gerlach JR, Sweeny JM, Baber U, Croft
LB, et al. High-efficiency SPECT MPI: Comparison of automated
quantification, visual interpretation, and coronary angiography. J
Nucl Cardiol 2013;20:763-73.
36. Wackers FJ. Science, art, and artifacts: How important is quan-
tification for the practicing physician interpreting myocardial
perfusion studies? J Nucl Cardiol 1994;1:S109-17.
37. Berman DS, Kang X, Van Train KF, Lewin HC, Cohen I, Areeda
J, et al. Comparative prognostic value of automatic quantitative
analysis versus semiquantitative visual analysis of exercise
myocardial perfusion single-photon emission computed tomogra-
phy. J Am Coll Cardiol 1998;32:1987-95.
38. Taillefer R, DePuey EG, Udelson JE, Beller GA, Latour Y, Reeves
F. Comparative diagnostic accuracy of Tl-201 and Tc-99m ses-
tamibi SPECT imaging (perfusion and ECG-gated SPECT) in
detecting coronary artery disease in women. J Am Coll Cardiol
1997;29:69-77.
39. Smanio PE, Watson DD, Segalla DL, Vinson EL, Smith WH,
Beller GA. Value of gating of technetium-99m sestamibi single-
photon emission computed tomographic imaging. J Am Coll
Cardiol 1997;30:1687-92.
40. Bailliez A, Lairez O, Merlin C, Piriou N, Legallois D, Blaire T,
et al. Left ventricular function assessment using 2 different cad-
mium-zinc-telluride cameras compared with a c-camera with
cardiofocal collimators: Dynamic cardiac phantom study and
clinical validation. J Nucl Med 2016;57:1370-5.
41. Cochet H, Bullier E, Gerbaud E, Durieux M, Godbert Y, Lederlin
M, et al. Absolute quantification of left ventricular global and
regional function at nuclear MPI using ultrafast CZT SPECT:
Initial validation versus cardiac MR. J Nucl Med 2013;54:556-63.
42. Giorgetti A, Masci PG, Marras G, Rustamova YK, Gimelli A,
Genovesi D, et al. Gated SPECT evaluation of left ventricular
function using a CZT camera and a fast low-dose clinical protocol:
Comparison to cardiac magnetic resonance imaging. Eur J Nucl
Med Mol Imaging 2013;40:1869-75.
Publisher’s Note Springer Nature remains neutral with regard to
jurisdictional claims in published maps and institutional affiliations.
Mannarino et al Journal of Nuclear Cardiology�Conventional and CZT cameras in women