-
Organizing Emergency Services in Psychiatry: The University
Health
Network Experience
Jodi Lofchy MD FRCPC
Director Psychiatric Emergency Services
University Health Network,
Associate Professor,
University of Toronto
Central LHIN Emergency Department
Quality Collaborative, Toronto
June 14, 2012
-
Overview
Models of best practice
The way we were…
Psychiatric Emergency Services Unit
[PESU]- the model
Systems and supports
Evaluation- what works and what doesn’t
A work in progress
-
Models of best practice
Goals:
Timely rendering of psychiatric emergency
care
Access to care
Safety/stabilization and assessment
Continuity of care
(Breslow R., Structure and Function of Psychiatric Emergency
Services from Emergency Psychiatry,
ed Allen M., 2002)
-
Models of {best} practice
{Consultation}
Psychiatric Emergency Services in Medical Emergency Settings
Psychiatric Emergency Service Facility
Crisis hospitalization
Crisis outpatient follow-up
Mobile teams
Crisis residences
Breslow, 2002
APA Task Force on Psychiatric Emergency Services 2002
-
Shifting Objectives in Emergency Psychiatry
Triage Model
– Rapid
evaluation
– Containment
– Rapid Referral
Treatment Model
– Comprehensive
assessment
– Broad range of
effective services.
“An Organizationally Unique Treatment Facility”
Gerson and Bassuk 1980
-
Organization and function of academic psychiatric emergency
services: Currier and Allen, General Hosp Psych 25 (2003)
124-129
Survey AAEP PES medical directors US- 51/56 (91%) response
77% (39/51) PES in general hospital– 64% (25/39) separate PES;
21% (8/39) component of med
ED; 13% (5/39) consultation
– 96% Ψ > 8 hr/d [26% Ψ 24/d]
– 77% had locked area in PES
– 69% (35/51) informal crisis beds; x = 9.2 beds
Admission rates: approx 1/3 (34%) admitted inpt Ψ
Length of stay [LOS]: x = 9.0 hrs (SD = 11.3 hr)
-
Hospital Based Services
Key System Components
Space Takes into account the needs of many, varied patients
Core Staff Nursing and other professional staff
Security officers
Psychiatric assistants
Psychiatrists and other medical specialists
Students
Support Services Toxicology
Therapeutic drug levels
Laboratory assays and imaging capability
-
The Views of the Client
Initial in-community contact
Alternatives to traditional services
More hopeful first contact
Intake and Waiting
– Comfortable physical environment
– Interpersonal emotional support
– Availability of peer advocate support
Assessment and Service Planning
– Respected person orientation
– Improved staff training
Treatment Interventions
– Patient-practitioner partnerships
Allen, M., (2003) What do Consumers Say they Want and Needs
During a
Psychiatric Emergency Journal of Psychiatric Practice Vol 9, No.
1.
-
Emergency Psychiatry at UHN
University Health Network [UHN] =
Toronto General Hospital [TGH] +
Toronto Western Hospital [TWH] +
Princess Margaret Hospital [PMH] +
Toronto Rehabilitation Institute [TRI]
ER Ψ at TWH
Inpatient Ψ at TGH:
– 18 general psych beds
– 6 acute care [ACU]
Outpatient Ψ at TWH, TGH, PMH
http://images.google.com/imgres?imgurl=http://www.cghr.org/images/UofT_logo.jpg&imgrefurl=http://www.cghr.org/events.htm&usg=__uv6WtnDyneRJ-aqWbL_6Wvg85QI=&h=1103&w=633&sz=91&hl=en&start=47&tbnid=FiZrvNVUxxdu2M:&tbnh=150&tbnw=86&prev=/images%3Fq%3DUNIVERSITY%2BHEALTH%2BNETWORK%2BLOGO%2BTORONTO%26start%3D40%26gbv%3D2%26ndsp%3D20%26hl%3Den%26sa%3DNhttp://images.google.com/imgres?imgurl=http://tubs.sa.utoronto.ca/2002/speakers_macgregor/index_files/logo.gif&imgrefurl=http://tubs.sa.utoronto.ca/2002/speakers_macgregor/index.htm&usg=__5zOy4On48CyQCE5liU1YIE83YQM=&h=94&w=90&sz=1&hl=en&start=61&tbnid=uQWzWwtghoCGvM:&tbnh=80&tbnw=77&prev=/images%3Fq%3DUNIVERSITY%2BHEALTH%2BNETWORK%2BLOGO%2BTORONTO%26start%3D60%26gbv%3D2%26ndsp%3D20%26hl%3Den%26sa%3DN
-
The Way we Were…. Early 1990’s until 2005
24 hr psychiatric consultation to the TGH and TWH EDs
Crisis Response Service 1996-2005 Multidisciplinary
clinicians
– 16 hrs/day 7 days/week Psychiatry assistants
– information collection, collateral, monitoring/escorting
patients
Emergency Psychiatry Assessment Unit [EPAU] – 8 bed secure unit
NOT in ED
Urgent Care Clinic [UCC]– patients mostly referred through the
ED’s– 3 clinics/week – appointments within 1 week of referral
-
What We Struggled with….
Responsiveness to Psychiatric consultation in ED
Lack of space in the ED for psychiatric assessment
– 2 designated beds
– Long waiting times
– ↑ frequency of ‘LWBS’ [left without being seen], agitation,
prolonged police stays
Length of Stay [LOS] on the inpatient unit
EPAU as satellite acute care unit– Form 3’s, 4’s!
– Review boards
– Inpatient charts, discharge summaries
– Too many beds (2/8 → Impact)
-
What We Struggled with….
Excessive use of resources to manage agitation– security –
codes– chemical & mechanical restraint
UCC– beyond brief therapy– 50% f/u visits > 20 session
guideline– Goal: 95% pts < 20 sessions
Insufficient time and resources to apply principles of crisis
intervention in the ED
-
PESU- the evolution 2005-07
CTAS modification [Canadian Triage and Acuity Scale*]
Development of the PES Model
PES/ED Integration Committee
Training and education
New unit design/function* *
Maintenance of the consultation model within the ED-based
PESU
*Beveridge R et al. Canadian Emergency Department Triage and
Acuity Scale
Can J Emerg Med 1999; 1(3 suppl):S2-28
-
PES MODEL – Triage Level
TRIAGEDirect to Psych (Physician to Physician)
ER Psychiatrist on call = MRP
MENTAL HEALTH
ISSUE ONLY
NO YES
As identified by ER Triage
Assistance can be provided by
ER Psych RN
ER
MENTAL HEALTH
CONSULT REQUIRED
All patients should have basic
physical assessment, i.e. vital signs
CONSULTATION
CRISIS
CONSULT
PSYCHIATRIC
CONSULT
-
PES MODEL – Consult Level
Emergency Psychiatry remains a
consultative model. Crisis consultation
still available independent of
psychiatric consultation
CRISIS
CONSULT
PSYCHIATRIC
CONSULT
May refer to Psychiatry prior to
complete assessment if:
- presenting complaint
Psychiatric in origin
- No obvious or acute medical
issues are present
- ED physician engages with
crisis clinician for input to
expedite an early referral
Involvement in referral
will be at psychiatrist’s
discretion
Psych will ask ED
physician reason for
psychiatric referral
PES Clinician
(Mon.-Sun. 0800-
2300) discusses
case with ER MD
DISCHARGEHOLDADMIT
PESU
-
PESU
Physically situated in the TWH Emergency Department
Safe, secure setting with a capacity for 8 patients, 4
stretchers, 2 lounges, 2 wait spaces
Dedicated psychiatric nursing staff, psychiatry assistants,
crisis clinicians and on-site resident and staff psychiatrists
PES Model supports decisions made by the team
-
ADMIT HOLD DISCHARGE
Decision to admit made,
patient transferred to bed
“Admit no bed” will
automatically trigger a
“psych bed alert”. ER MD no
longer responsible for
patient while in ER
Medical issues to be referred
to Medical consults
Decision to hold would be
based on clinical decision,
i.e.: patient’s condition, need
for collateral in an after
hours situation, awaiting
acceptance to another
facility (no longer than 12
hours)
If any acute decompensation
in a patient’s condition, ER
will be notified and respond
Refer to Urgent
Care Clinic, Clerk
Crisis Clinic or
Crisis follow up
Reconnect with
community support
Refer on to other
services
Considerations
Six hours post-consult, ER Psych becomes MRP
If patient requires medical attention, Medical Consults will
be
consulted
PESU
PES MODEL - Disposition
-
PESU: who are the patients in our unit?
Emergency Hold Admit
ER MD = MRP*
Pt. s/b ED Physician +/-
clinician or PESU nurse
1. Pt. discharged from ED
by ER MD
2. Pt referred to psychiatry
for consultation then d/c’d
by Ψ
Ψ= MRP
Pts referred to psychiatry-
decision to hold as an
emergency patient for
following reasons:
Crisis stabilization
Risk assessment
Further collateral
required
Not likely to require
admission
Ψ= MRP
Disposition after
psychiatric consultation:
Complex diagnosis
Known pt. with pattern
of high risk
decompensation
Will need further
stabilization and /or
treatment
*MRP= Most Responsible Physician
-
Systems and supports
Departmental
Emergency department
Hospital
ER Alliance
Computerization
Communication
– High risk pts: EMI’s
– Cross-site meetings
– ER/Psych meetings
– M&M ER/Psych rounds
– PALC
-
PESU Staffing (2012)
Days:
1 Staff Psychiatrist (0830-1700)
Resident and/or Clinical Clerk (0830-1700)
2 RNs (0730-1930)
2 Clinicians (0800-2000 and 1100-2300)
2 Psychiatric Assistants (0730-1930 and 1100-2300)
Nights: 1 Resident on call/Staff Psychiatrist
2 RNs (1930-0730)
1 Psychiatric Assistant (1930-0730)
-
What’s Working………
Patients are seen straight from triage if
presenting with a Mental Health
complaint- less wait time
-
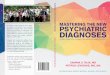
Average Crisis Response Times Under 2 Hours
64%70%
83% 82% 81% 80% 83% 82% 82%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
2004 2005 2006 2007 2008 2009 2010 2011 2012
EPAU PESU
-
What’s Working………
Patients are seen straight from triage if
presenting with a Mental Health complaint-
less wait time
Decrease in number of admits
Increased overall volumes
-
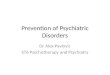
PRE AND POST PESU COMPARISON
0
2,000
4,000
6,000
8,000
Tot. Visits 1,173 4,580 7,555
Tot. Admits 453 696 956
% 38.60% 15.50% 12.70%
2004-2005 2005-2007 2008-2012
PESUEPAU
Avg. % Admits
vs. Total Pts Seen
2004-2005
38.6%
2005-2012
13.6%*
*Currier & Allen,
2003: x = 34%
-
What’s Working………
Patients are seen straight from triage if
presenting with a Mental Health complaint-
less wait time
Decrease in number of admits
Increased overall volumes
Current average LOS in PESU 9.8 hrs
Less use of chemical restraint
Less use of security
-
Other variables….
Length of Stay
Pre-PESU/EPAU- 2005 Avg. LOS: 8 days
Post-PESU- 2006-2012 Avg. LOS: 10.4 hours*
- 2011-2012 Avg. LOS : 9.8 hours*
*Currier & Allen, 2003: x = 9 hrs
Chemical Restraint
PESU vs. EPAU: less chemical restraint - received fewer meds
overall, less multiple medications, less Haldol used
Hypotheses:–Less wait time to see Ψ
–De-escalation by psychiatric staff
–Containment of a locked unit(Venos et al, 2006)
-
What’s Working………
Patients are seen straight from triage if presenting with a
Mental Health complaint- less wait time
Current LOS in PESU @ approx 9.8 hrs
Decrease in number of admits
Increased overall volumes
Less use of chemical restraint
More capacity for crisis intervention work in the ER
More capacity for crisis f/u: 4 UCC clinics, max 10 sessions
Improved staff morale- recruitment/retention; consumer
satisfaction
Increased communication, collegiality with ER
-
Rich educational venue
Morning report revised- resident driven
Increasing numbers of students:
– Medical student electives
2003-04: 20
2005-11: 61
– Resident electives:
2008-11: 13
– Nursing
– Social work
Sharing model with other centres across the country
– 13 Local
– 11 National
-
A Work in progress…
Inpatient beds located at TGH site
Challenges unique to UHN and PESU
Ongoing communication!
Model refinement
Medical consultation
Managing change
Outcome measures-best practices
HOLDING AND HELPING….
-
PESU TORONTO WESTERN HOSPITAL ED