Embed Size (px)
Citation preview

Oregon Conference: Transforming Care 2013
Tara LarsonBehavioral Health and Primary Care Integration
in North CarolinaJanuary 8, 2013

2
ObjectivesOutline several efforts to support the behavioral health
needs of the Medicaid population in North Carolina through integration between Community Care of NC and the behavioral health Managed Care Organizations.
Describe the complex medical/residential program.Describe the A+KIDS antipsychotic safety registry in North
Carolina.
2

3
Causes of Health Disparities in Behavioral Health
Medications (though problems evident BEFORE antipsychotics where available)
High rates of smoking, lack of weight management/nutrition, and physical inactivity
Lack of access to/utilization of preventive community healthcare, including health promotion services and resources
PovertySocial isolationSeparation of health and mental health into separate systems
at the federal, state and local level with lack of coordinated infrastructure, policy, planning, quality improvement strategies, regulation or reimbursement
Parks,J, Radke,A, Mazade,N, and Mauer,B NASMHPD 16th Technical Report : Measurement of Health Status for People with Serious Mental Illness. October 16, 2008. 3

4
What is the Behavioral Health Initiative?Increase the use of evidence based treatment guidelines for
behavioral health including depression, substance abuse, and ADHD
Increase the number of co-located providersDecrease the re-hospitalization rate for primary psychiatric
admissionsIncrease access to preventive health care to people with
mh/dd/saIncrease coordination of the care for people with mh/dd/sa
through case consultations, data mining, designation of lead coordination
Decrease out of state placements for people with mh/dd/sa and complex medical needs
4

5
Why the Behavioral Health Initiative?CHCS Center for Health Care Strategies, Inc., Dec 2010
Clarifying Multi-morbidity Patterns to Improve Targeting and Delivery of Clinical Services for Medicaid Populations
The analysis confirms the overwhelming pervasiveness of physical and behavioral health co-morbidity among Medicaid’s highest-cost beneficiaries.
Reinforcing earlier analyses, the findings demonstrate that most beneficiaries with the highest hospitalization rates and costs have not one condition, but many. Based upon Medicaid paid claims, 50% of all ED or inpatient admissions had mh/sa/dd diagnosis.
Mental illness is nearly universal among the highest-cost, most frequently hospitalized beneficiaries, and similarly, the presence of mental illness and/or drug and alcohol disorders is associated with substantially higher per capita costs and hospitalization rates.
5

6
Community Care of NC (CCNC): “How it works”
Primary care medical home available to 1.2 million individuals in all 100 counties.
Provides 4,500 local primary care physicians( 94% of all NC PCPs) with resources to better manage Medicaid population
Links local community providers (health systems, hospitals, health departments and other community providers) to primary care physicians , including mental health providers
Every network provides local care managers (600), pharmacists (50+), psychiatrists (14+) and medical directors (20) to improve local health care delivery
Coordinates behavioral health care through the behavioral health MCO/LMEs
7
Eligibility and Enrollment in Health Homes
Eligibility for Community Care of North Carolina enrollment includes all categorically-eligible Medicaid recipients including dually eligible individuals and persons enrolled in 1915b/c mh/dd/sa waivers.
Enrollment in the Health Homes program is opt out through enrollment in CCNC.

8
Population Management Components for CCNCOutreach / Education / Enrollment / CommunicationScreening / Assessment / Care PlanRisk Stratification / Identify Target PopulationPatient Centered Medical Home – Evidence-based best
practices and team based careTargeted Disease and Care Management Interventions
and Best PracticesPharmacy Management, Medication ReconciliationBehavioral Health Integration Transitional CareSelf Management of Chronic Conditions
9
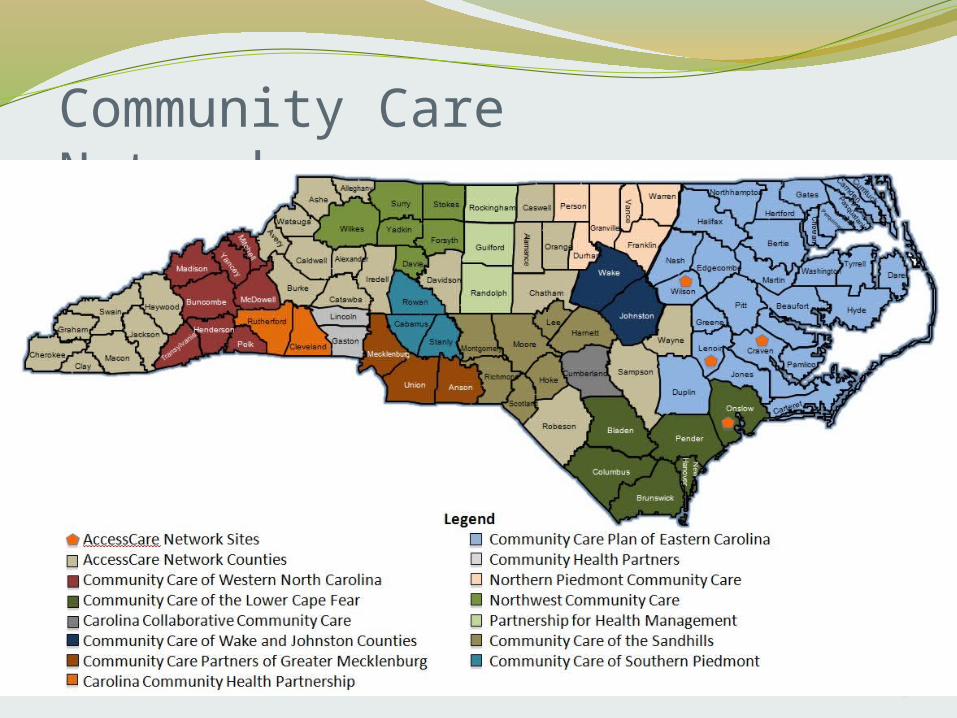
Community Care Networks
10
Each CCNC network has:Clinical Director
A physician who is well known in the community Works with network physicians to build compliance with care
improvement objectivesProvides oversight for quality improvement in practices Serves on the Sate Clinical Directors Committee
Network Director who manages daily operationsCare Managers to help coordinate services for enrollees/practicesPharmD to assist with Med management of high cost patientsPsychiatrist to assist in mental health integration

11
Current State-wide Diseaseand Care Management Initiatives
Asthma (1998 – 1st Initiative) Diabetes (began in 2000) Dental Screening and Fluoride Varnish (piloted for the state in 2000) Pharmacy Management
Prescription Advantage List (PAL) - 2003 Nursing Home Poly-pharmacy (piloted for the state 2002 - 2003) Pharmacy Home (2007) E-prescribing (2008) Medication Reconciliation (July 2009)
Emergency Department Utilization Management (began with Pediatrics 2004 / Adults 2006 )Case Management of High Cost-High Risk (2004 in concert with rollout of
initiatives) Congestive Heart Failure (pilot 2005; roll-out 2007)Chronic Care Program – including Aged, Blind and Disabled
Pilot in 9 networks 2005 – 2007 Began statewide implementation 2008 - 2009
Behavioral Health Integration (began fall 2010) Palliative Care (began fall 2010)

12
1915 B/C Behavioral Health Waiver1915 B/C Behavioral Health WaiverOperated through 11 “quazi governmental entities”
referred to as Local Management Entities (LMEs)Began in 5 counties in 2005 – will be statewide (100
counties) by June 30, 2013. By February 1, 99 counties will be live.
Fully Capitated, at risk for all mh/dd/sa services including ED visits, inpatient, ICF-MR, outpatient, enhanced mh/dd/sa services. Pharmacy is carved out. Some codes in primary care are “unmanaged” for med management and basic services To encourage one stop service delivery

13
Proposed Local Management Entity - Managed Care Organizations (LME-MCOs)and their Member Counties - by July 1, 2013
Anson
Ashe
Avery
Beaufort
Bertie
Bladen
Brunswick
Burke
Cabarrus
Caldwell
Carteret
Catawba Chatham
CherokeeClay
Cleveland
Columbus
Craven
Currituck
Forsyth
Gates
Graham
Granville Halifax
HarnettHenderson
Hertford
Jackson
Jones
LeeLincoln
Macon
Madison
MontgomeryMoore
Nash
Northampton
Onslow
Pamlico
Pender
Pitt
Polk
Robeson
Rockingham
Rowan
Rutherford
StokesSurry
Swain
Union
Vance
Wake
Warren
Watauga Wilkes
Wilson
Yadkin
Yancey
Smoky Mountain Center Jul 2012
Unless otherwise indicated, the LME name is the county name(s).The lead LME name for the proposed LME-MCO is shown first. Dates shown are the planned Waiver start dates.Reflects plans as of February 9, 2012.
Orange
Transylvania
Person
Western Region Central Region Eastern Region
Cumberland
Scotland
Haywood
New Hanover
Durham
Alleghany
Alamance
Iredell
Johnston
DuplinSampson
Wayne Lenoir
Dare
Hyde
Martin TyrrellWashington
Camden
PerquimansPasquotank
Greene
Alexander
Mitchell
Gaston
Buncombe
CenterPoint Human Services Jan 2013
Caswell
Chowan
Edgecombe
Western Highlands NetworkJan 2012
Davidson
StanlyMecklenburg
McDowell
Durham/ Wake/ Johnston/ Cumberland
Jan 2013
Davie
Coastal Care System(Southeastern Center/ OCBHS)
Jan 2013
Guilford
Randolph
Richmond
# Sandhills Center/ GuilfordDec 2012
East Carolina Behavioral Health Apr 2012
Eastpointe/ Southeastern Regional/
Beacon Center Jan 2013
Mecklenburg Feb 2013
Franklin
Hoke
Partners Behavioral Health Management (Pathways/ MH Partners/ Crossroads)
Jan 2013
PBH/ Alamance Caswell Oct 2011/ Five County Jan 2012/
OPC Apr 2012
13

14
1915b/c Waiver GoalsImproved Quality of CareIncreased Cost BenefitPredictable Medicaid Costs (2009 $22.57 per person, 2012$ 20.88)Combine the management of State/Medicaid Service Funds at the
Community LevelSupport the purchase and delivery of best practice servicesEnsure that services are managed and delivered within a quality
management frameworkEmpower the LME/MCOs to build partnerships with consumers,
providers and community stakeholders with the goal of creating a more responsive system of community care.
Increased consistency and economies of scale in the management of community services
15
What does the MCO/LME do for Medicaid? Enroll & monitor providers (statewide)Call Center—Customer SupportMake sure consumers with greatest need get connected to
providers and have treatment plans (Care Coordination)Authorize “medically necessary” servicesPay for mh/sa/dd servicesProvide education about ALL Medicaid benefits to recipients
& consumers (website, mailings, seminars)Reviews, Medications, Hearings (Due Process)Gap analysis/community developmentCCNC collaboration
16
Health Homes & Local Management Entities/Managed Care Organizations
CCNC (Community Care of NC) is NC’s Health Home Model with the LME/MCO to address the behavioral health needs through the 1915 b/c waiver
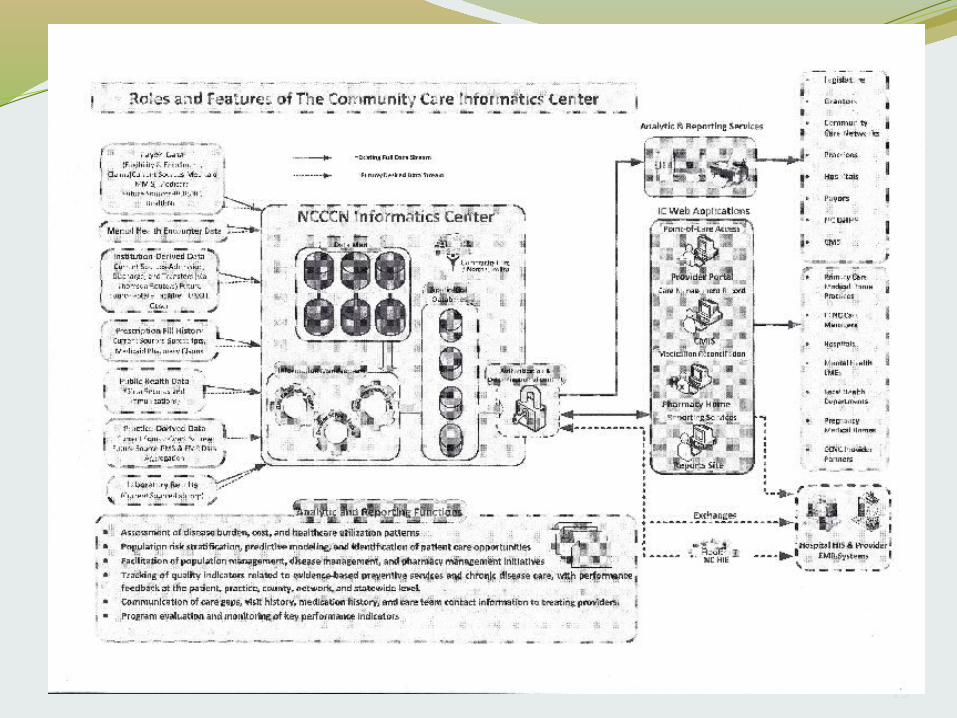
Much work has been done to interface the data sharing and to clarify the roles/responsibilities of LME/MCOs and CCNC (informatics chart attached)
Four Quadrant Care Management ModelDetermines who takes the lead in care managementQuadrants 1 and 3 – CCNC/Primary Care take leadQuadrant 2 – LME/MCO/Behavioral Health take leadQuadrant 4 – flexible sharing of responsibilities

17
Four Quadrant Care Management Model
Quadrant I:
Low MH/DD/SA health
Low physical health complexity/risk
Quadrant II:
High MH/DD/SA health
Low physical health complexity/risk
Quadrant III:
Low MH/DD/SA health
High physical health complexity/risk
Quadrant IV:
High MH/DD/SA health
High physical health complexity/risk

18
Health Homes & Local Management Entities/Managed Care Organizations Continued . . .
Shared Care Management of recipientsIdentification, linkage to servicesCoordination of MH/SA/DD & physical health needs
Data exchange into InformaticsLME/MCOs signed data-sharing agreements with the CCNC
Informatics CenterCollaboration on integrated care practicesMonthly-quarterly partnership meetings
19
20
Integrated Care Toolkit In August 2011 an MH/DD/SA Integrated Care Toolkit was published to
assist MH/DD/SA providers in collaborating with CCNC and primary care
Among other items, the toolkit includes:A flowchart to determine if an individual has a CCNC health home or
primary care providerA detailed description of the Four Quadrant Care Management Model
Responsibilities
More information on the toolkit can be found in the August 2011 Medicaid Bulletin – http://www.ncdhhs.gov/dma/bulletin/0811bulletin.html#car

21
Managing Complex CasesMost recent initiative to integrate medical and behavioral healthcare
NC has historically had to place children out of state who have complex medical and mh issues (such as brittle diabetic and bi-polar disorder)
Team formed with major regional hospital and medical school, specialty physicians, CCNC network, LME/MCO, private providers offering behavioral health residential care (in-home, therapeutic family living and PRTF)
Team follows childSingle payment made for cost of total care (hospital, outpatient) –
bundled paymentLead entity will pay all components providing care Incentive payments will be made for meeting outcomesHas been piloted through state dollars - will be Medicaid funded
beginning February 1, 2013 through EPSDT

ANTIPSYCHOTICS-KEEPING IT DOCUMENTED FOR SAFETY
(A+KIDS)
Initial Experience and Findings from a State Medication Safety Registry

23
Psychoactive Medication Use in Vulnerable Population ConcernsDisproportionate use of psychoactive medications in
foster populationsPossibly over-reliance on pharmacotherapy to address
behavioral concernsPsychoactive medication polypharmacy without clear
evidence basis Off-label use and limited short-term efficacy data or long-
term adverse effect studies (off-label use may be an appropriate practice in many cases)
Lack of monitoring and coordination of care
23

24
Foster Population in NCter80% are enrolled in CCNC PCMH (increase from 31% in
October, 2011)No clinically meaningful differences in Medicaid non-
fosters and fosters in physical health indicators (asthma, diabetes, etc)
Marked differences in behavioral health indicator prevalence
24

25
Foster Population in NCFoster recipients 3X more likely to have a mental health
diagnosis (49% versus 13%)More likely to have an intellectual disability (13% versus
5%)More likely to have PTSD (8.5% versus 0.5%)More likely to have depression (6% compared to 1%)More likely to have bipolar d/o (3.6% versus 0.3%)Differences were insignificant for schizophrenia and other
psychoses
25

26
Foster Population in NCFoster recipients had more OP visits, spent more on Rxs,
more on mental health treatment, more on inpatient and ED visits and cost significantly more overall than non-foster Medicare children/adolescents ($9,040 versus $1,864 annually)
Foster children enrolled in a CCNC PCMH cost less than non-enrolled similar ($8,333 compared to $9,040 annual mean cost/patient)
This cost difference underscores the effort to get fosters enrolled in PCMH
26
27
NC Response: A+KIDSWhat
Web-based safety registry system with fax optionClinical data entry at point of care by prescriberAutomated Authorization at time of submission
Provider participation is only requirementUse of “Over-rides”
No one should go without medication regardless of prescriber participation
WhoAll Medicaid Funded Youth 0-17Any antipsychotic Rx, New or RefillAll Medicaid prescribers regardless of discipline
27

28
NC Response: A+KIDSHow
Community Care North Carolina Network InfrastructureAll Medicaid prescribers regardless of discipline or area of
practice were registeredPhased introduction (0-12, 12-17, NC Healthchoice -SCHIP)Endorsement from advocacy and stakeholder groupsClose Partnership with web development firm
Infina Connect, LLC
28

29
A+KIDS Initial FindingsProvider ParticipationFrom April 2011-August 21, 2012
1241 prescribers with at least 1 authorization from the registry 1522 registered providers have not attempted to authorize a Rx
29,691 total authorizations15,194 total patients1842 foster children in the registry
29

30
Meds- 35% risperidone, 25% aripiprazole, 11% quetiapine
74% of A+KIDS patients are reported to be in some form of psychotherapy
Top 5% of prescribers account for 40% of authorizations2 prescribers account for 4% of all authorizations
Top 25% of prescribers account for 81% of authorizations
A+KIDS Initial FindingsResource Utilization Features
30

31
A+KIDS Initial FindingsParticipation
Developmen-tal Pediatrician
2%
Psychiatric NP3%
Psychiatric PA1%
Psychiatrist MD/DO61%
Non-Psychia-trist MD/DO
20%
Participating Prescriber Types After 6 Months of A+KIDS*
Developmental Pediatrician
Psychiatric Nurse Practioner
Psychiatric Physicians Assistant
Psychiatrist MD/DO
Non-Psychiatrist MD/DO
Non-Psychiatrist MD/DO(but patient also has a Psychiatrist)
Unknown
* Ages 0-12 Only
31

32
A+KIDS Initial Findings Clinical Features
*Ages 0-17
Unspecifi
ed Mood Diso
rder
Disruptive
Behavior D
isord
ers
ASD/P
DD
Bipolar Diso
rder
ADHDOth
er
Psychosis
Major D
epressi
ve Diso
rder
PTSD
Agitati
on/Hyp
erkinesia
Anxiety
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
Primary Dx Cited in A+KIDS Registry- First Year*
32

33
A+KIDS Initial FindingsClinical Features
33

34
A+KIDS Initial FindingsClinical Features-Body Mass Index
34

35
A+KIDS Initial FindingsClinical Features-Body Mass IndexEarly Informal Comparisons, Adolescents
Source Prevalence Overweight*(%)
Prevalence Obese**(%)
NC A+KIDS, 2011-2012, (Ages 13-17)
19.6 30.6
North Carolina, 2009 (Ages 10-17)CHAMP, BRFSS
16 16
North Carolina, 2007-2008(Ages 13-16)Medicaid Enrollees*
16 25
*Lazorick S, Peaker B, Perrin EM, Schmid D, Pennington T, Yow A, DuBard CA. Prevention and treatment of childhood obesity: care received by a state Medicaid population. Clin Pediatric (Phila). 2011 Sep;50(9):816-26.
35
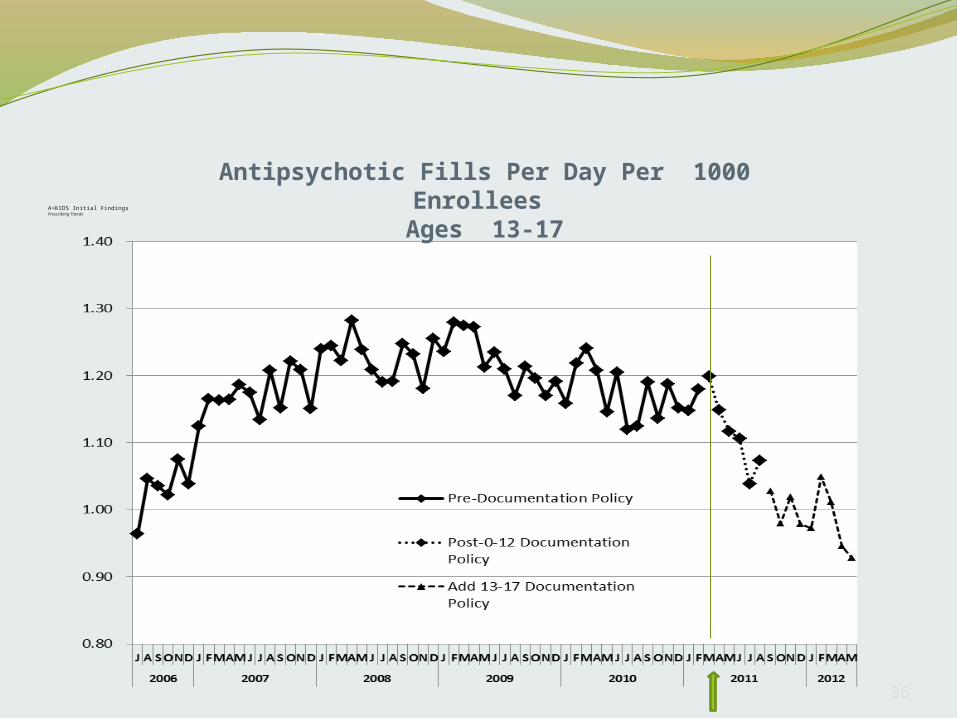
36
A+KIDS Initial FindingsPrescribing Trends
Antipsychotic Fills Per Day Per 1000 Enrollees Ages 13-17
36

37
Next Steps with Foster Care PopulationOngoing efforts to align foster population with
LME/MCO-CCNCShared definition of population across all state agenciesImproved descriptive statistics which characterize the
population healthcare resource utilization and risk factorsTask force at state agency level to address development
of programs to support needs of this at risk populationCase and provider profiling to identify specific follow-up
educational and/or consultative needs
37

38
Questions?





























