Embed Size (px)
Citation preview

VOL. 98, NO. 4 LETTERS TO THE JOURNAL 517
of kidney transplantation. The only significantly positive titers were for varicella zoster, which first increased and then diminished. Herpes zoster retinitis3 has been reported as part of herpes zoster ophthalmicus but the latter typically includes skin lesions over dermatomes supplied by the trigeminal nerve.
The cause of the acute retinal necrosis syndrome is uncertain. Hayreh4 suggested that the clinical manifestations of acute retinal necrosis are secondary to acute choroidal ischemia from ocular perivascu-litis of unknown origin. Culbertson and associates2'5 found large amounts of a her-pesvirus in the necrotic retinal layers of two eyes with clinically diagnosed acute retinal necrosis. The herpes group includes cytomegalovirus, herpes simplex virus, and varicella zoster virus and each member alone can cause necrotizing retinitis. Varicella zoster, however, has a predilection for causing occlusive arteri-tis, a feature which has been observed in at least one histopathologic specimen of acute retinal necrosis.2 Additionally, granulomatous angiitis of the central nervous system has been associated with previous herpes zoster involvement of the thorax.6 We speculate that acute retinal necrosis may be caused by undetected varicella zoster infections in some cases.
REFERENCES 1. Fisher, J. P., Lewis, M. L., Blumenkranz, M.,
Culbertson, W. W., Flynn, H. W., Jr., Clarkson, J. G., Gass, J. D. M., and Norton, E. W. D. : The acute retinal necrosis syndrome. I. Clinical manifestations. Ophthalmology 89:1309, 1982.
2. Culbertson, W. W., Blumenkranz, M. S., Haines, H., Gass, J. D. M., Mitchell, K. B., and Norton, E. W. D.: Ophthalmology 89:1317, 1982.
3. Naumann, G., Gass, J. D. M., and Font, R. L.: Histopathology of herpes zoster ophthalmicus. Am. J. Ophthalmol. 65:533, 1968.
4. Hayreh, S. S.: Acute retinal necrosis, letter. Am. J. Ophthalmol. 97:661, 1984.
5. Culbertson, W. W., Clarkson, J. G., Blumenkranz, M., and Lewis, M. L. : Reply to S. S. Havreh, letter. Am. J. Ophthalmol. 97:662, 1984.
6. Rosenblum, W. L, Hadfield, M.. G., and Young, H. F.: Granulomatous angiitis with preceding varicella zoster. Ann. Neurol. 3:374, 1978.
ORBITAL EXTENSION OF CHOROIDAL MELANOMA WITHIN A SHORT POSTERIOR CILIARY NERVE
A N D R E W P. F E R R Y , M.D.
Department of Ophthalmology, Medical College of Virginia.
Inquiries to Andrew P. Ferry, M. D., Department of Ophthalmology, Medical College of Virginia, Virginia Commonwealth University, P. O. Box 262, Richmond, VA 23298.
Wolter1 recently reported extension of a choroidal melanoma to the orbit via a ciliary nerve. The tumor extended within the nerve, rather than in the more commonly observed pattern in which the tumor courses along the exterior of a ciliary nerve or artery as these structures pass through their scierai canals Although extrascleral extension of tumor has been found in 13% to 15% of enucleated melanoma-containing eyes,2 review of both current and older textbooks of ophthalmic pathology discloses neither mention nor demonstration of transscler-al extension of choroidal melanoma within the substance of a nerve.
We have received in our laboratory an eye containing a melanoma with findings similar to the unique case described by Wolter. The patient was an 82-year-old woman who had undergone lens extraction. Postoperatively a choroidal mass was found and the eye was enucleated two weeks after cataract surgery had been done. At the time of gross examination in the laboratory we found, upon inspecting the posterior surface of the eye, two small transscleral extensions of tumor that had been overlooked in the operating room by the practitioner. The melanoma (spindle B cell type) originated in the choroid and extended transsclerally within the substance of two widely separated short posterior ciliary nerves (Figs. 1 and 2). This was the sole source of extraocular extension. About one third to one half of
518 AMERICAN JOURNAL OF OPHTHALMOLOGY OCTOBER, 1984
■»*·*,
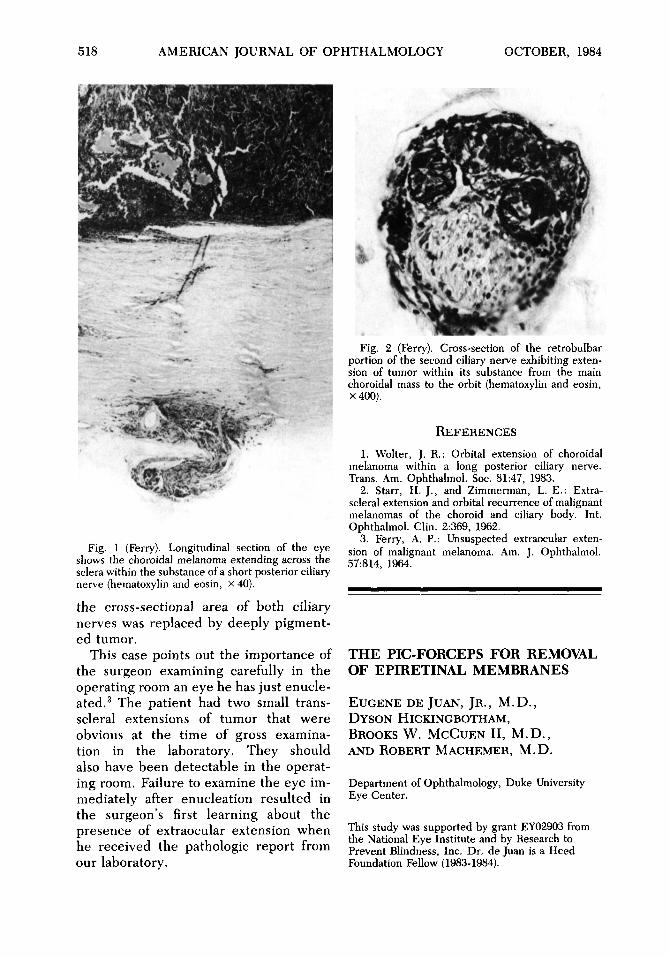
Fig. 1 (Ferry). Longitudinal section of the eye shows the choroidal melanoma extending across the sciera within the substance of a short posterior ciliary nerve (hematoxylin and eosin, x 40).
the cross-sectional area of both ciliary nerves was replaced by deeply pigment-ed tumor.
This case points out the importance of the surgeon examining carefully in the operating room an eye he has just enucleated.3 The patient had two small trans-scleral extensions of tumor that were obvious at the time of gross examination in the laboratory. They should also have been detectable in the operating room. Failure to examine the eye immediately after enucleation resulted in the surgeon's first learning about the presence of extraocular extension when he received the pathologic report from our laboratory.
Fig. 2 (Ferry). Cross-section of the retrobulbar portion of the second ciliary nerve exhibiting extension of tumor within its substance from the main choroidal mass to the orbit (hematoxylin and eosin, X400).
REFERENCES 1. Wolter, J. R.: Orbital extension of choroidal
melanoma within a long posterior ciliary nerve. Trans. Am. Ophthalmol. Soc. 81:47, 1983.
2. Starr, H. J., and Zimmerman, L. E.: Extra-scleral extension and orbital recurrence of malignant melanomas of the choroid and ciliary body. Int. Ophthalmol. Clin. 2:369, 1962.
3. Ferry, A. P.: Unsuspected extraocular extension of malignant melanoma. Am. J. Ophthalmol. 57:814, 1964.
THE PIC-FORCEPS FOR REMOVAL OF EPIRETINAL MEMBRANES
E U G E N E D E JUAN, J R . , M.D. , D Y S O N HICKINGBOTHAM, BROOKS W. M C C U E N II, M.D. , AND R O B E R T M A C H E M E R , M.D.
Department of Ophthalmology, Duke University Eye Center.
This study was supported by grant ΕΥ02903 from the National Eye Institute and by Research to Prevent Blindness, Inc. Dr. de Juan is a Heed Foundation Fellow (1983-1984).


![Comparison of Intravitreal Ranibizumab and Bevacizumab ... · chroidal nevus, melanoma, choroidal rupture, polypoidal choroidal vasculopathy (PCV) and idiopathic causes [2,4]. Among](https://img.dokumen.tips/doc/110x75/602950428aaed502c576bd94/comparison-of-intravitreal-ranibizumab-and-bevacizumab-chroidal-nevus-melanoma.jpg)











![Successful carbon-ion radiotherapy for choroidal melanoma ... › pdf › NFO-3-158.pdf · Choroidal melanoma is a rare but life-threatening intraocular malignant tumor [1]. Local](https://img.dokumen.tips/doc/110x75/5ed9830c1b54311e7967b2a8/successful-carbon-ion-radiotherapy-for-choroidal-melanoma-a-pdf-a-nfo-3-158pdf.jpg)














![Ophthalmology Update - Cleveland Clinicchoroidal nevi prevalence and choroidal melanoma incidence. The results, published in Ophthalmol-ogy [Singh AD, et al. Ophthalmology 2005;112:1784-89],](https://img.dokumen.tips/doc/110x75/5ed991a01b54311e7967ce4b/ophthalmology-update-cleveland-clinic-choroidal-nevi-prevalence-and-choroidal.jpg)