Embed Size (px)
Citation preview

Oral Chemotherapy Clinical Pearls in AML
Rob Walchack, PharmD, BCOP
Hematology/Cellular Therapy Clinical Pharmacy Specialist
UK HealthCare
September 17, 2021

Disclosures
I do not have (nor does any immediate family member have) a vested interest in or affiliation with any corporate organization offering financial support or grant monies for this continuing education activity, or any affiliation with an organization whose philosophy could potentially bias my presentation.

Objectives
Identify relevant drug-drug interactions with oral chemotherapy agents in AML
Describe oral chemotherapy dose adjustments in AML

Abbreviations
FLT3-ITD = fms-related tyrosine kinase 3 gene-internal tandem duplication
FLT3-TKD = fms-related tyrosine kinase 3 gene-tyrosine kinase domain
IDH1, IDH2 = isocitrate dehydrogenase 1 and 2
BCL2 = B-cell lymphoma 2
IC = intensive chemotherapy
7+3 = cytarabine continuous infusion x 7 days + daunorubicin x 3 days
VEN = venetoclax
LDAC = low-dose cytarabine
HMA = hypomethylating agent
DEC = decitabine
AZA = azacitidine
FluMel = fludarabine + melphalan
AML = acute myeloid leukemia
sAML = secondary acute myeloid leukemia
ADR = adverse drug reaction
AlloHCT = allogeneic hematopoietic cell transplantation
BM = bone marrow
CYP = cytochrome P450
QTc = corrected QT interval
P-gp = P-glycoprotein
G-CSF = granulocyte colony-stimulating factor
TLS = tumor lysis syndrome
NF = neutropenic fever
ND = newly-diagnosed
R/R = relapsed/refractory
WBC = white blood cell count
ANC = absolute neutrophil count
PLT = platelets
CBC = complete blood count
Hgb = hemoglobin
ORR = overall response rate
DOR = duration of response
NR = no response
OS = overall survival
CR = complete remission
CRi = complete remission with incomplete hematologic recovery
MLFS = morphological leukemia-free state
BMBx = bone marrow biopsy

Background
Cytotoxic and targeted oral chemotherapy represents a new concept in AML
Historically, intravenous cytotoxic chemotherapy-based regimens
Recently, paradigm shift incorporating oral chemotherapy agents

FDA Approval Timeline
MidostaurinEnasidenib
IvosidenibGlasdegibGilteritinib
Azacitidine (oral)Venetoclax

Place In Therapy
Agent Target(s) Treatment Naïve Relapsed/Refractory Maintenance post IC
Midostaurin FLT3-ITD FLT3-TKD
Enasidenib IDH2
Ivosidenib IDH1
Glasdegib
Gilteritinib FLT3-ITDFLT3-TKD
Azacitidine
Venetoclax BCL2
FDA Approved
combined with 7+3
combined with LDAC
combined with HMA/LDAC
Rydapt (midostaurin) [prescribing information]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; April 2021.Idhifa (enasidenib) [prescribing information]. Summit, NJ: Celgene Corporation; November 2020.Tibsovo (ivosidenib) [prescribing information]. Cambridge, MA: Agios Pharmaceuticals; May 2019.
Daurismo (glasdegib) [prescribing information]. New York, NY: Pfizer Labs; March 2020.Xospata (gilteritinib) [prescribing information]. Northbrook, IL: Astellas Pharma US, Inc; May 2019.Onureg (azacitidine) [prescribing information]. Summit, NJ: Celgene Corporation; March 2021.
Venclexta (venetoclax) [prescribing information]. North Chicago, IL: AbbVie Inc; November 2020.

Notable Drug-Drug Interactions
Agent CYP3A4 inducers/inhibitors
QTc-prolonging agents
P-glycoproteininducers
P-glycoproteininhibitors
Midostaurin
Enasidenib
Ivosidenib
Glasdegib
Gilteritinib
Azacitidine
Venetoclax
Rydapt (midostaurin) [prescribing information]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; April 2021.Idhifa (enasidenib) [prescribing information]. Summit, NJ: Celgene Corporation; November 2020.Tibsovo (ivosidenib) [prescribing information]. Cambridge, MA: Agios Pharmaceuticals; May 2019.
Daurismo (glasdegib) [prescribing information]. New York, NY: Pfizer Labs; March 2020.Xospata (gilteritinib) [prescribing information]. Northbrook, IL: Astellas Pharma US, Inc; May 2019.Onureg (azacitidine) [prescribing information]. Summit, NJ: Celgene Corporation; March 2021.
Venclexta (venetoclax) [prescribing information]. North Chicago, IL: AbbVie Inc; November 2020.

Notable Drug-Drug Interactions
Moderate CYP3A4 inhibitors
E.g. fluconazole, isavuconazole
Venetoclax dose 200 mg
Strong CYP3A4 inhibitors
E.g. posaconazole, voriconazole
Venetoclax dose 100 mg
50-70 mg with posaconazole?
Venetoclax

Literature Review

VIALE-A Trial
Phase 3, multicenter, randomized, double-blind, placebo-controlled trial
N = 431 patients with previously untreated AML ineligible for intensive chemotherapy Venetoclax 400 mg PO once daily D1-28 + Azacitidine 75 mg/m2 SQ/IV D1-7 q28d Placebo + Azacitidine 75 mg/m2 SQ/IV D1-7 q28d
OS, CR, CRi Gr3+ thrombocytopenia, neutropenia, NF, infections
DiNardo CD, et al. N Engl J Med. 2020. 383(7):617-629.
Endpoint Ven/Aza Placebo/Aza P-valueOS 14.7 mo 9.6 mo <0.001CR 36.7% 17.9% <0.001CRi 66.4% 28.3% <0.001

VIALE-A Trial
Azole antifungals allowed
WBC < 25 x 109/L prior to treatment initiation 1% incidence of TLS
Venetoclax given D1-28 with all cycles BMBx performed on D28 If in CR/CRi/MLFS hold until ANC >500 or up to 14 days Time to response 1.3 mo vs. 2.8 mo
DiNardo CD, et al. N Engl J Med. 2020. 383(7):617-629.
Venetoclax dose Ven dose with modCYP3A or P-gp inhibitor
Ven dose with strong CYP3A inhibitor
100 mg (C1 D1 only) 50 mg 10 mg200 mg (C1 D2 only) 100 mg 20 mg
400 mg 200 mg 50 mg

VIALE-A Trial
Treatment modifications due to myelosuppression
DiNardo CD, et al. N Engl J Med. 2020. 383(7):617-629.
Cycle CBC on Day 29 Dose ModificationsAfter Cycle 1 CRi Hold chemo until ANC > 500 or up to 14d
After Cycle 2 ANC < 500 x > 1 week* Hold chemo until ANC > 500 or up to 14d
After Cycle 3 ANC < 500 or PLT < 50k Hold chemo until ANC > 500 or PLT > 50k or up to 14d. Reduce VEN to 21d on/7d off
After Cycle 4
ANC > 1000 or PLT > 100k within 14d of Day 29
ANC or PLT not increased by 25% from Day 14 (nadir)
ANC or PLT not increased by 25% from Day 14 (nadir) within 14d of Day 29
Reduce VEN to 21d on/7d off
Reassess CBC every 7d
If no count recovery within 21d of Day 29, check BMBx:-BM cellularity 15-50%: Aza by 50%-BM cellularity <15%: Aza by 67%
*unless due to underlying disease

DEC10-VEN Trial

DEC10-VEN Trial
Phase 2, single center trial
N = 168 patients with ND or R/R AML Venetoclax 400 mg PO once daily D1-28 + Decitabine 20 mg/m2 IV D1-10 q28d Cycle 2 on Venetoclax 400 mg PO once daily D1-21 q28d Once in CR/CRi Decitabine 20 mg/m2 IV D1-5 q28d
Grade 3-4 ADRs: infection (47%), NF (29%)
DiNardo CD, et al. Lancet Haematol. 2020. 7(10):e724-e736.
Endpoint Overall ND ND sAML R/R AML R/R sAMLORR 74% 89% 80% 62% 61%OS --- 18.1 mo 7.8 mo 7.8 mo 6.0 mo
DOR --- NR 5.1 mo 16.8 mo NR

DEC10-VEN Trial
Azole antifungals allowed
WBC < 10 x 109/L prior to treatment initiation 2% incidence of TLS
BMBx on D21 hold VEN if aplasia or <5% blasts to allow for count recovery
Once ANC ≥ 500/μL and PLT >50 x 109/L, resume treatment
Time to response ~1.5 mo
DiNardo CD, et al. Lancet Haematol. 2020. 7(10):e724-e736.
Venetoclax dose VEN dose with modCYP3A inhibitor
VEN dose with strong CYP3A inhibitor
100 mg (C1 D1 only) 100 mg 100 mg200 mg (C1 D2 only) 200 mg 100 mg
400 mg 200 mg 100 mg

DEC10-VEN Trial
DiNardo CD, et al. Lancet Haematol. 2020. 7(10):e724-e736.
Dose Level DEC dose (mg/m2) VEN dose (mg) VEN duration0 (starting dose) 20 400 21 days
-1 15 200 21 days-2 10 200 14 days
No treatment delay Delay treatment until count recovery then resume at same doses If delayed >14 days (>D42), delay treatment until
count recovery then resume with dose adjustments for DEC, VEN, or both per table below
If D29 ANC <500/μL and PLT <50 x 109/L
Evidence of AML No evidence of AML

How I Treat AML in the Era of New Drugs
Post-induction BMBx on D21-28 of cycle 1 If > 5% blasts proceed with next cycle without delay If < 5% blasts hold VEN and resume at full dose once ANC > 500/μL and PLT > 50 x
109/L (hematologic recovery). G-CSF may be used.
Subsequent cycles (< 5% BM blasts) If ANC < 500/μL for >7d or severe complications hold VEN and start G-CSF until ANC recovery
Do not dose-reduce VEN to manage myelosuppression
If hematologic recovery takes >14d after holding VEN resume once hematologic recovery achieved with stepwise VEN duration reduction (28d 21d 14d) May reduce HMA dose based on BM cellularity if responding with delayed/lack of hematologic recovery 15-30% cellularity decrease HMA by 50% <15% cellularity decrease HMA by 67%
Consider G-CSF prophylaxis after HMA (D8) or LDAC (D11)DiNardo CD, et al. Blood. 2020. 135(2):85-96.

Venetoclax Package Insert
Venclexta (venetoclax) [prescribing information]. North Chicago, IL: AbbVie Inc; November 2020.
WBC < 25 x 109/L prior to treatment initiation
Only available as 10 mg, 50 mg, or 100 mg tablets
*Continue until progression/toxicity**Monitor closely for hematologic toxicities and TLS. Resume previous VEN dose 2-3d after CYP3A4 inhibitor discontinuation
Cycle 1 VEN dose VEN dose with mod CYP3A or P-gp inhibitor**
VEN dose with strongCYP3A inhibitor**
VEN dose with posaconazole**
Day 1 100 mg -No specific ramp-up recommendations
- VEN dose by at least 50%
10 mg 10 mgDay 2 200 mg 20 mg 20 mgDay 3 400 mg 50 mg 50 mg
Day 4 on* 400 mg (HMA)600 mg (LDAC) 100 mg 70 mg

Venetoclax Package Insert
Venclexta (venetoclax) [prescribing information]. North Chicago, IL: AbbVie Inc; November 2020.
Treatment modifications due to myelosuppressionANC < 500 or PLT <
25,000 Management*
Prior to remission Don’t interrupt VEN/HMA/LDAC BMBx recommended
1st occurrence after remission and lasting > 7d
Delay next cycle and monitor CBCOnce ANC > 1,000 resume regimen at same doses
Subsequent occurrences after remission and lasting
> 7d
Delay next cycle and monitor CBCOnce ANC > 1,000 resume regimen and reduce VEN
duration by 7d
*Consider supportive care (e.g. antimicrobial prophylaxis, G-CSF), as clinically necessary for all situations

Pharmacokinetic Study
Pharmacokinetic analysis of 12 patients
DEC 20 mg/m2 IV on D1-5 and VEN ramp up to 400 mg once daily through D20
Posaconazole 300 mg once daily with VEN 50 mg or 100 mg on D21-28
Blood samples collected before VEN and up to 24h after VEN on D20 and D28
Agarwal SK, et al. Clin Ther. 2017. 39:359-367.
Compared to VEN 400 mg
alone
Endpoints VEN 50 mg +Posaconazole
VEN 100 mg +Posaconazole
Mean VEN Cmax increased 53% increased 93%Mean AUC0-24 increased 76% increased 155%
With concomitant posaconazole… Both VEN 50 mg and 100 mg were well-tolerated Dose-reduce VEN by at least 75%

Retrospective Study
Retrospective, single-center analysis
N = 64 patients with ND AML in CR/CRi after 1 cycle of VEN + HMA
VEN given D1-28; stopped if D21 BMBx showed aplasia or < 5% blasts
Primary outcome Time to count recovery (ANC > 500-1000/μL and PLT >50-100 x 109/L)
Rausch CR, et al. Cancer. 2021. 0:1-11.
VEN dose N (%)No azole 400 mg 17 (27%)
Moderate CYP3A4 inhibitor 200 mg 21 (33%)Strong CYP3A4 inhibitor 100 mg 26 (41%)

Retrospective Study
Rausch CR, et al. Cancer. 2021. 0:1-11.
Selected endpoints (median) Voriconazole Posaconazole P-valueDays to ANC > 500/μL 35 35 NS
Days to ANC > 1000/μL 38 35 NSDays to PLT > 50 x 109/L 28 25 < 0.05Days to PLT > 100 x 109/L 32 26 NS
With 1 cycle of HMA + VEN…Posaconazole doesn’t prolong time to count recovery compared to
other azole antifungalsVEN 100 mg can be given safely with either posaconazole or
voriconazole

Patient Case
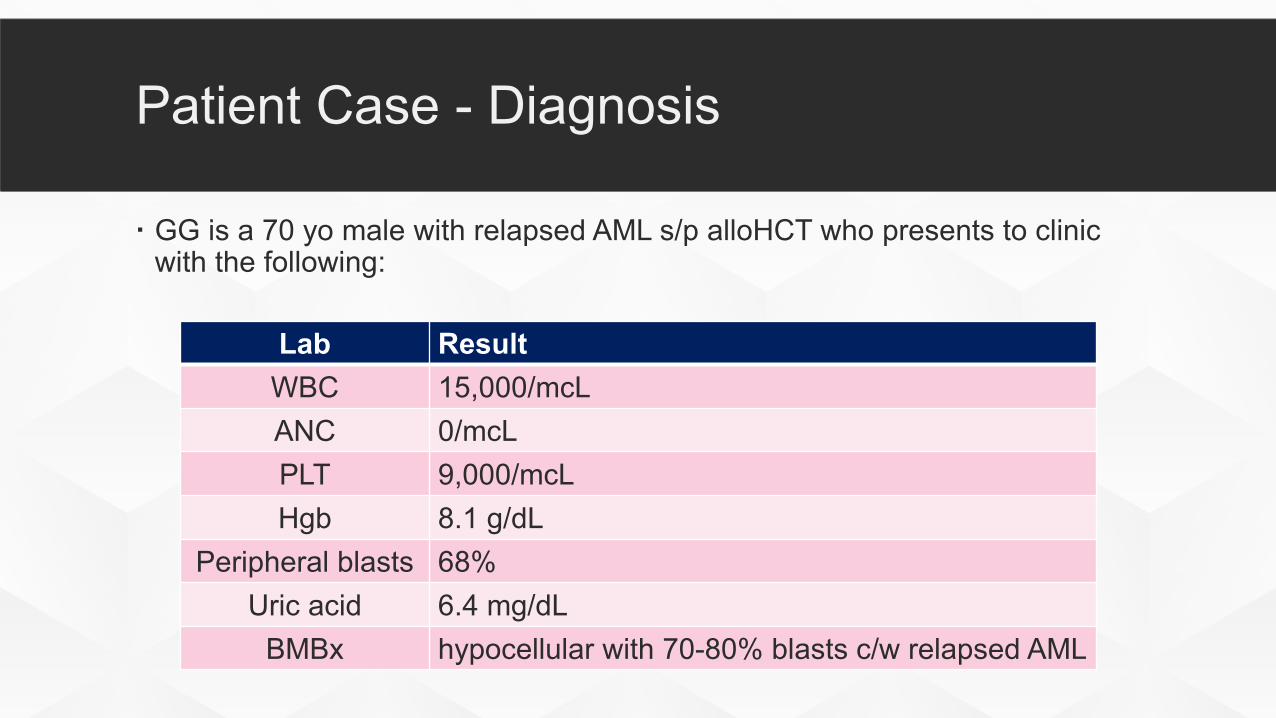
Patient Case - Diagnosis
GG is a 70 yo male with relapsed AML s/p alloHCT who presents to clinic with the following:
Lab ResultWBC 15,000/mcLANC 0/mcLPLT 9,000/mcLHgb 8.1 g/dL
Peripheral blasts 68%Uric acid 6.4 mg/dL
BMBx hypocellular with 70-80% blasts c/w relapsed AML

Patient Case – Cycle 1
Azacitidine + venetoclax selected Since WBC > 10,000-25,000/mcL started on cytoreduction with hydroxyurea x 3 days Since ANC < 500/mcL started on fluconazole, acyclovir, and levofloxacin prophylaxis Since concomitant fluconazole VEN 100 mg on D1, 200 mg once daily thereafter
Cycle 1 Day 1 (C1D1) of AZA 75 mg/m2 x 7d + VEN 200 mg once daily q28d
Lab ResultWBC 9,000/mcLANC 0/mcLPLT 21,000/mcLHgb 7.3 g/dL
Peripheral blasts 75%Uric acid 4.1 mg/dL

Patient Case – Cycle 1-2
C1D29 – VEN held due to pancytopenia pending BMBx pathology
C1D30 – AZA cycle 2 started, VEN held x 1 week Antimicrobial prophylaxis continued
Lab ResultWBC 590/mcLANC 10/mcLPLT 24,000/mcLHgb 7.2 g/dL
Peripheral blasts 0%BMBx normocellular with 5% blasts

Patient Case – Cycle 2-3
C2D31 – Patient seen in clinic prior and started on cycle 3
C2D31 – AZA + VEN cycle 3 started. VEN frequency decreased to D1-21 q28d per MD discretion since patient held x 1 week at start of cycle 2 Antimicrobial prophylaxis continued
Lab ResultWBC 1,640/mcLANC 850/mcLPLT 134,000/mcLHgb 9.6 g/dL
Peripheral blasts 0%
Patient Case – Cycle 3-4
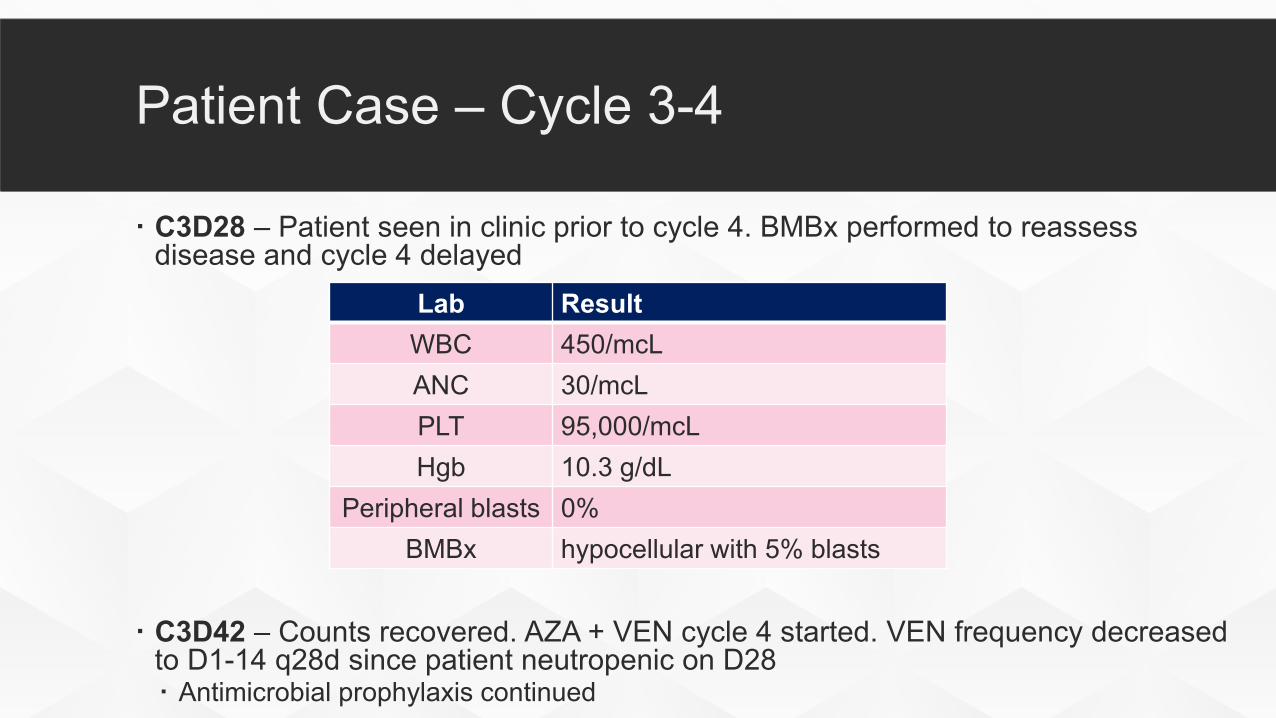
C3D28 – Patient seen in clinic prior to cycle 4. BMBx performed to reassess disease and cycle 4 delayed
C3D42 – Counts recovered. AZA + VEN cycle 4 started. VEN frequency decreased to D1-14 q28d since patient neutropenic on D28 Antimicrobial prophylaxis continued
Lab ResultWBC 450/mcLANC 30/mcLPLT 95,000/mcLHgb 10.3 g/dL
Peripheral blasts 0%BMBx hypocellular with 5% blasts

Patient Case – Cycle 4-5
C4D30 – Patient seen in clinic prior to cycle 5. Cycle 5 delayed due to pancytopenia
C4D44 – Counts recovered. AZA + VEN cycle 5 started. AZA decreased from 7d to 5d, VEN decreased from D1-14 to D1-10, and cycle prolonged to q35d since patient pancytopenic on D30 Antimicrobial prophylaxis continued
Lab ResultWBC 690/mcLANC 150/mcLPLT 35,000/mcLHgb 8.3 g/dL
Peripheral blasts 0%

Patient Case – Cycle 5-6
VEN held since C5D10 and Cycle 6 delayed due to persistent pancytopenia
Interim BMBx – variably cellular with 3-4% blasts
Cycle 6 resumed after 7 week delay. AZA continued on D1-5 q35d, VEN discontinued Antimicrobial prophylaxis continued

Patient Case – Cycle 6-7
C6D36 – Patient seen in clinic prior to cycle 7. Cycle 7 delayed due to pancytopenia
C6D50 – Still pancytopenic, but now has 8% peripheral blasts, so Cycle 7 resumed. AZA frequency increased to D1-7, VEN 200 mg D1-28 resumed, and cycle length decreased to q28d Antimicrobial prophylaxis continued
Lab ResultWBC 1,370/mcLANC 80/mcLPLT <5,000/mcLHgb 8.5 g/dL
Peripheral blasts 0%

Patient Case – Cycle 7-8
C7D29 – Patient seen in clinic prior to cycle 8. Cycle 8 initiated with no dose changes
C8D29 Still pancytopenic despite peripheral blast clearance BMBx – recurrent AML with 22% blasts Chemo regimen changed to gemtuzumab ozogamicin (GO) Admitted with NF and progressive disease. Discharged with home hospice and expired 20
days after starting GO
Lab ResultWBC 1,440/mcLANC 140/mcLPLT 18,000/mcLHgb 7.5 g/dL
Peripheral blasts 4%

Key Takeaways
Check D21-28 BMBx with cycle 1 If in CR/CRi/MLFS hold VEN and delay cycle 2 until ANC > 500, PLT > 50 If > 5% blasts continue VEN and start cycle 2 without delay
Once in CR, low threshold to reduce VEN to D1-21 regardless of cytopeniasresulting in treatment delays
If hematologic recovery takes >7-14d after holding VEN, consider BMBx to assess for relapse then proceed with stepwise reductions Shorten VEN duration (28d 21d 14d) Decrease HMA dose and/or consider decreasing number of HMA doses per cycle Consider prolonging treatment cycle (28d 35d 42d)

UK Markey Cancer Center Approach

Learning Assessment

QUESTION #1
JW is a 67 yo male with relapsed FLT3-ITD mutated AML s/p induction with 7+3+midostaurin, consolidation with HiDAC + midostaurin x 2 cycles and FluMel alloHCT. The team decides to start him on gilteritinib. What antifungal prophylaxis agent would you NOT recommend?
A. VoriconazoleB. FluconazoleC. IsavuconazoleD. Posaconazole

QUESTION #2
A 73 yo female with no significant past medical history is admitted to the inpatient hematology service. She is found to have newly diagnosed de novo AML with normal cytogenetics, no gene mutations, and WBC = 57 x 109/L. The team does not consider her to be a candidate for intensive induction and wants to start her on a HMA + VEN. The patient is currently on antimicrobial prophylaxis with posaconazole, acyclovir, and levofloxacin. Which of the following is your recommendation to the team?
A. Start AZA 75 mg/m2 IV D1-7 + VEN 400 mg PO once dailyB. Start hydroxyurea until WBC < 10-25 x 109/L then begin AZA 75 mg/m2 IV D1-7 + VEN 50-100
mg PO once dailyC. Start DEC 20 mg/m2 IV D1-10 + VEN 200 mg PO once dailyD. Start hydroxyurea until WBC < 10-25 x 109/L then begin DEC 20 mg/m2 IV D1-10 + VEN 200 mg
PO once daily

QUESTION #3
This patient is started on hydroxyurea until WBC < 10-25 x 109/L then started on AZA 75 mg/m2 IV D1-7 + VEN 100 mg PO once daily. Her D28 BMBx indicates aplasia with 2% blasts and her ANC = 0/μL. What is your recommendation to the team?
A. Stop VEN and delay cycle 2 until ANC > 500/μL or up to 14 daysB. Continue VEN and repeat BMBx on D35C. Stop VEN and delay cycle 2 by 7 days regardless of ANC at that timeD. Continue VEN and start cycle 2 without delay

Oral Chemotherapy Clinical Pearls in AML
Rob Walchack, PharmD, BCOP
Hematology/Cellular Therapy Clinical Pharmacy Specialist
UK HealthCare
September 17, 2021