Embed Size (px)
Citation preview

Surgical Options for Weight Regain
(or Poor Weight Loss)
After Sleeve Gastrectomy
Jin S. Yoo M.D.
Assistant Professor of Surgery
Duke University Medical Center

Financial Disclosures
• Covidien (consultant / speaker)
• Cook Medical (consultant / speaker)
• W.L. Gore (consultant / speaker)
• Teleflex (consultant)

Meta-analysis of outcomes of SG in high/
risk staged approach versus primary procedure
Page 3
• 36 SG studies
- 2 RCTs (112 patients with 56
SG patients)
- 1 non-randomized controlled
trial (91 patients with 39 SG
patients)
- 33 cases series (2,475 SG
patients)
Brethauer SA et al. SOARD 2009; 14 (6): 469-75

Review Article on SG studies
Page 4 Shi X et al. Obes Surg 2010; 20: 1171-7.
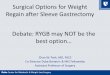
Sleeve versus the other procedures
Page 5 Shi X et al. Obes Surg 2010; 20: 1171-7.
Definition of “Weight Regain” and
“Poor Weight Loss”
• DEFINITION ARBITRARY and TEMPORAL FACTOR
• “Poor Weight Loss”
- < 30-50% of EWL after primary procedure (at least 2 years out)
• “Weight Regain”
- After “successful” weight loss, regain of “significant” weight (>
20% of weight regain from their nadir)
Page 6

Data from Interntional Sleeve Gastrectomy
Expert Panel Consensus Statement
Page 7 Rosenthal RJ et al. SOARD 2012; 8: 8-19
SURGEON Cases (n) Average BMI Bougie Size (Fr) Reinforcement Stricture (%) Leak (%) Post-op GERD (%) Wt Regain or Poor Wt Loss (%)
Ramos-Galvao 714 45 32 1 0.14 0.42 6.02 0.84
Shah-Todkar 498 49 36 1 0.2 0.4 28 1
Aceves 1127 42 36 1 0.35 0.62 18 1
Jossart 617 47 32 1 0 0.6 20 1.6
Noca 700 46 36 0 0 3.9 15 2.8
Lakdawala 484 44 36 3 0 1.2 10 3.3
Vix 350 46 36 1 0.5 3 10 3.5
Prager 267 50 48 3 0.8 3.3 31 4.9
Basso 505 47 48 3 0 2.7 10 6.1
France 716 43 34 2 1.4 0.7 7 8
Zundel 892 42 34 1 1 0 1 12
Baker 828 54 34 2 0.12 0.5 15 15
Boza 1431 37 50 1 0.06 0.5 0.5 18.5
Bellanger 675 44 34 0 0 0 5 23
Jacobs 526 45 36 3 0.19 1.5 NR 28
Rosenthal 547 45 42 1 0.2 0.36 27 NR
Himpens 710 43 32 3 1 2.9 23 NR
Arvidsson 700 35 32 1 0.3 1.1 10 NR
Jorgenson 512 45 36 2 0.5 0 10 NR

Causes of POOR WEIGHT LOSS after SG
• Lost to follow-up
- no guidance or education
- no accountability
- also increase risk of developing long-term
complications
• Dietary non-compliance
- due to complacency
- due to lack of guidance and/or education
- recurrence or new development of maladaptive
eating habit / disorder
Page 8

Causes of POOR WEIGHT LOSS after SG
CONT
• Increase in portion size
- sleeve dilation?
- psychologic?
Page 9
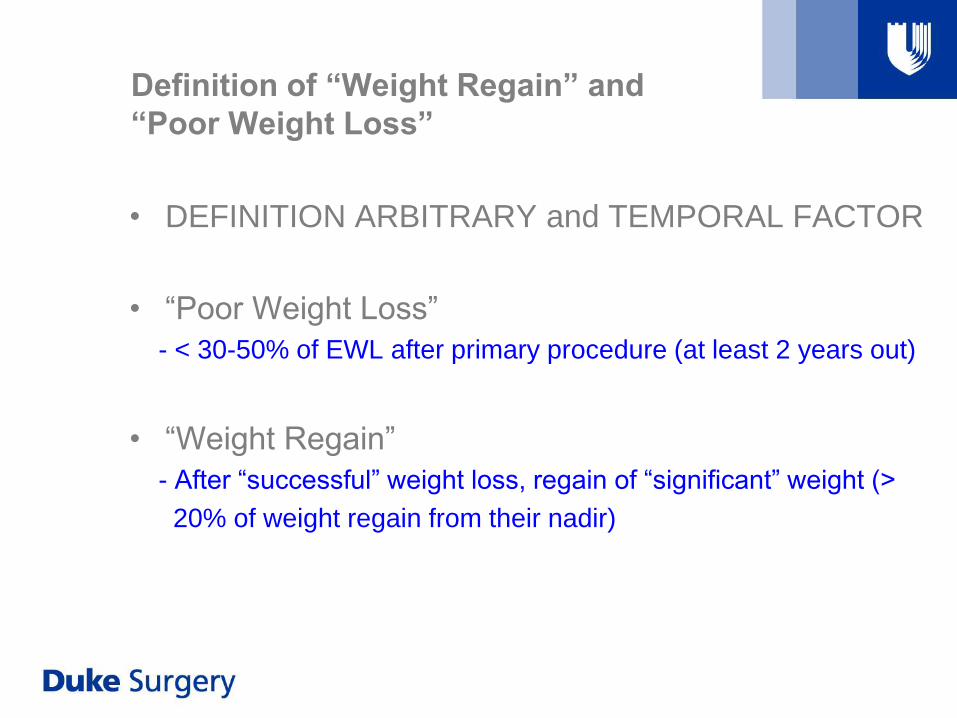
Page 10 Slide borrowed from Dr. Rudolf Weiner’s 8 year follow-up after SG

Weight regain and/or poor weight loss
is NOT an urgent indication for revision…
• A thorough evaluation is a must
- review op note, pre-op/post-op clinic notes
- obtain UGI series and EGD
- consider esophageal manometry (if UGI series abnormal)
• Evaluation with psychologist and dietician
• Proof of compliant behavior and follow-up
• Surgeon/Patient expectation
Page 11
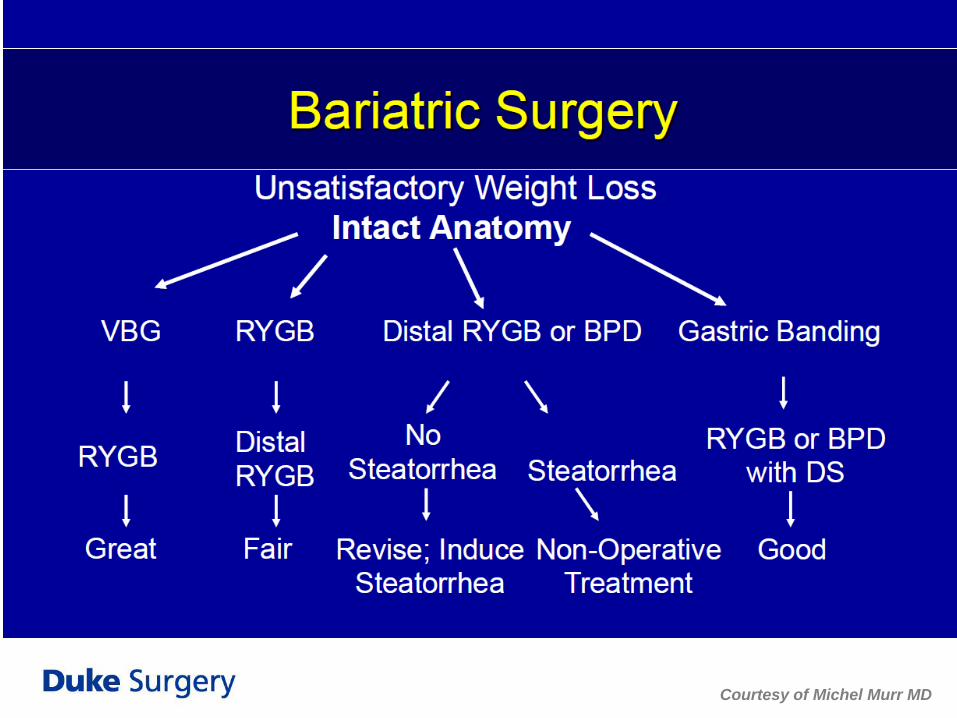
Page 12
Courtesy of Michel Murr MD

Page 13
Courtesy of Michel Murr MD
Insufficient Weight Loss and/or Weight Regain
Re-sleeve
• Perfect candidate:
1) has a correctable anatomic defect – dilation of sleeve
stomach
2) someone who had good weight loss, but regained some
weight despite “perfect” diet.
3) someone who had insufficient weight loss, despite “perfect”
diet
4) still doesn’t (or cannot have) gastric bypass
• If the patient does not have a correctable anatomic
defect, then not a good option (do something else)
14

Insufficient Weight Loss and/or Weight Regain
Re-sleeve
• Possible causes of sleeve dilation
- last fire of stapler > 1 cm away from GE junction
- missing posterior gastric fold of the fundus near GE junction
- missing a hiatal hernia
- creating a gastric tube that is too large
- antral dilation
15

Page 16
Etiology of sleeve enlargement CONT
How close do you get to the GE junction?

Page 17
Etiology of sleeve enlargement
Bougie size? How close do you snug the Bougie?
RISK OF STRICTURE/LEAK RISK OF DILATION

Etiology of Pre-pyloric dilation
Does it matter where you start?
Page 18
INCREASE RISK OF GERD INCREASE RISK OF WEIGHT REGAIN

• fgfggfgf
Page 19 Iannelli A et al. Obes Surg 2011; 21: 832-5. (France)
-13 patients
-all had proximal stomach dilation
-Mean BMI 44.6 32.3 -> 32 -> 27.5
1m 6m 12m

Considerations when re-sleeving
Sleeve dilation
Page 20
• Use a smaller bougie
and/or hug the
bougie tighter
• Make sure the new
staple line stays
INSIDE the old
staple line (avoid
creating ischemic
zone)
• Anticipate thicker
tissues
AREA OF ISCHEMIA

• RATIONALE:
1) To slow passage of food bolus across the proximal part of the
stomach to achieve satiety while…
2) Maintaining fast transit of food bolus into small intestines to
trigger the “ileal break” mechanism (and other hormonal
changes)
• Another example adding a restrictive procedure to
another restrictive procedure.
- BOB (band over bypass)
- BUB (bypass under band)
21
Insufficient Weight Loss and/or Weight Regain
Band over a sleeve

Insufficient Weight Loss and/or Weight Regain
Band over a sleeve
• First case report of adjustable gastric banding after
“failed”gastrectomy
• 42yo male who failed to lose sufficient weight after SG
• Patient refused adding malabsorptive component due to
dependence on several anti-psychotic medications
• At 9 months from his second surgery, he has achieved 57%
EWL from his original weight of 390 lbs
22 Greenstein AJ et al. Surg Endosc 2009; 23: 884

Insufficient Weight Loss and/or Weight Regain
Band over a sleeve
• First case report of adjustable gastric
banded sleeve gastrectomy as a
primary procedure
• 39yo female, BMI 80
• Band secured 6cm distal to GE
junction, secured laterally with sutures
to peri-pancreatic tissue
• Doing well 6 weeks post-op
23 Agrawal S et al. Obes Surg 2010; 20: 1161-3 (UK)

Page 24 Obes Surg 2009; 19: 1591-6

Insufficient Weight Loss and/or Weight Regain
Sleeve to Gastric Bypass
• Historically, BPD/DS and RYGB has been the
second part of the “staged approach” for high-risk
patients
• Sleeve-to-bypass revision are now being performed
for other indications – insufficient weight loss,
significant weight regain, significant post-op GERD,
stricture, and chronic fistula
25

Page 26 Obes Surg 2010; 20: 835-40. (Austria)

Page 27 Obes Surg 2013; 23: 212-5. (France)
Technical Considerations
Sleeve to Gastric Bypass
• Straightforward… transect the gastric tube, 5-6 cm
distal to the GE junction to create gastric pouch
• Things to keep in mind…
- managing small-caliber gastric pouch
- in cases with lot of adhesions, limit dissection on the lesser
curvature of the proximal gastric tube
- be careful of clips!!!
- should the gastric tube remanant be resected?
28

Insufficient Weight Loss and/or Weight Regain
Sleeve to BPD / DS
• SG is part of the BPD / DS
• Historically, conversion of SG to BPD/DS (or RYGB)
is the expected 2nd procedure of a staged approach
for high risk patients
• Now, also being performed for insufficient weight
loss / significant weight regain
29

Technical Considerations
Sleeve to BPD / DS
• Straightforward… continue on with BPD/DS
procedure
• Things to keep in mind…
- consider re-sleeving the gastric tube (if dilation found)
30
Summary
• Proper patient selection is key for any revisional
surgery, especially when done for poor weight loss
or weight regain
• Technical improvements on the way we do sleeves
have been recommended by sleeve experts to
minimize “surgical failures” as the cause of poor
weight loss or weight regain.
• Good intermediate results are possible with RYGB
and SG after failure of SG.
Page 31
Which one of these statements is FALSE regarding revisional
surgery after sleeve gastrectomy?
A) Surgical failure (i.e. sleeve dilation) is the most common
cause of insufficient weight loss and/or weight regain after
sleeve gastrectomy.
B) A more intense pre-operative evaluation should be
implemented for patients who are considering revisional
surgery for poor weight loss or weight regain.
C) When performing re-sleeving procedure, care should be taken
not to cross the previous gastric transection staple line to
avoid ischemic complications.
Page 32