Embed Size (px)
Citation preview

Optimizing Diabetes and Hyperglycemia Management
in the Inpatient Setting - Overview
Greg Maynard M.D., Clinical Professor of Medicine
Director, UCSD Center for Innovation and Improvement Science
CMO, Society of Hospital Medicine
Introductory Session 1 of 4: NYSP4P Initiative

Greg Maynard - Conflict of Interest Statement
• AHRQ grants to improve glycemic control and reduce
hypoglycemia
• SHM CMO - SHM is not-for-profit that offers some
products for glycemic control QI initiatives and
measurement tools. No personal fiscal COI.

Session I - Feb 12th Dr. Greg Maynard
– Why inpatient glycemic control is important
– Overview of IV and SC insulin best practices, how to implement
– Framework for Improvement
• Session II - Feb 26th Dr. Kristi Kulasa
– Inpatient glycemic team structure -
– Coordination of meals / insulin / testing
– Top things we teach / reinforce
– Basal / bolus cases and special situations (TPN, TF, NPO, Steroids, Transition IV to SC insulin)
• Session III - March 12th Dr. Greg Maynard
– Safe use of insulin summary
– Hypoglycemia Management and Prevention
– Measurement and Monitoring – month to month and day to day
– SHM and other resources
• Session IV - March 19th Drs. Kulasa and Maynard
– FAQs / Q&A
– Transitions
– Barriers and How to Overcome Them

Mentored Implementation
Collaborative

Why Glycemic Control? (It’s about more than infusion insulin glycemic targets!)
• DM / Hyperglycemia Very Common - More common in Hispanic groups and African Americans
• Opportunity to identify and intervene
– poorly controlled DM, previously undiagnosed DM, stress hyperglycemia (pre-diabetes)
• Hypoglycemia and extreme hyperglycemia
– Safety problem and a Quality problem
• Inpatient Care - Complex w/ unique challenges
– Education alone insufficient, need systems change
• Huge Implementation Gap - Chaotic baseline
• Public reporting, regulatory guidelines etc.
Society of Hospital Medicine.
http://www.hospitalmedicine.org/ResourceRoomRedesign/ pdf/GC_Workbook.pdf.

Distribution of patient-day-weighted mean POC BG values for ICU & non-ICU settings
DATA from ~49 million POC-BG testing) from 3.5 million patients. The
mean POC-BG was 167 mg/dL for ICU patients and 166 mg/dL for non-
ICU patients.
Swanson et al. Endocrine Practice, October 2011

SHM Benchmarking tools – Scatterplot
Uncontrolled hyperglycemia Y Axis
Hypoglycemia rate - X axis Both are highly variable

Michelangelo's famous statue, David, returns
to Italy after tour of United States
Global Prevalence of DM to double by 2030!
Essential Elements Successful PI Efforts
• Institutional support – buy in – Staff engagement and training
– Standardization of order sets, help with measures
• Teams and Culture of Improvement
• Understand Current Process
• Willingness to Redesign process
• Defined goals
• Metrics – reliable, practical, rapid feedback
• Guidance in order sets and other venues
• Hardwire - Reliable Interventions
• Ongoing informed improvement
• Educational programs


A Series of Linked Protocols: Reinforce protocols by multiple methods, hardwire whenever possible
Basic Protocols Always More to Do
SC insulin SC Insulin Pumps
IV infusion insulin Monitoring
Periop management Coordination: CHO / BG test / insulin
Hypoglycemia Management Transitions
Patient Education Provider Education / competency

How do I get medical staff and others on board?

Getting the docs on board Changing culture as well as practice
• Build the burning platform…and a way to get off of it!
• Institutional carrots and sticks
• Easy to understand message (marketing)
• Influential / high volume champion
• Path of least resistance first.
• Local data and anecdotes rule.
• Just-in-time education and feedback.
• Make it easy to do right thing, harder to do wrong thing.
• Show that your protocol works.
• Address misconceptions / misinterpretations up front

Sutter Sacramento Examples Staff engagement
“2 over 200” Campaign
– Modeled after political campaign
– 600 providers signed “petition” stating they would address add or
increase insulin for every inpatient with two BG values > 200 mg/dL
– Buttons and posters “Our patients may be insulin resistant, but we’re
not!”
“Sugar Stars”
– Competition between inpatient units
– Star on public board every time high BG values were addressed
– Unit with most stars - Pizza Party!

1.ACE/ADA Task Force on Inpatient Diabetes. Diabetes Care. 2006 & 2009 2.Diabetes Care. 2009;31(suppl 1):S1-S110.
Antihyperglycemic Therapy
Insulin
Recommended
OADs
Not Generally Recommended
IV Insulin
Critically ill patients in the
ICU
SC Insulin
Non-critically ill patients
Recommendations for Managing Patients With Diabetes in the Hospital Setting

NICE-SUGAR Study Outcomes (only 20% had diagnosis of DM)
Outcome
Measure
Intensive
Group
Conventional
Group
Morning BG (mg/dL)
118 + 25
145 + 26
Hypoglycemia
(≤ 40mg/dL)
206/3016
(6.8%)
15/3014
(0.5%)
28 Day Mortality
(p=0.17) 22.3% 20.8%
90 Day Mortality
(p=0.02) 27.5% 24.9%
The NICE-SUGAR Study Investigators. N Engl J Med. 360:1283-1297, 2009.
97% infusion 69% infusion

NICE-SUGAR vs UCSD
NICE
Intervention
NICE
“Usual”
UCSD
N = 200
Target
(mg/dL)
80 – 110 144 - 180 90 – 150
Median
Glucose
107 141 121
Glucose
< 40 mg/dL
6.8% 0.5% 1%
Local Data Needed to Set Upper Limit Target < 180 mg / dL

Critical Care Medicine 2012; 40:3251-3276

Glycemic Targets – When to Initiate Insulin
SCCM - BG ≥ 150 mg/dL should trigger initiation of
infusion, titrated to keep <150 mg/dL, absolutely < 180
mg/dL.
ADA – Initiate at threshold no higher than 180 mg/dL to keep
between 140 – 180 mg/dL. Lower targets 110-140 mg/dL
may be beneficial in some populations, IF that goal can be
achieved with low hypoglycemia rates.
Don’t target euglycemia < 110 mg/dL

Insulin Infusion Regimens
• Computerized models may have an edge in RCTs
– Rate changes triggered by both glucose value and a multiplier that
relates to insulin sensitivity factors
• Paper based control can be quite good and safe too
– Complexity can be a problem
– Regimens that do not take rate of glucose change into account might
be problematic
• Both require effort and safety culture to achieve optimal use
• Consistent CHO intake makes life easier
– Use CHO counting and SQ insulin if boluses
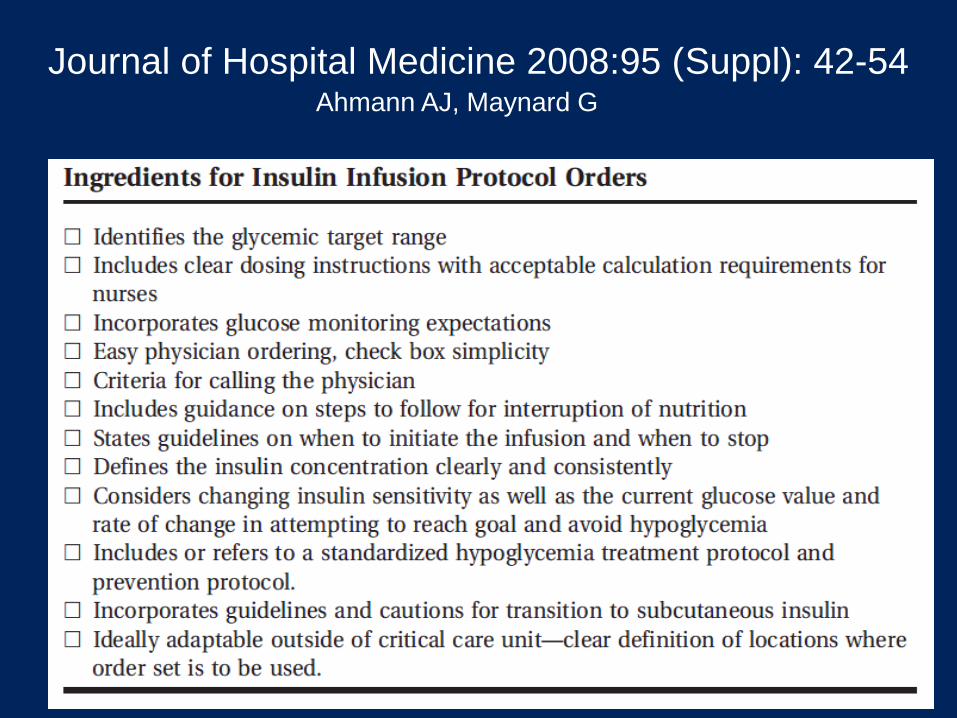
Journal of Hospital Medicine 2008:95 (Suppl): 42-54 Ahmann AJ, Maynard G
Administering IV insulin infusion
• Prime the tubing
• Standard concentrations of 1 unit/mL
• Smart pumps
• Monitor q 1 – 2 hours
• Know limitations of glucometers
• Arterial or whole blood sampling preferred if severe edema, shock, vasopressors
• Look for ways to reduce nursing burden

Transition from Intravenous to Subcutaneous Insulin
• Patients with type 1 and type 2 diabetes should
be transitioned to scheduled SC insulin therapy
at least 1–2 h before discontinuation of CII.
• Administer SC insulin before discontinuation of
CII for patients without a history of diabetes who
have hyperglycemia requiring ≥ 2 U/h.
• POC testing with daily adjustment of the insulin
regimen after discontinuation of CII.
Endocrine Society Non-ICU Guideline. J Clin Endocrinol Metabol 97: January 2012

Focus on the non-ICU Wards: Implementation Gap
• > 1/3 with mean glucose > 180 mg/dL
• 60%-70% of insulin regimens sliding scale only (even if horrible control)
• >15% with hypoglycemic episodes during their stay
• 5.7% of patient-days hypoglycemic in non-critical care units
• 40% of patients with hypoglycemia have more events
• Uneven training / performance amongst staff
• Poor coordination of tray delivery, monitoring, and insulin
• Inconsistent transitions
• Patients often confused or angry

Integrate Best Practice into protocols, order sets, documentation
• Actionable glycemic target
• Constant carbohydrate / dietary / consult
• A1c
• Education plan
• Hypoglycemia protocol
• Guidance for transitions (linked protocols)
• Coordinated monitoring / nutrition / insulin
• DC oral agents, insulin preferred
• Insulin regimens for different conditions
• Dosing guidance



Mandatory order set use,
prompt to DC oral agents
Glycemic target, prompt for
education, Diets all CHO limited.

Admonition to avoid sliding scale.
Dosing guidance for transition from
infusion.
Different SQ regimens for different intake.
Hypoglycemia protocol
A1c order checked off.

For eating patient:
Dosing guidance
Basal / Bolus default
Last glucose / A1c displayed
Correction scale matches TDD

Glycemic Targets in Non-Critical Care Setting
1. Premeal BG target of <140 mg/dl and random BG <180 mg/dl for the majority of patients.
2. Glycemic targets be modified according to clinical status. – For patients who achieve and maintain glycemic control without
hypoglycemia, a lower target range may be reasonable.
– For patients with terminal illness and/or with limited life expectancy or at high risk for hypoglycemia, a higher target range (BG <200 mg/dl) may be reasonable.
3. For avoidance of hypoglycemia, we suggest that antidiabetic therapy be reassessed when BG values are 100 mg/dl). Modification of glucose-lowering treatment is usually necessary when BG values are <70 mg/dl.


A1C for Diagnosis of
Diabetes in the Hospital In-hospital hyperglycemia is defined as an admission or
inhospital BG > 140 mg/dl.
A1c > 6.5% can be identified as having diabetes, < 5.2% can exclude diabetes.
Implementation of A1C testing can be useful:
assist with differentiation of newly diagnosed diabetes from stress hyperglycemia
assess glycemic control prior to admission
designing an optimal regimen at the time of discharge
Moghissi ES, et al; AACE/ADA Inpatient Glycemic Control Consensus
Panel. Endocr Pract. 2009;15(4).
Umpierrez et al, Endocrine Society Non-ICU Guideline. J Clin
Endocrinol Metabol 97(1):16-38, 2012

Antihyperglycemic Therapy
SC Insulin
Recommended for
most medical-surgical
patients
OADs
Not Generally
Recommended
Pharmacological Treatment of Hyperglycemia in Non-ICU Setting
1.ACE/ADA Task Force on Inpatient Diabetes. 2.Diabetes Care. 2006 & 2009 3.Umpierrez et al, Endocrine Society Non-ICU Guideline. J Clin
Endocrinol Metabol 97: January 2012
Continuous IV Infusion Selected medical-surgical
patients

Key things to know about SC insulin management in the hospital White font – today Yellow font – future sessions
• Just do it! (when glucose over target)
• Basal / Nutritional (prandial) / Correctional
• What do I do when the nutrition stops? NPO p MN?
• Giving that first dose (how do I do this)?
• 50:50 rule –
• Perioperative management?
• How should we manage at transitions?
• How do we manage inpatients in special situations?
– steroids, TPN, etc
• Best strategies to reduce iatrogenic hypoglycemia?

Physiologic Insulin Secretion: Basal-Bolus Concept
Breakfast Lunch Supper
Insu
lin
(µU
/mL
)
Glu
co
se
(mg
/dL
)
Basal glucose
150
100
50
0 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9
A.M. P.M.
Time of Day
Basal insulin
50
25
0
Nutritional glucose
Nutritional (prandial) insulin
Suppresses glucose
production between
meals and overnight
The 50/50 rule

Which Patients Need Basal Insulin?
• “Insulin-deficient” patients should always have basal insulin (even NPO): – Type 1 DM or DKA, pancreatic insufficiency
– A history of type 2 DM for 10 years or more
– On any insulin for 5 years or more
– Wide fluctuations of glucose values
• Preprandial glucose > 140 mg/dL consistently
• Random glucose > 180 mg/dL


Constructing a Profile for Scheduled Subcutaneous Insulin ….
6 am 12 pm 6 pm 12 am
Glargine
Detemir
NPH
Regular
Glulisine
Lispro
Aspart

Calculating Insulin Dosage (Total Daily Dose)
• Calculate from insulin infusion amount
– Recent steady state hourly rate x 20, for example
• Add up insulins taken at home, adjust for glycemic control and other factors
• Calculate from weight, body habitus, other factors

Calculate starting total daily dose (TDD)
0.4 – 0.5 units/kg/day
Reduce to 0.3 units/kg/day if hypoglycemia risk
increase to 0.5 – 0.6 units/kg/day if overweight / obese
Adjust TDD up or down based on
Past response to insulin
Presence of hyperglycemia inducing agents, stress
Basal insulin = 50% of TDD
Glargine q HS or q AM, detemir in 1 or 2 doses
Starting Basal-Bolus from Scratch

Case 1 : Initiating Subcutaneous Insulin in an obese patient eating regular meals
• 56 year old man admitted with diabetic foot infection, eating regular meals.
• Obese, weighs 100 kg
• Home regimen – 2 OHG’s and 20 units of NPH q HS
• Baseline Control: – HbA1c of 10, POC glucose in ED 240 mg/dL
• What are your initial orders?

Obese male eating regular meals 2 oral agents, 100 kg, A1c 10, BG 240 Best regimen?
A. Continue oral agents and increase NPH by 10 units
B. Continue oral agents, discontinue NPH, start glargine 30 units q HS
C. DC oral agents: Glargine 30 units q HS Lispro 10 units q ac
D. DC oral agents: Glargine 15 units q HS Lispro 10 units q ac

Solutions for Obese, eating patient
• Best answer is C
• POC BG checks AC and HS
• Stop oral agents and NPH insulin
• TDD: 100 kg x 0.6 units/kg/day = 60 units
largine (Lantus) Alternative
– Basal: Glargine 30 units q HS
– Nutritional: Lispro 10 units q ac
– Correction: Lispro per scale q ac and HS

Case continued - Patient to be NPO after midnight for debridement in the morning. Expected to be eating again by noon. How do you handle insulin?
A. Discontinue all insulin after evening meal to avoid hypoglycemia
B. Discontinue all insulin after evening meal except correction dose (sliding
scale) insulin.
C. Do not give AM nutritional insulin. Reduce glargine to 15 units, give
correction insulin.
D. Do not give AM nutritional insulin. Give glargine 30 units SC AND
correction dose insulin.
E. Do not give AM nutritional insulin. Give glargine 25 units SC AND
correction dose insulin
F. D or E are both acceptable

Case continued - Patient to be NPO after midnight for debridement in the morning. Expected to be eating again by noon. How do you handle insulin?
A. Discontinue all insulin after evening meal to avoid hypoglycemia
B. Discontinue all insulin after evening meal except correction dose (sliding
scale) insulin.
C. Do not give AM nutritional insulin. Reduce glargine to 15 units, give
correction insulin.
D. Do not give AM nutritional insulin. Give glargine 30 units SC AND
correction dose insulin.
E. Do not give AM nutritional insulin. Give glargine 25 units SC AND
correction dose insulin
F. D or E are both acceptable

Give 70 to 100 % of usual dose of glargine or
detemir insulin (or 50 to 70 % of NPH insulin)
PLEASE don’t hold basal insulin altogether!
Nurses, this means you too!
Reduction in basal dose advisable if patient
tightly controlled, or if they take basal insulin
to cover nutritional needs as well as basal
needs.
Pre-op recommendations for insulin
treated patients with diabetes
DiNardo MM et al Endo Pract 17:552 2011

211 Patients with type 2 DM that underwent general surgery
Glargine + Glulisine (Gla+Glu)
N= 104
Group 1: 0.5 U/kg
Half as glargine once daily Half as glulisine before meals
Sliding scale insulin (SSRI) N= 107
OPEN - LABELED RANDOMIZATION
Group 2:
4 times/day for BG >140 mg/dl
RABBIT SURGERY TRIAL
Umpierrez et al, RABBIT 2 Surgical. Diabetes Care. 2011 Feb;34(2):256-61. Epub 2011 Jan 12.

Rabbit Surgery Trial
Glucose levels during basal bolus and SSI therapy
*
† ‡ *
Duration of Treatment (days)
† †
R 1 3 2 4
Glargine+Glulisine
Sliding Scale Insulin
5 6 7 8 9 10
* p<0.001; † p=0.01 ‡p=0.02
R= Randomization
Umpierrez et al, Diabetes Care 34 (2):1–6, 2011

Postoperative Complications
P=0.003
P=NS
P=0.05 P=0.10
P=0.24
Glargine+Glulisine
Sliding Scale Insulin
Umpierrez et al, Diabetes Care 34 (2):1–6, 2011
* Composite of hospital complications: wound infection, pneumonia, respiratory
failure, acute renal failure, and bacteremia.

Session I - Feb 12th Dr. Greg Maynard
– Why inpatient glycemic control is important
– Overview of IV and SC insulin best practices, how to implement
– Framework for Improvement
• Session II - Feb 26th Dr. Kristi Kulasa
– Inpatient glycemic team structure -
– Coordination of meals / insulin / testing
– Top things we teach / reinforce
– Basal / bolus cases and special situations (TPN, TF, NPO, Steroids, Transition IV to SC insulin)
• Session III - March 12th Dr. Greg Maynard
– Safe use of insulin summary
– Hypoglycemia Management and Prevention
– Measurement and Monitoring – month to month and day to day
– SHM and other resources
• Session IV - March 19th Drs. Kulasa and Maynard
– FAQs / Q&A
– Transitions
– Barriers and How to Overcome Them

Safe Glycemic Control
A Team Sport
Questions and Comments?
Next Session Feb 26th -
Dr. Kristi Kulasa





























