Embed Size (px)
Citation preview

Opioid Dependence: Treatment Options
Walter Ling MDIntegrated Substance Abuse Programs(ISAP)
UCLA
Suboxone Advisory Board MeetingKaohsiung, TaiwanNovember 4, 2007

Treating Opioid Addiction: Aims
• Getting off opioids: detoxification– Agonist opioid based detoxification– Non-opioid based detoxification– Antagonist based detoxification
• Staying of opioids: relapse prevention– Agonist maintenance: methadone/others– Antagonist maintenance: naltrexone– Partial agonist maintenance: buprenorphine
• Changing life style

Phases of Opioid Withdrawal1. Anticipatory withdrawal (3-4 hrs)
Fear of withdrawalAnxietyDrug seeking
2. Early Withdrawal (8-10 hrs)
Anxiety
Restlessness
Nausea
Nasal stuffiness
Abdominal cramps
Drug seeking
Hypertension
Tachycardia
Yawning
Sweating
Rhinorrhea
Lacrimation
Dilated pupils
3. Fully Developed Withdrawal3. Fully Developed Withdrawal(1-3 days)
Severe anxiety
Restlessness
Muscle spasm
Elevated BP
Fever/Chills
Drug seeking
Tremor Piloerection
Vomiting
Diarrhea
Tachycardia
4. Protracted Abstinence4. Protracted Abstinence (up to 6 mos.)
Hypotension
Bradycardia
Insomnia
Loss of appetiteLoss of energyCue induced craving

Determinants of Withdrawal Severity• Triggers and intensity of withdrawal
– Amount and regularity of use – Rate of withdrawal– Patient physical & psychological
condition and expectation• Settings and the severity of withdrawal
– Presence of opiates vs absence – Treatment setting and environment – Physician confidence and attitude – Medications for symptom relief and general nutrition

Detoxification
• Relieve Symptoms of withdrawal
• Reverse neuro-adaptation from chronic heroin use
• Reduce degree of physical dependence
• Promote long term treatment leading to life style changes
• Transitional treatment strategy
CH3 CH2CH2 CH N
CH3CH3
CH3
O
Methods and Medications• Methadone and buprenorphine
– Opioids agonist and partial agonist
– Short and long term
• Clonidine and Lofexidine– Non-opioids; alpha adrenergic
agonists
• Antagonists assisted – Naloxone /Naltrexone
– Rapid and ultra-rapid detoxifications

Detoxification• The most common
outcome of detoxification, by whatever means and for however long, is relapse. “Detoxification may be good for a lot of things; staying off drugs is not one of them”
0
20
40
60
80
100
1 2 3 4 5 6 7 8 9 10 11 12
In Treatment
Rate
28.9%
Months Since Drop Out
1-3Months
Later
4-6MonthsLater
45.5%
57.6%
72.7%
82.1%
7-9Months
Later
10-12MonthsLater
Ball, JC, Ross A. The Effectiveness of Methadone Maintenance Treatment, Springer-Verlag, New York, 1991
Pe
rce
nt
IV U
se
rs
Relapse to IV Drug Use After Termination of Methadone Maintenance Treatment
Clonidine for Opioid Withdrawal -2 adrenergic agonist binds to
pre-synaptic autoreceptors on adrenergic neurons– In Locus Coeruleus– Possibly in A1 and A2 cell groups
of the caudal medulla that project to BNST (extended amygdala)
• FDA approved for hypertension– Limiting side effect: hypotension
• Reduces W/D signs and sx:– Significantly better than placebo– Nearly comparable to slow
methadone taper
• Doses: 0.1 mg tid to 0.4 mg tid
• Push dose until withdrawal sx abate or diastolic BP <60
• Use adjunctive benzodiazepines, anti-emetics, anti-diarrheals

Rapid &Ultra Rapid Opioid Withdrawal
• Patient placed under deep sedation or general anesthesia • Administer opioid antagonists to provoke W/D
• Manage emergent sx with:– Clonidine/ Lofexidine
– Benzodiazepines
– Antiemetics
– Antidiarrheals
• W/D essentially resolved in 12-24 hours (ultra rapid) or 2-3 days (rapid) with patient ± on full dose of antagonist (naltrexone)

Opioid Substitution or Maintenance Therapy
• Reduce symptoms & signs of withdrawal
• Reduce or eliminate craving
• Blocks effects of illicit opioids
• Restored normal physiology
• Promote psychosocial rehabilitation and non-drug life style
OOH O
N
OH
Maintenance Medications:• Methadone maintenance
(agonist)• Naltrexone (antagonist)• Buprenorphine (partial
agonist)– Buprenorphine (Subutex)
– Buprenorphine-naloxone (Suboxone)
CH3 CH2CH2 CH N
CH3CH3
CH3
O

Methadone: Clinical Properties
Orally active synthetic μ opioid agonist with morphine-like properties
Action—CNS depressant/ Analgesic
Quick absorption, slow elimination, long half-life
Effects last 24 hours; once daily dosing maintains constant blood level
Prevent withdrawal, reduce craving and use
Long term treatment normalize physiological function
Facilitates rehabilitation
CH3 CH2CH2 CH N
CH3CH3
CH3
O
Methadone Pharmacokinetics•Good oral bioavailability; fast and complete absorption•Peak plasma concentration 21/2 hrs (liquid), 31/2 hrs (tablet); mean half-life 24 hrs, steady state 3-10 days•96% plasma protein bound•Variable bioavailability (40%-99%);genetic variations in protein binding, oxidative metabolism and GI (majority) and renal (minor) excretion, capacity limited clearance•Onset of analgesia 15-20 min; difficult to predict initial dose and dosing frequency.•Metabolism mediated via P450 cytochrome, primarily
•CYP3A4, but also CYP2D6, CYP1A2, CYP2C9 CYP2C19
Clinically significant drug/drug interactions

Methadone and CYP3A4 Enzyme
• CYP3A4: Inducible enzyme– Methadone induces its own metabolism; levels vary
over time; 3.5 fold increase in clearance between induction and steady state
• Increases metabolism of certain drugs:– Dilantin, Tegretol, Barbiturates, Rifampin, Cypro,
Verapamil, Zidovudine, amitryptyline, spinololactone, and others
• Decrease metabolism of certain other drugs:– Fluvoxamine, Nefazedone, Omeprazole, Indinavir, Nelfinavir, Ritonavir, Fluoxetine, Saquinavir, other
SSRI’s

Pharmacodynamics• Full agonist; receptor affinity lower than Ms
– Main action on mu receptors• inhibit adenyl cyclase = cAMP potasium channel opening calcium channel opening
– also inhibit serotonin reuptake– also non competitive antagonist NMDA receptor
• No known active metabolites; limited toxicity– No significant cognitive impairment with chronic use– No organ toxicity with chronic use
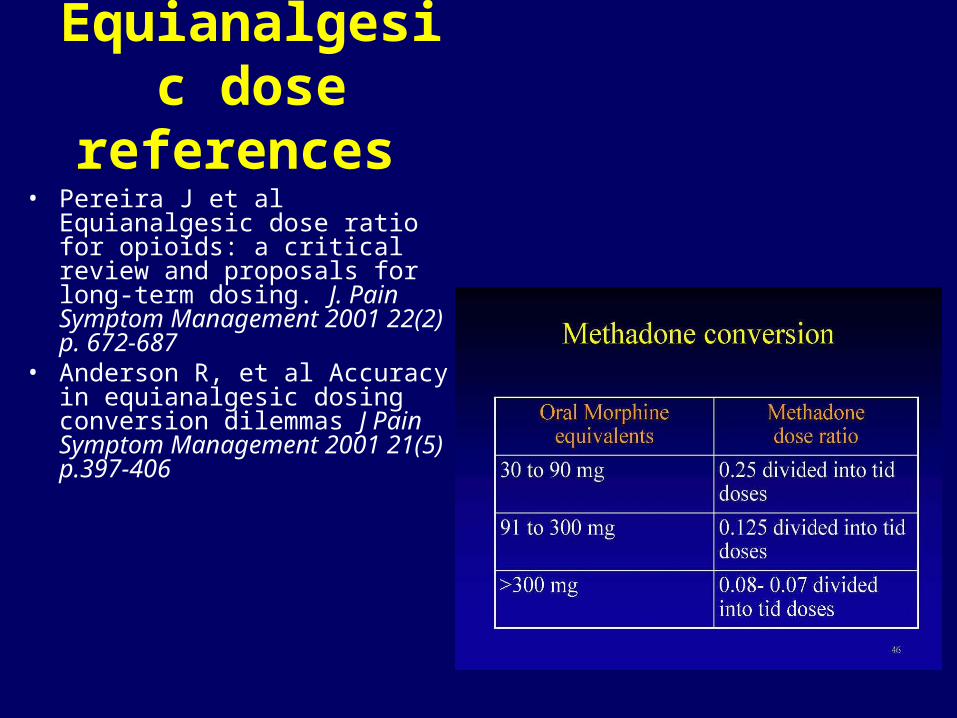
Equianalgesic dose references
• Pereira J et al Equianalgesic dose ratio for opioids: a critical review and proposals for long-term dosing. J. Pain Symptom Management 2001 22(2) p. 672-687
• Anderson R, et al Accuracy in equianalgesic dosing conversion dilemmas J Pain Symptom Management 2001 21(5) p.397-406

Phases of Treatment: • Assessments:
– Agreed treatment goals– Level of tolerance and dependence– Use/dependence on other drugs – Co-existing conditions– What social support systems
• Initial Treatment Phase– Adequacy of dosing; clinic
visits & dose changes – S&S of withdrawal– Side effects and toxicity– Drug/drug interactions
• On going Management:– Co-occurring disorders – Smoking, alcohol & other drugs – Adequate pain management – Dose and duration of treatment – Ancillary services &social support – Quality of therapeutic relationship
• Life Changes:– Experience creates memory– Memory leads to protein synthesis– Protein synthesis alters gene
expression– Gene expression creates new
behavior– New behavior leads to life changes
“You can change a man’s life by altering his genes; but you can also do that by paying off his credit card”—James Watson

Methadone Maintenance
0
2
4
6
8
MatchedCohort
Methadone VoluntaryDischarge
InvoluntaryDischarge
Untreated
0.150.85
1.65
6.91 7.20
Death Rates in Treated and Untreated Heroin Addicts
Annu
al R
ate
0
5,000
10,000
15,000
20,000
25,000
Untreated Incarceration Adolescent Adult Methadone Drug Free
Residential Outpatient
$1,575$1,750
$8,250$9,825
$20,000$21,500No Treatment
In Treatment Program
Compare the CostsCosts are for a 6 month
period, per person 47%
23%
17%
12.5%
6%0%
10%20%30%40%50%
Not in Tx
Currently in TxIn Tx 5 years
C&D
No needle
use since admission to TxA B C D
HIV Rates

Naltrexone: The Perfect Drug
• Orally Effective
• Rapid onset of action
• Long duration of action
• Safe
• Few side effects
• Blocks effects of heroin
• Non-addicting One reason not to take
• No tolerance naltrexone: can’t get high
• No dependence “It’s like taking nothing”
• No withdrawal
OOH O
N
OH

Buprenorphine: Pharmacological Characteristics
Partial Agonist (ceiling effect)
• high safety profile
• low dependence
Tight Receptor Binding• long duration of action
• slow onset mild abstinence
02468
1012141618
p 1 2 4 8 16 32
Buprenorphine (mg)
Bre
ath
s/m
inu
te
0
20
40
60
80
100
p 0.5 2 8 16 32
Buprenorphine (mg)
Peak
Sco
re
3.75 15 60
Methadone (mg)

Study # 999A: Buprenorphine’sEffect on Opiate Use
0
5
10
15
20
25
% S
s W
ith
13 C
onse
cuti
ve
Opi
ate
Fre
e U
rine
s
Buprenorphine dose (mg)
1
4
8
16
0102030405060708090
100
1 2 3 4 5 6 7 8 9 10 11 12 13 14
Day
Perc
ent
Placebo (n=60)2 mg (n=60)8 mg (n=30)
Dose change option in effect
Percent Patients on Initial Dose Johnson et al., 1998
Study 1008: Suboxone
Study #1008 Buprenorphine
4/76 15/85 22/77
Mono
% o
f G
oo
d O
utc
om
e
Number of Good Patients/TotalPBO = 5.26 Combo = 17.65 Mono = 28.57 Statistics Value ProbChi-Square 13.641 0.001Mantel-Haenszel 13.591 0.001
*
(8 Urines)
30
05
10152025
PBO
Combo*
• 16mg mono SL tablets (Subutex) and 16mg/4mg combo SL (Suboxone) are equally efficacious.
• Most reported adverse effects were those commonly seen in patients treated with opioids.

Buprenorphine and Methadone dose responsesfrom four studies using “Joint Probability”
0
10
20
30
40
50
Join
t Pro
babi
lity S
core
Week 8 Week 17
Schottenfeld, et al. 1997 -4 mg
Johnson et al. 1992 - 8 mg
Ling et al. 1996- 8 mg
Strain et al. 1994 (8 variable)
Schottenfeld et al. 1997 -12 mg
0
10
20
30
40
50
60
70
80
Week 8 Week 17
ARC 20 mg
Schottenfeld 20 mg
LA 30 mg
Strain (50 variable)
ARC 60 mg
Schottenfeld 65 mg
LA 80 mg
N remaining in treatmentX
Total N of subjects
N giving clean urinesN remaining in treatment
Joint Probability

Opiate Agonist Measures VAS Good Drug Effect (0-100)
0
25
50
0 15 30 45 60Minutes
buprenorphine (2mg)buprenorphine (2mg) and naloxone (1 mg)buprenorphine (2 mg) and naloxone (0.5 mg)buprenorphine (2 mg) and nalxone (0.25 mg)morphine (15 mg)placebo
02468
101214
0 5 1015202530354045505560
Bup
MS 4.1
8:1
2:1Plac
Adding Naloxone to Buprenorphine
Value of a Dose in Dollars
Dol
lars
Minutes
• Naloxone not absorbed sufficiently to interfere with buprenorphine when the combination is taken sublingually
• Sublingual absorption of buprenorphine @ 70%; naloxone @ 10%
• If injected, BUP/NX will precipitate withdrawal in a moderately to severely dependent addict

Suboxone vs Clonidine
0
10
20
30
40
50
60
70
80
90
100
Day 3 or 4 Day 7 or 8 Day 10 or 11 Day 13 or 14
ClonidineBup/Nx
0
5
10
15
20
25
30
35
40
45
50
Day 3 or 4 Day 7 or 8 Day 10 or 11 Day 13 or 14
ClonidineBup/Nx
Percent Present and CleanCTN 0001 (Inpatient)
Percent Present and Clean0002 (Outpatient)
NNT: Number Needed to TreatNNT for Bup/Nx 77/59 = 1.31 NNT for Clonidine 36/8 = 4.5NNT Clonidine : BupNx = 3.44
NNT:Number Needed to TreatNNT for Bup/Nx: 157/46 = 3.4 NNT for Clonidine: 74/4 = 18.5 NNT Clonidine : Bup/Nx = 5.44

In Conclusion• Opioid addiction is a serious chronic
relapsing but treatable disorder• Treatment must be sustained, detoxification
alone insufficient for long term outcome• Treatment must address both disordered
physiology and disrupted lives• There are no right or wrong medications,
only the right and wrong ways to use them.
• Medications can only change physiology, but new behavior can change lives
Thank you
Thank you Thank you





























