Embed Size (px)
Citation preview

Ophthalmic manifestationand management of CNStumors in paediatricpopulationExpert Rev. Ophthalmol. Early online, 1–13 (2014)
Evangelos Drimtzias*and Ian SimmonsDepartment of Ophthalmology, Leeds
Teaching Hospitals NHS Trust, St. James
University Hospital, Beckett Street,
Leeds, West Yorkshire, LS9 7TF, UK
*Author for correspondence:
Tel.: +44 011 3243 3144
Fax: +44 011 3216 6055
Brain tumors constitute the most frequent solid tumors in childhood. The presentation dependson age, developmental stage and tumor location. The aim of this study is to present theophthalmic manifestation of paediatric neuro-oncology disease and to discuss their screeningand management based on methods of practice developed at Leeds Teaching Hospitals NationalHealth Service (NHS) Trust using internationally developed standardized protocols. Children withbrain malignancies may present to ophthalmologists with a variety of reasons including visualsigns and symptoms, radiation and chemotherapy induced ocular complications and screeningfor oncogenic syndromes. Magnetic resonance imaging is the preferred method of imaging.However, quantitative monocular vision testing is found to be the most useful screening tool foroptic pathway gliomas. Surgery, irradiation and chemotherapy may be used in the managementof brain tumors. New treatment modalities including anti-VEGF therapy and molecular targetedtherapy are promising therapies for the treatment of optic pathway gliomas.
KEYWORDS: anti-VEGF • chemotherapy • craniopharyngiomas • magnetic resonance imaging • neurofibromatosis
• optic pathway gliomas • optical coherence tomography • paediatric brain tumors • visual acuity
Brain tumors constitute the most frequentsolid tumors in childhood, accounting for15–20% of pediatric malignant disease [1].They are the second most common pediatrictumors with an incidence of 2.8/100000/yearslightly lower compared to 3.1/100000/yeardocumented in leukemia.
Glial tumors represent over half of braintumors in children mainly involving the opticnerve and chiasm but also showing a predilec-tion for the posterior fossa and brain stem.Embryonal tumors of the CNS represent abouta quarter of pediatric brain malignancies. Otherchildhood CNS tumors that present to ophthal-mologists include craniopharyngiomas, germcell tumors arising in the suprasellar or pinealregion and parameningeal rhabdomyosarcomas(RMS). A number of tumors can arise in associ-ation with inherited syndromes such as neurofi-bromatosis (NF) type 1 and 2, tuberous sclerosisand Li–Fraumeni syndrome. A classification ofpediatric brain tumors is presented in TABLE 1.
The presentation depends on age, develop-mental stage and tumor location, and symptoms
are usually nonspecific. Infants present withincreasing head circumference, lethargy, nausea,vomiting and loss of developmental skills whileolder children tend to present more frequentlywith headache, behavioral changes, loss of cog-nitive skills, seizures and endocrine dysfunction.In addition, brain tumors frequently presentwith a constellation of typical symptoms andsigns involving the visual system. Lag times arelonger than for any other pediatric cancer, anddelay in diagnosis may result in increased long-term disability.
The aim of this study is to present theophthalmic manifestation of pediatric neuro-oncology diseases which are known to have vari-ous ophthalmic presentations including reducedvision, proptosis, nystagmus or new onset ofsquint (TABLE 2). Children may present via theoptometrist or the primary care physician withswollen optic discs found on routine examina-tion as well as due to screening for oncogenicsyndromes. The screening and management ofthese patients will be discussed based on themethods of practice developed at Leeds
informahealthcare.com 10.1586/17469899.2015.987755 � 2014 Informa UK Ltd ISSN 1746-9899 1
Review
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 82
.3.1
94.1
94 o
n 11
/27/
14Fo
r pe
rson
al u
se o
nly.

Teaching Hospitals National Health Service (NHS) Trust usinginternationally developed standardized protocols.
Ocular manifestation of pediatric CNS tumorsVision loss
Brain tumors can affect vision in three different ways. Visionloss can occur either by intrinsic optic pathway tumors or byextrinsic direct compression of the visual pathway as well asdue to papilledema and optic disc atrophy secondary to raisedintracranial pressure (RICP).
Visual loss is a commonly presenting sign in children withintrinsic optic pathway tumors. Optic pathway gliomas (OPGs)are the most common intracranial optic pathway tumors pre-senting with decreased visual acuity (VA). Although the mecha-nism is not entirely clear, vision loss from OPGs is typicallycaused by damage to the axons of the visual pathway, directnerve fiber compression and demyelination [2]. Overall 25% ofOPGs are confined to the optic nerve, while 40–75% involvethe chiasm [3].
OPGs show a highly variable growth pattern ranging fromindolent to rapidly progressive causing severe visual loss. Mostchildren with NF 1-OPG have an indolent or even asymptomaticcourse and therefore benefit from screening and early detection.50–75% of patients are asymptomatic at the time of diagnosis. In
contrast, sporadic OPGs nearly always present with diminishedvision ranging from mild visual loss to complete blindness.
The natural history of vision loss in children with OPG isdynamic and can occur at any age and can be separated bymany months or years and can vary in severity. This unpredict-ability of the disease course reflects the poor understanding ofOPG clinical behavior. However, some authors advocate thatdiagnosis of late-onset OPGs may be previously undiagnosedtumors and the late onset of symptoms may be indicative offurther disease progression [4].
Balcer et al. suggested that VA loss might be dependent onthe tumor extent and location by MRI at the time of diagno-sis [5]. In their study, a significantly higher proportion of chil-dren with involvement of the postchiasmal visual pathwaydeveloped visual loss (62%) compared with those with chiasmaland or optic nerve involvement alone (32%). Similarly, previ-ous studies demonstrated worse prognosis for binocular acuityin tumors with chiasmal involvement, indicating that isolatedoptic nerve gliomas have a better clinical course [6].
Craniopharyngiomas may present with visual failure as aresult of compression of the visual pathway, particularly thechiasm. However, the extent of visual loss is often not appreci-ated until other abnormalities become apparent. This tumor‘sclose relationship to the anterior visual pathway gives rise to a
Table 1. Anatomical classification of pediatric brain tumors.
Posterior fossa Supratentorial
Intraparenchymal Extra-axial Sellar/suprasellar
Astrocytoma Astrocytoma Choroid plexus papilloma/carcinoma Craniopharyngioma
Medulloblastoma Ependymoma Langerhans cell histiocytosis Astrocytoma
Ependymoma Desmoplastic neuroepithelial tumor Metastasis Hypothalamic hamartoma
Brainstem glioma Dysembryoplastic neuroepithelial tumor Germ cell tumors
Ganglioglioma/Gangliocytoma Pituitary adenoma
Teratoma Langerhans cell histiocytosis
Embryonal tumors
Atypical teratoid/rhabdoid tumors
Table 2. List of reasons that children with brain malignancies present to ophthalmologist.
Ocular symptoms Ocular signs Screeningfor NF 1
Complications ofchemotherapy
Complications ofradiotherapy
Vision loss Papilledema/optic
disc atrophy
Anterior segment (corneal toxicity) Anterior segment (cataract,
dry eye, facial hypoplasia)
Visual field
impairment
Nystagmus Posterior segment (optic neuropathy,
retinopathy, maculopathy)
Posterior segment (optic
neuropathy, retinopathy)
Ocular motility
disorders
Neuro-ophthalmic (cortical blindness,
cranial nerve palsies,
accommodation palsy)
Proptosis
NF: Neurofibromatosis.
Review Drimtzias & Simmons
doi: 10.1586/17469899.2015.987755 Expert Rev. Ophthalmol.
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 82
.3.1
94.1
94 o
n 11
/27/
14Fo
r pe
rson
al u
se o
nly.

variety of visual signs. Patients generally present late, and thevisual symptoms are often preceded by a long history ofsystemic symptoms.
According to previous reports, VA loss is the most commonocular complaint and constitutes the circumstance of diagnosisin 30–50% of patients with craniopharyngiomas [7]. In chil-dren, ophthalmological signs are not the main circumstances ofdiagnosis because young patients do not complain of a mild orunilateral reduction in VA or visual field (VF) loss.
Age less than 6 years is an unfavorable predictor of the visualoutcome as many of children of this age group have poorvision at the time of diagnosis [8]. This may be attributed tolate diagnosis diminishing the chance of visual recovery. Inaddition, visual symptoms, optic disc atrophy and calcificationat presentation of craniopharyngioma were associated with asignificant poorer visual outcome [9].
VF impairment
Craniopharyngiomas and pituitary tumors tend to compressthe chiasm from behind and above as they grow on the infun-dibulum between the brain and the pituitary gland. This post-erosuperior compression of the chiasm produces variablebitemporal hemianopia. Several authors have documentedbitemporal hemianopia as the most common initial VF defectin children with craniopharyngioma [10].
In these cases, the extensive loss of the temporal VF disruptsfusion, and children can then suffer VF-related diplopia. Thesepatients can also describe a hemiretinal slide because the VF ofboth eyes are segregated from one another and cannot be syn-chronized by the normal fusion. This creates significant readingproblems with either deletion or duplication of portion of thetarget in children with convergent and divergent squint,respectively.
In addition, patients with bitemporal hemianopia may pres-ent with post-fixational blindness defined by a blind area distalto the fixation point. These patients while fixing bifoveally can-not respond to targets beyond the fixation target which causeslack of perception of the object.
VF in children with craniopharyngiomas is sometimes atypi-cal due to the infiltrating nature of the tumor. Variable tempo-ral changes in VF defects have been reported as a characteristicfeature of the tumor resulting from intermittent emptying ofcyst fluid into the ventricular system [7].
Germ cell tumors arising in the suprasellar region often pres-ent with VF defects. Bitemporal hemianopia is a sequel to thesetumors as they expand dorsally and compress or invade theoptic chiasm.
Progressive VF loss, including central depression and bitem-poral hemianopia, is reported in 70% of patients withOPGs [11]. With extrinsic compression of the optic nerve, theVF typically shows a central scotoma with ‘breaking through’as the defect increases. This leaves a peripheral crescent of pre-served vision. However, in young children, VF defects may notbe readily apparent and are only infrequently a presentingsymptom without associated VA loss.
Screening of children with NF 1
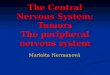
Children might present to ophthalmologists to have visualscreening and surveillance of NF 1. Approximately 15% ofpatients with NF 1 have low-grade pilocytic astrocytomas ofthe optic pathway [5,6,12]. In NF 1 children, the most commonpresenting signs are proptosis and VA loss (FIGURE 1) [6].
One-third to one-half of children with NF 1-OPG mayexperience vision loss, and in those cases in which tumor isconfined to the optic nerve, proptosis is a frequent clinical pre-sentation [13]. Interestingly, absence of the greater wing of thesphenoid bone in NF 1 may lead to pulsatile proptosis. Greaterthan one-third of NF 1 subjects may also develop opticdisc atrophy.
The likelihood of vision loss in children with NF 1-associ-ated OPGs is dependent on the tumor extent and location [5].Although NF 1-OPGs typically involve the anterior visualpathway (optic nerves, chiasm and tracts), significant optic radi-ation involvement posterior to the lateral geniculate ganglionhas also been reported [14]. Bilateral optic nerve gliomas with-out chiasmal involvement are virtually diagnostic of NF 1.
The natural history of NF 1-associated OPGs is unpredict-able. Most OPGs in children with NF 1 are diagnosed beforeage 6 years after which the appearance of symptomatic OPGsand progression of known OPGs requiring therapy is uncom-mon [12,15]. However, a number of reports have demonstratednewly symptomatic NF 1-OPGs even after previously normalneuroimaging in children older than 8 years [12].
Compared with sporadic OPGs, NF 1-related gliomas areless likely to have visual impairment at diagnosis and are morelikely to remain stable over time [16]. Most patients with NF1 had stable or even normal VA, but some experienced slowprogressive visual loss and a few developed sudden and pro-found vision loss according to previous study [17]. A high pro-portion of NF 1 patients (28%) in Balcer et al. seriesdeveloped visual loss between 1 and 6 years after the diagnosisof OPG [5].
While most NF 1-OPGs are diagnosed before 6 years ofage, the typical age of presentation for sporadic OPGs is lessthan 8 years [18]. However, onset can occur in the seconddecade. Nearly 90% of children with sporadic OPGs presentwith neurologic or ophthalmic pathology requiring neuroimag-ing. In addition, diagnosis may be assisted by accompanyingendocrinopathy or short stature.
Impaired VA is more common at presentation in sporadicOPGs. Children without NF 1 are more likely to present withnystagmus and hydrocephalus. Sporadic OPGs are frequentlyassociated with RICP and neurological findings as they mainlyaffect the posterior optic pathway including the chiasm andhypothalamus. In cases of chiasmal or hypothalamic invasion,precocious puberty is the presenting manifestation found in40% of children [19].
Papilledema/optic disc atrophy
Papilledema is the crucial clinical sign of RICP resulting fromaxoplasmic flow stasis with intra-axonal edema in the area of
Ophthalmic manifestation & management of CNS tumors in paediatric population Review
informahealthcare.com doi: 10.1586/17469899.2015.987755
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 82
.3.1
94.1
94 o
n 11
/27/
14Fo
r pe
rson
al u
se o
nly.

the optic disc. Most symptoms are secondary to the underlyingelevation in intracranial pressure including headaches, nauseaand vomiting, whereas, occasionally, cases can be found onroutine examinations in asymptomatic individuals.
Vision is usually well preserved with acute papilledema.With prolonged RICP, the disc becomes paler secondary to adecrease in number of physiologically active nerve fibers. Thiseventually leads to consecutive optic disc atrophy which is oftenassociated with VA or VF loss, although this might be mild.
Children with intracranial OPGs can present with obstruc-tive hydrocephalus with subsequent obstruction of the ventricu-lar system and RICP [13,20]. Signs and symptoms of RICP,including headache and papilledema, are more often noted inlarger chiasmal-hypothalamic sporadic OPGs [18].
Optic atrophy occurs in up to 60% of children with cranio-pharyngioma and is commoner than disc swelling [21]. How-ever, papilledema is more common in children compared toadults [21]. Longstanding chiasmal compression produces bitem-poral hemianopia with loss of half of the maculopapillary bun-dle on the temporal side and the hemiretinal fibers into thenasal side of the optic disc taking the form of ‘bow-tie’ atro-phy. With RICP, papilledema occurs only in the remainingtemporal retinal nerve fibers streaming into the top and bottomof the disc. This type of swelling was named ‘twin-peaks’papilledema.
Over 80% of children with pineal and brain stem tumors have,at presentation, features of RICP and subsequent papilledemadue to blockage of the Sylvian aqueduct. Similar presentation canbe found in tumors of the cerebellopontine angle and midlinemalignancies including medulloblastomas, as well as in tumorsarising in the lateral, third and fourth ventricles, with ependymo-mas being the most frequently involved neoplasm (FIGURE 2).
Nystagmus
Nystagmus from an OPG can be horizontal, rotary, asymmetricor monocular. Gliomas affecting the chiasm and the nerves asym-metrically may cause a dissociated, high-frequency, low-ampli-tude, horizontal, asymmetric and pendular nystagmus mimickingspasmus nutans. Other features of spasmus nutans, includinghead nodding and torticollis, may or may not be present.
In young subjects, asymmetric nystagmus particularly in thepresence of optic atrophy or hydrocephalus is suggestive of chias-mal glioma with or without posterior extension into the optictracts. In infancy, a common presentation of OPGs is often withvertical or asymmetric rotary nystagmus, an association known asRussel diencephalic syndrome frequently associated withincreased appetite and hypermetabolism. Binning et al. advocatedthat nystagmus is more commonly present in patients withoutNF 1 [3].
Seesaw nystagmus described by intorsion and elevation ofone eye and simultaneous extorsion and depression of the fel-low eye is a rare sign seen with large suprasellar tumors involv-ing the chiasm and extending into the third ventricle as well aswith focal lesions confined to the rostral mesencephalon.
Convergence-retraction nystagmus is a disorder in whichattempted elevation produces a series of rapid jerky convergentmovements with associated retraction of the globes. This syn-chronous retraction and convergence of the eyes is seen almostexclusively in the setting of dorsal midbrain syndrome.
Dorsal midbrain syndrome in infancy suggests the diagnosisof congenital hydrocephalus producing the characteristic‘setting sun’ sign characterized by upgaze paresis and downwarddrifting of the eyes. Its recurrence in children who have had aventriculoperitoneal (VP) shunt placed for hydrocephalus usu-ally signifies shunt failure. In contrast, the onset of dorsal mid-brain syndrome in an older child usually indicates the presenceof pineal tumor.
Upbeating nystagmus, in which the fast phase is in theupward direction, is a common sign seen with pontine syn-dromes. It is usually mild in the primary position and increasesin the upgaze. Upbeating nystagmus in infancy is frequentlyassociated with congenital abnormalities of the afferent visualsystem, while in older children it is caused by structural lesionsinvolving the brainstem or cerebellum.
In contrast, downbeating nystagmus, in which the fast phaseis downward, is a characteristic feature of medullary diseaseand lesions of the craniocervical junction, with medulloblasto-mas being the most commonly involved neoplasms. Down-nbeating nystagmus is diagnostic and helps to localize the siteof pathology to the area of craniocervical junction and is acommon finding in children with Chiari Type 1 malformation.
The presence of opsoclonus characterized by involuntary,chaotic, multidirectional saccades, also known as ‘dancing eyessyndrome’, usually suggests occult localized neuroblastoma.These movements can persist during sleep. An autoimmunemechanism has been proposed in the pathogenesis of opsoclo-nus. Autoantibodies directed against neurofilaments, surfaceand intracellular antigens of neuroblastoma cell lines as well as
Figure 1. Neuroimaging in a 2-year-old female withneurofibromatosis type 1 presented with left proptosisand anisohypermetropia revealed low-grade pilocyticastrocytoma of the left optic nerve with chiasmal invasion.
Review Drimtzias & Simmons
doi: 10.1586/17469899.2015.987755 Expert Rev. Ophthalmol.
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 82
.3.1
94.1
94 o
n 11
/27/
14Fo
r pe
rson
al u
se o
nly.

secondary lymphoid follicles observed in neuroblastomas havesupported its autoimmune origin [22]. Neuroblastoma constitutesthe major diagnostic consideration for opsoclonus in the first sev-eral years of life and is found in approximately half of cases withopsoclonus in this age range [23]. However, the primary tumor inthese cases is in the chest or abdomen and not in the brain.
Posterior fossa malformations can give rise to periodic alter-nating nystagmus (PAN) characterized by periodic changes innystagmus direction and in head posture. This occurs becauseof an actively shifting null zone always seen in PAN, which isdefined as the position of gaze where the nystagmus is less andtherefore vision is better. Although in childhood PAN is fre-quently associated with albinism, a high incidence was foundwith structural lesions involving the cerebellum as well as withArnold–Chiari malformation.
Cerebellar and brain stem disease almost always present withnystagmus. The commonest presentation is with horizontal jerknystagmus arising from lesions of the vestibullocerebellar path-ways or vestibular nuclei. The nystagmus may be spontaneousin the primary position but is more often seen with greateramplitude on gaze to the side of lesion.
Nystagmus is present in over 60–90% of cerebellopontineangle tumors, with acoustic schwannomas and pontine gliomasbeing the most common types presenting in this area. Thegaze-evoked nystagmus to the side opposite to the lesion is fineand rapid, whereas to the side of the lesion the nystagmus is oflow frequency and large amplitude.
Ocular motility disorders
Brain tumors can present with a variety of ocular motility defi-cits as a result of involvement of the cranial nerves. Singleinfranuclear cranial nerve palsies, especially sixth or fourthnerve palsy, may be a false localizing sign of RICP.
The acute-onset incomittant esotropia is often the initial andonly sign of intracranial pathology in the young population. Itoccurs in the context of RICP caused by stretching of the nervein its long intracranial course, or compression against thepetrous ligament or the ridge of the petrous temporal bone.
The abducens nerve leaves the brain stem at the ponto-medullary junction and may therefore be damaged by tumorsof the pons and medulla. Thus, the acute-onset esotropia in anolder child needs to be investigated. Similarly, such tumors cancause horizontal gaze palsies, while skew deviation is wellrecorded, with both pontine and medullary malignancies invad-ing the median longitudinal fasciculus (FIGURE 3).
Upgaze palsy is a common feature of early dorsal midbrainsyndrome, while a similar presentation can be found in tumorsof the third ventricle with ependymomas being the most com-mon type and in germ cell tumors arising in the pineal region.In addition, dorsal midbrain syndrome is frequently associatedwith bilateral fourth nerve palsies.
Cranial nerve palsies are less common presenting signs inOPGs. However, fascicular lesions of the oculomotor nerve arefrequently diagnosed in children with mesencephalic gliomas [24].
Advanced parameningeal rhabdomyosarcoma with skull baseinvasion may present with ophthalmic signs. Cranial neuropa-thies constitute the most common presentation resulting frominfiltration or compression of affected cranial nerves. The abdu-cens nerve is the most vulnerable. However, further invasion ofthe skull base or cavernous sinus may cause additional third,fourth and fifth nerve palsies [25].
Proptosis
OPGs involving the intraorbital portion of the nerve may presentwith axial proptosis. The enlarged intraorbital portion of thetumor has a predisposition to kink and reflect downward, causingthe posterior aspect of a slightly proptotic globe to rotate upwards.Proptosis was found to be a common accompanying sign in NF
Figure 2. Radiographic imaging showed medulloblastomawith associated hydrocephalus in a child presented withpapilledema.
Figure 3. A 6-year-old child presented with acute-onset leftesotropia, headaches and abduction deficit. Magneticresonance imaging revealed pontine glioma.
Ophthalmic manifestation & management of CNS tumors in paediatric population Review
informahealthcare.com doi: 10.1586/17469899.2015.987755
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 82
.3.1
94.1
94 o
n 11
/27/
14Fo
r pe
rson
al u
se o
nly.

1 patients [6]. Similar findings were reported by Grill et al. as intheir series proptosis was significantly more frequent in patientswith NF 1 (21.5%) than in those without (5.5%) [26].
Orbital metastasis of neuroblastomas commonly present withsudden onset and rapid progression of proptosis. Interestingly,periorbital ecchymoses may frequently be the only presentingsign of neuroblastomas and is seen in 25% of the cases.
Patients with orbital RMS generally present with proptosisand globe displacement in 80%. Proptosis can develop morerapidly in newborns and infants, whereas in older children ittends to have a slower course.
Complications of chemotherapy
Systemic drug-induced ocular side effects are increasing becauseof the number of new chemotherapeutic agents being intro-duced. Although the eye is usually considered a protected site,the visual system has a potentially high degree of sensitivity totoxic substances. The increased use of new drugs has resultedin longer patient survival. Consequently, the ophthalmologist isseeing more patients with adverse ocular side effects secondaryto these antineoplastic agents.
Ocular toxicity includes a broad spectrum of disorders which canbe grouped into adnexal, anterior/posterior segment and neuro-ophthalmic [27]. Dose reduction or discontinuation of incriminateddrugs may help in reducing severity and duration of side effects.
Posterior segment involvement including optic neuropathy,retinopathy and maculopathy is commonly seen with adminis-tration of chemotherapeutic agents used for the treatment ofCNS tumors such as cisplatin, vincristine, etoposide and carbo-platine. Visual loss has been reported with the use of cisplatinand may be bilateral and irreversible [28]. In addition, corticalblindness in association with cisplatin may occur.
Anterior segment side effects have been reported less fre-quently, with corneal toxicity being the most common adverseevent. Cranial nerve palsies can occur occasionally with the useof vinblastine and vincristine. In addition, children receivingvinca alkaloids commonly present with neurotoxicities, includ-ing encephalopathies and eyelid ptosis. Interestingly, fibrosisand thickening of the extraocular muscles has been recordedwith local injection of carboplatin and cisplatin [29].
Reversible accommodation palsy is common in children withstage 4 advanced neuroblastoma following intravenous infusionwith anti-disialoganglioside antibodies [30]. Short-term optical treat-ment with +3.0 dioptres sphere convex lenses can be usedconcurrently during the course of immunotherapy providingsymptomatic relief.
Complications of radiotherapy
Delayed radiation-induced damage to components of the visualsystem results in morbidities varying in severity and latency.Anterior segment involvement is more frequently observed withexternal beam radiotherapy, while plaque-brachytherapy mainlyhas its effect on the posterior segment.
Radiation-induced cataracts are usually posterior sub-capsularopacities. The severity of cataract formation is related to total
dose and fractionation, and the onset is usually within 2 to3 years [31]. A threshold for detectable opacity has been suggestedto be 2 Gy on a single exposure, although other studies have dem-onstrated the cataract formation to occur at doses 8–10 Gy [32].
Dry eye is commonly reported as a frequent radiation-induced complication resulting from the effects of radiation tothe conjunctival epithelium, goblet cells, cornea and lacrimalglands. For doses over 45 Gy, symptoms developed within1 month after radiation, whereas the mean time to manifesta-tion of corneal damage was reported to be 9 months [33]. Dryeye is a common complication following radiation therapy forRMS. Children often need long-term conservative treatmentwith ocular lubrication, whereas resistant cases may be managedby punctal occlusion.
Radiation-induced retinopathy usually presents with the non-proliferative form at an early stage, progressing rapidly to theproliferative type due to capillary closure, retinal ischemia andneovascularization. The upper limit of a safe dose was sug-gested to be 35 Gy in one early study, but cases of retinopathyhave been reported with doses as low as 20 Gy [34].
The incidence of radiation-induced optic neuropathyincreases with an increase in the total dose to the optic nerveover 55 Gy, although optic chiasmal damage at 50 Gy hasbeen observed [35]. However, the effect of radiation on theoptic nerve is not yet fully understood.
Monitoring of pediatric CNS tumorsMRI scanning
MRI is the preferred method of imaging for CNS tumors.However, in OPGs, although standard MRI assessment canidentify and delineate the extent of the tumor, it cannot beused to predict the likelihood of tumor progression or changein visual function [15,36].
Historically, in OPGs, the decision to initiate treatment isbased on the clinical or radiographic progression of the tumor [37].However, there continues to be little agreement about the indica-tion for initiating treatment of an OPG beyond decline in VA.Although neuroimaging progression is cited frequently, there stillare many who believe that this should not drive treatment in theabsence of changes in vision [38].
Neuroimaging in OPGs is usually reserved for those withsymptoms or abnormal findings on examination and should beconsidered in cases when accurate and reliable VA testing is notpossible. In addition, symptomatic OPGs can develop in a nervethat appears normal in the first year of life; thus, normal neuro-imaging findings in an infant or young child would not provideassurance that the optic nerve will remain tumor free [39].
VA testing
Due to the poor correlation between VA and radiographic out-comes found in previous studies, routine radiographic imagingof asymptomatic NF 1 patients should not be used as a screen-ing tool for the disease [40–42]. Visual deterioration can precedethe appearance of OPG on imaging studies, and OPGs canmanifest radiologic progression without visual symptoms or
Review Drimtzias & Simmons
doi: 10.1586/17469899.2015.987755 Expert Rev. Ophthalmol.
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 82
.3.1
94.1
94 o
n 11
/27/
14Fo
r pe
rson
al u
se o
nly.

signs [15,39,42]. The first occurs because pilocytic astrocytomascan invade optic nerve fascicles, thereby compromising bloodsupply or interfering with neuronal–glial interactions, thuscausing loss of visual function despite stable tumor volume onradiographic imaging. The second mainly occurs in cases wheretumor growth is confined to adjacent neural structures but notdirectly compromising the visual pathway axons.
Since the majority of asymptomatic children with inciden-tally diagnosed OPG do not progress to require treatment andtherefore do not gain from a screening MRI, the neuro-ophthalmic examination is a key component in the diagnosisand management of OPGs.
A quantitative assessment of VA is the most important factorguiding the decision to initiate or change treatment [43,44]. Qualita-tive measures of VA are insufficient because subtle and even largechanges in VA may not be adequately detected be these methods.
VA is a psychophysical measure since it relies on patient’scooperation and attention. This is especially true for childrenwith NF 1 where learning difficulties and executive functiondeficits can compromise accurate and reliable testing of VA. Toaccount for differences in scoring and quantifying the magni-tude of VA changes, standardized methods are being used [45].
Different VA testing methods are used depending on thechild’s age. For infants and very young preverbal children,Teller acuity cards (TAC) are used for providing reliable meas-urements. VA is assessed by the preferential looking test whichis considered a grating acuity testing method. In older childrenwho have learned all of the letters of the alphabet, VA can bemeasured by having the child verbalize or point to the match-ing HOTV letter or Lea symbol. These computer-basedHOTV testing methods are considered recognition acuitytests [43].
Both grating and recognition acuity values can be convertedinto Snellen equivalents providing reproducible VA values. Inyounger children, scoring one line better or worse on repeattesting is not uncommon since testing methods require cooper-ation and attention.
In an effort to standardize VA results, the logarithm of mini-mal angle of resolution (logMAR) can be used where acuitycharts have each line separated by 0.1 logMAR units [46]. Thismethod facilitates better description of VA changes and produ-ces continued VA values providing an international unit idealfor data analysis in longitudinal clinical trials. Since several fac-tors can influence VA results, a ‘two line’ decline in VA is rec-ommended as progression sufficient to initiate treatment [15,47].
VF testing
VF testing in very young children can be difficult, and the clin-ical significance of small field changes is often unclear. How-ever, previous reports have documented the reliability of VFexamination in children as young as the age of 4, whereasSafran et al. showed that automated VF examination is feasiblein children between 5 and 8 years of age [48].
Nevertheless, testing by confrontation should be attemptedat all visits when more objective testing is not possible due to
patient’s age. In older children, better VF assessment is pro-vided by Goldmann perimeter assessing the extent of visionalong both horizontal and vertical axes measured in degrees.
Color vision & contrast sensitivity testing
There is no evidence in literature that color vision and contrast sen-sitivity testing add value to screening for pediatric CNS tumors.
Relative afferent papillary defect
An afferent papillary defect always accompanies optic nervechanges. Relative afferent papillary defect (RAPD) representssignificant optic nerve damage and is therefore vital for the cli-nician to look for papillary reactivity if the diagnosis of opticnerve compression is to be made.
Visual evoked potentials
Attempts have been made to detect vision loss or correlate VAwith visual evoked potentials (VEP) in children withOPGs [11,49,50]. VA represents the central 2˚ of the VF, whilethe VEP is generated by cortical neurons representing the mac-ula and the surrounding central 20˚ of the VF [15].
Several groups have evaluated VEP in the detection ofOPGs and showed a sensitivity between 67 and 93% andspecificity between 60 and 87% [49,51]. Similarly, Kelly et al.found a higher sensitivity and specificity of VEP comparedwith VA for detection or radiological tumor progression [42].In their study, sensitivity and specificity of between-visit var-iations in VA and VEP were evaluated and correlated withchanges in tumor volume and VEPs found to show a highercorrespondence with MRI findings (68–86%) than VA simi-lar to previous report [40]. However, in previous study con-ducted by the same authors, VEP was found to be superiorto VA only at presentation and detection of early optic nervedamage [47].
Previous studies advocated that severe pre-existing damage inthe visual system limits detection of OPG progression usingVEP testing and thus do not support its use as a screeningtool [49,50]. It is not certain how much of a change of VEPdefines worsening when patients are followed longitudinallyand the ability to detect progressive visual loss in a child withseverely reduced VEP is limited [15,52].
Additional limitation in the use of VEPs for screening andsurveillance of OPGs is the difficulty in interpreting smallchanges in amplitude without changes in VA while it is knownthat the accuracy of VEP testing and interpretation relies onexperienced electrophysiologists who are not widely available.Therefore, a number of experts recommend against the use ofVEPs for monitoring of OPG s in the long term [15,52].
In addition, no role of VEPs for screening of craniopharyng-iomas has been demonstrated in literature.
Optical coherence tomography
Many young children with OPGs have difficulties completingquantitative VA and VF testing, whereas others may not com-plain of vision loss. To better guide therapy, a reliable
Ophthalmic manifestation & management of CNS tumors in paediatric population Review
informahealthcare.com doi: 10.1586/17469899.2015.987755
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 82
.3.1
94.1
94 o
n 11
/27/
14Fo
r pe
rson
al u
se o
nly.

quantitative biomarker of vision that does not rely on patient‘scooperation is needed in young children with OPGs [38].
A recent study demonstrated a strong relationship betweenvisual function and retinal nerve fiber thickness (RNFL) mea-sured by optical coherence tomography (OCT) in children of6 years or older with sporadic or NF 1-associated OPG [53].RNFL was found to be decreased in the majority of children.Similarly, Chang et al. found that older subjects with OPGhad a thinner RNFL compared with control individuals usingthe Stratus time-domain OCT [54].
Although the use of Stratus OCT is also limited by subject‘scooperation, it is to a lesser extent than VF testing requiringonly seconds of cooperation. Despite variability in cooperationamong children younger than 6, reliable OCT imaging has beenobtained in children as young as 3 years of age [55]. However, itis likely that very young patients who cannot cooperate with VAtesting are unable to cooperate with conventional OCT devices.
Recently, a number of investigators have used a spectral-domain handheld (HH) OCT device to image the optic nerveof infants and young children with a variety of conditions [56].Avery et al. used the spectral-domain HH-OCT during seda-tion in young subjects with OPG and extended the findings ofprevious studies where testing was performed with the time-domain OCT [57]. The authors demonstrated that the spectral-domain is a much higher resolution device compared with thetime-domain OCT.
OCT may aid in early detection of OPGs, thus allowing fortimely initiation of chemotherapy and arrest of visual deteriora-tion. This is critical because lost vision has not widely beendocumented to recover with current treatment. OCT could beused as a noninvasive and inexpensive screening tool for OPGsreducing the need and frequency of MRIs, visit duration andtotal cost. In addition, repeated HH-OCT imaging sessions aresafe and fall well within standard recommendations.
Management of pediatric CNS tumorsSurgery
The role of surgery in the treatment of OPGs is controversialbecause of the risk of further visual compromise due to theintrinsic to the optic pathway nature of the tumor. However,surgery is the primary therapy for pediatric low-grade astrocyto-mas in other brain locations [58].
Ahn et al. found that radical removal of OPGs was of nosurvival benefit, although a benefit was documented in control-ling hydrocephalus and postponing radiation therapy in youn-ger children [59]. Surgery is typically not warranted inNF 1 subjects as they tend to have more diffuse disease andsurgical intervention tends to fail at a rate almost twice than oftheir counterparts without NF 1 [13].
The optimal therapeutic approach of craniopharyngiomas con-tinues to polarize options. Given the increased morbidity andinability to depend on radiotherapy in the very young population,several authors agree with radical resection of tumor by anexperienced surgeon as the optimal management of this agegroup [60].
Previous reports demonstrated less postoperative VA deficitsfollowing transcranial surgery compared to the transsphenoidalgroup, whereas others advocated better visual outcomes withthe endoscopic endonasal approach [61,62]. Radical resection ofcraniopharyngiomas was associated with decreased recurrencerate in children aged less than 6 [60]. However, surgery for cra-niopharyngioma is related with hypothalamic obesity withincreased risk of weight gain and polyphagia.
Radiation therapy
Despite documented tumor stability and prevention of recur-rence following irradiation, this treatment can yield a myriadof adverse side effects [63]. Radiation detrimental effects werefound to be more pronounced in children younger than 5 andinclude further visual decline, hormone deficits, cerebrovasculardisease, neurocognitive deficits, progressive decline of IQ andsecondary malignant neoplasms [64]. The latter is especially truefor NF 1 subjects. In contrast, sporadic OPGs have a secondtumor occurrence rate of zero after radiation [4].
Radiotherapy is therefore reserved for children older than5 to 7 years of age or even for younger individuals who haveexhausted chemotherapy options, while it should be avoided inthe treatment of oncogenic conditions [15].
Chemotherapy
Given the risks of surgery and radiotherapy, chemotherapy isthe initial treatment for most OPGs (FIGURE 4). The combinationof carboplatin and vincristine is the most common regime witha 3-year progression-free survival of 77% and a 5-yearprogression-free survival of 69% in NF 1 children [65]. Temo-zolamide and vinblastine are both effective as single agents forrecurrent or refractory low-grade OPGs [66].
Although several studies suggested that vision loss prior toOPG treatment is irreversible, Fisher et al. reported VAimprovement or stabilization in most subjects of their studyfollowing chemotherapy [67]. Moreno et al. reported that 50%of children had stable VA and 14% showed improvement afterchemotherapy [68]. Overall, it has been shown that some visualimprovement may occur only when treatment starts relativelyearly during the natural course of OPGs. Unfortunately, if VAis not regained after treatment, the VA loss is permanent.
However, it has been reported in the literature that somepatients with NF 1-OPG and VA loss improve spontaneously,and this has been suggested as a reason to hesitate initiatingchemotherapy in patients with vision loss. Despite several dem-onstrated poor prognostic factors including age less than 2 ormore than 5 years and optic disc pallor at the time of treat-ment, there were children who regained vision with chemother-apy [67]. However, although chemotherapy is found to stabilizeor reduce tumor, up to 60% of children demonstrate tumorprogression after 5 years [69].
Anti-VEGF
Previous findings indicate that continues glioma growthdepends mostly on its angiogenic potency [70]. Bartels et al.
Review Drimtzias & Simmons
doi: 10.1586/17469899.2015.987755 Expert Rev. Ophthalmol.
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 82
.3.1
94.1
94 o
n 11
/27/
14Fo
r pe
rson
al u
se o
nly.

investigated the prognostic significance ofangiogenic features in OPGs and foundthat angiogenesis and microvessel densitywas a predictor of tumor progression [71].
It has been demonstrated that tumorcells recognize oxygen deficits via recep-tors and respond with a release of VEGFthat induces neovascularization to allowfurther tumor growth [72]. Thus, drugstargeting tumor angiogenesis have beenintroduced and are being evaluated forthe treatment of recurrent and refractoryOPGs. Treatment was thought to bereasonable as VEGF receptor is found tobe overexpressed in pediatric OPGs [71].Vinblastine as an anti-angiogenic agenthas been widely used in children withOPGs [66]. In addition, several studieshave demonstrated objective responseand long-term efficacy of bevacizumab-based therapy in children with recurrent low-grade glio-mas [73,74]. Objective response rates were observed to be ashigh as 86% [73].
Combination therapy with irinotecan was found to bemore effective than the drugs utilized individually [75]. Thisapparent synergy was attributed to the assumption that beva-cizumab suppresses the pro-angiogenic effect of glioma stemcells allowing for irinotecan to target the more differentiatedtumor cells.
In pediatrics, there is limited experience with bevacizumab asa single agent. The issues of potential thromboembolic disease,impaired renal failure, intracranial hemorhages or hypertensivecrisis are problematic. However, in previous studies, toxicitywas not significant and in most cases was irreversible [73]. Over-all, bevacizumab-based therapy in OPGs may greatly improvevisual outcomes and should be considered in appropriate clini-cal situations. However, further study regarding optimal dosingand long-term toxicity is warranted.
Cyclic AMP targeted therapy
In addition to anti-angiogenic therapy, further investigation ofthe biological mechanisms involved in the pathogenesis ofOPGs is ongoing. Warrington et al. found that cyclic AMPsuppression via expression of phosphodiesterase 4A1 (PDE4A1)is sufficient to induce gliomagenesis in a mouse model ofNF 1 [76].
Since OPGs seem to grow where there are low levels ofcyclic AMP, the authors hypothesized that pharmacologic eleva-tion of cyclic AMP and targeted inhibition of PDE4A1 maydramatically inhibit optic glioma growth and attenuate tumorsize, thus justifying the implementation of cyclic AMP-targetedtherapies for OPG.
Interestingly, cyclic AMP levels were found to rise with age,and this may be likely responsible for the decreased incidenceof OPG in the older population.
New molecular targeted therapy
The outstanding progress in advanced molecular technologieshas allowed a better understanding of the molecular patho-genesis of pediatric brain tumors. This knowledge has alteredthe way that pediatric CNS tumors are being categorized,allowing stratification of patients into appropriate risk groupsby identifying prognostic markers. In addition, furtherinsights into tumorigenesis have opened new avenues for tar-geted therapies.
Pfister et al. uncovered mechanisms of mitogen-activatedprotein kinase activation in pilocytic astrocytomas. In addi-tion, they identified a tandem duplication of the BRAF genelocus (7q34) in more than 50% of these tumors [77]. Thus, anumber of Phase I and Phase II clinical trials are ongoingusing these targets for novel therapeutic approaches. Targetedtherapies testing small-molecule inhibitors of mitogen-activatedprotein kinase are currently being used for the treatment ofOPGs [78].
Recent studies have provided further insights into the dysre-gulated signaling pathways in diffuse intrinsic pontine gli-oma [79]. Overexpression of EGFR and platelet-derived growthfactor receptor a (PDGFRa) have been reported, and clinicaltrials with the respective inhibitors are in progress.
When compared to standard chemotherapy and radiation,the use of biological agents has several advantages. They cantarget cancer cells and spare normal cells in the developingCNS of children and can be used to delay irradiation avoidingits detrimental effects. In addition, their low molecular weightsallow for better blood–brain barrier penetration. However, theirefficacy has not yet been proven.
Surveillance of pediatric CNS tumorsMRI scanning remains the gold-standard diagnostic test andrecommended means of follow-up in children with braintumors. However, due to the poor correlation between VA and
A B
Figure 4. Optic pathway glioma. (A) Pre-treatment and (B) post-treatmentshowing significant shrinkage of the tumor on neuroimaging followingchemotherapy with combination regime.
Ophthalmic manifestation & management of CNS tumors in paediatric population Review
informahealthcare.com doi: 10.1586/17469899.2015.987755
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 82
.3.1
94.1
94 o
n 11
/27/
14Fo
r pe
rson
al u
se o
nly.

MRI findings, radiographic imaging should not be used as ascreening tool for OPGs.
Given the variable natural history of OPG, initial manage-ment in most case is close observation with serial neuro-ophthalmic evaluations. Quantitative monocular VA testing isthe most useful test in detecting OPGs requiring treatment [37].All children must have TAC testing and HOTV-computer-based assessment when old enough.
A clinically significant change in VA of more than two linesis most important and should drive the decision to treat [38].No other visual or investigative test is mandatory. Among othertools that have been used, OCT may provide a reliable andquantitative structural marker of visual pathway integrity thatcan be followed over time and should be welcome [57].
As OPG progression mainly occurs in the first 2 years afterdiagnosis, frequent follow-up examinations are indicated duringthis critical period [33]. In addition, due to the potential for latediagnosis of OPGs, vigilant observation of patients until age12 is currently recommended [26].
In Leeds, the current practice for the follow-up of childrenwith NF 1 and not identified OPG include neuro-ophthalmologicexaminations at 3-month intervals during the first 2 years of life.Children are then followed at 6-month intervals until the age of4 and thereafter annually until age 8. Beyond this age, patientsare being discharged to the community optometrist.
Children with NF 1 and known OPGs are followed at3-month intervals for the first 12 months following diagnosis.Thereafter, neuro-ophthalmic assessment is performed at 6-monthintervals for 2 years, then annually through adolescence.
VA is a useful tool in monitoring for recurrence in childrenwith craniopharyngioma. However, its role in diagnosis shouldnot be overestimated and cannot replace radiographic imagingsince by the time that causes new visual deterioration, tumor issizable and the likelihood of retrieval therapy is diminished.Thus, MRI remains the recommended means of follow-up in achild with craniopharyngioma. The UK consensus guidelinesrecommend MRI surveillance at 6-month intervals [80]. In con-trast, most centers in North America suggest neuroimagingwithin 2 years after definitive treatment as most tumors tend torecur beyond this period.
ConclusionTo provide optimal care for children with OPGs and brain tumorsaffecting the optic pathway one must provide a multidisciplinaryapproach including neurosurgery, pediatrics, neuro-oncology andophthalmology. Oncologists and neuro-ophthalmologists shouldwork more closely so that patients with OPG can benefit from thecombined expertise of physicians in both disciplines.
Given the clinical and molecular heterogeneity of OPGs,more studies are still needed to establish evidence-based guide-lines for the management of children with these lesions. Oncol-ogists have to make the tough ‘red button’ decisions, butophthalmologists can help. VA testing is mandatory, and a lowthreshold for suspicion regarding amblyopia, headaches andacquired strabismus with diplopia is needed.
Although surgery, radiation therapy and chemotherapy arecurrently involved in the management of CNS tumors, thereare new treatments and more on the near horizon targeting cel-lular microenvironment which make it worth screening fortumors affecting the optic pathway. Children with braintumors are best managed in a tertiary center, but there areoften cases that present more locally.
Expert commentaryBrain tumors may cause a variety of ocular symptoms and signs.MRI scanning remains the gold-standard diagnostic test and rec-ommended means of follow-up in children with brain tumors.However, quantitative monocular VA testing is the most usefultest in detecting OPGs requiring treatment. The current practicefor the follow-up of children with NF 1 with/without OPGs devel-oped in Leeds is presented using internationally developed stan-dardized protocols. The neuro-ophthalmic examination is a keycomponent in the diagnosis and management of OPGs. RAPDalways signifies significant optic nerve damage and is therefore vitalfor the clinician to look for it. Gross total resection of tumor isrelated with longer recurrence-free intervals. However, when tumortotal removal is not possible, irradiation may prevent recurrence,although it is not recommended in young children and inNF 1 patients due to increased risk of radiation detrimental effects.Combination chemotherapy regimens are being used with variablesuccess in the treatment of pediatric brain tumors. Bevacizumab-based therapy in OPGs may greatly improve visual outcomes andshould be considered in appropriate clinical situations, while theimplementation of molecular targeted therapies for OPG is prom-ising. A multidisciplinary approach including neurosurgery, pediat-rics, neuro-oncology and ophthalmology is essential in order toprovide optimal care in children with brain tumors.
Five-year viewHand-held OCT may provide a reliable and quantitative struc-tural marker of visual pathway integrity that can be followedover time and is welcome. It could be used as a noninvasiveand inexpensive screening tool for OPGs reducing visit dura-tion and total cost. New techniques of delivering radiationincluding fractionated stereotactic and proton beam radiother-apy are being pursued. Drugs targeting tumor angiogenesissuch as bevacizumab may be widely used for the treatment ofrecurrent and refractory OPGs as long as issues regarding opti-mal dosing and long-term toxicity are solved. In addition, thereare new treatments and more on the near horizon targeting cel-lular microenvironment which make it worth screening fortumors affecting the optic pathway.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with
any organization or entity with a financial interest in or financial conflict
with the subject matter or materials discussed in the manuscript. This
includes employment, consultancies, honoraria, stock ownership or options,
expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Review Drimtzias & Simmons
doi: 10.1586/17469899.2015.987755 Expert Rev. Ophthalmol.
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 82
.3.1
94.1
94 o
n 11
/27/
14Fo
r pe
rson
al u
se o
nly.

Key issues
• Children with brain tumors can present to ophthalmologist with a variety of ocular symptoms and signs.
• MRI is the preferred method of imaging for CNS tumors. However, due to the poor correlation between visual acuity and MRI findings,
radiographic imaging should not be used as a screening tool for optic pathway gliomas (OPGs).
• Quantitative monocular visual acuity testing is the most useful test in detecting OPGs requiring treatment. All children must have teller
acuity card testing and HOTV-computer based assessment when old enough. No other visual or investigative test is mandatory.
• OCT may aid in early detection of OPGs, thus allowing for timely initiation of chemotherapy and arrest of visual deterioration.
• The fundamental goal of surgery in children with brain tumors is removal as much of the tumor as possible in order to improve long-
term survival and decrease recurrence rate. However, surgery is not warranted in NF 1 subjects as they tend to have more
diffuse disease.
• Radiotherapy is efficacious for the management of pediatric brain malignancies, although it should be avoided in children younger than
5 years of age and in subjects with oncogenic conditions.
• Combination chemotherapy regimens are being used with variable success in the treatment of pediatric brain tumors. The combination
of carboplatin and vincristine is the most common regime in NF 1-related OPGs.
• Bevacizumab-based therapy in OPGs may greatly improve visual outcomes and should be considered in appropriate clinical situations,
while the implementation of molecular targeted therapies is promising.
• Oncologists and neuro-ophthalmologists should work more closely so that patients with OPG can benefit from the combined expertise
of physicians in both disciplines.
• Leeds Teaching Hospitals NHS Trust has developed methods of practice for the screening of NF 1 patients with/without OPGs using
internationally developed standardized protocols.
References
Papers of special note have been highlighted as:
• of interest
•• of considerable interest
1. Plowman PN, Brada M. Paediatric brain
tumours. Br Med Bull 1996;52:802-17
2. Avery RA, Ferner RE, Listernick R, et al.
Visual acuity in children with low grade
gliomas of the visual pathway: implications
for patient care and clinical research. J
Neurooncol 2012;110:1-7
3. Binning MJ, Liu JK, Kestle JR, et al. Optic
pathway gliomas: a review. Neurosurg Focus
2007;23:E2
4. Sylvester CL, Drohan LA, Sergott RC.
Optic-nerve gliomas, chiasmal gliomas and
neurofibromatosis type 1. Curr Opin
Ophthalmol 2006;17:7-11
5. Balcer LJ, Liu GT, Heller G, et al. Visual
loss in children with neurofibromatosis
type 1 and optic pathway gliomas: relation
to tumor location by magnetic resonance
imaging. Am J Ophthalmol 2001;131:442-5
6. Gayre GS, Scott IU, Feuer W, et al.
Long-term visual outcome in patients with
anterior visual pathway gliomas. J
Neuroophthalmol 2001;21:1-7
7. Defoort-Dhellemmes S, Moritz F,
Bouacha I, et al. Craniopharyngioma:
ophthalmological aspects at diagnosis.
J Pediatr Endocrinol Metab 2006;
19(Suppl 1):321-4
8. Abrams LS, Repka MX. Visual outcome of
craniopharyngioma in children. J Pediatr
Ophthalmol Strabismus 1997;34:223-8
9. Drimtzias E, Falzon K, Picton S, et al.
The ophthalmic natural history of
paediatric craniopharyngioma: a long-term
review. J Neurooncol 2014. [Epub ahead
of print]
10. Chen C, Okera S, Davies PE, et al.
Craniopharyngioma: a review of long-term
visual outcome. Clin Experiment
Ophthalmol 2003;31:220-8
11. Kelly JP, Weiss AH. Comparison of pattern
visual-evoked potentials to perimetry in the
detection of visual loss in children with
optic pathway gliomas. J AAPOS 2006;10:
298-306
12. Listernick R, Ferner RE, Piersall L, et al.
Late-onset optic pathway tumors in children
with neurofibromatosis 1. Neurology
2004;63:1944-6
13. Jahraus CD, Tarbell NJ. Optic pathway
gliomas. Pediatr Blood Cancer 2006;46:
586-96
14. Liu GT, Brodsky MC, Phillips PC, et al.
Optic radiation involvement in optic
pathway gliomas in neurofibromatosis. Am J
Ophthalmol 2004;137:407-14
15. Listernick R, Ferner RE, Liu GT, et al.
Optic pathway gliomas in
neurofibromatosis-1: controversies and
recommendations. Ann Neurol 2007;61:
189-98
16. Astrup J. Natural history and clinical
management of optic pathway glioma. Br J
Neurosurg 2003;17:327-35
17. Miller NR, Newman NJ, Biousse V,
Kerrison JB. Editors Walsh and Hoyt’sClinical Neuro-Ophthalmology, 6th edition.
Volume 3, Baltimore: Lippincott-Williams
& Wilkins; 2005
18. Nicolin G, Parkin P, Mabbott D, et al.
Natural history and outcome of optic
pathway gliomas in children. Pediatr Blood
Cancer 2009;53:1231-7
19. King A, Listernick R, Charrow J, et al.
Optic pathway gliomas in neurofibromatosis
type 1: the effect of presenting symptoms
on outcome. Am J Med Genet A
2003;122A:95-9
20. Liu GT. Optic gliomas of the anterior
visual pathway. Curr Opin Ophthalmol
2006;17:427-31
21. Van Effenterre R, Boch AL.
Craniopharyngioma in adults and children:
a study of 122 surgical cases. J Neurosurg
2002;97:3-11
22. Matthay KK, Blaes F, Hero B, et al.
Opsoclonus myoclonus syndrome in
neuroblastoma a report from a workshop on
the dancing eyes syndrome at the advances
in neuroblastoma meeting in Genoa, Italy,
2004. Cancer Lett 2005;228:275-82
23. Tate ED, Allison TJ, Pranzatelli MR, et al.
Neuroepidemiologic trends in 105 US cases
of pediatric opsoclonus-myoclonus
Ophthalmic manifestation & management of CNS tumors in paediatric population Review
informahealthcare.com doi: 10.1586/17469899.2015.987755
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 82
.3.1
94.1
94 o
n 11
/27/
14Fo
r pe
rson
al u
se o
nly.

syndrome. J Pediatr Oncol Nurs 2005;22:
8-19
24. Tow SL, Chandela S, Miller NR, et al.
Long-term outcome in children with
gliomas of the anterior visual pathway.
Pediatr Neurol 2003;28:262-70
25. Mullaney PB, Nabi NU, Thorner P, et al.
Ophthalmic involvement as a presenting
feature of nonorbital childhood
parameningeal embryonal
rhabdomyosarcoma. Ophthalmology
2001;108:179-82
26. Grill J, Laithier V, Rodriguez D, et al.
When do children with optic pathway
tumours need treatment? An oncological
perspective in 106 patients treated in a
single centre. Eur J Pediatr 2000;159:692-6
27. Omoti AE, Omoti CE. Ocular toxicity of
systemic anticancer chemotherapy. Pharm
Pract (Granada) 2006;4:55-9
28. Katz BJ, Ward JH, Digre KB, et al.
Persistent severe visual and
electroretinographic abnormalities after
intravenous Cisplatin therapy. J
Neuroophthalmol 2003;23:132-5
29. Mulvihill A, Budning A, Jay V, et al.
Ocular motility changes after subtenon
carboplatin chemotherapy for
retinoblastoma. Arch Ophthalmol 2003;121:
1120-4
30. Kremens B, Hero B, Esser J, et al. Ocular
symptoms in children treated with
human-mouse chimeric anti-GD2 mAb
ch14.18 for neuroblastoma. Cancer
Immunol Immunother 2002;51:107-10
31. Durkin SR, Roos D, Higgs B, et al.
Ophthalmic and adnexal complications of
radiotherapy. Acta Ophthalmol Scand
2007;85:240-50
32. Hall EJ, Henry S. Kaplan Distinguished
Scientist Award 2003. The crooked shall be
made straight; dose-response relationships
for carcinogenesis. Int J Radiat Biol
2004;80:327-37
33. Parsons JT, Bova FJ, Fitzgerald CR, et al.
Severe dry-eye syndrome following external
beam irradiation. Int J Radiat Oncol Biol
Phys 1994;30:775-80
34. Robertson DM, Buettner H, Gorman CA,
et al. Retinal microvascular abnormalities in
patients treated with external radiation for
graves ophthalmopathy. Arch Ophthalmol
2003;121:652-7
35. Bhandare N, Monroe AT, Morris CG,
et al. Does altered fractionation influence
the risk of radiation-induced optic
neuropathy? Int J Radiat Oncol Biol Phys
2005;62:1070-7
36. Ferner RE, Huson SM, Thomas N, et al.
Guidelines for the diagnosis and
management of individuals with
neurofibromatosis 1. J Med Genet 2007;44:
81-8
37. Fisher MJ, Loguidice M, Gutmann DH,
et al. Visual outcomes in children with
neurofibromatosis type 1-associated optic
pathway glioma following chemotherapy:
a multicenter retrospective analysis. Neuro
Oncol 2012;14:790-7
38. Avery RA, Fisher MJ, Liu GT. Optic
pathway gliomas. J Neuroophthalmol
2011;31:269-78
39. Blazo MA, Lewis RA, Chintagumpala MM,
et al. Outcomes of systematic screening for
optic pathway tumors in children with
Neurofibromatosis Type 1. Am J Med
Genet A 2004;127A:224-9
40. Falsini B, Ziccardi L, Lazzareschi I, et al.
Longitudinal assessment of childhood optic
gliomas: relationship between flicker visual
evoked potentials and magnetic resonance
imaging findings. J Neurooncol 2008;88:
87-96
41. Dalla Via P, Opocher E, Pinello ML, et al.
Visual outcome of a cohort of children with
neurofibromatosis type 1 and optic pathway
glioma followed by a pediatric
neuro-oncology program. Neuro Oncol
2007;9:430-7
42. Kelly JP, Weiss AH. Detection of tumor
progression in optic pathway glioma with
and without neurofibromatosis type 1.
Neuro Oncol 2013;15:1560-7
43. Avery RA, Ferner RE, Listernick R, et al.
Visual acuity in children with low grade
gliomas of the visual pathway: implications
for patient care and clinical research. J
Neurooncol 2012;110:1-7
44. Avery RA, Bouffet E, Packer RJ, et al.
Feasibility and comparison of visual acuity
testing methods in children with
neurofibromatosis type 1 and/or optic
pathway gliomas. Invest Ophthalmol Vis Sci
2013;54:1034-8
•• Authors highlight the importance of
quantitative visual acuity testing as a
useful tool in detecting optic pathway
gliomas (OPGs) requiring treatment.
45. Lambert SR, Buckley EG, Drews-Botsch C,
et al. A randomized clinical trial comparing
contact lens with intraocular lens correction
of monocular aphakia during infancy:
grating acuity and adverse events at age
1 year. Arch Ophthalmol 2010;128:810-18
46. Beck RW, Maguire MG, Bressler NM,
et al. Visual acuity as an outcome measure
in clinical trials of retinal diseases.
Ophthalmology 2007;114:1804-9
47. Kelly JP, Leary S, Khanna P, et al.
Longitudinal measures of visual function,
tumor volume, and prediction of visual
outcomes after treatment of optic pathway
gliomas. Ophthalmology 2012;119:1231-7
48. Safran AB, Laffi GL, Bullinger A, et al.
Feasibility of automated visual field
examination in children between 5 and
8 years of age. Br J Ophthalmol 1996;80:
515-18
49. Chang BC, Mirabella G, Yagev R, et al.
Screening and diagnosis of optic pathway
gliomas in children with neurofibromatosis
type 1 by using sweep visual evoked
potentials. Invest Ophthalmol Vis Sci
2007;48:2895-902
50. Trisciuzzi MT, Riccardi R, Piccardi M,
et al. A fast visual evoked potential method
for functional assessment and follow-up of
childhood optic gliomas. Clin Neurophysiol
2004;115:217-26
51. Wolsey DH, Larson SA, Creel D, et al. Can
screening for optic nerve gliomas in patients
with neurofibromatosis type I be performed
with visual-evoked potential testing? J
AAPOS 2006;10:307-11
52. Siatkowski RM. VEP testing and visual
pathway gliomas: not quite ready for prime
time. J AAPOS 2006;10:293-5
53. Avery RA, Liu GT, Fisher MJ, et al. Retinal
nerve fiber layer thickness in children with
optic pathway gliomas. Am J Ophthalmol
2011;151:542-9
54. Chang L, El-Dairi MA, Frempong TA,
et al. Optical coherence tomography in the
evaluation of neurofibromatosis
type-1 subjects with optic pathway gliomas.
J AAPOS 2010;14:511-17
55. El-Dairi MA, Asrani SG, Enyedi LB, et al.
Optical coherence tomography in the eyes
of normal children. Arch Ophthalmol
2009;127:50-8
56. Maldonado RS, Izatt JA, Sarin N, et al.
Optimizing hand-held spectral domain
optical coherence tomography imaging for
neonates, infants, and children. Invest
Ophthalmol Vis Sci 2010;51:2678-85
57. Avery RA, Hwang EI, Ishikawa H, et al.
Handheld optical coherence tomography
during sedation in young children with
optic pathway gliomas. JAMA Ophthalmol
2014;132:265-71
• Authors advocate that hand-held optical
coherence tomography may be a reliable,
noninvasive and inexpensive screening
Review Drimtzias & Simmons
doi: 10.1586/17469899.2015.987755 Expert Rev. Ophthalmol.
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 82
.3.1
94.1
94 o
n 11
/27/
14Fo
r pe
rson
al u
se o
nly.

tool for OPGs reducing visit duration
and cost.
58. Sievert AJ, Fisher MJ. Pediatric low-grade
gliomas. J Child Neurol 2009;24:1397-408
59. Ahn Y, Cho BK, Kim SK, et al. Optic
pathway glioma: outcome and prognostic
factors in a surgical series. Childs Nerv Syst
2006;22:1136-42
60. Elliott RE, Wisoff JH. Successful surgical
treatment of craniopharyngioma in very
young children. J Neurosurg Pediatr
2009;3:397-406
61. Elliott RE, Jane JA Jr, Wisoff JH. Surgical
management of craniopharyngiomas in
children: meta-analysis and comparison of
transcranial and transsphenoidal approaches.
Neurosurgery 2011;69:630-43
62. Komotar RJ, Starke RM, Raper DM, et al.
Endoscopic endonasal compared with
microscopic transsphenoidal and open
transcranial resection of
craniopharyngiomas. World Neurosurg
2012;77:329-41
63. Grabenbauer GG, Schuchardt U,
Buchfelder M, et al. Radiation therapy of
optico-hypothalamic gliomas (OHG)–
radiographic response, vision and late
toxicity. Radiother Oncol 2000;54:239-45
64. Sharif S, Ferner R, Birch JM, et al. Second
primary tumors in neurofibromatosis
1 patients treated for optic glioma:
substantial risks after radiotherapy. J Clin
Oncol 2006;24:2570-5
65. Ater JL, Zhou T, Holmes E, et al.
Randomized study of two chemotherapy
regimens for treatment of low-grade glioma
in young children: a report from the
Children’s Oncology Group. J Clin Oncol
2012;30:2641-7
66. Bouffet E, Jakacki R, Goldman S, et al.
Phase II study of weekly vinblastine in
recurrent or refractory pediatric low-grade
glioma. J Clin Oncol 2012;30:1358-63
67. Fisher MJ, Loguidice M, Gutmann DH,
et al. Visual outcomes in children with
neurofibromatosis type 1-associated optic
pathway glioma following chemotherapy:
a multicenter retrospective analysis. Neuro
Oncol 2012;14:790-7
68. Moreno L, Bautista F, Ashley S, et al. Does
chemotherapy affect the visual outcome in
children with optic pathway glioma?
A systematic review of the evidence. Eur J
Cancer 2010;46:2253-9
69. Laithier V, Grill J, Le Deley MC, et al.
Progression-free survival in children with
optic pathway tumors: dependence on age and
the quality of the response to chemotherapy–
results of the first French prospective study for
the French Society of Pediatric Oncology. J
Clin Oncol 2003;21:4572-8
70. Goldbrunner RH, Wagner S, Roosen K,
et al. Models for assessment of angiogenesis
in gliomas. J Neuro Oncol 2000;50:53-62
71. Bartels U, Hawkins C, Jing M, et al.
Vascularity and angiogenesis as predictors of
growth in optic pathway/hypothalamic
gliomas. J Neurosurg 2006;104:314-20
72. Machein MR, Plate KH. VEGF in brain
tumors. J Neurooncol 2000;50:109-20
73. Hwang EI, Jakacki RI, Fisher MJ, et al.
Long-term efficacy and toxicity of
bevacizumab-based therapy in children with
recurrent low-grade gliomas. Pediatr Blood
Cancer 2013;60:776-82
74. Avery RA, Hwang EI, Jakacki RI, et al.
Marked recovery of vision in children with
optic pathway gliomas treated with
bevacizumab. JAMA Ophthalmol 2014;132:
111-14
• Authors highlight the role of anti-VEGF
agents for the treatment of recurrent or
refractory OPGs.
75. Bokstein F, Shpigel S, Blumenthal DT.
Treatment with bevacizumab and irinotecan
for recurrent high-grade glial tumors.
Cancer 2008;112:2267-73
76. Warrington NM, Gianino SM, Jackson E,
ET AL. Cyclic AMP suppression is
sufficient to induce gliomagenesis in a
mouse model of neurofibromatosis-1.
Cancer Res 2010;70:5717-27
77. Pfister S, Janzarik WG, Remke M, et al.
BRAF gene duplication constitutes a
mechanism of MAPK pathway activation in
low-grade astrocytomas. J Clin Invest
2008;118:1739-49
78. Jones DT, Gronych J, Lichter P, et al.
MAPK pathway activation in pilocytic
astrocytoma. Cell Mol Life Sci 2012;69:
1799-811
•• New clinical trials and targeted molecular
therapies may open new avenues for the
treatment of pediatric brain tumors.
79. Jansen MH, Kaspers GJ. A new era for
children with diffuse intrinsic pontine
glioma: hope for cure? Expert Rev
Anticancer Ther 2012;12:1109-12
80. Spoudeas HA. Paediatric endocrine
tumours. A multidisciplinary consensus
statement of best practice from a working
group convened under the auspices of the
BSPED and UKCCSG. Novo Nordisk Ltd;
Crawley: 2005
Ophthalmic manifestation & management of CNS tumors in paediatric population Review
informahealthcare.com doi: 10.1586/17469899.2015.987755
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 82
.3.1
94.1
94 o
n 11
/27/
14Fo
r pe
rson
al u
se o
nly.