Embed Size (px)
Citation preview

OPG/RANKL/RANK axis is a critical inflammatorysignaling system in ischemic brain in miceMunehisa Shimamuraa, Hironori Nakagamia, Mariana K. Osakoa,1, Hitomi Kurinamia, Hiroshi Koriyamaa,Pang Zhengdab, Hideki Tomiokac, Akiko Tenmaa, Kouji Wakayamad, and Ryuichi Morishitac,2
aDivision of Vascular Medicine and Epigenetics, Osaka University United Graduate School of Child Development, Osaka 565-0871, Japan; bDepartment ofGeriatric Medicine and Nephrology, Osaka University Graduate School of Medicine, Japan; cDepartment of Clinical Gene Therapy, Osaka University GraduateSchool of Medicine, Osaka 565-0871, Japan; and dDepartment of Advanced Clinical Science and Therapeutics, Graduate School of Medicine, The University ofTokyo, Tokyo 113-8655, Japan
Edited by Michael Karin, University of California, San Diego School of Medicine, La Jolla, CA, and approved April 24, 2014 (received for reviewJanuary 13, 2014)
Osteoprotegerin (OPG) is a soluble secreted protein and a decoyreceptor, which inhibits a receptor activator of nuclear factor κB(NF-κB) ligand (RANKL)/the receptor activator of NF-κB (RANK)signaling. Recent clinical studies have shown that a high-serum-OPG level is associated with unfavorable outcome in ischemicstroke, but it is unclear whether OPG is a culprit or an innocentbystander. Here we demonstrate that enhanced RANKL/RANK sig-naling inOPG−/− mice or recombinant RANKL-treated mice contrib-uted to the reduction of infarct volume and brain edema viareduced postischemic inflammation. On the contrary, infarct vol-ume was increased by reduced RANKL/RANK signaling in OPG−/−
mice and WT mice treated with anti-RANKL neutralizing antibody.OPG, RANKL, and RANK mRNA were increased in the acute stageand were expressed in activated microglia and macrophages.Although enhanced RANKL/RANK signaling had no effects inglutamate, CoCl2, or H2O2-stimulated neuronal culture, enhancedRANKL/RANK signaling showed neuroprotective effects with re-duced expression in inflammatory cytokines in LPS-stimulatedneuron-glia mixed culture, suggesting that RANKL/RANK signalingcan attenuate inflammation through a Toll-like receptor signalingpathway in microglia. Our findings propose that increased OPGcould be a causal factor of reducing RANKL/RANK signaling and in-creasing postischemic inflammation. Thus, the OPG/RANKL/RANK axisplays critical roles in controlling inflammation in ischemic brains.
cerebral ischemia | neuroprotection | immune cells
An elevated serum osteoprotegerin (OPG) level has beenreported to be associated with the severity (1, 2), subtype (2),
poor functional outcome (1), and long-term mortality of ischemicstroke (2, 3). However, it is still unclear why a high-serum-OPGlevel could result in a poor prognosis in ischemic stroke.OPG is a soluble secreted protein that lacks transmembrane
and cytoplasmic domains. It binds to a receptor activator of nu-clear factor-кB ligand (RANKL) (4, 5), whose receptor is the re-ceptor activator of NF-κB (RANK), and inhibits RANKL/RANKsignaling. The OPG/RANKL/RANK system in bone (6) andvasculature (7) is well known to work on bone metabolism (8) andvascular calcification (7). In addition, immune cells (6, 9–12) ex-press these molecules, and this system is believed to be associatedwith the regulation of inflammatory and immune responses (13,14). RANKL is expressed in CD4+T cells (6) andmacrophages (9,10), whereas OPG is expressed in mature B cells (6) and macro-phages (11, 12). RANK is expressed in macrophage and dendriticcells (6). One of the functions of RANKL/RANK signaling in theimmune system is to control the thymocyte-mediated medullaformation and the formation of self-tolerance in T cells (14), aswell as the number of regulatory T cells (Treg) (15). Additionally,RANKLdirectly contributes to the regulation of proinflammatorycytokine production in macrophages (13, 16).Despite these characteristics of the OPG/RANKL/RANK
system, its action on inflammation in central nervous systemdiseases has yet to be studied. Ischemic stroke is a typical acute
inflammatory disease, and postischemic inflammation affects theoutcome, i.e., the infarct volume (17). These inflammatory cyto-kines are produced mainly from microglia in the early phase andfrom mixed microglia/macrophage (M/M) in the delayed phase,i.e., 12–24 h after ischemia, whereas neutrophilic granulocytes arenot responsible for the production of those inflammatory cyto-kines (17). Because OPG/RANKL/RANK is expressed in mac-rophages (6, 9–12) and affects inflammatory responses (13), wehypothesized that one of the mechanisms of poor outcome inhigh-level OPGmight reflect themodulation of such postischemicinflammations by the OPG/RANKL/RANK signaling system.Interestingly, OPG, RANKL, and RANK have also been re-
ported to be expressed in normal brain in rodents, although thedistribution of their expression is controversial. Early reportsshowed that RANKL mRNA was expressed in neurons in thecerebral cortex (18) and that RANK (19) and OPG (5) mRNAwas expressed in normal brain. However, a recent report re-vealed that the RANK protein was specifically expressed inneurons and astrocytes in the preoptic area and the medial septalnucleus, whereas RANKL mRNA was expressed in the lateralseptal nucleus (20). In normal brain, RANKL/RANK signalingwas reported to be associated with fever and body temperature
Significance
Although a high-serum osteoprotegerin (OPG) level is associ-ated with an unfavorable outcome in ischemic stroke, it is un-clearwhetherOPG is a culprit or an innocent bystander. Hereweshow that the deletion of OPG and enhanced RANKL/RANKsignaling contribute to the reduction of infarct volume withlower brain edema, whereas infarct volume is increased by re-duced RANKL/RANK signaling in OPG−/− mice and WT micetreated with anti-RANKL neutralizing antibody. OPG, RANKL,and RANK mRNA were increased in ischemic brain and wereexpressed in activated microglia and macrophages. EnhancedRANKL/RANK signaling showed neuroprotective effects withreduced expression in inflammatory cytokines in LPS-stimulatedneuron-gliamixed culture.Our findings propose anti-inflammatoryroles for RANKL/RANK signaling in ischemic brains.
Author contributions: M.S. and R.M. designed research; M.S., M.K.O., and H. Kurinamiperformed research; H.N., H. Koriyama, P.Z., H.T., A.T., and K.W. analyzed data; and M.S.,H.N., and R.M. wrote the paper.
Conflict of interest statement: The Department of Clinical Gene Therapy is financiallysupported by AnGes MG, Novartis, Shionogi, Boeringher, and Rohto. The Division ofVascular Medicine and Epigenetics is financially supported by Bayer. R.M. is a founderand stockholder of AnGes MG and a former board member.
This article is a PNAS Direct Submission.1Present address: Department of Cell and Molecular Biology, Ribeirão Preto MedicalSchool, University of São Paulo, Ribeirão Preto, 04044-010 São Paulo, Brazil.
2To whom correspondence should be addressed. E-mail: [email protected].
This article contains supporting information online at www.pnas.org/lookup/suppl/doi:10.1073/pnas.1400544111/-/DCSupplemental.
www.pnas.org/cgi/doi/10.1073/pnas.1400544111 PNAS | June 3, 2014 | vol. 111 | no. 22 | 8191–8196
MED
ICALSC
IENCE
S

control (20). Because body temperature is associated with theoutcome in ischemic stroke, we also hypothesized that themodulation of body temperature by the OPG/RANKL/RANKsystem might be another mechanism behind a poor outcome inischemic stroke. To clarify these hypotheses, we examined theaction of the OPG/RANKL/RANK signaling system in a transientmiddle cerebral artery occlusion (MCAo) model using OPG−/−
mice and treated RANK fragment crystalizable (Fc) chimera toinhibit the function of RANKL or recombinant RANKL.
ResultsEffect of OPG/RANKL/RANK Signaling on Infarct Volume. Becausea high-serum-OPG level is associated with stroke severity inclinical trials (1–3), we examined the effects of OPG in ischemicbrain using OPG−/− mice (Fig. 1A). The OPG−/− mice showeda significant reduction in infarct volume compared with WT mice(Fig. 1A), which was associated with a significant decrease incerebral edema (Fig. 1B). Although the differences in thestructure of cerebral vessels and microcirculations could affectstroke outcome, no differences were observed in the pial arterialanastomoses in middle cerebral arteries and anterior cerebralarteries and the microcirculations in cerebral cortex betweennormal OPG−/− mice and WT mice (Fig. S1). In addition, ce-rebral blood flow (CBF) was also similar between OPG−/− miceand WT mice during surgery (Fig. S2A). Although body tem-perature could be a critical factor for stroke outcome, there wasno significant difference in the circadian rhythm of rectal tem-perature between OPG−/− and WT mice (Fig. S2B) or thechange in rectal temperature after MCAo (Fig. S2C). These dataindicate that OPG might work as an exacerbation factor for is-chemic insult, independent of body temperature and CBF.Because OPG is a decoy receptor for RANKL and because
RANKL/RANK signaling was augmented in OPG−/− mice (21),we hypothesized that an enhancement of RANKL/RANK sig-naling might be responsible for the reduction of infarct volume
in OPG−/− mice. To elucidate the role of this system, we ex-amined the inhibition of RANKL/RANK signaling using an i.c.v.injection of a neutralizing anti-RANKL antibody, RANK Fc/chimera, in OPG−/− mice. As expected, the OPG−/− mice treatedwith RANK Fc/chimera exhibited a significant increase in infarctvolume (Fig. 1C). To examine whether RANKL/RANK signal-ing would be associated with the outcome even in WT mice,RANK Fc/chimera was also injected i.c.v. in a mild ischemic model.The infarct volume was also significantly exacerbated (Fig. 1D),although the extent was less than that observed in OPG−/−
mice (Fig. S3A). These results suggest that RANKL/RANKsignaling might act as a protective signal in the ischemic brainin both OPG−/− and WT mice. However, RANKL/RANK sig-naling might not be fully stimulated in WT mice due to thepossibility that OPG partly blocks the RANKL/RANK signalingin WT mice.To further examine the action of RANKL, WT mice in a se-
vere ischemic model were treated with i.c.v. of RANKL startingat 4 h after MCAo (Fig. 1 E and F). The mice treated withRANKL showed a tendency to have a low mortality rate (Fig.S3B), a significantly lower infarct volume (Fig. 1E), and lessformation of cerebral edema (Fig. 1F). Similar to OPG−/− mice,no differences in CBF were observed during the surgery (Fig.S4A). Because a single i.c.v. injection of RANKL was reported toaffect the core body temperature (20), we examined the changeof core body temperature using data loggers (Fig. S4 B–D). Thecore body temperature was not affected by the i.c.v. injection ofRANKL in normal mice (Fig. S4B) and mice exposed to MCAo(Fig. S4 C and D). These results indicated that the stimulation ofRANKL/RANK signaling resulted in a reduction of ischemicinjury without changes in body temperature or CBF.
Temporal Profile of RANK, RANKL, and OPG mRNA Expression. Next,we examined the temporal expression of RANK, RANKL, andOPG mRNA in the ischemic brain in WT mice (Fig. 2). RANKmRNA was increased starting at 4 h after MCAo and peaked at12 h after MCAo. RANKL and OPG mRNA showed a biphasicprofile. The peak of RANKL expression occurred at 7 and 48 hafter MCAo, and OPG expression peaked at 12–24 and 72 hafter MCAo. In OPG−/− mice, RANK and RANKL mRNA werealso increased after MCAo (Fig. 2 A and B) although the
Fig. 1. Infarct volume and brain edema in OPG−/− mice and mice treatedwith anti-RANKL neutralizing antibody or RANKL. The infarct volume at 72 hafter 45 min middle cerebral artery occlusion (MCAo) (A–C), 35 min MCAo(D), and 70 min MCAo (E and F). (A and B) OPG−/− mice showed a reducedinfarct volume and brain edema compared with WT mice. **P < 0.01 vs. WTmice. n = 8 in WT mice and n = 7 in OPG−/− mice. (C) Intracerebroventricularinjection of anti-RANKL neutralizing antibody, which inhibited RANKL/RANKsignaling, exacerbated the infarct volume in OPG−/− mice. *P < 0.05 vs. BSA-injected mice. n = 6 in each group. (D) Treatment with anti-RANKL neu-tralizing antibody in WT mice also showed an increased infarct volume.**P < 0.01; *P < 0.05 vs. BSA injected mice. n = 10 in BSA-treated mice; n = 11in RANKL-treated mice. (E) WT mice treated with RANKL showed lower in-farct volume when the mice survived to 72 h after MCAo (Fig. S3B) werecompared. **P < 0.01; *P < 0.05 vs. BSA injected mice. (F) There was a lowerformation of brain edema in RANKL-treated mice. n = 8 in RANKL-treatedmice and n = 5 in BSA-treated mice.
Fig. 2. Temporal expression profile of RANK, RANKL, or OPG mRNA in theischemic brain. The expression of RANK (A), RANKL (B), or OPG (C) mRNAwas analyzed by real-time RT-PCR. RANK mRNA was increased starting at 4 hafter MCAo and peaked at 12 h after MCAo. RANKL and OPG mRNA showeda biphasic profile. The peak of RANKL expression was at 7 and 48 h afterMCAo, and OPG expression peaked at 12–24 and 72 h after MCAo in WTmice. The expression of RANK and RANKL in OPG−/− mice was also shown.(n = 3 in each time point.)
8192 | www.pnas.org/cgi/doi/10.1073/pnas.1400544111 Shimamura et al.
expression level of RANK was lower than that in WT mice (Fig.2A). Thus, OPG, RANKL, and RANK were up-regulated in theacute phase of cerebral ischemia. Immunohistochemistry showedthat RANK, RANKL, and OPG were expressed in F4/80-posi-tive or Iba1-expressing M/M in the border between the infarctand intact areas, whereas the nonischemic hemisphere showedno expression of RANK, RANKL, and OPG (Fig. 3). OPG−/−
mice also showed expression of RANK and RANKL in M/M inthe ischemic hemisphere (Fig. S5). These data indicate that OPG,RANKL, and RANK work primarily in M/M in the acute stage ofischemic brain.
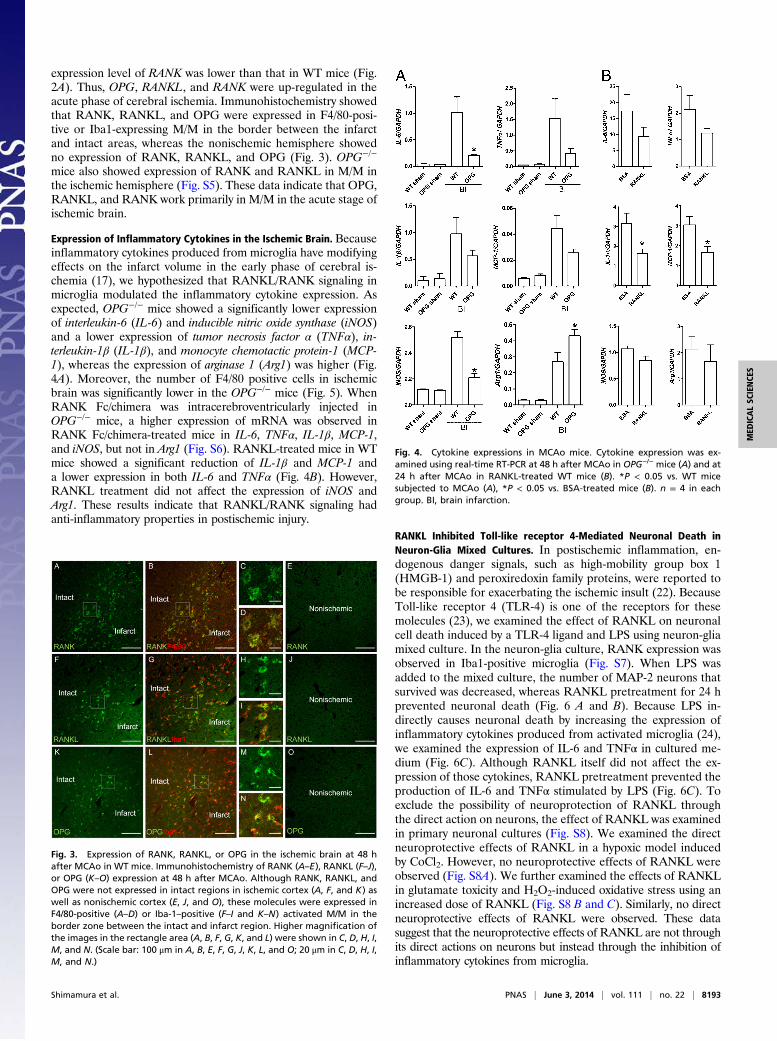
Expression of Inflammatory Cytokines in the Ischemic Brain. Becauseinflammatory cytokines produced from microglia have modifyingeffects on the infarct volume in the early phase of cerebral is-chemia (17), we hypothesized that RANKL/RANK signaling inmicroglia modulated the inflammatory cytokine expression. Asexpected, OPG−/− mice showed a significantly lower expressionof interleukin-6 (IL-6) and inducible nitric oxide synthase (iNOS)and a lower expression of tumor necrosis factor α (TNFα), in-terleukin-1β (IL-1β), and monocyte chemotactic protein-1 (MCP-1), whereas the expression of arginase 1 (Arg1) was higher (Fig.4A). Moreover, the number of F4/80 positive cells in ischemicbrain was significantly lower in the OPG−/− mice (Fig. 5). WhenRANK Fc/chimera was intracerebroventricularly injected inOPG−/− mice, a higher expression of mRNA was observed inRANK Fc/chimera-treated mice in IL-6, TNFα, IL-1β, MCP-1,and iNOS, but not in Arg1 (Fig. S6). RANKL-treated mice in WTmice showed a significant reduction of IL-1β and MCP-1 anda lower expression in both IL-6 and TNFα (Fig. 4B). However,RANKL treatment did not affect the expression of iNOS andArg1. These results indicate that RANKL/RANK signaling hadanti-inflammatory properties in postischemic injury.
RANKL Inhibited Toll-like receptor 4-Mediated Neuronal Death inNeuron-Glia Mixed Cultures. In postischemic inflammation, en-dogenous danger signals, such as high-mobility group box 1(HMGB-1) and peroxiredoxin family proteins, were reported tobe responsible for exacerbating the ischemic insult (22). BecauseToll-like receptor 4 (TLR-4) is one of the receptors for thesemolecules (23), we examined the effect of RANKL on neuronalcell death induced by a TLR-4 ligand and LPS using neuron-gliamixed culture. In the neuron-glia culture, RANK expression wasobserved in Iba1-positive microglia (Fig. S7). When LPS wasadded to the mixed culture, the number of MAP-2 neurons thatsurvived was decreased, whereas RANKL pretreatment for 24 hprevented neuronal death (Fig. 6 A and B). Because LPS in-directly causes neuronal death by increasing the expression ofinflammatory cytokines produced from activated microglia (24),we examined the expression of IL-6 and TNFα in cultured me-dium (Fig. 6C). Although RANKL itself did not affect the ex-pression of those cytokines, RANKL pretreatment prevented theproduction of IL-6 and TNFα stimulated by LPS (Fig. 6C). Toexclude the possibility of neuroprotection of RANKL throughthe direct action on neurons, the effect of RANKL was examinedin primary neuronal cultures (Fig. S8). We examined the directneuroprotective effects of RANKL in a hypoxic model inducedby CoCl2. However, no neuroprotective effects of RANKL wereobserved (Fig. S8A). We further examined the effects of RANKLin glutamate toxicity and H2O2-induced oxidative stress using anincreased dose of RANKL (Fig. S8 B and C). Similarly, no directneuroprotective effects of RANKL were observed. These datasuggest that the neuroprotective effects of RANKL are not throughits direct actions on neurons but instead through the inhibition ofinflammatory cytokines from microglia.
Fig. 3. Expression of RANK, RANKL, or OPG in the ischemic brain at 48 hafter MCAo in WT mice. Immunohistochemistry of RANK (A–E), RANKL (F–J),or OPG (K–O) expression at 48 h after MCAo. Although RANK, RANKL, andOPG were not expressed in intact regions in ischemic cortex (A, F, and K) aswell as nonischemic cortex (E, J, and O), these molecules were expressed inF4/80-positive (A–D) or Iba-1–positive (F–I and K–N) activated M/M in theborder zone between the intact and infarct region. Higher magnification ofthe images in the rectangle area (A, B, F, G, K, and L) were shown in C, D, H, I,M, and N. (Scale bar: 100 μm in A, B, E, F, G, J, K, L, and O; 20 μm in C, D, H, I,M, and N.)
Fig. 4. Cytokine expressions in MCAo mice. Cytokine expression was ex-amined using real-time RT-PCR at 48 h after MCAo in OPG−/− mice (A) and at24 h after MCAo in RANKL-treated WT mice (B). *P < 0.05 vs. WT micesubjected to MCAo (A), *P < 0.05 vs. BSA-treated mice (B). n = 4 in eachgroup. BI, brain infarction.
Shimamura et al. PNAS | June 3, 2014 | vol. 111 | no. 22 | 8193
MED
ICALSC
IENCE
S

DiscussionIn the present study, we demonstrate that the stimulation ofRANKL/RANK signaling through the deletion of OPG or ex-ogenous RANKL addition prevented the further exacerbation ofinfarct volume and cerebral edema by inhibiting the productionof inflammatory cytokines. This stimulation was independent ofbody temperature and CBF, whereas the blockade of RANKL/RANK signaling resulted in the exacerbation of infarct volume.OPG, RANKL, and RANK were up-regulated in M/M in theischemic border. Because microglia are responsible for the pro-duction of inflammatory cytokines in the early phase of ischemicbrain (17) and because RANK expression starts to be up-regu-lated at 4 h after MCAo, RANKL could act on microglia first.Thereafter, RANKL could work on M/M in the later phase be-cause both macrophages and microglia produce inflammatorycytokines 12–24 h after MCAo (17). Because LPS-induced neu-ronal death in mixed neuronal glia was prevented by RANKLthrough the inhibition of inflammatory cytokine production, onepossiblemechanismmight involve an inhibitory effect of RANKL/RANK signaling on TLR-4 signaling in activated microglia, whichhas been reported to be responsible for the receptor of intrinsicdanger signals in the ischemic brain (25). Similarly, in the laterphase, inflammatory cytokines from macrophages might be in-hibited by RANKL because a previous report demonstrated theanti-inflammatory action of RANKL in LPS-stimulated bone-marrow–derived macrophages and peritoneal macrophages (13).Therefore, the association of high OPG with poor functionaloutcome in clinics (1–3) could result from the attenuated anti-inflammatory function of RANKL/RANK signaling due to thehigher level of OPG, although the effects of the OPG/RANKL/RANK axis on bone metabolism (8) and vascular calcification (7)should be carefully considered.The molecular mechanisms that determine how RANKL affects
TLR signaling inmicroglia have yet to be clarified, but one possiblemechanism in the OPG−/− model could be associated with drivingthe alternative activation of M/M (M2) because iNOS mRNA wasdecreased and Arg1 mRNA was increased in the ischemic brainin OPG−/− mice. Unexpectedly, the blockade of RANKL/RANKsignaling with RANK Fc chimera did not decrease the expressionof Arg1 in OPG−/− mice, but we speculate that this might be dueto the functional compensation in the knockout mouse instead ofRANKL/RANK signaling. Further studies are necessary to clarifythe mechanisms that determine how OPG deletion influenceson phenotype of M/M. On the contrary, the i.c.v. injection of
RANKL in WT mice did not affect the expression of iNOS andArg1 mRNA. This finding suggests that the temporal stimulationof RANKLmight have anti-inflammatory effects without changesin M/M polarization. Because the previous study showed thatmyeloid differentiation primary response 88 (Myd88) expression wasdecreased in bone-marrow–derived macrophages by recombinantRANKL treatment (13), RANKL might work downstream ofTLR signaling in both microglia and macrophages. Furtherstudies are necessary to clarify the detailed mechanisms.In the present study, the expression level of RANK mRNA was
lower in OPG−/− mice, probably due to the chronic stimulationof RANKL in OPG−/− mice. Previous reports showed an in-consistent expression level of RANK and RANKL in OPG−/−
mice compared with WT mice: increased mRNA levels of RANKand RANKL in the aorta (21); the same expression level of RANKLmRNA expression in osteoblasts (26, 27); and a decreased ex-pression level of RANK mRNA in osteoclasts in 12-wk-old micefollowed by an increased level at 20 and 28 wk (28). From thisviewpoint, the expression level of RANK and RANKL in OPG−/−
might be dependent in cells or tissue.Compared with a previous report showing the site-specific
expression of RANK and RANKL in the normal brain, i.e., thepreoptic area and medial septal nucleus or the lateral septalnucleus (20), the present study showed that these moleculesstarted to be diffusely expressed in the cerebral cortex in theischemic border zone. These data indicate that the RANKL/RANK axis might not work in neurons and astrocytes in thecortex but that this axis might work in the activated microgliawhen the brain is exposed to ischemia. This speculation is sup-ported by the data indicating that RANKL exhibited neuro-protective effects in the mixed glia-neuron culture but not incultured neurons from the cerebral cortex. In addition, becauseOPG is expressed in activated M/M with the expression ofRANK, the OPG/RANKL/RANK axis might work through auto-crine and/or paracrine action in M/M. Thus, the RANKL/RANK
WT OPG-/- WT OPG-/-0
500
1000
1500
2000
**
Ischemic Nonischemic
Tota
l num
ber
of F
4/80
posi
tive
cells
Intact
Infarct
A
C
Intact
Infarct
BWT OPG-/- WT OPG-/-
OPG-/- OPG-/-
Fig. 5. Activated macrophage/microglia in the peri-infarct region in WT andOPG−/− mice. Immunohistochemistry for F4/80 was shown in ischemic cortex(A) and nonischemic brain (B) in WT (Left) or OPG−/− mice (Right). Thenumber of F4/80-positive cells was counted at 0.7 mm from the bregma (C).n = 8 in WT mice and n = 7 in OPG−/− mice. **P < 0.01 vs. WT mice. Ischemic,ischemic hemisphere; Nonischemic, nonischemic hemisphere.
Fig. 6. Prevention of LPS-triggered neuronal death by RANKL treatment.Typical immunohistochemical images for MAP2 in mixed neuron-glia cul-tures at 5 d after LPS stimulation (A). The cells were pretreated with 100 ng/mLRANKL for 24 h and exposed to 10 μg/mL LPS for 5 d. The LPS-treated cultureshowed a lower number of MAP2-positive cells compared with RANKL-treatedculture (B, n = 4 in each group). The expression of TNFα and IL-6 in medium at24 h after exposure to LPS was less in the group treated with 100 ng/mL RANKL(C). n = 3 in the cells without LPS; n = 10 in LPS-stimulated cells. #P < 0.05 vs.cells without LPS and RANKL; *P < 0.05 vs. LPS-stimulated cells without RANKL.
8194 | www.pnas.org/cgi/doi/10.1073/pnas.1400544111 Shimamura et al.

axis could be associated with other central nervous system dis-eases such as multiple sclerosis and Alzheimer’s disease, whereactivated microglia work as a deteriorative factor.Although the role of the RANKL/RANK axis in the patho-
logical brain has not been reported, except in the present study,its role in the control of body temperature and fever has beenreported in normal rodent brain (20). In this previous study,RANKL-injected mice (1, 10, or 100 ng single i.c.v. injection)showed the induction of fever at 6 h after injection, with theactivation of specific brain regions involved in thermoregula-tion and induction via the COX2-PGE2/EP3R pathway (20). Incontrast, the present study demonstrated that RANKL-injectedWT mice and OPG−/− mice did not show any differences incore body temperature in either normal mice or mice subjectedto MCAo. Although the cause of discrepancy between the pre-vious report (20) and the present study is still unclear, the betteroutcome in OPG−/− mice and RANKL-treated WT mice couldnot be explained by the differences in body temperature.Although we focused on the OPG/RANKL/RANK axis in
M/M in the acute stage of ischemic brain, it is possible that theOPG/RANKL/RANK axis might influence both the control ofT-cell–mediated immune responses because RANKL regulatesthe formation of self-tolerance in T cells (14) and any immuno-suppressive effects by controlling the number of Treg in allergiccontact hypersensitivity responses and the development of sys-temic autoimmunity (15). Because T lymphocytes are significantlyincreased at day 3 (29) and because Foxp3+ Treg cells work ascerebroprotective immunomodulators in the more delayed phase,i.e., 3–7 d after MCAo (30), the OPG/RANKL/RANK axis couldalso be associated with the regulation of T-cell–mediated immuneresponses in the delayed phase. Further studies are necessary toclarify the actions of the OPG/RANKL/RANK axis on the T-cell–mediated immune response.In conclusion, in the present study we demonstrate that the
OPG/RANKL/RANK system might be one of the key signalsregulating M/M-derived inflammatory responses in ischemicbrain. Because the i.c.v. injection of RANKL a minimum of 4 hafter MCAo decreased the infarct volume, RANKL/RANKsignaling might be a therapeutic target to treat ischemic stroke.Although the development of a delivery system and a modifi-cation of RANKL are needed to avoid RANKL-induced osteo-porosis, further studies on the OPG/RANKL/RANK system inthe brain might shed light on the molecular mechanism involvedin postischemic inflammation and lead to the development ofnew therapeutic options for ischemic stroke.
Materials and MethodsSurgical Procedure. All procedures were approved by the Institutional AnimalCare and Use Committee of Osaka University. OPG−/− mice on C57Bl6/J back-ground and C57Bl6/J mice (wild-type) were obtained from CLEA Japan, Inc.
Transient Middle Cerebral Artery Occlusion. Mice were anesthetized with iso-flurane (1.4%). Cerebral blood flow was measured using a laser Dopplerflowmeter (Unique Acquisition software; UniqueMedical). A 6.0monofilamentsurgical suture was advanced into the internal carotid artery to obstruct theorigin of themiddle cerebral artery. The filament was left in place for 35, 45, or70 min and then withdrawn. Because the effect of deleting OPG was not clearin the first experiment, we chose 45 min of ischemia, which caused moderateischemia and was suitable for observing both deteriorating and improvingeffects. To examine the deteriorative effect of neutralizing anti-RANKL anti-body both in WT mice and OPG−/− mice, 45- and 35-min ischemic models wereapplied in OPG−/− and WT mice because the average infarct volume betweenOPG−/− and WT mice was almost the same in that ischemic duration. To assessthe therapeutic effect of RANKL, 70 min of ischemia to cause a severe infarctwas also applied. Only animals that exhibited a typical reduction pattern andmore than 82% reduction in CBF during MCAo, in which CBF recovered by 30–80% after 5 min of reperfusion, were included in the study. In all mice, rectaltemperature was kept at 37.0 ± 0.5 °C during surgery and in the recoveryperiod until animals regained consciousness. The overall mortality was 27% at72 h after ischemia.
Measurement of Infarction Volume. Ischemic damage was evaluated usingsections stained with cresyl violet at 72 h after MCAo. Coronal sections (12-μmthickness) were made at −1.4, −0.7, 0, 0.7, and 1.4 mm from the bregma,mounted on the stereomicroscope, and photographed. The hemisphericlesion area (HLA) in the coronal sections was calculated. The corrected HLAwas calculated as HLA (%) = [LT-(RT-RI)]/LT × 100, where LT is the area of theleft hemisphere, RT is the area of the right hemisphere, and RI is the infarctedarea (23). Brain edema was calculated as brain edema (%) = [RT-LT]/LT × 100.
Measurement of Body Temperature. In OPG−/− mice, body temperature wasmeasured by rectal probe thermometer (Unique Medical) without anesthe-sia. Core body temperature was continuously recorded using temperaturedata loggers (KN Laboratories) implanted into the peritoneal cavity. Thedata loggers were programmed to record body temperature every 3 minwith a resolution of 0.1 °C. Following the implant, animals were allowed 4 dto recover.
Fluorescein Angiography. The structure of cerebral vessels, capillary density,and blood–brain barrier leakage was assessed using an angiographic tech-nique with FITC-conjugated albumin (31). The depicted brain was fixed in4% (wt/vol) paraformaldehyde (PFA), and the image was acquired usinga fluorescence stereoscope (SZX 12, Olympus). The brains were frozen, cut into20-μm-long sections, and examined using a Nikon A1 confocal scanning lasermicroscope. The images were analyzed using NIS Elements software (Nikon).
Administration of Recombinant RANKL and RANK/Fc Chimera. Recombinantmouse RANKL [5 ng in 2 μL artificial cerebrospinal fluid (aCSF)] was purchasedfrom Peprotech EC. Recombinant mouse RANK/TNFRSF11a Fc Chimera(neutralizing anti-RANKL antibody, 4 μg in 2 μL aCSF) was obtained fromR&D Systems. Intracerebroventricle injection was performed using a pulledglass micropipette (anteroposterior 1.0 mm, lateral 1.2 mm from bregma,depth 1.7 mm). Recombinant RANKL was injected at 4, 24, and 48 h afterMCAo. Recombinant mouse RANK/TNFRSF11a Fc Chimera was intra-cerebroventricularly injected 2 h before MCAo. For the controls, BSA (NacalaiTesque) was used at the same concentration with each reagent. FITC- conju-gated albumin (10 μg/2 μl, Sigma-Aldrich) was intracerebroventricularly injec-ted at 4 or 24 h after MCAo to examine whether the injected proteins couldpenetrate the cortex in ischemic brain. The concentration of FITC-conjugatedalbumin was half that in the previous report examining the fluorescein angi-ography (31). At 2 h after injection, the fluorescence was observed around themicroglia in the ischemic cortex (Fig. S9).
Real-Time RT-PCR. The ischemic hemisphere was collected at 48 h after MCAoin OPG−/− mice. With the RANKL-treatment being 70-min ischemia in WTmice, the sample was collected at 24 h because the survival rate was low inmice at 48 h (Fig. S3B). The mRNAs were isolated using QIAGEN RNeasy LipidTissue Mini Kit (Qiagen), according to the manufacturer’s recommendations.The cDNA reaction was performed using a High-Capacity cDNA Archive kit(Applied Biosystems) according to the manufacturer’s instructions. The oli-gonucleotide primers used exclusively in the in vitro experiments werepurchased according to the identification RANK: Mm00437135; RANKL:Mm01313944; OPG: Mm00435451; MCP1: Mm00441243; IL-6: Mm00446190;Arg1: Mm00475988; iNOS: Mm00440502; IL-17a: Mm004329618; IL-10:Mm01288386; IL-1β: Mm99999061; and GAPDH: Mm99999915 (AppliedBiosystems). The 5′ nuclease assay PCRs were performed in a MicroAmpOptical 384-well reaction plate using ABI PRISM 7900 Sequence DetectionSystem. The levels of the target genes were quantified by comparing thefluorescence generated by each sample with that of the serially dilutedstandard, and the target gene expressions were normalized by the level ofGAPDH expression in each individual sample.
Cell Culture. Primary neuron-glial cultures were prepared from postnatal days1–2 in C57BL/6J mice using the method of Araki with some modifications(32). The entire cerebral cortex was dissected and minced in Neurobasal-A(Invitrogen) with B-27 supplement (Invitrogen, Neurobasal-A/B-27) afterremoving the meninx. Cells were treated with papain (25 U/mL) and DNaseI(25 U/mL) for 30 min at 30 °C. The cells were dissociated mechanically inNeurobasal-A/B-27 with 0.25 mM Glutamax (Invitrogen) and 10% horse serumby using a siliconized Pasteur pipette. Cells were plated on polyethyleneimine-coated 24-well plates at 7 × 105/well. Cultures were maintained at 37 °C in ahumidified atmosphere containing 5% CO2. Half of the medium was replacedwith Neurobasal-A/B-27 and 5% horse serum twice per week. After 9 d ofplating, the cells were composed of 42 ± 5% neurons, 56 ± 5% astrocytes, and2 ± 1% microglia. In the experiment on neural death, cells were treated withRANKL (100 ng/mL) for 24 h, and the medium was replaced with Neurobasal-A
Shimamura et al. PNAS | June 3, 2014 | vol. 111 | no. 22 | 8195
MED
ICALSC
IENCE
S

containing N2 supplement (Invitrogen, Neurobasa-A/N2), 1% horse serum, LPS(10 μg/mL), and RANKL (100 ng/mL). Cells were immunostained with MAP-2 todetermine the survival of the neurons at 5 d after the addition of LPS. Theimages were then digitized by microscope (FSX-100, Olympus). The acquiredimages were converted to grayscale with GIMP 2.8.6, and the stained area wascalculated using ImageJ (National Institutes of Health). In the experiment ex-amining the expression of TNFα or IL-6, the mediumwas collected at 24 h afterLPS stimulation. The concentration of these cytokines was checked usingcommercially available ELISA kits [TNFα: Quantikine Mouse TNF-α ELISA Kit(R&D systems); IL-6: Quantikine Mouse IL-6 ELISA Kit (R&D Systems)].
For the primary neuronal culture, mouse embryonic cerebral cortexneurons were obtained from pregnant C57BL/6J mice on the 18th day ofgestation and cultured (33). The cerebral cortex was dissected, and individualcells were isolated by treatment with papain and triturated in Leibovitz’sL-15 medium (Invitrogen). Cells were plated on polyethyleneimine-coated24-well plastic culture dishes with Neurobasal (Invitrogen)/B-27 (Invitrogen)with 0.25 nM Glutamax (Invitrogen) at 37 °C in a humidified atmosphere of95% air-5% CO2. The medium was changed on the fourth day. On day 9, themedium was changed to Neurobasal/N2 (Invitrogen) containing BSA orRANKL (10 or 100 ng/mL). Thereafter, CoCl2 (100 μM, 48 h), glutamate (100μM, 10 min), or H2O2 (100 μM, 24 h) was added to the medium. To check cellviability, cells were assessed using a 3-(4,5-dimethylthiazol-2-yl)-5-(3-car-boxymethoxyphenyl)-2-(4-sulfophenyl)-2H-tetrazolium (MTS) assay follow-ing the manufacturer’s protocol (CellTiter 96 AQueous One Solution CellProliferation Assay) at the following time points after the stimulation:CoCl2—48 h; H2O2—24 h; and glutamate—24 h.
Immunohistochemical Staining.Micewere perfusedwith 4%PFA, and the brainwas cut into 12-μm-thick sections. For double immunostaining, these sectionswere fixed and then blocked. The sections were incubated with anti-F4/80(1:50, AbD Serotec), anti-Iba1 (1:1,000, Wako), or anti-CD11b (1:100, AbDSerotec). Then, the sections were incubated with anti-rat fluorescent antibody
(1:500 for F4/80 and CD11b, Alexa Flour 546, Invitrogen) or anti-rabbit fluores-cent antibody (1:500 for Iba-1, Alexa Flour 546, Invitrogen). The sections wereblocked again and were incubated in streptavidin/biotin blocking kit (VectorLab, Vector Laboratories). Then they were incubated with anti-RANK antibody(1:13, R&D systems) or RANKL (1:50, eBioscience). As a negative control, thesame concentration of normal control IgG (Santa Cruz) was applied. Then theywere incubated in biotinylated anti-goat IgG antibody (1:200 for RANK; VectorLab) or anti-rat IgG antibody (1:200 for RANKL; Vector Lab) followed by fluo-rescent streptavidin conjugates (1:1,000, Alexa 488; Invitrogen). In the immu-nohistochemistry for OPG, the sections were blocked with 20% horse serum andthen incubated with streptavidin/biotin blocking kit (Vector Lab), followed byincubation with biotin affinity-purified polyclonal antibody for OPG (1:10, R&DSystems). Then the sections were incubated with fluorescent streptavidinconjugates (1:1,000, Alexa 488; Invitrogen).
Immunohistochemical staining was examined using Nikon A1 confocalscanning laser microscope, and the images were analyzed using NIS Elementssoftware (Nikon). All parameters were set in a similar manner when the signalintensity was compared.
Statistical Analysis. All values are expressed as the mean ± SEM. Multiplecomparisons were evaluated by ANOVA followed by Dunnett’s MultipleComparison Test. Two groups were compared using an unpaired t test.Survival rates were evaluated using a log-rank test. The core body temper-atures with data loggers were analyzed by a two-way repeated-measuresANOVA with Bonferroni posttests. Differences were considered significantat P < 0.05. The statistical analysis were performed with the software Prism5.0 (GraphPad Software).
ACKNOWLEDGMENTS. This work was supported by the grants from TheIchiro Kanehara Foundation (M.S.), the SENSHIN Medical Research Founda-tion (M.S.), and Japan Society for the Promotion of Science Grants-in-Aid forScientific Research (KAKENHI) Grant 25462214 (to M.S.).
1. Song T-J, et al. (2012) Association of plasma osteoprotegerin levels with stroke se-verity and functional outcome in acute ischaemic stroke patients. Biomarkers 17(8):738–744.
2. Üstünda�g M, et al. (2011) The role of serum osteoprotegerin and S-100 protein levelsin patients with acute ischaemic stroke: Determination of stroke subtype, severity andmortality. J Int Med Res 39(3):780–789.
3. Jensen JK, et al. (2010) Osteoprotegerin concentrations and prognosis in acute is-chaemic stroke. J Intern Med 267(4):410–417.
4. Simonet WS, et al. (1997) Osteoprotegerin: A novel secreted protein involved in theregulation of bone density. Cell 89(2):309–319.
5. Yasuda H, et al. (1998) Identity of osteoclastogenesis inhibitory factor (OCIF) andosteoprotegerin (OPG): A mechanism by which OPG/OCIF inhibits osteoclastogenesisin vitro. Endocrinology 139(3):1329–1337.
6. Ferrari-Lacraz S, Ferrari S (2011) Do RANKL inhibitors (denosumab) affect inflammationand immunity? Osteoporos Int 22(2):435–446.
7. Osako MK, et al. (2010) Estrogen inhibits vascular calcification via vascular RANKLsystem: Common mechanism of osteoporosis and vascular calcification. Circ Res107(4):466–475.
8. Tomimori Y, et al. (2009) Evaluation of pharmaceuticals with a novel 50-hour animalmodel of bone loss. J Bone Miner Res 24(7):1194–1205.
9. Crotti TN, et al. (2002) Receptor activator NF-kappaB ligand (RANKL) expression insynovial tissue from patients with rheumatoid arthritis, spondyloarthropathy, osteo-arthritis, and from normal patients: Semiquantitative and quantitative analysis. AnnRheum Dis 61(12):1047–1054.
10. Vernal R, et al. (2006) RANKL in human periapical granuloma: Possible involvement inperiapical bone destruction. Oral Dis 12(3):283–289.
11. Yamada N, et al. (2005) Down-regulation of osteoprotegerin production in bonemarrow macrophages by macrophage colony-stimulating factor. Cytokine 31(4):288–297.
12. To M, Ito K, Ausin PM, Kharitonov SA, Barnes PJ (2011) Osteoprotegerin in sputum isa potential biomarker in COPD. Chest 140(1):76–83.
13. Maruyama K, et al. (2006) Receptor activator of NF-kappa B ligand and osteoprote-gerin regulate proinflammatory cytokine production in mice. J Immunol 177(6):3799–3805.
14. Ohigashi I, Nitta T, Lkhagvasuren E, Yasuda H, Takahama Y (2011) Effects of RANKLon the thymic medulla. Eur J Immunol 41(7):1822–1827.
15. Loser K, et al. (2006) Epidermal RANKL controls regulatory T-cell numbers via acti-vation of dendritic cells. Nat Med 12(12):1372–1379.
16. Zhang P, et al. (2011) TLR2-dependent modulation of osteoclastogenesis by Por-phyromonas gingivalis through differential induction of NFATc1 and NF-kappaB.J Biol Chem 286(27):24159–24169.
17. Lambertsen KL, Biber K, Finsen B (2012) Inflammatory cytokines in experimental andhuman stroke. J Cereb Blood Flow Metab 32(9):1677–1698.
18. Kartsogiannis V, et al. (1999) Localization of RANKL (receptor activator of NF kappa Bligand) mRNA and protein in skeletal and extraskeletal tissues. Bone 25(5):525–534.
19. Nakagawa N, et al. (1998) RANK is the essential signaling receptor for osteoclastdifferentiation factor in osteoclastogenesis. Biochem Biophys Res Commun 253(2):395–400.
20. Hanada R, et al. (2009) Central control of fever and female body temperature byRANKL/RANK. Nature 462(7272):505–509.
21. Osako MK, et al. (2013) Cross-talk of receptor activator of nuclear factor-κB ligandsignaling with renin-angiotensin system in vascular calcification. Arterioscler ThrombVasc Biol 33(6):1287–1296.
22. Shichita T, Sakaguchi R, Suzuki M, Yoshimura A (2012) Post-ischemic inflammation inthe brain. Front Immunol 3:132.
23. Abe T, et al. (2010) Key role of CD36 in Toll-like receptor 2 signaling in cerebral is-chemia. Stroke 41(5):898–904.
24. Lehnardt S, et al. (2003) Activation of innate immunity in the CNS triggers neuro-degeneration through a Toll-like receptor 4-dependent pathway. Proc Natl Acad SciUSA 100(14):8514–8519.
25. Buchanan MM, Hutchinson M, Watkins LR, Yin H (2010) Toll-like receptor 4 in CNSpathologies. J Neurochem 114(1):13–27.
26. Udagawa N, et al. (2000) Osteoprotegerin produced by osteoblasts is an importantregulator in osteoclast development and function. Endocrinology 141(9):3478–3484.
27. Lerner UH (2004) New molecules in the tumor necrosis factor ligand and receptorsuperfamilies with importance for physiological and pathological bone resorption.Crit Rev Oral Biol Med 15(2):64–81.
28. Liang Q-Q, et al. (2011) The expression of osteoprotegerin is required for maintainingthe intervertebral disc endplate of aged mice. Bone 48(6):1362–1369.
29. Gelderblom M, et al. (2009) Temporal and spatial dynamics of cerebral immune cellaccumulation in stroke. Stroke 40(5):1849–1857.
30. Liesz A, et al. (2009) Regulatory T cells are key cerebroprotective immunomodulatorsin acute experimental stroke. Nat Med 15(2):192–199.
31. Cavaglia M, et al. (2001) Regional variation in brain capillary density and vascularresponse to ischemia. Brain Res 910(1-2):81–93.
32. Araki E, Forster C, Dubinsky JM, Ross ME, Iadecola C (2001) Cyclooxygenase-2 inhibitorns-398 protects neuronal cultures from lipopolysaccharide-induced neurotoxicity.Stroke 32(10):2370–2375.
33. Brewer GJ, Torricelli JR, Evege EK, Price PJ (1993) Optimized survival of hippocampalneurons in B27-supplemented Neurobasal, a new serum-free medium combination.J Neurosci Res 35(5):567–576.
8196 | www.pnas.org/cgi/doi/10.1073/pnas.1400544111 Shimamura et al.








![CANNABINOID-LIKE ANTI-INFLAMMATORY COMPOUNDS …signaling pathway that inhibits pro-inflammatory and increases anti-inflammatory gene expression [18-20]. ... chromatograph with a PDA](https://img.dokumen.tips/doc/110x75/609561177fd04d6d4c1f28b1/cannabinoid-like-anti-inflammatory-compounds-signaling-pathway-that-inhibits-pro-inflammatory.jpg)

![ASK1/p38-mediated NLRP3 inflammasome signaling pathway … · 49 with diabetes [5]. Therefore, the inhibition of inflammatory signaling can become a 50 treatment for DR therapy. 51](https://img.dokumen.tips/doc/110x75/5f245fa10874dd37252a09e5/ask1p38-mediated-nlrp3-inflammasome-signaling-pathway-49-with-diabetes-5-therefore.jpg)






![RESEARCH ARTICLE Open Access Molecular Signaling Pathways … · 2017. 8. 26. · RANKL does not completely block tumor development and progression in bone tissue [25]. These findings](https://img.dokumen.tips/doc/110x75/60af630a23ae3b4c2a18759d/research-article-open-access-molecular-signaling-pathways-2017-8-26-rankl-does.jpg)











