Embed Size (px)
Citation preview

lable at ScienceDirect
The Journal of Foot & Ankle Surgery 49 (2010) 25–32
Contents lists avai
The Journal of Foot & Ankle Surgery
journal homepage: www.j fas .org
Operative versus Nonoperative Treatment of Displaced Intra-articular CalcanealFractures in Elderly Patients
Attilio Basile, MD 1
1 Orthopaedic Trauma Surgeon, Department of Orthopaedics and Traumatology, Ospedale San Giovanni-Addolorata Roma (Italia), Rome, Italy
a r t i c l e i n f o
Level of Clinical Evidence: 2Keywords:calcaneusposttraumatic arthrosis
subtalar jointsurgerytraumaFinancial Disclosure: None reported.Conflict of Interest: None reported.Address correspondence to Attilio Basile, MD, D
Traumatology, Ospedale San Giovanni-Addolorata Ro00149 Roma, Italy.
E-mail address: [email protected]
1067-2516/$ – see front matter � 2010 by the Ameridoi:10.1053/j.jfas.2009.08.001
a b s t r a c t
We compared the outcomes of displaced intra-articular calcaneal fractures in 33 patients aged 65 to 75 years,who were treated either operatively (n ¼ 18) or nonsurgically (n ¼ 15), between December 2001 andDecember 2005. The operative treatment group scored higher on the American Orthopaedic Foot & AnkleSociety ankle-hindfoot score and had less pain as measured with the 10-cm visual analog scale than did thenonsurgically treated group, with the differences being statistically significant (P � .05), suggesting thatresults can be improved by operative treatment. Bohler’s angle, the quality of operative reduction, subtalarjoint motion, gender, and the Sanders type of fracture were also analyzed and compared between thetreatment groups. The results confirmed that Bohler’s angle, the quality of the reduction, and subtalar jointmotion were important prognostic factors related to outcome, regardless of treatment; whereas gender andSanders type had less influence on the results at the 2-year follow-up evaluation. The prevalence ofcomplications observed in the surgically treated group was similar to that reported in prior publications,except for subtalar arthritis (38.9%), which may have been higher because of the age of our patients and theduration of follow-up.
� 2010 by the American College of Foot and Ankle Surgeons. Published by Elsevier Inc. All rights reserved.
Historically, displaced intra-articular calcaneal fractures have beentreated nonsurgically, before the development of open reduction andfixation methods that yield predictable results (1–3). Operativetreatment has become more accepted in the past 10 to 15 years, asa result of improvements in preoperative evaluation, the use ofintraoperative imaging to verify the quality of reduction, andadvancements in surgical techniques that include specialized hard-ware and soft tissue management (4). The goals of operative inter-vention are anatomical reduction of the joint surfaces, andreestablishment of the hindfoot and gastrocnemius-soleus biome-chanics (5). Reconstruction of the joint surfaces and restoration of theoriginal bone alignment should enable the patient to have the bestchance for resumption of preinjury function, regardless of the degreeof cartilage injury produced by the trauma.
It is also interesting to note that literature supports the recom-mendation to avoid surgery in all patients older than 50 because ofthe expectation of poor outcomes (4, 6, 7). Recently, an investigationperformed by Herscovici et al (8) challenged this philosophy, and
epartment of Orthopaedics andma (Italia), Via Nicola Pellati 45,
can College of Foot and Ankle Surgeo
showed that open reduction and internal fixation (ORIF) appeared tobe an acceptable method of treatment for displaced intra-articularcalcaneal fractures in a carefully selected population of elderlypatients. The weaknesses of that study were its retrospective natureand the lack of a control group for comparison of outcomes.
The purpose of our investigation was to review and compare theoutcomes of displaced intra-articular calcaneal fractures in a group ofpatients aged 65 to 75 years who were treated operatively and non-surgically. To the best of our knowledge this is the first article in whichsuch a comparison has been undertaken. Our hypothesis was thatORIF of displaced intra-articular calcaneal fractures in healthy andactive elderly patients would result in better outcomes in comparisonwith nonoperative treatment.
Patients and Methods
We performed a multicenter retrospective investigation of patients aged 65 to 75years who had sustained a displaced intra-articular calcaneal fracture that was treatedeither by means of ORIF or nonoperative care between December 2001 and December2005. Protocols were different between the 2 hospitals involved in the study in thesense that in one center all the displaced intra-articular calcaneal fractures in patientsolder than 65 years were treated without surgery, whereas in the other hospital, dis-placed intra-articular fractures in elderly patients were treated operatively if specificcriteria were identified. Institutional review board approval was obtained for the study,and all the patients also provided informed consent to the research project. Thecalcaneal fractures were categorized according to the Sanders classification system (9),
ns. Published by Elsevier Inc. All rights reserved.
Table 1Results for operative treatment group at 2 years postoperative (n ¼ 18)
Patient Age Sex Class* Bohler’s angle (�) Quality of Reduction Subtalar Joint Motion (�) Score
Uninjured Injured Uninjured Injured AOFAS VAS
Pronate Supinate Total Pronate Supinate Total
1 69 M II 25 25 Anatomic 10 18 28 4 14 18 85 252 65 F II 34 34 Anatomic 7 20 27 5 16 21 92 123 71 F II 40 40 Anatomic 5 16 21 5 10 15 96 64 73 M II 32 28 Nearly 8 17 25 5 10 15 81 225 69 F II 30 30 Anatomic 12 20 32 12 20 32 100 06 74 F II 45 45 Anatomic 5 19 24 5 15 20 93 187 65 M II 24 24 Nearly 10 18 28 5 10 15 82 218 65 M III 42 47 Nearly 9 18 27 0 8 8 55 879 68 M III 36 32 Nearly 7 15 22 3 8 11 77 31
10 67 M III 28 28 Anatomic 8 16 24 5 12 17 93 1111 70 F III 33 33 Anatomic 11 22 33 5 16 21 87 1812 68 M III 44 44 Anatomic 5 16 21 5 10 15 90 1313 73 M III 45 45 Anatomic 3 14 17 0 10 10 87 2114 66 F III 36 36 Anatomic 10 18 28 5 12 17 89 2315 69 F III 42 39 Nearly 7 19 26 3 10 13 79 3016 75 M III 28 28 Anatomic 6 18 24 4 15 19 91 1117 68 F III 33 33 Anatomic 8 17 25 8 17 25 95 718 66 M III 40 40 Anatomic 11 19 30 5 10 15 80 22
M, male; F, female; Nearly, nearly anatomic; AOFAS, American Orthopaedic Foot & Ankle Society hindfoot-ankle score; VAS, visual analog scale for subjective pain assessment (0¼ nopain, 100 ¼ the worst pain).
* Sanders classification.
A. Basile / The Journal of Foot & Ankle Surgery 49 (2010) 25–3226
and the operating surgeons performed the preoperative and postoperative clinical andradiographic assessments.
Entry criteria for all patients enrolled in the trial were patients (1) aged 65 to 75years affected by isolated intra-articular calcaneal fractures that were displaced morethan 2 mm from anatomical position as demonstrated by axial and coronal computedtomography (CT) scan of the posterior facet (excluding Sanders type IV and openfractures) and with a Bohler’s angle of less than 15� (measured on the lateral plain filmat admission); (2) with no prior involvement of ipsilateral foot and/or ankle surgery,fracture, symptomatic osteoarthritis, or inflammatory arthritis; (3) with no majorunderlying medical comorbidity, such as uncontrolled hypertension, previousmyocardial infarction, cancer, history of stroke or transient ischemic attacks, chronicobstructive lung disease, cardiac arrhythmia, morbid obesity, diabetes mellitus,peripheral vascular disease, or peripheral neuropathy; (4) who were nonsmokers; (5)who, at the time of the injury, either had a full-time occupation (working at least 38hours per week) or participated in moderate to strenuous recreational activities(walking, jogging, golfing, tennis, bowling, weightlifting, bicycling, and/or otherstrenuous activities); (6) with a minimum follow-up of 2 years; and (7) who had noinvolvement in a Workers’ Compensation claim.
Patients who were treated without surgery had no attempt at closed reduction ofthe displaced intra-articular calcaneal fracture and were treated with ice, elevation and
Table 2Results for nonoperative treatment group at 2 years postoperative (n ¼ 15)
Patient Age Sex Class* Bohler’s Angle (�) Quality of Reduction
Uninjured Injured
1 66 M II 36 15 Unreduced2 69 M II 28 10 Unreduced3 65 M II 38 5 Unreduced4 72 F II 30 11 Unreduced5 67 M II 42 7 Unreduced6 65 F II 33 9 Unreduced7 65 F II 25 10 Unreduced8 75 M III 28 13 Unreduced9 69 F III 45 0 Unreduced
10 67 M III 39 �4 Unreduced11 73 F III 35 0 Unreduced12 65 M III 36 0 Unreduced13 68 F III 30 13 Unreduced14 70 M III 41 6 Unreduced15 66 F III 32 4 Unreduced
M, male; F, female; AOFAS, American Orthopaedic Foot & Ankle Society hindfoot-ankle scorepain).
* Sanders classification.
rest, non–weight bearing, and gradual rehabilitation. Patients who were treatedoperatively underwent open reduction and internal fixation with plate and screws,after the soft tissue envelope was determined to be stable. An extensile lateral approachwas used to gain access to the target structures, and the reduction and fixation tech-niques were those popularized by Benirschke and Sangeorzan (10, 11). The use of a bonegraft, either autograft or allograft, was left to the discretion of the operating surgeon.Postoperatively, a short-leg splint was applied for 3 weeks for soft tissue protection,after which the skin sutures were removed and the patient started on a regimen ofphysical therapy. For patients in the nonoperative group, the short-leg splint was usedfor the first 3 weeks, after which physiotherapy was initiated. Physical therapy includedcompression for control of swelling, range of motion exercises for the ankle and sub-talar joints, progressive partial weight bearing, and gait training. Full weight bearingwas allowed at 12 weeks following operation or the date of the fracture in those treatednonsurgically.
Objective and subjective data for the 2 treatment groups were analyzed andcompared at the 2-year follow-up end point. Follow-up radiographic assessmentconsisted of serial radiographs and CT scans. Specific radiograph views included thelateral and 30� Broden and Harris projections, which were taken at 6 and 12 weeks andat 1 and 2 years postoperative, or after the injury in the nonsurgical group. CT scanswere obtained using 3-mm cuts in 3 planes, and were obtained in the immediate
Subtalar Joint Motion (�) Score
Uninjured Injured AOFAS VAS
Pronate Supinate Total Pronate Supinate Total
8 16 24 0 4 4 56 7910 18 28 3 7 10 67 58
7 18 25 2 10 12 65 525 14 19 0 8 8 86 27
10 20 30 6 16 22 75 227 16 23 5 10 15 88 199 17 26 5 15 20 90 75 15 20 2 7 9 69 457 18 25 0 0 0 55 78
10 18 28 0 0 0 51 7712 20 32 0 0 0 59 75
4 14 18 0 9 9 73 3413 21 34 7 11 18 82 1511 18 29 5 9 14 70 33
9 17 26 0 8 8 68 40
; VAS, visual analog scale for subjective pain assessment (0 ¼ no pain, 100 ¼ the worst

Table 3Comparison of demographic and outcome variables between treatment groups (N ¼ 33)
Variable Operative (n ¼ 18) Nonoperative (n ¼ 15) P value*
Age, y 68.94 � 3.17 68.13 � 3.18 .4706Male sex, count (%) 10 (55.56) 8 (53.33) .9Sanders type III calcaneal fracture, count (%) 11 (61.11) 7 (38.89) .6576Bohler’s angle (�) at long-term follow-up
Uninjured 35.39 � 6.82 34.53 � 5.79 .7073Injured 35.06 � 7.29 6.6 � 5.69 < .0001
Subtalar joint motion (�) at long-term follow upUninjured
Pronation 7.89 � 2.49 8.47 � 2.64 .5237Supination 17.78 � 1.96 17.33 � 2.09 .5337Total 25.67 � 4.02 25.8 � 4.6 .9297
InjuredPronation 4.67 � 2.61 2.33 � 2.61 .0157Supination 12.39 � 3.43 7.6 � 4.93 .0026Total 17.06 � 5.62 9.93 � 7.07 .003
Reduction anatomical at long-term follow-up, count (%) 13 (72.22) 0 .0001AOFAS score at long-term follow up 86.22 � 10.09 70.26 � 12.24 .0003100-mm VAS score at long-term follow-up 21.0 � 18.44 44.06 � 24.69 .0044
AOFAS, American Orthopaedic Foot & Ankle Society hindfoot-ankle score; VAS, visual analog scale for subjective pain assessment (0 ¼ no pain, 100 ¼ the worst pain).* Unpaired Student t test for continuous numeric data, or Wilcoxon rank sum (Mann Whitney U) test for categorical data.
A. Basile / The Journal of Foot & Ankle Surgery 49 (2010) 25–32 27
postoperative period as well as at 6 months and 2 years after the surgery, or after theinjury in the nonsurgical group. The American Orthopaedic Foot and Ankle Society(AOFAS) ankle-hindfoot score (12) and the visual analog scale (VAS) (13) were used asa quantification of the clinical and subjective evaluations. The AOFAS ankle-hindfootscore is widely used to assess patient outcomes, while the VAS scoring system had beenvalidated in several trials to determine functional results in patients with displacedintra-articular calcaneal fractures (13–16). Use of the 10-cm VAS involved having thepatient mark the horizontal line at a point on or between the anchors, with 0 mmindicative of no pain, and 100 mm indicative of very severe pain. The score wasdetermined by measuring, in millimeters, the distance from the left-hand end (no pain)of the horizontal line to the point marked by the patient. Pain, as measured by the10-cm VAS, as well as AOFAS scores, was obtained at the 2-year follow-up visit.
A number of other demographic variables, including Bohler’s angle, subtalardegenerative changes, the quality of the fracture reduction, subtalar joint motion,Sanders classification (9), gender, and complications, were analyzed and comparedbetween the 2 treatment groups. Bohler’s angle was measured with a hand-heldgoniometer placed over the lateral plain film radiograph, and values for this angle wereobtained at the time of the patient’s initial presentation and at subsequent follow-upvisits, and these were compared to the same angle as measured in the uninjured foot.This method of measurement of Bohler’s angle has previously been show to providevalid results (4, 17–19). Subtalar arthrosis was graded as mild (diminished joint space),moderate (diminished joint space and subchondral sclerosis), or severe (markedlydiminished or no joint space) (19). Posterior facet joint congruency was used to cate-gorize the quality of the fracture reduction, in accordance with the method describedby Janzen (20). The quality of the reduction was categorized as anatomical, nearlyanatomical (joint surface step-off< 2 mm), or nonanatomical (joint surface step-off> 2mm). Hindfoot alignment was categorized as either varus, valgus, or neutral, based onthe orientation of the long axis of the calcaneus relative to the long axis of the leg.Subtalar joint motion was measured using the method described by Morrey andWiedeman (17), which has also been used by other investigators (8, 20). Passiveinversion and eversion of the calcaneus were evaluated with the patient supine and theankle in neutral position, and subtalar joint motion of the injured foot was recorded andcompared with the motion of the uninjured foot. Complications were categorized asminor or major. Minor complications were defined as those that could be managednonsurgically, and major complications were those that required surgical interventionfor resolution. Preoperative and postoperative x-ray and CT images, as well as theAOFAS and VAS scores, were reviewed and recorded by surgeons not involved in anyway with the treatment of any of the patients. Student t test was used to compare theresults between patient groups for continuous numeric data, and the Wilcoxon ranksum (Mann Whitney U) test was used to compare categorical data, and statisticalsignificance was defined at the 5% (P � .05) level.
Table 4Comparison of AOFAS and VAS scores between operative treatment subgroups based on re
Variable Anatomical (n ¼ 13)
AOFAS score 90.6 � 5.18VAS score 14.38 � 7.51
AOFAS, American Orthopaedic Foot & Ankle Society hindfoot-ankle score; VAS, visual analo* Unpaired Student t test.
Results
Based on our inclusion criteria, 33 patients were available for theanalyses used in this retrospective cohort study, and 18 (54.6%) ofthese underwent surgical repair of their calcaneal fracture, whereas15 (45.5%) were treated nonsurgically. Results for the treatmentgroups at the 2-year follow-up evaluation are summarized in Tables 1and 2, and Table 3 depicts statistical comparisons for the demographicand outcome variables between the treatment groups. The mean agefor the patients in the operative treatment group was 68.94 � 3.17years, whereas that for those in the nonsurgical treatment group was68.13 � 3.18 years; this difference was not statistically significant (P ¼.4706). There were 10 (55.6%) males in the operatively treated group,and 8 (53.3%) males in the nonsurgically treated group; this differencewas not statistically significant (P ¼ .9). There were 11 (61.1%) Sanderstype III joint depression fractures in the operatively treated group, and7 (38.9%) in the nonsurgically treated group; this difference was notstatistically significant (P ¼ .6576). All of the remaining calcanealfractures, in both groups, were categorized as Sanders type II. Subtalarjoint motion, including the range of pronation, supination, and thetotal range of motion, was not statistically significantly differentbetween the treatment groups for the uninjured extremity; however,on the injured side, statistically significantly greater range of motionwas observed in the group that underwent surgical repair (Table 3).Additional results (not shown in the tables) showed the mechanism ofinjury to have been a fall or jump from a height in 22 (66.7%) cases anda motor vehicle accident in 11 (33.3%) cases, and the preoperativeBohler’s angle of the injured foot was not statistically significantlydifferent between the treatment groups (results not shown). For thosewho underwent surgical repair, the mean duration of time betweenthe injury and the operation was 16.2 � 4.5 (range 9 to 25) days.
Patients in the operative treatment group (n ¼ 18) scored higher,indicative of better function and patient satisfaction, on the AOFASscale, and lower, indicative of less pain, on the VAS, in comparison
duction of the subtalar joint (n ¼ 18)
Nearly anatomical (n ¼ 5) P value*
74.8 � 11.23 .002638.2 � 27.65 .0089
g scale for subjective pain assessment (0 ¼ no pain, 100 ¼ the worst pain).

Table 5Comparison of AOFAS and VAS scores between nearly anatomical operative and nonoperative treatment groups (n ¼ 20)
Variable Nearly anatomical (n ¼ 5) Nonoperative (n ¼ 15) P value*
AOFAS score 74.8 � 11.2 70.26 � 12.24 .4748VAS score 38.2 � 27.6 44.06 � 24.69 .6598
AOFAS, American Orthopaedic Foot & Ankle Society hindfoot-ankle score; VAS, visual analog scale for subjective pain assessment (0 ¼ no pain, 100 ¼ the worst pain).* Unpaired Student t test.
A. Basile / The Journal of Foot & Ankle Surgery 49 (2010) 25–3228
with patients in the nonoperative group; these differences werestatistically significant (P ¼ .0003 and P ¼ .044, respectively)(Table 3). All of the patients in the operative group displayed satis-factory restoration of Bohler’s angle and subtalar joint congruity,whereas no improvement of this angle or joint congruity occurred inthe nonoperative group. In the operative treatment group, 4 (22.2%)patients displayed radiographic signs of mild, 2 (11.1%) moderate, and1 (5.6%) severe, subtalar joint arthritis; making the prevalence ofsubtalar arthritis 38.9% (7 cases in 18 patients). The 1 (5.6%) case withsevere degenerative joint changes was treated with a fusion for painmanagement at 18 months following the surgery for repair of thefracture. One (5.6%) of the cases with moderate arthritis was symp-tomatic in the sense that he stated that pain severely limited his dailyand recreational activities and, despite these complaints, he refusedto undergo arthrodesis and, instead, settled for partial relief withshoe modification. Four (22.2%) of the remaining 5 cases stated thatthey were only occasionally symptomatic. One (5.6%) patientrequired shoe modification for painless ambulation. None of theoperatively treated patients required surgery for malunion ornonunion.
In the nonoperative group (n ¼ 15), all of the patients experiencedsymptomatic subtalar arthritis, with 4 (26.7%) patients considered tosuffer moderate symptoms and 11 (73.3%) considered to suffer severesymptoms. Eight (53.3%) of these patients required hindfoot realign-ment by means of subtalar arthrodesis in conjunction with lateral wallexostectomy, peroneal tendon debridement, and/or osteotomy of theposterior calcaneal tuberosity. Five (33.3%) of these patients requiredthe use of a custom-made orthosis and/or shoe modifications to effectsatisfactory ambulation.
A number of specific subgroup analyses were also undertaken. Inthe surgically treated group, statistically significant improvementswere observed for AOFAS and VAS scores when those patients withradiographic evidence of anatomical reduction of the subtalar jointwere compared with those with nearly anatomical reduction (P ¼.0026 and .0089, respectively) (Table 4). Furthermore, AOFAS and VASoutcomes for surgically treated patients who had even a smallresidual step defect (nearly anatomical reduction) in the subtalar jointwere not statistically significantly better than those for the non-surgically treated patients (P ¼ .4748 and .6598, respectively) (Table5). In regard to gender, in the operatively treated group, femalesscored higher (91.75 � 6.56) than did males (82.10 � 10.84) on theAOFAS scale at the 2-year follow-up visit, and this difference wasstatistically significant (P ¼ .0491). No statistically significant differ-ences were observed for the AOFAS score between males and femalesin the nonsurgically treated group, and sex did not effect a statisticallysignificantly difference in the 100-mm pain VAS in either treatmentgroup (Table 6).
Table 6Comparison of AOFAS and VAS scores between male and female patients by treatment grou
Variable Operative (n ¼ 18) P v
Female (n ¼ 8) Male (n ¼ 10)
AOFAS score 91.75 � 6.56 82.10 � 10.84 .04VAS score 14.25 � 9.86 26.4 � 22.22 .17
AOFAS, American Orthopaedic Foot & Ankle Society hindfoot-ankle score; VAS, visual analo* Unpaired Student t test.
In regard to complications, there were 5 complications (27.7%) inthe operative group, 2 minor (11.1%) and 3 major (16.6%). The minorcomplications entailed a case of wound edge necrosis that wassuccessfully managed with local wound care, and a case that requiredshoe modification for painless ambulation. The 3 major complicationsconsisted of a case of partial wound breakdown with bone andhardware exposure that was successfully treated with a local fas-ciocutaneous flap, and 2 cases of painful subtalar joint arthritis forwhich we recommended subtalar joint fusion. In the group treatednonsurgically, we observed 13 complications (86.6%), 5 minor (33.3%)and 8 major (53.3%). Five of these patients required a custom-madefoot orthosis and/or shoe modifications to achieve painless ambula-tion, and 8 subtalar joint fusions, often in conjunction with adjunctprocedures about the hindfoot, were undertaken to relieve pain andto realign and stabilize deformity and joint degeneration.
We also undertook nonparametric correlation analyses in an effortto better understand the association of the risk factors with the AOFASand VAS scores; these results are depicted in Table 7. The followingvalues for Spearman’s rho were observed for the AOFAS and VAS scores,respectively: (1) injured side 2-years postoperative Bohler’s angle(r¼0.5544 [P¼ .0008] and r¼–0.4533 [P¼ .0081]) (Figure 1 and 2), (2)injured side 2-years postoperative range of subtalar pronation(r¼ 0.6866 [P< .0001] and r¼ –0.7818 [P< 0.0001]) (Figures 3 and 4),(3) injured side 2-years postoperative range of subtalar supination(r¼ 0.7958 [P< .0001] and r¼ –0.8284 [P< .0001]) (Figures 5 and 6),(4) total range of injured side 2-years postoperative subtalar range ofmotion (r¼ 0.7858 [P< .0001] and r¼ –0.8387 [P< .0001]) (Figures 7and 8), and (5) reduction (congruency) of the subtalar joint (r¼ 0.7194[P < .0001] and r ¼ –0.6246 [P ¼ .0001]) (Figures 9 and 10).
Discussion
Controversy exists as to which is the best treatment for displacedintra-articular calcaneal fractures. A number of retrospective and fewsmall prospective studies reported better results with operativetreatment than with nonsurgical management (20–23). The meta-analysis of Randle et al. (21) reported a trend for a better outcomefrom surgical treatment of calcaneal fractures, but the authorsstressed their concerns for the weakness of their evidence fordeciding on the optimal management of this type of fracture. In regardto randomized controlled trials (RCTs) comparing operative versusnonoperative treatment of joint depression calcaneal fractures (17,24), no statistically significant differences in functional resultsbetween the two groups were identified, although the patients thatwere treated surgically were more likely to develop clinically signif-icant complications (7). Buckley et al (4), in a large prospectiverandomized controlled multicenter trial, one in which the analyses
p (N ¼ 33)
alue Nonoperative (n ¼ 15) P value*
Female Male
91 70.28 � 9.19 70.25 � 15.07 .130917 42.71 � 20.22 44.75 � 28.78 .3382
g scale for subjective pain assessment (0 ¼ no pain, 100 ¼ the worst pain).

Table 7Spearman’s correlation coefficient and probabilities
Variable Score Spearman’s rho (r)* P value
Injured side Bohler’s angle at 2-year follow-up AOFAS 0.5544 .0008VAS �0.4533 .0081
Injured side range of subtalar pronation at 2-year follow-up AOFAS 0.6866 < .0001VAS �0.7818 < .0001
Injured side range of subtalar supination at 2-year follow-up AOFAS 0.7958 < .0001VAS �0.8284 < .0001
Injured side total subtalar range of motion at 2-year follow-up AOFAS 0.7858 < .0001VAS �0.8387 < .0001
Anatomical reduction of the subtalar joint AOFAS 0.7194 <.0001VAS �0.6246 .0001
AOFAS, American Orthopaedic Foot & Ankle Society hindfoot-ankle score; VAS, visual analog scale for subjective pain assessment (0 ¼ no pain, 100 ¼ the worst pain); since a lowerscore on the VAS was indicative of less pain, a negative correlation coefficient was indicative of a better outcome.
A. Basile / The Journal of Foot & Ankle Surgery 49 (2010) 25–32 29
involved stratification of the patients based on risk factors, demon-strated that women, patients who were not receiving Workers’Compensation, younger males, patients with a higher Bohler’s angle,patients with a lighter workload, and those with a single simpledisplaced intra-articular fracture had better results after operativetreatment in comparison with those who did not undergo openreduction and internal fixation. They also stated that anatomical ornearly anatomical reductions enhanced outcomes, whereas commi-nution and/or poor reductions produced long-term outcomes thatwere less satisfactory, and that arthrodesis rates were significantlyreduced with operative treatment. Furthermore, they pointed out thatpatients who benefited from nonoperative treatment were those 50years or older, receiving Workers’ Compensation benefits for theinjury, and those with highly comminuted articular fractures.
Our review of existing biomedical literature suggested that theresults of the treatment of joint depression calcaneal fractures doesnot just depend on the specific type of fracture, rather, a variety ofother patient characteristics substantially influence the outcome (4, 7,17, 20–24). In our study, we compared the outcomes in patients aged65 to 75 years without major medical comorbidities, who weretreated operatively and nonsurgically for displaced intra-articularcalcaneal fractures. Our hypothesis was that ORIF of displaced intra-articular calcaneal fractures in healthy and active elderly patientswould result in better outcomes compared with nonsurgical treat-ment. After considering the results of our investigation, we believethat this hypothesis was confirmed. The operative treatment groupscored higher on the AOFAS hindfoot and ankle score and the 100-mm
Fig. 1. Correlation of American Orthopaedic Foot and Ankle Society hindfoot-ankle scorewith Bohler’s angle at 2-year follow-up.Spearman’s correlation coefficient, r ¼ 0.5544.
VAS pain score, when compared with patients in the nonsurgicalgroup. These findings suggest that the outcomes of treatment ofdisplaced, joint depression calcaneal fractures can be improved bymeans of operative intervention.
In regard to other variables that have previously been shown to bestatistically significantly associated with prognosis in regard to thesefractures, Bohler’s angle, quality of subtalar reduction, subtalar jointdegeneration, subtalar joint motion, and gender were analyzed andcompared between groups (4, 18, 23). Because the validity of some ofthese outcome measurements has been questioned in the past (17, 18,25), we felt that it was important to undertake a number of subgroupanalyses to further characterize the influence of these variables on theoutcome. Evidence exists in the literature to support the concept thatrestoration of Bohler’s angle and the quality of subtalar joint reduc-tion predict outcome in the treatment of displaced intra-articularcalcaneal fracture, regardless of the type of treatment received (4, 18,24) and, based on our results, we agree with this supposition. In fact,in our cohort, patients with restoration of the Bohler angle to itsoriginal value and with anatomical reconstruction of the subtalar jointsurface experienced statistically significantly better outcome AOFASand VAS scores, regardless of treatment. This was made clear by thefact that, among patients in the operative group, we detected betteroutcome AOFAS and VAS scores for cases wherein Bohler’s angle andsubtalar congruency were anatomically restored, in comparison withcases wherein these surgical parameters were not restored to theiranatomical alignment, and this difference was statistically significant(P ¼ .0026 and P ¼ .0089, respectively, for the AOFAS and VAS scores)
Fig. 2. Correlation of 100-mm visual analog scale (VAS) pain score with Bohler’s angle at2-year follow-up.Spearman’s correlation coefficient, r ¼ �0.4533.

Fig. 3. Correlation of American Orthopaedic Foot and Ankle Society hindfoot-ankle scorewith range of subtalar joint pronation at 2-year follow-up.Spearman’s correlation coef-ficient, r ¼ 0.6866.
Fig. 5. Correlation of American Orthopaedic Foot and Ankle Society hindfoot-ankle scorewith range of subtalar joint supination at 2-year follow-up.Spearman’s correlation coef-ficient, r ¼ 0.7958.
A. Basile / The Journal of Foot & Ankle Surgery 49 (2010) 25–3230
(Table 4). Although the correlation between restoration of Bohler’sangle and the AOFAS score was weakly positively correlated, thisassociation was highly statistically significant (Table 7, Figure 1). And,although the correlation between restoration of Bohler’s angle andthe VAS score was even weaker, it was negative and indicated thata more normal angle correlated with less pain at the 2-year post-operative examination, and this association was also highly statisti-cally significant (Table 7, Figure 2).
Because even a small residual posterior facet step defect resultedin a statistically significant decrease in outcome scores, in comparisonwith an anatomically reduced fracture, and no statistically significantdifference was noted between near anatomically reduced surgicallytreated and nonsurgically treated fractures (Tables 4 and 5), ourresults strongly suggest that a more anatomical reduction providesa better outcome following joint depression calcaneal fracture inelderly patients.
Subtalar joint motion has also been considered an importantoutcome measurement in previously published studies concernedwith displaced intra-articular calcaneal fractures (26–30), although
Fig. 4. Correlation of 100-mm visual analog scale (VAS) pain score with subtalar jointpronation at 2-year follow-up.Spearman’s correlation coefficient, r ¼ �0.7818.
the conclusions drawn from these studies have been questionedbased on the suspected lack of reliability of the measurements ofsubtalar joint motion (31–33). To minimize error related to themeasurement of subtalar motion, some authors have advocated thatthese measurements be reported as a percentage of normal (26).Nonetheless, there is no clear consensus in the literature as towhether or not it is worthwhile to consider subtalar joint motion asa prognostic factor for outcome following displaced intra-articularcalcaneal fracture. It has also been argued that subtalar joint stiffnessdoes not necessarily correlate with posttraumatic disability (3, 24, 34,35). In contrast, an association has been demonstrated betweensubtalar joint motion and overall outcome (24, 36, 37). In our inves-tigation, we found a statistically significant difference in subtalarmotion between operatively and nonoperatively treated patients, anda strong positive correlation between AOFAS scores and the range ofsubtalar pronation, supination, and total range of motion at the 2-yearpostoperative follow-up after surgical reduction and fixation of jointdepression calcaneal fractures in the elderly (Table 7; Figures 3, 5, and7). Similarly, we observed rather strong negative correlations
Fig. 6. Correlation of 100-mm visual analog scale (VAS) pain score with range of subtalarjoint supination at 2-year follow-up.Spearman’s correlation coefficient, r ¼ �0.8284.
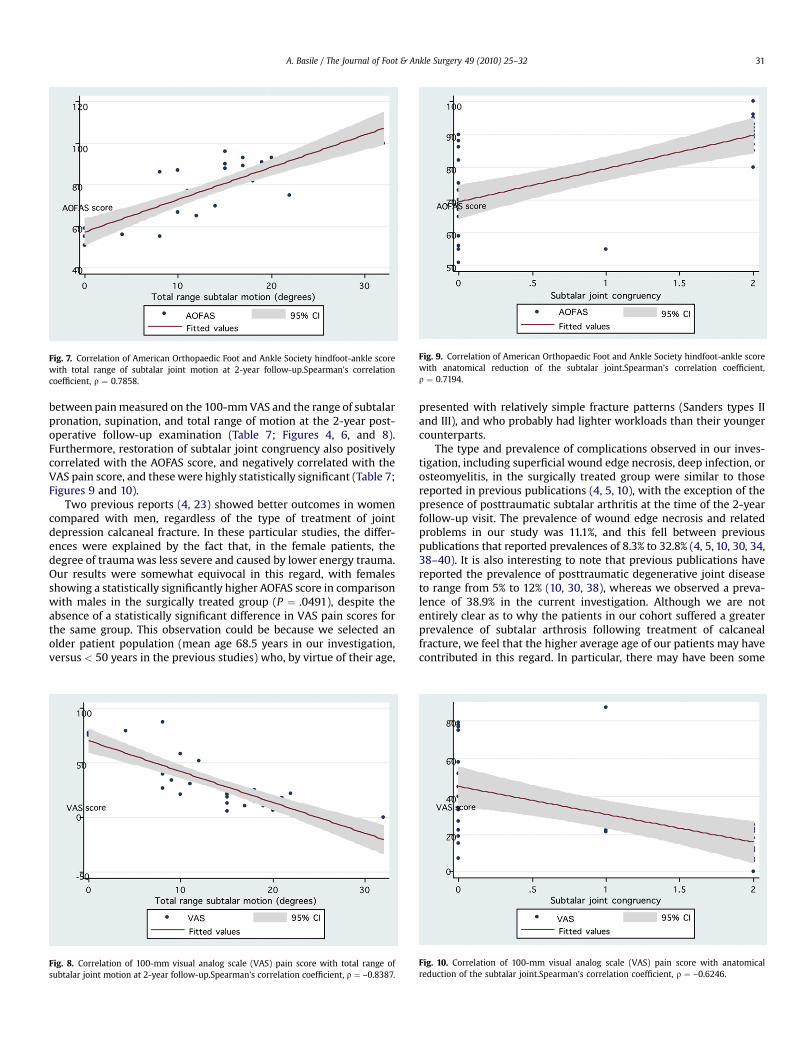
Fig. 7. Correlation of American Orthopaedic Foot and Ankle Society hindfoot-ankle scorewith total range of subtalar joint motion at 2-year follow-up.Spearman’s correlationcoefficient, r ¼ 0.7858.
Fig. 9. Correlation of American Orthopaedic Foot and Ankle Society hindfoot-ankle scorewith anatomical reduction of the subtalar joint.Spearman’s correlation coefficient,r ¼ 0.7194.
A. Basile / The Journal of Foot & Ankle Surgery 49 (2010) 25–32 31
between pain measured on the 100-mm VAS and the range of subtalarpronation, supination, and total range of motion at the 2-year post-operative follow-up examination (Table 7; Figures 4, 6, and 8).Furthermore, restoration of subtalar joint congruency also positivelycorrelated with the AOFAS score, and negatively correlated with theVAS pain score, and these were highly statistically significant (Table 7;Figures 9 and 10).
Two previous reports (4, 23) showed better outcomes in womencompared with men, regardless of the type of treatment of jointdepression calcaneal fracture. In these particular studies, the differ-ences were explained by the fact that, in the female patients, thedegree of trauma was less severe and caused by lower energy trauma.Our results were somewhat equivocal in this regard, with femalesshowing a statistically significantly higher AOFAS score in comparisonwith males in the surgically treated group (P ¼ .0491), despite theabsence of a statistically significant difference in VAS pain scores forthe same group. This observation could be because we selected anolder patient population (mean age 68.5 years in our investigation,versus < 50 years in the previous studies) who, by virtue of their age,
Fig. 8. Correlation of 100-mm visual analog scale (VAS) pain score with total range ofsubtalar joint motion at 2-year follow-up.Spearman’s correlation coefficient, r ¼ –0.8387.
presented with relatively simple fracture patterns (Sanders types IIand III), and who probably had lighter workloads than their youngercounterparts.
The type and prevalence of complications observed in our inves-tigation, including superficial wound edge necrosis, deep infection, orosteomyelitis, in the surgically treated group were similar to thosereported in previous publications (4, 5, 10), with the exception of thepresence of posttraumatic subtalar arthritis at the time of the 2-yearfollow-up visit. The prevalence of wound edge necrosis and relatedproblems in our study was 11.1%, and this fell between previouspublications that reported prevalences of 8.3% to 32.8% (4, 5, 10, 30, 34,38–40). It is also interesting to note that previous publications havereported the prevalence of posttraumatic degenerative joint diseaseto range from 5% to 12% (10, 30, 38), whereas we observed a preva-lence of 38.9% in the current investigation. Although we are notentirely clear as to why the patients in our cohort suffered a greaterprevalence of subtalar arthrosis following treatment of calcanealfracture, we feel that the higher average age of our patients may havecontributed in this regard. In particular, there may have been some
Fig. 10. Correlation of 100-mm visual analog scale (VAS) pain score with anatomicalreduction of the subtalar joint.Spearman’s correlation coefficient, r ¼ –0.6246.

A. Basile / The Journal of Foot & Ankle Surgery 49 (2010) 25–3232
preexisting subtalar degeneration before the injury. Despite thesefindings, however, only 2 (11.1%) of the 18 patients treated surgicallyrequired subtalar fusion to restore a pain-free gait. We also agree withHerscovici et al (8), who stated that it did not appear that age playeda clinically significant role in the development of soft tissue compli-cation or osseous infection; rather, it is more likely that the presenceof preexisting medical comorbidities may be a more important factorin the development of postoperative complications (8). The decisionto treat these elderly patients surgically was based on the samecriteria that we use for younger patients who present with a displacedintra-articular calcaneal fracture. The goal of surgical repair, in ourpractice, is to restore the articular surface, Bohler’s angle, and calca-neal position, thereby decreasing the likelihood of developing lateproblems with shoe wear, gait abnormalities, and chronic pain.
The main weaknesses of the present study are its retrospectivenature and the small sample size, although we were nonetheless ableto identify a number of statistically significant differences betweenthe patients who underwent surgical repair and those who weretreated without an operation to realign the fractured calcaneus. Theprimary reason for the small sample size was felt to be because of thestrict inclusion criteria used for the selection of patients for theanalyses. Other shortcomings included our use of the results ofprevious publications for comparison with our results, our lack of anexplanatory analysis involving univariate and multiple variablemethods, as well as the lack of a sensitivity analysis that could havedetermined the resistance of our results to the potential influence ofan unmeasured confounding variable. Moreover, the operatingsurgeons performed the radiographic measurements and categorizedthe quality of the articular realignment. Despite these limitations, wefeel that our findings are probably valid, especially in light of the factthat we followed the patients for at least 2 years, and refined ouranalyses to older patients. Moreover, we were able to show statisti-cally significant differences between valid health measurements,namely the AOFAS and VAS scores, which provide subjective patientinformation that pertains to foot-related quality of life.
Although we cannot draw definitive conclusions because ofmethodological shortcomings, our results showed statistically signif-icantly better outcomes in a strictly selected cohort of active elderlypatients treated with open reduction and internal fixation for displacedintra-articular calcaneal fractures, in comparison with the samemeasurements in an elderly group of patients with similar fractureswho were treated nonsurgically. Restoration of Bohler’s angle,improved subtalar joint motion, and better articular congruity and facetalignment appear to explain the improved outcomes in patients treatedoperatively. Despite these findings, and although we did not actuallyinvestigate this theory, we believe that nonoperative treatment shouldalways be considered for elderly patients who have low physicaldemand and/or major medical comorbidities that predispose tosurgical complications. Finally, we believe that the results of thisinvestigation could be useful in the development of future randomizedcontrolled trials and prospective cohort studies that focus on thetreatment of joint depression calcaneal fractures in elderly patients.
References
1. Lindsay R, Dewar F. Fracture of the os calcis. Am J Surg 95:555–576, 1958.2. Rowe CR, Sakellarides HT, Freeman PA, Sorbie C. Fractures of the calcaneus. JAMA
184:920–923, 1963.3. Jarvholm U, Korner L, Thoren O, Wiklund LM. Fractures of the calcaneus. A
comparison of open and closed treatment. Acta Orthop Scand 55:652–656, 1984.4. Buckley R, Tough S, McCormack R, Pate G, Leighton R, Petrie D, Galpin R. Operative
compared with nonoperative treatment of displaced intra-articular calcanealfractures. J Bone Joint Surg Am 84:1733–1744, 2002.
5. Zwipp H, Tscherne H, Thermann H, Weber T. Osteosynthesis of displaced intra-articular calcaneal fractures of the calcaneus. Clin Orthop 290:76–86, 1993.
6. Paley D, Hall H. Intra-articular fractures of the calcaneus. A critical analysis ofresults and prognostic factors. J Bone Joint Surg Am 75:342–354, 1993.
7. Howard JL, Buckley R, McCormack R. Complications following management ofdisplaced intra-articular calcaneal fractures: a prospective randomized trialcomparing open reduction internal fixation with nonoperative management. JOrthop Trauma 17:241–249, 2003.
8. Herscovici D, Widmaier J, Scaduto J. Operative treatment of calcaneal fractures inelderly patients. J Bone Joint Surg Am 87(6):1260–1263, 2005.
9. Sanders R, Fortin P, DiPasquale T, Walling A. Operative treatment of 120 displacedintraarticular calcaneal fractures. Results using a prognostic computed tomog-raphy scan classification. Clin Orthop Relat Res 290:87–95, 1993.
10. Benirschke SK, Sangeorzan BJ. Extensive extra-articular fractures of the foot. ClinOrthop 292:128–134, 1993.
11. Harvey EJ, Grujic L, Early JS, Benirschke SK, Sangeorzan BJ. Morbidity associatedwith ORIF of intra-articular calcaneal fractures using a lateral approach. Foot AnkleInt 22(11):868–873, 2001.
12. Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS, Sanders M. Clinicalrating systems for the ankle-hindfoot, midfoot, hallux and lesser toes. Foot AnkleInt 15:349–353, 1994.
13. Hildebrand KA, Buckley RE, Mohtadi NG, Faris P. Functional outcome measures afterdisplaced intra-articular calcaneal fractures. J Bone Joint Surg Br 78-B:119–123,1996.
14. O’Brien J, Buckley R, McCormack R, Pate G, Leighton R, Petrie D, Galpin R. Personalgait satisfaction after displaced intraarticular calcaneal fractures: a 2–8 yearfollow-up. Foot Ankle Int 25(9):657–665, 2004.
15. Duncan GH, Bushnell MC, Lavigne GJ. Comparison of verbal and visual analoguescales for measuring the intensity and unpleasantness of experimental pain. Pain7:295–303, 1989.
16. Morin P, Buckley R, Stewart R, Vande Gutche R. Oral analogue scale as an outcomemeasure after displaced intra-articular calcaneal fractures. Foot Ankle Int19:694–697, 1998.
17. Morrey BF, Wiedeman GP. Complications and long term results of ankle arthrod-esis following trauma. J Bone Joint Surg Am 62:777–784, 1980.
18. Loucks C, Buckley R. Bohler’s angle: correlation with outcome in displaced intra-articular calcaneal fractures. J Orthop Trauma 13:554–558, 1999.
19. Mittlmeier T, Morlock MM, Hertlein H, Fassler M, Mutschler W, Bauer G, Lob G.Analysis of morphology and gait function after intra-articular calcaneal fracture.J Orthop Trauma 7:303–310, 1993.
20. Janzen D, Connell DG, Munk PL. Intra-articular fractures of the calcaneus: value ofthe CT findings in determining prognosis. Am J Roentgenol 158:1271–1274, 1992.
21. Randle JA, Kreder HJ, Stephen D, Williams J, Jaglal S, Hu R. Should calcaneal fracturesbe treated surgically? A meta-analysis. Clin Orthop Relat Res 377:217–227, 2000.
22. O’Farrell DA, O’Byrne JM, McCabe JP, Stephens MM. Fracture of the os calcis:improved results with internal fixation. Injury 24:263–265, 1993.
23. Thordarson DB, Krieger LE. Operative versus non operative treatment of intra-articularfractures of the calcaneus: a prospective randomized trial. Foot Ankle Int 17:2–9,1996.
24. Barla J, Buckley R, McCormack R, Pate G, Leighton R, Petrie D, Galpin R. CanadianOrthopaedic Trauma Society. Displaced intra-articular calcaneal fractures: long-term outcome in women. Foot Ankle Int 25:853–856, 2004.
25. Parmar HV, Triffit PD, Triffit PJ. Intra-articular fractures of the calcaneum treatedoperatively or conservatively. A prospective study. J Bone Joint Surg Br75:932–937, 1993.
26. Hutchinson F III, Huebner MK. Treatment of os calcis fractures by open reductionand internal fixation. Foot Ankle Int 15:225–232, 1994.
27. Kingwell S, Buckley R, Willis N. The association between subtalar joint motion andoutcome satisfaction in patients with displaced intraarticular calcaneal fractures.Foot Ankle Int 25(9):666–673, 1994.
28. Benirschke SK, Sangeorzan BJ. Extensive intraarticular fracture of the foot. Surgicalmanagement of calcaneal fractures. Clin Orthop 292:128–134, 1993.
29. Crosby LA, Fitzgibbons T. Intraarticular calcaneal fractures. Results of closedtreatment. Clin Orthop 290:47–54, 1993.
30. Fortina A, Bertone C, Rondini A. Reconstruction of calcaneal skeletal defects causedby trauma. J Foot Ankle Surg 37:386–390, 1998.
31. Sanders R. Intraarticular fractures of the calcaneus. J Bone Joint Surg Am82-A:225–250, 2000.
32. Buckley R, Hunt D. Reliability of clinical measurement of subtalar joint movement.Foot Ankle Int 18:229–232, 1997.
33. Elveru RA, Rothstein JM, Lamb RL. Goniometric reliability in a clinical setting.Subtalar and ankle joint measurements. Phys Ther 68:672–677, 1988.
34. Pierce TJ, Buckley R. Subtalar joint movement: clinical and computer tomographyscan correlation. Foot Ankle Int 20:428–432, 1999.
35. Kundel K, Funk E, Brutscher M, Bickel R. Calcaneal fractures: operative vsnonoperative treatment. J Trauma 41:839–845, 1996.
36. Zmurko MG, Karges DE. Functional outcome of patients following operativereduction internal fixation for bilateral calcaneus fractures. Foot Ankle Int23(10):917–921, 2002.
37. Pozo JL, Kirwan EO, Jackson AM. The long-term results of conservative manage-ment in severely displaced fractures of the calcaneus. J Bone Joint Surg Br66-B:386–390, 1984.
38. Kitaoka HB, Schaap EJ, Chao EY, An KN. Displaced intraarticular fractures of thecalcaneus treated non-operatively. J Bone Joint Surg Am 76-A:1531–1540, 1994.
39. Bezes H, Massart P, Delvaux D, Fourquet JP, Tazi F. The operative treatment of intra-articular calcaneal fractures. Indications, technique, and results in 257 cases. ClinOrthop Relat Res 290:55–59, 1993.
40. Abidi NA, Dhawan S, Gruen GS, Vogt MT, Conti SF. Wound healing risk factors afteropen reduction and internal fixation of calcaneal fractures. Foot Ankle Int19:856–861, 1998.





























