Embed Size (px)
Citation preview

OPERATION THEATRE MANAGEMENT
PAPER-402Ms. SUSMITA BHAUMIK
An OT is that specialised facility of the hospital where life saving or life improving procedures are carried out on human body by invasive methods under strict aseptic conditions in a controlled environment by specially trained personnel to promote healing and cure with maximum safety, comfort and economy
Function
Operating theaters had a raised table or chair of some sort at the center for performing operations, and were surrounded by several rows of seats (operating theaters could be cramped or spacious) so students and other spectators could observe the case in progress.
The surgeon wore his street clothes with an apron to protect them from blood stains, and he operated bare-handed with unsterile instruments and supplies. (Gut and silk sutures were sold as open strands with reusable, hand-threaded needles; packing gauze was made of sweepings from the floors of cotton mills.)
In contrast to today's concept of surgery as a profession that emphasizes cleanliness and conscientiousness, at the beginning of the 20th century the mark of a busy and successful surgeon was the profusion of blood and fluids on his clothes.

OPERATION THEATRE
The operating theatre is based on whole system thinking and includes a whole of hospital perspective on effective and efficient theatre utilisation.
Goals
Key elements to efficient use of operating theatres are:
• Effective management
• Good communication
• Well trained staff
• Appropriate facilities and equipment
• Operational layout that allows flow of patients.
Support services play a large part in maximising efficiency by providing:• Pre-operative preparation and assessment• Available beds• Sterile theatre equipment• Portering, cleaning and maintenance staff.
•Effective planning and scheduling systems will enable smooth patient flow thus increasing capacity, improving patient and carer experience, improved employee satisfaction and morale
The operation theatre complex consists of four main systems,
•Surgical support system (the environment)
•Traffic and commerce (the activities)
•Communication and information (the records)
•Administration ( the management)

ADMINISTRATION
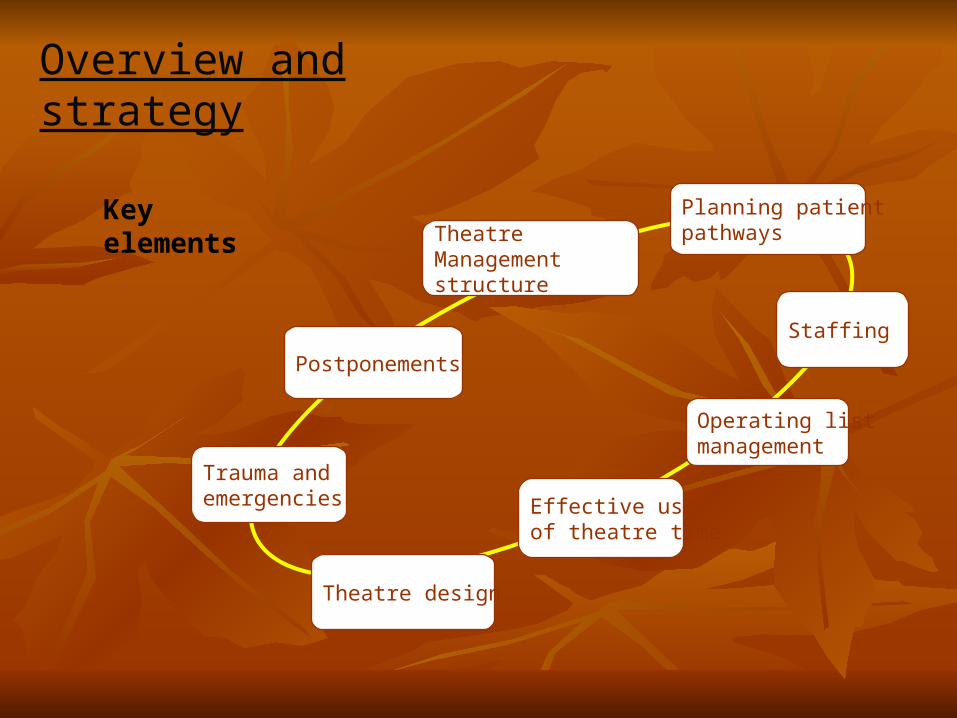
Overview and strategy
Theatre Management structure
Planning patient pathways
Staffing
Operating list management
Effective use of theatre time
Theatre design
Trauma and emergencies
Postponements
Key elements
Theatre management structure
Theatre management structure should be clearly defined with accountability for:
•Full budgetary authority•Adequate sessional allowance•Information systems•Utilisation•Administrative, medical and nursing staff.
Day to day management should be provided by an experienced trained and skilled theatre manager, who is responsible for clear communication, ensuring competent staffing and suitable equipping of all theatres. Suitable systems for planning activity should be available to allow allocation of staff, and to respond safely and flexibly when changes take place to routines. Policies should be developed to deal effectively with changes to operating lists. Operating lists should be clearly posted well in advance and in suitable locations. Theatre management team should regularly review utilisation, cancellations, list overruns, late starts and waiting lists.
Planning patients pathways
Patients pathways should take into account ways to maximise use of theatres and bed availability. Patients admitted to pre-operative units can be transferred to wards following surgery allowing time for discharge of previous patients.
Integration of pre-operative assessment and day case recovery area located adjacent to theatres provides an efficient use of space, skilled staff and may aid patient transport to and from theatres. This scheme also reduces time on ward rounds for surgeons and anaesthetist as patients are in one place.
StaffingDepartment should provide a system of staffing that works locally and is acceptable to staff
•Department staffing should match clinical activity, with sufficient cover for elective and emergencies
A lead anaesthetic consultant should be identified to support the theatre management team and trainees
•Adequate orientation of new or locum staff should be made a priority
•Adequate staffing should be available to cover governance tasks of note recording and data entry.
Operating list management
• Close communication and coordination between pre-op area and theatre using agreed procedures is essential
• A nominated person should liaise with wards and transport staff from theatres
• A suitable holding area staffed and equipped will assist with smooth flow
• Agreement should be made for preparation and transport of patients to and from theatres
• Policies on fasting, anticoagulation, shaving, dentures, jewellery, appropriate underwear and removal of make-up should be developed
• Units should agree the level of training needed to escort patients to and from theatres
• A documented system of handover and identification of patient should be in place
• A system to book critical care beds for elective admissions should be in place and booking confirmed before anaesthesia for surgery.
Theatre design and operational layout
Design of operating theatres is essential for maximising patient flow, consideration needs to be made for:
• Large multi-purpose accommodation to enable increase in complexity and equipment
• Transport routes that flow through stages of theatre care
• Internal communication IT systems that facilitate appropriate communication and supervision.
Trauma and emergency surgery
Effective planning for emergency and trauma surgery is needed to prevent cancellation of elective surgery.
Provision of exclusive emergency list will assist in preventing cancelled elective surgery. Good communication enables clinical decisions to be made rapidly, increasing the number of surgical procedures carried out in a safe time and environment. Time should be allowed for the Anaesthetist to assess emergency patients to their satisfaction. Experienced surgical staff should prepare patients who have multiple and complex medical problems, this can prevent cancellation at anaesthetic assessment. Pre-operative assessment for patients who are elderly, have multiple and complex medical problems can benefit from a team approach between anaesthetist, surgeon and physician.
Cancellations of surgery
It is extremely distressing and stressful to patients who are postponed surgery, many cancellations can be prevented by assisting patient flow with good planning in:
• Pre-operative assessment• Increased communication
Regular review of cancellation can assist with target areas for redesign and innovation.
Cancellation data should be collected and reviewed weekly with agreed action plans.
It is essential for operating theatre innovation to have a skilled, trained and committed innovation team.The team should consist of representatives of all theatre staff groups.
Management – clinical/non clinical
Nursing – Pre op and theatres, including operating department
practitioners
Clinical – Anaesthetist/Surgeons
Administration – Admin and Portering
Processes
AdmissionReceive patient to ward following operation
Administration Processes will also need to map demonstrating process from:
Initial recording of overall patient processes should be made covering:
Allocation totheatre list
Theatre reception on day of operation
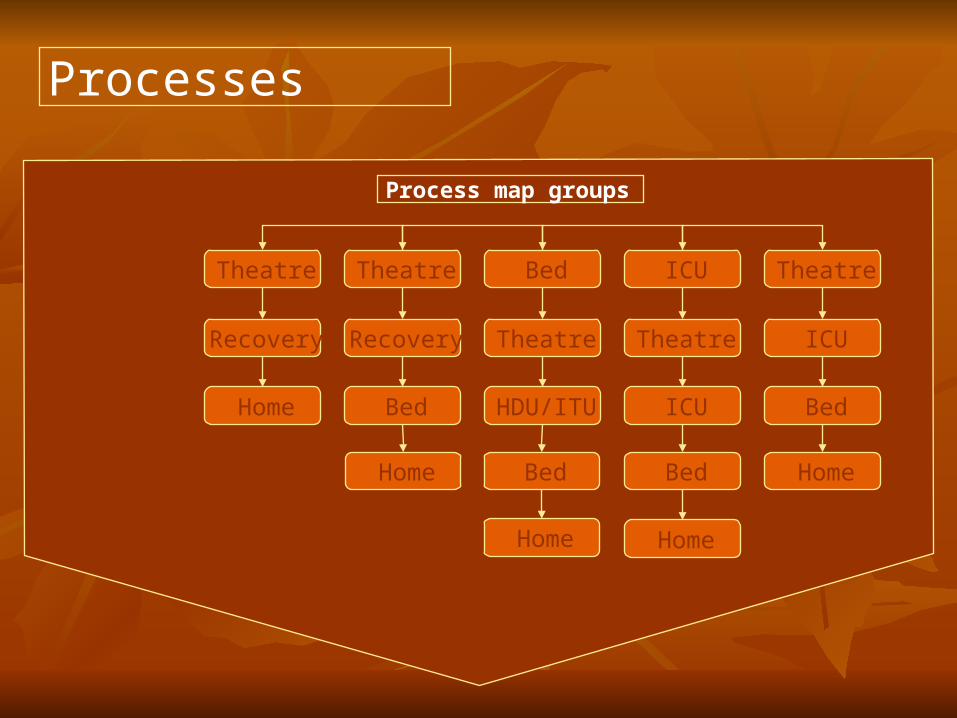
Processes
Theatre
Recovery
Home
Theatre
Recovery
Bed
Home
Bed
Theatre
HDU/ITU
Bed
Home
ICU
Theatre
ICU
Bed
Home
Theatre
ICU
Bed
Home
Process map groups
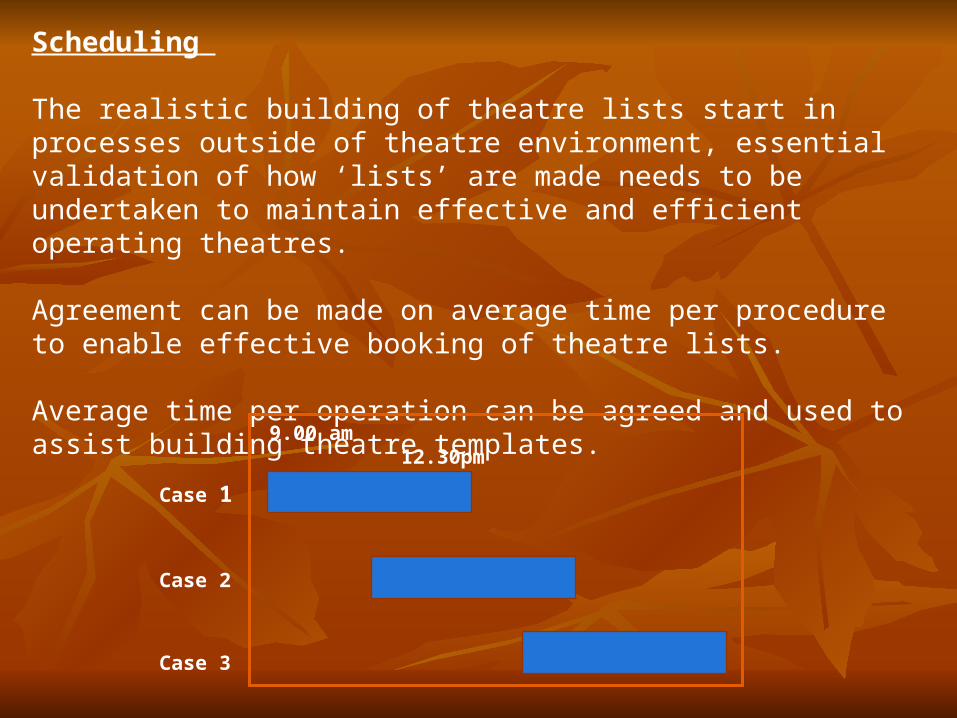
Scheduling
The realistic building of theatre lists start in processes outside of theatre environment, essential validation of how ‘lists’ are made needs to be undertaken to maintain effective and efficient operating theatres. Agreement can be made on average time per procedure to enable effective booking of theatre lists. Average time per operation can be agreed and used to assist building theatre templates.
Case 1
Case 2
Case 3
9.00 am 12.30pm
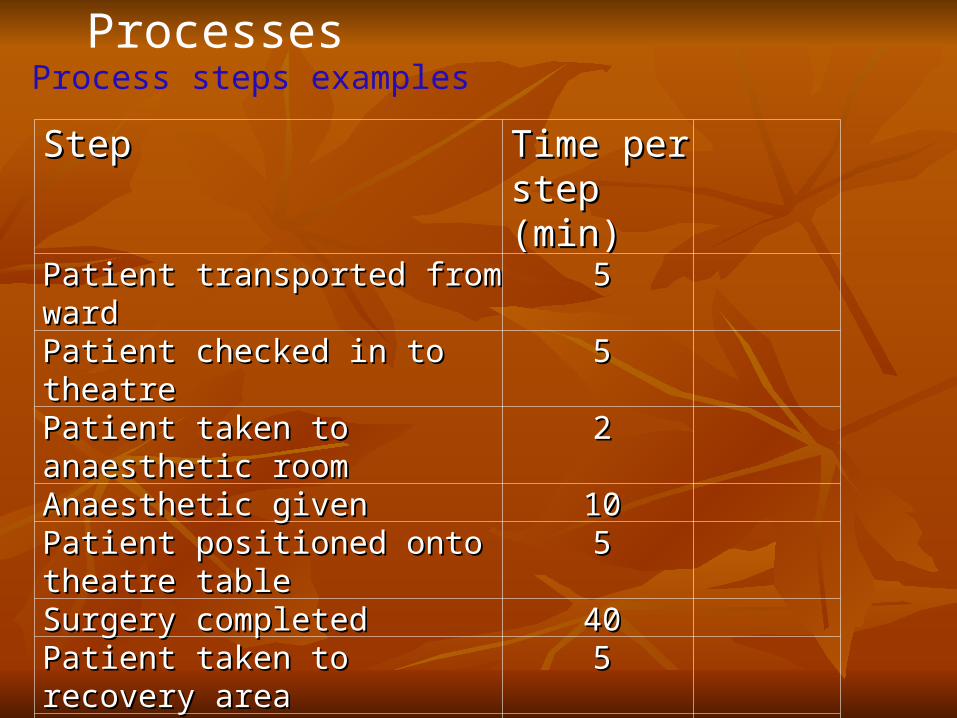
Process steps examplesProcesses
StepStep Time per Time per step (min)step (min)
Patient transported from wardPatient transported from ward 55Patient checked in to theatrePatient checked in to theatre 55Patient taken to anaesthetic Patient taken to anaesthetic roomroom
22
Anaesthetic givenAnaesthetic given 1010Patient positioned onto theatre Patient positioned onto theatre tabletable
55
Surgery completed Surgery completed 4040Patient taken to recovery areaPatient taken to recovery area 55Patient in post opPatient in post op 2020Patient taken to wardPatient taken to ward 55Theatre hands over patient to Theatre hands over patient to wardward
55
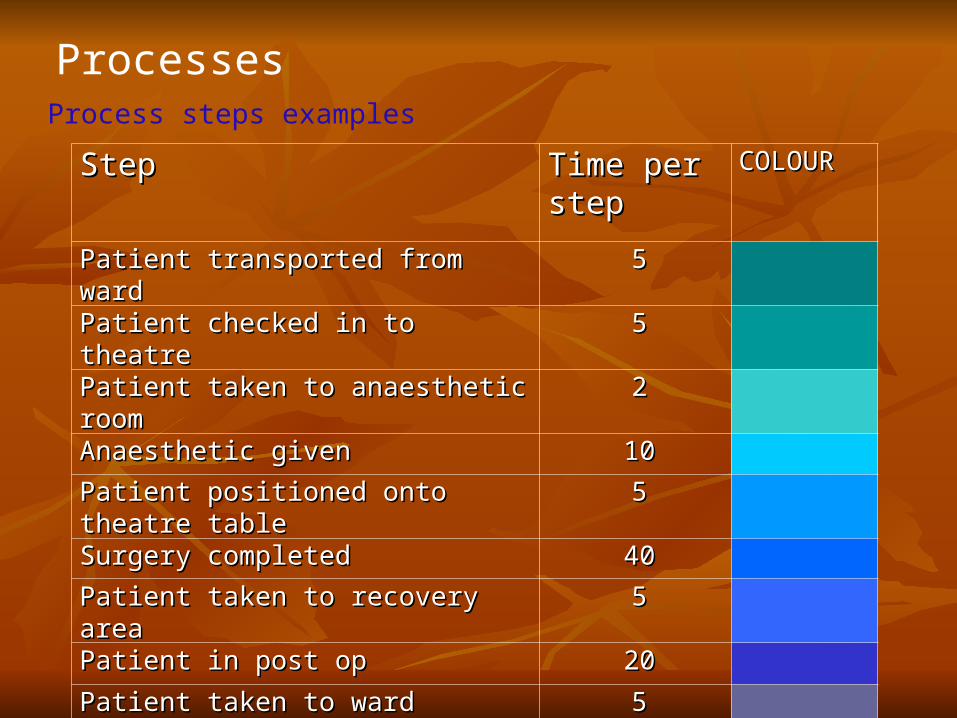
Process steps examples
Processes
StepStep Time per Time per stepstep
COLOURCOLOUR
Patient transported from wardPatient transported from ward 55
Patient checked in to theatrePatient checked in to theatre 55
Patient taken to anaesthetic roomPatient taken to anaesthetic room 22
Anaesthetic givenAnaesthetic given 1010
Patient positioned onto theatre tablePatient positioned onto theatre table 55
Surgery completed Surgery completed 4040
Patient taken to recovery areaPatient taken to recovery area 55
Patient in post opPatient in post op 2020
Patient taken to wardPatient taken to ward 55
Theatre hands over patient to wardTheatre hands over patient to ward 55
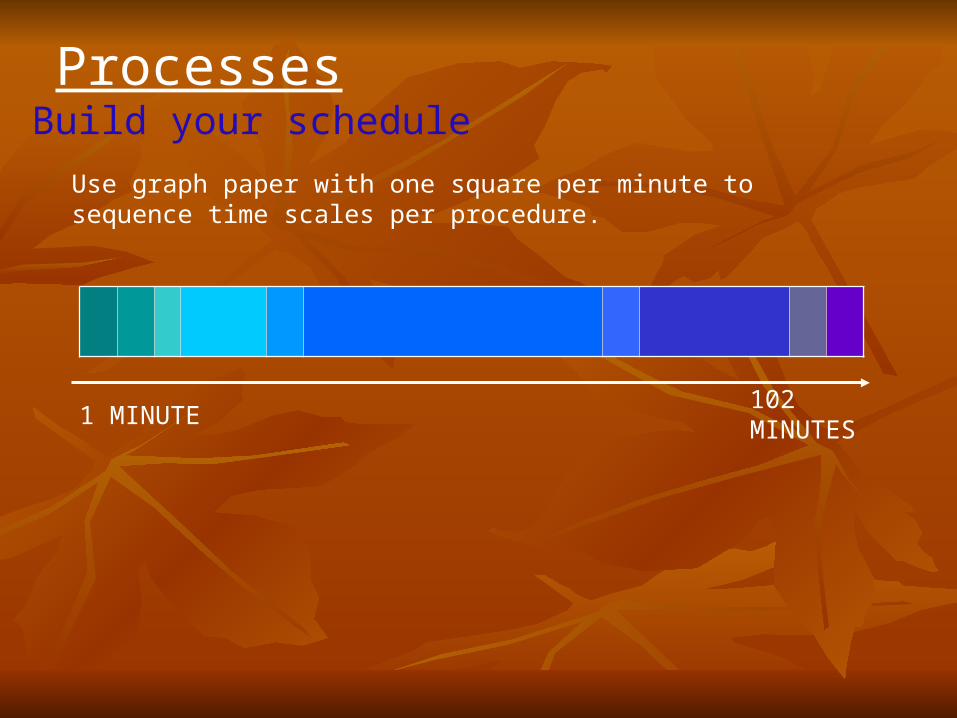
Build your scheduleProcesses
Use graph paper with one square per minute to sequence time scales per procedure.
1 MINUTE102 MINUTES
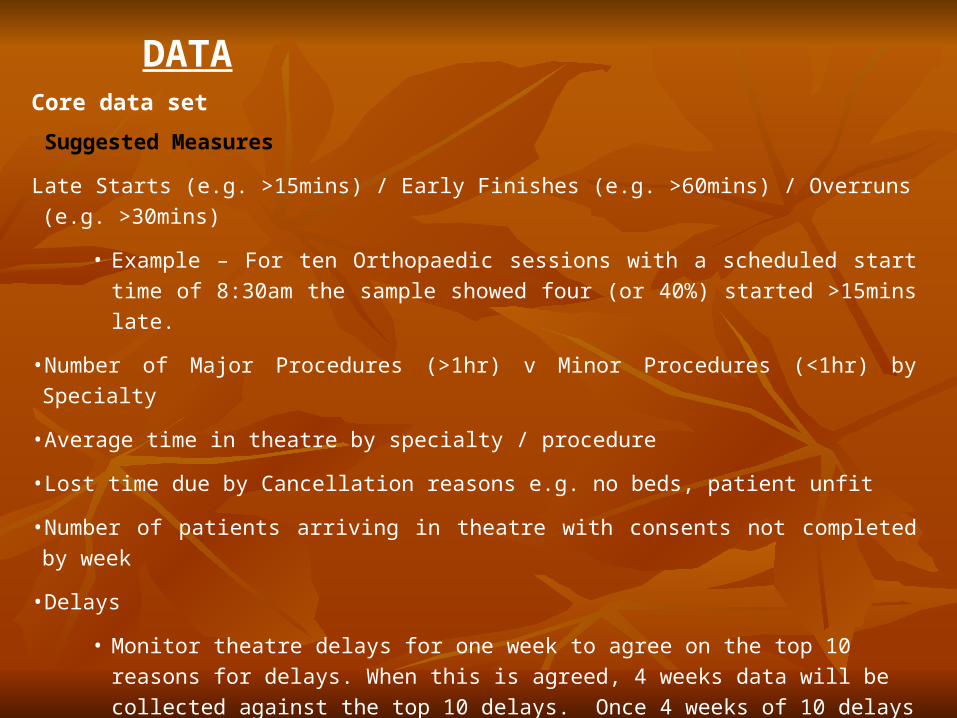
Core data set
Suggested Measures
Late Starts (e.g. >15mins) / Early Finishes (e.g. >60mins) / Overruns (e.g. >30mins)
• Example – For ten Orthopaedic sessions with a scheduled start time of 8:30am the
sample showed four (or 40%) started >15mins late.
• Number of Major Procedures (>1hr) v Minor Procedures (<1hr) by Specialty
• Average time in theatre by specialty / procedure
• Lost time due by Cancellation reasons e.g. no beds, patient unfit
• Number of patients arriving in theatre with consents not completed by week
• Delays
• Monitor theatre delays for one week to agree on the top 10 reasons for delays. When
this is agreed, 4 weeks data will be collected against the top 10 delays. Once 4
weeks of 10 delays have been gathered, charts will need to be produced. Time needs
to be collected against each reason(s) per day, as the top ten offenders may not
amount to the longest waste in time.
DATA
Resources Aim: To increase the utilisation and quality of care within operating theatres. Change Concepts •Review operating theatre utilisation
•Scheduling
•Identify system to report delays daily via agreed criteria
•Remove delays, complexity and hand offs within administration process
•Smooth process from Emergency Department / Inpatient wards to Operating Room and back to ward
•Review stages of Transfer from ward /Emergency Department, recovery to ward
•Review capacity and demand for emergency and elective theatre
•Review role of theatre coordinator and joint work with Pre-Operative and bed management
•Review equipment turn around times via Central Sterilising Services Department and booking of equipment
•Review recovery and transfer procedures – develop appropriate ‘pull’ process to theatre/wards
PLANNING AND DESIGNING PLANNING AND DESIGNING OF OPERATION THEATREOF OPERATION THEATRE
PAPER-402PAPER-402 MS.SUSMITA BHAUMIKMS.SUSMITA BHAUMIK
OBJECTIVES OF PLANNING Promote high standards of asepis Ensure maximum standard of safety Optimum utilisation of OT and staff time Optimize working conditions Patient and staff comfort in terms of thermal, acoustic and lighting
requirements Allow flexibility Facilities coordinated services Minimize maintenance Ensures functional separation of spaces Provide a smoothing environment Regulate the flow of traffic
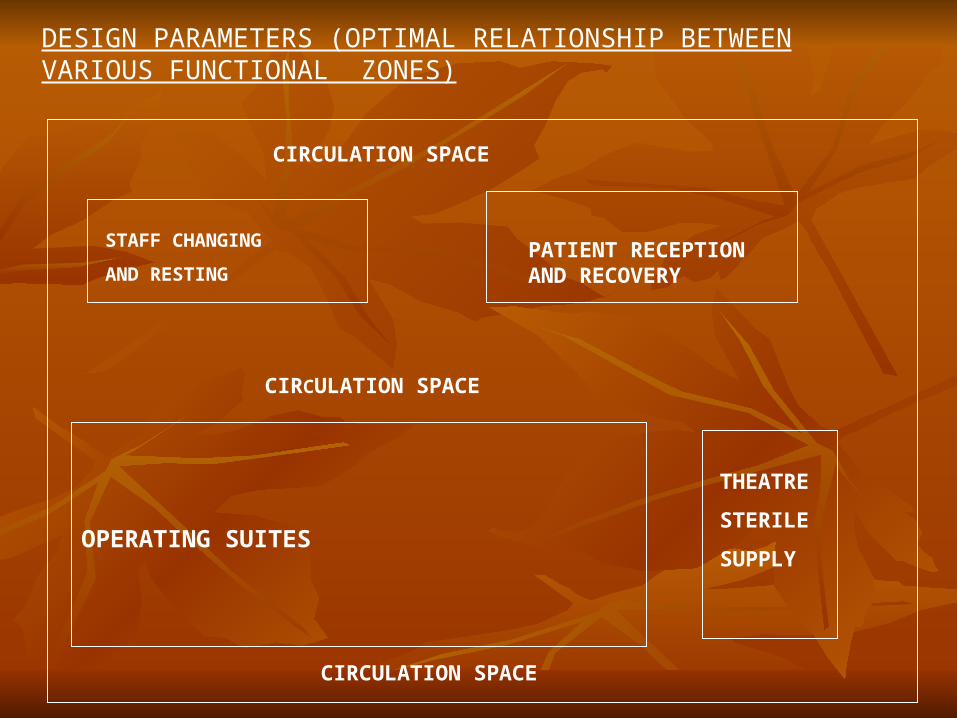
DESIGN PARAMETERS (OPTIMAL RELATIONSHIP BETWEEN VARIOUS FUNCTIONAL ZONES)
CIRCULATION SPACE
STAFF CHANGING
AND RESTINGPATIENT RECEPTION AND RECOVERY
CIRCULATION SPACE
OPERATING SUITES
THEATRE
STERILE
SUPPLY
CIRCULATION SPACE
DESIGN PARAMETERS Avoidance of unrelated hospital traffic flow Convenient functional flow between related departments like
ICU,ITU ETC Avoidance of outdoor noise Provision for future expansion Sliding doors Desirable floors to be smooth and non-slippery Ceilings to be painted with washable paints Taps in scrub room should be knee/elbow operated /infrared operated. Provisions of high speed autoclaves Essential pharmaceutical storage X-ray films illuminators Emergency communicators that can be activated without the use of
hand Toilets
PHYSICAL EVIRONMENTPHYSICAL EVIRONMENT
TEMPERATURETEMPERATURE HUMIDITYHUMIDITY VENTILATIONVENTILATION
Areas with higher hygienic requirements for air quality.
Areas with high clean-air requirements include the operating theatre,
any sterile preparation and pre-operative areas,
sterile storage, the anesthesia and equipment storerooms and the
entrances and the exits. The highest clean-air requirements apply to
the operation area and the sterile preparation area.
With respect to air treatment, the operating theatre and a number of
adjacent areas have to comply with the provisions of the working
conditions policy regulation.
From a technical point of view, the protective effect of the air surrounding the patient, operation team and instrument table, can be achieved by installing a large Laminar Air Flow (LAF) device (plenum). This LAF device with a downflow has a surface area of 8 to 9 m2 (e.g. square or octagonal 3 x 3m, rectangular 2.8 x 3.2m).
The air velocity from the downflow plenum is 24 to 30 cm/sec and flow temperature from the LAF device is 1 to 2°C lower than the ambient air.
There are also possible solutions and satisfactory results in
environmental control using special LAF devices in which the supplied
air has different speeds and temperatures and which also improved the
thermal comfort of the surgical team.
In order to be able to safeguard the requisite air quality in the operating theatre, a very large air flow is necessary. A re-circulation downflow system can be installed for this purpose. Part of the air from the down flow system is recirculated via fans to the HEPA filter. (HIGH EFFICIENCY PARTICULATE AIR)
In order to be able to evaluate whether the air system, the air flow profiles are correctly functioning, a CFD calculation is recommended at the design stage. This also makes it possible to ascertain whether, at a specific internal heat load, the selected diffused air temperature and the selected air velocity will not lead to an excessively high level of cooling in the operating theatre. This will also reveal at an early stage any short-circuiting between air supplied from the plenum and the site of the intake openings for air recirculation
Assuming that the air from the HEPA filter is sterile, the only possible emission source will be the operation team, the OT staff, the patient, the material used and the equipment.
With respect to the sterile preparationarea with direct access to the operating theatres, a higher pressure is recommended compared to all rooms adjacent to this area.
POSSILE AIR CLEALIESS:The desired germ level of less than 10 colony forming units (CFU) per m3
Air DistributionAir Distribution
TurbulentTurbulent or mixing air distribution system Downward displacement piston system Unidirectional air flow system (laminar flow)
Basic quality requirements for the technical facilities are:
• The surgical department has to be equipped with a mechanical
ventilation system.
•The operating theatre has to be equipped with a laminar downflow
system with a large air plenum (8 to 9 m2). Under working conditions
with operation lights switched on and the presence of the operation
team, the air supply and blast air profile are chosen in such a way that
the air does not pass through any sources of contamination before
flowing into the operation area or over the instrument table.
•There must be no windows that can be opened and outside walls
must be completely sealed.
The most important basic quality requirements concerning spatialrelationships are:
The surgical department is independent of traffic flows in the
rest of the hospital; through traffic is not permitted through this
department.
Airlocks physically seal a surgical department from the rest of
the hospital.
Staff working in the operating theatre complex can move from
one ‘clean’ area to another without needing to pass through ‘non-
clean’ areas.
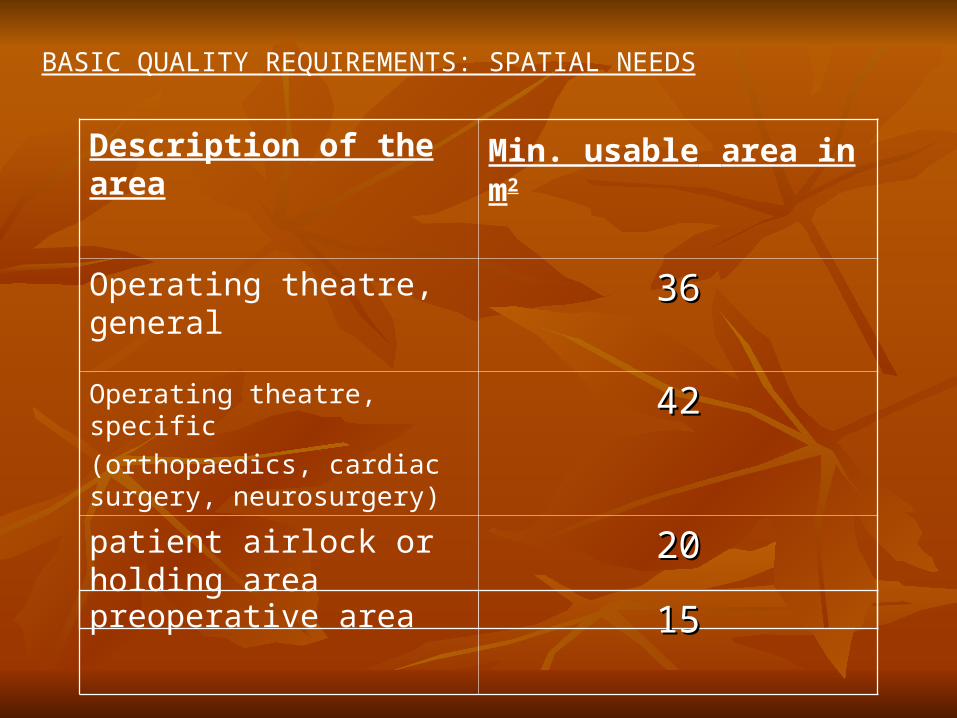
Description of the area Min. usable area in m2
Operating theatre, general 3636
Operating theatre, specific
(orthopaedics, cardiac surgery, neurosurgery)
4242
patient airlock or holding area
2020
preoperative area 1515
BASIC QUALITY REQUIREMENTS: SPATIAL NEEDS
TEMPERATURE AND HUMIDITY
Normal person at rest (unclothed) – 240-270c with relative
humidity of 50%
Body looses heat during anesthesia.
So,So,1. R.H – 45-60% recommended (adults 40% , children and infants
55%-60%)
2. In UK, 200 – 220 c with R.H. 50% to 60%
3. In US, 210 -24.50 c with R.H 50-60%
Other basic quality requirements
The following basic quality requirements apply to the use of equipment, operational
reliability of installations and finish in a surgical department: Health risks to staff such as exposure to microbiological and chemical
Contamination, and lasers and ionizing radiation can be avoided as far as
possible by drawing up guidelines and protocols.
Operational reliability of the technical installations and an optimal indoor
environment for both patients and staff form the basis for the design
and maintenance of the mechanical engineering and electro technical installations.
The finish of floors, walls and ceilings must be smooth, flawless or closed.
Corners and transitions between floors and walls will be rounded to prevent
accumulation of dirt. The different areas should be constructed and furnished in such
a way as to allow effective cleaning and if necessary disinfection with commonly
used cleaning agents and permitted disinfectants.

ZONING IN OT
CONSISTS of 4 zones
A. OUTERZONE - Areas for receivingpatients messengers,toilets,administrative Function
B. RESTRICTED ZONE OR CLEAN ZONE –
- Changing room - Patient transfer area- Stores room - Nursing staff room -Anaesthetist room - Recovery room
C. ASEPTIC ZONE –
•Scrub area•Preparation room,•Operation theatre,•Area for instrument packing and
sterilization.
D. DISPOSAL ZONE
Area where used equipment are cleanedand biohazardous waste is disposed
OPERATION ROOM
1. Big enough for free circulation
2. Two openings (optional)
Towards scrub area
Towards sterile area
3.Openings fitted with swing doors.
4.Marble or polished stone flooring
5.Glaze tiled walls
6.No false ceiling
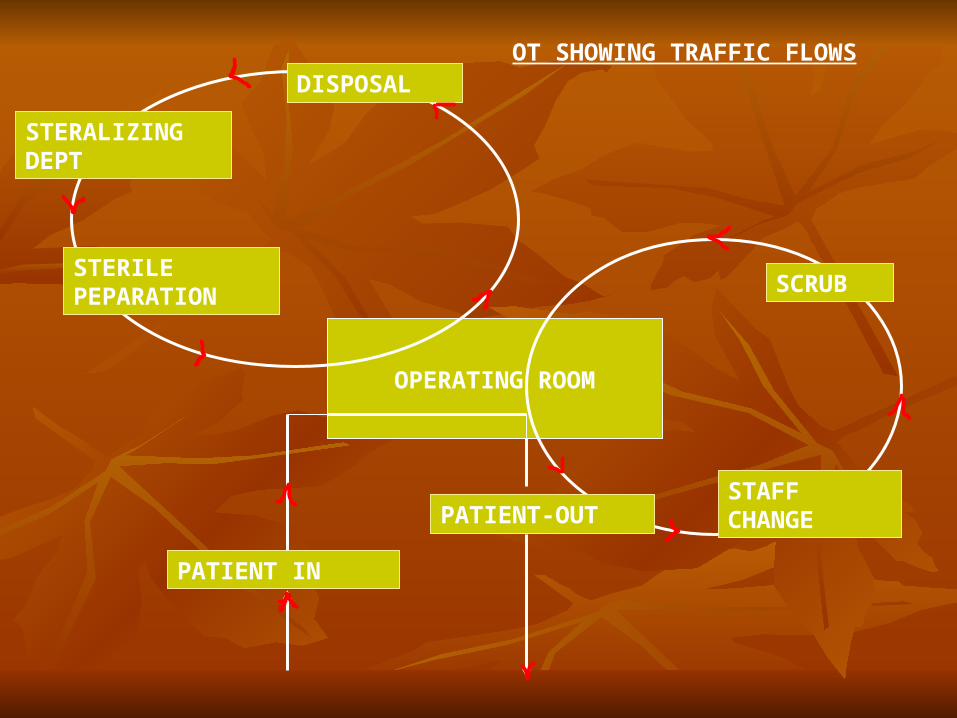
OPERATING ROOM
PATIENT IN
STERALIZING DEPT
STERILE PEPARATION
DISPOSAL
SCRUB
STAFF CHANGEPATIENT-OUT
OT SHOWING TRAFFIC FLOWS

NUMBER OF OPERTING SUITES
Number and type of Number and type of surgeonssurgeons
Type of hospitalsType of hospitals Hospital policy and
procedure Bed strength Number and type of
surgery patients Number of operations
per day
Time aTime allowed for staff breaks
Average time for operations
Time allowed for maintenance of OT
Expected ALOS Size of an average OT
list
1. According to Rao committee
-One operation theatre for 50 surgical beds
2. American pattern
One operation theatre for 25 surgical beds
3. European countries
One operation theatre for 50 surgical beds
LOCATION
GROUND FLOOR/ TOP FLOOR/ ANYWHERE IN THE HOSPITAL
LIGHTING IN OT
O.T. Light
Hospital furniture is important aspect owing to its specialized design. This furniture has certain functions needed to support patients who have decreased mobility. In such cases the specialized design of hospital furniture serves the need of providing the required support.
Operation theatre (OT) light comes with the following features:
• perfect• comfortable• Lights brilliant • Exclusive design • Trouble free• Mounting is economic
Shadow less Ceiling Operating light combination that provides the superior performance for all kinds if surgeries. Compact, Light weight and sealed dome made of aluminium consists of glass diachronic reflector to provide cool, bright and homogenous illumination.
OT Lights are made to spot light the operation table area. They illuminate the area to the right level of brightness with effective heat absorbing and color correcting provided for cool, white and brilliant light field for operational convenience
Venus O.T. Lights
WORKFLOW
1. Singe corridor system
2. Double corridor system
• disposal traffic
• Patient and disposal traffic
• Patient and staff traffic

EQUIPMENT PLANNING
The most efficient type of operating suite in terms of maximum utilisation of resources as well as the most cost-effective, will display the following characteristics:
1. It will be without a separate anesthetic room
2. It will have shared scrub facilities between theatres
3. It will have a disposal bay or room servicing two theatres
4. It will have a centrally located supply room servicing a no. of theatres
FURNITURES & GADGETS
• Special fixtures: anesthesia cabinet, instrument storage cabinet, scrub station, x-ray viewing, writing board, inter-communication.
• Special furniture: instrument trolley, bowl stand, infusion stand, step stair, disposal bag holder, stool, endoscopes,
• CCTV
• Assembly tables, sterilization equipments, patient monitoring and resuscitation equipments
• Medical gases
• Anesthesia equipments
• Operating radiography and micrographic instruments

THANK YOU





























