Embed Size (px)
Citation preview

Click to edit Master title style
Click to edit Master subtitle style
Operating Room Turnover Analysis and Improvement
Reza Maleki and Melissa KramDepartment of Industrial and Manufacturing Engineering
North Dakota State University

Project Background
• Reflects the work of a team of students who, on behalf of MeritCare Health System, undertook the project “Operating Room Turnover”
• Conducted as a partial fulfillment for the Program and Project Management Capstone course
Client OverviewMeritCare Health System• Providing excellent care since 1905
• Largest practicing group in NDTwo Hospitals and 42 Supporting Clinics
• Over 1.5 million patients served a year with a service area that spans 250 miles
MeritCare Medical Center – Downtown Fargo• 380 Bed Facility
• Houses 11 surgical suites
• 2003 Surgical Department Synopsis:Over 9,400 cases and 22,400 case hours
Generated 37 million dollars in revenue

Project BackgroundNeeds Identification
Increasing efficiency of key profit center: Surgical Department
Focus on Turnover Efficiency in the Operating Room
MeritCare ContactsQuality Management Engineer
Executive Partner Surgical Services
Surgical Service Educator
CRNA Manager
Operating Room Manager
Statement of Work and Deliverables

Presentation Overview
• Project Objective
• Project Work and Research Activities
• Recommendations
• Project Benefits
• Suggestions for Future Projects
• Lessons Learned
• Questions

Project ObjectiveDetermine and propose methods to minimize the operating room downtime
Recommend ways to improve utilization by reducing turnover time
Room CleanupPatient Emergence Room Setup Patient Preparation
T u r n o v e r T i m e
Close Incision

Project Work & Research Activities
• Observations at MeritCare
• Meeting with individual staff members
• Outside discussions with professionals
• Research
• Data analysis
• Documentation

Turnover Process
Readying the RoomFinishing First Case Preparing Next Patient
Incision Closure• Incision closed• Dressing applied• Emergence from anesthesia
Patient Out of OR• Patient moved from OR table to
gurney• Patient transported to PACU
(recovery room)
Readying the RoomFinishing First Case Preparing Next Patient
Finishing First Case
Project Work & Research Activities
Reference: Clockwork Surgery, Hardwiring Efficiency into the Perioperative Process

Readying the RoomFinishing First Case Preparing Next Patient
OR Cleanup• Trash discarded• Case cart removed• Equipment collected for
reprocessing• OR floor & surfaces cleaned
OR Setup• Case cart delivered to OR suite• Instruments & supplies laid out• Sterile supplies opened• Missing items retrieved• Equipment positioned & Setup checked
Readying the RoomFinishing First Case Preparing Next Patient
Readying the Room
Turnover ProcessProject Work & Research Activities
Reference: Clockwork Surgery, Hardwiring Efficiency into the Perioperative Process

Readying the RoomFinishing First Case Preparing Next Patient
Patient to OR• Patient transported to OR• Patient moved from gurney to OR
table• Patient positioned & prepped• Additional lines may be placed
Incision• Patient induced• First incision made
Preparing Next Patient
Readying the RoomFinishing First Case Preparing Next Patient
Turnover ProcessProject Work & Research Activities
Reference: Clockwork Surgery, Hardwiring Efficiency into the Perioperative Process

Example TurnoverClockTime Event9:32 incision closed9:39 patient leaves (with CRNA & aide)9:43 room cleaned9:47 CRNA starts set up9:53 CRNA finishes set up
10:04 patient enters10:09 scrub nurse finishes room set10:23 patient prepped10:34 patient draped and incision made
Patient Waits
Staff Waits
Total Turnover Time = 62 min
Project Work & Research Activities

Attainability of Additional CasesProject Work & Research Activities
7:308:008:309:009:30
10:0010:3011:0011:3012:0012:301:001:302:002:303:003:304:00
Overtime Overtime
Long Cases Short Cases
Case 1
Case 2
Case 3
Case 1
Case 3
Case 2
Case 4
Case 1
Case 2
Case 3
Case 4
Case 5
Case 6
Case 1
Case 2
Case 3
Case 4
Case 5
Case 6
Case 7
Reference: Clockwork Surgery, Hardwiring Efficiency into the Perioperative Process

Recommendations
1. Early Patient Entry
2. Local Certified Registered Nurse Anesthetist (CRNA)
3. Front Loaded Anesthesia
4. Redefining Patient Transportation

Early Patient Entry
Time Saved
Room Cleanup
Patient in Holding Area Anesthesia Preparation
Room Setup
Patient Waits
OR Waits
TransportationInduction
Patient
OR
Recommendations
%25≈
Room Cleanup
Patient in Holding Area
Room Setup
Anesthesia Preparation TransportationInduction
Patient
OR
Reference: Clockwork Surgery, Hardwiring Efficiency into the Perioperative Process
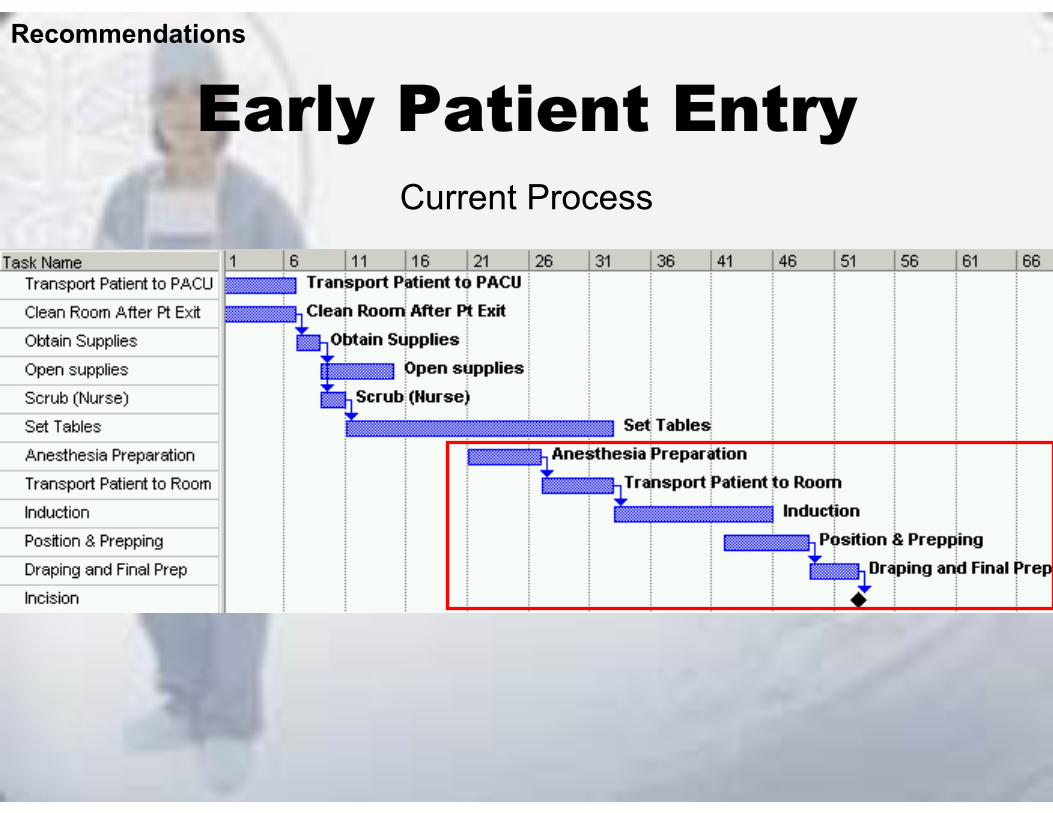
Early Patient EntryCurrent Process
Recommendations

Early Patient EntryProposed Process
Recommendations
Time Saved
%25≈

Early Patient Entry
• Shortened wait time experienced by both patient and operating room staff
• Balanced activities to eliminate bottlenecks in the process
• Potential to increase number of cases
Recommendations
Benefits

Recommendations
1. Early Patient Entry
2. Local Certified Registered Nurse Anesthetist (CRNA)
3. Front Loaded Anesthesia
4. Redefining Patient Transportation

• Excluding first cases, an Anesthesiologist is responsible for completing all preoperative anesthesia evaluations
• Anesthesiologists have other equally important duties throughout the hospital
• Delays arise from varying demand
Recommendations
Local CRNA
Current Practice

Local CRNA
Delays by Department
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
40.00%
Surgeon Anesthesia Patient Other/ER Casein Progress
Nursing Lab/X-Ray Other
Recommendations
33%Anesthesia

Local CRNA
Recommendations
Anesthesia Delays
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
40.00%
Pt. Waiting
to be
seen by
Ane
s.Diff i
culty
Startin
g Line
sLin
e's in
Progres
s inHold
ing
MD Una
vaila
bleAne
sthes
ia Delay
s
CRNA Una
vaila
bleCRNA no
t ready
for Pt. Y
et.
Waiting to be seen by anesthesia
36%

Local CRNA
• Tried and true method
• Supports early patient entry
• Reduces patient and staff wait times
• Decreases delays caused by a busy anesthesiologist
• CRNA, who is more economical, is qualified to conduct the preoperative anesthesia evaluation
Recommendations
Benefits

Recommendations
1. Early Patient Entry
2. Local Certified Registered Nurse Anesthetist (CRNA)
3. Front Loaded Anesthesia
4. Redefining Patient Transportation

• For small cases, large percentage of patients come to the OR with no anesthetic work done
• An additional task for the in-room CRNA
• Delays in the OR suite are more costly
Front Loaded Anesthesia
Recommendations
Current Practice / Issues
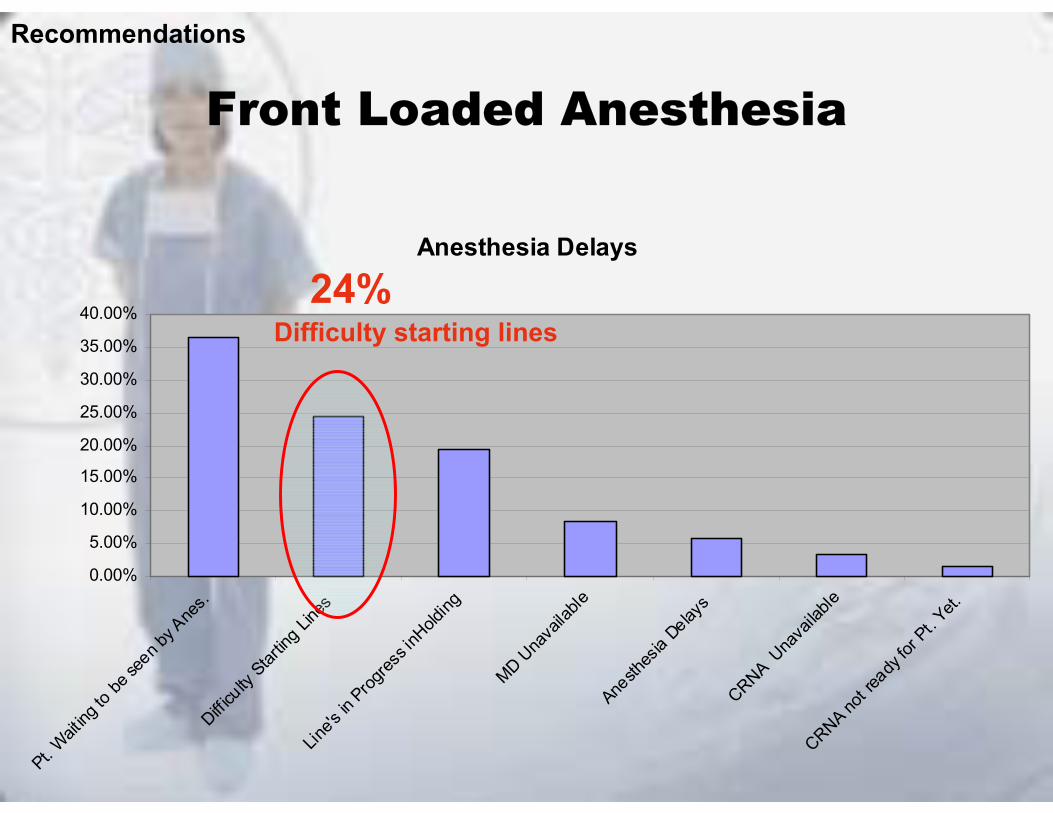
Front Loaded Anesthesia
Anesthesia Delays
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
40.00%
Pt. Waiting
to be
seen by
Ane
s.Diff i
culty
Startin
g Line
sLin
e's in
Progres
s inHold
ing
MD Una
vaila
bleAne
sthes
ia Delay
s
CRNA Una
vaila
bleCRNA no
t ready
for Pt. Y
et.
Recommendations
Difficulty starting lines24%

Front Loaded Anesthesia
• Reduces the impact of possible delays during the turnover process
• Limits negative effects of problem cases
• Reduces workload for in-room CRNA
Recommendations
Benefits

Recommendations
1. Early Patient Entry
2. Local Certified Registered Nurse Anesthetist (CRNA)
3. Front Loaded Anesthesia
4. Redefining Patient Transportation

CRNA• Complete in-room setup • Transport patient into OR suite• Tasks are serial
Circulating Nurse• Usually has idle time at some point during
turnover process– After opening of supplies
Redefining Patient Transportation
Recommendations
Current Practice

Redefining Patient TransportationResource Utilization
Recommendations

Redefining Patient Transportation
• Supports early patient entry
• Frees up a crucial resource
• Assists in having the patient in the operating suite as soon they can be accommodated
Recommendations
Benefits

Example TurnoverClockTime Event9:32 surgery over9:39 patient leaves (with CRNA & aide)9:43 room cleaned9:47 CRNA starts set up9:53 CRNA finishes set up
10:04 patient enters10:09 scrub nurse finishes room set10:23 patient prepped10:34 patient draped and incision made
11 minutes
3 minutes
• Early Patient Entry
– Local CRNA
– Redefining Patient Transportation
• Front Loaded Anesthesia
Time Saved:
14 minutes – 22%

• Increased surgeon satisfaction
• Surgeon replacement costs of $20,000-$85,000
• Short-staffed one surgeon can result in lost revenue of over $100,000 monthly
Project Benefits

Project Benefits
• Costs negligible
• Possible additional cases and revenue
Potential profit could be upwards of $100,000 per suite if only one case a week is added (Source: MeritCare)
With one additional case per day, per operating room suite could translate to $4 - $7 million in annual revenue (Source: HFMA and Health Care Advisory Board)

Recommendations for Future Projects
SchedulingResearch has shown scheduling to having the largest impact on utilization and revenue
CommunicationIntegrated Information Technology Systems
First Case Start Times
SURGICAL DEPARTMENT

Lessons Learned• Work with staff & openly ask questions to learn the
complex perioperative process.
• Do not point out people or departments as problems, but instead stress the particular process as the problem.
• Keeping an open mind and recognizing the importance of compromising to ultimately reach the goal of the project.
• Make recommendations that will work and will receive buy-in from management and staff.
• Such projects provide enhanced learning opportunities for students, faculty, and business/industry clients.

Questions

Slide 1
Operating R
oom T
urnover Analysis and Im
provement
Reza M
aleki and Melissa K
ram
Departm
ent of Industrial and Manufacturing Engineering
North D
akota State University
Fargo, North D
akota 58105
Reza M
aleki, Ph.D., P.E
., C.M
fg.E.
Phone: (701) 231-8071
Fax: (701) 231-7195
Email:
Reza.M
http://ww
w.ndsu.edu/ndsu/m
aleki/Biography.doc
Melissa K
ram
Phone: (701) 367-4994
Email:
Melissa.K
ram@
ndsu.nodak.edu
Slide 2
This presentation reflects the work of a team
of students, who on behalf of M
eritCare H
ealth System
, undertook the project “Operating R
oom Turnover Efficiency.”
The project was also conducted as partial fulfillm
ent for the Program and Project
Managem
ent/Capstone course. The course is aim
ed at providing students with the opportunity to
work on real-w
orld projects for business/industry clients.
Slide 3
Project Client - M
eritCare H
ealth System
MeritC
are Health System
, an entire network of care, is an integrated hospital and clinical system
w
ith headquarters in Fargo, North D
akota. Established in 1905, MeritC
are has grown to be the
largest group practice in North D
akota, with 72 specialty areas of m
edicine. MeritC
are Medical
Group currently serves nearly tw
o million people a year across a service area that spans 250
miles w
est to east.
MeritC
are Health System
, in Fargo, consists of two hospitals and 42 supporting clinics. The tw
o hospital locations include M
eritCare M
edical Center (dow
ntown Fargo) and M
eritCare South
University. The M
eritCare M
edical Center has 380 adult and pediatric licensed beds.

Betw
een the two locations, there are currently tw
enty-one operating room suites. M
eritCare
Dow
ntown M
edical Center houses the m
ain operating rooms, w
hich consists of eleven suites. In 2003, the m
ain operating rooms had over 9,400 cases and over 22,400 case hours w
hich generated 37 m
illion dollars in revenue. In the fall of 2004 a twelfth suite w
as added, that is used for block scheduling part-tim
e and for add-on cases part time.
Slide 4
Like many other healthcare providers, M
eritCare m
akes every effort to better manage existing
resources, minim
ize waste, and increase the efficiency of various departm
ents. MeritC
are recognized the advantages of focusing on their key profit center – the Surgical D
epartment.
MeritC
are’s Operating R
oom Im
provement Team
had realized the potential for improvem
ents w
ith the current processes surrounding and involving the operating room suite turnover.
The project team’s first task w
as to set up and attend meetings w
ith MeritC
are contacts in order to gain as m
uch information as possible pertaining to developm
ent of the scope of the project, including learning and understanding the perioperative process. D
uring initial meetings, the
group met w
ith several mem
bers of MeritC
are Health System
staff including people from
surgical services, executive board, and quality managem
ent. Throughout these meetings, process
and project information w
as gathered and the ground rules were laid out.
After m
eetings with M
eritCare personnel and careful consideration of the needs and problem
s discussed, a statem
ent of work and deliverables w
as drafted and ultimately finalized.
Project Team
Deliverables
1. D
ocumentation of the current turnover process of the operation room
suites. 2.
Docum
ent with recom
mendations for im
proving operating room suites.
3. D
ocumentation providing cost/benefit analysis for the proposed im
provements.
4. A
n outline of recomm
endations for future projects and further improvem
ents.
Slide 5
Slide 6
The statement of w
ork included the agreed-upon project objective.
Project Objective
The objective of this project is to determine and propose m
ethods to minim
ize the operating room
downtim
e and, more specifically, recom
mend w
ays to improve utilization by reducing
turnover time.

Turnover rate, defined by MeritC
are, is the difference between the closure tim
e of one operation and the incision tim
e of the succeeding operation; including patient emergence, room
clean-up from
the previous case, suite setup and patient preparation for the subsequent case.
Slide 7
Observations / D
ata Collection
The project team’s first step tow
ards data collection was to becom
e familiar w
ith the complex
perioperative process, the medical jargon used, the job tasks of the staff, and the surgical
department environm
ent through numerous observations. C
ollecting the data was definitely the
most tim
e-consuming portion of the project. M
embers of the project team
made observations of
the turnover process between the cases occurring am
ong the 11 operating room suites. M
any tim
es, team m
embers w
ould pair up so one could watch the turnover, w
hile the other could follow
the patient from A
M adm
issions and the holding room to the surgical suite. O
ther cases involved one m
ember w
atching the turnover in the suite, while the other follow
ed the patient to the PA
CU
or recovery room. This allow
ed the team m
embers to w
itness all the processes directly related to the turnover and the associated possible delays. A
ll together, the project team
was able to accum
ulate over 25 observations and document m
ost of them. A
t first, there was a
concern with how
the staff would react to the team
mem
ber’s being present in the operating suites. H
owever, w
ith managem
ent support, that concern was never an issue. The m
anagement
of the surgical department inform
ed the staff of the team’s purpose and introduced the team
m
embers to m
any of the surgeons and anesthesiologists. Fortunately the majority of the staff
welcom
ed the team’s endless questions.
During the observation tim
e spent at MeritC
are, the observations that were taken involved m
uch m
ore than just watching the current process. The group felt that videotaping the turnover in the
room, w
ithout exposing the patient to ensure confidentiality, would be valuable for the first
observations. This allowed the team
to capture the process and have record of the observation, used to study the process and to later reference once the key factors w
ere identified. Since every operating room
suite generally performs different types of procedures, the group w
as able to observe a large variety of cases involving a num
ber of tear down, cleaning, and setting up
procedures. Since there was a variety of cases observed, team
mem
bers were able to w
itness different turnover team
s and equipment, as w
ell as the varying tasks that need to be performed
for a specific type of case.
Research
Research done prior to and during the project consisted of m
any different phases. The primary
reference used was C
lockwork Surgery, H
ardwiring E
fficiency into the Perioperative P
rocess,published by the C
linical Advisory B
oard in 2001. The book goes into great graphical detail on m
any of the aspects involved in our presentation, and also provided a template for som
e of the team
’s future recomm
endations.
Other research w
as done on the internet, particularly researching healthcare specific organizations. These resources enabled the project team
to find various methods used by
professionals working in the industry to tackle som
e of the same needs the project encom
passed.

Data A
nalysis The data and inform
ation gathered from observations, interview
s, meetings, and conversations or
emails w
ere organized into useful information to support the project team
in the development of
their recomm
endations.
Besides the data gathered by the group, the project team
was provided w
ith historical data from
previous and current projects and observations made by the client. The historical data w
as analyzed for accuracy and applicability to ensure that it w
as of use within the scope of the
project. One set of historical data w
as used to construct Pareto charts. Based on the charts, as
well as other inform
ation, the project team w
as able to identify two leading contributors to the
type of delay.
The project team also did analysis on data for room
occupancy times. A
lthough the data provided figures on the room
set-up and clean times, m
ost cases studied were not concurrent by
our definition of turnover, providing little significance.
Slide 8
A list of events that occur during each phase and factors influencing the turnover rate is com
piled and available through the reference book, C
lockwork Surgery, H
ardwiring E
fficiency into the P
erioperative Process. The team
used this resource as a guide to learn and understand the turnover process, but the process elem
ents were verified w
ith the actual process.
The T
urnover Process The operative process includes the entire turnover process that this project encom
passes. As
previously defined, operating room turnover tim
e is the difference between the closure tim
e of one operation and the incision tim
e of the succeeding operation; including patient emergence and
clean-up from the previous case along w
ith suite and patient preparation for the subsequent case.
The turnover process includes three sequential phases; finishing the first case, readying the room,
and preparing the next patient. There are a number of events that take place during each phase of
the process, along with a num
ber of factors that influence the turnover rate. There are various steps in each phase that m
ust be completed chronologically to ensure a sterile environm
ent.
Finishing First Case
The first phase of the turnover process is finishing the first case. This phase includes incision closure and transport of the patient out of the operating room
suite to the PAC
U for recovery.
Incision closure includes wound closure, dressing application, and em
ergence from anesthesia.
When transporting the patient, the patient is m
oved from the operating room
table to a transport bed and transported to the PA
CU
by the circulating nurse and anesthesia caregiver.
Slide 9

The T
urnover Process
Readying the R
oom
The second phase of the turnover process is readying the room, w
hich includes two m
ain steps; the cleanup of the previous case is com
pleted and then setup of the following case is started. The
operating room suite cleanup consists of discarding all drapes and trash, rem
oving the case cart, collecting equipm
ent for reprocessing, and cleaning the floor and surfaces (damp dusting). A
case cart is a shelving cart that holds all prepackaged supplies for the particular case. O
nce the cleaning tasks are com
plete, the staff continues by setting up for the next case. Setting up consists of delivering the case cart to the operating room
suite, laying out all supplies and instrum
ents, and opening sterile supplies. If there are any missing item
s, they are tracked down,
all the equipment is positioned, and finally, the setup is checked against the surgical preference
card for completeness.
Slide 10
The T
urnover Process
Preparing Next Patient
The third and final phase of the turnover process is preparing for the next patient. The patient is transported to the operating room
suite and moved from
the gurney to the operating room table,
where the patient is positioned and prepped for surgery. A
nesthesiology then inserts any additional lines not previously placed in the holding room
. Shortly thereafter, the patient is induced and the incision is m
ade by the surgeon. The turnover is complete.
Efficient room turnover requires careful orchestration of a large am
ount of staff mem
bers perform
ing an array of interconnected tasks. With the inherent com
plexity of the process, often tim
es a lengthy turnover is the rule rather than the exception.
Slide 11
An exam
ple of data collected during observation of the turnover process.
Slide 12
After som
e analysis of the current process, considerations to research, and discussions with key
MeritC
are personnel, it was decided that the length of case varied greatly. W
ith the timeline of
project a decision needed to be made as to the focus of the project, either shorter or longer cases.

Here, the definition of a shorter case is a case in w
hich the surgical time is an hour or less. A
s show
n in the figure, the shorter cases offer the greatest potential for attainability of additional cases. If the duration of the case is too long, the freed tim
e will be less than the tim
e it takes to perform
a case, pushing the last case into staff overtime, w
hich is not a desired effect.
Nevertheless, focusing on recom
mendations for shorter cases w
ill definitely provide the possibility of additional cases and in turn have the m
ost potential for a direct economic benefit.
Once the focus w
as determined to be the shorter cases, four m
ain recomm
endations were
formulated.
Slide 13
Recom
mendations
Based on their research, the project team
came up w
ith the following four recom
mendations:
1. Early Patient Entry
2. Local C
ertified Registered N
urse Anesthetist (C
RN
A)
3. Front Loaded A
nesthesia 4.
Redefining Patient Transportation
Slide 14
Early Patient E
ntry
The theory behind early patient entry is to get the patient into the room as early as possible to
allow anesthetic, positioning, and preparatory w
ork to begin. Currently, there is a w
aiting period experienced by both the patient and the operating room
, but at different times throughout the
process. Since these wait tim
es are not in series, the elimination of both w
ait periods seems to be
a beneficial step.
The figure shown on this slide represents a basic exam
ple of the events taking place in the operation room
(top of the figure) and the events experienced by the patient (bottom of the
figure) prior to the surgery and after the previous patient has left the operating suite. Although
these waiting tim
es are not series in nature, they are definitely not independent. The wait
experienced by the patient when w
aiting to be transported to the room creates the w
ait in the room
while the patient is being transported.
By sim
ply moving up the tim
e that the patient transportation to the operating suite takes place, both w
ait times can
be eliminated (or at a m
inimum
reduced). The slide animation show
s the new
process and the expected time saved, for a saving in tim
e about 22% of the total average
turnover time.

Slide 15
Early Patient E
ntry
This and the next slide show the turnover process, broken dow
n by task in a Gantt chart, to m
ore specifically show
how early patient entry can benefit the turnover process.
The figure on this slide shows an exam
ple of the current process, compiled using average tim
es found during observations, from
research, and the documents provided by the client. There are
certain tasks that must follow
in a serial manner; how
ever, the current process is not taking full advantage of parallel processes w
ith a certain group of tasks. It appears that there is a lack of parallel processing w
hen it comes to the w
ork done by anesthesia in coordination with the rest of
the process tasks and employee utilization.
Slide 16
Early Patient E
ntry
The figure on this slide demonstrates w
hat the ideal process would look like. N
otice that none of the task lengths have been altered or dependencies elim
inated. Instead, by having the patient enter the room
imm
ediately when the room
is allowed to accept the patient (w
hen all supplies are opened) the overall turnover tim
e can be substantially reduced by about 25%.
The chart shows an idyllic process for turnover in the room
. In this case, the CR
NA
comes back
from the PA
CU
and begins setup almost im
mediately. Tim
e has been allotted for completing
paperwork and checking narcotics in and out. The total tw
elve minutes that the C
RN
A is show
n to be out of the room
is felt to be an adequate amount of tim
e for the average non-problematic
case.
A m
ilestone has also been added to this chart to show the im
portance of the surgeon getting to the operating suite at an appropriate tim
e. Most of the tim
e, the surgeon needs to be present to position the patient properly and check the setup. O
ne of the most difficult things about
implem
enting a new plan is having the involved personnel accept it.
In order for early patient entry to work, all personnel involved w
ith the perioperative process m
ust be adaptive to parallel processing and some support features m
ust be in place. In order for the patient to be prepared to enter the operating room
, all preoperative work m
ust be done; including tests, paperw
ork, evaluations, etc. Delays in these areas w
ill inevitably delay the start tim
e of the procedure.
Slide 17

Early Patient E
ntry
The following benefits can be realized from
implem
enting early patient entry: •
Shortened wait tim
e experienced by both patient and operating room staff
• B
alanced activities to eliminate bottlenecks in the process
• Potential to increase num
ber of cases
Slide 18
Slide 19
Local C
ertified Registered N
urse Anesthetist (C
RN
A)
One of the processes prior to transporting the patient to the operating suite is the preoperative
anesthesia evaluation process. Currently (excluding the first cases of the day) an anesthesiologist
is responsible for seeing patients in AM
admissions for the preoperative anesthesia evaluation.
AM
admissions is located on another floor, requiring the anesthesiologist to travel a noticeable
distance in the hospital. The problem w
ith this process is that anesthesiologists are also responsible for m
any other equally important activities throughout the hospital.
Observations show
ed situations where the patient in the A
M adm
issions area had to wait to be
visited by the anesthesiologist before they could proceed to the operating room area. The
anesthesiologist was late because of other tasks that they w
ere working on that could
understandably not be abandoned or delayed. So the problem becom
es how to elim
inate such delays w
ithout being a hindrance to the quality of care provided to other areas of the hospital.
Slide 20
Local C
ertified Registered N
urse Anesthetist (C
RN
A)
Historical data, w
hich was provided by the client, also supports the project team
’s observation of delays due to the patients w
aiting to be seen by the anesthesia caregiver. The figure on this slide show
s the overall delays caused by various departments. A
ccording to the figure, the anesthesia departm
ent is the second major contributor to the delays. This figure is based on the year 2003
data.Slide 21
Local C
ertified Registered N
urse Anesthetist (C
RN
A)

Further analysis of the historical data shows that the prim
ary anesthesia delay (about 36%) w
as the patient w
aiting to be seen by an anesthesiologist.
The proposed solution is to have a staff capable of doing preoperative anesthesia evaluations perm
anently located in the admissions area. In the first case scenario, there is a m
aximum
of two
CR
NA
’s or MD
A’s located in the A
M adm
issions area to see upwards of nine patients nearly
simultaneously. The first case is generally the busiest tim
e for the admissions area, so there
definitely should be no need for any more than tw
o throughout the day and there is a strong possibility that one could handle the m
ajority of the day, only having an anesthesiologist come
down to help w
hen needed.
Slide 22
Local C
ertified Registered N
urse Anesthetist (C
RN
A)
A local C
RN
A is a tried and true m
ethod at MeritC
are. This was the standard practice until
roughly five years ago when the shortage of C
RN
A’s caused m
anagement to m
ove that individual into the operating suites. N
ow that the anesthesiology departm
ent is close to their full C
RN
A staff, the C
RN
A M
anager felt that they had the capacity to fill the position in AM
A
dmissions.
This recomm
endation supports early patient entry as it will aid in reducing both patient and staff
wait tim
es. This will also decrease delays caused by a busy anesthesiologist.
Having a C
RN
A in the adm
issions area for preoperative anesthesia evaluation is a template
followed by a num
ber of different practices. One hospital system
, the University of W
ashington M
edical Center (a 450-bed com
prehensive care facility), went as far as to give nursing staff
specialty training to perform the anesthesia evaluation. Patient records and nursing assessm
ents are then review
ed then by an anesthesiologist or a nurse anesthetist prior to surgery.
Another possible benefit seen from
implem
enting a nurse anesthetist in AM
admissions is
allowing the anesthesiologists to spend m
ore of their time in the surgical departm
ent. This could possibly have a large im
pact on facilitating problem anesthetic cases and getting problem
atic lines started on tim
e. This idea opens the door to a third recomm
endation – front loaded anesthesia.
Slide 23
Slide 24
Front Loaded A
nesthesia

The current practices and issues involved with front loaded anesthesia include:
• For sm
all cases, large percentage of patients come to the O
R w
ith no anesthetic work done
• A
n additional task for the in-room C
RN
A
• D
elays in the OR
suite are more costly
Front loaded anesthesia is the practice of doing as much anesthesia w
ork as possible before the patient is brought to the operating suite. That w
ill help to reduce and/or prevent related potential delays in the operating room
. The thought behind this recomm
endation are the delays that are not the every day occurrence, but w
hen they happen, are detrimental to the turnover process and
case start times. There can be tim
es when there is difficulty starting even the basic lines, such as
IVs. If this delay occurs in the A
M adm
issions area or the holding room it is not directly
affecting the turnover time in the operating suite.
Slide 25
Front Loaded A
nesthesia
The second leading anesthesia delay is difficulty starting lines in a patient, according to the historical data from
2003. Although the causes for those delays are not w
ithin the scope of this project, rem
oving the delays from the operating room
(during the turnover process) is within the
scope of this project.
Slide 26
Front Loaded A
nesthesia
This recomm
endation can not be looked at as a cure all, as it does not apply to all cases. Once
again the primary benefits from
implem
entation will com
e from the sm
aller cases where there
seems to be a tendency to have all of the anesthesia w
ork done in the operating room, rather than
having a patient be burdened by an IV tree.
There are many interdependencies am
ong various perioperative processes and a delay in any one area w
ill cause major delays in the entire turnover. This reason alone should be enough to show
the im
portance of controlling and offloading delays that can not be eliminated.
Front loaded anesthesia would lim
it the effects of problem cases w
hen considering the total turnover tim
e. This will also reduce the w
orkload for the in-room C
RN
A, the critical resource.
This brings us to the final recomm
endation – redefining patient transportation.
Slide 27

Slide 28
Redefining Patient T
ransportation
Observations have show
n that in most occasions, the C
RN
A is responsible for retrieving the next
patient. This is another example of tying up a valuable resource. There w
ere documented
instances when the circulator, or som
etimes also an aide, w
ere waiting in the room
for the CR
NA
to finish setting up their equipm
ent so that same C
RN
A could go retrieve the patient from
the holding room
. From interview
ing staff about this situation, it was learned that patient retrieval
was not alw
ays one of the CR
NA
’s standard job tasks, but instead had become the practice over
time. Slide 29
Redefining Patient T
ransportation
This slide shows the utilization of som
e of the resources during the turnover process. One can
conclude that one of the options is, where and w
hen possible, to redistribute workload for m
ore equitable use of the em
ployee resources.
The proposed idea is to have the circulating nurse retrieve the patient. Observations have show
n that in m
ost cases due to the current process, the circulating nurse has idle time right after
opening the supplies. This is also supported by the collected data during year 2000 by a M
eritCare study that charted resource usage and tim
es. You can see here in the G
antt chart w
here in the process redefining patient transportation is important.
If the circulating nurse should happen to be truly busy, a mem
ber of the holding room staff or the
operating room orderly staff w
ill be responsible for bringing the patient to the operating room.
The CR
NA
, the critical resource in the turnover process, should be leaving the room to retrieve
the patient only when it is absolutely necessary. Since the tasks perform
ed by the in-room
CR
NA
are quite serial, this will autom
atically create a delay in the process. Therefore, this option should be evaluated very carefully.
Transportation of a patient to the operating rooms from
the OR
holding room takes, on the
average, six minutes for an average shorter case, and can be upw
ards of 20 minutes if the patient
must be retrieved from
the AM
admissions area. The accum
ulation of six to twenty m
inute transports over the course of a day can add up very quickly.
Slide 30

Redefining Patient T
ransportation
The benefits of redefining patient transportation include: •
Supports early patient entry •
Frees up a crucial resource •
Assists in having the patient in the operating suite as soon they can be accom
modated
Slide 31
Revisiting the E
xample T
urnover to Show E
ffects of Recom
mendations
To show you the effects of our four recom
mendations, let’s revisit the exam
ple turnover discussed earlier. There w
ere eleven minutes in this turnover w
here the patient was w
aiting to enter the operating suite and the operating room
was w
aiting for the patient to begin prep. The patient could have entered the operating suite as soon as the C
RN
A finished their set up. Y
ou can see how
early patient entry would have decreased the total turnover tim
e with the support of a
local CR
NA
and redefining of patient transportation. There was also a three m
inute delay in this case, considering the tim
e that it took the CR
NA
to place the anesthesia line. While the line w
as being placed the rest of the personnel w
ere idle. Front Loaded Anesthesia, placing the line prior
to entering the operating suite, would have elim
inated this delay in the process. These im
provements w
ould have brought about a time savings of 14 m
inutes or about 22% in the
overall process.
Slide 32
Project Benefits
As justification for the project recom
mendations, there w
ere two m
ain areas that the project team
identified as benefits to be gained from im
plementation of the recom
mendations. The first
benefit is increased surgeon and staff satisfaction. Secondly, by decreasing downtim
e of the operating room
, there is potentially room in the schedule for additional surgical cases and
income.
When it com
es to surgeon satisfaction, the truth is, it is expensive to not have one. Recruitm
ent costs for a new
surgeon can cost anywhere from
$20,000 for just recruitment costs, to upw
ards of $85,000 if a sign-on bonus is needed and a recruiter is utilized. These m
ay be one-time costs,
but the loss in revenue from being short-staffed a surgeon is even m
ore substantial since one surgeon can provide over $1 m
illion dollars in revenue every year. The costs alone make it
important to hold surgeon satisfaction as a high priority, not to m
ention the non-quantifiable effects losing a good surgeon can have on a practice as far as recognition and recruiting other quality staff.

Maintaining surgeon satisfaction is of utm
ost importance to m
anagement of m
edical facilities. Surgeons are an integral part of the healthcare com
munity and certain considerations should be
made to achieve a high satisfaction rate. A
ccording to a national survey conducted by the B
arnes-Jewish St. Peters H
ospital, 74% of surgeons rated the im
portance of surgical turnover as “very im
portant”.
It was also found by the national survey, that the ideal turnover tim
e for 54% of surgeons
surveyed is a 10-15 minute turnover tim
e. Although that short of a tim
e is rather unrealistic for m
ost cases, it shows how
important of a factor short turnover tim
es are for surgeon satisfaction, and the benefits that can be gained from
working to reduce turnover tim
es.
As a general conclusion, if surgeons are satisfied w
ith the system in w
hich they work, they w
ill be m
ore likely to stay and become an asset to the facility.
Slide 33
Project Benefits
The implem
entation costs of the recomm
endations given are negligible to MeritC
are, requiring no additional capital or labor investm
ents. The primary financial benefit w
ould be revenue generated from
additional cases. Reducing room
turnover rates alone will not guarantee tim
e for additional cases in every room
, however, the reduction of accum
ulating unproductive time
throughout the day will provide opportunity for additional cases in the room
s that hold smaller
cases and turnover time accounts for a m
ore substantial portion of the daily scheduled time.
Here again the focus of the project team
has been on the achievable smaller cases. Sm
all cases (laparoscopic gallbladders for exam
ple) that are done in the general surgery rooms have healthy
per case. These cases have actual procedure times of about 25 m
inutes, and the entire case can be facilitated in less than an hour. If an average of 15 m
inutes can be saved between at least four
successive cases in one day, it would provide am
ple room for an additional sm
all case. A
ccording to figures given by MeritC
are, the amount of profit generated w
ould be upwards of
$100,000 per room if only one case a w
eek can be added. The best case scenario of three rooms
adding one small surgery five days a w
eek would generate profit of over $1.3 m
illion dollars. A
ccording to the Healthcare Financial M
anagement A
ssociation (HFM
A) and the H
ealth Care
Advisory B
oard, improvem
ents resulting in one additional case per day per operating room suite
could translate to four to seven million dollars in annual revenue.
Slide 34
Recom
mendations for Future Projects
Based on the research and observations m
ade, the project team recom
mended a num
ber of projects that have potential to further im
prove turnover process.

The current scheduling process needs to be analyzed and improved. The current scheduling
process does not provide for efficient utilization of operation rooms. Im
proved scheduling procedure should provide for appropriate block tim
e utilization and scheduling proper length per case.
Incorporating an integrated IT system w
ould facilitate for simultaneous relay of real tim
e case data to all pertinent locations. The IT system
also allows for instantaneous changes that w
ould help in scheduling preoperative patient activities and having the patients prepared and available to go into the operating suite w
hen it becomes available.
In addition, the project team recom
mended to M
eritCare that the O
perating Room
Improvem
ent Team
continue their efforts to increase the number of on-tim
e starts for first cases.
Slide 35
Slide 36





























