Embed Size (px)
Citation preview
Injury Extra (2007) 38, 365—368
www.elsevier.com/locate/inext
CASE REPORT
Open postero-medial dislocation of the elbowin a 11-year oldA case report
D. Lui *, S. Boran, B. Lenehan, D. Jones, E. Fogarty
Paediatric Orthopaedic Department, Our Ladys Children Hospital in Crumlin, Dublin, Ireland
Accepted 21 December 2006
Background
Closed posterior dislocation of the elbow is a com-mon injury. Open dislocations are rare,2 but asso-ciated with neurovascular injury due to the natureof the proximity of the structures and is extremelywell documented as early as 1952.1,3,4,6,9—17,21—27,29—32,35—44 We present a case of a 11-year-oldboy who sustained an open postero-medial disloca-tion of the elbow with no associated neurovascularinjury. There have been no similar paediatric casesreported in the literature.
Case presentation
A 11-year-old boy was bicycling along a 6 ft highwall and fell on an extended, adducted and exter-nally rotated left arm. He walked home and pre-sented to the casualty department 1 h later. Hehad an open contaminated dislocation of his leftelbow joint (Fig. 1). There was difficulty assessingsubjectively due to anxiety, objectively he had noobvious neurovascular compromise. Radiographs
* Corresponding author at: Our Lady’s Children Hospital inCrumlin, Crumlin Rd, Dublin 12.
E-mail address: [email protected] (D. Lui).
1572-3461/$ — see front matter # 2007 Elsevier Ltd. All rights resedoi:10.1016/j.injury.2006.12.192
revealed a postero-medial elbow dislocation(Figs. 2 and 3).
He was emergently transferred to the operatingtheatre. Surgical debridement and reduction of thejoint was performed. Intra-operative findingsshowed that the distal humerus had penetratedthrough the anterior cubital fossa. In doing so thecrucial lateral and medial collateral ligamentouscomplexes which play an important role in stabilitywere destroyed.
Themedian nervewas noted to be draped over theanterior aspect of the humerus but intact. Brachialartery was in continuity and protected throughoutthe procedure. The common flexor origin on themedial aspect had been displaced anteriorly.
Despite almost complete disruption of the MCLand the muscular attachments, reduction was diffi-cult. The open wound was surgically extended.Reduction was achieved but there was inherentinstability and K wiring of the medial epicondylewas performed (Figs. 4 and 5).
The joint was irrigated with normal saline thor-oughly and the wounds were closed. An above elbowback slab was applied and the patient concluded 1week of antibiotic treatment with cefuroxime intra-venously.
Following the procedure, examination of thechild revealed paraesthesiae in the distribution of
rved.

366 D. Lui et al.
Figure 1 Photograph showing the open dislocation ofthe distal humerus though the anterior cubital fossa. (A)Note the median nerve and a cutaneous branch drapedover the trochlea. The medial (left) side shows completedisruption of the common flexor origin. Also note thedebris surrounding and inside the wound.
Figure 3 Lateral X-ray of elbow. Posterior dislocation ofelbow. Humerus displaced anteriorly.
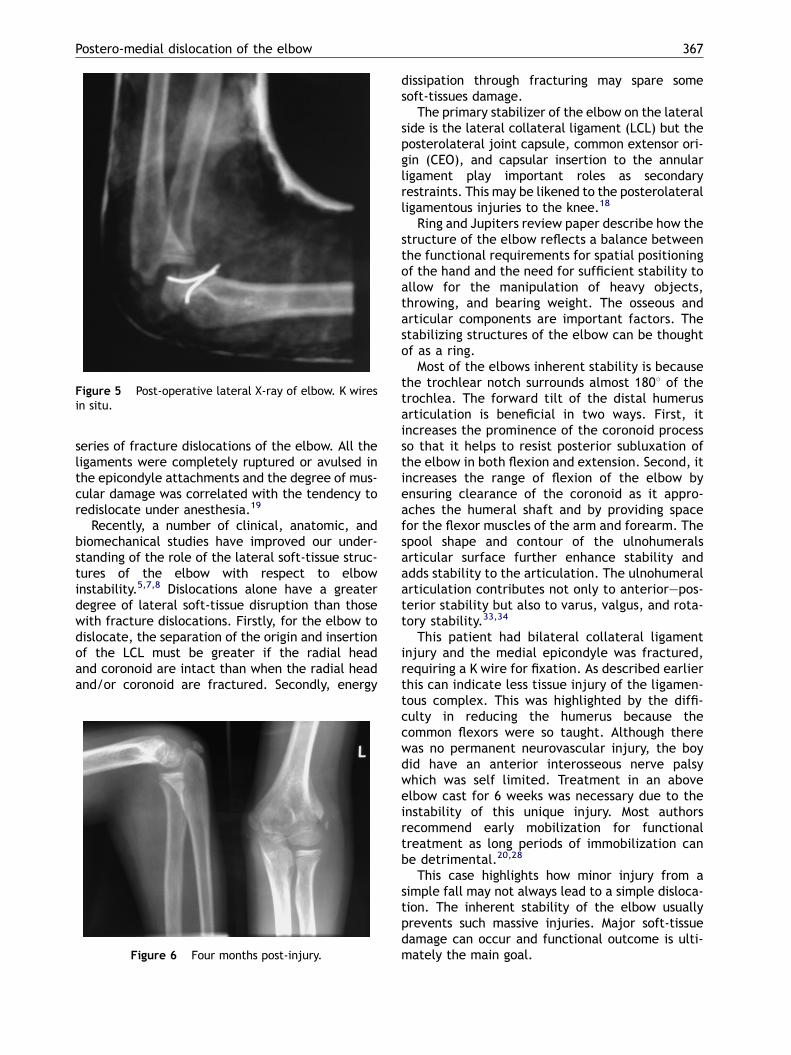
the anterior interosseous nerve. The elbow wasmaintained in an above elbow cast for 6 weeks.Serial radiographs were taken to monitor alignment(Fig. 6). Physiotherapy was instigated and at 6months had excellent functional recovery. His rangeof motion was 5—1308 and there was no neurovas-cular injury remaining.
Discussion
There are several reports documenting neurovascu-lar injury particularly brachial artery injury withclosed elbow dislocations. Open dislocations and
Figure 2 AP X-ray of elbow. Posterio-medial dislocation.
brachial artery injury is rare.35 Closed elbow dis-locations in adults are often simply treated incasualty after sedation and these usually reduceeasily.
There is significant instability and ligamentousinjury following dislocation of the elbow. In mostcases ligamentous ruptures are combined with rup-ture or avulsion of the muscular origins at theepicondyles. In a study by Josefsson et al., surgicalexposure and ligament suture were performed on a
Figure 4 Post-operative AP X-ray of elbow. K wires insitu medial epicondyle.
Postero-medial dislocation of the elbow 367
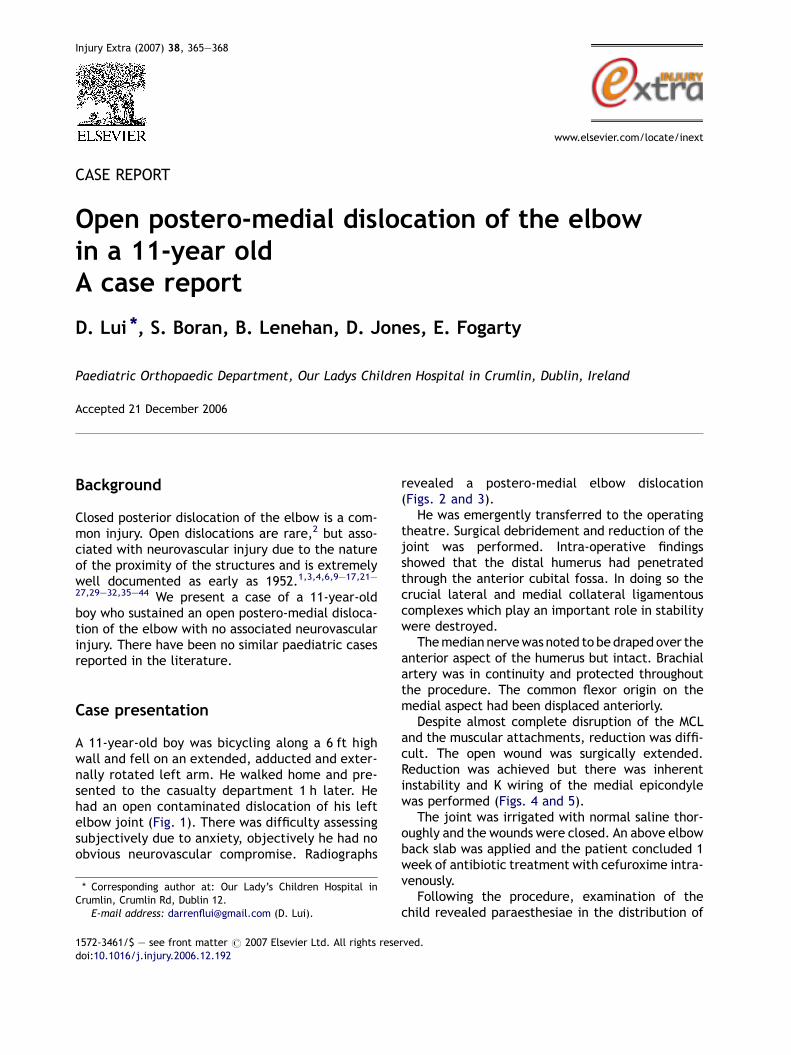
Figure 5 Post-operative lateral X-ray of elbow. K wiresin situ.
series of fracture dislocations of the elbow. All theligaments were completely ruptured or avulsed inthe epicondyle attachments and the degree of mus-cular damage was correlated with the tendency toredislocate under anesthesia.19
Recently, a number of clinical, anatomic, andbiomechanical studies have improved our under-standing of the role of the lateral soft-tissue struc-tures of the elbow with respect to elbowinstability.5,7,8 Dislocations alone have a greaterdegree of lateral soft-tissue disruption than thosewith fracture dislocations. Firstly, for the elbow todislocate, the separation of the origin and insertionof the LCL must be greater if the radial headand coronoid are intact than when the radial headand/or coronoid are fractured. Secondly, energy
Figure 6 Four months post-injury.
dissipation through fracturing may spare somesoft-tissues damage.
The primary stabilizer of the elbow on the lateralside is the lateral collateral ligament (LCL) but theposterolateral joint capsule, common extensor ori-gin (CEO), and capsular insertion to the annularligament play important roles as secondaryrestraints. This may be likened to the posterolateralligamentous injuries to the knee.18
Ring and Jupiters review paper describe how thestructure of the elbow reflects a balance betweenthe functional requirements for spatial positioningof the hand and the need for sufficient stability toallow for the manipulation of heavy objects,throwing, and bearing weight. The osseous andarticular components are important factors. Thestabilizing structures of the elbow can be thoughtof as a ring.
Most of the elbows inherent stability is becausethe trochlear notch surrounds almost 1808 of thetrochlea. The forward tilt of the distal humerusarticulation is beneficial in two ways. First, itincreases the prominence of the coronoid processso that it helps to resist posterior subluxation ofthe elbow in both flexion and extension. Second, itincreases the range of flexion of the elbow byensuring clearance of the coronoid as it appro-aches the humeral shaft and by providing spacefor the flexor muscles of the arm and forearm. Thespool shape and contour of the ulnohumeralsarticular surface further enhance stability andadds stability to the articulation. The ulnohumeralarticulation contributes not only to anterior—pos-terior stability but also to varus, valgus, and rota-tory stability.33,34
This patient had bilateral collateral ligamentinjury and the medial epicondyle was fractured,requiring a K wire for fixation. As described earlierthis can indicate less tissue injury of the ligamen-tous complex. This was highlighted by the diffi-culty in reducing the humerus because thecommon flexors were so taught. Although therewas no permanent neurovascular injury, the boydid have an anterior interosseous nerve palsywhich was self limited. Treatment in an aboveelbow cast for 6 weeks was necessary due to theinstability of this unique injury. Most authorsrecommend early mobilization for functionaltreatment as long periods of immobilization canbe detrimental.20,28
This case highlights how minor injury from asimple fall may not always lead to a simple disloca-tion. The inherent stability of the elbow usuallyprevents such massive injuries. Major soft-tissuedamage can occur and functional outcome is ulti-mately the main goal.

368 D. Lui et al.
References
1. al-Qattan MM, Zuker RM, Weinberg MJ, McKee N, McCall J.The use of a shunting catheter for a ruptured brachial arteryfollowing open elbow dislocation. Hand Surg Br 1994;19(6):788—90.
2. Alonso JA, Roy BR, Shaw DL. Open antero-lateral dislocationof the elbow. A case report. BMC Musculoskelet Disord2002;3:1.
3. Amsallem JL, Blankstein A, Bass A, Horoszowski H. Brachialartery injury. A complication of posterior elbow dislocation.Orthop Rev 1986;15(6):379—82.
4. Baulot E, Giroux EA, Ciry-Gomez M, Grammont PM. Brachialisarteria rupture following closed posterior elbow dislocation.Case report and literature review. Ann Chir Main Memb Super1997;16(3):258—62.
5. Cohen MS, Hastings II H. Rotatory instability of the elbow. Theanatomy and role of the lateral stabilizers. J Bone Joint SurgAm 1997;79(2):225—33.
6. Connolly JF, Duwelius PJ. Vascular injury associated with aposterior elbow dislocation. Nebr Med J 1985;70(4):124—6.
7. Dunning CE, Zarzour ZD, Patterson SD, Johnson JA, King GJ.Ligamentous stabilizers against posterolateral rotatoryinstability of the elbow. J Bone Joint Surg Am 2001;83-A(12):1823—8.
8. Dunning CE, Zarzour ZD, Patterson SD, Johnson JA, King GJ.Muscle forces and pronation stabilize the lateral ligamentdeficient elbow. Clin Orthop Relat Res 2001;(388):118—24.
9. Endean ED, Veldenz HC, Schwarcz TH, Hyde GL. Recognitionof arterial injury in elbow dislocation. J Vasc Surg 1992;16(3):402—6.
10. Ferrera PC. Elbow dislocation complicated by brachial arterylaceration. Am J Emerg Med 1999;17(1):103—5.
11. Fleischer G, Fletcher JP, Whiteway DW. Compound elbowdislocation and brachial artery rupture. Aust NZ J Surg1980;50(4):408—9.
12. Floyd III WE, Gebhardt MC, Emans JB. Intra-articular entrap-ment of themedian nerve after elbow dislocation in children.J Hand Surg Am 1987;12(5 Pt 1):704—7.
13. Friedmann E. Simple rupture of the brachial artery, sustainedin elbow dislocation. JAMA 1961;177:208—9.
14. Goldman MH, Kent S, Schaumburg E. Brachial artery injuriesassociated with posterior elbow dislocation. Surg GynecolObstet 1987;164(2):95—7.
15. Henderson RS, Robertson IM. Open dislocation of the elbowwith rupture of the brachial artery. J Bone Joint Surg Br B1952;34(4):636—7.
16. Hennig K, Franke D. Posterior displacement of brachial arteryfollowing closed elbow dislocation. J Trauma 1980;20(1):96—8.
17. Hofammann III KE, Moneim MS, Omer GE, Ball WS. Brachialartery disruption following closed posterior elbow dislocationin a child–—assessment with intravenous digital angiography.A case report with review of the literature. Clin Orthop RelatRes 1984;(184):145—9.
18. Hughston JC, Jacobson KE. Chronic posterolateral rotatoryinstability of the knee. J Bone Joint Surg Am 1985;67(3):351—9.
19. Josefsson PO, Johnell O, Wendeberg B. Ligamentous injuriesin dislocations of the elbow joint. Clin Orthop Relat Res1987;(221):221—5.
20. Jupiter JB, O’Driscoll SW, Cohen MS. The assessment andmanagement of the stiff elbow. Instr Course Lect 2003;52:93—111.
21. Kerin R. Elbow dislocation and its association with vasculardisruption. J Bone Joint Surg Am 1969;51(4):756—8.
22. Louis DS, Ricciardi JE, Spengler DM. Arterial injury: acomplication of posterior elbow dislocation. A clinicaland anatomical study. J Bone Joint Surg Am 1974;56(8):1631—6.
23. Mains DB, Freeark RJ. Report on compound dislocation of theelbow with entrapment of the brachial artery.. Clin OrthopRelat Res 1975;(106):180—5.
24. Manouel M, Minkowitz B, Shimotsu G, Haq I, Feliccia J.Brachial artery laceration with closed posterior elbow dis-location in an eight year old. Clin Orthop Relat Res1993;(296):109—12.
25. Marcheix B, Chaufour X, Ayel J, Hollington L, Mansat P, BarretA, et al. Transection of the brachial artery after closedposterior elbow dislocation. J Vasc Surg 2005;42(6):1230—2.
26. McMurtry IA, Bhullar TJ. Occult elbow dislocation: a rarecause of upper limb arterial insufficiency. J R Army Med Corps2000;146(3):230—1.
27. Nicoloff M, Dittmer H. Closed elbow dislocation with ruptureof the brachial artery. Unfallchirurg 1999;102(4):329—31.
28. O’Driscoll SW, Jupiter JB, Cohen MS, Ring D, McKee MD.Difficult elbow fractures: pearls and pitfalls. Instr CourseLect 2003;52:113—34.
29. Peabody CN. Rupture of the brachial artery in closed elbowdislocation: case report. Mil Med 1978;143(5):328—9.
30. Pearce MS. Radial artery entrapment. A rare complication ofposterior dislocation of the elbow. Int Orthop 1993;17(2):127—8.
31. Platz A, Heinzelmann M, Ertel W, Trentz O. Posterior elbowdislocation with associated vascular injury after blunttrauma. J Trauma 1999;46(5):948—50.
32. Reynders P, Broos P, Stoffelen D. Brachial artery injury inclosed posterior elbow dislocation case report. Acta OrthopBelg 2001;67(1):73—6.
33. Ring D, Jupiter JB. Fracture-dislocation of the elbow. HandClin 2002;18(1):55—63.
34. Ring D, Jupiter JB. Fracture-dislocation of the elbow. J BoneJoint Surg Am 1998;80(4):566—80.
35. Rubens MK, Aulicino PL. Open elbow dislocation with brachialartery disruption: case report and review of the literature.Orthopedics 1986;9(4):539—42.
36. Sadat-Ali M. Brachial artery injury in closed elbow disloca-tion. Case report and review of literature. Arch OrthopTrauma Surg 1990;109(5):288—90.
37. Seidman GD, Koerner PA. Brachial artery rupture associatedwith closed posterior elbow dislocation: a case report andreview of the literature. J Trauma 1995;38(2):318—21.
38. Slowik GM, Fitzimmons M, Rayhack JM. Closed elbow disloca-tion and brachial artery damage. J Orthop Trauma1993;7(6):558—61.
39. Squires NA, Tomaino MM. Brachial artery rupture withoutmedian nerve dysfunction after closed elbow dislocation. AmJ Orthop 2003;32(6):298—300.
40. Sturm JT, Rothenberger DA, Strate RG. Brachial artery disrup-tion following closed elbow dislocation. J Trauma 1978;18(5):364—6.
41. Taub PJ, Giannikis G, Shen HY, Kim U. Brachial artery trans-ection following closed elbow dislocation. J Trauma1999;47(1):176—8.
42. Thomas PJ, Noellert RC. Brachial artery disruption afterclosed posterior dislocation of the elbow. Am J Orthop1995;24(7):558—60.
43. Voiglio EJ. Brachial artery transection following closed elbowdislocation. J Trauma 2000;49(3):572—3.
44. Wilmshurst AD, Millner PA, Batchelor AG. Brachial arteryentrapment in closed elbow dislocation. Injury 1989;20(4):240—1.