Embed Size (px)
Citation preview

Open Capsular Release of the Elbow
William R. Beach, M.D.

“The Column Procedure: A Limited Lateral Approach for Extrinsic Contracture of the
Elbow”
• Mansat and Morrey, JBJS Nov. 1998.

Classification
• Extra-articular or extrinsic– capsule, ligament, muscle or combination
– heterotopic ossification of the soft tissue
• Intra-articular or intrinsic– articular cartilage abnormality

Conservative Treatment of Elbow Stiffness
• Flexion and/or extension splints– best if begun early
– dynamic splinting if tolerated
• Manipulation under anesthesia

Surgical Release
• Arthroscopic
• Open

Advantages of an Open Approach
• Safer and easier for most surgeons
• More predictable result
• Better anterior visualization of a severely scarred anterior compartment
• Easier conversion to conjunctive procedures

Disadvantages of an Open Approach
• Larger incision
• More difficult inspection of the entire joint
Indications for Open Release (Anterior and/or Posterior)
• Symptomatic extrinsic extension deficit (flexion contracture) – 20-30 degrees “gray zone”– >30 degrees
• Symptomatic extrinsic flexion deficit (extension contracture)– Flexion < 110 degrees

Open Conjunctive Procedures
• Biceps tendon lengthening
• Brachialis myotomy
• Collateral ligament release
• Radial head resection

Open Release Surgical Technique
• Pre-operative and intra-operative assessment of neurovascular status and range of motion
• Patient in supine position
• High arm tourniquet

Technique
• Exsanguinate the arm and elevate the tourniquet
• Prep and drape the arm in a sterile fashion

Incisions• Posterior
– long and requires large skin flaps
• Medial– requires mobilization of the ulnar nerve
• Anterior– greater risk to the neurovascular structures
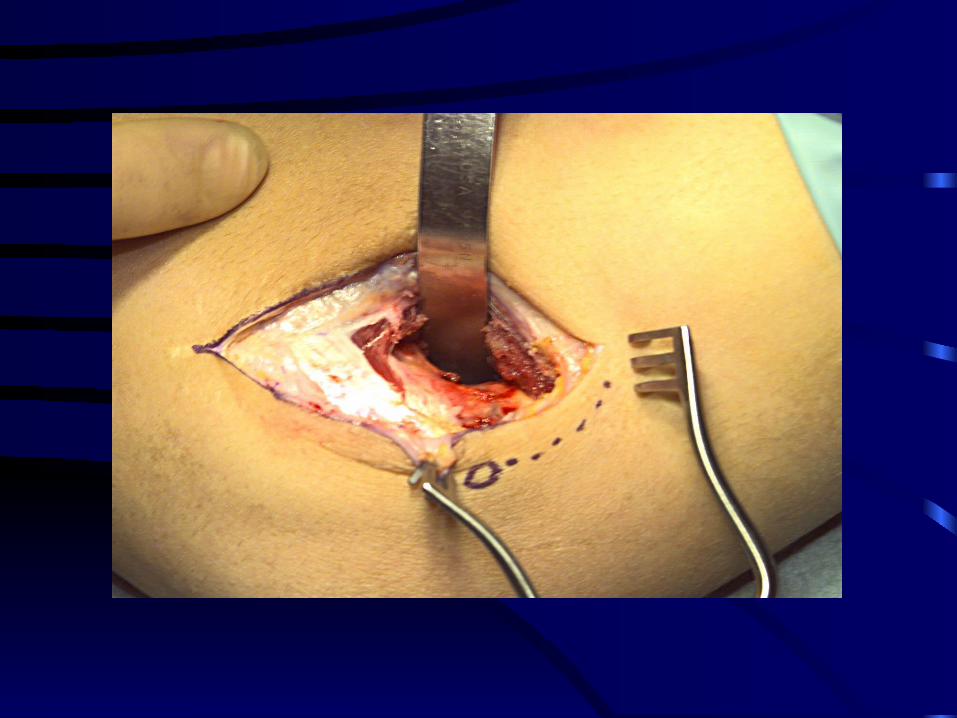
• Lateral– Preferred for safety and versatility

Interval• Along the anterior border of the lateral humeral
epicondyle
• The distal 1/3 of the brachioradialis and the extensor carpi radialis longus and brevis are released off the epicondyle
• This will allow exposure of the anterior joint capsule
• The capsule is often scarred to the bone extending to the articular surface

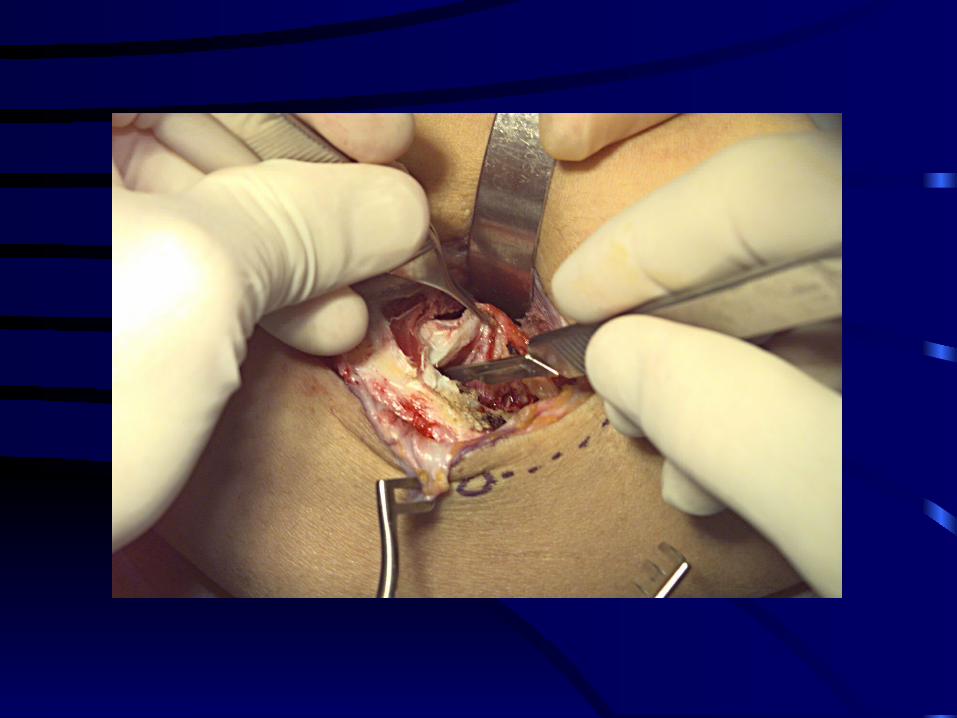
Capsule
• Once the capsule is identified a retractor is placed between the capsule and the brachialis
• This retractor must be long enough to extend across the entirety of the anterior elbow and wide enough to provide protection the anteriorly retracted neurovascular structures

“The Release”
• The capsule is incised from the radial side of the humerus from as far proximal as possible and down to the joint line
• The release is wide (2 cm) radially and tapers medially
• The ulnar side of the capsule is hard to visualize so go carefully

“Fine Tuning”
• With the capsule released and the retractor removed palpate the joint and slowly extend the elbow to determine if any capsule remains
• If so replace the retractor and take an elevator and bluntly finish the capsular release

Flexion Deficit
• Flex the elbow and determine if the coronoid process or the radial head abuts the anterior humerus
• If so a coronoid process osteotomy or debridement of the anterior lateral surface of the humerus may be required

Posterior Release
• At the level of the epicondyle the anconeus and triceps are elevated off the posterior humeral surface
• The posterior joint capsule is identified and incised

Posterior Release
• The olecranon process and olecranon fossa are identified and inspected
• The fossa is debrided of fibrous tissue, osteophytes or loose bodies
• Osteophytes are aggressively removed from the olecranon process

Limited Flexion
• Determine if the triceps tendon or muscle are adherent to the posterior humerus
• If so a Cobb elevator is used to release the adhesions

Final Check
• With all retractors removed palpate both the anterior and posterior sites to determine if there are any restrictions to flexion or extension
• If so address these structures

Post-operative Protocol
• Neurovascular exam in recovery room
• Extension splint from the axilla to the wrist
• Pad the wrist excessively to avoid a pressure ulcer
• Hang the arm in a “sky hook” sling to elevate the arm overhead for 18-24 hours

Post-operative Protocol
• 1st day post-op - axillary catheter (in-dwelling) or scalene block
• CPM for ROM as tolerated
• DC 2nd day to daily PT and home CPM
• Extension or flexion splinting
Post-operative Protocol
• Check incision 7-10 days and remove sutures
• Indocin or NSAID to limit swelling and HO
• Dynamic splinting or turnbuckle splints if motion is slow