Embed Size (px)
Citation preview

Open Access Scheduling “Doing today‟s work today”
MedInf404- DL Winter2011 Biljana Spasic Claire McCardle

Clinics
Edinburgh Hospital and Clinics •350 bed hospital •Emergency Department •20 Ambulatory Multi –Specialty Clinics •20K Discharges •200K clinic visits •Clinic practices 4-10 physicians per practice
•Clinic Services ( high volume) •Family Practice •Urgent Care •Ob/GYN •Pediatrics

Problem Definition
Traditional Clinic Scheduling ◦ Wait time for next routine appointment (3rd next
available appt > 45 days) ◦ Patient cycle time is currently 75minutes ◦ Care diversion to ED & Urgent Care ◦ Managing „no shows‟ & triaging calls ; No show rate of
50% ◦ Capacity planning „overbook‟ ◦ Managing appointment back logs
Impact
◦ Challenges with care coordination (28% of patients see PCP)
◦ Inadequate and timely access to a PCP is a major source of patient dissatisfaction
◦ Staff dissatisfaction

Objectives
1. Endorsement
◦ “Open Access‟ as a strategic initiative
2. Review
◦ Proposal for “Open Access” plan
3. Approval
◦ Budget approval for feasibility study

“Do Today’s Work Today”
Open Access
◦ Same day appointment scheduling
◦ Match patient to Primary Care Physician
◦ Appointments are scheduled by availability not by appointment type e.g., no differentiation between urgent and routine appointments
Paradigm Shift ◦ Underlying theory: demand is predictable
◦ Balance demand and provider capacity
◦ Simplify appointment types
◦ Optimize and consolidate services for each visit move from episodic care to continuity of care

Historical Challenges
◦ Adoption Physicians “volume is money” Giving up control of schedule Skepticism existing resources can manage demand Benefits not clearly defined for staff
◦ Cultural Routine care can “wait”
◦ Logistics Poor demand and capacity planning Lack of monitoring and reevaluation of demand Lack of contingency plans

Current Trends
Patient
Consumer Driven Market
New Business Models
Quality
Tech Advance
s
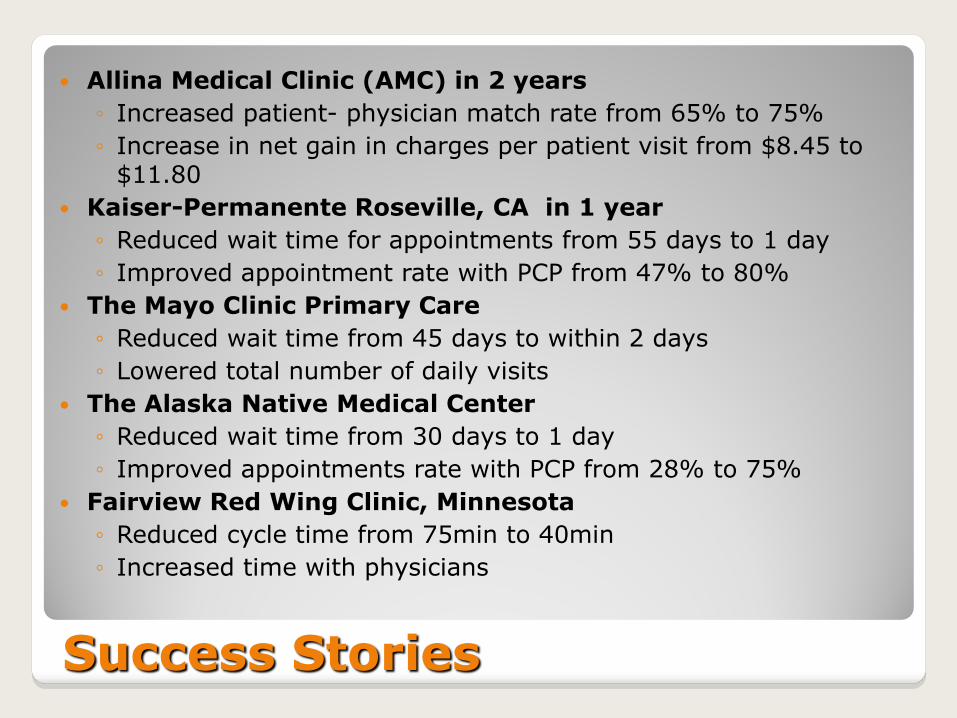
Success Stories
Allina Medical Clinic (AMC) in 2 years
◦ Increased patient- physician match rate from 65% to 75%
◦ Increase in net gain in charges per patient visit from $8.45 to $11.80
Kaiser-Permanente Roseville, CA in 1 year
◦ Reduced wait time for appointments from 55 days to 1 day
◦ Improved appointment rate with PCP from 47% to 80%
The Mayo Clinic Primary Care
◦ Reduced wait time from 45 days to within 2 days
◦ Lowered total number of daily visits
The Alaska Native Medical Center
◦ Reduced wait time from 30 days to 1 day
◦ Improved appointments rate with PCP from 28% to 75%
Fairview Red Wing Clinic, Minnesota
◦ Reduced cycle time from 75min to 40min
◦ Increased time with physicians

Proposal
Strategy &
Assessment
Phase 2
Rollout Operations,
Support
Vision Clinic 3 Clinic 4 Clinic n
Monitoring,
Improvement,
Support
Feasibility Clinic 2 Clinic 1
Phase 1
Pilot
Q2 2011 Q4 2011 Q4 2012
Vision
•Open Access strategic initiative
Feasibility
•Proposal for governance and adoption •Analysis of capacity and demand • Work effort for process redesign • Technical solution proposal and estimates • Plan and cost for the pilot • High Level Plan and cost for the project • Site visits or calls • Total cost of ownership • Benchmarking
Pilot • Scheduling process • Measures • Technical solution
Review and
approval,
start Pilot
Review and
approval,
start Rollout
Review and
approval,
close Project
BOD review
and approval,
start
Feasibility

Benefits
Practices reduce or
eliminate delays in
patient care without
adding resources
Demand for
appointments
decreases
Patients see their
own physicians
more often •enhanced continuity of care
•better health care
•higher patient satisfaction
Medical practices
often realize cost and
efficiency savings •clinical time used efficiently
•reduced hours managing “no
shows” and backlogs

Measures
Appointment Availability
measure un-booked capacity
third next available appointment
Demand include patients who tried to access the system but were unsuccessful
Continuity number of appointments with PCP
Panel size balance provider panels for size and acuity
Productivity office efficiency
No-shows number of missed appointments
Cycle time elapsed time from patient‟s arrival to patient‟s departure
Satisfaction patient
staff
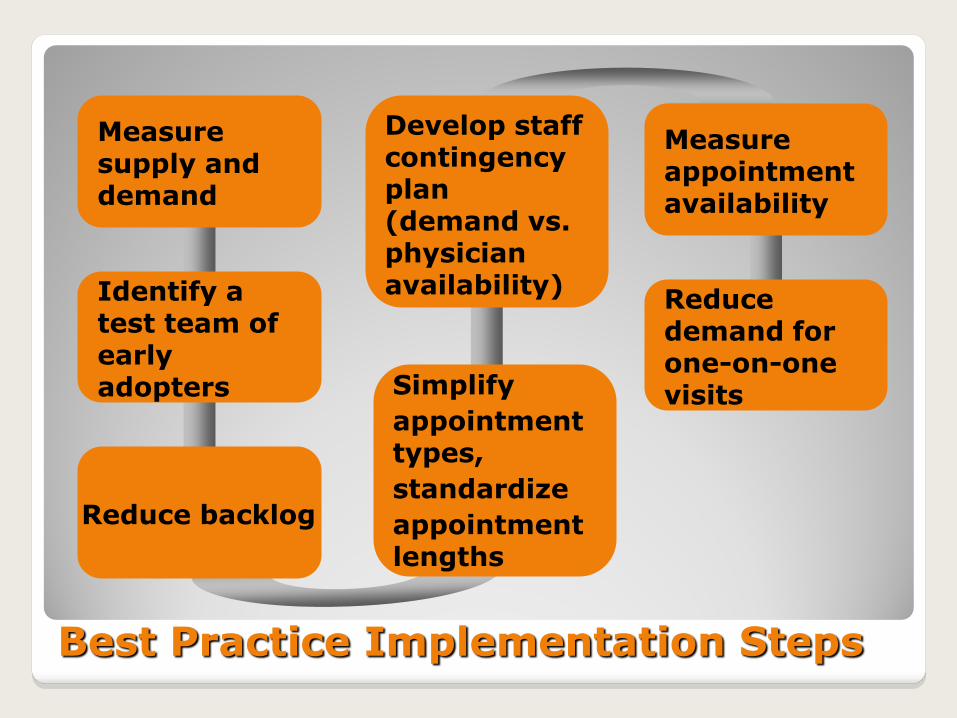
Best Practice Implementation Steps
Measure supply and demand
Identify a test team of early adopters Simplify
appointment types,
standardize
appointment lengths
Reduce backlog
Develop staff contingency plan (demand vs. physician availability)
Reduce demand for one-on-one visits
Measure appointment availability

Duration: ◦ three months
Resources: ◦ Internal
◦ Consultants
◦ Site visits
Cost: ◦ $100,000.00
Feasibility Study Requirements

Summary, Approvals
Endorsement
Review
Approval
•Open Access as a strategic initiative
•Proposal for “Open Access” plan
•Budget for the Feasibility Study
Questions

References
Murray M, Tantau,C. Exploding the Access Paradigm (FPM,September 2000: 45-50)
UD Department of Health & Human Services, AHRQ Agency for Healthcare Research and Quality, Open Access Scheduling for Routine and Urgent Appointments http://www.cahps.ahrq.gov/qiguide/content/interventions/OpenAccessScheduling.aspx
Murray M, Bodenheimer T, Rittenhouse D, et al. Improving timely access to primary care: case studies of the advanced access model. JAMA 2003;289(8): 1042-6.
Murray M and Tantau C. Must patients wait? Jt Comm J Qual Improv 1998;24(8): 423-5.
Murray M and Berwick DM Advanced access: reducing waiting and delays in primary care. JAMA 2003;289(8): 1035-40.
Commander‟s Guide to Access Success Appendix J 082807





























