Embed Size (px)
Citation preview

Telemonitoring after dischargefrom hospital with heart failurecost-effectiveness modelling ofalternative service designs
Praveen Thokala1 Hassan Baalbaki1 Alan Brennan1 Abdullah Pandor1
John W Stevens1 Tim Gomersall1 Jenny Wang1 Ameet Bakhai2
Abdallah Al-Mohammad3 John Cleland4 Martin R Cowie5 Ruth Wong1
To cite Thokala PBaalbaki H Brennan A et alTelemonitoring afterdischarge from hospital withheart failurecost-effectiveness modellingof alternative service designsBMJ Open 20133e003250doi101136bmjopen-2013-003250
Prepublication history andadditional material for thispaper is available online Toview these files please visitthe journal online(httpdxdoiorg101136bmjopen-2013-003250)
Received 18 May 2013Revised 10 July 2013Accepted 30 July 2013
For numbered affiliations seeend of article
Correspondence toDr Praveen Thokalapthokalasheffieldacuk
ABSTRACTObjectives To estimate the cost-effectiveness ofremote monitoring strategies versus usual care foradults recently discharged after a heart failure (HF)exacerbationDesign Decision analysis modelling of cost-effectiveness using secondary data sourcesSetting Acute hospitals in the UKPatients Patients recently discharged (within 28 days)after a HF exacerbationInterventions Structured telephone support (STS)via human to machine (STS HM) interface (2) STS viahuman to human (STS HH) contact and (3) hometelemonitoring (TM) compared with (4) usual careMain outcome measures The incremental cost perquality-adjusted life year (QALY) gained by eachstrategy compared to the next most effective alternativeand the probability of each strategy being cost-effectiveat varying willingness to pay per QALY gainedResults TM was the most cost-effective strategy inthe scenario using these base case costs Comparedwith usual care TM had an estimated incremental costeffectiveness ratio (ICER) of pound11 873QALY whereasSTS HH had an ICER of pound228 035QALY against TMSTS HM was dominated by usual care Thresholdanalysis suggested that the monthly cost of TM has tobe higher than pound390 to have an ICER greater thanpound20 000QALY against STS HH Scenario analysesperformed using higher costs of usual care highercosts of STS HH and lower costs of TM do notsubstantially change the conclusionsConclusions Cost-effectiveness analyses suggest thatTM was an optimal strategy in most scenarios butthere is considerable uncertainty in relation to cleardescriptions of the interventions and robust estimationof costs
BACKGROUNDHeart failure (HF) is associated with highlevels of morbidity and mortality with thehighest risk being immediately after
discharge from hospital1 A total of 20ndash30of patients are readmitted within 30 daysrising to 50 at 6 months2 Patients who aredischarged have around 28 risk of mortal-ity within the first year after HF discharge3
Strategies to slow disease progression areneeded for at-risk patients to improve theprognosis even among those receivingoptimal pharmaceutical therapy4
Remote monitoring (RM) of indicators ofdeterioration (eg weight arrhythmia blood
ARTICLE SUMMARY
Article focus Decision analysis modelling using secondary
data sources to estimate the cost-effectiveness ofremote monitoring strategies versus usual carefor adults recently discharged after a heart failureexacerbation
Clinical effectiveness parameters were estimatedfrom a network meta-analysis of the availableevidence and costs were estimated usinglsquobottom uprsquo costing methods
Key messages Base case cost-effectiveness analyses suggest
that telemonitoring during office hours (TM) isthe most cost-effective strategy at a threshold ofpound20 000QALY albeit with uncertainty
Scenario analyses performed (using higher usualcare costs lower TM costs and higher TM costs)do not substantially change the conclusions
Strengths and limitations of this study The model uses robust evidence from a recent
network-meta-analysis and appropriate sensitivityanalyses are presented around other keyparameters
The effectiveness parameters used are a synthe-sis of heterogeneous estimates and uncertaintiesstill remain about the assumptions made in thebottom-up costing of different scenarios
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 1
Open Access Research
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
pressure intrathoracic impedance heart rates duringrest and exertion and symptom control) can facilitateearly detection of clinically significant changes as well asearlier intervention to restabilise the syndrome preventemergency admissions and avoid complications5 RMcan be broadly classified into telemonitoring (TM) inwhich physiological data are electronically transmitted toa healthcare team and structured telephone support(STS) that is the use of phone calls usually by specialistnurses to deliver self-care support andor manage-ment6 For STS support can be provided by human-to-human contact (HH) or via a human-to-machine inter-face (HM) that is STS with an interactive responsesystem (eg a voice-interactive system) For TM supportcan be provided during office hours only or 24 h day7 daysweek (247) though few studies have used thelatter approachThe cost-effectiveness of an RM strategy can be esti-
mated by comparing the outcomes and costs associatedwith the strategy to the next most effective alternative Ifthese outcomes are estimated as quality-adjusted lifeyears (QALYs) then the incremental cost-effectivenessratio (ICER) or cost per QALY gained can be calcu-lated and compared to alternative uses of healthcarefunding In the UK (UK) the National Institute forHealth and Clinical Excellence (NICE) typically recom-mends in favour of funding interventions with an ICERbelow thresholds of pound20 000QALY requires consider-able clinical benefit to recommend funding interven-tions between pound20 000 and pound30 000QALY andrecommends against funding interventions with anICER above these thresholds The aim of this paper is toestimate the incremental cost per QALY of RM strategiescompared with usual care so as to determine which RMstrategy should be recommended according to typicalNICE thresholds for cost-effectiveness
METHODSModel scopeA Markov model was developed using MS Excel software(Microsoft Corporation) to estimate the cost-effectivenessof RM interventions with usual care for patients dis-charged in the past 28 days with a HF-related hospital-isation7 measured as the incremental cost per QALYgained by each strategy compared with the next mosteffective alternative on the cost-effectiveness frontierCost-effectiveness results are estimated as mean values of10 000 probabilistic sensitivity analysis (PSA) runs witheach PSA run using different estimates for the risks HRscosts and utilities sampled from probability distributionsrepresenting uncertainty in the parameter estimatesAdditionally the probability that each strategy would bethe most cost-effective was calculated at different thresh-olds for willingness to pay (WTP) for health gainCost-effectiveness acceptability curves were constructedby plotting the probability of each strategy being cost-effective against the WTP threshold
The following strategies postdischarge interventionswere tested in the modelA Usual careB STS HH (structured telephone support with
human-to-human contact)C STS HM (structured telephone support with
human-to-machine interface) andD TM (ie telemonitoring with transmitted data
reviewed by medical staff or medical support pro-vided during office hours)
The clinical effectiveness parameters of these threeRM strategies were estimated from a networkmeta-analysis of the available evidence8 and costs wereestimated using lsquobottom uprsquo costing methods It wasassumed that the interventions were provided for the6 months following discharge from the hospital as themajority of the RM trials included in the networkmeta-analysis used a 6-month follow-up duration8 At theend of 6 months all patients were assumed to receiveusual care as per the NICE Clinical Guidelines for theManagement of Adults with Chronic Heart Failure9 irre-spective of whether they received intervention or post-discharge usual care during the treatment period
Model structureIn the Markov model two different states wereconsideredA Alive at homeB DeadThe Markov model used a monthly cycle length with
half-cycle correction and assigned each patient with amonthly probability of death based on the time sincedischarge and the type of treatment In each period thepatients who were alive were under the risk of anaverage number of monthly rehospitalisations that isreadmissions to a hospital for HF or other causes Eachpatient then accrued lifetime QALYs and healthcarecosts according to their hospitalisation and treatmentstatus The model used a 30 year (patient lifetime)horizon although the impact of each intervention wasfor the first 6 months after an initial discharge Thecosts and QALYs were discounted at an annual discountrate of 35 and the economic perspective of the modelwas that of the NHS in England and Wales Repeat inter-ventions after repeat hospitalisations were not consid-ered in this model
Baseline mortality and hospitalisationThe baseline monthly probabilities of death were esti-mated from Candesartan in Heart failure Assessment ofReduction in Mortality and morbidity (CHARM) study10
which included 7572 patients with a mean age of655 years followed up for 38 months as it assessed theinfluence of non-fatal hospitalisation for heart failure onsubsequent mortality The data from the CHARMstudy10 showed that the mortality risk was highest imme-diately after hospital discharge and then decreased overtime as shown in table 1
2 Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
The mean numbers of HF-related and other-causehospitalisations (estimated as all-cause hospitalisationsminus the HF-related hospitalisations) were estimatedfrom a meta-analysis of 21 studies (5715 patientsmedian age 707 ranging from 45 to 78 years) reportedby Klersy et al11 The average number of monthlyHF-related and all cause rehospitalisations for patientsin usual care are as shown in table 2
Effectiveness of interventionsThe effectiveness parameters in the economic model werethe HRs for all-cause mortality all-cause hospitalisationsand HF-related hospitalisations for the different interven-tions (ie STS HM STS HM and TM) against standardcare These effectiveness parameters were estimated froma network meta-analysis (NMA) of 21 RM studies8 (total6317 patients with the mean age across studies rangingfrom 57 to 78 years) and applied to the baseline para-meters to estimate the hospitalisation and mortality riskparameters for the different interventions It was assumedthat the treatment effectiveness (and costs) lasts only forthe treatment duration of 6 months after which the base-line risks of hospitalisation and mortality are appliedIt should be noted that considerable heterogeneity
was identified in the manner in which RM and usualcare were performed among the studies included inNMA8 which resulted in heterogeneity between studiesin the estimate of HRs For example in RM there wasvariation between studies in the type of devices usedparameters monitored and the protocols for triage andfollow-up In particular the data from Dar et al12
(Home-HF trial conducted in three district general hos-pitals in West London) appeared to be inconsistent withthe data from the remaining studies because it showed ahigher incidence of mortality among the TM groupthan the usual care group However the 6-month
mortality rate in the usual care group (55) was sub-stantially lower than would be expected in a HF cohortreceiving care outside the context of a clinical trial (iebetween 13 and 21)3 which the authors attributedto the high-quality usual care (provided by a HF nursespecialist and a consultant with an interest in HF) Theimpact of this study was assessed in sensitivity analysesand HRs from both the NMAs are presented in table 3On deciding which of these results are most representa-
tive of their setting the key question for decision-makersrelate to the inclusion of the Home-HF study12 in theeffectiveness meta-analyses If one accepts that usual careis best represented by the usual care arm in the Home-HFstudy12 which is the only study showing a statistically signifi-cant difference in effectiveness of usual care over RMthen the results including Home-HF study12 might be con-sidered more relevant than those without If on the otherhand one considers that the performance of usual care isbetter represented by the other studies and that usual carein Home-HF study12 is not representative of current usualcare then the results excluding Home-HF study12 mightbe more generalisable This consideration predominantlyaffects the HRs around the telemonitoring interventiononly and does not impact substantially on the structuretelephone service interventions
Health-related quality of lifeA review was conducted to estimate the health-relatedquality of life (HRQoL) and four studies were found13ndash16 all of which reported utilities for recently dischargedHF patients under usual care around 057 to 06 Therewas no quantified evidence on the extent to which RMimproves the HRQoL of the patients in the RM studiesincluded in NMA and thus the same utility values wereused for HF patients in usual care as well as (each of thethree) RM strategies in the economic model The disutil-ity caused by rehospitalisation for HF was estimated as01 based on a study by Yao et al17 who estimated the dis-utility to be equivalent to the utility of one health statelower in terms of the New York Heart Association(NYHA) class and this disutility was assumed to last for1 year In the absence of evidence regarding the disutil-ity caused by rehospitalisation for other causes (not dir-ectly HF-related) it was assumed that there was nodisutility caused by rehospitalisation for other causesA utility score of 058 was applied to the patients for
each month in the first year after discharge and a utilityscore of 067 was used after the first year Any HF-relatedhospitalisation was assumed to result in a disutility of 01for a whole year that is the utility of the patient for that
Table 2 Monthly risk of hospitalisations per patient in usual care
Source Estimate Lower 95 CI Upper 95 CI
HF-related hospitalisations Klersy et al11 00350 00325 00375
All-cause hospitalisations Klersy et al11 00875 00841 00908
Table 1 Monthly mortality probability vs time since
discharge for patients with heart failure (HF) in usual care
Time since
discharge
(in months)
Mortality
probability
per month
Lower
95 CI
Upper
95 CI
0ndash1 004622 003616 005891
1ndash3 003306 002644 004124
3ndash6 002674 002166 003306
6ndash12 002353 001964 002831
12ndash24 001866 001565 002226
gt24 001467 001127 001911
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 3
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
year was 067ndash01 that is 057 Within the PSA theuncertainty in the utility values was represented using anormal distribution using the deterministic values as themean with an SD of 0015 and estimated based on thedifference between the utilities reported by Capomollaet al13 and Iqbal et al15 while the disutility was repre-sented using a triangular distribution with (minus008 011)as the range with minus01 as the mode
CostsThe costs used in the model are (1) costs of RM inter-ventions after initial discharge only (2) costs of usualcare and (3) repeat hospitalisation costs These costs aresummarised in table 4 and are described in detail in thissectionThe RM studies did not report clearly or in detail
what was involved in the usual postdischarge care orRM thus making it difficult to accurately determine thecosts8 Owing to the variation involved in the RM inter-ventions and usual care cost scenarios were developedfor each RM classification (ie STS HM STS HH andTM) and usual care These costs were estimated using
bottom-up costing methods for a typical health organisa-tion of 250 HF patients (estimated based on the mediansize of the NHS Foundation Trusts in the UK) for aperiod of 6 months Furthermore it was assumed thatafter 6 months all patients would receive usual care asrecommended in NICE clinical guidelines for the man-agement of adults with CHF9 irrespective of whetherthey received the remote monitoring intervention orpostdischarge usual care during the intervention periodIt was assumed that the usual postdischarge care was
the same as that described in the TEN-HMS study18 andthe usual care costs were estimated by applying thehourly NHS staff rates from PSSRU 201119 to theresource use data in the TEN-HMS study18 A high costusual postdischarge care scenario was also developedbased on discussions with the clinical expert group (ABAAM JC and MRC)The total costs of RM interventions were broken down
into the costs of the device monitoring costs andmedical care costs8 The costs of the RM devices wereelicited from an expert advisory group The monitoringcosts were estimated using activity-based costing for the
Table 4 Cost parameters used in the economic model
Costs (in pound) per 6 months
Base-case
scenario
Low-cost
scenario
High-cost
scenario Source
UC pound161 ndash pound592 TEN-HMS18 Clinical opinion
STS HM pound715 pound623 pound794 Clinical opinion
STS HH pound1075 pound1051 pound1152 Clinical opinion
TM pound1051 pound801 pound1288 Clinical opinion
Usual care costs (per month) after 6 month intervention duration
UC after 6 months pound823 ndash ndash NICE HF guidelines9
Hospitalisation costs Estimate Lower 95 CI Upper 95 CI
HF-related hospitalisations pound251449 pound1857 pound2809 NHS Reference Costs for
201121
Other-cause hospitalisationsdagger pound152979 pound1129 pound1709 NHS Reference Costs for
201121
Heart failure or shock (EB03H EB03I) non-elective inpatient (long stay) including excess bed days21
daggerNon-elective inpatient (long stay and short stay) including excess bed days21
Table 3 HRs for interventions versus usual care for all-cause mortality and hospitalisations
HRs for interventions versus usual care for mortality (all-cause) and hospitalisation (all-cause and HF) from NMA
including Home-HF12 study
Type
All-cause mortality HF-hospitalisation All-cause hospitalisation
R 95 PrI HR 95 PrI HR 95 PrI
STS HH 077 (031 186) 077 (050 119) 097 (038 243)
STS HM 098 (030 323) 103 (058 177) 106 (031 361)
TM 076 (030 191) 095 (059 162) 075 (028 191)
HRs for interventions versus usual care for mortality (all-cause) and hospitalisation (all-cause and HF) from NMA
excluding Home-HF12 study
STS HH 075 (045 127) 076 (051 113) 096 (042 218)
STS HM 098 (049 195) 102 (061 169) 106 (035 322)
TM 062 (035 109) 086 (054 138) 067 (026 153)
HR hazard ratio PrI predictive interval STS HM structured telephone support via human to machine interface STS HH structuredtelephone support via human to human contact TM telemonitoring
4 Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
resources spent by the staff on triage and follow-upbased on evidence from the literature20 The costs ofmedical care for the usual care arm STS and TM armswere estimated by applying the hourly NHS staff ratesfrom PSSRU 201119 to their respective medical careresource use data reported in the TEN-HMS study18
The mean inpatient admission cost for HF-related hos-pitalisations was calculated from the weighted average ofthe costs for the HRG lsquoHeart Failure or Shockrdquo (EB03HEB03I) based on the data obtained from the NHSReference Costs for 201121 For hospital admissions forany cause other than HF it was assumed that these costswere the same as the mean cost of hospital admissionfor the general population This was estimated as aweighted average of elective inpatient admissions andnon-elective inpatient admissions (including short andlong stay) based on the data from the NHS ReferenceCosts for 201121
RESULTSThe results of the cost-effectiveness analysis using basecase costs are presented in table 5 for both estimates ofeffectiveness including and excluding data from theHome-HF study12 to address the uncertainty inthe effectiveness evidence Results are also presented forfive cost scenarios (higher usual care cost scenariolower cost scenario of TM higher cost scenario of TMlower STS cost scenario and higher STS cost scenario)and the 12 month intervention duration scenario inonline supplementary tables S1 and S2 respectivelyIn the analysis using base case costs TM is the most
cost-effective strategy at a threshold of pound20 000QALY inboth analyses that is including and excluding theHome-HF study12 TM is also the most effective strategy(ie highest QALYs gained) in the analyses that excludedthe Home-HF study12 but not in the analyses thatincluded the Home-HF study12 with STS HH providingthe highest number of expected QALYs However the
additional QALYs gained by STS HH are not worth theadditional costs of the strategy as seen in the ICERs(against TM) greater than the threshold of pound20 000QALYIn the analyses that included the Home-HF study12
there is only a 40 chance of TM being cost-effective atthe threshold of pound20 000QALY as shown in figure 1Excluding the Home-HF study12 the probability that TMduring office hours is cost-effective increases to 73(figure 2)Scenario analyses performed using higher costs of
usual care higher costs of STS HH and lower costs ofTM do not substantially change the conclusions TM wasestimated to be the most cost-effective strategy in allthese scenarios Scenario analysis performed usinghigher costs of TM (pound215month) suggested that TM isdominated by STS HH This is because a small changein the difference between costs of TM and STS HH ledto a marked change in ICERs given the small difference(00021 QALYs) in expected QALYs between STS HHand TM in the analyses that included the Home-HFstudy12 However the same scenario analysis (ie highercost of TM of pound215month) that excluded the data fromthe Home-HF study12 suggested that TM is still the mostcost-effective strategy with an ICER of pound8223QALYagainst usual care (STS HH is extendedly dominated bya combination of usual care and TM) This is due to themuch higher difference in the expected QALYs betweenSTS HH and TM (00602 QALYs) where a small changein the difference between costs of TM and STS HHcannot lead to a marked change in the ICER Thethreshold analysis suggested that the monthly cost of TMhas to be higher than pound390month to have an ICERgreater than pound20 000QALY against STS HH The ICERof TM against usual care at this monthly cost of pound390 ispound13 357QALYScenario analyses performed using different estimates
of the disutility for HF-related and other cause hospitali-sations produced results similar to that in the base case
Table 5 Summary of the economic analysis results using base case costs
Usual care STS HM STS HH TM
Total costs
Including Home-HF12 pound8478 pound8965 pound9574 pound9437
Excluding Home-HF12 pound8478 pound9087 pound9658 pound9665
Total QALYs
Including Home-HF12 24137 23633 24950 24944
Excluding Home-HF12 24137 24043 25230 25847
ICERs
Including Home-HF12 Dominated pound228 035 pound11 873
Excluding Home-HF12 Dominated Extendedly dominated pound6942
Probability of cost-effectiveness ()
Including Home-HF12 6 19 35 40
Excluding Home-HF12 1 7 19 73
Last strategy in the cost-effectiveness frontierICERs incremental cost-effectiveness ratios QALYs quality adjusted life years STS HH structured telephone support via human to humancontact STS HM structured telephone support via human to machine interface TM telemonitoring
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 5
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
analysis that is the results are robust to the variations inthe disutility of hospitalisationsScenario analysis using a 12-month treatment duration
produced similar results as in the 6-month treatmentduration scenarios TM for 12 months was also cost-effective when compared with TM for 6 months with anICER of pound14 066QALY However treating 2timesN patientsusing TM for 6 months was cost-effective with it beingdominant against a combination of treating N patientsusing TM for 12 months with the rest of the N patientsunder usual care
DISCUSSIONThe results of the base case cost-effectiveness analysessuggest that TM is expected to be the most cost-effectivestrategy at a threshold of pound20 000QALY However thereis uncertainty involved in suggesting that TM is the mostprobable cost-effective strategy and in particular thereis greater uncertainty when data from the Home-HFstudy12 is included than when it is excluded For
decision-makers the key question is whether the usualcare arm in their local setting is similar to the usual carearm in the Home-HF study12 If so then the resultsincluding the Home-HF study12 might be consideredmore relevant and if not the results excluding theHome-HF study12 might be considered more relevantThe scenario analysis performed (using higher usualcare costs lower TM costs higher TM costs and higherSTS costs) did not substantially change the conclusionsTM was estimated to be the most cost-effective strategyin all these scenarios Furthermore TM for 12 monthswas also cost-effective when compared with TM for6 months which suggests that it is cost-effective to keepthe patients on TM beyond 6 months In situations witha limited number of TM devices assuming a homoge-neous patient group it is cost-effective to treat allpatients using TM for 6 months than using TM for12 months on half the patients with the other half of thepatients under usual careThere have been two cost-effectiveness analyses studies
of RM in HF but neither considered the different RM
Figure 1 Cost effectiveness
acceptability curve for base case
economic analysis using
effectiveness data including the
Home-HF study12
Figure 2 Cost effectiveness
acceptability curve for economic
analysis using effectiveness data
excluding the Home-HF study12
6 Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
approaches separately11 22 The analysis reported byMiller et al22 was based on a single trial of STS23
whereas Klersy et al11 included data from a meta-analysisof a wide range of RM studies Miller et al22 estimatedthat STS compared with usual care had an ICER around$43 650QALY this study did not include a PSA butunivariate sensitivity analyses (ICER varying from$28 691 to $129 738 per QALY) was performed Klersyet al11 focused mainly on the effectiveness rather thanthe costs and used a time horizon of 1 year A budgetimpact analysis was presented and the differentdiagnosis-related group (DRG) reimbursement tariffgroups as a proxy for hospitalisation costs were consid-ered with cost savings per patient ranging betweeneuro3068 and euro99294 However other costs such as RMcosts and outpatient visit costs were not considered Theauthors performed scenario analyses using differentDRG costs as part of the budget analysis to address theuncertainty in the hospitalisation costs but neitherdeterministic sensitivity analysis nor PSA was performedThe Whole systems demonstrator (WSD) pro-
gramme24 a randomised controlled trial of telehealththat included over 6000 patients analysed costs and out-comes for 965 patients monitored for 12 months 534receiving telehealth and 431 receiving usual careCost-effectiveness analysis estimated the ICER atpound92 000QALY when telehealth was added to usual carefor people with chronic conditions (diabetes HF andchronic obstructive pulmonary disease (COPD))However this trial-based evaluation (with a time horizonof 1 year) potentially underestimates the health benefitsas it does not include the long-term QALYs gained fromthe reduction in mortality Furthermore the WSD ana-lysis included all patients with chronic conditions (dia-betes HF and COPD) whereas the population underconsideration in our analysis included patients who hadbeen recently discharged with HF The cost-effectivenessresults for HF patients are not yet publicly available in apeer-reviewed journal and thus it is difficult to comparethe results of the current analysis with the results of theWSD analysisThe analysis reported in this paper also has some lim-
itations that need to be taken into account Any model-ling process involves simplifications and assumptionsthat may not accurately reflect clinical practice Owingto the lack of detail provided in research studiesincluded in the NMA concerning the components ofRM packages and usual care (eg communication proto-cols routine staff visits and resources used) scenariosfor different RM classifications were developed and theircosts were estimated using bottom-up costing methodsAlthough the users can decide which of these analyses ismost representative of their setting uncertainties stillremain about the assumptions made in the estimation ofthese costs However it should be noted that themonthly costs estimated were similar to those reportedin the WSD Implementation costs (such as set-up costsstaff training costs service reconfiguration costs costs
for dual running of usual care and RM services) werenot included in the model but are often a considerationfor the health organisationsRM interventions included in the NMA were heteroge-
neous in terms of monitored parameters and selectioncriteria for HF this was the case even within specifictypes of RM (STS HH STS HM and TM) and isreflected in the uncertainty of the effectiveness para-meters A limitation of the analyses is that the effective-ness parameters remained the same for the differentcost scenarios whereas in reality there might be somecorrelation between the costs and effectiveness of differ-ent RM strategies Also it was assumed that the effective-ness and costs of the interventions are constant overtime irrespective of the duration of deploymentFurthermore as the analysis is not severity specific itassumes that the interventions are equally effective indifferent severity groups within the population underconsideration (ie patients who are recently dischargedwith HF) Repeat interventions after repeat hospitaladmissions for heart failure are not modelled and themortality risk is not reset for patients who are readmit-ted as this would need detailed evidence on baselinerisks and effectiveness in different patient groups As thisdetailed evidence is not available the cohort model usesevidence about the overall average of the patients to esti-mate the cost-effectivenessSome of the assumptions above may not hold true in
reality and therefore further research is needed to addressthese issues Given the complex nature of RM interven-tions new research should seek to examine the lsquoactiveingredientsrsquo of RM and identify patient subgroups that canbenefit most from the intervention as well as patients inwhom these interventions are unlikely to be effective Inaddition usual care ought to be more robustly deter-mined reflecting best practice as defined in the currentguidelines although this is not commonly the caseFurthermore to aid robust cost-effectiveness estimationsthe costs associated with usual care and RM interventionsneed to be reported in detail (including the costs of HFtreatment pathways) and QoL needs to be reported withobservations at specific time points in order to estimatethe difference in the utility of the patients between theRM and usual care groups Future studies should providegreater detail on reconfiguration and set-up costs and linkmore clearly with the financial impact (eg cost variationwith scale and over time) on provider organisations Wideradaptation of RM in the NHS can be facilitated by provid-ing financial impact data (eg set-up costs quarterly costsof service costs of reconfiguration) along with the long-term cost-effectiveness informationThe results of the current analysis have important
implications for the healthcare systems facing risingdemand from emergency admissions HF is a leadingcause of hospitalisation in the UK with 58 164 admis-sions recorded for HF (as first diagnoses) between April2009 and March 2010 in England and Wales25 The costof inpatient bed days for HF alone has been estimated at
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 7
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
pound563 million26 with around 90 of HF admissions toemergency departments27 lasting a median of 9 days25
The evidence shows that use of RM could substantiallyreduce HF admissions with an associated reduction inpressure on acute beds and consequent cost savingsFurthermore the use of TM might allow the potentialtransfer from emergency admission to elective admis-sion that is scheduling admissions of patients directly(not via AampE) to either a ward or to a day unit for off-loading leading to major resource savings with lesspatient disutilityIndeed the Department of Health (DH) recognised
this potential and launched an initiative lsquo3 MillionLivesrdquo (3ML) to help at least three million peoplewith long-term conditions andor social care tobenefit from the use of telehealth and telecare ser-vices28 A concordat has been entered into by the DHand the telehealth and telecare industry to worktogether to accelerate the use of TM29 Thus far sevenpathfinder sites have agreed contracts with the indus-try to ensure that 100 000 people benefit from thetechnology in 201330 Implemented effectively as partof a whole system redesign of care TM may alleviatethe pressure on long-term NHS costs and improvepeoplersquos quality of life through better self-care in thehome setting
Author affiliations1ScHARR University of Sheffield Sheffield UK2Department of Cardiology Barnet and Chase Farm Hospitals NHS TrustEnfield UK3South Yorkshire Cardiothoracic Centre Sheffield Teaching Hospitals NHSFoundation Trust Sheffield UK4Department of Cardiology Castle Hill Hospital Hull York Medical SchoolUniversity of Hull Hull UK5National Heart amp Lung Institute Imperial College London (Royal BromptonHospital) London UK
Acknowledgements The authors would like to thank Mr Tim Ellis ResearchFellow University of Sheffield Professor Mark Hawley Professor of HealthServices Research University of Sheffield Hazel Marsh Research NurseBarnsley Hospital NHS Foundation Trust and Dr Rachel OrsquoHara Lecturer inPublic Health University of Sheffield for providing clinical and TM expertiseThey would also like to thank Dr Lizzie Coates for peer reviewing the draftpaper
Contributors PT developed the decision analytical model undertook theanalysis and drafted the paper HB assisted in parameter searches modeldevelopment and analysis AB provided expert modelling advice AP wasresponsible for conception and design he undertook the systematic reviewalong with TG and provided data for the meta-analysis JWS and JW providedthe meta-analysis results and statistical input AB AAM JC and MRCprovided expert clinical input RW developed and undertook the literaturesearches All authors commented on the draftfinal paper
Funding The project was funded by the National Institute for Health Research(NIHR) Health Technology Assessment (HTA) Programme (number 0910701) and sponsored by the University of Sheffield The study funders had norole in study design in the collection analysis and interpretation of data inthe writing of the report and in the decision to submit the paper forpublication The researchers were independent of the study funders
Competing interests MRCrsquos salary is supported by the NIHR BiomedicalResearch Unit at the Royal Brompton Hospital
Provenance and peer review Not commissioned externally peer reviewed
Data sharing statement No additional data are available
Open Access This is an Open Access article distributed in accordance withthe Creative Commons Attribution Non Commercial (CC BY-NC 30) licensewhich permits others to distribute remix adapt build upon this work non-commercially and license their derivative works on different terms providedthe original work is properly cited and the use is non-commercial See httpcreativecommonsorglicensesby-nc30
REFERENCES1 Riley JP Cowie MR Telemonitoring in heart failure Heart
2009951964ndash82 Hasan A Paul V Telemonitoring in chronic heart failure Eur Heart J
2011321457ndash643 National Heart Failure Audit April 2010 to March 2011 2012 http
yhhiec org ukwp-contentuploads20111011070604_Tele_Moni_Workbk pdf httpwwwuclacuknicorauditsheartfailureadditionalfilespdfsannualreportsannual11pdf (accessed Mar2012)
4 McKelvie RS Heart failure Clin Evid 2011201102045 Anker SD Koehler F Abraham WT Telemedicine and remote
management of patients with heart failure [Review] Lancet2011378731ndash9
6 Inglis SC Clark RA McAlister FA et al Structured telephonesupport or telemonitoring programmes for patients with chronic heartfailure Cochrane Database Syst Rev 2010(8)CD007228
7 Pandor A Thokala P Gomersall T et al Home telemonitoring orstructured telephone support programmes after recent discharge inpatients with heart failure systematic review and economicevaluation Health Technol Assess 201317
8 Pandor A Pandor A Gomersall T et al Remote monitoring afterrecent hospital discharge in patients with heart failure a systematicreview and network meta-analysis Heart Published Online First 16May 2013 doi101136heartjnl-2013-303811
9 National Clinical Guideline Centre Chronic heart failure themanagement of chronic heart failure in adults in primary andsecondary care London National Clinical Guideline Centre 2012
10 Solomon SD Dobson J Pocock S et al Influence of nonfatalhospitalization for heart failure on subsequent mortality in patientswith chronic heart failure Circulation 20071161482ndash7
11 Klersy C De SA Gabutti G et al Economic impact of remotepatient monitoring an integrated economic model derived from ameta-analysis of randomized controlled trials in heart failure Eur JHeart Failure 201113450ndash9
12 Dar O Riley J Chapman C et al A randomized trial of hometelemonitoring in a typical elderly heart failure population in NorthWest London results of the Home-HF study Eur J Heart Failure200911319ndash25
13 Capomolla S Pinna GD La Rovere MT et al Heart failure casedisease management program a pilot study of home telemonitoringversus usual care Eur Heart J 20046(Suppl F)F91ndash8
14 Calvert MJ Shankar A McManus RJ et al Evaluation of themanagement of heart failure in primary care Fam Pract200926145ndash53
15 Iqbal J Francis L Reid J et al Quality of life in patients with chronicheart failure and their carers a 3-year follow-up study assessinghospitalization and mortality Eur J Heart Failure 2010121002ndash8
16 Miller LC Cox KR Miller LC et al Case management for patientswith heart failure a quality improvement intervention J GerontolNurs 20053120ndash8
17 Yao G Freemantle N Flather M et al Long-term cost-effectivenessanalysis of nebivolol compared with standard care in elderly patientswith heart failure an individual patient-based simulation modelPharmacoeconomics 200826879ndash89
18 Cleland JG Louis AA Rigby AS et al Noninvasive hometelemonitoring for patients with heart failure at high risk of recurrentadmission and death The Trans-European Network-Home-CareManagments System (TEN-HMS) study J Am Coll Cardiol2005451654ndash64
19 PSSRU Unit costs of health and social care 2011 201120 Boyne J Vrijhoef HJ Nieman FH et al Telemonitoring in patients
with heart failure results from a multicenter randomized controlledtrial (the tehaf study) J Am Coll Cardiol 201157(14 Suppl 1)E389
21 Department of Health NHS reference costs 2007ndash08 2009 LondonUK 2009
22 Miller G Randolph S Forkner E et al Long-term cost-effectivenessof disease management in systolic heart failure Med Deci Making200929325ndash33
8 Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
23 Galbreath AD Krasuski RA Smith B et al Long-term healthcareand cost outcome of disease management in a large randomizedcommunity-based population with heart failure Circulation20041103518ndash26
24 Henderson C Knapp M Fernandez J-L et al Cost effectiveness oftelehealth for patients with long term conditions (Whole SystemsDemonstrator telehealth questionnaire study) nested economicevaluation in a pragmatic cluster randomised controlled trialBMJ 2013346f1035
25 NHS information centre National Heart Failure Audit 2010 httpwww npc nhs ukrapidreviewp=2479 2010 httpwwwnpcnhsukrapidreviewp=2479
26 Cleland JG McDonagh T Rigby AS et al The national heart failureaudit for England and Wales 2008ndash2009 Heart 201197876ndash86
27 HES Online Hospital Episode Statistics 2008ndash2009 2012 httpwwwhesonlinenhsuk
28 3millionlives Improving your access to telehealth and telecare 12 AD http3millionlivescouk
29 A concordat between the Department of Health and the telehealthand telecare industry 12 AD http3millionlivescoukwp-contentuploads201203Concordat-FINALpdf
30 100000 people with long-term conditions to benefit from technologyin 2013 12 AD http3millionlivescoukwp-contentuploads20121114-November-2012-press-releasepdf
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 9
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from

pressure intrathoracic impedance heart rates duringrest and exertion and symptom control) can facilitateearly detection of clinically significant changes as well asearlier intervention to restabilise the syndrome preventemergency admissions and avoid complications5 RMcan be broadly classified into telemonitoring (TM) inwhich physiological data are electronically transmitted toa healthcare team and structured telephone support(STS) that is the use of phone calls usually by specialistnurses to deliver self-care support andor manage-ment6 For STS support can be provided by human-to-human contact (HH) or via a human-to-machine inter-face (HM) that is STS with an interactive responsesystem (eg a voice-interactive system) For TM supportcan be provided during office hours only or 24 h day7 daysweek (247) though few studies have used thelatter approachThe cost-effectiveness of an RM strategy can be esti-
mated by comparing the outcomes and costs associatedwith the strategy to the next most effective alternative Ifthese outcomes are estimated as quality-adjusted lifeyears (QALYs) then the incremental cost-effectivenessratio (ICER) or cost per QALY gained can be calcu-lated and compared to alternative uses of healthcarefunding In the UK (UK) the National Institute forHealth and Clinical Excellence (NICE) typically recom-mends in favour of funding interventions with an ICERbelow thresholds of pound20 000QALY requires consider-able clinical benefit to recommend funding interven-tions between pound20 000 and pound30 000QALY andrecommends against funding interventions with anICER above these thresholds The aim of this paper is toestimate the incremental cost per QALY of RM strategiescompared with usual care so as to determine which RMstrategy should be recommended according to typicalNICE thresholds for cost-effectiveness
METHODSModel scopeA Markov model was developed using MS Excel software(Microsoft Corporation) to estimate the cost-effectivenessof RM interventions with usual care for patients dis-charged in the past 28 days with a HF-related hospital-isation7 measured as the incremental cost per QALYgained by each strategy compared with the next mosteffective alternative on the cost-effectiveness frontierCost-effectiveness results are estimated as mean values of10 000 probabilistic sensitivity analysis (PSA) runs witheach PSA run using different estimates for the risks HRscosts and utilities sampled from probability distributionsrepresenting uncertainty in the parameter estimatesAdditionally the probability that each strategy would bethe most cost-effective was calculated at different thresh-olds for willingness to pay (WTP) for health gainCost-effectiveness acceptability curves were constructedby plotting the probability of each strategy being cost-effective against the WTP threshold
The following strategies postdischarge interventionswere tested in the modelA Usual careB STS HH (structured telephone support with
human-to-human contact)C STS HM (structured telephone support with
human-to-machine interface) andD TM (ie telemonitoring with transmitted data
reviewed by medical staff or medical support pro-vided during office hours)
The clinical effectiveness parameters of these threeRM strategies were estimated from a networkmeta-analysis of the available evidence8 and costs wereestimated using lsquobottom uprsquo costing methods It wasassumed that the interventions were provided for the6 months following discharge from the hospital as themajority of the RM trials included in the networkmeta-analysis used a 6-month follow-up duration8 At theend of 6 months all patients were assumed to receiveusual care as per the NICE Clinical Guidelines for theManagement of Adults with Chronic Heart Failure9 irre-spective of whether they received intervention or post-discharge usual care during the treatment period
Model structureIn the Markov model two different states wereconsideredA Alive at homeB DeadThe Markov model used a monthly cycle length with
half-cycle correction and assigned each patient with amonthly probability of death based on the time sincedischarge and the type of treatment In each period thepatients who were alive were under the risk of anaverage number of monthly rehospitalisations that isreadmissions to a hospital for HF or other causes Eachpatient then accrued lifetime QALYs and healthcarecosts according to their hospitalisation and treatmentstatus The model used a 30 year (patient lifetime)horizon although the impact of each intervention wasfor the first 6 months after an initial discharge Thecosts and QALYs were discounted at an annual discountrate of 35 and the economic perspective of the modelwas that of the NHS in England and Wales Repeat inter-ventions after repeat hospitalisations were not consid-ered in this model
Baseline mortality and hospitalisationThe baseline monthly probabilities of death were esti-mated from Candesartan in Heart failure Assessment ofReduction in Mortality and morbidity (CHARM) study10
which included 7572 patients with a mean age of655 years followed up for 38 months as it assessed theinfluence of non-fatal hospitalisation for heart failure onsubsequent mortality The data from the CHARMstudy10 showed that the mortality risk was highest imme-diately after hospital discharge and then decreased overtime as shown in table 1
2 Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
The mean numbers of HF-related and other-causehospitalisations (estimated as all-cause hospitalisationsminus the HF-related hospitalisations) were estimatedfrom a meta-analysis of 21 studies (5715 patientsmedian age 707 ranging from 45 to 78 years) reportedby Klersy et al11 The average number of monthlyHF-related and all cause rehospitalisations for patientsin usual care are as shown in table 2
Effectiveness of interventionsThe effectiveness parameters in the economic model werethe HRs for all-cause mortality all-cause hospitalisationsand HF-related hospitalisations for the different interven-tions (ie STS HM STS HM and TM) against standardcare These effectiveness parameters were estimated froma network meta-analysis (NMA) of 21 RM studies8 (total6317 patients with the mean age across studies rangingfrom 57 to 78 years) and applied to the baseline para-meters to estimate the hospitalisation and mortality riskparameters for the different interventions It was assumedthat the treatment effectiveness (and costs) lasts only forthe treatment duration of 6 months after which the base-line risks of hospitalisation and mortality are appliedIt should be noted that considerable heterogeneity
was identified in the manner in which RM and usualcare were performed among the studies included inNMA8 which resulted in heterogeneity between studiesin the estimate of HRs For example in RM there wasvariation between studies in the type of devices usedparameters monitored and the protocols for triage andfollow-up In particular the data from Dar et al12
(Home-HF trial conducted in three district general hos-pitals in West London) appeared to be inconsistent withthe data from the remaining studies because it showed ahigher incidence of mortality among the TM groupthan the usual care group However the 6-month
mortality rate in the usual care group (55) was sub-stantially lower than would be expected in a HF cohortreceiving care outside the context of a clinical trial (iebetween 13 and 21)3 which the authors attributedto the high-quality usual care (provided by a HF nursespecialist and a consultant with an interest in HF) Theimpact of this study was assessed in sensitivity analysesand HRs from both the NMAs are presented in table 3On deciding which of these results are most representa-
tive of their setting the key question for decision-makersrelate to the inclusion of the Home-HF study12 in theeffectiveness meta-analyses If one accepts that usual careis best represented by the usual care arm in the Home-HFstudy12 which is the only study showing a statistically signifi-cant difference in effectiveness of usual care over RMthen the results including Home-HF study12 might be con-sidered more relevant than those without If on the otherhand one considers that the performance of usual care isbetter represented by the other studies and that usual carein Home-HF study12 is not representative of current usualcare then the results excluding Home-HF study12 mightbe more generalisable This consideration predominantlyaffects the HRs around the telemonitoring interventiononly and does not impact substantially on the structuretelephone service interventions
Health-related quality of lifeA review was conducted to estimate the health-relatedquality of life (HRQoL) and four studies were found13ndash16 all of which reported utilities for recently dischargedHF patients under usual care around 057 to 06 Therewas no quantified evidence on the extent to which RMimproves the HRQoL of the patients in the RM studiesincluded in NMA and thus the same utility values wereused for HF patients in usual care as well as (each of thethree) RM strategies in the economic model The disutil-ity caused by rehospitalisation for HF was estimated as01 based on a study by Yao et al17 who estimated the dis-utility to be equivalent to the utility of one health statelower in terms of the New York Heart Association(NYHA) class and this disutility was assumed to last for1 year In the absence of evidence regarding the disutil-ity caused by rehospitalisation for other causes (not dir-ectly HF-related) it was assumed that there was nodisutility caused by rehospitalisation for other causesA utility score of 058 was applied to the patients for
each month in the first year after discharge and a utilityscore of 067 was used after the first year Any HF-relatedhospitalisation was assumed to result in a disutility of 01for a whole year that is the utility of the patient for that
Table 2 Monthly risk of hospitalisations per patient in usual care
Source Estimate Lower 95 CI Upper 95 CI
HF-related hospitalisations Klersy et al11 00350 00325 00375
All-cause hospitalisations Klersy et al11 00875 00841 00908
Table 1 Monthly mortality probability vs time since
discharge for patients with heart failure (HF) in usual care
Time since
discharge
(in months)
Mortality
probability
per month
Lower
95 CI
Upper
95 CI
0ndash1 004622 003616 005891
1ndash3 003306 002644 004124
3ndash6 002674 002166 003306
6ndash12 002353 001964 002831
12ndash24 001866 001565 002226
gt24 001467 001127 001911
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 3
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
year was 067ndash01 that is 057 Within the PSA theuncertainty in the utility values was represented using anormal distribution using the deterministic values as themean with an SD of 0015 and estimated based on thedifference between the utilities reported by Capomollaet al13 and Iqbal et al15 while the disutility was repre-sented using a triangular distribution with (minus008 011)as the range with minus01 as the mode
CostsThe costs used in the model are (1) costs of RM inter-ventions after initial discharge only (2) costs of usualcare and (3) repeat hospitalisation costs These costs aresummarised in table 4 and are described in detail in thissectionThe RM studies did not report clearly or in detail
what was involved in the usual postdischarge care orRM thus making it difficult to accurately determine thecosts8 Owing to the variation involved in the RM inter-ventions and usual care cost scenarios were developedfor each RM classification (ie STS HM STS HH andTM) and usual care These costs were estimated using
bottom-up costing methods for a typical health organisa-tion of 250 HF patients (estimated based on the mediansize of the NHS Foundation Trusts in the UK) for aperiod of 6 months Furthermore it was assumed thatafter 6 months all patients would receive usual care asrecommended in NICE clinical guidelines for the man-agement of adults with CHF9 irrespective of whetherthey received the remote monitoring intervention orpostdischarge usual care during the intervention periodIt was assumed that the usual postdischarge care was
the same as that described in the TEN-HMS study18 andthe usual care costs were estimated by applying thehourly NHS staff rates from PSSRU 201119 to theresource use data in the TEN-HMS study18 A high costusual postdischarge care scenario was also developedbased on discussions with the clinical expert group (ABAAM JC and MRC)The total costs of RM interventions were broken down
into the costs of the device monitoring costs andmedical care costs8 The costs of the RM devices wereelicited from an expert advisory group The monitoringcosts were estimated using activity-based costing for the
Table 4 Cost parameters used in the economic model
Costs (in pound) per 6 months
Base-case
scenario
Low-cost
scenario
High-cost
scenario Source
UC pound161 ndash pound592 TEN-HMS18 Clinical opinion
STS HM pound715 pound623 pound794 Clinical opinion
STS HH pound1075 pound1051 pound1152 Clinical opinion
TM pound1051 pound801 pound1288 Clinical opinion
Usual care costs (per month) after 6 month intervention duration
UC after 6 months pound823 ndash ndash NICE HF guidelines9
Hospitalisation costs Estimate Lower 95 CI Upper 95 CI
HF-related hospitalisations pound251449 pound1857 pound2809 NHS Reference Costs for
201121
Other-cause hospitalisationsdagger pound152979 pound1129 pound1709 NHS Reference Costs for
201121
Heart failure or shock (EB03H EB03I) non-elective inpatient (long stay) including excess bed days21
daggerNon-elective inpatient (long stay and short stay) including excess bed days21
Table 3 HRs for interventions versus usual care for all-cause mortality and hospitalisations
HRs for interventions versus usual care for mortality (all-cause) and hospitalisation (all-cause and HF) from NMA
including Home-HF12 study
Type
All-cause mortality HF-hospitalisation All-cause hospitalisation
R 95 PrI HR 95 PrI HR 95 PrI
STS HH 077 (031 186) 077 (050 119) 097 (038 243)
STS HM 098 (030 323) 103 (058 177) 106 (031 361)
TM 076 (030 191) 095 (059 162) 075 (028 191)
HRs for interventions versus usual care for mortality (all-cause) and hospitalisation (all-cause and HF) from NMA
excluding Home-HF12 study
STS HH 075 (045 127) 076 (051 113) 096 (042 218)
STS HM 098 (049 195) 102 (061 169) 106 (035 322)
TM 062 (035 109) 086 (054 138) 067 (026 153)
HR hazard ratio PrI predictive interval STS HM structured telephone support via human to machine interface STS HH structuredtelephone support via human to human contact TM telemonitoring
4 Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
resources spent by the staff on triage and follow-upbased on evidence from the literature20 The costs ofmedical care for the usual care arm STS and TM armswere estimated by applying the hourly NHS staff ratesfrom PSSRU 201119 to their respective medical careresource use data reported in the TEN-HMS study18
The mean inpatient admission cost for HF-related hos-pitalisations was calculated from the weighted average ofthe costs for the HRG lsquoHeart Failure or Shockrdquo (EB03HEB03I) based on the data obtained from the NHSReference Costs for 201121 For hospital admissions forany cause other than HF it was assumed that these costswere the same as the mean cost of hospital admissionfor the general population This was estimated as aweighted average of elective inpatient admissions andnon-elective inpatient admissions (including short andlong stay) based on the data from the NHS ReferenceCosts for 201121
RESULTSThe results of the cost-effectiveness analysis using basecase costs are presented in table 5 for both estimates ofeffectiveness including and excluding data from theHome-HF study12 to address the uncertainty inthe effectiveness evidence Results are also presented forfive cost scenarios (higher usual care cost scenariolower cost scenario of TM higher cost scenario of TMlower STS cost scenario and higher STS cost scenario)and the 12 month intervention duration scenario inonline supplementary tables S1 and S2 respectivelyIn the analysis using base case costs TM is the most
cost-effective strategy at a threshold of pound20 000QALY inboth analyses that is including and excluding theHome-HF study12 TM is also the most effective strategy(ie highest QALYs gained) in the analyses that excludedthe Home-HF study12 but not in the analyses thatincluded the Home-HF study12 with STS HH providingthe highest number of expected QALYs However the
additional QALYs gained by STS HH are not worth theadditional costs of the strategy as seen in the ICERs(against TM) greater than the threshold of pound20 000QALYIn the analyses that included the Home-HF study12
there is only a 40 chance of TM being cost-effective atthe threshold of pound20 000QALY as shown in figure 1Excluding the Home-HF study12 the probability that TMduring office hours is cost-effective increases to 73(figure 2)Scenario analyses performed using higher costs of
usual care higher costs of STS HH and lower costs ofTM do not substantially change the conclusions TM wasestimated to be the most cost-effective strategy in allthese scenarios Scenario analysis performed usinghigher costs of TM (pound215month) suggested that TM isdominated by STS HH This is because a small changein the difference between costs of TM and STS HH ledto a marked change in ICERs given the small difference(00021 QALYs) in expected QALYs between STS HHand TM in the analyses that included the Home-HFstudy12 However the same scenario analysis (ie highercost of TM of pound215month) that excluded the data fromthe Home-HF study12 suggested that TM is still the mostcost-effective strategy with an ICER of pound8223QALYagainst usual care (STS HH is extendedly dominated bya combination of usual care and TM) This is due to themuch higher difference in the expected QALYs betweenSTS HH and TM (00602 QALYs) where a small changein the difference between costs of TM and STS HHcannot lead to a marked change in the ICER Thethreshold analysis suggested that the monthly cost of TMhas to be higher than pound390month to have an ICERgreater than pound20 000QALY against STS HH The ICERof TM against usual care at this monthly cost of pound390 ispound13 357QALYScenario analyses performed using different estimates
of the disutility for HF-related and other cause hospitali-sations produced results similar to that in the base case
Table 5 Summary of the economic analysis results using base case costs
Usual care STS HM STS HH TM
Total costs
Including Home-HF12 pound8478 pound8965 pound9574 pound9437
Excluding Home-HF12 pound8478 pound9087 pound9658 pound9665
Total QALYs
Including Home-HF12 24137 23633 24950 24944
Excluding Home-HF12 24137 24043 25230 25847
ICERs
Including Home-HF12 Dominated pound228 035 pound11 873
Excluding Home-HF12 Dominated Extendedly dominated pound6942
Probability of cost-effectiveness ()
Including Home-HF12 6 19 35 40
Excluding Home-HF12 1 7 19 73
Last strategy in the cost-effectiveness frontierICERs incremental cost-effectiveness ratios QALYs quality adjusted life years STS HH structured telephone support via human to humancontact STS HM structured telephone support via human to machine interface TM telemonitoring
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 5
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
analysis that is the results are robust to the variations inthe disutility of hospitalisationsScenario analysis using a 12-month treatment duration
produced similar results as in the 6-month treatmentduration scenarios TM for 12 months was also cost-effective when compared with TM for 6 months with anICER of pound14 066QALY However treating 2timesN patientsusing TM for 6 months was cost-effective with it beingdominant against a combination of treating N patientsusing TM for 12 months with the rest of the N patientsunder usual care
DISCUSSIONThe results of the base case cost-effectiveness analysessuggest that TM is expected to be the most cost-effectivestrategy at a threshold of pound20 000QALY However thereis uncertainty involved in suggesting that TM is the mostprobable cost-effective strategy and in particular thereis greater uncertainty when data from the Home-HFstudy12 is included than when it is excluded For
decision-makers the key question is whether the usualcare arm in their local setting is similar to the usual carearm in the Home-HF study12 If so then the resultsincluding the Home-HF study12 might be consideredmore relevant and if not the results excluding theHome-HF study12 might be considered more relevantThe scenario analysis performed (using higher usualcare costs lower TM costs higher TM costs and higherSTS costs) did not substantially change the conclusionsTM was estimated to be the most cost-effective strategyin all these scenarios Furthermore TM for 12 monthswas also cost-effective when compared with TM for6 months which suggests that it is cost-effective to keepthe patients on TM beyond 6 months In situations witha limited number of TM devices assuming a homoge-neous patient group it is cost-effective to treat allpatients using TM for 6 months than using TM for12 months on half the patients with the other half of thepatients under usual careThere have been two cost-effectiveness analyses studies
of RM in HF but neither considered the different RM
Figure 1 Cost effectiveness
acceptability curve for base case
economic analysis using
effectiveness data including the
Home-HF study12
Figure 2 Cost effectiveness
acceptability curve for economic
analysis using effectiveness data
excluding the Home-HF study12
6 Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
approaches separately11 22 The analysis reported byMiller et al22 was based on a single trial of STS23
whereas Klersy et al11 included data from a meta-analysisof a wide range of RM studies Miller et al22 estimatedthat STS compared with usual care had an ICER around$43 650QALY this study did not include a PSA butunivariate sensitivity analyses (ICER varying from$28 691 to $129 738 per QALY) was performed Klersyet al11 focused mainly on the effectiveness rather thanthe costs and used a time horizon of 1 year A budgetimpact analysis was presented and the differentdiagnosis-related group (DRG) reimbursement tariffgroups as a proxy for hospitalisation costs were consid-ered with cost savings per patient ranging betweeneuro3068 and euro99294 However other costs such as RMcosts and outpatient visit costs were not considered Theauthors performed scenario analyses using differentDRG costs as part of the budget analysis to address theuncertainty in the hospitalisation costs but neitherdeterministic sensitivity analysis nor PSA was performedThe Whole systems demonstrator (WSD) pro-
gramme24 a randomised controlled trial of telehealththat included over 6000 patients analysed costs and out-comes for 965 patients monitored for 12 months 534receiving telehealth and 431 receiving usual careCost-effectiveness analysis estimated the ICER atpound92 000QALY when telehealth was added to usual carefor people with chronic conditions (diabetes HF andchronic obstructive pulmonary disease (COPD))However this trial-based evaluation (with a time horizonof 1 year) potentially underestimates the health benefitsas it does not include the long-term QALYs gained fromthe reduction in mortality Furthermore the WSD ana-lysis included all patients with chronic conditions (dia-betes HF and COPD) whereas the population underconsideration in our analysis included patients who hadbeen recently discharged with HF The cost-effectivenessresults for HF patients are not yet publicly available in apeer-reviewed journal and thus it is difficult to comparethe results of the current analysis with the results of theWSD analysisThe analysis reported in this paper also has some lim-
itations that need to be taken into account Any model-ling process involves simplifications and assumptionsthat may not accurately reflect clinical practice Owingto the lack of detail provided in research studiesincluded in the NMA concerning the components ofRM packages and usual care (eg communication proto-cols routine staff visits and resources used) scenariosfor different RM classifications were developed and theircosts were estimated using bottom-up costing methodsAlthough the users can decide which of these analyses ismost representative of their setting uncertainties stillremain about the assumptions made in the estimation ofthese costs However it should be noted that themonthly costs estimated were similar to those reportedin the WSD Implementation costs (such as set-up costsstaff training costs service reconfiguration costs costs
for dual running of usual care and RM services) werenot included in the model but are often a considerationfor the health organisationsRM interventions included in the NMA were heteroge-
neous in terms of monitored parameters and selectioncriteria for HF this was the case even within specifictypes of RM (STS HH STS HM and TM) and isreflected in the uncertainty of the effectiveness para-meters A limitation of the analyses is that the effective-ness parameters remained the same for the differentcost scenarios whereas in reality there might be somecorrelation between the costs and effectiveness of differ-ent RM strategies Also it was assumed that the effective-ness and costs of the interventions are constant overtime irrespective of the duration of deploymentFurthermore as the analysis is not severity specific itassumes that the interventions are equally effective indifferent severity groups within the population underconsideration (ie patients who are recently dischargedwith HF) Repeat interventions after repeat hospitaladmissions for heart failure are not modelled and themortality risk is not reset for patients who are readmit-ted as this would need detailed evidence on baselinerisks and effectiveness in different patient groups As thisdetailed evidence is not available the cohort model usesevidence about the overall average of the patients to esti-mate the cost-effectivenessSome of the assumptions above may not hold true in
reality and therefore further research is needed to addressthese issues Given the complex nature of RM interven-tions new research should seek to examine the lsquoactiveingredientsrsquo of RM and identify patient subgroups that canbenefit most from the intervention as well as patients inwhom these interventions are unlikely to be effective Inaddition usual care ought to be more robustly deter-mined reflecting best practice as defined in the currentguidelines although this is not commonly the caseFurthermore to aid robust cost-effectiveness estimationsthe costs associated with usual care and RM interventionsneed to be reported in detail (including the costs of HFtreatment pathways) and QoL needs to be reported withobservations at specific time points in order to estimatethe difference in the utility of the patients between theRM and usual care groups Future studies should providegreater detail on reconfiguration and set-up costs and linkmore clearly with the financial impact (eg cost variationwith scale and over time) on provider organisations Wideradaptation of RM in the NHS can be facilitated by provid-ing financial impact data (eg set-up costs quarterly costsof service costs of reconfiguration) along with the long-term cost-effectiveness informationThe results of the current analysis have important
implications for the healthcare systems facing risingdemand from emergency admissions HF is a leadingcause of hospitalisation in the UK with 58 164 admis-sions recorded for HF (as first diagnoses) between April2009 and March 2010 in England and Wales25 The costof inpatient bed days for HF alone has been estimated at
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 7
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
pound563 million26 with around 90 of HF admissions toemergency departments27 lasting a median of 9 days25
The evidence shows that use of RM could substantiallyreduce HF admissions with an associated reduction inpressure on acute beds and consequent cost savingsFurthermore the use of TM might allow the potentialtransfer from emergency admission to elective admis-sion that is scheduling admissions of patients directly(not via AampE) to either a ward or to a day unit for off-loading leading to major resource savings with lesspatient disutilityIndeed the Department of Health (DH) recognised
this potential and launched an initiative lsquo3 MillionLivesrdquo (3ML) to help at least three million peoplewith long-term conditions andor social care tobenefit from the use of telehealth and telecare ser-vices28 A concordat has been entered into by the DHand the telehealth and telecare industry to worktogether to accelerate the use of TM29 Thus far sevenpathfinder sites have agreed contracts with the indus-try to ensure that 100 000 people benefit from thetechnology in 201330 Implemented effectively as partof a whole system redesign of care TM may alleviatethe pressure on long-term NHS costs and improvepeoplersquos quality of life through better self-care in thehome setting
Author affiliations1ScHARR University of Sheffield Sheffield UK2Department of Cardiology Barnet and Chase Farm Hospitals NHS TrustEnfield UK3South Yorkshire Cardiothoracic Centre Sheffield Teaching Hospitals NHSFoundation Trust Sheffield UK4Department of Cardiology Castle Hill Hospital Hull York Medical SchoolUniversity of Hull Hull UK5National Heart amp Lung Institute Imperial College London (Royal BromptonHospital) London UK
Acknowledgements The authors would like to thank Mr Tim Ellis ResearchFellow University of Sheffield Professor Mark Hawley Professor of HealthServices Research University of Sheffield Hazel Marsh Research NurseBarnsley Hospital NHS Foundation Trust and Dr Rachel OrsquoHara Lecturer inPublic Health University of Sheffield for providing clinical and TM expertiseThey would also like to thank Dr Lizzie Coates for peer reviewing the draftpaper
Contributors PT developed the decision analytical model undertook theanalysis and drafted the paper HB assisted in parameter searches modeldevelopment and analysis AB provided expert modelling advice AP wasresponsible for conception and design he undertook the systematic reviewalong with TG and provided data for the meta-analysis JWS and JW providedthe meta-analysis results and statistical input AB AAM JC and MRCprovided expert clinical input RW developed and undertook the literaturesearches All authors commented on the draftfinal paper
Funding The project was funded by the National Institute for Health Research(NIHR) Health Technology Assessment (HTA) Programme (number 0910701) and sponsored by the University of Sheffield The study funders had norole in study design in the collection analysis and interpretation of data inthe writing of the report and in the decision to submit the paper forpublication The researchers were independent of the study funders
Competing interests MRCrsquos salary is supported by the NIHR BiomedicalResearch Unit at the Royal Brompton Hospital
Provenance and peer review Not commissioned externally peer reviewed
Data sharing statement No additional data are available
Open Access This is an Open Access article distributed in accordance withthe Creative Commons Attribution Non Commercial (CC BY-NC 30) licensewhich permits others to distribute remix adapt build upon this work non-commercially and license their derivative works on different terms providedthe original work is properly cited and the use is non-commercial See httpcreativecommonsorglicensesby-nc30
REFERENCES1 Riley JP Cowie MR Telemonitoring in heart failure Heart
2009951964ndash82 Hasan A Paul V Telemonitoring in chronic heart failure Eur Heart J
2011321457ndash643 National Heart Failure Audit April 2010 to March 2011 2012 http
yhhiec org ukwp-contentuploads20111011070604_Tele_Moni_Workbk pdf httpwwwuclacuknicorauditsheartfailureadditionalfilespdfsannualreportsannual11pdf (accessed Mar2012)
4 McKelvie RS Heart failure Clin Evid 2011201102045 Anker SD Koehler F Abraham WT Telemedicine and remote
management of patients with heart failure [Review] Lancet2011378731ndash9
6 Inglis SC Clark RA McAlister FA et al Structured telephonesupport or telemonitoring programmes for patients with chronic heartfailure Cochrane Database Syst Rev 2010(8)CD007228
7 Pandor A Thokala P Gomersall T et al Home telemonitoring orstructured telephone support programmes after recent discharge inpatients with heart failure systematic review and economicevaluation Health Technol Assess 201317
8 Pandor A Pandor A Gomersall T et al Remote monitoring afterrecent hospital discharge in patients with heart failure a systematicreview and network meta-analysis Heart Published Online First 16May 2013 doi101136heartjnl-2013-303811
9 National Clinical Guideline Centre Chronic heart failure themanagement of chronic heart failure in adults in primary andsecondary care London National Clinical Guideline Centre 2012
10 Solomon SD Dobson J Pocock S et al Influence of nonfatalhospitalization for heart failure on subsequent mortality in patientswith chronic heart failure Circulation 20071161482ndash7
11 Klersy C De SA Gabutti G et al Economic impact of remotepatient monitoring an integrated economic model derived from ameta-analysis of randomized controlled trials in heart failure Eur JHeart Failure 201113450ndash9
12 Dar O Riley J Chapman C et al A randomized trial of hometelemonitoring in a typical elderly heart failure population in NorthWest London results of the Home-HF study Eur J Heart Failure200911319ndash25
13 Capomolla S Pinna GD La Rovere MT et al Heart failure casedisease management program a pilot study of home telemonitoringversus usual care Eur Heart J 20046(Suppl F)F91ndash8
14 Calvert MJ Shankar A McManus RJ et al Evaluation of themanagement of heart failure in primary care Fam Pract200926145ndash53
15 Iqbal J Francis L Reid J et al Quality of life in patients with chronicheart failure and their carers a 3-year follow-up study assessinghospitalization and mortality Eur J Heart Failure 2010121002ndash8
16 Miller LC Cox KR Miller LC et al Case management for patientswith heart failure a quality improvement intervention J GerontolNurs 20053120ndash8
17 Yao G Freemantle N Flather M et al Long-term cost-effectivenessanalysis of nebivolol compared with standard care in elderly patientswith heart failure an individual patient-based simulation modelPharmacoeconomics 200826879ndash89
18 Cleland JG Louis AA Rigby AS et al Noninvasive hometelemonitoring for patients with heart failure at high risk of recurrentadmission and death The Trans-European Network-Home-CareManagments System (TEN-HMS) study J Am Coll Cardiol2005451654ndash64
19 PSSRU Unit costs of health and social care 2011 201120 Boyne J Vrijhoef HJ Nieman FH et al Telemonitoring in patients
with heart failure results from a multicenter randomized controlledtrial (the tehaf study) J Am Coll Cardiol 201157(14 Suppl 1)E389
21 Department of Health NHS reference costs 2007ndash08 2009 LondonUK 2009
22 Miller G Randolph S Forkner E et al Long-term cost-effectivenessof disease management in systolic heart failure Med Deci Making200929325ndash33
8 Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
23 Galbreath AD Krasuski RA Smith B et al Long-term healthcareand cost outcome of disease management in a large randomizedcommunity-based population with heart failure Circulation20041103518ndash26
24 Henderson C Knapp M Fernandez J-L et al Cost effectiveness oftelehealth for patients with long term conditions (Whole SystemsDemonstrator telehealth questionnaire study) nested economicevaluation in a pragmatic cluster randomised controlled trialBMJ 2013346f1035
25 NHS information centre National Heart Failure Audit 2010 httpwww npc nhs ukrapidreviewp=2479 2010 httpwwwnpcnhsukrapidreviewp=2479
26 Cleland JG McDonagh T Rigby AS et al The national heart failureaudit for England and Wales 2008ndash2009 Heart 201197876ndash86
27 HES Online Hospital Episode Statistics 2008ndash2009 2012 httpwwwhesonlinenhsuk
28 3millionlives Improving your access to telehealth and telecare 12 AD http3millionlivescouk
29 A concordat between the Department of Health and the telehealthand telecare industry 12 AD http3millionlivescoukwp-contentuploads201203Concordat-FINALpdf
30 100000 people with long-term conditions to benefit from technologyin 2013 12 AD http3millionlivescoukwp-contentuploads20121114-November-2012-press-releasepdf
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 9
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from

The mean numbers of HF-related and other-causehospitalisations (estimated as all-cause hospitalisationsminus the HF-related hospitalisations) were estimatedfrom a meta-analysis of 21 studies (5715 patientsmedian age 707 ranging from 45 to 78 years) reportedby Klersy et al11 The average number of monthlyHF-related and all cause rehospitalisations for patientsin usual care are as shown in table 2
Effectiveness of interventionsThe effectiveness parameters in the economic model werethe HRs for all-cause mortality all-cause hospitalisationsand HF-related hospitalisations for the different interven-tions (ie STS HM STS HM and TM) against standardcare These effectiveness parameters were estimated froma network meta-analysis (NMA) of 21 RM studies8 (total6317 patients with the mean age across studies rangingfrom 57 to 78 years) and applied to the baseline para-meters to estimate the hospitalisation and mortality riskparameters for the different interventions It was assumedthat the treatment effectiveness (and costs) lasts only forthe treatment duration of 6 months after which the base-line risks of hospitalisation and mortality are appliedIt should be noted that considerable heterogeneity
was identified in the manner in which RM and usualcare were performed among the studies included inNMA8 which resulted in heterogeneity between studiesin the estimate of HRs For example in RM there wasvariation between studies in the type of devices usedparameters monitored and the protocols for triage andfollow-up In particular the data from Dar et al12
(Home-HF trial conducted in three district general hos-pitals in West London) appeared to be inconsistent withthe data from the remaining studies because it showed ahigher incidence of mortality among the TM groupthan the usual care group However the 6-month
mortality rate in the usual care group (55) was sub-stantially lower than would be expected in a HF cohortreceiving care outside the context of a clinical trial (iebetween 13 and 21)3 which the authors attributedto the high-quality usual care (provided by a HF nursespecialist and a consultant with an interest in HF) Theimpact of this study was assessed in sensitivity analysesand HRs from both the NMAs are presented in table 3On deciding which of these results are most representa-
tive of their setting the key question for decision-makersrelate to the inclusion of the Home-HF study12 in theeffectiveness meta-analyses If one accepts that usual careis best represented by the usual care arm in the Home-HFstudy12 which is the only study showing a statistically signifi-cant difference in effectiveness of usual care over RMthen the results including Home-HF study12 might be con-sidered more relevant than those without If on the otherhand one considers that the performance of usual care isbetter represented by the other studies and that usual carein Home-HF study12 is not representative of current usualcare then the results excluding Home-HF study12 mightbe more generalisable This consideration predominantlyaffects the HRs around the telemonitoring interventiononly and does not impact substantially on the structuretelephone service interventions
Health-related quality of lifeA review was conducted to estimate the health-relatedquality of life (HRQoL) and four studies were found13ndash16 all of which reported utilities for recently dischargedHF patients under usual care around 057 to 06 Therewas no quantified evidence on the extent to which RMimproves the HRQoL of the patients in the RM studiesincluded in NMA and thus the same utility values wereused for HF patients in usual care as well as (each of thethree) RM strategies in the economic model The disutil-ity caused by rehospitalisation for HF was estimated as01 based on a study by Yao et al17 who estimated the dis-utility to be equivalent to the utility of one health statelower in terms of the New York Heart Association(NYHA) class and this disutility was assumed to last for1 year In the absence of evidence regarding the disutil-ity caused by rehospitalisation for other causes (not dir-ectly HF-related) it was assumed that there was nodisutility caused by rehospitalisation for other causesA utility score of 058 was applied to the patients for
each month in the first year after discharge and a utilityscore of 067 was used after the first year Any HF-relatedhospitalisation was assumed to result in a disutility of 01for a whole year that is the utility of the patient for that
Table 2 Monthly risk of hospitalisations per patient in usual care
Source Estimate Lower 95 CI Upper 95 CI
HF-related hospitalisations Klersy et al11 00350 00325 00375
All-cause hospitalisations Klersy et al11 00875 00841 00908
Table 1 Monthly mortality probability vs time since
discharge for patients with heart failure (HF) in usual care
Time since
discharge
(in months)
Mortality
probability
per month
Lower
95 CI
Upper
95 CI
0ndash1 004622 003616 005891
1ndash3 003306 002644 004124
3ndash6 002674 002166 003306
6ndash12 002353 001964 002831
12ndash24 001866 001565 002226
gt24 001467 001127 001911
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 3
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
year was 067ndash01 that is 057 Within the PSA theuncertainty in the utility values was represented using anormal distribution using the deterministic values as themean with an SD of 0015 and estimated based on thedifference between the utilities reported by Capomollaet al13 and Iqbal et al15 while the disutility was repre-sented using a triangular distribution with (minus008 011)as the range with minus01 as the mode
CostsThe costs used in the model are (1) costs of RM inter-ventions after initial discharge only (2) costs of usualcare and (3) repeat hospitalisation costs These costs aresummarised in table 4 and are described in detail in thissectionThe RM studies did not report clearly or in detail
what was involved in the usual postdischarge care orRM thus making it difficult to accurately determine thecosts8 Owing to the variation involved in the RM inter-ventions and usual care cost scenarios were developedfor each RM classification (ie STS HM STS HH andTM) and usual care These costs were estimated using
bottom-up costing methods for a typical health organisa-tion of 250 HF patients (estimated based on the mediansize of the NHS Foundation Trusts in the UK) for aperiod of 6 months Furthermore it was assumed thatafter 6 months all patients would receive usual care asrecommended in NICE clinical guidelines for the man-agement of adults with CHF9 irrespective of whetherthey received the remote monitoring intervention orpostdischarge usual care during the intervention periodIt was assumed that the usual postdischarge care was
the same as that described in the TEN-HMS study18 andthe usual care costs were estimated by applying thehourly NHS staff rates from PSSRU 201119 to theresource use data in the TEN-HMS study18 A high costusual postdischarge care scenario was also developedbased on discussions with the clinical expert group (ABAAM JC and MRC)The total costs of RM interventions were broken down
into the costs of the device monitoring costs andmedical care costs8 The costs of the RM devices wereelicited from an expert advisory group The monitoringcosts were estimated using activity-based costing for the
Table 4 Cost parameters used in the economic model
Costs (in pound) per 6 months
Base-case
scenario
Low-cost
scenario
High-cost
scenario Source
UC pound161 ndash pound592 TEN-HMS18 Clinical opinion
STS HM pound715 pound623 pound794 Clinical opinion
STS HH pound1075 pound1051 pound1152 Clinical opinion
TM pound1051 pound801 pound1288 Clinical opinion
Usual care costs (per month) after 6 month intervention duration
UC after 6 months pound823 ndash ndash NICE HF guidelines9
Hospitalisation costs Estimate Lower 95 CI Upper 95 CI
HF-related hospitalisations pound251449 pound1857 pound2809 NHS Reference Costs for
201121
Other-cause hospitalisationsdagger pound152979 pound1129 pound1709 NHS Reference Costs for
201121
Heart failure or shock (EB03H EB03I) non-elective inpatient (long stay) including excess bed days21
daggerNon-elective inpatient (long stay and short stay) including excess bed days21
Table 3 HRs for interventions versus usual care for all-cause mortality and hospitalisations
HRs for interventions versus usual care for mortality (all-cause) and hospitalisation (all-cause and HF) from NMA
including Home-HF12 study
Type
All-cause mortality HF-hospitalisation All-cause hospitalisation
R 95 PrI HR 95 PrI HR 95 PrI
STS HH 077 (031 186) 077 (050 119) 097 (038 243)
STS HM 098 (030 323) 103 (058 177) 106 (031 361)
TM 076 (030 191) 095 (059 162) 075 (028 191)
HRs for interventions versus usual care for mortality (all-cause) and hospitalisation (all-cause and HF) from NMA
excluding Home-HF12 study
STS HH 075 (045 127) 076 (051 113) 096 (042 218)
STS HM 098 (049 195) 102 (061 169) 106 (035 322)
TM 062 (035 109) 086 (054 138) 067 (026 153)
HR hazard ratio PrI predictive interval STS HM structured telephone support via human to machine interface STS HH structuredtelephone support via human to human contact TM telemonitoring
4 Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
resources spent by the staff on triage and follow-upbased on evidence from the literature20 The costs ofmedical care for the usual care arm STS and TM armswere estimated by applying the hourly NHS staff ratesfrom PSSRU 201119 to their respective medical careresource use data reported in the TEN-HMS study18
The mean inpatient admission cost for HF-related hos-pitalisations was calculated from the weighted average ofthe costs for the HRG lsquoHeart Failure or Shockrdquo (EB03HEB03I) based on the data obtained from the NHSReference Costs for 201121 For hospital admissions forany cause other than HF it was assumed that these costswere the same as the mean cost of hospital admissionfor the general population This was estimated as aweighted average of elective inpatient admissions andnon-elective inpatient admissions (including short andlong stay) based on the data from the NHS ReferenceCosts for 201121
RESULTSThe results of the cost-effectiveness analysis using basecase costs are presented in table 5 for both estimates ofeffectiveness including and excluding data from theHome-HF study12 to address the uncertainty inthe effectiveness evidence Results are also presented forfive cost scenarios (higher usual care cost scenariolower cost scenario of TM higher cost scenario of TMlower STS cost scenario and higher STS cost scenario)and the 12 month intervention duration scenario inonline supplementary tables S1 and S2 respectivelyIn the analysis using base case costs TM is the most
cost-effective strategy at a threshold of pound20 000QALY inboth analyses that is including and excluding theHome-HF study12 TM is also the most effective strategy(ie highest QALYs gained) in the analyses that excludedthe Home-HF study12 but not in the analyses thatincluded the Home-HF study12 with STS HH providingthe highest number of expected QALYs However the
additional QALYs gained by STS HH are not worth theadditional costs of the strategy as seen in the ICERs(against TM) greater than the threshold of pound20 000QALYIn the analyses that included the Home-HF study12
there is only a 40 chance of TM being cost-effective atthe threshold of pound20 000QALY as shown in figure 1Excluding the Home-HF study12 the probability that TMduring office hours is cost-effective increases to 73(figure 2)Scenario analyses performed using higher costs of
usual care higher costs of STS HH and lower costs ofTM do not substantially change the conclusions TM wasestimated to be the most cost-effective strategy in allthese scenarios Scenario analysis performed usinghigher costs of TM (pound215month) suggested that TM isdominated by STS HH This is because a small changein the difference between costs of TM and STS HH ledto a marked change in ICERs given the small difference(00021 QALYs) in expected QALYs between STS HHand TM in the analyses that included the Home-HFstudy12 However the same scenario analysis (ie highercost of TM of pound215month) that excluded the data fromthe Home-HF study12 suggested that TM is still the mostcost-effective strategy with an ICER of pound8223QALYagainst usual care (STS HH is extendedly dominated bya combination of usual care and TM) This is due to themuch higher difference in the expected QALYs betweenSTS HH and TM (00602 QALYs) where a small changein the difference between costs of TM and STS HHcannot lead to a marked change in the ICER Thethreshold analysis suggested that the monthly cost of TMhas to be higher than pound390month to have an ICERgreater than pound20 000QALY against STS HH The ICERof TM against usual care at this monthly cost of pound390 ispound13 357QALYScenario analyses performed using different estimates
of the disutility for HF-related and other cause hospitali-sations produced results similar to that in the base case
Table 5 Summary of the economic analysis results using base case costs
Usual care STS HM STS HH TM
Total costs
Including Home-HF12 pound8478 pound8965 pound9574 pound9437
Excluding Home-HF12 pound8478 pound9087 pound9658 pound9665
Total QALYs
Including Home-HF12 24137 23633 24950 24944
Excluding Home-HF12 24137 24043 25230 25847
ICERs
Including Home-HF12 Dominated pound228 035 pound11 873
Excluding Home-HF12 Dominated Extendedly dominated pound6942
Probability of cost-effectiveness ()
Including Home-HF12 6 19 35 40
Excluding Home-HF12 1 7 19 73
Last strategy in the cost-effectiveness frontierICERs incremental cost-effectiveness ratios QALYs quality adjusted life years STS HH structured telephone support via human to humancontact STS HM structured telephone support via human to machine interface TM telemonitoring
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 5
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
analysis that is the results are robust to the variations inthe disutility of hospitalisationsScenario analysis using a 12-month treatment duration
produced similar results as in the 6-month treatmentduration scenarios TM for 12 months was also cost-effective when compared with TM for 6 months with anICER of pound14 066QALY However treating 2timesN patientsusing TM for 6 months was cost-effective with it beingdominant against a combination of treating N patientsusing TM for 12 months with the rest of the N patientsunder usual care
DISCUSSIONThe results of the base case cost-effectiveness analysessuggest that TM is expected to be the most cost-effectivestrategy at a threshold of pound20 000QALY However thereis uncertainty involved in suggesting that TM is the mostprobable cost-effective strategy and in particular thereis greater uncertainty when data from the Home-HFstudy12 is included than when it is excluded For
decision-makers the key question is whether the usualcare arm in their local setting is similar to the usual carearm in the Home-HF study12 If so then the resultsincluding the Home-HF study12 might be consideredmore relevant and if not the results excluding theHome-HF study12 might be considered more relevantThe scenario analysis performed (using higher usualcare costs lower TM costs higher TM costs and higherSTS costs) did not substantially change the conclusionsTM was estimated to be the most cost-effective strategyin all these scenarios Furthermore TM for 12 monthswas also cost-effective when compared with TM for6 months which suggests that it is cost-effective to keepthe patients on TM beyond 6 months In situations witha limited number of TM devices assuming a homoge-neous patient group it is cost-effective to treat allpatients using TM for 6 months than using TM for12 months on half the patients with the other half of thepatients under usual careThere have been two cost-effectiveness analyses studies
of RM in HF but neither considered the different RM
Figure 1 Cost effectiveness
acceptability curve for base case
economic analysis using
effectiveness data including the
Home-HF study12
Figure 2 Cost effectiveness
acceptability curve for economic
analysis using effectiveness data
excluding the Home-HF study12
6 Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
approaches separately11 22 The analysis reported byMiller et al22 was based on a single trial of STS23
whereas Klersy et al11 included data from a meta-analysisof a wide range of RM studies Miller et al22 estimatedthat STS compared with usual care had an ICER around$43 650QALY this study did not include a PSA butunivariate sensitivity analyses (ICER varying from$28 691 to $129 738 per QALY) was performed Klersyet al11 focused mainly on the effectiveness rather thanthe costs and used a time horizon of 1 year A budgetimpact analysis was presented and the differentdiagnosis-related group (DRG) reimbursement tariffgroups as a proxy for hospitalisation costs were consid-ered with cost savings per patient ranging betweeneuro3068 and euro99294 However other costs such as RMcosts and outpatient visit costs were not considered Theauthors performed scenario analyses using differentDRG costs as part of the budget analysis to address theuncertainty in the hospitalisation costs but neitherdeterministic sensitivity analysis nor PSA was performedThe Whole systems demonstrator (WSD) pro-
gramme24 a randomised controlled trial of telehealththat included over 6000 patients analysed costs and out-comes for 965 patients monitored for 12 months 534receiving telehealth and 431 receiving usual careCost-effectiveness analysis estimated the ICER atpound92 000QALY when telehealth was added to usual carefor people with chronic conditions (diabetes HF andchronic obstructive pulmonary disease (COPD))However this trial-based evaluation (with a time horizonof 1 year) potentially underestimates the health benefitsas it does not include the long-term QALYs gained fromthe reduction in mortality Furthermore the WSD ana-lysis included all patients with chronic conditions (dia-betes HF and COPD) whereas the population underconsideration in our analysis included patients who hadbeen recently discharged with HF The cost-effectivenessresults for HF patients are not yet publicly available in apeer-reviewed journal and thus it is difficult to comparethe results of the current analysis with the results of theWSD analysisThe analysis reported in this paper also has some lim-
itations that need to be taken into account Any model-ling process involves simplifications and assumptionsthat may not accurately reflect clinical practice Owingto the lack of detail provided in research studiesincluded in the NMA concerning the components ofRM packages and usual care (eg communication proto-cols routine staff visits and resources used) scenariosfor different RM classifications were developed and theircosts were estimated using bottom-up costing methodsAlthough the users can decide which of these analyses ismost representative of their setting uncertainties stillremain about the assumptions made in the estimation ofthese costs However it should be noted that themonthly costs estimated were similar to those reportedin the WSD Implementation costs (such as set-up costsstaff training costs service reconfiguration costs costs
for dual running of usual care and RM services) werenot included in the model but are often a considerationfor the health organisationsRM interventions included in the NMA were heteroge-
neous in terms of monitored parameters and selectioncriteria for HF this was the case even within specifictypes of RM (STS HH STS HM and TM) and isreflected in the uncertainty of the effectiveness para-meters A limitation of the analyses is that the effective-ness parameters remained the same for the differentcost scenarios whereas in reality there might be somecorrelation between the costs and effectiveness of differ-ent RM strategies Also it was assumed that the effective-ness and costs of the interventions are constant overtime irrespective of the duration of deploymentFurthermore as the analysis is not severity specific itassumes that the interventions are equally effective indifferent severity groups within the population underconsideration (ie patients who are recently dischargedwith HF) Repeat interventions after repeat hospitaladmissions for heart failure are not modelled and themortality risk is not reset for patients who are readmit-ted as this would need detailed evidence on baselinerisks and effectiveness in different patient groups As thisdetailed evidence is not available the cohort model usesevidence about the overall average of the patients to esti-mate the cost-effectivenessSome of the assumptions above may not hold true in
reality and therefore further research is needed to addressthese issues Given the complex nature of RM interven-tions new research should seek to examine the lsquoactiveingredientsrsquo of RM and identify patient subgroups that canbenefit most from the intervention as well as patients inwhom these interventions are unlikely to be effective Inaddition usual care ought to be more robustly deter-mined reflecting best practice as defined in the currentguidelines although this is not commonly the caseFurthermore to aid robust cost-effectiveness estimationsthe costs associated with usual care and RM interventionsneed to be reported in detail (including the costs of HFtreatment pathways) and QoL needs to be reported withobservations at specific time points in order to estimatethe difference in the utility of the patients between theRM and usual care groups Future studies should providegreater detail on reconfiguration and set-up costs and linkmore clearly with the financial impact (eg cost variationwith scale and over time) on provider organisations Wideradaptation of RM in the NHS can be facilitated by provid-ing financial impact data (eg set-up costs quarterly costsof service costs of reconfiguration) along with the long-term cost-effectiveness informationThe results of the current analysis have important
implications for the healthcare systems facing risingdemand from emergency admissions HF is a leadingcause of hospitalisation in the UK with 58 164 admis-sions recorded for HF (as first diagnoses) between April2009 and March 2010 in England and Wales25 The costof inpatient bed days for HF alone has been estimated at
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 7
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
pound563 million26 with around 90 of HF admissions toemergency departments27 lasting a median of 9 days25
The evidence shows that use of RM could substantiallyreduce HF admissions with an associated reduction inpressure on acute beds and consequent cost savingsFurthermore the use of TM might allow the potentialtransfer from emergency admission to elective admis-sion that is scheduling admissions of patients directly(not via AampE) to either a ward or to a day unit for off-loading leading to major resource savings with lesspatient disutilityIndeed the Department of Health (DH) recognised
this potential and launched an initiative lsquo3 MillionLivesrdquo (3ML) to help at least three million peoplewith long-term conditions andor social care tobenefit from the use of telehealth and telecare ser-vices28 A concordat has been entered into by the DHand the telehealth and telecare industry to worktogether to accelerate the use of TM29 Thus far sevenpathfinder sites have agreed contracts with the indus-try to ensure that 100 000 people benefit from thetechnology in 201330 Implemented effectively as partof a whole system redesign of care TM may alleviatethe pressure on long-term NHS costs and improvepeoplersquos quality of life through better self-care in thehome setting
Author affiliations1ScHARR University of Sheffield Sheffield UK2Department of Cardiology Barnet and Chase Farm Hospitals NHS TrustEnfield UK3South Yorkshire Cardiothoracic Centre Sheffield Teaching Hospitals NHSFoundation Trust Sheffield UK4Department of Cardiology Castle Hill Hospital Hull York Medical SchoolUniversity of Hull Hull UK5National Heart amp Lung Institute Imperial College London (Royal BromptonHospital) London UK
Acknowledgements The authors would like to thank Mr Tim Ellis ResearchFellow University of Sheffield Professor Mark Hawley Professor of HealthServices Research University of Sheffield Hazel Marsh Research NurseBarnsley Hospital NHS Foundation Trust and Dr Rachel OrsquoHara Lecturer inPublic Health University of Sheffield for providing clinical and TM expertiseThey would also like to thank Dr Lizzie Coates for peer reviewing the draftpaper
Contributors PT developed the decision analytical model undertook theanalysis and drafted the paper HB assisted in parameter searches modeldevelopment and analysis AB provided expert modelling advice AP wasresponsible for conception and design he undertook the systematic reviewalong with TG and provided data for the meta-analysis JWS and JW providedthe meta-analysis results and statistical input AB AAM JC and MRCprovided expert clinical input RW developed and undertook the literaturesearches All authors commented on the draftfinal paper
Funding The project was funded by the National Institute for Health Research(NIHR) Health Technology Assessment (HTA) Programme (number 0910701) and sponsored by the University of Sheffield The study funders had norole in study design in the collection analysis and interpretation of data inthe writing of the report and in the decision to submit the paper forpublication The researchers were independent of the study funders
Competing interests MRCrsquos salary is supported by the NIHR BiomedicalResearch Unit at the Royal Brompton Hospital
Provenance and peer review Not commissioned externally peer reviewed
Data sharing statement No additional data are available
Open Access This is an Open Access article distributed in accordance withthe Creative Commons Attribution Non Commercial (CC BY-NC 30) licensewhich permits others to distribute remix adapt build upon this work non-commercially and license their derivative works on different terms providedthe original work is properly cited and the use is non-commercial See httpcreativecommonsorglicensesby-nc30
REFERENCES1 Riley JP Cowie MR Telemonitoring in heart failure Heart
2009951964ndash82 Hasan A Paul V Telemonitoring in chronic heart failure Eur Heart J
2011321457ndash643 National Heart Failure Audit April 2010 to March 2011 2012 http
yhhiec org ukwp-contentuploads20111011070604_Tele_Moni_Workbk pdf httpwwwuclacuknicorauditsheartfailureadditionalfilespdfsannualreportsannual11pdf (accessed Mar2012)
4 McKelvie RS Heart failure Clin Evid 2011201102045 Anker SD Koehler F Abraham WT Telemedicine and remote
management of patients with heart failure [Review] Lancet2011378731ndash9
6 Inglis SC Clark RA McAlister FA et al Structured telephonesupport or telemonitoring programmes for patients with chronic heartfailure Cochrane Database Syst Rev 2010(8)CD007228
7 Pandor A Thokala P Gomersall T et al Home telemonitoring orstructured telephone support programmes after recent discharge inpatients with heart failure systematic review and economicevaluation Health Technol Assess 201317
8 Pandor A Pandor A Gomersall T et al Remote monitoring afterrecent hospital discharge in patients with heart failure a systematicreview and network meta-analysis Heart Published Online First 16May 2013 doi101136heartjnl-2013-303811
9 National Clinical Guideline Centre Chronic heart failure themanagement of chronic heart failure in adults in primary andsecondary care London National Clinical Guideline Centre 2012
10 Solomon SD Dobson J Pocock S et al Influence of nonfatalhospitalization for heart failure on subsequent mortality in patientswith chronic heart failure Circulation 20071161482ndash7
11 Klersy C De SA Gabutti G et al Economic impact of remotepatient monitoring an integrated economic model derived from ameta-analysis of randomized controlled trials in heart failure Eur JHeart Failure 201113450ndash9
12 Dar O Riley J Chapman C et al A randomized trial of hometelemonitoring in a typical elderly heart failure population in NorthWest London results of the Home-HF study Eur J Heart Failure200911319ndash25
13 Capomolla S Pinna GD La Rovere MT et al Heart failure casedisease management program a pilot study of home telemonitoringversus usual care Eur Heart J 20046(Suppl F)F91ndash8
14 Calvert MJ Shankar A McManus RJ et al Evaluation of themanagement of heart failure in primary care Fam Pract200926145ndash53
15 Iqbal J Francis L Reid J et al Quality of life in patients with chronicheart failure and their carers a 3-year follow-up study assessinghospitalization and mortality Eur J Heart Failure 2010121002ndash8
16 Miller LC Cox KR Miller LC et al Case management for patientswith heart failure a quality improvement intervention J GerontolNurs 20053120ndash8
17 Yao G Freemantle N Flather M et al Long-term cost-effectivenessanalysis of nebivolol compared with standard care in elderly patientswith heart failure an individual patient-based simulation modelPharmacoeconomics 200826879ndash89
18 Cleland JG Louis AA Rigby AS et al Noninvasive hometelemonitoring for patients with heart failure at high risk of recurrentadmission and death The Trans-European Network-Home-CareManagments System (TEN-HMS) study J Am Coll Cardiol2005451654ndash64
19 PSSRU Unit costs of health and social care 2011 201120 Boyne J Vrijhoef HJ Nieman FH et al Telemonitoring in patients
with heart failure results from a multicenter randomized controlledtrial (the tehaf study) J Am Coll Cardiol 201157(14 Suppl 1)E389
21 Department of Health NHS reference costs 2007ndash08 2009 LondonUK 2009
22 Miller G Randolph S Forkner E et al Long-term cost-effectivenessof disease management in systolic heart failure Med Deci Making200929325ndash33
8 Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
23 Galbreath AD Krasuski RA Smith B et al Long-term healthcareand cost outcome of disease management in a large randomizedcommunity-based population with heart failure Circulation20041103518ndash26
24 Henderson C Knapp M Fernandez J-L et al Cost effectiveness oftelehealth for patients with long term conditions (Whole SystemsDemonstrator telehealth questionnaire study) nested economicevaluation in a pragmatic cluster randomised controlled trialBMJ 2013346f1035
25 NHS information centre National Heart Failure Audit 2010 httpwww npc nhs ukrapidreviewp=2479 2010 httpwwwnpcnhsukrapidreviewp=2479
26 Cleland JG McDonagh T Rigby AS et al The national heart failureaudit for England and Wales 2008ndash2009 Heart 201197876ndash86
27 HES Online Hospital Episode Statistics 2008ndash2009 2012 httpwwwhesonlinenhsuk
28 3millionlives Improving your access to telehealth and telecare 12 AD http3millionlivescouk
29 A concordat between the Department of Health and the telehealthand telecare industry 12 AD http3millionlivescoukwp-contentuploads201203Concordat-FINALpdf
30 100000 people with long-term conditions to benefit from technologyin 2013 12 AD http3millionlivescoukwp-contentuploads20121114-November-2012-press-releasepdf
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 9
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from

year was 067ndash01 that is 057 Within the PSA theuncertainty in the utility values was represented using anormal distribution using the deterministic values as themean with an SD of 0015 and estimated based on thedifference between the utilities reported by Capomollaet al13 and Iqbal et al15 while the disutility was repre-sented using a triangular distribution with (minus008 011)as the range with minus01 as the mode
CostsThe costs used in the model are (1) costs of RM inter-ventions after initial discharge only (2) costs of usualcare and (3) repeat hospitalisation costs These costs aresummarised in table 4 and are described in detail in thissectionThe RM studies did not report clearly or in detail
what was involved in the usual postdischarge care orRM thus making it difficult to accurately determine thecosts8 Owing to the variation involved in the RM inter-ventions and usual care cost scenarios were developedfor each RM classification (ie STS HM STS HH andTM) and usual care These costs were estimated using
bottom-up costing methods for a typical health organisa-tion of 250 HF patients (estimated based on the mediansize of the NHS Foundation Trusts in the UK) for aperiod of 6 months Furthermore it was assumed thatafter 6 months all patients would receive usual care asrecommended in NICE clinical guidelines for the man-agement of adults with CHF9 irrespective of whetherthey received the remote monitoring intervention orpostdischarge usual care during the intervention periodIt was assumed that the usual postdischarge care was
the same as that described in the TEN-HMS study18 andthe usual care costs were estimated by applying thehourly NHS staff rates from PSSRU 201119 to theresource use data in the TEN-HMS study18 A high costusual postdischarge care scenario was also developedbased on discussions with the clinical expert group (ABAAM JC and MRC)The total costs of RM interventions were broken down
into the costs of the device monitoring costs andmedical care costs8 The costs of the RM devices wereelicited from an expert advisory group The monitoringcosts were estimated using activity-based costing for the
Table 4 Cost parameters used in the economic model
Costs (in pound) per 6 months
Base-case
scenario
Low-cost
scenario
High-cost
scenario Source
UC pound161 ndash pound592 TEN-HMS18 Clinical opinion
STS HM pound715 pound623 pound794 Clinical opinion
STS HH pound1075 pound1051 pound1152 Clinical opinion
TM pound1051 pound801 pound1288 Clinical opinion
Usual care costs (per month) after 6 month intervention duration
UC after 6 months pound823 ndash ndash NICE HF guidelines9
Hospitalisation costs Estimate Lower 95 CI Upper 95 CI
HF-related hospitalisations pound251449 pound1857 pound2809 NHS Reference Costs for
201121
Other-cause hospitalisationsdagger pound152979 pound1129 pound1709 NHS Reference Costs for
201121
Heart failure or shock (EB03H EB03I) non-elective inpatient (long stay) including excess bed days21
daggerNon-elective inpatient (long stay and short stay) including excess bed days21
Table 3 HRs for interventions versus usual care for all-cause mortality and hospitalisations
HRs for interventions versus usual care for mortality (all-cause) and hospitalisation (all-cause and HF) from NMA
including Home-HF12 study
Type
All-cause mortality HF-hospitalisation All-cause hospitalisation
R 95 PrI HR 95 PrI HR 95 PrI
STS HH 077 (031 186) 077 (050 119) 097 (038 243)
STS HM 098 (030 323) 103 (058 177) 106 (031 361)
TM 076 (030 191) 095 (059 162) 075 (028 191)
HRs for interventions versus usual care for mortality (all-cause) and hospitalisation (all-cause and HF) from NMA
excluding Home-HF12 study
STS HH 075 (045 127) 076 (051 113) 096 (042 218)
STS HM 098 (049 195) 102 (061 169) 106 (035 322)
TM 062 (035 109) 086 (054 138) 067 (026 153)
HR hazard ratio PrI predictive interval STS HM structured telephone support via human to machine interface STS HH structuredtelephone support via human to human contact TM telemonitoring
4 Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
resources spent by the staff on triage and follow-upbased on evidence from the literature20 The costs ofmedical care for the usual care arm STS and TM armswere estimated by applying the hourly NHS staff ratesfrom PSSRU 201119 to their respective medical careresource use data reported in the TEN-HMS study18
The mean inpatient admission cost for HF-related hos-pitalisations was calculated from the weighted average ofthe costs for the HRG lsquoHeart Failure or Shockrdquo (EB03HEB03I) based on the data obtained from the NHSReference Costs for 201121 For hospital admissions forany cause other than HF it was assumed that these costswere the same as the mean cost of hospital admissionfor the general population This was estimated as aweighted average of elective inpatient admissions andnon-elective inpatient admissions (including short andlong stay) based on the data from the NHS ReferenceCosts for 201121
RESULTSThe results of the cost-effectiveness analysis using basecase costs are presented in table 5 for both estimates ofeffectiveness including and excluding data from theHome-HF study12 to address the uncertainty inthe effectiveness evidence Results are also presented forfive cost scenarios (higher usual care cost scenariolower cost scenario of TM higher cost scenario of TMlower STS cost scenario and higher STS cost scenario)and the 12 month intervention duration scenario inonline supplementary tables S1 and S2 respectivelyIn the analysis using base case costs TM is the most
cost-effective strategy at a threshold of pound20 000QALY inboth analyses that is including and excluding theHome-HF study12 TM is also the most effective strategy(ie highest QALYs gained) in the analyses that excludedthe Home-HF study12 but not in the analyses thatincluded the Home-HF study12 with STS HH providingthe highest number of expected QALYs However the
additional QALYs gained by STS HH are not worth theadditional costs of the strategy as seen in the ICERs(against TM) greater than the threshold of pound20 000QALYIn the analyses that included the Home-HF study12
there is only a 40 chance of TM being cost-effective atthe threshold of pound20 000QALY as shown in figure 1Excluding the Home-HF study12 the probability that TMduring office hours is cost-effective increases to 73(figure 2)Scenario analyses performed using higher costs of
usual care higher costs of STS HH and lower costs ofTM do not substantially change the conclusions TM wasestimated to be the most cost-effective strategy in allthese scenarios Scenario analysis performed usinghigher costs of TM (pound215month) suggested that TM isdominated by STS HH This is because a small changein the difference between costs of TM and STS HH ledto a marked change in ICERs given the small difference(00021 QALYs) in expected QALYs between STS HHand TM in the analyses that included the Home-HFstudy12 However the same scenario analysis (ie highercost of TM of pound215month) that excluded the data fromthe Home-HF study12 suggested that TM is still the mostcost-effective strategy with an ICER of pound8223QALYagainst usual care (STS HH is extendedly dominated bya combination of usual care and TM) This is due to themuch higher difference in the expected QALYs betweenSTS HH and TM (00602 QALYs) where a small changein the difference between costs of TM and STS HHcannot lead to a marked change in the ICER Thethreshold analysis suggested that the monthly cost of TMhas to be higher than pound390month to have an ICERgreater than pound20 000QALY against STS HH The ICERof TM against usual care at this monthly cost of pound390 ispound13 357QALYScenario analyses performed using different estimates
of the disutility for HF-related and other cause hospitali-sations produced results similar to that in the base case
Table 5 Summary of the economic analysis results using base case costs
Usual care STS HM STS HH TM
Total costs
Including Home-HF12 pound8478 pound8965 pound9574 pound9437
Excluding Home-HF12 pound8478 pound9087 pound9658 pound9665
Total QALYs
Including Home-HF12 24137 23633 24950 24944
Excluding Home-HF12 24137 24043 25230 25847
ICERs
Including Home-HF12 Dominated pound228 035 pound11 873
Excluding Home-HF12 Dominated Extendedly dominated pound6942
Probability of cost-effectiveness ()
Including Home-HF12 6 19 35 40
Excluding Home-HF12 1 7 19 73
Last strategy in the cost-effectiveness frontierICERs incremental cost-effectiveness ratios QALYs quality adjusted life years STS HH structured telephone support via human to humancontact STS HM structured telephone support via human to machine interface TM telemonitoring
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 5
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
analysis that is the results are robust to the variations inthe disutility of hospitalisationsScenario analysis using a 12-month treatment duration
produced similar results as in the 6-month treatmentduration scenarios TM for 12 months was also cost-effective when compared with TM for 6 months with anICER of pound14 066QALY However treating 2timesN patientsusing TM for 6 months was cost-effective with it beingdominant against a combination of treating N patientsusing TM for 12 months with the rest of the N patientsunder usual care
DISCUSSIONThe results of the base case cost-effectiveness analysessuggest that TM is expected to be the most cost-effectivestrategy at a threshold of pound20 000QALY However thereis uncertainty involved in suggesting that TM is the mostprobable cost-effective strategy and in particular thereis greater uncertainty when data from the Home-HFstudy12 is included than when it is excluded For
decision-makers the key question is whether the usualcare arm in their local setting is similar to the usual carearm in the Home-HF study12 If so then the resultsincluding the Home-HF study12 might be consideredmore relevant and if not the results excluding theHome-HF study12 might be considered more relevantThe scenario analysis performed (using higher usualcare costs lower TM costs higher TM costs and higherSTS costs) did not substantially change the conclusionsTM was estimated to be the most cost-effective strategyin all these scenarios Furthermore TM for 12 monthswas also cost-effective when compared with TM for6 months which suggests that it is cost-effective to keepthe patients on TM beyond 6 months In situations witha limited number of TM devices assuming a homoge-neous patient group it is cost-effective to treat allpatients using TM for 6 months than using TM for12 months on half the patients with the other half of thepatients under usual careThere have been two cost-effectiveness analyses studies
of RM in HF but neither considered the different RM
Figure 1 Cost effectiveness
acceptability curve for base case
economic analysis using
effectiveness data including the
Home-HF study12
Figure 2 Cost effectiveness
acceptability curve for economic
analysis using effectiveness data
excluding the Home-HF study12
6 Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
approaches separately11 22 The analysis reported byMiller et al22 was based on a single trial of STS23
whereas Klersy et al11 included data from a meta-analysisof a wide range of RM studies Miller et al22 estimatedthat STS compared with usual care had an ICER around$43 650QALY this study did not include a PSA butunivariate sensitivity analyses (ICER varying from$28 691 to $129 738 per QALY) was performed Klersyet al11 focused mainly on the effectiveness rather thanthe costs and used a time horizon of 1 year A budgetimpact analysis was presented and the differentdiagnosis-related group (DRG) reimbursement tariffgroups as a proxy for hospitalisation costs were consid-ered with cost savings per patient ranging betweeneuro3068 and euro99294 However other costs such as RMcosts and outpatient visit costs were not considered Theauthors performed scenario analyses using differentDRG costs as part of the budget analysis to address theuncertainty in the hospitalisation costs but neitherdeterministic sensitivity analysis nor PSA was performedThe Whole systems demonstrator (WSD) pro-
gramme24 a randomised controlled trial of telehealththat included over 6000 patients analysed costs and out-comes for 965 patients monitored for 12 months 534receiving telehealth and 431 receiving usual careCost-effectiveness analysis estimated the ICER atpound92 000QALY when telehealth was added to usual carefor people with chronic conditions (diabetes HF andchronic obstructive pulmonary disease (COPD))However this trial-based evaluation (with a time horizonof 1 year) potentially underestimates the health benefitsas it does not include the long-term QALYs gained fromthe reduction in mortality Furthermore the WSD ana-lysis included all patients with chronic conditions (dia-betes HF and COPD) whereas the population underconsideration in our analysis included patients who hadbeen recently discharged with HF The cost-effectivenessresults for HF patients are not yet publicly available in apeer-reviewed journal and thus it is difficult to comparethe results of the current analysis with the results of theWSD analysisThe analysis reported in this paper also has some lim-
itations that need to be taken into account Any model-ling process involves simplifications and assumptionsthat may not accurately reflect clinical practice Owingto the lack of detail provided in research studiesincluded in the NMA concerning the components ofRM packages and usual care (eg communication proto-cols routine staff visits and resources used) scenariosfor different RM classifications were developed and theircosts were estimated using bottom-up costing methodsAlthough the users can decide which of these analyses ismost representative of their setting uncertainties stillremain about the assumptions made in the estimation ofthese costs However it should be noted that themonthly costs estimated were similar to those reportedin the WSD Implementation costs (such as set-up costsstaff training costs service reconfiguration costs costs
for dual running of usual care and RM services) werenot included in the model but are often a considerationfor the health organisationsRM interventions included in the NMA were heteroge-
neous in terms of monitored parameters and selectioncriteria for HF this was the case even within specifictypes of RM (STS HH STS HM and TM) and isreflected in the uncertainty of the effectiveness para-meters A limitation of the analyses is that the effective-ness parameters remained the same for the differentcost scenarios whereas in reality there might be somecorrelation between the costs and effectiveness of differ-ent RM strategies Also it was assumed that the effective-ness and costs of the interventions are constant overtime irrespective of the duration of deploymentFurthermore as the analysis is not severity specific itassumes that the interventions are equally effective indifferent severity groups within the population underconsideration (ie patients who are recently dischargedwith HF) Repeat interventions after repeat hospitaladmissions for heart failure are not modelled and themortality risk is not reset for patients who are readmit-ted as this would need detailed evidence on baselinerisks and effectiveness in different patient groups As thisdetailed evidence is not available the cohort model usesevidence about the overall average of the patients to esti-mate the cost-effectivenessSome of the assumptions above may not hold true in
reality and therefore further research is needed to addressthese issues Given the complex nature of RM interven-tions new research should seek to examine the lsquoactiveingredientsrsquo of RM and identify patient subgroups that canbenefit most from the intervention as well as patients inwhom these interventions are unlikely to be effective Inaddition usual care ought to be more robustly deter-mined reflecting best practice as defined in the currentguidelines although this is not commonly the caseFurthermore to aid robust cost-effectiveness estimationsthe costs associated with usual care and RM interventionsneed to be reported in detail (including the costs of HFtreatment pathways) and QoL needs to be reported withobservations at specific time points in order to estimatethe difference in the utility of the patients between theRM and usual care groups Future studies should providegreater detail on reconfiguration and set-up costs and linkmore clearly with the financial impact (eg cost variationwith scale and over time) on provider organisations Wideradaptation of RM in the NHS can be facilitated by provid-ing financial impact data (eg set-up costs quarterly costsof service costs of reconfiguration) along with the long-term cost-effectiveness informationThe results of the current analysis have important
implications for the healthcare systems facing risingdemand from emergency admissions HF is a leadingcause of hospitalisation in the UK with 58 164 admis-sions recorded for HF (as first diagnoses) between April2009 and March 2010 in England and Wales25 The costof inpatient bed days for HF alone has been estimated at
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 7
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
pound563 million26 with around 90 of HF admissions toemergency departments27 lasting a median of 9 days25
The evidence shows that use of RM could substantiallyreduce HF admissions with an associated reduction inpressure on acute beds and consequent cost savingsFurthermore the use of TM might allow the potentialtransfer from emergency admission to elective admis-sion that is scheduling admissions of patients directly(not via AampE) to either a ward or to a day unit for off-loading leading to major resource savings with lesspatient disutilityIndeed the Department of Health (DH) recognised
this potential and launched an initiative lsquo3 MillionLivesrdquo (3ML) to help at least three million peoplewith long-term conditions andor social care tobenefit from the use of telehealth and telecare ser-vices28 A concordat has been entered into by the DHand the telehealth and telecare industry to worktogether to accelerate the use of TM29 Thus far sevenpathfinder sites have agreed contracts with the indus-try to ensure that 100 000 people benefit from thetechnology in 201330 Implemented effectively as partof a whole system redesign of care TM may alleviatethe pressure on long-term NHS costs and improvepeoplersquos quality of life through better self-care in thehome setting
Author affiliations1ScHARR University of Sheffield Sheffield UK2Department of Cardiology Barnet and Chase Farm Hospitals NHS TrustEnfield UK3South Yorkshire Cardiothoracic Centre Sheffield Teaching Hospitals NHSFoundation Trust Sheffield UK4Department of Cardiology Castle Hill Hospital Hull York Medical SchoolUniversity of Hull Hull UK5National Heart amp Lung Institute Imperial College London (Royal BromptonHospital) London UK
Acknowledgements The authors would like to thank Mr Tim Ellis ResearchFellow University of Sheffield Professor Mark Hawley Professor of HealthServices Research University of Sheffield Hazel Marsh Research NurseBarnsley Hospital NHS Foundation Trust and Dr Rachel OrsquoHara Lecturer inPublic Health University of Sheffield for providing clinical and TM expertiseThey would also like to thank Dr Lizzie Coates for peer reviewing the draftpaper
Contributors PT developed the decision analytical model undertook theanalysis and drafted the paper HB assisted in parameter searches modeldevelopment and analysis AB provided expert modelling advice AP wasresponsible for conception and design he undertook the systematic reviewalong with TG and provided data for the meta-analysis JWS and JW providedthe meta-analysis results and statistical input AB AAM JC and MRCprovided expert clinical input RW developed and undertook the literaturesearches All authors commented on the draftfinal paper
Funding The project was funded by the National Institute for Health Research(NIHR) Health Technology Assessment (HTA) Programme (number 0910701) and sponsored by the University of Sheffield The study funders had norole in study design in the collection analysis and interpretation of data inthe writing of the report and in the decision to submit the paper forpublication The researchers were independent of the study funders
Competing interests MRCrsquos salary is supported by the NIHR BiomedicalResearch Unit at the Royal Brompton Hospital
Provenance and peer review Not commissioned externally peer reviewed
Data sharing statement No additional data are available
Open Access This is an Open Access article distributed in accordance withthe Creative Commons Attribution Non Commercial (CC BY-NC 30) licensewhich permits others to distribute remix adapt build upon this work non-commercially and license their derivative works on different terms providedthe original work is properly cited and the use is non-commercial See httpcreativecommonsorglicensesby-nc30
REFERENCES1 Riley JP Cowie MR Telemonitoring in heart failure Heart
2009951964ndash82 Hasan A Paul V Telemonitoring in chronic heart failure Eur Heart J
2011321457ndash643 National Heart Failure Audit April 2010 to March 2011 2012 http
yhhiec org ukwp-contentuploads20111011070604_Tele_Moni_Workbk pdf httpwwwuclacuknicorauditsheartfailureadditionalfilespdfsannualreportsannual11pdf (accessed Mar2012)
4 McKelvie RS Heart failure Clin Evid 2011201102045 Anker SD Koehler F Abraham WT Telemedicine and remote
management of patients with heart failure [Review] Lancet2011378731ndash9
6 Inglis SC Clark RA McAlister FA et al Structured telephonesupport or telemonitoring programmes for patients with chronic heartfailure Cochrane Database Syst Rev 2010(8)CD007228
7 Pandor A Thokala P Gomersall T et al Home telemonitoring orstructured telephone support programmes after recent discharge inpatients with heart failure systematic review and economicevaluation Health Technol Assess 201317
8 Pandor A Pandor A Gomersall T et al Remote monitoring afterrecent hospital discharge in patients with heart failure a systematicreview and network meta-analysis Heart Published Online First 16May 2013 doi101136heartjnl-2013-303811
9 National Clinical Guideline Centre Chronic heart failure themanagement of chronic heart failure in adults in primary andsecondary care London National Clinical Guideline Centre 2012
10 Solomon SD Dobson J Pocock S et al Influence of nonfatalhospitalization for heart failure on subsequent mortality in patientswith chronic heart failure Circulation 20071161482ndash7
11 Klersy C De SA Gabutti G et al Economic impact of remotepatient monitoring an integrated economic model derived from ameta-analysis of randomized controlled trials in heart failure Eur JHeart Failure 201113450ndash9
12 Dar O Riley J Chapman C et al A randomized trial of hometelemonitoring in a typical elderly heart failure population in NorthWest London results of the Home-HF study Eur J Heart Failure200911319ndash25
13 Capomolla S Pinna GD La Rovere MT et al Heart failure casedisease management program a pilot study of home telemonitoringversus usual care Eur Heart J 20046(Suppl F)F91ndash8
14 Calvert MJ Shankar A McManus RJ et al Evaluation of themanagement of heart failure in primary care Fam Pract200926145ndash53
15 Iqbal J Francis L Reid J et al Quality of life in patients with chronicheart failure and their carers a 3-year follow-up study assessinghospitalization and mortality Eur J Heart Failure 2010121002ndash8
16 Miller LC Cox KR Miller LC et al Case management for patientswith heart failure a quality improvement intervention J GerontolNurs 20053120ndash8
17 Yao G Freemantle N Flather M et al Long-term cost-effectivenessanalysis of nebivolol compared with standard care in elderly patientswith heart failure an individual patient-based simulation modelPharmacoeconomics 200826879ndash89
18 Cleland JG Louis AA Rigby AS et al Noninvasive hometelemonitoring for patients with heart failure at high risk of recurrentadmission and death The Trans-European Network-Home-CareManagments System (TEN-HMS) study J Am Coll Cardiol2005451654ndash64
19 PSSRU Unit costs of health and social care 2011 201120 Boyne J Vrijhoef HJ Nieman FH et al Telemonitoring in patients
with heart failure results from a multicenter randomized controlledtrial (the tehaf study) J Am Coll Cardiol 201157(14 Suppl 1)E389
21 Department of Health NHS reference costs 2007ndash08 2009 LondonUK 2009
22 Miller G Randolph S Forkner E et al Long-term cost-effectivenessof disease management in systolic heart failure Med Deci Making200929325ndash33
8 Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
23 Galbreath AD Krasuski RA Smith B et al Long-term healthcareand cost outcome of disease management in a large randomizedcommunity-based population with heart failure Circulation20041103518ndash26
24 Henderson C Knapp M Fernandez J-L et al Cost effectiveness oftelehealth for patients with long term conditions (Whole SystemsDemonstrator telehealth questionnaire study) nested economicevaluation in a pragmatic cluster randomised controlled trialBMJ 2013346f1035
25 NHS information centre National Heart Failure Audit 2010 httpwww npc nhs ukrapidreviewp=2479 2010 httpwwwnpcnhsukrapidreviewp=2479
26 Cleland JG McDonagh T Rigby AS et al The national heart failureaudit for England and Wales 2008ndash2009 Heart 201197876ndash86
27 HES Online Hospital Episode Statistics 2008ndash2009 2012 httpwwwhesonlinenhsuk
28 3millionlives Improving your access to telehealth and telecare 12 AD http3millionlivescouk
29 A concordat between the Department of Health and the telehealthand telecare industry 12 AD http3millionlivescoukwp-contentuploads201203Concordat-FINALpdf
30 100000 people with long-term conditions to benefit from technologyin 2013 12 AD http3millionlivescoukwp-contentuploads20121114-November-2012-press-releasepdf
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 9
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from

resources spent by the staff on triage and follow-upbased on evidence from the literature20 The costs ofmedical care for the usual care arm STS and TM armswere estimated by applying the hourly NHS staff ratesfrom PSSRU 201119 to their respective medical careresource use data reported in the TEN-HMS study18
The mean inpatient admission cost for HF-related hos-pitalisations was calculated from the weighted average ofthe costs for the HRG lsquoHeart Failure or Shockrdquo (EB03HEB03I) based on the data obtained from the NHSReference Costs for 201121 For hospital admissions forany cause other than HF it was assumed that these costswere the same as the mean cost of hospital admissionfor the general population This was estimated as aweighted average of elective inpatient admissions andnon-elective inpatient admissions (including short andlong stay) based on the data from the NHS ReferenceCosts for 201121
RESULTSThe results of the cost-effectiveness analysis using basecase costs are presented in table 5 for both estimates ofeffectiveness including and excluding data from theHome-HF study12 to address the uncertainty inthe effectiveness evidence Results are also presented forfive cost scenarios (higher usual care cost scenariolower cost scenario of TM higher cost scenario of TMlower STS cost scenario and higher STS cost scenario)and the 12 month intervention duration scenario inonline supplementary tables S1 and S2 respectivelyIn the analysis using base case costs TM is the most
cost-effective strategy at a threshold of pound20 000QALY inboth analyses that is including and excluding theHome-HF study12 TM is also the most effective strategy(ie highest QALYs gained) in the analyses that excludedthe Home-HF study12 but not in the analyses thatincluded the Home-HF study12 with STS HH providingthe highest number of expected QALYs However the
additional QALYs gained by STS HH are not worth theadditional costs of the strategy as seen in the ICERs(against TM) greater than the threshold of pound20 000QALYIn the analyses that included the Home-HF study12
there is only a 40 chance of TM being cost-effective atthe threshold of pound20 000QALY as shown in figure 1Excluding the Home-HF study12 the probability that TMduring office hours is cost-effective increases to 73(figure 2)Scenario analyses performed using higher costs of
usual care higher costs of STS HH and lower costs ofTM do not substantially change the conclusions TM wasestimated to be the most cost-effective strategy in allthese scenarios Scenario analysis performed usinghigher costs of TM (pound215month) suggested that TM isdominated by STS HH This is because a small changein the difference between costs of TM and STS HH ledto a marked change in ICERs given the small difference(00021 QALYs) in expected QALYs between STS HHand TM in the analyses that included the Home-HFstudy12 However the same scenario analysis (ie highercost of TM of pound215month) that excluded the data fromthe Home-HF study12 suggested that TM is still the mostcost-effective strategy with an ICER of pound8223QALYagainst usual care (STS HH is extendedly dominated bya combination of usual care and TM) This is due to themuch higher difference in the expected QALYs betweenSTS HH and TM (00602 QALYs) where a small changein the difference between costs of TM and STS HHcannot lead to a marked change in the ICER Thethreshold analysis suggested that the monthly cost of TMhas to be higher than pound390month to have an ICERgreater than pound20 000QALY against STS HH The ICERof TM against usual care at this monthly cost of pound390 ispound13 357QALYScenario analyses performed using different estimates
of the disutility for HF-related and other cause hospitali-sations produced results similar to that in the base case
Table 5 Summary of the economic analysis results using base case costs
Usual care STS HM STS HH TM
Total costs
Including Home-HF12 pound8478 pound8965 pound9574 pound9437
Excluding Home-HF12 pound8478 pound9087 pound9658 pound9665
Total QALYs
Including Home-HF12 24137 23633 24950 24944
Excluding Home-HF12 24137 24043 25230 25847
ICERs
Including Home-HF12 Dominated pound228 035 pound11 873
Excluding Home-HF12 Dominated Extendedly dominated pound6942
Probability of cost-effectiveness ()
Including Home-HF12 6 19 35 40
Excluding Home-HF12 1 7 19 73
Last strategy in the cost-effectiveness frontierICERs incremental cost-effectiveness ratios QALYs quality adjusted life years STS HH structured telephone support via human to humancontact STS HM structured telephone support via human to machine interface TM telemonitoring
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 5
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
analysis that is the results are robust to the variations inthe disutility of hospitalisationsScenario analysis using a 12-month treatment duration
produced similar results as in the 6-month treatmentduration scenarios TM for 12 months was also cost-effective when compared with TM for 6 months with anICER of pound14 066QALY However treating 2timesN patientsusing TM for 6 months was cost-effective with it beingdominant against a combination of treating N patientsusing TM for 12 months with the rest of the N patientsunder usual care
DISCUSSIONThe results of the base case cost-effectiveness analysessuggest that TM is expected to be the most cost-effectivestrategy at a threshold of pound20 000QALY However thereis uncertainty involved in suggesting that TM is the mostprobable cost-effective strategy and in particular thereis greater uncertainty when data from the Home-HFstudy12 is included than when it is excluded For
decision-makers the key question is whether the usualcare arm in their local setting is similar to the usual carearm in the Home-HF study12 If so then the resultsincluding the Home-HF study12 might be consideredmore relevant and if not the results excluding theHome-HF study12 might be considered more relevantThe scenario analysis performed (using higher usualcare costs lower TM costs higher TM costs and higherSTS costs) did not substantially change the conclusionsTM was estimated to be the most cost-effective strategyin all these scenarios Furthermore TM for 12 monthswas also cost-effective when compared with TM for6 months which suggests that it is cost-effective to keepthe patients on TM beyond 6 months In situations witha limited number of TM devices assuming a homoge-neous patient group it is cost-effective to treat allpatients using TM for 6 months than using TM for12 months on half the patients with the other half of thepatients under usual careThere have been two cost-effectiveness analyses studies
of RM in HF but neither considered the different RM
Figure 1 Cost effectiveness
acceptability curve for base case
economic analysis using
effectiveness data including the
Home-HF study12
Figure 2 Cost effectiveness
acceptability curve for economic
analysis using effectiveness data
excluding the Home-HF study12
6 Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
approaches separately11 22 The analysis reported byMiller et al22 was based on a single trial of STS23
whereas Klersy et al11 included data from a meta-analysisof a wide range of RM studies Miller et al22 estimatedthat STS compared with usual care had an ICER around$43 650QALY this study did not include a PSA butunivariate sensitivity analyses (ICER varying from$28 691 to $129 738 per QALY) was performed Klersyet al11 focused mainly on the effectiveness rather thanthe costs and used a time horizon of 1 year A budgetimpact analysis was presented and the differentdiagnosis-related group (DRG) reimbursement tariffgroups as a proxy for hospitalisation costs were consid-ered with cost savings per patient ranging betweeneuro3068 and euro99294 However other costs such as RMcosts and outpatient visit costs were not considered Theauthors performed scenario analyses using differentDRG costs as part of the budget analysis to address theuncertainty in the hospitalisation costs but neitherdeterministic sensitivity analysis nor PSA was performedThe Whole systems demonstrator (WSD) pro-
gramme24 a randomised controlled trial of telehealththat included over 6000 patients analysed costs and out-comes for 965 patients monitored for 12 months 534receiving telehealth and 431 receiving usual careCost-effectiveness analysis estimated the ICER atpound92 000QALY when telehealth was added to usual carefor people with chronic conditions (diabetes HF andchronic obstructive pulmonary disease (COPD))However this trial-based evaluation (with a time horizonof 1 year) potentially underestimates the health benefitsas it does not include the long-term QALYs gained fromthe reduction in mortality Furthermore the WSD ana-lysis included all patients with chronic conditions (dia-betes HF and COPD) whereas the population underconsideration in our analysis included patients who hadbeen recently discharged with HF The cost-effectivenessresults for HF patients are not yet publicly available in apeer-reviewed journal and thus it is difficult to comparethe results of the current analysis with the results of theWSD analysisThe analysis reported in this paper also has some lim-
itations that need to be taken into account Any model-ling process involves simplifications and assumptionsthat may not accurately reflect clinical practice Owingto the lack of detail provided in research studiesincluded in the NMA concerning the components ofRM packages and usual care (eg communication proto-cols routine staff visits and resources used) scenariosfor different RM classifications were developed and theircosts were estimated using bottom-up costing methodsAlthough the users can decide which of these analyses ismost representative of their setting uncertainties stillremain about the assumptions made in the estimation ofthese costs However it should be noted that themonthly costs estimated were similar to those reportedin the WSD Implementation costs (such as set-up costsstaff training costs service reconfiguration costs costs
for dual running of usual care and RM services) werenot included in the model but are often a considerationfor the health organisationsRM interventions included in the NMA were heteroge-
neous in terms of monitored parameters and selectioncriteria for HF this was the case even within specifictypes of RM (STS HH STS HM and TM) and isreflected in the uncertainty of the effectiveness para-meters A limitation of the analyses is that the effective-ness parameters remained the same for the differentcost scenarios whereas in reality there might be somecorrelation between the costs and effectiveness of differ-ent RM strategies Also it was assumed that the effective-ness and costs of the interventions are constant overtime irrespective of the duration of deploymentFurthermore as the analysis is not severity specific itassumes that the interventions are equally effective indifferent severity groups within the population underconsideration (ie patients who are recently dischargedwith HF) Repeat interventions after repeat hospitaladmissions for heart failure are not modelled and themortality risk is not reset for patients who are readmit-ted as this would need detailed evidence on baselinerisks and effectiveness in different patient groups As thisdetailed evidence is not available the cohort model usesevidence about the overall average of the patients to esti-mate the cost-effectivenessSome of the assumptions above may not hold true in
reality and therefore further research is needed to addressthese issues Given the complex nature of RM interven-tions new research should seek to examine the lsquoactiveingredientsrsquo of RM and identify patient subgroups that canbenefit most from the intervention as well as patients inwhom these interventions are unlikely to be effective Inaddition usual care ought to be more robustly deter-mined reflecting best practice as defined in the currentguidelines although this is not commonly the caseFurthermore to aid robust cost-effectiveness estimationsthe costs associated with usual care and RM interventionsneed to be reported in detail (including the costs of HFtreatment pathways) and QoL needs to be reported withobservations at specific time points in order to estimatethe difference in the utility of the patients between theRM and usual care groups Future studies should providegreater detail on reconfiguration and set-up costs and linkmore clearly with the financial impact (eg cost variationwith scale and over time) on provider organisations Wideradaptation of RM in the NHS can be facilitated by provid-ing financial impact data (eg set-up costs quarterly costsof service costs of reconfiguration) along with the long-term cost-effectiveness informationThe results of the current analysis have important
implications for the healthcare systems facing risingdemand from emergency admissions HF is a leadingcause of hospitalisation in the UK with 58 164 admis-sions recorded for HF (as first diagnoses) between April2009 and March 2010 in England and Wales25 The costof inpatient bed days for HF alone has been estimated at
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 7
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
pound563 million26 with around 90 of HF admissions toemergency departments27 lasting a median of 9 days25
The evidence shows that use of RM could substantiallyreduce HF admissions with an associated reduction inpressure on acute beds and consequent cost savingsFurthermore the use of TM might allow the potentialtransfer from emergency admission to elective admis-sion that is scheduling admissions of patients directly(not via AampE) to either a ward or to a day unit for off-loading leading to major resource savings with lesspatient disutilityIndeed the Department of Health (DH) recognised
this potential and launched an initiative lsquo3 MillionLivesrdquo (3ML) to help at least three million peoplewith long-term conditions andor social care tobenefit from the use of telehealth and telecare ser-vices28 A concordat has been entered into by the DHand the telehealth and telecare industry to worktogether to accelerate the use of TM29 Thus far sevenpathfinder sites have agreed contracts with the indus-try to ensure that 100 000 people benefit from thetechnology in 201330 Implemented effectively as partof a whole system redesign of care TM may alleviatethe pressure on long-term NHS costs and improvepeoplersquos quality of life through better self-care in thehome setting
Author affiliations1ScHARR University of Sheffield Sheffield UK2Department of Cardiology Barnet and Chase Farm Hospitals NHS TrustEnfield UK3South Yorkshire Cardiothoracic Centre Sheffield Teaching Hospitals NHSFoundation Trust Sheffield UK4Department of Cardiology Castle Hill Hospital Hull York Medical SchoolUniversity of Hull Hull UK5National Heart amp Lung Institute Imperial College London (Royal BromptonHospital) London UK
Acknowledgements The authors would like to thank Mr Tim Ellis ResearchFellow University of Sheffield Professor Mark Hawley Professor of HealthServices Research University of Sheffield Hazel Marsh Research NurseBarnsley Hospital NHS Foundation Trust and Dr Rachel OrsquoHara Lecturer inPublic Health University of Sheffield for providing clinical and TM expertiseThey would also like to thank Dr Lizzie Coates for peer reviewing the draftpaper
Contributors PT developed the decision analytical model undertook theanalysis and drafted the paper HB assisted in parameter searches modeldevelopment and analysis AB provided expert modelling advice AP wasresponsible for conception and design he undertook the systematic reviewalong with TG and provided data for the meta-analysis JWS and JW providedthe meta-analysis results and statistical input AB AAM JC and MRCprovided expert clinical input RW developed and undertook the literaturesearches All authors commented on the draftfinal paper
Funding The project was funded by the National Institute for Health Research(NIHR) Health Technology Assessment (HTA) Programme (number 0910701) and sponsored by the University of Sheffield The study funders had norole in study design in the collection analysis and interpretation of data inthe writing of the report and in the decision to submit the paper forpublication The researchers were independent of the study funders
Competing interests MRCrsquos salary is supported by the NIHR BiomedicalResearch Unit at the Royal Brompton Hospital
Provenance and peer review Not commissioned externally peer reviewed
Data sharing statement No additional data are available
Open Access This is an Open Access article distributed in accordance withthe Creative Commons Attribution Non Commercial (CC BY-NC 30) licensewhich permits others to distribute remix adapt build upon this work non-commercially and license their derivative works on different terms providedthe original work is properly cited and the use is non-commercial See httpcreativecommonsorglicensesby-nc30
REFERENCES1 Riley JP Cowie MR Telemonitoring in heart failure Heart
2009951964ndash82 Hasan A Paul V Telemonitoring in chronic heart failure Eur Heart J
2011321457ndash643 National Heart Failure Audit April 2010 to March 2011 2012 http
yhhiec org ukwp-contentuploads20111011070604_Tele_Moni_Workbk pdf httpwwwuclacuknicorauditsheartfailureadditionalfilespdfsannualreportsannual11pdf (accessed Mar2012)
4 McKelvie RS Heart failure Clin Evid 2011201102045 Anker SD Koehler F Abraham WT Telemedicine and remote
management of patients with heart failure [Review] Lancet2011378731ndash9
6 Inglis SC Clark RA McAlister FA et al Structured telephonesupport or telemonitoring programmes for patients with chronic heartfailure Cochrane Database Syst Rev 2010(8)CD007228
7 Pandor A Thokala P Gomersall T et al Home telemonitoring orstructured telephone support programmes after recent discharge inpatients with heart failure systematic review and economicevaluation Health Technol Assess 201317
8 Pandor A Pandor A Gomersall T et al Remote monitoring afterrecent hospital discharge in patients with heart failure a systematicreview and network meta-analysis Heart Published Online First 16May 2013 doi101136heartjnl-2013-303811
9 National Clinical Guideline Centre Chronic heart failure themanagement of chronic heart failure in adults in primary andsecondary care London National Clinical Guideline Centre 2012
10 Solomon SD Dobson J Pocock S et al Influence of nonfatalhospitalization for heart failure on subsequent mortality in patientswith chronic heart failure Circulation 20071161482ndash7
11 Klersy C De SA Gabutti G et al Economic impact of remotepatient monitoring an integrated economic model derived from ameta-analysis of randomized controlled trials in heart failure Eur JHeart Failure 201113450ndash9
12 Dar O Riley J Chapman C et al A randomized trial of hometelemonitoring in a typical elderly heart failure population in NorthWest London results of the Home-HF study Eur J Heart Failure200911319ndash25
13 Capomolla S Pinna GD La Rovere MT et al Heart failure casedisease management program a pilot study of home telemonitoringversus usual care Eur Heart J 20046(Suppl F)F91ndash8
14 Calvert MJ Shankar A McManus RJ et al Evaluation of themanagement of heart failure in primary care Fam Pract200926145ndash53
15 Iqbal J Francis L Reid J et al Quality of life in patients with chronicheart failure and their carers a 3-year follow-up study assessinghospitalization and mortality Eur J Heart Failure 2010121002ndash8
16 Miller LC Cox KR Miller LC et al Case management for patientswith heart failure a quality improvement intervention J GerontolNurs 20053120ndash8
17 Yao G Freemantle N Flather M et al Long-term cost-effectivenessanalysis of nebivolol compared with standard care in elderly patientswith heart failure an individual patient-based simulation modelPharmacoeconomics 200826879ndash89
18 Cleland JG Louis AA Rigby AS et al Noninvasive hometelemonitoring for patients with heart failure at high risk of recurrentadmission and death The Trans-European Network-Home-CareManagments System (TEN-HMS) study J Am Coll Cardiol2005451654ndash64
19 PSSRU Unit costs of health and social care 2011 201120 Boyne J Vrijhoef HJ Nieman FH et al Telemonitoring in patients
with heart failure results from a multicenter randomized controlledtrial (the tehaf study) J Am Coll Cardiol 201157(14 Suppl 1)E389
21 Department of Health NHS reference costs 2007ndash08 2009 LondonUK 2009
22 Miller G Randolph S Forkner E et al Long-term cost-effectivenessof disease management in systolic heart failure Med Deci Making200929325ndash33
8 Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
23 Galbreath AD Krasuski RA Smith B et al Long-term healthcareand cost outcome of disease management in a large randomizedcommunity-based population with heart failure Circulation20041103518ndash26
24 Henderson C Knapp M Fernandez J-L et al Cost effectiveness oftelehealth for patients with long term conditions (Whole SystemsDemonstrator telehealth questionnaire study) nested economicevaluation in a pragmatic cluster randomised controlled trialBMJ 2013346f1035
25 NHS information centre National Heart Failure Audit 2010 httpwww npc nhs ukrapidreviewp=2479 2010 httpwwwnpcnhsukrapidreviewp=2479
26 Cleland JG McDonagh T Rigby AS et al The national heart failureaudit for England and Wales 2008ndash2009 Heart 201197876ndash86
27 HES Online Hospital Episode Statistics 2008ndash2009 2012 httpwwwhesonlinenhsuk
28 3millionlives Improving your access to telehealth and telecare 12 AD http3millionlivescouk
29 A concordat between the Department of Health and the telehealthand telecare industry 12 AD http3millionlivescoukwp-contentuploads201203Concordat-FINALpdf
30 100000 people with long-term conditions to benefit from technologyin 2013 12 AD http3millionlivescoukwp-contentuploads20121114-November-2012-press-releasepdf
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 9
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from

analysis that is the results are robust to the variations inthe disutility of hospitalisationsScenario analysis using a 12-month treatment duration
produced similar results as in the 6-month treatmentduration scenarios TM for 12 months was also cost-effective when compared with TM for 6 months with anICER of pound14 066QALY However treating 2timesN patientsusing TM for 6 months was cost-effective with it beingdominant against a combination of treating N patientsusing TM for 12 months with the rest of the N patientsunder usual care
DISCUSSIONThe results of the base case cost-effectiveness analysessuggest that TM is expected to be the most cost-effectivestrategy at a threshold of pound20 000QALY However thereis uncertainty involved in suggesting that TM is the mostprobable cost-effective strategy and in particular thereis greater uncertainty when data from the Home-HFstudy12 is included than when it is excluded For
decision-makers the key question is whether the usualcare arm in their local setting is similar to the usual carearm in the Home-HF study12 If so then the resultsincluding the Home-HF study12 might be consideredmore relevant and if not the results excluding theHome-HF study12 might be considered more relevantThe scenario analysis performed (using higher usualcare costs lower TM costs higher TM costs and higherSTS costs) did not substantially change the conclusionsTM was estimated to be the most cost-effective strategyin all these scenarios Furthermore TM for 12 monthswas also cost-effective when compared with TM for6 months which suggests that it is cost-effective to keepthe patients on TM beyond 6 months In situations witha limited number of TM devices assuming a homoge-neous patient group it is cost-effective to treat allpatients using TM for 6 months than using TM for12 months on half the patients with the other half of thepatients under usual careThere have been two cost-effectiveness analyses studies
of RM in HF but neither considered the different RM
Figure 1 Cost effectiveness
acceptability curve for base case
economic analysis using
effectiveness data including the
Home-HF study12
Figure 2 Cost effectiveness
acceptability curve for economic
analysis using effectiveness data
excluding the Home-HF study12
6 Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
approaches separately11 22 The analysis reported byMiller et al22 was based on a single trial of STS23
whereas Klersy et al11 included data from a meta-analysisof a wide range of RM studies Miller et al22 estimatedthat STS compared with usual care had an ICER around$43 650QALY this study did not include a PSA butunivariate sensitivity analyses (ICER varying from$28 691 to $129 738 per QALY) was performed Klersyet al11 focused mainly on the effectiveness rather thanthe costs and used a time horizon of 1 year A budgetimpact analysis was presented and the differentdiagnosis-related group (DRG) reimbursement tariffgroups as a proxy for hospitalisation costs were consid-ered with cost savings per patient ranging betweeneuro3068 and euro99294 However other costs such as RMcosts and outpatient visit costs were not considered Theauthors performed scenario analyses using differentDRG costs as part of the budget analysis to address theuncertainty in the hospitalisation costs but neitherdeterministic sensitivity analysis nor PSA was performedThe Whole systems demonstrator (WSD) pro-
gramme24 a randomised controlled trial of telehealththat included over 6000 patients analysed costs and out-comes for 965 patients monitored for 12 months 534receiving telehealth and 431 receiving usual careCost-effectiveness analysis estimated the ICER atpound92 000QALY when telehealth was added to usual carefor people with chronic conditions (diabetes HF andchronic obstructive pulmonary disease (COPD))However this trial-based evaluation (with a time horizonof 1 year) potentially underestimates the health benefitsas it does not include the long-term QALYs gained fromthe reduction in mortality Furthermore the WSD ana-lysis included all patients with chronic conditions (dia-betes HF and COPD) whereas the population underconsideration in our analysis included patients who hadbeen recently discharged with HF The cost-effectivenessresults for HF patients are not yet publicly available in apeer-reviewed journal and thus it is difficult to comparethe results of the current analysis with the results of theWSD analysisThe analysis reported in this paper also has some lim-
itations that need to be taken into account Any model-ling process involves simplifications and assumptionsthat may not accurately reflect clinical practice Owingto the lack of detail provided in research studiesincluded in the NMA concerning the components ofRM packages and usual care (eg communication proto-cols routine staff visits and resources used) scenariosfor different RM classifications were developed and theircosts were estimated using bottom-up costing methodsAlthough the users can decide which of these analyses ismost representative of their setting uncertainties stillremain about the assumptions made in the estimation ofthese costs However it should be noted that themonthly costs estimated were similar to those reportedin the WSD Implementation costs (such as set-up costsstaff training costs service reconfiguration costs costs
for dual running of usual care and RM services) werenot included in the model but are often a considerationfor the health organisationsRM interventions included in the NMA were heteroge-
neous in terms of monitored parameters and selectioncriteria for HF this was the case even within specifictypes of RM (STS HH STS HM and TM) and isreflected in the uncertainty of the effectiveness para-meters A limitation of the analyses is that the effective-ness parameters remained the same for the differentcost scenarios whereas in reality there might be somecorrelation between the costs and effectiveness of differ-ent RM strategies Also it was assumed that the effective-ness and costs of the interventions are constant overtime irrespective of the duration of deploymentFurthermore as the analysis is not severity specific itassumes that the interventions are equally effective indifferent severity groups within the population underconsideration (ie patients who are recently dischargedwith HF) Repeat interventions after repeat hospitaladmissions for heart failure are not modelled and themortality risk is not reset for patients who are readmit-ted as this would need detailed evidence on baselinerisks and effectiveness in different patient groups As thisdetailed evidence is not available the cohort model usesevidence about the overall average of the patients to esti-mate the cost-effectivenessSome of the assumptions above may not hold true in
reality and therefore further research is needed to addressthese issues Given the complex nature of RM interven-tions new research should seek to examine the lsquoactiveingredientsrsquo of RM and identify patient subgroups that canbenefit most from the intervention as well as patients inwhom these interventions are unlikely to be effective Inaddition usual care ought to be more robustly deter-mined reflecting best practice as defined in the currentguidelines although this is not commonly the caseFurthermore to aid robust cost-effectiveness estimationsthe costs associated with usual care and RM interventionsneed to be reported in detail (including the costs of HFtreatment pathways) and QoL needs to be reported withobservations at specific time points in order to estimatethe difference in the utility of the patients between theRM and usual care groups Future studies should providegreater detail on reconfiguration and set-up costs and linkmore clearly with the financial impact (eg cost variationwith scale and over time) on provider organisations Wideradaptation of RM in the NHS can be facilitated by provid-ing financial impact data (eg set-up costs quarterly costsof service costs of reconfiguration) along with the long-term cost-effectiveness informationThe results of the current analysis have important
implications for the healthcare systems facing risingdemand from emergency admissions HF is a leadingcause of hospitalisation in the UK with 58 164 admis-sions recorded for HF (as first diagnoses) between April2009 and March 2010 in England and Wales25 The costof inpatient bed days for HF alone has been estimated at
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 7
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
pound563 million26 with around 90 of HF admissions toemergency departments27 lasting a median of 9 days25
The evidence shows that use of RM could substantiallyreduce HF admissions with an associated reduction inpressure on acute beds and consequent cost savingsFurthermore the use of TM might allow the potentialtransfer from emergency admission to elective admis-sion that is scheduling admissions of patients directly(not via AampE) to either a ward or to a day unit for off-loading leading to major resource savings with lesspatient disutilityIndeed the Department of Health (DH) recognised
this potential and launched an initiative lsquo3 MillionLivesrdquo (3ML) to help at least three million peoplewith long-term conditions andor social care tobenefit from the use of telehealth and telecare ser-vices28 A concordat has been entered into by the DHand the telehealth and telecare industry to worktogether to accelerate the use of TM29 Thus far sevenpathfinder sites have agreed contracts with the indus-try to ensure that 100 000 people benefit from thetechnology in 201330 Implemented effectively as partof a whole system redesign of care TM may alleviatethe pressure on long-term NHS costs and improvepeoplersquos quality of life through better self-care in thehome setting
Author affiliations1ScHARR University of Sheffield Sheffield UK2Department of Cardiology Barnet and Chase Farm Hospitals NHS TrustEnfield UK3South Yorkshire Cardiothoracic Centre Sheffield Teaching Hospitals NHSFoundation Trust Sheffield UK4Department of Cardiology Castle Hill Hospital Hull York Medical SchoolUniversity of Hull Hull UK5National Heart amp Lung Institute Imperial College London (Royal BromptonHospital) London UK
Acknowledgements The authors would like to thank Mr Tim Ellis ResearchFellow University of Sheffield Professor Mark Hawley Professor of HealthServices Research University of Sheffield Hazel Marsh Research NurseBarnsley Hospital NHS Foundation Trust and Dr Rachel OrsquoHara Lecturer inPublic Health University of Sheffield for providing clinical and TM expertiseThey would also like to thank Dr Lizzie Coates for peer reviewing the draftpaper
Contributors PT developed the decision analytical model undertook theanalysis and drafted the paper HB assisted in parameter searches modeldevelopment and analysis AB provided expert modelling advice AP wasresponsible for conception and design he undertook the systematic reviewalong with TG and provided data for the meta-analysis JWS and JW providedthe meta-analysis results and statistical input AB AAM JC and MRCprovided expert clinical input RW developed and undertook the literaturesearches All authors commented on the draftfinal paper
Funding The project was funded by the National Institute for Health Research(NIHR) Health Technology Assessment (HTA) Programme (number 0910701) and sponsored by the University of Sheffield The study funders had norole in study design in the collection analysis and interpretation of data inthe writing of the report and in the decision to submit the paper forpublication The researchers were independent of the study funders
Competing interests MRCrsquos salary is supported by the NIHR BiomedicalResearch Unit at the Royal Brompton Hospital
Provenance and peer review Not commissioned externally peer reviewed
Data sharing statement No additional data are available
Open Access This is an Open Access article distributed in accordance withthe Creative Commons Attribution Non Commercial (CC BY-NC 30) licensewhich permits others to distribute remix adapt build upon this work non-commercially and license their derivative works on different terms providedthe original work is properly cited and the use is non-commercial See httpcreativecommonsorglicensesby-nc30
REFERENCES1 Riley JP Cowie MR Telemonitoring in heart failure Heart
2009951964ndash82 Hasan A Paul V Telemonitoring in chronic heart failure Eur Heart J
2011321457ndash643 National Heart Failure Audit April 2010 to March 2011 2012 http
yhhiec org ukwp-contentuploads20111011070604_Tele_Moni_Workbk pdf httpwwwuclacuknicorauditsheartfailureadditionalfilespdfsannualreportsannual11pdf (accessed Mar2012)
4 McKelvie RS Heart failure Clin Evid 2011201102045 Anker SD Koehler F Abraham WT Telemedicine and remote
management of patients with heart failure [Review] Lancet2011378731ndash9
6 Inglis SC Clark RA McAlister FA et al Structured telephonesupport or telemonitoring programmes for patients with chronic heartfailure Cochrane Database Syst Rev 2010(8)CD007228
7 Pandor A Thokala P Gomersall T et al Home telemonitoring orstructured telephone support programmes after recent discharge inpatients with heart failure systematic review and economicevaluation Health Technol Assess 201317
8 Pandor A Pandor A Gomersall T et al Remote monitoring afterrecent hospital discharge in patients with heart failure a systematicreview and network meta-analysis Heart Published Online First 16May 2013 doi101136heartjnl-2013-303811
9 National Clinical Guideline Centre Chronic heart failure themanagement of chronic heart failure in adults in primary andsecondary care London National Clinical Guideline Centre 2012
10 Solomon SD Dobson J Pocock S et al Influence of nonfatalhospitalization for heart failure on subsequent mortality in patientswith chronic heart failure Circulation 20071161482ndash7
11 Klersy C De SA Gabutti G et al Economic impact of remotepatient monitoring an integrated economic model derived from ameta-analysis of randomized controlled trials in heart failure Eur JHeart Failure 201113450ndash9
12 Dar O Riley J Chapman C et al A randomized trial of hometelemonitoring in a typical elderly heart failure population in NorthWest London results of the Home-HF study Eur J Heart Failure200911319ndash25
13 Capomolla S Pinna GD La Rovere MT et al Heart failure casedisease management program a pilot study of home telemonitoringversus usual care Eur Heart J 20046(Suppl F)F91ndash8
14 Calvert MJ Shankar A McManus RJ et al Evaluation of themanagement of heart failure in primary care Fam Pract200926145ndash53
15 Iqbal J Francis L Reid J et al Quality of life in patients with chronicheart failure and their carers a 3-year follow-up study assessinghospitalization and mortality Eur J Heart Failure 2010121002ndash8
16 Miller LC Cox KR Miller LC et al Case management for patientswith heart failure a quality improvement intervention J GerontolNurs 20053120ndash8
17 Yao G Freemantle N Flather M et al Long-term cost-effectivenessanalysis of nebivolol compared with standard care in elderly patientswith heart failure an individual patient-based simulation modelPharmacoeconomics 200826879ndash89
18 Cleland JG Louis AA Rigby AS et al Noninvasive hometelemonitoring for patients with heart failure at high risk of recurrentadmission and death The Trans-European Network-Home-CareManagments System (TEN-HMS) study J Am Coll Cardiol2005451654ndash64
19 PSSRU Unit costs of health and social care 2011 201120 Boyne J Vrijhoef HJ Nieman FH et al Telemonitoring in patients
with heart failure results from a multicenter randomized controlledtrial (the tehaf study) J Am Coll Cardiol 201157(14 Suppl 1)E389
21 Department of Health NHS reference costs 2007ndash08 2009 LondonUK 2009
22 Miller G Randolph S Forkner E et al Long-term cost-effectivenessof disease management in systolic heart failure Med Deci Making200929325ndash33
8 Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
23 Galbreath AD Krasuski RA Smith B et al Long-term healthcareand cost outcome of disease management in a large randomizedcommunity-based population with heart failure Circulation20041103518ndash26
24 Henderson C Knapp M Fernandez J-L et al Cost effectiveness oftelehealth for patients with long term conditions (Whole SystemsDemonstrator telehealth questionnaire study) nested economicevaluation in a pragmatic cluster randomised controlled trialBMJ 2013346f1035
25 NHS information centre National Heart Failure Audit 2010 httpwww npc nhs ukrapidreviewp=2479 2010 httpwwwnpcnhsukrapidreviewp=2479
26 Cleland JG McDonagh T Rigby AS et al The national heart failureaudit for England and Wales 2008ndash2009 Heart 201197876ndash86
27 HES Online Hospital Episode Statistics 2008ndash2009 2012 httpwwwhesonlinenhsuk
28 3millionlives Improving your access to telehealth and telecare 12 AD http3millionlivescouk
29 A concordat between the Department of Health and the telehealthand telecare industry 12 AD http3millionlivescoukwp-contentuploads201203Concordat-FINALpdf
30 100000 people with long-term conditions to benefit from technologyin 2013 12 AD http3millionlivescoukwp-contentuploads20121114-November-2012-press-releasepdf
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 9
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from

approaches separately11 22 The analysis reported byMiller et al22 was based on a single trial of STS23
whereas Klersy et al11 included data from a meta-analysisof a wide range of RM studies Miller et al22 estimatedthat STS compared with usual care had an ICER around$43 650QALY this study did not include a PSA butunivariate sensitivity analyses (ICER varying from$28 691 to $129 738 per QALY) was performed Klersyet al11 focused mainly on the effectiveness rather thanthe costs and used a time horizon of 1 year A budgetimpact analysis was presented and the differentdiagnosis-related group (DRG) reimbursement tariffgroups as a proxy for hospitalisation costs were consid-ered with cost savings per patient ranging betweeneuro3068 and euro99294 However other costs such as RMcosts and outpatient visit costs were not considered Theauthors performed scenario analyses using differentDRG costs as part of the budget analysis to address theuncertainty in the hospitalisation costs but neitherdeterministic sensitivity analysis nor PSA was performedThe Whole systems demonstrator (WSD) pro-
gramme24 a randomised controlled trial of telehealththat included over 6000 patients analysed costs and out-comes for 965 patients monitored for 12 months 534receiving telehealth and 431 receiving usual careCost-effectiveness analysis estimated the ICER atpound92 000QALY when telehealth was added to usual carefor people with chronic conditions (diabetes HF andchronic obstructive pulmonary disease (COPD))However this trial-based evaluation (with a time horizonof 1 year) potentially underestimates the health benefitsas it does not include the long-term QALYs gained fromthe reduction in mortality Furthermore the WSD ana-lysis included all patients with chronic conditions (dia-betes HF and COPD) whereas the population underconsideration in our analysis included patients who hadbeen recently discharged with HF The cost-effectivenessresults for HF patients are not yet publicly available in apeer-reviewed journal and thus it is difficult to comparethe results of the current analysis with the results of theWSD analysisThe analysis reported in this paper also has some lim-
itations that need to be taken into account Any model-ling process involves simplifications and assumptionsthat may not accurately reflect clinical practice Owingto the lack of detail provided in research studiesincluded in the NMA concerning the components ofRM packages and usual care (eg communication proto-cols routine staff visits and resources used) scenariosfor different RM classifications were developed and theircosts were estimated using bottom-up costing methodsAlthough the users can decide which of these analyses ismost representative of their setting uncertainties stillremain about the assumptions made in the estimation ofthese costs However it should be noted that themonthly costs estimated were similar to those reportedin the WSD Implementation costs (such as set-up costsstaff training costs service reconfiguration costs costs
for dual running of usual care and RM services) werenot included in the model but are often a considerationfor the health organisationsRM interventions included in the NMA were heteroge-
neous in terms of monitored parameters and selectioncriteria for HF this was the case even within specifictypes of RM (STS HH STS HM and TM) and isreflected in the uncertainty of the effectiveness para-meters A limitation of the analyses is that the effective-ness parameters remained the same for the differentcost scenarios whereas in reality there might be somecorrelation between the costs and effectiveness of differ-ent RM strategies Also it was assumed that the effective-ness and costs of the interventions are constant overtime irrespective of the duration of deploymentFurthermore as the analysis is not severity specific itassumes that the interventions are equally effective indifferent severity groups within the population underconsideration (ie patients who are recently dischargedwith HF) Repeat interventions after repeat hospitaladmissions for heart failure are not modelled and themortality risk is not reset for patients who are readmit-ted as this would need detailed evidence on baselinerisks and effectiveness in different patient groups As thisdetailed evidence is not available the cohort model usesevidence about the overall average of the patients to esti-mate the cost-effectivenessSome of the assumptions above may not hold true in
reality and therefore further research is needed to addressthese issues Given the complex nature of RM interven-tions new research should seek to examine the lsquoactiveingredientsrsquo of RM and identify patient subgroups that canbenefit most from the intervention as well as patients inwhom these interventions are unlikely to be effective Inaddition usual care ought to be more robustly deter-mined reflecting best practice as defined in the currentguidelines although this is not commonly the caseFurthermore to aid robust cost-effectiveness estimationsthe costs associated with usual care and RM interventionsneed to be reported in detail (including the costs of HFtreatment pathways) and QoL needs to be reported withobservations at specific time points in order to estimatethe difference in the utility of the patients between theRM and usual care groups Future studies should providegreater detail on reconfiguration and set-up costs and linkmore clearly with the financial impact (eg cost variationwith scale and over time) on provider organisations Wideradaptation of RM in the NHS can be facilitated by provid-ing financial impact data (eg set-up costs quarterly costsof service costs of reconfiguration) along with the long-term cost-effectiveness informationThe results of the current analysis have important
implications for the healthcare systems facing risingdemand from emergency admissions HF is a leadingcause of hospitalisation in the UK with 58 164 admis-sions recorded for HF (as first diagnoses) between April2009 and March 2010 in England and Wales25 The costof inpatient bed days for HF alone has been estimated at
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 7
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
pound563 million26 with around 90 of HF admissions toemergency departments27 lasting a median of 9 days25
The evidence shows that use of RM could substantiallyreduce HF admissions with an associated reduction inpressure on acute beds and consequent cost savingsFurthermore the use of TM might allow the potentialtransfer from emergency admission to elective admis-sion that is scheduling admissions of patients directly(not via AampE) to either a ward or to a day unit for off-loading leading to major resource savings with lesspatient disutilityIndeed the Department of Health (DH) recognised
this potential and launched an initiative lsquo3 MillionLivesrdquo (3ML) to help at least three million peoplewith long-term conditions andor social care tobenefit from the use of telehealth and telecare ser-vices28 A concordat has been entered into by the DHand the telehealth and telecare industry to worktogether to accelerate the use of TM29 Thus far sevenpathfinder sites have agreed contracts with the indus-try to ensure that 100 000 people benefit from thetechnology in 201330 Implemented effectively as partof a whole system redesign of care TM may alleviatethe pressure on long-term NHS costs and improvepeoplersquos quality of life through better self-care in thehome setting
Author affiliations1ScHARR University of Sheffield Sheffield UK2Department of Cardiology Barnet and Chase Farm Hospitals NHS TrustEnfield UK3South Yorkshire Cardiothoracic Centre Sheffield Teaching Hospitals NHSFoundation Trust Sheffield UK4Department of Cardiology Castle Hill Hospital Hull York Medical SchoolUniversity of Hull Hull UK5National Heart amp Lung Institute Imperial College London (Royal BromptonHospital) London UK
Acknowledgements The authors would like to thank Mr Tim Ellis ResearchFellow University of Sheffield Professor Mark Hawley Professor of HealthServices Research University of Sheffield Hazel Marsh Research NurseBarnsley Hospital NHS Foundation Trust and Dr Rachel OrsquoHara Lecturer inPublic Health University of Sheffield for providing clinical and TM expertiseThey would also like to thank Dr Lizzie Coates for peer reviewing the draftpaper
Contributors PT developed the decision analytical model undertook theanalysis and drafted the paper HB assisted in parameter searches modeldevelopment and analysis AB provided expert modelling advice AP wasresponsible for conception and design he undertook the systematic reviewalong with TG and provided data for the meta-analysis JWS and JW providedthe meta-analysis results and statistical input AB AAM JC and MRCprovided expert clinical input RW developed and undertook the literaturesearches All authors commented on the draftfinal paper
Funding The project was funded by the National Institute for Health Research(NIHR) Health Technology Assessment (HTA) Programme (number 0910701) and sponsored by the University of Sheffield The study funders had norole in study design in the collection analysis and interpretation of data inthe writing of the report and in the decision to submit the paper forpublication The researchers were independent of the study funders
Competing interests MRCrsquos salary is supported by the NIHR BiomedicalResearch Unit at the Royal Brompton Hospital
Provenance and peer review Not commissioned externally peer reviewed
Data sharing statement No additional data are available
Open Access This is an Open Access article distributed in accordance withthe Creative Commons Attribution Non Commercial (CC BY-NC 30) licensewhich permits others to distribute remix adapt build upon this work non-commercially and license their derivative works on different terms providedthe original work is properly cited and the use is non-commercial See httpcreativecommonsorglicensesby-nc30
REFERENCES1 Riley JP Cowie MR Telemonitoring in heart failure Heart
2009951964ndash82 Hasan A Paul V Telemonitoring in chronic heart failure Eur Heart J
2011321457ndash643 National Heart Failure Audit April 2010 to March 2011 2012 http
yhhiec org ukwp-contentuploads20111011070604_Tele_Moni_Workbk pdf httpwwwuclacuknicorauditsheartfailureadditionalfilespdfsannualreportsannual11pdf (accessed Mar2012)
4 McKelvie RS Heart failure Clin Evid 2011201102045 Anker SD Koehler F Abraham WT Telemedicine and remote
management of patients with heart failure [Review] Lancet2011378731ndash9
6 Inglis SC Clark RA McAlister FA et al Structured telephonesupport or telemonitoring programmes for patients with chronic heartfailure Cochrane Database Syst Rev 2010(8)CD007228
7 Pandor A Thokala P Gomersall T et al Home telemonitoring orstructured telephone support programmes after recent discharge inpatients with heart failure systematic review and economicevaluation Health Technol Assess 201317
8 Pandor A Pandor A Gomersall T et al Remote monitoring afterrecent hospital discharge in patients with heart failure a systematicreview and network meta-analysis Heart Published Online First 16May 2013 doi101136heartjnl-2013-303811
9 National Clinical Guideline Centre Chronic heart failure themanagement of chronic heart failure in adults in primary andsecondary care London National Clinical Guideline Centre 2012
10 Solomon SD Dobson J Pocock S et al Influence of nonfatalhospitalization for heart failure on subsequent mortality in patientswith chronic heart failure Circulation 20071161482ndash7
11 Klersy C De SA Gabutti G et al Economic impact of remotepatient monitoring an integrated economic model derived from ameta-analysis of randomized controlled trials in heart failure Eur JHeart Failure 201113450ndash9
12 Dar O Riley J Chapman C et al A randomized trial of hometelemonitoring in a typical elderly heart failure population in NorthWest London results of the Home-HF study Eur J Heart Failure200911319ndash25
13 Capomolla S Pinna GD La Rovere MT et al Heart failure casedisease management program a pilot study of home telemonitoringversus usual care Eur Heart J 20046(Suppl F)F91ndash8
14 Calvert MJ Shankar A McManus RJ et al Evaluation of themanagement of heart failure in primary care Fam Pract200926145ndash53
15 Iqbal J Francis L Reid J et al Quality of life in patients with chronicheart failure and their carers a 3-year follow-up study assessinghospitalization and mortality Eur J Heart Failure 2010121002ndash8
16 Miller LC Cox KR Miller LC et al Case management for patientswith heart failure a quality improvement intervention J GerontolNurs 20053120ndash8
17 Yao G Freemantle N Flather M et al Long-term cost-effectivenessanalysis of nebivolol compared with standard care in elderly patientswith heart failure an individual patient-based simulation modelPharmacoeconomics 200826879ndash89
18 Cleland JG Louis AA Rigby AS et al Noninvasive hometelemonitoring for patients with heart failure at high risk of recurrentadmission and death The Trans-European Network-Home-CareManagments System (TEN-HMS) study J Am Coll Cardiol2005451654ndash64
19 PSSRU Unit costs of health and social care 2011 201120 Boyne J Vrijhoef HJ Nieman FH et al Telemonitoring in patients
with heart failure results from a multicenter randomized controlledtrial (the tehaf study) J Am Coll Cardiol 201157(14 Suppl 1)E389
21 Department of Health NHS reference costs 2007ndash08 2009 LondonUK 2009
22 Miller G Randolph S Forkner E et al Long-term cost-effectivenessof disease management in systolic heart failure Med Deci Making200929325ndash33
8 Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
23 Galbreath AD Krasuski RA Smith B et al Long-term healthcareand cost outcome of disease management in a large randomizedcommunity-based population with heart failure Circulation20041103518ndash26
24 Henderson C Knapp M Fernandez J-L et al Cost effectiveness oftelehealth for patients with long term conditions (Whole SystemsDemonstrator telehealth questionnaire study) nested economicevaluation in a pragmatic cluster randomised controlled trialBMJ 2013346f1035
25 NHS information centre National Heart Failure Audit 2010 httpwww npc nhs ukrapidreviewp=2479 2010 httpwwwnpcnhsukrapidreviewp=2479
26 Cleland JG McDonagh T Rigby AS et al The national heart failureaudit for England and Wales 2008ndash2009 Heart 201197876ndash86
27 HES Online Hospital Episode Statistics 2008ndash2009 2012 httpwwwhesonlinenhsuk
28 3millionlives Improving your access to telehealth and telecare 12 AD http3millionlivescouk
29 A concordat between the Department of Health and the telehealthand telecare industry 12 AD http3millionlivescoukwp-contentuploads201203Concordat-FINALpdf
30 100000 people with long-term conditions to benefit from technologyin 2013 12 AD http3millionlivescoukwp-contentuploads20121114-November-2012-press-releasepdf
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 9
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from

pound563 million26 with around 90 of HF admissions toemergency departments27 lasting a median of 9 days25
The evidence shows that use of RM could substantiallyreduce HF admissions with an associated reduction inpressure on acute beds and consequent cost savingsFurthermore the use of TM might allow the potentialtransfer from emergency admission to elective admis-sion that is scheduling admissions of patients directly(not via AampE) to either a ward or to a day unit for off-loading leading to major resource savings with lesspatient disutilityIndeed the Department of Health (DH) recognised
this potential and launched an initiative lsquo3 MillionLivesrdquo (3ML) to help at least three million peoplewith long-term conditions andor social care tobenefit from the use of telehealth and telecare ser-vices28 A concordat has been entered into by the DHand the telehealth and telecare industry to worktogether to accelerate the use of TM29 Thus far sevenpathfinder sites have agreed contracts with the indus-try to ensure that 100 000 people benefit from thetechnology in 201330 Implemented effectively as partof a whole system redesign of care TM may alleviatethe pressure on long-term NHS costs and improvepeoplersquos quality of life through better self-care in thehome setting
Author affiliations1ScHARR University of Sheffield Sheffield UK2Department of Cardiology Barnet and Chase Farm Hospitals NHS TrustEnfield UK3South Yorkshire Cardiothoracic Centre Sheffield Teaching Hospitals NHSFoundation Trust Sheffield UK4Department of Cardiology Castle Hill Hospital Hull York Medical SchoolUniversity of Hull Hull UK5National Heart amp Lung Institute Imperial College London (Royal BromptonHospital) London UK
Acknowledgements The authors would like to thank Mr Tim Ellis ResearchFellow University of Sheffield Professor Mark Hawley Professor of HealthServices Research University of Sheffield Hazel Marsh Research NurseBarnsley Hospital NHS Foundation Trust and Dr Rachel OrsquoHara Lecturer inPublic Health University of Sheffield for providing clinical and TM expertiseThey would also like to thank Dr Lizzie Coates for peer reviewing the draftpaper
Contributors PT developed the decision analytical model undertook theanalysis and drafted the paper HB assisted in parameter searches modeldevelopment and analysis AB provided expert modelling advice AP wasresponsible for conception and design he undertook the systematic reviewalong with TG and provided data for the meta-analysis JWS and JW providedthe meta-analysis results and statistical input AB AAM JC and MRCprovided expert clinical input RW developed and undertook the literaturesearches All authors commented on the draftfinal paper
Funding The project was funded by the National Institute for Health Research(NIHR) Health Technology Assessment (HTA) Programme (number 0910701) and sponsored by the University of Sheffield The study funders had norole in study design in the collection analysis and interpretation of data inthe writing of the report and in the decision to submit the paper forpublication The researchers were independent of the study funders
Competing interests MRCrsquos salary is supported by the NIHR BiomedicalResearch Unit at the Royal Brompton Hospital
Provenance and peer review Not commissioned externally peer reviewed
Data sharing statement No additional data are available
Open Access This is an Open Access article distributed in accordance withthe Creative Commons Attribution Non Commercial (CC BY-NC 30) licensewhich permits others to distribute remix adapt build upon this work non-commercially and license their derivative works on different terms providedthe original work is properly cited and the use is non-commercial See httpcreativecommonsorglicensesby-nc30
REFERENCES1 Riley JP Cowie MR Telemonitoring in heart failure Heart
2009951964ndash82 Hasan A Paul V Telemonitoring in chronic heart failure Eur Heart J
2011321457ndash643 National Heart Failure Audit April 2010 to March 2011 2012 http
yhhiec org ukwp-contentuploads20111011070604_Tele_Moni_Workbk pdf httpwwwuclacuknicorauditsheartfailureadditionalfilespdfsannualreportsannual11pdf (accessed Mar2012)
4 McKelvie RS Heart failure Clin Evid 2011201102045 Anker SD Koehler F Abraham WT Telemedicine and remote
management of patients with heart failure [Review] Lancet2011378731ndash9
6 Inglis SC Clark RA McAlister FA et al Structured telephonesupport or telemonitoring programmes for patients with chronic heartfailure Cochrane Database Syst Rev 2010(8)CD007228
7 Pandor A Thokala P Gomersall T et al Home telemonitoring orstructured telephone support programmes after recent discharge inpatients with heart failure systematic review and economicevaluation Health Technol Assess 201317
8 Pandor A Pandor A Gomersall T et al Remote monitoring afterrecent hospital discharge in patients with heart failure a systematicreview and network meta-analysis Heart Published Online First 16May 2013 doi101136heartjnl-2013-303811
9 National Clinical Guideline Centre Chronic heart failure themanagement of chronic heart failure in adults in primary andsecondary care London National Clinical Guideline Centre 2012
10 Solomon SD Dobson J Pocock S et al Influence of nonfatalhospitalization for heart failure on subsequent mortality in patientswith chronic heart failure Circulation 20071161482ndash7
11 Klersy C De SA Gabutti G et al Economic impact of remotepatient monitoring an integrated economic model derived from ameta-analysis of randomized controlled trials in heart failure Eur JHeart Failure 201113450ndash9
12 Dar O Riley J Chapman C et al A randomized trial of hometelemonitoring in a typical elderly heart failure population in NorthWest London results of the Home-HF study Eur J Heart Failure200911319ndash25
13 Capomolla S Pinna GD La Rovere MT et al Heart failure casedisease management program a pilot study of home telemonitoringversus usual care Eur Heart J 20046(Suppl F)F91ndash8
14 Calvert MJ Shankar A McManus RJ et al Evaluation of themanagement of heart failure in primary care Fam Pract200926145ndash53
15 Iqbal J Francis L Reid J et al Quality of life in patients with chronicheart failure and their carers a 3-year follow-up study assessinghospitalization and mortality Eur J Heart Failure 2010121002ndash8
16 Miller LC Cox KR Miller LC et al Case management for patientswith heart failure a quality improvement intervention J GerontolNurs 20053120ndash8
17 Yao G Freemantle N Flather M et al Long-term cost-effectivenessanalysis of nebivolol compared with standard care in elderly patientswith heart failure an individual patient-based simulation modelPharmacoeconomics 200826879ndash89
18 Cleland JG Louis AA Rigby AS et al Noninvasive hometelemonitoring for patients with heart failure at high risk of recurrentadmission and death The Trans-European Network-Home-CareManagments System (TEN-HMS) study J Am Coll Cardiol2005451654ndash64
19 PSSRU Unit costs of health and social care 2011 201120 Boyne J Vrijhoef HJ Nieman FH et al Telemonitoring in patients
with heart failure results from a multicenter randomized controlledtrial (the tehaf study) J Am Coll Cardiol 201157(14 Suppl 1)E389
21 Department of Health NHS reference costs 2007ndash08 2009 LondonUK 2009
22 Miller G Randolph S Forkner E et al Long-term cost-effectivenessof disease management in systolic heart failure Med Deci Making200929325ndash33
8 Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from
23 Galbreath AD Krasuski RA Smith B et al Long-term healthcareand cost outcome of disease management in a large randomizedcommunity-based population with heart failure Circulation20041103518ndash26
24 Henderson C Knapp M Fernandez J-L et al Cost effectiveness oftelehealth for patients with long term conditions (Whole SystemsDemonstrator telehealth questionnaire study) nested economicevaluation in a pragmatic cluster randomised controlled trialBMJ 2013346f1035
25 NHS information centre National Heart Failure Audit 2010 httpwww npc nhs ukrapidreviewp=2479 2010 httpwwwnpcnhsukrapidreviewp=2479
26 Cleland JG McDonagh T Rigby AS et al The national heart failureaudit for England and Wales 2008ndash2009 Heart 201197876ndash86
27 HES Online Hospital Episode Statistics 2008ndash2009 2012 httpwwwhesonlinenhsuk
28 3millionlives Improving your access to telehealth and telecare 12 AD http3millionlivescouk
29 A concordat between the Department of Health and the telehealthand telecare industry 12 AD http3millionlivescoukwp-contentuploads201203Concordat-FINALpdf
30 100000 people with long-term conditions to benefit from technologyin 2013 12 AD http3millionlivescoukwp-contentuploads20121114-November-2012-press-releasepdf
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 9
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from

23 Galbreath AD Krasuski RA Smith B et al Long-term healthcareand cost outcome of disease management in a large randomizedcommunity-based population with heart failure Circulation20041103518ndash26
24 Henderson C Knapp M Fernandez J-L et al Cost effectiveness oftelehealth for patients with long term conditions (Whole SystemsDemonstrator telehealth questionnaire study) nested economicevaluation in a pragmatic cluster randomised controlled trialBMJ 2013346f1035
25 NHS information centre National Heart Failure Audit 2010 httpwww npc nhs ukrapidreviewp=2479 2010 httpwwwnpcnhsukrapidreviewp=2479
26 Cleland JG McDonagh T Rigby AS et al The national heart failureaudit for England and Wales 2008ndash2009 Heart 201197876ndash86
27 HES Online Hospital Episode Statistics 2008ndash2009 2012 httpwwwhesonlinenhsuk
28 3millionlives Improving your access to telehealth and telecare 12 AD http3millionlivescouk
29 A concordat between the Department of Health and the telehealthand telecare industry 12 AD http3millionlivescoukwp-contentuploads201203Concordat-FINALpdf
30 100000 people with long-term conditions to benefit from technologyin 2013 12 AD http3millionlivescoukwp-contentuploads20121114-November-2012-press-releasepdf
Thokala P Baalbaki H Brennan A et al BMJ Open 20133e003250 doi101136bmjopen-2013-003250 9
Open Access
on Decem
ber 14 2020 by guest Protected by copyright
httpbmjopenbm
jcom
BM
J Open first published as 101136bm
jopen-2013-003250 on 18 Septem
ber 2013 Dow
nloaded from












![Telemonitoring of Wind Turbines[1]](https://img.dokumen.tips/doc/110x75/577d29731a28ab4e1ea6d22a/telemonitoring-of-wind-turbines1.jpg)





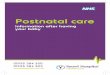


![More than Telemonitoring [JMIR2015]](https://img.dokumen.tips/doc/110x75/58ecd3931a28ab72278b4597/more-than-telemonitoring-jmir2015.jpg)







