Embed Size (px)
Citation preview

One-Stage Pharyngoesophageal and Oral Mucocutaneous
Reconstruction With Two Segments of
One Musculocutaneous Flap
Gordon Ft. Tobin, MD, Louisville, Kentucky
John S. Spratt, MD, Louisville, Kentucky
Kirby I. Bland, MD, Louisville, Kentucky
Leonard J. Weiner, MD, Louisville, Kentucky
This report describes a surgical technique that pro- vides both cover and lining in one stage to mucocu- taneous defects of the pharyngoesophageal mucosa neck skin or oral mucosa and facial skin using a single musculocutaneous flap split between anatomic seg- ments into two independent flaps. Each segmental branch of the muscle carries an island skin paddle. The skin paddle of one segment provides an epithe- lial lining surface, and the skin paddle of the other segment of the same flap provides overlying skin cover. This technique minimizes the number of flaps or lining grafts required for mucocutaneous defect reconstruction and eliminates staged surgical pro- cedures, thereby lessening both patient donor defects and hospitalization time.
Both latissimus dorsi and pectoralis major mus- culocutaneous flaps have become major instruments for reconstruction of head and neck defects. Both of these musculocutaneous units have the segmental morphology and neurovascular anatomy necessary for the applications described herein [I ,2].
Anatomic Studies
We have recently reported studies of both latissimus dorsi and pectoralis major anatomy based on dissection, specimen angiography, and arterial dye perfusion of 115 human latissimus dorsi and 95 human pectoralis major musculocutaneous units [I ,2]. In both musculocutaneous units, a segmental morphology and neurovascular anatomy were consistently found. Each segmental branch of either
From the Division of Plastic Surgery, Department of Surgery, University of Louisville, Louisville, Kentucky.
Requests for reprints should be addressed to Gordon R. Tobin, MD, Division of Plastic Surgery, Department of Surgery, University of Louisville, Louisville, Kentuckv 40292.
Presented at the 28th Annual Meeting of the Society of Head and Neck Surgeons, Marco Island, Florida, April 18-23. 1982.
flap has an independent neurovascular supply, carries island musculocutaneous paddles, and can be surgically separated from other segments by dissection along ana- tomic lines.
The latissimus dorsi musculocutaneous unit has two segmental subunits (medial and lateral) defined by the intramuscular courses of the two major branches of the thoracodorsal vessels (Figure 1). The thoracodorsal vessels bifurcate at the latissimus dorsi neurovascular hilum on the ventral muscle surface 8.7 f 1.4 cm (mean f standard deviation) distal to the thoracodorsal artery origin [I]. The medial vascular branch courses horizontally, parallel to the muscle’s scapular border and supplies that segment of muscle originating on the thoracic perispinal fascia. The lateral vascular branch courses parallel to the muscle’s axillary border and supplies the segment of muscle origi- nating at the lowest ribs, the iliac crest, and the lumbo- dorsal fascia. The two latissimus dorsi segments are sur- gically defined by dividing the muscle in the line of its fi- bers between the two neurovascular watersheds [3]. The arc of rotation of both segments covers the oral cavity and mid-face (Figure 2).
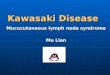
The pectoralis major musculocutaneous unit has three segmental subunits (clavicular, sternocostal, and external), which are defined by three independent neurovascular supplies [2] (Figure 3). The thoracoacromial vessels branch beneath the clavicular midpoint to supply the clavicular and sternocostal musculocutaneous segments. The superior branch of these vessels supplies the clavicular segment. The inferior (pectoral) branch supplies the sternocostal seg- ment. The external segment is supplied both by the lateral thoracic vessels and by the lateral branches of the thora- coacromial pectoral vessels. The lateral thoracic vessels also provide a direct cutaneous supply to the lower axillary skin that is adjacent to the external muscle segment Thus, large cutaneous paddles carried on these vessels have both musculocutaneous and direct cutaneous blood supplies [2]. The arc of rotation of the clavicular segment covers only the cervical region. The external and sternocostal segments
Volume 144. October 1992 489

Tobin et al
Figure 1. SegmentaNy split lattsslmus dorsl muscutocutarteous flarra Left. the seamental vascular anatomy. TD = thoracodorsal
A = lateral muscutocutaneous segment vascular supply. Right, deslgn of skln paddles for cover and llnlng flaps. S = medlal segment musculocutaneous flap; A = lateral segment musculo- cutaneous flap.
cover the oral cavity and the mid-face as well (Figure 4). Accordingly, we chose the external and sternocostal muscle segments to carry cover and lining skin paddles for recon- struction in the cases presented herein.
Animal Studies
Both the pectoralis and latissimus dorsi musculocuta- neous units of dogs have a segmental morphology analo- gous to that of man. Either canine musculocutaneous unit provides two segmental flaps that will each carry an island skin paddle. Accordingly, we used dogs experimentally to test the technique for mucocutaneous defect reconstruction in one stage.
We previously reported an experimental study of seg- mentally split latissimus dorsi musculocutaneous flaps in dogs [3]. This series included seven segmentally split lat- issimus dorsi musculocutaneous flaps that simultaneously provided two segmental cover and lining flaps for one-stage reconstruction of defects of the cervical esophagus and overlying neck skin, or defects of the oral floor and over- lying submental skin. We have also used segmentally split pectoralis musculocutaneous flaps to simultaneously provide two segmental cover and lining flaps for one-stage reconstruction of defects of the cervical esophagus and overlying neck skin (Tobin GR, unpublished data). In contrast with man, canine pectoralis flaps do not reach the oral cavity or face.
Figure 2. 7ne arc of rotatlon of split latlsslmus dorsl musculocu- taneous flaps covers the oral cavity and mid-face, as shown In thls cadaver. P = skln paddles; S = segmentally split muscle branches,
Clinical Applications
We have used this technique of segmentally splitting either latissimus dorsi or pectoralis major musculocutaneous flaps to provide cover and lining in one stage to patients with mucocutaneous defects of the oral cavity, oropharynx, hypopharynx, or cervical esophagus. In each case, island skin paddles were carried on two segments of one musculocuta- neous flap.
Segmental pectoralis major flaps were used for defects of the buccal mucosa and cheek skin, the oral floor and submental skin, and the hypopharynx- cervical esophagus and neck skin. Skin paddles that were carried on the sternocostal and external pec- toralis major muscle segments were passed over the clavicle to the mucocutaneous defects. Innervated pectoralis major clavicular segments were left in situ to preserve donor motor function [4].
Segmental latissimus dorsi flaps were used for
490 The American Journal ol Surgery
One-Stage Pharyngoesophageal and Oral Mucocutaneous Reconstruction
Figure 3. Segmentalty split pectoral/s major musculocutaneous flaps. Left, the segmental morphology and neurovascular suppty. TA = thoracoacromlal vessels; L T = lateral thoracic vessels; C = clavlcular muscul~utaneous segment; S = sternocostal musculocutaneous segment; E = external (abdominal) muscu- kxutaneous segment, Rtght, deslgn of skln paddles for cover and llntng flaps. S = stemocostal segment musculocutaneous flap; E = external segment musculocutaneous flap.
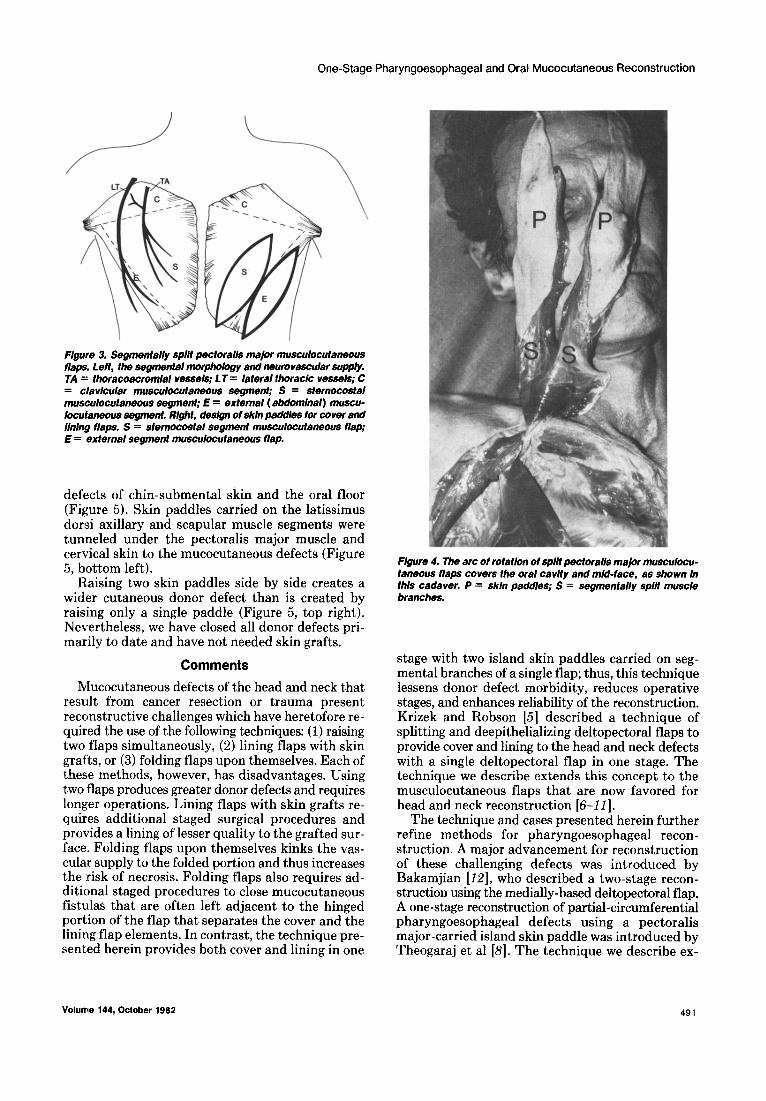
defects of chin-submental skin and the oral floor (Figure 5). Skin paddles carried on the latissimus dorsi axillary and scapular muscle segments were tunneled under the pectoralis major muscle and cervical skin to the mucocutaneous defects (Figure 5, bottom left).
Raising two skin paddles side by side creates a wider cutaneous donor defect than is created by raising only a single paddle (Figure 5, top right). Nevertheless, we have closed all donor defects pri- marily to date and have not needed skin grafts.
Comments
Mucocutaneous defects of the head and neck that result from cancer resection or trauma present reconstructive challenges which have heretofore re- quired the use of the following techniques: (1) raising two flaps simultaneously, (2) lining flaps with skin grafts, or (3) folding flaps upon themselves. Each of these methods, however, has disadvantages. Using two flaps produces greater donor defects and requires longer operations. Lining flaps with skin grafts re- quires additional staged surgical procedures and provides a lining of lesser quality to the grafted sur- face. Folding flaps upon themselves kinks the vas- cular supply to the folded portion and thus increases the risk of necrosis. Folding flaps also requires ad- ditional staged procedures to close mucocutaneous fistulas that are often left adjacent to the hinged portion of the flap that separates the cover and the lining flap elements. In contrast, the technique pre- sented herein provides both cover and lining in one
Figure 4. The arc of rotation of split pectoralis ma/or musculocu- taneous flaps covers the oral cavtty and mkt-face, as shown In this cadaver. P = skln paddles; S = segmentally split muscle branches.
stage with two island skin paddles carried on seg- mental branches of a single flap; thus, this technique lessens donor defect morbidity, reduces operative stages, and enhances reliability of the reconstruction. Krizek and Robson [5] described a technique of splitting and deepithelializing deltopectoral flaps to provide cover and lining to the head and neck defects with a single deltopectoral flap in one stage. The technique we describe extends this concept to the musculocutaneous flaps that are now favored for head and neck reconstruction [6--I 11.
The technique and cases presented herein further refine methods for pharyngoesophageal recon- struction. A major advancement for reconstruction of these challenging defects was introduced by Bakamjian [12], who described a two-stage recon- struction using the medially-based deltopectoral flap. A one-stage reconstruction of partial-circumferential pharyngoesophageal defects using a pectoralis major-carried island skin paddle was introduced by Theogaraj et al [8]. The technique we describe ex-
Volume 144, October 1992 491
Tobin et al
Figure 5. One-stage orofactal reconstructfon wtth spftt latfsstmus dorsf muscukx~~taneous flaps. Top left, mucocutaneous defect of oral floor and chin-submental skin. Top right, two Wand cutaneous paddles ( P) carded on split lattssknus dorsf muscle segments ( S). Bottom teft, muscuknxdaneous paddles ( P) passed sufJpectora/ty to th head and neck regton. Bottom rfght, one paddle restores oral fkwr lining ( P) . The otfter paddle restores chfn-submental skln cover ( P) .
tends the concept of one-stage musculocutaneous flap reconstruction of pharyngoesophageal defects by providing flap closure to both mucosal and cuta- neous defects with the same flap. In addition, we introduce latissimus dorsi musculocutaneous flap reconstruction of pharyngoesophageal defects.
To date, none of the human pharyngoesophageal defects that we have reconstructed with musculo- cutaneous flaps have been totally circumferential. The experimental animal pharyngoesophageal re- constructions presented in this report were done on circumferential defects created by surgical excision of an esophageal segment. Both human pectoralis major and latissimus dorsi musculocutaneous flaps carry sufficiently large paddles to reconstruct cir- cumferential pharyngoesophageal defects; however, this application has yet to be clinically established.
The technique we describe can be combined with other described refinements of pectoralis major and latissimus dorsi musculocutaneous flaps to provide additional versatility to head and neck reconstruc- tion. Extension of pectoralis major skin paddles be- yond the muscle borders to include epigastric or presternal skin provides longer cutaneous paddles and arcs of rotation and also preserves breast position and substance in females [13,14]. Epigastric skin can be carried on the pectoralis major external segment flap. Presternal skin can be carried on the pectoralis major sternocostal segment flap.
Our technique can also be combined with sev- eral methods that carry vascularized bone on the same flap for mandibular reconstruction. Tobin and associates transferred both serratus anticus-carried ribs and latissimus dorsi-carried skin flaps on sub-
492 The American Journal of Surgery

One-Stage Pharyngoesophageal and Oral Mucocutaneous Reconstruction
scapular vessel pedicles (Tobin GR, et al., unpublished data). Schlenker et al [15,16] carried ribs on latissi- mus dorsi-intercostal vessel perforator pedicles. Cunio and Ariyan [17] carried ribs on pectoralis major pedicles. Green et al [18] carried sternum on pectoralis major pedicles. Thus, segmentally split musculocutaneous flaps combined with techniques that carry vascularized bone on the same muscle pedicles provide reconstruction of the mandible, oral lining, and skin cover in one stage with one com- pound flap.
Herein we report the use of pedicle transfers to reconstruct mucocutaneous defects of the head and neck. Microvascular free tissue transfer techniques extend these concepts to more distant anatomic sites.
Summary
This report describes a one-stage technique that provides both cover and lining to mucocutaneous defects of the head and neck with either latissimus dorsi or pectoralis major musculocutaneous units that are split into anatomic segments to create two independent flaps from one musculocutaneous unit. In addition, this technique further refines recon- struction of pharyngoesophageal defects. Techniques of simultaneous mandibular reconstruction with vascularized bone carried on these same segmental flaps are also commented on.
References
1. Tobin GR, Schusterman M, Peterson GH, Nichols G, Bland KI. The intramuscular neurovascular anatomy of the latissimus dorsi muscle: the basis for splitting the flap. Plast Reconstr Surg 1981;87:837-41.
2. Tobin GR, Bland KI, Adcock R. Surgical anatomy of the mus- cufus pectoralis major and neurovascular supply. Surg Forum 1981;32:573-75.
3. Tobin GR, Moberg AW, DuBou RH, Weiner LJ, Bland KI. The split latissimus dorsi myocutaneous flap. Ann Plast Surg 1981; 7:272-80.
4. Tobin GR, Gordon JA, Smith B, Schusterman M. Preserving motor function by splitting muscle and myocutaneous ped- icles. Plast Surg Forum 1980;111:160-1.
5. Krizek TJ, Robson MC. Split flap in head and neck recon- struction. Am J Surg 1973; 126:488-g 1.
6. Ariyan S. The pectoralis major myocutaneous flap. A versatile flap for reconstruction in the head and neck. Plast Reconstr Surg 1979;63:73-81.
7. Ariyan S. Further experiences with the pectoralis major myo- cutaneous flap for the immediate repair for defects from excisions of head and neck cancers. Plast Reconstr Surg 1979;64:605-12.
8. Theogaraj SD, Merritt WH, Acharya G, Cohen IK. The pectoralis major musculocutaneous island flap in single-stage recon- struction of the pharyngoesophageal region. Plast Reconstr Surg 1980;65:267-76.
9. Baek SM, Lawson W, Biller HF. Analysis of 133 pectoralis major myocutaneous flaps. Plast Reconstr Surg 1982;69:460-7.
10. Quillen CG, Shearin JC, Georgeaide G. Use of the latissimus dorsi myocutaneous island flap for reconstruction in the head and neck area. Plast Reconstr Surg 1978;62:113-7.
11. Quillen CG. Latissimus dorsi myocutaneous flaps in head and neck reconstruction. Plast Reconstr Surg 1979;63:664- 70.
12. Bakamjian VY. A two stage method for pharyngoesophageal reconstruction with a primary pectoral skin flap. Plast Rec- onstr Surg 1965; 19: 173-84.
13. Magee WP, McGraw JB, Horton CE, Mclnnis WD. Pectoralis “paddle” myocutaneous flaps, the workhorse of head and neck reconstruction. Am J Surg 1980;140:507-13.
14. Sharzar LA, Kalisman M, Silver CE, Strauch B. The parasternal paddle: a modification of the pectoralis major myocutaneous flap. Plast Reconstr Surg 1981;67:753-62.
15. Schlenker JD, lndresano AT, Raine T, Merideth SC, Robson MC. A new flap in the dog containing a vascularized rib graft-the latissimus dorsi myoosteocutaneous flap. J Surg Res 1980;29: 172-83.
16. Schlenker JD, Robson MC, Parsons RW. Methods and results of reconstruction with free flaps following resection of squamous cell carcinoma of the head and neck. Ann Plast Surg 1981;6:362-73.
17. Cuono CB, Ariyan S. Immediate reconstruction of a composite mandibular defect with a regional osteomusculocutaneous flap. Plast Reconstr Surg 1980;65:477-83.
18. Green MF, Gibson JR, Dryson JR, Thompson E. A l-stage correction of mandibular defects using a split sternum Pectoralis major osteo-musculocutaneous transfer. Br J Plast Surg 1981;34:11-6.
volume 144. October 1982 493