Embed Size (px)
Citation preview

6/2/2014
1
Patent Foramen Ovale: Much Ado About Nothing?
Brian Ó Murchú MD
Associate Professor of Medicine
Director, Structural Heart Disease Intervention
Section of Cardiology
Temple University Hospital
June 7 2014
Why a Patent Foramen Ovale is relevant
Courtesy of Chip Jungreis MD
ABCs and 1-2-3s of PFO
• A is for apple, but PE isn’t just for pulmonary embolism
• Leonardo DaVinci did more than paint ceilings
• PFO and ASD: same thing, right?
• ASA can stand for more than for acetylsalicylic acid (aspirin)
• The number of devices currently approved in the US for transcatheter closure of PFO after a FIRST cryptogenic stroke

6/2/2014
2
courtesy of Alex Davidson, MD
TEE: tubular thrombus through a patent foramen ovale
Koullias G J et al. Circulation 2004;109:3056-3057
Intraoperative demonstration of the large thrombus traversing the patent foramen ovale (arrows).
Koullias G J et al. Circulation 2004;109:3056-3057

6/2/2014
3
Reconstruction of thrombus through the patent foramen ovale (arrows) and in the pulmonary artery
Koullias G J et al. Circulation 2004;109:3056-3057
PE
Intermittent Right to Left shunt: Potential for Paradoxical Embolism
Res ipsa loquitur
Images courtesy of Alex Davidson MD
Septum Primum
Ostium Primum
Ostium Secundum
Right Atrium Left Atrium
Tricuspid Mitral
IVC
SVC
Endocardial cushion
Embryology: Common Atrium35 days

6/2/2014
4
Ostium Secundum
Right Atrium Left Atrium
Tricuspid Mitral
IVC
SVC
Endocardial cushion
Septum Secundum
Foramen ovale
This persists from day 55 until birthDay 35-55
Right Atrium Left Atrium
Tricuspid Mitral
IVC
SVC
Septum Secundum
Septum Primum
At birth…..
• The apposing portions of septum primum and septum secundumgradually fuse
• This is complete by age 2 in 75% of people
• In 25% of people, fusion fails to occur and a residual tunnel persists (patent foramen ovale)
How prevalent is a PFO? Autopsy Study
• Overall incidence 27.3% (263/965)
• No gender differences
• Far more frequent than being left-handed (7-10%)
Hagen et al Mayo Clin Proc 1984;59:17-20

6/2/2014
5
Size Distribution of PFO
Number ofPFO
Size of PFO (mm) Hagen et al Mayo Clin Proc 1984;59:17-20
Mean PFO diameter 4.9 mm range 1-19 mm1-10 mm in 98%
Incidence of PFO by Decade
Hagen et al Mayo Clin Proc 1984;59:17-20
%
Right Atrium Left Atrium
Tricuspid Mitral
IVC
SVC
3 out of 4 of us in this room
Fused Septum Primumand Septum Secundum
CO(Qs)
CO(Qp) =

6/2/2014
6
Right Atrium Left Atrium
Tricuspid Mitral
IVC
SVC
The 75% meet UFO
Fused Septum Primumand Septum Secundum
RV
RA
LV
LA
The “Bubble” Study
Right Atrium Left Atrium
Tricuspid Mitral
IVC
SVC
UFO meets PFO
Potential for
Paradoxical Embolism

6/2/2014
7
RV
RA
LA
PFO
LV (Next Stop: The Brain)
Plane of the Atrial Septum
Intermittent Right to Left shunt: Potential for Paradoxical Embolism
Res ipsa loquitur
Images courtesy of Alex Davidson MD
ASD. PFO.
Same thing, right?
Wrong!

6/2/2014
8
ASD: Great big hole
Right Atrium Left Atrium
Tricuspid Mitral
IVC
SVC
ASD:
ASD
Qp COQs
Deficient Septum Secundum
QsLifelong Volume Overload
of the Right Heart
ASD. PFO.
Same thing, right?
Wrong!

6/2/2014
9
Important Differences between ASD and PFO:
PFO
• PFO: Normal septal growth with failed fusion of the apposing walls of the foramen ovale • Right-to-left communication• Volume is NOT the concern• Concern is for paradoxical embolism of thrombus,
platelets, air bubbles, endogenous substances, desaturated blood…………….
• ASD: Deficient septal growth leaving a hole• Predominantly left-to-right shunting from the higher
pressure LA to the lower pressure RA• Volume IS the concern• Shunting of blood causes lifelong volume overload of
the right heart which results in dilation and ultimately in clinical symptoms and signs of right heart failure (not left)• Minor right-to-left component
Important Differences between ASD and PFO:
ASD
6/2/2014
10
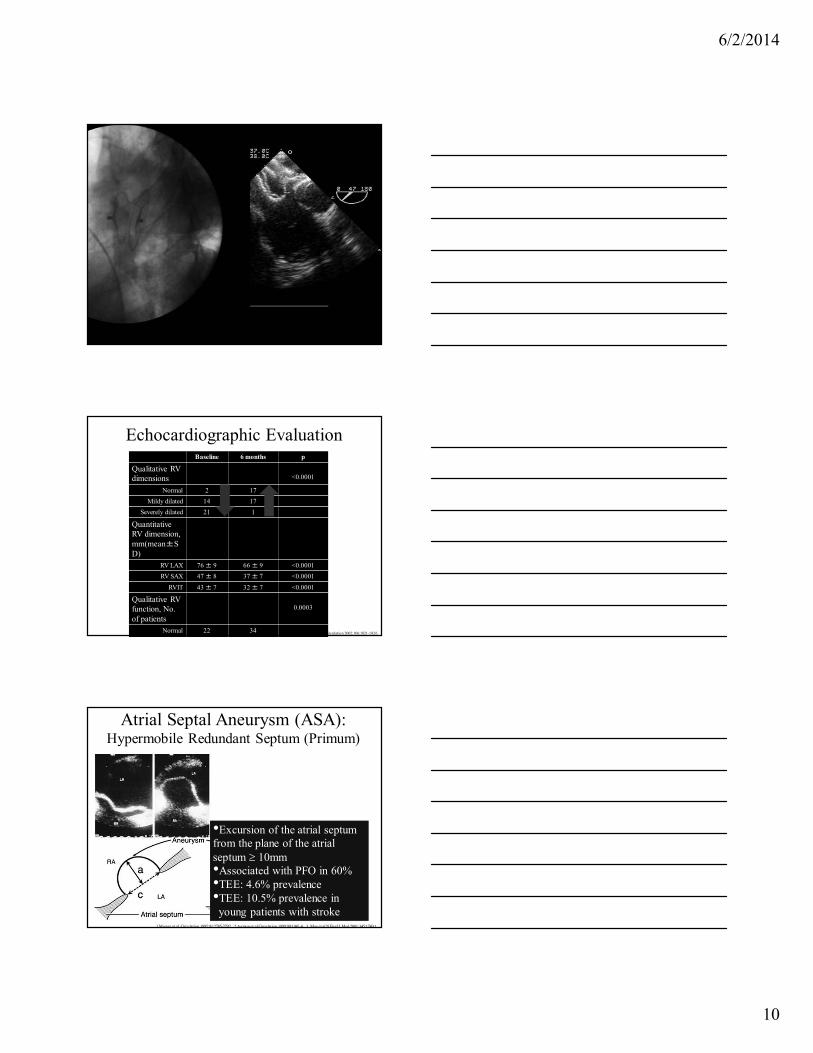
Echocardiographic EvaluationBaseline 6 months p
Qualitative RV dimensions <0.0001
Normal 2 17
Mildy dilated 14 17
Severely dilated 21 1
Quantitative RV dimension, mm(mean±SD)
RV LAX 76 ± 9 66 ± 9 <0.0001
RV SAX 47 ± 8 37 ± 7 <0.0001
RVIT 43 ± 7 32 ± 7 <0.0001
Qualitative RV function, No. of patients
0.0003
Normal 22 34 Brochu et al Circulation 2002;106:1821-1826
1.Mugge et al. Circulation 1995;91:2785-2792. 2.Agmon et al Circulation 1999;99:1942-4. 3. Mas et al N Engl J Med 2001;345:1740-6
Atrial Septal Aneurysm (ASA):Hypermobile Redundant Septum (Primum)
•Excursion of the atrial septum from the plane of the atrial septum ≥ 10mm•Associated with PFO in 60%•TEE: 4.6% prevalence•TEE: 10.5% prevalence in young patients with stroke

6/2/2014
11
Why do we care?
Courtesy of Chip Jungreis MD
Patent Foramen Ovale: PFO Under indictment……
• Unexplained Stroke (especially in young people): due to presumed paradoxical embolism through a PFO
• Right-to-left shunting causing hypoxia (Platypnea-Orthodeoxyia)
• Decompression sickness
• Migraine
• ??High-Altitude Pulmonary Edema
Cryptogenic (unexplained) Stroke and PFO
How so?
• In patients under 55 years of age, up to 40% of strokes are cryptogenic
• Transthoracic echo and bubble study have allowed for the noninvasive, in vivo diagnosis of PFO with right to left shunting

6/2/2014
12
Diagnosis and Quantification of PFO: The “bubble study”
RV
RA
LV
LA
Autopsy: 27%Transthoracic: 5-15%Transesophageal 25%
Size: Number of bubblesWidth of the tunnel
Agmon et al Am J Cardiol 2001;88:330
Prevalence of PFO in Patients with Cryptogenic Stroke age <55
Cryptogenic Stroke
Control p
Lechat 1988 54% 10% <0.01
Webster 1988 50% 15% <0.01
Di Tullio 1992 48% 4% <0.01
Lechat et al N Engl J Med 1988;318:1148-52Webster et al Lancet 1988;2:11-12Di Tullio et al Ann Intern Med 1992;117:461-5
•Association is weaker in older patients: or maybe not..
Association of PFO and PFO with ASA with Cryptogenic Stroke:
Maybe it’s not just in the young
Handke M et al. N Engl J Med 2007;357:2262-2268

6/2/2014
13
Suspected paradoxical embolism: Is it just the PFO?
•Atrial anatomy•Size of the PFO•Atrial septal aneurysm•Fetal Remnants (Eustachian valve, Chiari network)
630 patients (ages 30-85) with PFO (TEE) and Stroke
Patent Foramen Ovale in Cryptogenic Stroke Study (PICCS)
Determined cause
n=351
Cryptogenic
n=250 p
PFO 29.9% (105/351) 39.2% (98/250) <0.02
Large PFO 9.7% (34/351) 20% (50/250) <0.001
Homma et al Circulation 2002;105:2625-2631
Atrial Septal Aneurysm and PFO:Increases the risk of Stroke Recurrence
Mas et al N Engl J Med 2001;345:1740-6
581 patients<56 yearsCryptogenic strokeAspirin

6/2/2014
14
Prevalence of PFO in Patients with Cryptogenic Stroke or with
Stroke of Known Cause
Handke M et al. N Engl J Med 2007;357:2262-2268
PFO and Stroke:Why the association with Atrial Septal
Aneurysm?
Homma et al J Am Coll Cardiol 2003;42:1066-72
PICSS Trial
Clinical Profile ComparisonPermanent and Valsalva-only Shunt
Patients
Rigatelli et al. J Am Coll Cardiol 2011;58:2257

6/2/2014
15
Paradoxical Embolism: Trifecta
• Potential transit route: PFO…….
• Venous Source
• Intermittent opening of the foramen.........
Is there a venous source of embolus when cryptogenic stroke occurs in
young patients with PFO?
• Occult Leg DVT: inconclusive results • Other venous sources: Pelvic veins?• 95 patients with Stroke • Cause determined: 49• Cryptogenic: 46• Magnetic Resonance Venography of pelvis within
72 hours of stroke
Stollberger et al Ann Intern Med 1993;119:461-465Ranoux et al Stroke 1993;24:31-34Cramer et al Stroke 2004;35:46-50
Determined (n=49)
Cryptogenic (n=46)
p
Age 49 42 0.0002
PFO (%) 19 59 0.0002
ASD (%) 0 2 1.0
High Probability for Pelvic DVT, n (%)
2/49 (4) 9/46 (20) 0.025
Acute 0/47 (0) 3/40 (7) 0.093
Chronic 2/49 (4) 6/43 (13) 0.14
Paradoxical Emboli from Large Veins in Ischemic Stroke (PELVIS)
Cramer et al Stroke 2004;35:46-50

6/2/2014
16
Atrial Hemodynamics:Might outcome of Pulmonary Embolism
be worse when a PFO is present?
• PE: well, it sure is a source of embolism
• Abrupt increase in right sided filling pressure
• 139 patients with major PE: Contrast echo for PFO detection (1988-1994)
• PFO absent 91 (65%)
• PFO present 48 (35%)
Konstantinides et al Circulation 1998;97:1946-1951
Atrial Hemodynamics:Might outcome of Pulmonary Embolism
be worse when a PFO is present?
• Mortality 29/139 (21%)
• Ischemic Stroke: 8/139 (5.8%)
• Arterial Embolism: 7/139 (5%)
• Were these events associated with PFO?
Konstantinides et al Circulation 1998;97:1946-1951
Event
PFO Present (n=48)
n, (%)
PFO Absent (n=91)
n, (%) p
Ischemic Stroke
6 (13) 2 (2.2) 0.02
Peripheral arterial embolism
7 (15) 0 <0.001
Death 16 (33) 13 (14) 0.015
Pulmonary Embolism: Is outcome worse with a PFO?
Konstantinides et al Circulation 1998;97:1946-51

6/2/2014
17
Reconstruction of thrombus through the patent foramen ovale (arrows) and in the pulmonary artery
Koullias G J et al. Circulation 2004;109:3056-3057
PE
PFO and Cryptogenic Stroke
• Association especially in younger patients
• May be influenced by specific atrial anatomy, concurrent venous thrombosis and acute changes in atrial hemodynamics
Prospective Circumspection Stroke Prevention: Assessment of Risk in a
Community (SPARC) study
Meiss ner et al J Am Coll Cardiol 2006;47:440-5
585 patients Age >45 (mean age 66)
PFO in 140 patients (24.3%) Atrial Septal Aneurysm 11 (1.9%)
PFO +ASA : 6/140 (4.3%)Fused FO +ASA: 5/437 (1.1%) p=0.0028
41 patients had a stroke PFO had no effect on strokeMean age 66………Atrial septal aneurysm was weakly associated with a higher stroke risk

6/2/2014
18
Cryptogenic Stroke and PFO: Is it Paradoxical Embolism?
A Presumptive Diagnosis of Exclusion based on
Circumstantial Evidence
Cryptogenic Stroke in patients with PFO?
• What is the best, current management of a young patient with a FIRST cryptogenic stroke when all that can be found at the crime scene is a smoking PFO…………..?
• Should treatment be with Aspirin, Warfarin, or should the defect be closed?
Cryptogenic Stroke with PFO:Treatment to prevent recurrence
• Antiplatelet therapy
• Anticoagulation
• Surgical closure
• Percutaneous closure

6/2/2014
19
Surgical Closure
• 28 patients with cryptogenic stroke and PFO• mean age 41±13, 19 months follow up• Recurrence in 4 (14.3%), all in patients over 45 years
Homma et al Stroke 1997;28:2376-81
Prevention of Recurrent Stroke:Aspirin
Mas et al N Engl J Med 2001;345:1740-6
581 patients<56 yearsCryptogenic strokeAspirin
PFO: 12% Recurrent strokeor TIA rate over 4 years
PFO with ASA:Failure
• Warfarin Aspirin Recurrent Stroke Study (WARSS): 2206 patients aged 30-85 followed for 2 years for death or recurrent stroke
• Excluded: Cardiogenic source or planned CEA for high-grade carotid stenosis
• Aspirin (325mg) vs Anticoagulation (INR 1.4-2.8)
Prevention of Recurrent Stroke:Antiplatelet and Anticoagulant Therapy
Thompson et al N Engl J Med 2001;345:1444-1451
6/2/2014
20
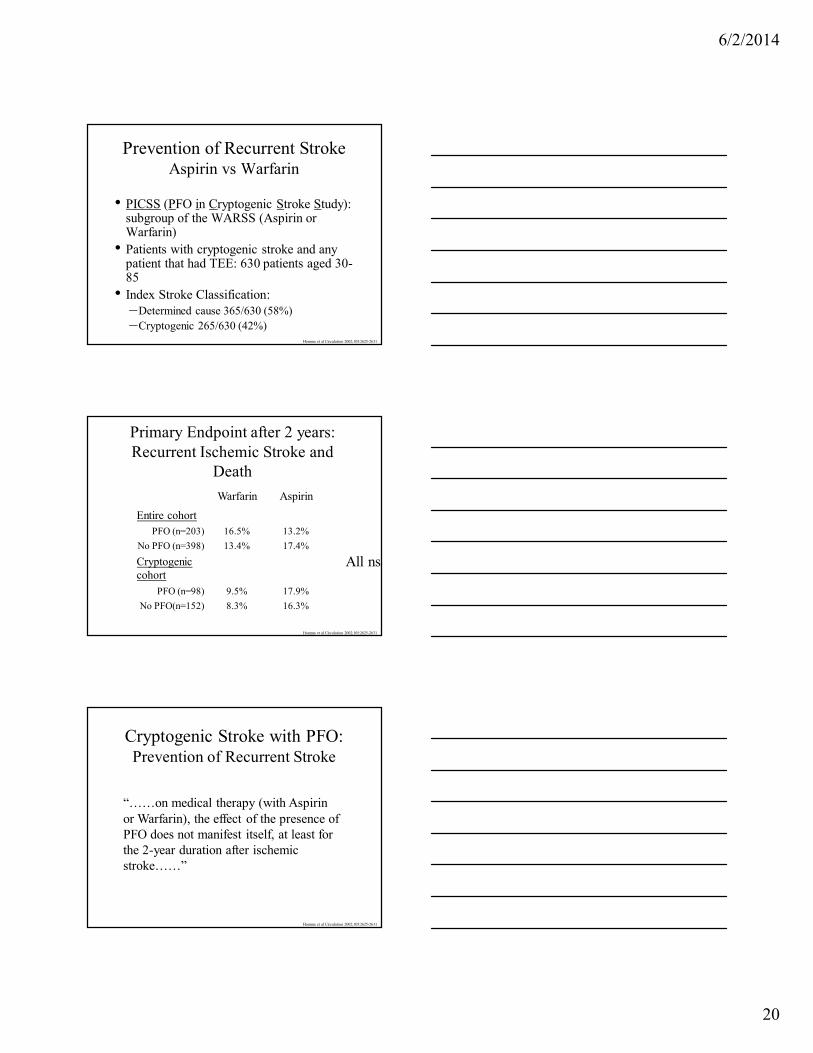
• PICSS (PFO in Cryptogenic Stroke Study): subgroup of the WARSS (Aspirin or Warfarin)
• Patients with cryptogenic stroke and any patient that had TEE: 630 patients aged 30-85
• Index Stroke Classification:–Determined cause 365/630 (58%)–Cryptogenic 265/630 (42%)
Homma et al Circulation 2002;105:2625-2631
Prevention of Recurrent StrokeAspirin vs Warfarin
Warfarin Aspirin
Entire cohortPFO (n=203) 16.5% 13.2%
No PFO (n=398) 13.4% 17.4%
Cryptogenic cohort
PFO (n=98) 9.5% 17.9%
No PFO(n=152) 8.3% 16.3%
Primary Endpoint after 2 years:Recurrent Ischemic Stroke and
Death
Homma et al Circulation 2002;105:2625-2631
All ns
Cryptogenic Stroke with PFO:Prevention of Recurrent Stroke
Homma et al Circulation 2002;105:2625-2631
“……on medical therapy (with Aspirin or Warfarin), the effect of the presence of PFO does not manifest itself, at least for the 2-year duration after ischemic stroke……”
6/2/2014
21
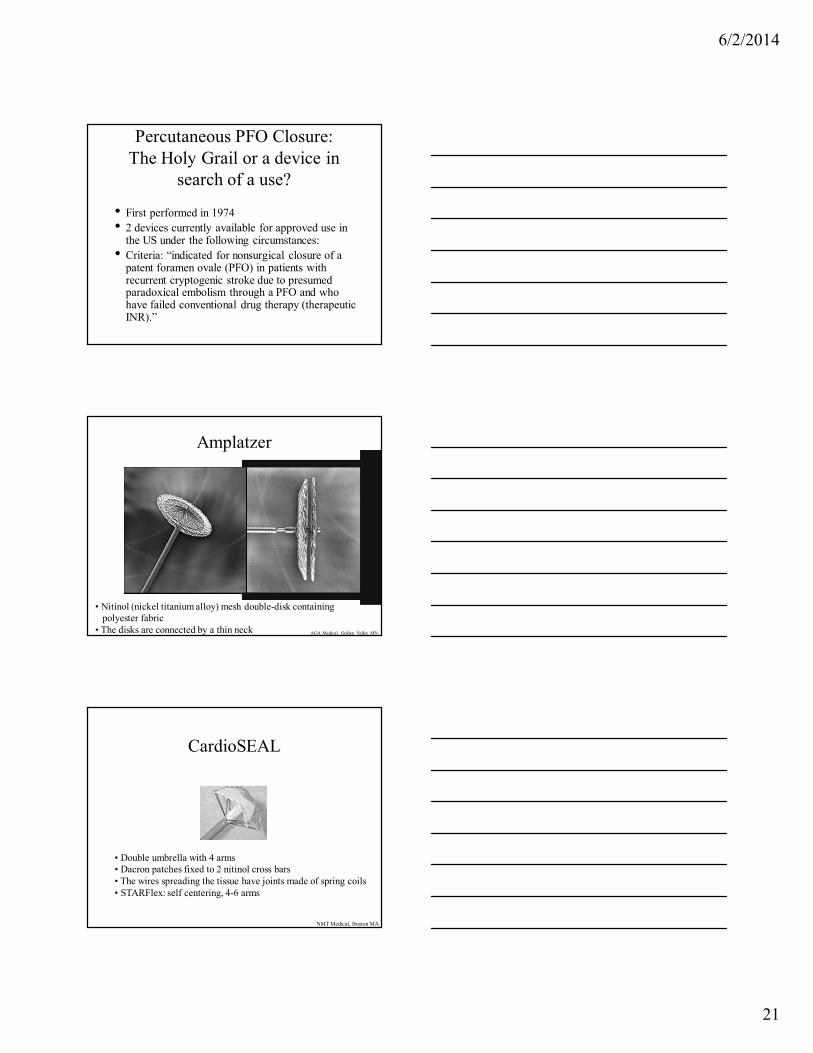
Percutaneous PFO Closure:The Holy Grail or a device in
search of a use?
• First performed in 1974• 2 devices currently available for approved use in
the US under the following circumstances: • Criteria: “indicated for nonsurgical closure of a
patent foramen ovale (PFO) in patients with recurrent cryptogenic stroke due to presumed paradoxical embolism through a PFO and who have failed conventional drug therapy (therapeutic INR).”
Amplatzer
AGA Medical, Golden Valley MN
• Nitinol (nickel titanium alloy) mesh double-disk containing polyester fabric
• The disks are connected by a thin neck
CardioSEAL
NMT Medical, Boston MA
• Double umbrella with 4 arms• Dacron patches fixed to 2 nitinol cross bars • The wires spreading the tissue have joints made of spring coils• STARFlex: self centering, 4-6 arms

6/2/2014
22
Endothelialization
Sharafuddin et al Circulation 1997;95:2162-8

6/2/2014
23
Medical Therapy versus Percutaneous Closure
Mean
Age
Duration of Follow up
Annual Stroke Rate
Annual Death rate
Annual rate for Stroke or
Death
Medical Therapy
(n=943)
9 studies
45 33 months 1.98% 0.94% 3.12%
Percutaneous Closure
(n=1430)
12 studies
46 18 months 0.19% 0.66% 1.15%
Adapted from Homma et al Circulation 2005;112:1063-1072
Composite Outcomes in the propensity score–matched cohort
Wahl A et al. Circulation 2012;125:803-812
Randomized Trials: CLOSURE-1
• Evaluation of the STARFlex Septal Closure System in Patients with a Stroke or TIA due to the Possible Passage of Clot of Unknown Origin through a Patent Foramen Ovale

6/2/2014
24
CLOSURE-1Closure or Medical Therapy for Cryptogenic
Stroke with Patent Foramen Ovale
Furlan AJ et al. N Engl J Med 2012;366:991-999
•Prospective, multicenter, randomized, open-label, two-group superiority trial
•Inclusion Criteria:
18-60 years old
First Ischemic stroke or TIA within the previous 6 months
Presence of a PFO (contrast TEE)
•Exclusion Criteria:
Known other cause of stroke (carotid disease, atrial fibrillation,
complex aortic arch atheroma, LV dysfunction or aneurysm)
Prothrombotic disorder, APLA (pre-randomization testing)
SLE, GCA
•Randomized 1:1
Device Closure plus Medical Therapy (aspirin 81 or 325mg for 2 years,
Clopidogrel 75mg for 6 months)
OR
Medical Therapy alone: either Aspirin 325mg OR Warfarin (INR 2-3)
at the discretion of the site PI, for 2 years
CLOSURE 1: Assessment of Degree of Shunt
Furlan AJ et al. N Engl J Med 2012;366:991-999
Defintion of shunt: appearance of bubbles in the left atrium within 5 cardiac cycles
after opacification of the right atrium, either at rest or after Valsalva maneuver
Degree of Right to Left shunt:
None: no bubbles
Trace 1-10 bubbles
Moderate 10-25 bubbles
Substantial ≥25 bubbles
PFO size was measured in the device closure arm by indentation with a soft
balloon during catheterization (mean PFO size 10.2±±±±5.1mm)
CLOSURE 1: Definition of Primary Endpoint
Furlan AJ et al. N Engl J Med 2012;366:991-999
Primary Endpoint: Composite of
Stroke OR TIA during 2 year follow up
Death from any cause during the first 30 days
Death from Neurologic cause between day 31 and 2 years
Furlan AJ et al. N Engl J Med 2012;366:991-999

6/2/2014
25
Furlan AJ et al. N Engl J Med 2012;366:991-999
Primary End Point at 2 Years
Furlan AJ et al. N Engl J Med 2012;366:991-999
Primary End Point through 2 Years of Follow-up
Furlan AJ et al. N Engl J Med 2012;366:991-999

6/2/2014
26
Furlan AJ et al. N Engl J Med 2012;366:991-999
CLOSURE 1: Subgroup analysis
Serious Adverse Events
Device Performance: 6 month TEE to assess Effectiveness of closure: Definition of Effective Closure: None or trace residual shunt
366 patients had TEE:Effective closure in 315 (86.1%)
Thrombus in the Left atrium: 4 of 366 (1.1%) 2/4 sustained stroke
PC TRIAL
PERCUTANEOUS PFO CLOSURE
Amplatzer PFO Occluder
Acetylsalicylic acid (100-325mg qd)
and ticlopidine (250-500mg qd)
or clopidogrel (75mg qd)
for 6 months
1:1
RCT
MEDICAL TREATMENT
Oral anticoagulation or
Antiplatelet therapy
at the discretion of the neurologist
Meier B et al. N Engl J Med 2013;368:1083-1091

6/2/2014
27
Study End Points: Death, non-fatal stroke, TIA or peripheral embolism
Primary End Point: Death, non-fatal stroke, TIA or peripheral embolism
Meier B et al. N Engl J Med 2013;368:1083-1091
Any hint as to where benefit might be lurking?
Meier B et al. N Engl J Med 2013;368:1083-1091

6/2/2014
28
Randomized Trials
• RESPECT: Randomized Evaluation of Recurrent Stroke Comparing PFO Closure to Established Current Standard of Care Treatment
RESPECTUSA and Canada
Inclusion Criteria:
★★★★Age 18 to 60
★Cryptogenic Stroke within 270 days: acute ischemic focal neurological deficitand either symptoms persisting 1) ≥ 24 hours, or 2) < 24 hours with MR or CT onfirmed new, neuroanatomically relevant, cerebral infarct
★PFO: TEE, bubbles in the left atrium within 3 cardiac cycles of their appearance in the right atrium at rest and/or during Valsalva release
Key Exclusion Criteria:
Carotid disease, atrial fibrillation, structural heart disease, hypercoagulable states.
Any other reason to expect limited life expectancy, inability to attend follow-upvisits, or inability to provide informed consent
Carroll JD et al. N Engl J Med 2013;368:1092-1100
Grading of Right to Left Shunt
Carroll JD et al. N Engl J Med 2013;368:1092-1100

6/2/2014
29
Carroll JD et al. N Engl J Med 2013;368:1092-1100
RESPECT: Trial Endpoints
Primary Endpoints
★★★★ Recurrence of a nonfatal ischemic stroke or★★★★ Fatal ischemic stroke or★★★★ Early post-randomization death defined as all-cause mortality
Device group – within 30 days after implant or 45 days after randomization, whichever occurs latest
Medical group – within 45 days after randomization
Secondary Endpoints
★★★★ Complete closure of the defect demonstrated by TEE bubble study at 6-month follow-up (Device Group)
★★★★ Absence of recurrent cryptogenic nonfatal stroke or cardiovascular death★★★★ Absence of transient ischemic attack (TIA)
Carroll JD et al. N Engl J Med 2013;368:1092-1100
RESPECT: Power Analysis and Event Driven Design★★★★ Estimated rate of primary efficacy events at 2
years was 4.3% in the medical group and 1.05% in the device group
� An event driven trial design was employed since event rates were estimated to be low★★★★ Enrollment was stopped December 29, 2011
when the decision rule of 25 primary endpoint events was reached which led to the presentation of results
Carroll JD et al. N Engl J Med 2013;368:1092-1100
6/2/2014
30
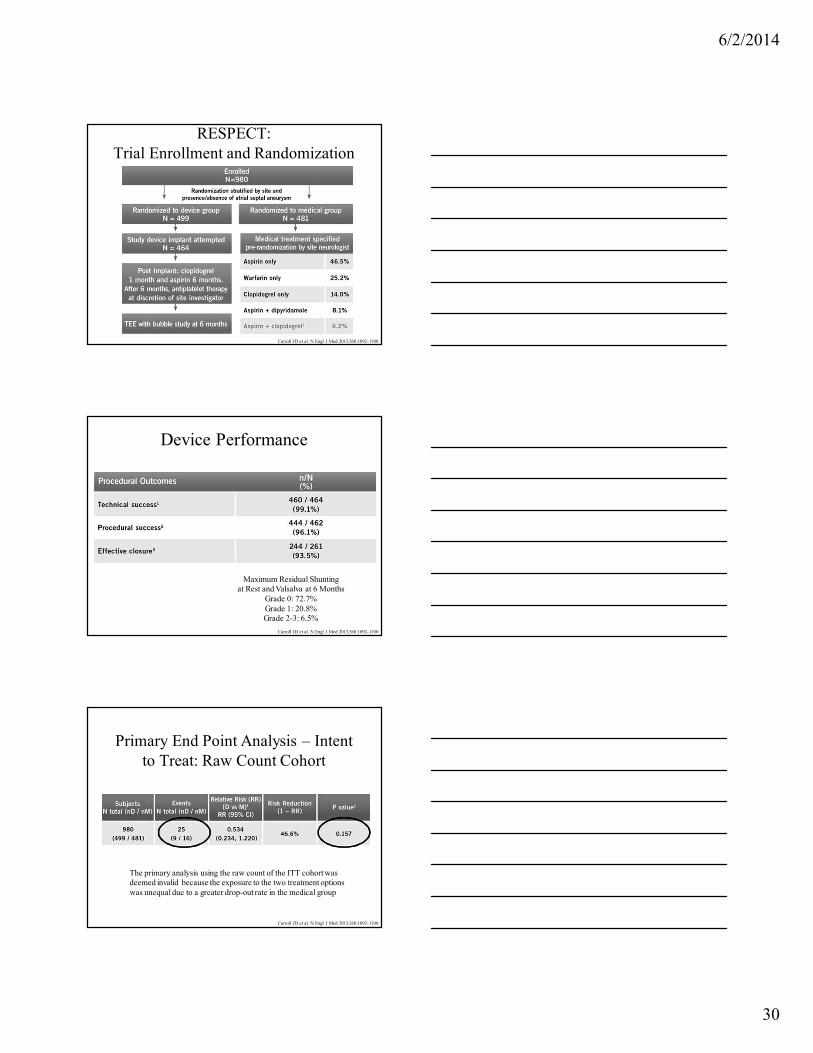
RESPECT: Trial Enrollment and Randomization
Carroll JD et al. N Engl J Med 2013;368:1092-1100
Device Performance
Maximum Residual Shuntingat Rest and Valsalva at 6 Months
Grade 0: 72.7%Grade 1: 20.8%Grade 2-3: 6.5%
Carroll JD et al. N Engl J Med 2013;368:1092-1100
Primary End Point Analysis – Intent to Treat: Raw Count Cohort
The primary analysis using the raw count of the ITT cohort wasdeemed invalid because the exposure to the two treatment optionswas unequal due to a greater drop-out rate in the medical group
Carroll JD et al. N Engl J Med 2013;368:1092-1100

6/2/2014
31
Baseline Characteristics of Study Patients
Carroll JD et al. N Engl J Med 2013;368:1092-1100
Primary End-Point:Intention-to-Treat and As-Treated Cohorts.
Carroll JD et al. N Engl J Med 2013;368:1092-1100
Subgroup Analysis: Big shunt, ASA?
Carroll JD et al. N Engl J Med 2013;368:1092-1100

6/2/2014
32
Procedure related Adverse outcomes
Carroll JD et al. N Engl J Med 2013;368:1092-1100
Primary Endpoint Analysis – ITT Cohort50.8% risk reduction in favor of device
3/9 device group patients did not have a device at time of endpoint strokeCarroll JD et al. N Engl J Med 2013;368:1092-1100
Primary Endpoint: As Treated Cohort72.7% risk reduction in favor of device
Outcome treatment according to treatment actually received, regardless of randomization assignment
Carroll JD et al. N Engl J Med 2013;368:1092-1100

6/2/2014
33
Recurrent Stroke Size(Methods pre-specified; analysis post-hoc)
Site-reported recurrent stroke size suggests that recurrent strokes in the medical group are larger than in device-treated patients
Carroll JD et al. N Engl J Med 2013;368:1092-1100
Randomized Trials: Questions answered or not?
Detection of Atrial Fibrillation
Jabaudon D et al. Stroke 2004;35:1647-1651

6/2/2014
34
Healey JS et al. N Engl J Med 2012;366:120-129
Risk of Ischemic Stroke or Systemic Embolism over 2.5 years of follow up:
Significance of Subclinical Atrial Arrhythmias 261/2451(10.1%)
4.2%
(11/261)
1.69% per year
1.7%
(40/2319)
0.69% per year
p=0.007
Cryptogenic Stroke with PFO:Prevention of Recurrence
• Antiplatelet therapy
• Anticoagulation
• Percutaneous closure
Cryptogenic Stroke with PFO: When should percutaneous
closure be offered?
• Patient
• Defect
• Device

6/2/2014
35
Evaluation of the Young Patient with Stroke
• MRI/MRA
• Duplex of extracranial carotid arteries
• Basic: ESR, Rheumatoid factor, RPR, Antiphospholipid antibodies, UDS (cocaine)
• Hematologic abnormality: C, S, ATIII, APCR, Prothrombin mutation, Factor V Leiden
• EKG, ?Holter, event recorder in older patients
• Transthoracic echo with bubble study
• TEE
No argument
• Transcatheter Closure of PFO: •Recurrent Cryptogenic Stroke in a young
person despite therapeutic anticoagulation
• Incidental Finding: leave it alone
Nothing BUT Argument• First Cryptogenic Stroke: primary results of randomized
studies are negative, with some suggestions……..
• Accurate Stroke diagnosis (embolic): 100% Neurology
• Comprehensive evaluation including hypercoagulability
work-up: Hematology/Rheumatology
• Comprehensive cardiac evaluation: TEE, Holter or Event recording
• Younger……
• Large PFO, atrial septal aneurysm, multiple events
• Individualized management
• Informed patient: off-label use

6/2/2014
36
Procedures have Complications
• Device Erosion and embolism
• Tamponade
• Atrial Perforation
• Aorto atrial communication
Late Thrombus Complicating Percutaneous Closure: 1000 cases
Krumsdorf et al J Am Coll Cardiol 2004;43:302-9
• Specific Device affects closure rate
Successful Closure may be device specific
Rashkind Occluder
CardioSeal StarFlex Amplatzer Septal
Occluder
Amplatzer PFO
Occluder
Number of patients
7 50 20 18 72
Occlusion rate 70% 90% 90% 100% 99%
Schuchlenz et al Int J Cardiol 2005;101:77-82

6/2/2014
37
The Beatles, PFO and Migraine





























