Embed Size (px)
Citation preview
BABCOCK UNIVERSITY
SCHOOL OF PUBLIC AND ALLIED HEALTH
DEPARTMENT OF MEDICAL LABORATORY SCIENCE
20152016 SEMINAR PRESENTATION ON
THE UTILITY OF BONE MARKERS MEASUREMENT IN THE
DIAGNOSIS AND MANAGEMENT OF OSTEOPOROSIS
BY
OMOVIYE EMMANUEL O 111909
FEBRUARY 18 2016 1
Summary as presented
2
Outline
bull Bone definition
bull Structure and functions of bone
bull Formation and resorption of bone
bull Osteoporosis
bull Diagnostic bone markers in osteoporosis
bull Conclusion
bull Selected references 3
Bone definition
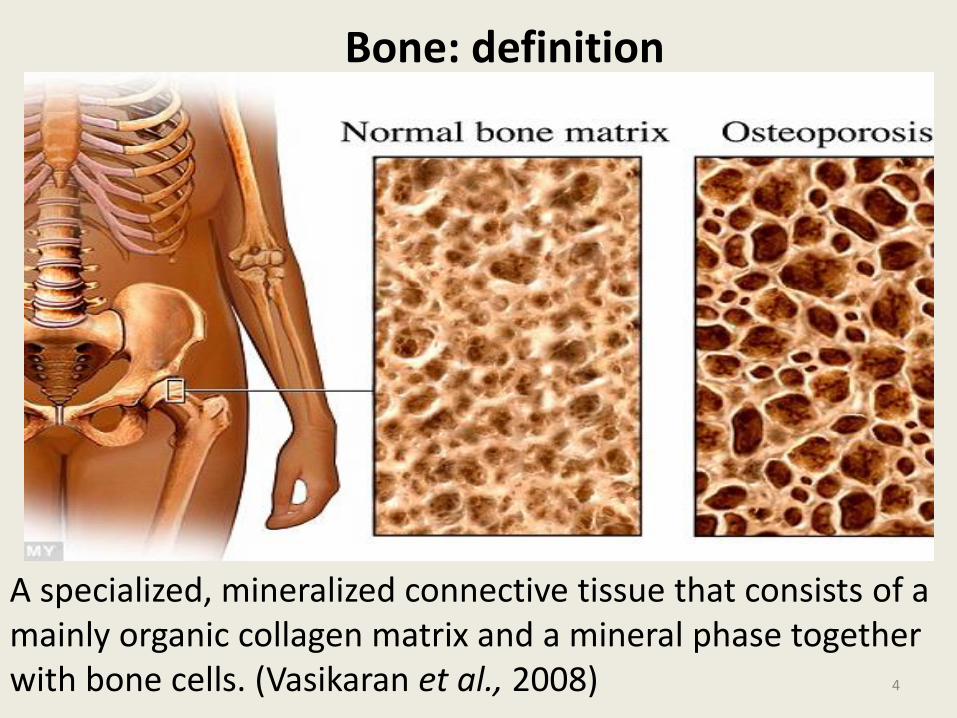
A specialized mineralized connective tissue that consists of a mainly organic collagen matrix and a mineral phase together with bone cells (Vasikaran et al 2008)
4
Bone Structure and Function
Bone
Structure
Extracellular matrix
Cellular constituents
Function
Mechanical Synthetic Metabolic
5
Bone Formation and Resorption
bull Metabolically active and constantly being repaired and remodelled
throughout an individuals lifetime
bull Formation involves actively synthesizing osteoblasts while its
resorption involves multinucleated osteoclasts (Vasikaran et al
2008)
bull Osteoporosis occurs when bone resorption is the more active
(Wheater et al 2013) 6
Osteoporosis
bull A systemic skeletal disease characterized by low bone mass and
micro-architectural deterioration of bone tissue with a
consequent increase in bone fragility and susceptibility to
fractures (Burch et al 2014)
bull Risk factors Age hormonal disturbances genetic lifestyle drugs
and some diseases like hyperthyroidism
bull Results in substantial morbidity and an estimated health cost gt
$14billion annually (McCormick 2007)
7
Osteoporosis Epidemiology
bull Prevalence 30 in women living in developed countries
bull Age and Sex 3 in 5 women gt 65 years and 1 in 5 men gt 75
years
bull Race predominant among Caucasians and Asians
bull Genetics studies suggest a significant genetic component
bull Geography most common in developed countries
(McCormick 2007)
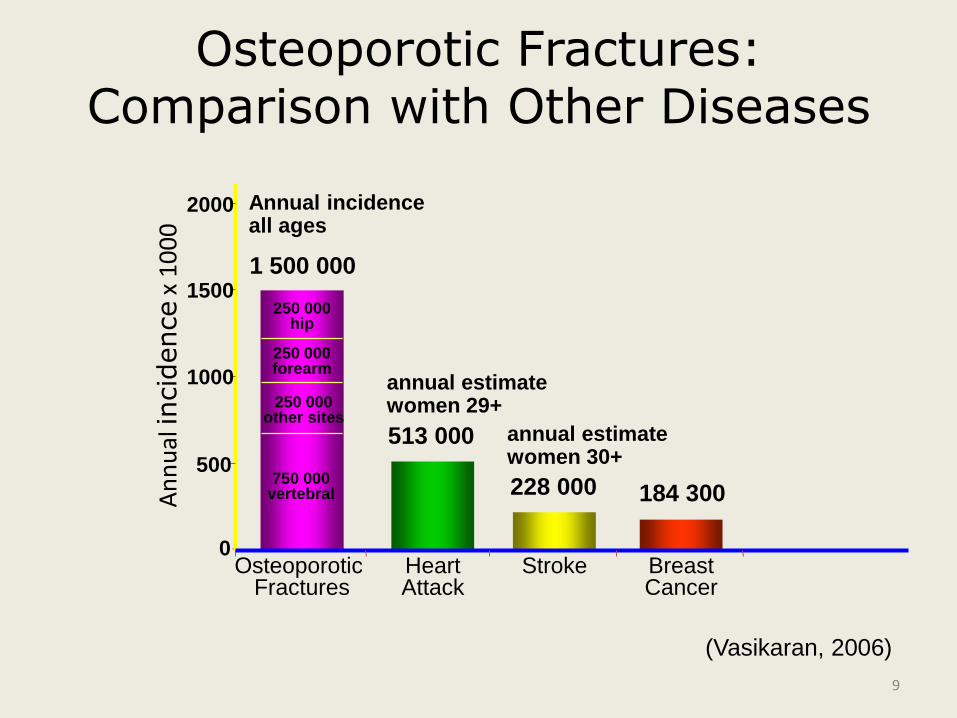
Osteoporotic Fractures Comparison with Other Diseases
184 300 750 000
vertebral
250 000 other sites
250 000 forearm
250 000 hip
0
500
1000
1500
2000
Osteoporotic Fractures
Heart Attack
Stroke Breast Cancer
An
nu
al in
cid
ence
x 1
00
0
1 500 000
Annual incidence all ages
513 000
annual estimate women 29+
228 000
annual estimate women 30+
(Vasikaran 2006)
9
Vertebrae
Hip
Wrist
50 60 70 80
40
30
20
10
Age (Years)
An
nu
al in
cid
en
ce p
er
10
00
w
om
en
Incidence of Osteoporotic Fractures in European Women
(Burch et al 2014)
Diagnostic Tools in Osteoporosis
bull Bone Mineral Density (BMD) scanning using dual-energy X-
ray absorptiometry (DXA) is the WHO standard for
diagnosis of osteoporosis (McCormick 2007)
bull DXA measures the amount of bone mineral in bone tissue
bull BMD is used in cliinical medicine as an indirect indicator of
osteoporosis
bull Poor sensitivity of DXA means that potential fractures will
be missed if it is used alone (Wheater et al 2013)
11
Limitations of BMD measurements in the Diagnosis of Osteoporosis
bull Changes in bone metabolism after therapy are detectable
only after about 2 years
bull Limited access to the technology
bull It is relatively expensive
bull The exposure to radiation although small is best avoided
bull Bone biomarkers offer an alternative monitoring strategy
(Burch et al 2014)
12
Diagnostic Bone Markers in Osteoporosis
bull Specifically derived biomarkers that reflect both bone formation by osteoblasts and resorption by osteoclasts
bull Include both enzymes and peptides derived from cellular and non-cellular compartments of bone
bull May be measured in synovial fluid blood or urine
bull Techniques for their measurements are abundant
bull Classified as bone formation and resorption markers (Seibel 2005) 13
Diagnostic Bone Markers in Osteoporosis
bull Detect metabolic changes in bone after about 3-6 months
(McCormick 2007)
bull Relatively cheap compared with DXA (Wheater et al 2013)
bull No exposure to radiation
bull Helpful tools in the diagnostic prognostic and therapeutic
assessment of osteoporosis
14
Diagnostic Bone Markers in Osteoporosis
15
Markers of Bone Formation
16
Bone Alkaline Phosphatase (BALP)
bull Total alkaline phosphatase has several isoforms in serum
(Liver bone placental intestine spleen and kidney)
bull 40ndash50 of the total alkaline phosphatase activity arises from
the bone as a result of osteoblast activity (Siebel 2005)
bull Residual low cross-reactivity (16) with liver ALP limits its use
in patients with liver disease (Yang and Grey 2006) 17
Bone Alkaline Phosphatase (BALP) Assays
bull Immunoradiometric assay (IRMA)
bull Enzyme-linked immunosorbent assay (ELISA)
bull Ease of measurement cost efficiency and higher
specificity in detecting small changes makes BALP a
good marker for bone formation (Burch et al
2008) 18
Osteocalcin
bull A non collagenous matrix protein
bull Detected using enzyme linked immunosorbent assays (ELISA) or radioimmunoassays (RIA)
bull It is tissue specific widely available (Eapen et al 2008)
bull Heterogeneity of the fragments in the serum is thought to limit its use (Burch etal 2014)
bull May be affected by use of warfarin (Yang and Grey 2006)
Markers of Bone Resorption
20
Carboxy-terminal telopeptide cross-linked type 1 collagen (CTX)
bull Peptide fragments from the carboxy-terminal end of type 1
collagen produced during osteoclastic resorption
bull Detected in urine or serum using enzyme linked
immunosorbent assay (ELISA)
bull More accurate when monitoring the response to specific
treatments (eg with bisphosphonates) (Burch et al2014) 21
Amino-terminal telopeptide cross-linked type I collagen (NTX)
bull Peptide fragments from the amino terminal end of
type 1 collagen produced during osteoclastic
resorption
bull Detected in the urine or serum with competitive
inhibition ELISA or chemiluminescence assay
bull It is non-invasive and may be preferred by patients
(Yang and Grey 2006) 22
Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25

Summary as presented
2
Outline
bull Bone definition
bull Structure and functions of bone
bull Formation and resorption of bone
bull Osteoporosis
bull Diagnostic bone markers in osteoporosis
bull Conclusion
bull Selected references 3
Bone definition
A specialized mineralized connective tissue that consists of a mainly organic collagen matrix and a mineral phase together with bone cells (Vasikaran et al 2008)
4
Bone Structure and Function
Bone
Structure
Extracellular matrix
Cellular constituents
Function
Mechanical Synthetic Metabolic
5
Bone Formation and Resorption
bull Metabolically active and constantly being repaired and remodelled
throughout an individuals lifetime
bull Formation involves actively synthesizing osteoblasts while its
resorption involves multinucleated osteoclasts (Vasikaran et al
2008)
bull Osteoporosis occurs when bone resorption is the more active
(Wheater et al 2013) 6
Osteoporosis
bull A systemic skeletal disease characterized by low bone mass and
micro-architectural deterioration of bone tissue with a
consequent increase in bone fragility and susceptibility to
fractures (Burch et al 2014)
bull Risk factors Age hormonal disturbances genetic lifestyle drugs
and some diseases like hyperthyroidism
bull Results in substantial morbidity and an estimated health cost gt
$14billion annually (McCormick 2007)
7
Osteoporosis Epidemiology
bull Prevalence 30 in women living in developed countries
bull Age and Sex 3 in 5 women gt 65 years and 1 in 5 men gt 75
years
bull Race predominant among Caucasians and Asians
bull Genetics studies suggest a significant genetic component
bull Geography most common in developed countries
(McCormick 2007)
Osteoporotic Fractures Comparison with Other Diseases
184 300 750 000
vertebral
250 000 other sites
250 000 forearm
250 000 hip
0
500
1000
1500
2000
Osteoporotic Fractures
Heart Attack
Stroke Breast Cancer
An
nu
al in
cid
ence
x 1
00
0
1 500 000
Annual incidence all ages
513 000
annual estimate women 29+
228 000
annual estimate women 30+
(Vasikaran 2006)
9
Vertebrae
Hip
Wrist
50 60 70 80
40
30
20
10
Age (Years)
An
nu
al in
cid
en
ce p
er
10
00
w
om
en
Incidence of Osteoporotic Fractures in European Women
(Burch et al 2014)
Diagnostic Tools in Osteoporosis
bull Bone Mineral Density (BMD) scanning using dual-energy X-
ray absorptiometry (DXA) is the WHO standard for
diagnosis of osteoporosis (McCormick 2007)
bull DXA measures the amount of bone mineral in bone tissue
bull BMD is used in cliinical medicine as an indirect indicator of
osteoporosis
bull Poor sensitivity of DXA means that potential fractures will
be missed if it is used alone (Wheater et al 2013)
11
Limitations of BMD measurements in the Diagnosis of Osteoporosis
bull Changes in bone metabolism after therapy are detectable
only after about 2 years
bull Limited access to the technology
bull It is relatively expensive
bull The exposure to radiation although small is best avoided
bull Bone biomarkers offer an alternative monitoring strategy
(Burch et al 2014)
12
Diagnostic Bone Markers in Osteoporosis
bull Specifically derived biomarkers that reflect both bone formation by osteoblasts and resorption by osteoclasts
bull Include both enzymes and peptides derived from cellular and non-cellular compartments of bone
bull May be measured in synovial fluid blood or urine
bull Techniques for their measurements are abundant
bull Classified as bone formation and resorption markers (Seibel 2005) 13
Diagnostic Bone Markers in Osteoporosis
bull Detect metabolic changes in bone after about 3-6 months
(McCormick 2007)
bull Relatively cheap compared with DXA (Wheater et al 2013)
bull No exposure to radiation
bull Helpful tools in the diagnostic prognostic and therapeutic
assessment of osteoporosis
14
Diagnostic Bone Markers in Osteoporosis
15
Markers of Bone Formation
16
Bone Alkaline Phosphatase (BALP)
bull Total alkaline phosphatase has several isoforms in serum
(Liver bone placental intestine spleen and kidney)
bull 40ndash50 of the total alkaline phosphatase activity arises from
the bone as a result of osteoblast activity (Siebel 2005)
bull Residual low cross-reactivity (16) with liver ALP limits its use
in patients with liver disease (Yang and Grey 2006) 17
Bone Alkaline Phosphatase (BALP) Assays
bull Immunoradiometric assay (IRMA)
bull Enzyme-linked immunosorbent assay (ELISA)
bull Ease of measurement cost efficiency and higher
specificity in detecting small changes makes BALP a
good marker for bone formation (Burch et al
2008) 18
Osteocalcin
bull A non collagenous matrix protein
bull Detected using enzyme linked immunosorbent assays (ELISA) or radioimmunoassays (RIA)
bull It is tissue specific widely available (Eapen et al 2008)
bull Heterogeneity of the fragments in the serum is thought to limit its use (Burch etal 2014)
bull May be affected by use of warfarin (Yang and Grey 2006)
Markers of Bone Resorption
20
Carboxy-terminal telopeptide cross-linked type 1 collagen (CTX)
bull Peptide fragments from the carboxy-terminal end of type 1
collagen produced during osteoclastic resorption
bull Detected in urine or serum using enzyme linked
immunosorbent assay (ELISA)
bull More accurate when monitoring the response to specific
treatments (eg with bisphosphonates) (Burch et al2014) 21
Amino-terminal telopeptide cross-linked type I collagen (NTX)
bull Peptide fragments from the amino terminal end of
type 1 collagen produced during osteoclastic
resorption
bull Detected in the urine or serum with competitive
inhibition ELISA or chemiluminescence assay
bull It is non-invasive and may be preferred by patients
(Yang and Grey 2006) 22
Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25

Outline
bull Bone definition
bull Structure and functions of bone
bull Formation and resorption of bone
bull Osteoporosis
bull Diagnostic bone markers in osteoporosis
bull Conclusion
bull Selected references 3
Bone definition
A specialized mineralized connective tissue that consists of a mainly organic collagen matrix and a mineral phase together with bone cells (Vasikaran et al 2008)
4
Bone Structure and Function
Bone
Structure
Extracellular matrix
Cellular constituents
Function
Mechanical Synthetic Metabolic
5
Bone Formation and Resorption
bull Metabolically active and constantly being repaired and remodelled
throughout an individuals lifetime
bull Formation involves actively synthesizing osteoblasts while its
resorption involves multinucleated osteoclasts (Vasikaran et al
2008)
bull Osteoporosis occurs when bone resorption is the more active
(Wheater et al 2013) 6
Osteoporosis
bull A systemic skeletal disease characterized by low bone mass and
micro-architectural deterioration of bone tissue with a
consequent increase in bone fragility and susceptibility to
fractures (Burch et al 2014)
bull Risk factors Age hormonal disturbances genetic lifestyle drugs
and some diseases like hyperthyroidism
bull Results in substantial morbidity and an estimated health cost gt
$14billion annually (McCormick 2007)
7
Osteoporosis Epidemiology
bull Prevalence 30 in women living in developed countries
bull Age and Sex 3 in 5 women gt 65 years and 1 in 5 men gt 75
years
bull Race predominant among Caucasians and Asians
bull Genetics studies suggest a significant genetic component
bull Geography most common in developed countries
(McCormick 2007)
Osteoporotic Fractures Comparison with Other Diseases
184 300 750 000
vertebral
250 000 other sites
250 000 forearm
250 000 hip
0
500
1000
1500
2000
Osteoporotic Fractures
Heart Attack
Stroke Breast Cancer
An
nu
al in
cid
ence
x 1
00
0
1 500 000
Annual incidence all ages
513 000
annual estimate women 29+
228 000
annual estimate women 30+
(Vasikaran 2006)
9
Vertebrae
Hip
Wrist
50 60 70 80
40
30
20
10
Age (Years)
An
nu
al in
cid
en
ce p
er
10
00
w
om
en
Incidence of Osteoporotic Fractures in European Women
(Burch et al 2014)
Diagnostic Tools in Osteoporosis
bull Bone Mineral Density (BMD) scanning using dual-energy X-
ray absorptiometry (DXA) is the WHO standard for
diagnosis of osteoporosis (McCormick 2007)
bull DXA measures the amount of bone mineral in bone tissue
bull BMD is used in cliinical medicine as an indirect indicator of
osteoporosis
bull Poor sensitivity of DXA means that potential fractures will
be missed if it is used alone (Wheater et al 2013)
11
Limitations of BMD measurements in the Diagnosis of Osteoporosis
bull Changes in bone metabolism after therapy are detectable
only after about 2 years
bull Limited access to the technology
bull It is relatively expensive
bull The exposure to radiation although small is best avoided
bull Bone biomarkers offer an alternative monitoring strategy
(Burch et al 2014)
12
Diagnostic Bone Markers in Osteoporosis
bull Specifically derived biomarkers that reflect both bone formation by osteoblasts and resorption by osteoclasts
bull Include both enzymes and peptides derived from cellular and non-cellular compartments of bone
bull May be measured in synovial fluid blood or urine
bull Techniques for their measurements are abundant
bull Classified as bone formation and resorption markers (Seibel 2005) 13
Diagnostic Bone Markers in Osteoporosis
bull Detect metabolic changes in bone after about 3-6 months
(McCormick 2007)
bull Relatively cheap compared with DXA (Wheater et al 2013)
bull No exposure to radiation
bull Helpful tools in the diagnostic prognostic and therapeutic
assessment of osteoporosis
14
Diagnostic Bone Markers in Osteoporosis
15
Markers of Bone Formation
16
Bone Alkaline Phosphatase (BALP)
bull Total alkaline phosphatase has several isoforms in serum
(Liver bone placental intestine spleen and kidney)
bull 40ndash50 of the total alkaline phosphatase activity arises from
the bone as a result of osteoblast activity (Siebel 2005)
bull Residual low cross-reactivity (16) with liver ALP limits its use
in patients with liver disease (Yang and Grey 2006) 17
Bone Alkaline Phosphatase (BALP) Assays
bull Immunoradiometric assay (IRMA)
bull Enzyme-linked immunosorbent assay (ELISA)
bull Ease of measurement cost efficiency and higher
specificity in detecting small changes makes BALP a
good marker for bone formation (Burch et al
2008) 18
Osteocalcin
bull A non collagenous matrix protein
bull Detected using enzyme linked immunosorbent assays (ELISA) or radioimmunoassays (RIA)
bull It is tissue specific widely available (Eapen et al 2008)
bull Heterogeneity of the fragments in the serum is thought to limit its use (Burch etal 2014)
bull May be affected by use of warfarin (Yang and Grey 2006)
Markers of Bone Resorption
20
Carboxy-terminal telopeptide cross-linked type 1 collagen (CTX)
bull Peptide fragments from the carboxy-terminal end of type 1
collagen produced during osteoclastic resorption
bull Detected in urine or serum using enzyme linked
immunosorbent assay (ELISA)
bull More accurate when monitoring the response to specific
treatments (eg with bisphosphonates) (Burch et al2014) 21
Amino-terminal telopeptide cross-linked type I collagen (NTX)
bull Peptide fragments from the amino terminal end of
type 1 collagen produced during osteoclastic
resorption
bull Detected in the urine or serum with competitive
inhibition ELISA or chemiluminescence assay
bull It is non-invasive and may be preferred by patients
(Yang and Grey 2006) 22
Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25
Bone definition
A specialized mineralized connective tissue that consists of a mainly organic collagen matrix and a mineral phase together with bone cells (Vasikaran et al 2008)
4
Bone Structure and Function
Bone
Structure
Extracellular matrix
Cellular constituents
Function
Mechanical Synthetic Metabolic
5
Bone Formation and Resorption
bull Metabolically active and constantly being repaired and remodelled
throughout an individuals lifetime
bull Formation involves actively synthesizing osteoblasts while its
resorption involves multinucleated osteoclasts (Vasikaran et al
2008)
bull Osteoporosis occurs when bone resorption is the more active
(Wheater et al 2013) 6
Osteoporosis
bull A systemic skeletal disease characterized by low bone mass and
micro-architectural deterioration of bone tissue with a
consequent increase in bone fragility and susceptibility to
fractures (Burch et al 2014)
bull Risk factors Age hormonal disturbances genetic lifestyle drugs
and some diseases like hyperthyroidism
bull Results in substantial morbidity and an estimated health cost gt
$14billion annually (McCormick 2007)
7
Osteoporosis Epidemiology
bull Prevalence 30 in women living in developed countries
bull Age and Sex 3 in 5 women gt 65 years and 1 in 5 men gt 75
years
bull Race predominant among Caucasians and Asians
bull Genetics studies suggest a significant genetic component
bull Geography most common in developed countries
(McCormick 2007)
Osteoporotic Fractures Comparison with Other Diseases
184 300 750 000
vertebral
250 000 other sites
250 000 forearm
250 000 hip
0
500
1000
1500
2000
Osteoporotic Fractures
Heart Attack
Stroke Breast Cancer
An
nu
al in
cid
ence
x 1
00
0
1 500 000
Annual incidence all ages
513 000
annual estimate women 29+
228 000
annual estimate women 30+
(Vasikaran 2006)
9
Vertebrae
Hip
Wrist
50 60 70 80
40
30
20
10
Age (Years)
An
nu
al in
cid
en
ce p
er
10
00
w
om
en
Incidence of Osteoporotic Fractures in European Women
(Burch et al 2014)
Diagnostic Tools in Osteoporosis
bull Bone Mineral Density (BMD) scanning using dual-energy X-
ray absorptiometry (DXA) is the WHO standard for
diagnosis of osteoporosis (McCormick 2007)
bull DXA measures the amount of bone mineral in bone tissue
bull BMD is used in cliinical medicine as an indirect indicator of
osteoporosis
bull Poor sensitivity of DXA means that potential fractures will
be missed if it is used alone (Wheater et al 2013)
11
Limitations of BMD measurements in the Diagnosis of Osteoporosis
bull Changes in bone metabolism after therapy are detectable
only after about 2 years
bull Limited access to the technology
bull It is relatively expensive
bull The exposure to radiation although small is best avoided
bull Bone biomarkers offer an alternative monitoring strategy
(Burch et al 2014)
12
Diagnostic Bone Markers in Osteoporosis
bull Specifically derived biomarkers that reflect both bone formation by osteoblasts and resorption by osteoclasts
bull Include both enzymes and peptides derived from cellular and non-cellular compartments of bone
bull May be measured in synovial fluid blood or urine
bull Techniques for their measurements are abundant
bull Classified as bone formation and resorption markers (Seibel 2005) 13
Diagnostic Bone Markers in Osteoporosis
bull Detect metabolic changes in bone after about 3-6 months
(McCormick 2007)
bull Relatively cheap compared with DXA (Wheater et al 2013)
bull No exposure to radiation
bull Helpful tools in the diagnostic prognostic and therapeutic
assessment of osteoporosis
14
Diagnostic Bone Markers in Osteoporosis
15
Markers of Bone Formation
16
Bone Alkaline Phosphatase (BALP)
bull Total alkaline phosphatase has several isoforms in serum
(Liver bone placental intestine spleen and kidney)
bull 40ndash50 of the total alkaline phosphatase activity arises from
the bone as a result of osteoblast activity (Siebel 2005)
bull Residual low cross-reactivity (16) with liver ALP limits its use
in patients with liver disease (Yang and Grey 2006) 17
Bone Alkaline Phosphatase (BALP) Assays
bull Immunoradiometric assay (IRMA)
bull Enzyme-linked immunosorbent assay (ELISA)
bull Ease of measurement cost efficiency and higher
specificity in detecting small changes makes BALP a
good marker for bone formation (Burch et al
2008) 18
Osteocalcin
bull A non collagenous matrix protein
bull Detected using enzyme linked immunosorbent assays (ELISA) or radioimmunoassays (RIA)
bull It is tissue specific widely available (Eapen et al 2008)
bull Heterogeneity of the fragments in the serum is thought to limit its use (Burch etal 2014)
bull May be affected by use of warfarin (Yang and Grey 2006)
Markers of Bone Resorption
20
Carboxy-terminal telopeptide cross-linked type 1 collagen (CTX)
bull Peptide fragments from the carboxy-terminal end of type 1
collagen produced during osteoclastic resorption
bull Detected in urine or serum using enzyme linked
immunosorbent assay (ELISA)
bull More accurate when monitoring the response to specific
treatments (eg with bisphosphonates) (Burch et al2014) 21
Amino-terminal telopeptide cross-linked type I collagen (NTX)
bull Peptide fragments from the amino terminal end of
type 1 collagen produced during osteoclastic
resorption
bull Detected in the urine or serum with competitive
inhibition ELISA or chemiluminescence assay
bull It is non-invasive and may be preferred by patients
(Yang and Grey 2006) 22
Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25

Bone Structure and Function
Bone
Structure
Extracellular matrix
Cellular constituents
Function
Mechanical Synthetic Metabolic
5
Bone Formation and Resorption
bull Metabolically active and constantly being repaired and remodelled
throughout an individuals lifetime
bull Formation involves actively synthesizing osteoblasts while its
resorption involves multinucleated osteoclasts (Vasikaran et al
2008)
bull Osteoporosis occurs when bone resorption is the more active
(Wheater et al 2013) 6
Osteoporosis
bull A systemic skeletal disease characterized by low bone mass and
micro-architectural deterioration of bone tissue with a
consequent increase in bone fragility and susceptibility to
fractures (Burch et al 2014)
bull Risk factors Age hormonal disturbances genetic lifestyle drugs
and some diseases like hyperthyroidism
bull Results in substantial morbidity and an estimated health cost gt
$14billion annually (McCormick 2007)
7
Osteoporosis Epidemiology
bull Prevalence 30 in women living in developed countries
bull Age and Sex 3 in 5 women gt 65 years and 1 in 5 men gt 75
years
bull Race predominant among Caucasians and Asians
bull Genetics studies suggest a significant genetic component
bull Geography most common in developed countries
(McCormick 2007)
Osteoporotic Fractures Comparison with Other Diseases
184 300 750 000
vertebral
250 000 other sites
250 000 forearm
250 000 hip
0
500
1000
1500
2000
Osteoporotic Fractures
Heart Attack
Stroke Breast Cancer
An
nu
al in
cid
ence
x 1
00
0
1 500 000
Annual incidence all ages
513 000
annual estimate women 29+
228 000
annual estimate women 30+
(Vasikaran 2006)
9
Vertebrae
Hip
Wrist
50 60 70 80
40
30
20
10
Age (Years)
An
nu
al in
cid
en
ce p
er
10
00
w
om
en
Incidence of Osteoporotic Fractures in European Women
(Burch et al 2014)
Diagnostic Tools in Osteoporosis
bull Bone Mineral Density (BMD) scanning using dual-energy X-
ray absorptiometry (DXA) is the WHO standard for
diagnosis of osteoporosis (McCormick 2007)
bull DXA measures the amount of bone mineral in bone tissue
bull BMD is used in cliinical medicine as an indirect indicator of
osteoporosis
bull Poor sensitivity of DXA means that potential fractures will
be missed if it is used alone (Wheater et al 2013)
11
Limitations of BMD measurements in the Diagnosis of Osteoporosis
bull Changes in bone metabolism after therapy are detectable
only after about 2 years
bull Limited access to the technology
bull It is relatively expensive
bull The exposure to radiation although small is best avoided
bull Bone biomarkers offer an alternative monitoring strategy
(Burch et al 2014)
12
Diagnostic Bone Markers in Osteoporosis
bull Specifically derived biomarkers that reflect both bone formation by osteoblasts and resorption by osteoclasts
bull Include both enzymes and peptides derived from cellular and non-cellular compartments of bone
bull May be measured in synovial fluid blood or urine
bull Techniques for their measurements are abundant
bull Classified as bone formation and resorption markers (Seibel 2005) 13
Diagnostic Bone Markers in Osteoporosis
bull Detect metabolic changes in bone after about 3-6 months
(McCormick 2007)
bull Relatively cheap compared with DXA (Wheater et al 2013)
bull No exposure to radiation
bull Helpful tools in the diagnostic prognostic and therapeutic
assessment of osteoporosis
14
Diagnostic Bone Markers in Osteoporosis
15
Markers of Bone Formation
16
Bone Alkaline Phosphatase (BALP)
bull Total alkaline phosphatase has several isoforms in serum
(Liver bone placental intestine spleen and kidney)
bull 40ndash50 of the total alkaline phosphatase activity arises from
the bone as a result of osteoblast activity (Siebel 2005)
bull Residual low cross-reactivity (16) with liver ALP limits its use
in patients with liver disease (Yang and Grey 2006) 17
Bone Alkaline Phosphatase (BALP) Assays
bull Immunoradiometric assay (IRMA)
bull Enzyme-linked immunosorbent assay (ELISA)
bull Ease of measurement cost efficiency and higher
specificity in detecting small changes makes BALP a
good marker for bone formation (Burch et al
2008) 18
Osteocalcin
bull A non collagenous matrix protein
bull Detected using enzyme linked immunosorbent assays (ELISA) or radioimmunoassays (RIA)
bull It is tissue specific widely available (Eapen et al 2008)
bull Heterogeneity of the fragments in the serum is thought to limit its use (Burch etal 2014)
bull May be affected by use of warfarin (Yang and Grey 2006)
Markers of Bone Resorption
20
Carboxy-terminal telopeptide cross-linked type 1 collagen (CTX)
bull Peptide fragments from the carboxy-terminal end of type 1
collagen produced during osteoclastic resorption
bull Detected in urine or serum using enzyme linked
immunosorbent assay (ELISA)
bull More accurate when monitoring the response to specific
treatments (eg with bisphosphonates) (Burch et al2014) 21
Amino-terminal telopeptide cross-linked type I collagen (NTX)
bull Peptide fragments from the amino terminal end of
type 1 collagen produced during osteoclastic
resorption
bull Detected in the urine or serum with competitive
inhibition ELISA or chemiluminescence assay
bull It is non-invasive and may be preferred by patients
(Yang and Grey 2006) 22
Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25
Bone Formation and Resorption
bull Metabolically active and constantly being repaired and remodelled
throughout an individuals lifetime
bull Formation involves actively synthesizing osteoblasts while its
resorption involves multinucleated osteoclasts (Vasikaran et al
2008)
bull Osteoporosis occurs when bone resorption is the more active
(Wheater et al 2013) 6
Osteoporosis
bull A systemic skeletal disease characterized by low bone mass and
micro-architectural deterioration of bone tissue with a
consequent increase in bone fragility and susceptibility to
fractures (Burch et al 2014)
bull Risk factors Age hormonal disturbances genetic lifestyle drugs
and some diseases like hyperthyroidism
bull Results in substantial morbidity and an estimated health cost gt
$14billion annually (McCormick 2007)
7
Osteoporosis Epidemiology
bull Prevalence 30 in women living in developed countries
bull Age and Sex 3 in 5 women gt 65 years and 1 in 5 men gt 75
years
bull Race predominant among Caucasians and Asians
bull Genetics studies suggest a significant genetic component
bull Geography most common in developed countries
(McCormick 2007)
Osteoporotic Fractures Comparison with Other Diseases
184 300 750 000
vertebral
250 000 other sites
250 000 forearm
250 000 hip
0
500
1000
1500
2000
Osteoporotic Fractures
Heart Attack
Stroke Breast Cancer
An
nu
al in
cid
ence
x 1
00
0
1 500 000
Annual incidence all ages
513 000
annual estimate women 29+
228 000
annual estimate women 30+
(Vasikaran 2006)
9
Vertebrae
Hip
Wrist
50 60 70 80
40
30
20
10
Age (Years)
An
nu
al in
cid
en
ce p
er
10
00
w
om
en
Incidence of Osteoporotic Fractures in European Women
(Burch et al 2014)
Diagnostic Tools in Osteoporosis
bull Bone Mineral Density (BMD) scanning using dual-energy X-
ray absorptiometry (DXA) is the WHO standard for
diagnosis of osteoporosis (McCormick 2007)
bull DXA measures the amount of bone mineral in bone tissue
bull BMD is used in cliinical medicine as an indirect indicator of
osteoporosis
bull Poor sensitivity of DXA means that potential fractures will
be missed if it is used alone (Wheater et al 2013)
11
Limitations of BMD measurements in the Diagnosis of Osteoporosis
bull Changes in bone metabolism after therapy are detectable
only after about 2 years
bull Limited access to the technology
bull It is relatively expensive
bull The exposure to radiation although small is best avoided
bull Bone biomarkers offer an alternative monitoring strategy
(Burch et al 2014)
12
Diagnostic Bone Markers in Osteoporosis
bull Specifically derived biomarkers that reflect both bone formation by osteoblasts and resorption by osteoclasts
bull Include both enzymes and peptides derived from cellular and non-cellular compartments of bone
bull May be measured in synovial fluid blood or urine
bull Techniques for their measurements are abundant
bull Classified as bone formation and resorption markers (Seibel 2005) 13
Diagnostic Bone Markers in Osteoporosis
bull Detect metabolic changes in bone after about 3-6 months
(McCormick 2007)
bull Relatively cheap compared with DXA (Wheater et al 2013)
bull No exposure to radiation
bull Helpful tools in the diagnostic prognostic and therapeutic
assessment of osteoporosis
14
Diagnostic Bone Markers in Osteoporosis
15
Markers of Bone Formation
16
Bone Alkaline Phosphatase (BALP)
bull Total alkaline phosphatase has several isoforms in serum
(Liver bone placental intestine spleen and kidney)
bull 40ndash50 of the total alkaline phosphatase activity arises from
the bone as a result of osteoblast activity (Siebel 2005)
bull Residual low cross-reactivity (16) with liver ALP limits its use
in patients with liver disease (Yang and Grey 2006) 17
Bone Alkaline Phosphatase (BALP) Assays
bull Immunoradiometric assay (IRMA)
bull Enzyme-linked immunosorbent assay (ELISA)
bull Ease of measurement cost efficiency and higher
specificity in detecting small changes makes BALP a
good marker for bone formation (Burch et al
2008) 18
Osteocalcin
bull A non collagenous matrix protein
bull Detected using enzyme linked immunosorbent assays (ELISA) or radioimmunoassays (RIA)
bull It is tissue specific widely available (Eapen et al 2008)
bull Heterogeneity of the fragments in the serum is thought to limit its use (Burch etal 2014)
bull May be affected by use of warfarin (Yang and Grey 2006)
Markers of Bone Resorption
20
Carboxy-terminal telopeptide cross-linked type 1 collagen (CTX)
bull Peptide fragments from the carboxy-terminal end of type 1
collagen produced during osteoclastic resorption
bull Detected in urine or serum using enzyme linked
immunosorbent assay (ELISA)
bull More accurate when monitoring the response to specific
treatments (eg with bisphosphonates) (Burch et al2014) 21
Amino-terminal telopeptide cross-linked type I collagen (NTX)
bull Peptide fragments from the amino terminal end of
type 1 collagen produced during osteoclastic
resorption
bull Detected in the urine or serum with competitive
inhibition ELISA or chemiluminescence assay
bull It is non-invasive and may be preferred by patients
(Yang and Grey 2006) 22
Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25
Osteoporosis
bull A systemic skeletal disease characterized by low bone mass and
micro-architectural deterioration of bone tissue with a
consequent increase in bone fragility and susceptibility to
fractures (Burch et al 2014)
bull Risk factors Age hormonal disturbances genetic lifestyle drugs
and some diseases like hyperthyroidism
bull Results in substantial morbidity and an estimated health cost gt
$14billion annually (McCormick 2007)
7
Osteoporosis Epidemiology
bull Prevalence 30 in women living in developed countries
bull Age and Sex 3 in 5 women gt 65 years and 1 in 5 men gt 75
years
bull Race predominant among Caucasians and Asians
bull Genetics studies suggest a significant genetic component
bull Geography most common in developed countries
(McCormick 2007)
Osteoporotic Fractures Comparison with Other Diseases
184 300 750 000
vertebral
250 000 other sites
250 000 forearm
250 000 hip
0
500
1000
1500
2000
Osteoporotic Fractures
Heart Attack
Stroke Breast Cancer
An
nu
al in
cid
ence
x 1
00
0
1 500 000
Annual incidence all ages
513 000
annual estimate women 29+
228 000
annual estimate women 30+
(Vasikaran 2006)
9
Vertebrae
Hip
Wrist
50 60 70 80
40
30
20
10
Age (Years)
An
nu
al in
cid
en
ce p
er
10
00
w
om
en
Incidence of Osteoporotic Fractures in European Women
(Burch et al 2014)
Diagnostic Tools in Osteoporosis
bull Bone Mineral Density (BMD) scanning using dual-energy X-
ray absorptiometry (DXA) is the WHO standard for
diagnosis of osteoporosis (McCormick 2007)
bull DXA measures the amount of bone mineral in bone tissue
bull BMD is used in cliinical medicine as an indirect indicator of
osteoporosis
bull Poor sensitivity of DXA means that potential fractures will
be missed if it is used alone (Wheater et al 2013)
11
Limitations of BMD measurements in the Diagnosis of Osteoporosis
bull Changes in bone metabolism after therapy are detectable
only after about 2 years
bull Limited access to the technology
bull It is relatively expensive
bull The exposure to radiation although small is best avoided
bull Bone biomarkers offer an alternative monitoring strategy
(Burch et al 2014)
12
Diagnostic Bone Markers in Osteoporosis
bull Specifically derived biomarkers that reflect both bone formation by osteoblasts and resorption by osteoclasts
bull Include both enzymes and peptides derived from cellular and non-cellular compartments of bone
bull May be measured in synovial fluid blood or urine
bull Techniques for their measurements are abundant
bull Classified as bone formation and resorption markers (Seibel 2005) 13
Diagnostic Bone Markers in Osteoporosis
bull Detect metabolic changes in bone after about 3-6 months
(McCormick 2007)
bull Relatively cheap compared with DXA (Wheater et al 2013)
bull No exposure to radiation
bull Helpful tools in the diagnostic prognostic and therapeutic
assessment of osteoporosis
14
Diagnostic Bone Markers in Osteoporosis
15
Markers of Bone Formation
16
Bone Alkaline Phosphatase (BALP)
bull Total alkaline phosphatase has several isoforms in serum
(Liver bone placental intestine spleen and kidney)
bull 40ndash50 of the total alkaline phosphatase activity arises from
the bone as a result of osteoblast activity (Siebel 2005)
bull Residual low cross-reactivity (16) with liver ALP limits its use
in patients with liver disease (Yang and Grey 2006) 17
Bone Alkaline Phosphatase (BALP) Assays
bull Immunoradiometric assay (IRMA)
bull Enzyme-linked immunosorbent assay (ELISA)
bull Ease of measurement cost efficiency and higher
specificity in detecting small changes makes BALP a
good marker for bone formation (Burch et al
2008) 18
Osteocalcin
bull A non collagenous matrix protein
bull Detected using enzyme linked immunosorbent assays (ELISA) or radioimmunoassays (RIA)
bull It is tissue specific widely available (Eapen et al 2008)
bull Heterogeneity of the fragments in the serum is thought to limit its use (Burch etal 2014)
bull May be affected by use of warfarin (Yang and Grey 2006)
Markers of Bone Resorption
20
Carboxy-terminal telopeptide cross-linked type 1 collagen (CTX)
bull Peptide fragments from the carboxy-terminal end of type 1
collagen produced during osteoclastic resorption
bull Detected in urine or serum using enzyme linked
immunosorbent assay (ELISA)
bull More accurate when monitoring the response to specific
treatments (eg with bisphosphonates) (Burch et al2014) 21
Amino-terminal telopeptide cross-linked type I collagen (NTX)
bull Peptide fragments from the amino terminal end of
type 1 collagen produced during osteoclastic
resorption
bull Detected in the urine or serum with competitive
inhibition ELISA or chemiluminescence assay
bull It is non-invasive and may be preferred by patients
(Yang and Grey 2006) 22
Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25
Osteoporosis Epidemiology
bull Prevalence 30 in women living in developed countries
bull Age and Sex 3 in 5 women gt 65 years and 1 in 5 men gt 75
years
bull Race predominant among Caucasians and Asians
bull Genetics studies suggest a significant genetic component
bull Geography most common in developed countries
(McCormick 2007)
Osteoporotic Fractures Comparison with Other Diseases
184 300 750 000
vertebral
250 000 other sites
250 000 forearm
250 000 hip
0
500
1000
1500
2000
Osteoporotic Fractures
Heart Attack
Stroke Breast Cancer
An
nu
al in
cid
ence
x 1
00
0
1 500 000
Annual incidence all ages
513 000
annual estimate women 29+
228 000
annual estimate women 30+
(Vasikaran 2006)
9
Vertebrae
Hip
Wrist
50 60 70 80
40
30
20
10
Age (Years)
An
nu
al in
cid
en
ce p
er
10
00
w
om
en
Incidence of Osteoporotic Fractures in European Women
(Burch et al 2014)
Diagnostic Tools in Osteoporosis
bull Bone Mineral Density (BMD) scanning using dual-energy X-
ray absorptiometry (DXA) is the WHO standard for
diagnosis of osteoporosis (McCormick 2007)
bull DXA measures the amount of bone mineral in bone tissue
bull BMD is used in cliinical medicine as an indirect indicator of
osteoporosis
bull Poor sensitivity of DXA means that potential fractures will
be missed if it is used alone (Wheater et al 2013)
11
Limitations of BMD measurements in the Diagnosis of Osteoporosis
bull Changes in bone metabolism after therapy are detectable
only after about 2 years
bull Limited access to the technology
bull It is relatively expensive
bull The exposure to radiation although small is best avoided
bull Bone biomarkers offer an alternative monitoring strategy
(Burch et al 2014)
12
Diagnostic Bone Markers in Osteoporosis
bull Specifically derived biomarkers that reflect both bone formation by osteoblasts and resorption by osteoclasts
bull Include both enzymes and peptides derived from cellular and non-cellular compartments of bone
bull May be measured in synovial fluid blood or urine
bull Techniques for their measurements are abundant
bull Classified as bone formation and resorption markers (Seibel 2005) 13
Diagnostic Bone Markers in Osteoporosis
bull Detect metabolic changes in bone after about 3-6 months
(McCormick 2007)
bull Relatively cheap compared with DXA (Wheater et al 2013)
bull No exposure to radiation
bull Helpful tools in the diagnostic prognostic and therapeutic
assessment of osteoporosis
14
Diagnostic Bone Markers in Osteoporosis
15
Markers of Bone Formation
16
Bone Alkaline Phosphatase (BALP)
bull Total alkaline phosphatase has several isoforms in serum
(Liver bone placental intestine spleen and kidney)
bull 40ndash50 of the total alkaline phosphatase activity arises from
the bone as a result of osteoblast activity (Siebel 2005)
bull Residual low cross-reactivity (16) with liver ALP limits its use
in patients with liver disease (Yang and Grey 2006) 17
Bone Alkaline Phosphatase (BALP) Assays
bull Immunoradiometric assay (IRMA)
bull Enzyme-linked immunosorbent assay (ELISA)
bull Ease of measurement cost efficiency and higher
specificity in detecting small changes makes BALP a
good marker for bone formation (Burch et al
2008) 18
Osteocalcin
bull A non collagenous matrix protein
bull Detected using enzyme linked immunosorbent assays (ELISA) or radioimmunoassays (RIA)
bull It is tissue specific widely available (Eapen et al 2008)
bull Heterogeneity of the fragments in the serum is thought to limit its use (Burch etal 2014)
bull May be affected by use of warfarin (Yang and Grey 2006)
Markers of Bone Resorption
20
Carboxy-terminal telopeptide cross-linked type 1 collagen (CTX)
bull Peptide fragments from the carboxy-terminal end of type 1
collagen produced during osteoclastic resorption
bull Detected in urine or serum using enzyme linked
immunosorbent assay (ELISA)
bull More accurate when monitoring the response to specific
treatments (eg with bisphosphonates) (Burch et al2014) 21
Amino-terminal telopeptide cross-linked type I collagen (NTX)
bull Peptide fragments from the amino terminal end of
type 1 collagen produced during osteoclastic
resorption
bull Detected in the urine or serum with competitive
inhibition ELISA or chemiluminescence assay
bull It is non-invasive and may be preferred by patients
(Yang and Grey 2006) 22
Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25
Osteoporotic Fractures Comparison with Other Diseases
184 300 750 000
vertebral
250 000 other sites
250 000 forearm
250 000 hip
0
500
1000
1500
2000
Osteoporotic Fractures
Heart Attack
Stroke Breast Cancer
An
nu
al in
cid
ence
x 1
00
0
1 500 000
Annual incidence all ages
513 000
annual estimate women 29+
228 000
annual estimate women 30+
(Vasikaran 2006)
9
Vertebrae
Hip
Wrist
50 60 70 80
40
30
20
10
Age (Years)
An
nu
al in
cid
en
ce p
er
10
00
w
om
en
Incidence of Osteoporotic Fractures in European Women
(Burch et al 2014)
Diagnostic Tools in Osteoporosis
bull Bone Mineral Density (BMD) scanning using dual-energy X-
ray absorptiometry (DXA) is the WHO standard for
diagnosis of osteoporosis (McCormick 2007)
bull DXA measures the amount of bone mineral in bone tissue
bull BMD is used in cliinical medicine as an indirect indicator of
osteoporosis
bull Poor sensitivity of DXA means that potential fractures will
be missed if it is used alone (Wheater et al 2013)
11
Limitations of BMD measurements in the Diagnosis of Osteoporosis
bull Changes in bone metabolism after therapy are detectable
only after about 2 years
bull Limited access to the technology
bull It is relatively expensive
bull The exposure to radiation although small is best avoided
bull Bone biomarkers offer an alternative monitoring strategy
(Burch et al 2014)
12
Diagnostic Bone Markers in Osteoporosis
bull Specifically derived biomarkers that reflect both bone formation by osteoblasts and resorption by osteoclasts
bull Include both enzymes and peptides derived from cellular and non-cellular compartments of bone
bull May be measured in synovial fluid blood or urine
bull Techniques for their measurements are abundant
bull Classified as bone formation and resorption markers (Seibel 2005) 13
Diagnostic Bone Markers in Osteoporosis
bull Detect metabolic changes in bone after about 3-6 months
(McCormick 2007)
bull Relatively cheap compared with DXA (Wheater et al 2013)
bull No exposure to radiation
bull Helpful tools in the diagnostic prognostic and therapeutic
assessment of osteoporosis
14
Diagnostic Bone Markers in Osteoporosis
15
Markers of Bone Formation
16
Bone Alkaline Phosphatase (BALP)
bull Total alkaline phosphatase has several isoforms in serum
(Liver bone placental intestine spleen and kidney)
bull 40ndash50 of the total alkaline phosphatase activity arises from
the bone as a result of osteoblast activity (Siebel 2005)
bull Residual low cross-reactivity (16) with liver ALP limits its use
in patients with liver disease (Yang and Grey 2006) 17
Bone Alkaline Phosphatase (BALP) Assays
bull Immunoradiometric assay (IRMA)
bull Enzyme-linked immunosorbent assay (ELISA)
bull Ease of measurement cost efficiency and higher
specificity in detecting small changes makes BALP a
good marker for bone formation (Burch et al
2008) 18
Osteocalcin
bull A non collagenous matrix protein
bull Detected using enzyme linked immunosorbent assays (ELISA) or radioimmunoassays (RIA)
bull It is tissue specific widely available (Eapen et al 2008)
bull Heterogeneity of the fragments in the serum is thought to limit its use (Burch etal 2014)
bull May be affected by use of warfarin (Yang and Grey 2006)
Markers of Bone Resorption
20
Carboxy-terminal telopeptide cross-linked type 1 collagen (CTX)
bull Peptide fragments from the carboxy-terminal end of type 1
collagen produced during osteoclastic resorption
bull Detected in urine or serum using enzyme linked
immunosorbent assay (ELISA)
bull More accurate when monitoring the response to specific
treatments (eg with bisphosphonates) (Burch et al2014) 21
Amino-terminal telopeptide cross-linked type I collagen (NTX)
bull Peptide fragments from the amino terminal end of
type 1 collagen produced during osteoclastic
resorption
bull Detected in the urine or serum with competitive
inhibition ELISA or chemiluminescence assay
bull It is non-invasive and may be preferred by patients
(Yang and Grey 2006) 22
Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25

Vertebrae
Hip
Wrist
50 60 70 80
40
30
20
10
Age (Years)
An
nu
al in
cid
en
ce p
er
10
00
w
om
en
Incidence of Osteoporotic Fractures in European Women
(Burch et al 2014)
Diagnostic Tools in Osteoporosis
bull Bone Mineral Density (BMD) scanning using dual-energy X-
ray absorptiometry (DXA) is the WHO standard for
diagnosis of osteoporosis (McCormick 2007)
bull DXA measures the amount of bone mineral in bone tissue
bull BMD is used in cliinical medicine as an indirect indicator of
osteoporosis
bull Poor sensitivity of DXA means that potential fractures will
be missed if it is used alone (Wheater et al 2013)
11
Limitations of BMD measurements in the Diagnosis of Osteoporosis
bull Changes in bone metabolism after therapy are detectable
only after about 2 years
bull Limited access to the technology
bull It is relatively expensive
bull The exposure to radiation although small is best avoided
bull Bone biomarkers offer an alternative monitoring strategy
(Burch et al 2014)
12
Diagnostic Bone Markers in Osteoporosis
bull Specifically derived biomarkers that reflect both bone formation by osteoblasts and resorption by osteoclasts
bull Include both enzymes and peptides derived from cellular and non-cellular compartments of bone
bull May be measured in synovial fluid blood or urine
bull Techniques for their measurements are abundant
bull Classified as bone formation and resorption markers (Seibel 2005) 13
Diagnostic Bone Markers in Osteoporosis
bull Detect metabolic changes in bone after about 3-6 months
(McCormick 2007)
bull Relatively cheap compared with DXA (Wheater et al 2013)
bull No exposure to radiation
bull Helpful tools in the diagnostic prognostic and therapeutic
assessment of osteoporosis
14
Diagnostic Bone Markers in Osteoporosis
15
Markers of Bone Formation
16
Bone Alkaline Phosphatase (BALP)
bull Total alkaline phosphatase has several isoforms in serum
(Liver bone placental intestine spleen and kidney)
bull 40ndash50 of the total alkaline phosphatase activity arises from
the bone as a result of osteoblast activity (Siebel 2005)
bull Residual low cross-reactivity (16) with liver ALP limits its use
in patients with liver disease (Yang and Grey 2006) 17
Bone Alkaline Phosphatase (BALP) Assays
bull Immunoradiometric assay (IRMA)
bull Enzyme-linked immunosorbent assay (ELISA)
bull Ease of measurement cost efficiency and higher
specificity in detecting small changes makes BALP a
good marker for bone formation (Burch et al
2008) 18
Osteocalcin
bull A non collagenous matrix protein
bull Detected using enzyme linked immunosorbent assays (ELISA) or radioimmunoassays (RIA)
bull It is tissue specific widely available (Eapen et al 2008)
bull Heterogeneity of the fragments in the serum is thought to limit its use (Burch etal 2014)
bull May be affected by use of warfarin (Yang and Grey 2006)
Markers of Bone Resorption
20
Carboxy-terminal telopeptide cross-linked type 1 collagen (CTX)
bull Peptide fragments from the carboxy-terminal end of type 1
collagen produced during osteoclastic resorption
bull Detected in urine or serum using enzyme linked
immunosorbent assay (ELISA)
bull More accurate when monitoring the response to specific
treatments (eg with bisphosphonates) (Burch et al2014) 21
Amino-terminal telopeptide cross-linked type I collagen (NTX)
bull Peptide fragments from the amino terminal end of
type 1 collagen produced during osteoclastic
resorption
bull Detected in the urine or serum with competitive
inhibition ELISA or chemiluminescence assay
bull It is non-invasive and may be preferred by patients
(Yang and Grey 2006) 22
Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25

Diagnostic Tools in Osteoporosis
bull Bone Mineral Density (BMD) scanning using dual-energy X-
ray absorptiometry (DXA) is the WHO standard for
diagnosis of osteoporosis (McCormick 2007)
bull DXA measures the amount of bone mineral in bone tissue
bull BMD is used in cliinical medicine as an indirect indicator of
osteoporosis
bull Poor sensitivity of DXA means that potential fractures will
be missed if it is used alone (Wheater et al 2013)
11
Limitations of BMD measurements in the Diagnosis of Osteoporosis
bull Changes in bone metabolism after therapy are detectable
only after about 2 years
bull Limited access to the technology
bull It is relatively expensive
bull The exposure to radiation although small is best avoided
bull Bone biomarkers offer an alternative monitoring strategy
(Burch et al 2014)
12
Diagnostic Bone Markers in Osteoporosis
bull Specifically derived biomarkers that reflect both bone formation by osteoblasts and resorption by osteoclasts
bull Include both enzymes and peptides derived from cellular and non-cellular compartments of bone
bull May be measured in synovial fluid blood or urine
bull Techniques for their measurements are abundant
bull Classified as bone formation and resorption markers (Seibel 2005) 13
Diagnostic Bone Markers in Osteoporosis
bull Detect metabolic changes in bone after about 3-6 months
(McCormick 2007)
bull Relatively cheap compared with DXA (Wheater et al 2013)
bull No exposure to radiation
bull Helpful tools in the diagnostic prognostic and therapeutic
assessment of osteoporosis
14
Diagnostic Bone Markers in Osteoporosis
15
Markers of Bone Formation
16
Bone Alkaline Phosphatase (BALP)
bull Total alkaline phosphatase has several isoforms in serum
(Liver bone placental intestine spleen and kidney)
bull 40ndash50 of the total alkaline phosphatase activity arises from
the bone as a result of osteoblast activity (Siebel 2005)
bull Residual low cross-reactivity (16) with liver ALP limits its use
in patients with liver disease (Yang and Grey 2006) 17
Bone Alkaline Phosphatase (BALP) Assays
bull Immunoradiometric assay (IRMA)
bull Enzyme-linked immunosorbent assay (ELISA)
bull Ease of measurement cost efficiency and higher
specificity in detecting small changes makes BALP a
good marker for bone formation (Burch et al
2008) 18
Osteocalcin
bull A non collagenous matrix protein
bull Detected using enzyme linked immunosorbent assays (ELISA) or radioimmunoassays (RIA)
bull It is tissue specific widely available (Eapen et al 2008)
bull Heterogeneity of the fragments in the serum is thought to limit its use (Burch etal 2014)
bull May be affected by use of warfarin (Yang and Grey 2006)
Markers of Bone Resorption
20
Carboxy-terminal telopeptide cross-linked type 1 collagen (CTX)
bull Peptide fragments from the carboxy-terminal end of type 1
collagen produced during osteoclastic resorption
bull Detected in urine or serum using enzyme linked
immunosorbent assay (ELISA)
bull More accurate when monitoring the response to specific
treatments (eg with bisphosphonates) (Burch et al2014) 21
Amino-terminal telopeptide cross-linked type I collagen (NTX)
bull Peptide fragments from the amino terminal end of
type 1 collagen produced during osteoclastic
resorption
bull Detected in the urine or serum with competitive
inhibition ELISA or chemiluminescence assay
bull It is non-invasive and may be preferred by patients
(Yang and Grey 2006) 22
Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25

Limitations of BMD measurements in the Diagnosis of Osteoporosis
bull Changes in bone metabolism after therapy are detectable
only after about 2 years
bull Limited access to the technology
bull It is relatively expensive
bull The exposure to radiation although small is best avoided
bull Bone biomarkers offer an alternative monitoring strategy
(Burch et al 2014)
12
Diagnostic Bone Markers in Osteoporosis
bull Specifically derived biomarkers that reflect both bone formation by osteoblasts and resorption by osteoclasts
bull Include both enzymes and peptides derived from cellular and non-cellular compartments of bone
bull May be measured in synovial fluid blood or urine
bull Techniques for their measurements are abundant
bull Classified as bone formation and resorption markers (Seibel 2005) 13
Diagnostic Bone Markers in Osteoporosis
bull Detect metabolic changes in bone after about 3-6 months
(McCormick 2007)
bull Relatively cheap compared with DXA (Wheater et al 2013)
bull No exposure to radiation
bull Helpful tools in the diagnostic prognostic and therapeutic
assessment of osteoporosis
14
Diagnostic Bone Markers in Osteoporosis
15
Markers of Bone Formation
16
Bone Alkaline Phosphatase (BALP)
bull Total alkaline phosphatase has several isoforms in serum
(Liver bone placental intestine spleen and kidney)
bull 40ndash50 of the total alkaline phosphatase activity arises from
the bone as a result of osteoblast activity (Siebel 2005)
bull Residual low cross-reactivity (16) with liver ALP limits its use
in patients with liver disease (Yang and Grey 2006) 17
Bone Alkaline Phosphatase (BALP) Assays
bull Immunoradiometric assay (IRMA)
bull Enzyme-linked immunosorbent assay (ELISA)
bull Ease of measurement cost efficiency and higher
specificity in detecting small changes makes BALP a
good marker for bone formation (Burch et al
2008) 18
Osteocalcin
bull A non collagenous matrix protein
bull Detected using enzyme linked immunosorbent assays (ELISA) or radioimmunoassays (RIA)
bull It is tissue specific widely available (Eapen et al 2008)
bull Heterogeneity of the fragments in the serum is thought to limit its use (Burch etal 2014)
bull May be affected by use of warfarin (Yang and Grey 2006)
Markers of Bone Resorption
20
Carboxy-terminal telopeptide cross-linked type 1 collagen (CTX)
bull Peptide fragments from the carboxy-terminal end of type 1
collagen produced during osteoclastic resorption
bull Detected in urine or serum using enzyme linked
immunosorbent assay (ELISA)
bull More accurate when monitoring the response to specific
treatments (eg with bisphosphonates) (Burch et al2014) 21
Amino-terminal telopeptide cross-linked type I collagen (NTX)
bull Peptide fragments from the amino terminal end of
type 1 collagen produced during osteoclastic
resorption
bull Detected in the urine or serum with competitive
inhibition ELISA or chemiluminescence assay
bull It is non-invasive and may be preferred by patients
(Yang and Grey 2006) 22
Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25

Diagnostic Bone Markers in Osteoporosis
bull Specifically derived biomarkers that reflect both bone formation by osteoblasts and resorption by osteoclasts
bull Include both enzymes and peptides derived from cellular and non-cellular compartments of bone
bull May be measured in synovial fluid blood or urine
bull Techniques for their measurements are abundant
bull Classified as bone formation and resorption markers (Seibel 2005) 13
Diagnostic Bone Markers in Osteoporosis
bull Detect metabolic changes in bone after about 3-6 months
(McCormick 2007)
bull Relatively cheap compared with DXA (Wheater et al 2013)
bull No exposure to radiation
bull Helpful tools in the diagnostic prognostic and therapeutic
assessment of osteoporosis
14
Diagnostic Bone Markers in Osteoporosis
15
Markers of Bone Formation
16
Bone Alkaline Phosphatase (BALP)
bull Total alkaline phosphatase has several isoforms in serum
(Liver bone placental intestine spleen and kidney)
bull 40ndash50 of the total alkaline phosphatase activity arises from
the bone as a result of osteoblast activity (Siebel 2005)
bull Residual low cross-reactivity (16) with liver ALP limits its use
in patients with liver disease (Yang and Grey 2006) 17
Bone Alkaline Phosphatase (BALP) Assays
bull Immunoradiometric assay (IRMA)
bull Enzyme-linked immunosorbent assay (ELISA)
bull Ease of measurement cost efficiency and higher
specificity in detecting small changes makes BALP a
good marker for bone formation (Burch et al
2008) 18
Osteocalcin
bull A non collagenous matrix protein
bull Detected using enzyme linked immunosorbent assays (ELISA) or radioimmunoassays (RIA)
bull It is tissue specific widely available (Eapen et al 2008)
bull Heterogeneity of the fragments in the serum is thought to limit its use (Burch etal 2014)
bull May be affected by use of warfarin (Yang and Grey 2006)
Markers of Bone Resorption
20
Carboxy-terminal telopeptide cross-linked type 1 collagen (CTX)
bull Peptide fragments from the carboxy-terminal end of type 1
collagen produced during osteoclastic resorption
bull Detected in urine or serum using enzyme linked
immunosorbent assay (ELISA)
bull More accurate when monitoring the response to specific
treatments (eg with bisphosphonates) (Burch et al2014) 21
Amino-terminal telopeptide cross-linked type I collagen (NTX)
bull Peptide fragments from the amino terminal end of
type 1 collagen produced during osteoclastic
resorption
bull Detected in the urine or serum with competitive
inhibition ELISA or chemiluminescence assay
bull It is non-invasive and may be preferred by patients
(Yang and Grey 2006) 22
Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25

Diagnostic Bone Markers in Osteoporosis
bull Detect metabolic changes in bone after about 3-6 months
(McCormick 2007)
bull Relatively cheap compared with DXA (Wheater et al 2013)
bull No exposure to radiation
bull Helpful tools in the diagnostic prognostic and therapeutic
assessment of osteoporosis
14
Diagnostic Bone Markers in Osteoporosis
15
Markers of Bone Formation
16
Bone Alkaline Phosphatase (BALP)
bull Total alkaline phosphatase has several isoforms in serum
(Liver bone placental intestine spleen and kidney)
bull 40ndash50 of the total alkaline phosphatase activity arises from
the bone as a result of osteoblast activity (Siebel 2005)
bull Residual low cross-reactivity (16) with liver ALP limits its use
in patients with liver disease (Yang and Grey 2006) 17
Bone Alkaline Phosphatase (BALP) Assays
bull Immunoradiometric assay (IRMA)
bull Enzyme-linked immunosorbent assay (ELISA)
bull Ease of measurement cost efficiency and higher
specificity in detecting small changes makes BALP a
good marker for bone formation (Burch et al
2008) 18
Osteocalcin
bull A non collagenous matrix protein
bull Detected using enzyme linked immunosorbent assays (ELISA) or radioimmunoassays (RIA)
bull It is tissue specific widely available (Eapen et al 2008)
bull Heterogeneity of the fragments in the serum is thought to limit its use (Burch etal 2014)
bull May be affected by use of warfarin (Yang and Grey 2006)
Markers of Bone Resorption
20
Carboxy-terminal telopeptide cross-linked type 1 collagen (CTX)
bull Peptide fragments from the carboxy-terminal end of type 1
collagen produced during osteoclastic resorption
bull Detected in urine or serum using enzyme linked
immunosorbent assay (ELISA)
bull More accurate when monitoring the response to specific
treatments (eg with bisphosphonates) (Burch et al2014) 21
Amino-terminal telopeptide cross-linked type I collagen (NTX)
bull Peptide fragments from the amino terminal end of
type 1 collagen produced during osteoclastic
resorption
bull Detected in the urine or serum with competitive
inhibition ELISA or chemiluminescence assay
bull It is non-invasive and may be preferred by patients
(Yang and Grey 2006) 22
Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25

Diagnostic Bone Markers in Osteoporosis
15
Markers of Bone Formation
16
Bone Alkaline Phosphatase (BALP)
bull Total alkaline phosphatase has several isoforms in serum
(Liver bone placental intestine spleen and kidney)
bull 40ndash50 of the total alkaline phosphatase activity arises from
the bone as a result of osteoblast activity (Siebel 2005)
bull Residual low cross-reactivity (16) with liver ALP limits its use
in patients with liver disease (Yang and Grey 2006) 17
Bone Alkaline Phosphatase (BALP) Assays
bull Immunoradiometric assay (IRMA)
bull Enzyme-linked immunosorbent assay (ELISA)
bull Ease of measurement cost efficiency and higher
specificity in detecting small changes makes BALP a
good marker for bone formation (Burch et al
2008) 18
Osteocalcin
bull A non collagenous matrix protein
bull Detected using enzyme linked immunosorbent assays (ELISA) or radioimmunoassays (RIA)
bull It is tissue specific widely available (Eapen et al 2008)
bull Heterogeneity of the fragments in the serum is thought to limit its use (Burch etal 2014)
bull May be affected by use of warfarin (Yang and Grey 2006)
Markers of Bone Resorption
20
Carboxy-terminal telopeptide cross-linked type 1 collagen (CTX)
bull Peptide fragments from the carboxy-terminal end of type 1
collagen produced during osteoclastic resorption
bull Detected in urine or serum using enzyme linked
immunosorbent assay (ELISA)
bull More accurate when monitoring the response to specific
treatments (eg with bisphosphonates) (Burch et al2014) 21
Amino-terminal telopeptide cross-linked type I collagen (NTX)
bull Peptide fragments from the amino terminal end of
type 1 collagen produced during osteoclastic
resorption
bull Detected in the urine or serum with competitive
inhibition ELISA or chemiluminescence assay
bull It is non-invasive and may be preferred by patients
(Yang and Grey 2006) 22
Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25

Markers of Bone Formation
16
Bone Alkaline Phosphatase (BALP)
bull Total alkaline phosphatase has several isoforms in serum
(Liver bone placental intestine spleen and kidney)
bull 40ndash50 of the total alkaline phosphatase activity arises from
the bone as a result of osteoblast activity (Siebel 2005)
bull Residual low cross-reactivity (16) with liver ALP limits its use
in patients with liver disease (Yang and Grey 2006) 17
Bone Alkaline Phosphatase (BALP) Assays
bull Immunoradiometric assay (IRMA)
bull Enzyme-linked immunosorbent assay (ELISA)
bull Ease of measurement cost efficiency and higher
specificity in detecting small changes makes BALP a
good marker for bone formation (Burch et al
2008) 18
Osteocalcin
bull A non collagenous matrix protein
bull Detected using enzyme linked immunosorbent assays (ELISA) or radioimmunoassays (RIA)
bull It is tissue specific widely available (Eapen et al 2008)
bull Heterogeneity of the fragments in the serum is thought to limit its use (Burch etal 2014)
bull May be affected by use of warfarin (Yang and Grey 2006)
Markers of Bone Resorption
20
Carboxy-terminal telopeptide cross-linked type 1 collagen (CTX)
bull Peptide fragments from the carboxy-terminal end of type 1
collagen produced during osteoclastic resorption
bull Detected in urine or serum using enzyme linked
immunosorbent assay (ELISA)
bull More accurate when monitoring the response to specific
treatments (eg with bisphosphonates) (Burch et al2014) 21
Amino-terminal telopeptide cross-linked type I collagen (NTX)
bull Peptide fragments from the amino terminal end of
type 1 collagen produced during osteoclastic
resorption
bull Detected in the urine or serum with competitive
inhibition ELISA or chemiluminescence assay
bull It is non-invasive and may be preferred by patients
(Yang and Grey 2006) 22
Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25

Bone Alkaline Phosphatase (BALP)
bull Total alkaline phosphatase has several isoforms in serum
(Liver bone placental intestine spleen and kidney)
bull 40ndash50 of the total alkaline phosphatase activity arises from
the bone as a result of osteoblast activity (Siebel 2005)
bull Residual low cross-reactivity (16) with liver ALP limits its use
in patients with liver disease (Yang and Grey 2006) 17
Bone Alkaline Phosphatase (BALP) Assays
bull Immunoradiometric assay (IRMA)
bull Enzyme-linked immunosorbent assay (ELISA)
bull Ease of measurement cost efficiency and higher
specificity in detecting small changes makes BALP a
good marker for bone formation (Burch et al
2008) 18
Osteocalcin
bull A non collagenous matrix protein
bull Detected using enzyme linked immunosorbent assays (ELISA) or radioimmunoassays (RIA)
bull It is tissue specific widely available (Eapen et al 2008)
bull Heterogeneity of the fragments in the serum is thought to limit its use (Burch etal 2014)
bull May be affected by use of warfarin (Yang and Grey 2006)
Markers of Bone Resorption
20
Carboxy-terminal telopeptide cross-linked type 1 collagen (CTX)
bull Peptide fragments from the carboxy-terminal end of type 1
collagen produced during osteoclastic resorption
bull Detected in urine or serum using enzyme linked
immunosorbent assay (ELISA)
bull More accurate when monitoring the response to specific
treatments (eg with bisphosphonates) (Burch et al2014) 21
Amino-terminal telopeptide cross-linked type I collagen (NTX)
bull Peptide fragments from the amino terminal end of
type 1 collagen produced during osteoclastic
resorption
bull Detected in the urine or serum with competitive
inhibition ELISA or chemiluminescence assay
bull It is non-invasive and may be preferred by patients
(Yang and Grey 2006) 22
Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25

Bone Alkaline Phosphatase (BALP) Assays
bull Immunoradiometric assay (IRMA)
bull Enzyme-linked immunosorbent assay (ELISA)
bull Ease of measurement cost efficiency and higher
specificity in detecting small changes makes BALP a
good marker for bone formation (Burch et al
2008) 18
Osteocalcin
bull A non collagenous matrix protein
bull Detected using enzyme linked immunosorbent assays (ELISA) or radioimmunoassays (RIA)
bull It is tissue specific widely available (Eapen et al 2008)
bull Heterogeneity of the fragments in the serum is thought to limit its use (Burch etal 2014)
bull May be affected by use of warfarin (Yang and Grey 2006)
Markers of Bone Resorption
20
Carboxy-terminal telopeptide cross-linked type 1 collagen (CTX)
bull Peptide fragments from the carboxy-terminal end of type 1
collagen produced during osteoclastic resorption
bull Detected in urine or serum using enzyme linked
immunosorbent assay (ELISA)
bull More accurate when monitoring the response to specific
treatments (eg with bisphosphonates) (Burch et al2014) 21
Amino-terminal telopeptide cross-linked type I collagen (NTX)
bull Peptide fragments from the amino terminal end of
type 1 collagen produced during osteoclastic
resorption
bull Detected in the urine or serum with competitive
inhibition ELISA or chemiluminescence assay
bull It is non-invasive and may be preferred by patients
(Yang and Grey 2006) 22
Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25
Osteocalcin
bull A non collagenous matrix protein
bull Detected using enzyme linked immunosorbent assays (ELISA) or radioimmunoassays (RIA)
bull It is tissue specific widely available (Eapen et al 2008)
bull Heterogeneity of the fragments in the serum is thought to limit its use (Burch etal 2014)
bull May be affected by use of warfarin (Yang and Grey 2006)
Markers of Bone Resorption
20
Carboxy-terminal telopeptide cross-linked type 1 collagen (CTX)
bull Peptide fragments from the carboxy-terminal end of type 1
collagen produced during osteoclastic resorption
bull Detected in urine or serum using enzyme linked
immunosorbent assay (ELISA)
bull More accurate when monitoring the response to specific
treatments (eg with bisphosphonates) (Burch et al2014) 21
Amino-terminal telopeptide cross-linked type I collagen (NTX)
bull Peptide fragments from the amino terminal end of
type 1 collagen produced during osteoclastic
resorption
bull Detected in the urine or serum with competitive
inhibition ELISA or chemiluminescence assay
bull It is non-invasive and may be preferred by patients
(Yang and Grey 2006) 22
Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25
Markers of Bone Resorption
20
Carboxy-terminal telopeptide cross-linked type 1 collagen (CTX)
bull Peptide fragments from the carboxy-terminal end of type 1
collagen produced during osteoclastic resorption
bull Detected in urine or serum using enzyme linked
immunosorbent assay (ELISA)
bull More accurate when monitoring the response to specific
treatments (eg with bisphosphonates) (Burch et al2014) 21
Amino-terminal telopeptide cross-linked type I collagen (NTX)
bull Peptide fragments from the amino terminal end of
type 1 collagen produced during osteoclastic
resorption
bull Detected in the urine or serum with competitive
inhibition ELISA or chemiluminescence assay
bull It is non-invasive and may be preferred by patients
(Yang and Grey 2006) 22
Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25

Carboxy-terminal telopeptide cross-linked type 1 collagen (CTX)
bull Peptide fragments from the carboxy-terminal end of type 1
collagen produced during osteoclastic resorption
bull Detected in urine or serum using enzyme linked
immunosorbent assay (ELISA)
bull More accurate when monitoring the response to specific
treatments (eg with bisphosphonates) (Burch et al2014) 21
Amino-terminal telopeptide cross-linked type I collagen (NTX)
bull Peptide fragments from the amino terminal end of
type 1 collagen produced during osteoclastic
resorption
bull Detected in the urine or serum with competitive
inhibition ELISA or chemiluminescence assay
bull It is non-invasive and may be preferred by patients
(Yang and Grey 2006) 22
Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25

Amino-terminal telopeptide cross-linked type I collagen (NTX)
bull Peptide fragments from the amino terminal end of
type 1 collagen produced during osteoclastic
resorption
bull Detected in the urine or serum with competitive
inhibition ELISA or chemiluminescence assay
bull It is non-invasive and may be preferred by patients
(Yang and Grey 2006) 22
Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25

Conclusion
bull The biomarkers of bone metabolism are helpful tools to
detect the dynamics of the metabolic imbalance itself
and thus complement the static measures of bone
bull They show more rapid changes soon after initiating
treatment hence are better tools in the prognosis and
monitoring of patients receiving antiresorptive therapy 23
Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25

Selected References
Burch J Rice S Yang H Neilson A Stirk L Francis R Holloway P Selby P and Craig D (2014) Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment the secondary prevention of fractures and primary prevention of fractures in high-risk groups Health Technology Assessment 18 (11) 2-28
Eapen E Grey V Don-Wauchope A and Atkinson SA (2008) Bone Health in Childhood Usefulness of Biochemical Biomarkers eJIFCC 19 (2) 221-227
McCormick RK (2007) Osteoporosis Integrating Biomarkers and Other Diagnostic Correlates into the Management of Bone Fragility Alt Med Rev 12 (2) 469-478
Seibel MJ (2005) Biochemical markers of bone turnover part I biochemistry and variability Clin Biochem Rev 26 97ndash102
Vasikaran SD Glendenning P and Morris HA (2006) The Role of Biochemical Markers of Bone Turnover in Osteoporosis Management in Clinical Practice Clin Biochem Rev 27(3) 119ndash125
Wheater G Elshahaly M Tuck SP Datta HK and Van-Laar JM (2013) The clinical utility of bone marker measurements in osteoporosis J of Trans Med 11(201) 111-121
Yang L and Grey V (2006) Pediatric reference intervals for bone markers Clin Biochem 39(6)561ndash568
Thank you for listening
25

Thank you for listening
25
![Tissues copy paper binder paper band-aids white board markers [black ink is most useful!] page protectors/plastic sleeves black dry erase markers [fine](https://img.dokumen.tips/doc/110x75/56649d1b5503460f949f16e8/tissues-copy-paper-binder-paper-band-aids-white-board-markers-black-ink-is.jpg)




























