Embed Size (px)
Citation preview

Older Adults & Optimal Outcome
Individualizing Diabetes Management
Mary Moyer Janci BC-FNP BC-ADM CDETeaching Associate
Diabetes Care Center UWMC

What is Diabetes ?
• METABOLIC DISEASE
– Food breakdown (carbohydrates, proteins and fat)
– → fuel for the body ABNORMAL
2

3
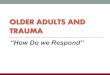
GLUCOSE STIMULATEDINSULIN SECRETION
GLUCOSE UPTAKE BY MUSCLE & FAT
HEPATIC GLUCOSE
RESPONSE
NORMAL PLASMA GLUCOSE
Controlled glucose production.
Enters blood.
Controlled glucose clearance.
Enters peripheal tissue.

4
GLUCOSE STIMULATEDINSULIN SECRETION
GLUCOSE UPTAKE BY MUSCLE & FAT
Controlled glucose production.
Enters blood.
Controlled glucose clearance.
Enters peripheal tissue.

Diabetes Types
Type 1, 1.5, LADA
Type 2 Adult
Secondary Diabetes• Disease/injury to the pancreas
• - pancreatitis, pancreatectomy, CFRD
• Meds increased insulin resistance » STEROID INDUCED HYPERGLYCEMIA

T2DM Pathophysiology
• Peripheral insulin resistance in muscle and fat
• Decreased pancreatic insulin secretion
• Increased hepatic glucose output
– Risk fx: African Americans, Latinos, American Indians, Alaska Natives, Asian Americans, Pacific Islanders
–
• PEARL: oral agents or insulin

T1DMPathophysiology
• Decreased pancreatic insulin secretion
• Peripheral insulin resistance in muscle and fat
• Increased hepatic glucose output
• PEARL: only insulin
Haffner SM, et al. Diabetes Care, 1999

What makes older adults at risk for diabetes?
– Decreased beta cell function • with loss of first phase insulin shows up in post prandial blood glucose
– AND• Loss of muscle mass
• Decreased physical activity
• Increased adiposity

What factors affect quality of life?
• Changes in cognitive status
• Decrease ability to care for myself
• Increase in use of caregivers
• Decrease life expectancy
Huang et al. J AM Geriatr Soc 2005;53:306-311

How does glycemic control affect the body ?
Hypoglycemia Hyperglycemia
Increase in Hypoglycemia unawareness
Dehydration
Cognitive changes / confusion
Urinary incontinence
Need assistance to treat lows
Electrolytes
Falls & unsteady gait Dizziness/ falls
More admissions tohospital? Cardiac events
ACCORD, ADVANCE,
More admissions to hospital from HHS, infection

•


Recommendations for the Comprehensive Care of Older Patients With T2D:Consensus Panel Framework presented ADA conference 2012
Health Status Rationale
Reason-able
A1C Goal
Fasting or
Preprandia
l Glucose
(mg/dL)
Bedtime
Glucose
(mg/dL)
Blood
Pressure
(mm Hg) Lipids
Healthy Longer life expectancy <7.5% 90–130 90–150 <140/80
Statin (unless
contraindicated
or not tolerated)
Complex/
Intermediate
Health
Intermediate life
expectancy; high
treatment burden;
hypoglycemia
vulnerability; fall risk
<8.0% 90–150 100–180 <140/80
Statin (unless
contraindicated
or not tolerated)
Very Complex/
Poor Health
Limited life expectancy;
treatment benefit
uncertain<8.5% 100–180 110–200 <150/90
Consider
benefit
with statin;
(secondary
prevention >
primary)
13
Healthy: few coexisting chronic illnesses, intact cognitive and functional status.Complex/Intermediate Health: multiple coexisting chronic illnesses, or 2+ instrumental ADL impairments, or mild to moderate cognitive impairment.Very Complex/Poor Health: long-term care or end-stage chronic illnesses or moderate to severe cognitive impairment or 2+ activities of daily living dependencies.
Kirkman S et al. Diabetes Care. 2012;35(12):2650–2664.

What are we dealing with?1,2
Older adult stats:
• 65 years +
– 72.1 million 2030 ~ 19% population
• 85 years +
– 5.5 million 2007
– 6.6 million 2020
• Today ~ 26% adults > 65 years have diabetes
1. US Dept of Health Human Services, Admi on Aging. www.aoa.gov/aoaroot/aging_statistics/Profile2. http://www.cdc.gov/diabetes/pubs/statsreport14/national-diabetes-report-web.pdf

What do most aging adults want?
–INDEPENDENCE For ADLsExploratory study T2DM 65+ n=2871% ranked Independence and ADLS as top priority
– What takes away independence?
• Polypharmacy “too many meds to manage” LEADS TO increased side effects
• Higher risk of hypoglycemia due to length of time with DM• Increased CVD • Decreased kidney function
Huang et al. J AM Geriatr Soc 2005;53:306-311

Treatment Goals
• Improving quality of life & quality of care
• Allowing choices in daily living
• Assisting individuals to make informed health decisions
ADA. Older adults. Sec. 10. In Standards of Medical Care in Diabetes-2016. Diabetes Care 2016.:39 (Suppl.1):S81-S85

Recommendations for the Comprehensive Care of Older Patients With T2D: Consensus Panel Framework
Health Status Rationale
Reason-
able A1C
Goal
Fasting or
Preprandial
Glucose
(mg/dL)
Bedtime
Glucose
(mg/dL)
Blood
Pressure
(mm Hg) Lipids
Healthy Longer life expectancy <7.5% 90–130 90–150 <140/80
Statin (unless
contraindicated or
not tolerated)
Complex/
Intermediate
Health
Intermediate life
expectancy; high
treatment burden;
hypoglycemia
vulnerability; fall risk
<8.0% 90–150 100–180 <140/80
Statin (unless
contraindicated or
not tolerated)
Very
Complex/
Poor Health
Limited life expectancy;
treatment benefit
uncertain
<8.5% 100–180 110–200 <150/90
Consider benefit
with statin;
(secondary
prevention >
primary)
17
Healthy: few coexisting chronic illnesses, intact cognitive and functional status.Complex/Intermediate Health: multiple coexisting chronic illnesses, or 2+ instrumental ADL impairments, or mild to moderate cognitive impairment.Very Complex/Poor Health: long-term care or end-stage chronic illnesses or moderate to severe cognitive impairment or 2+ activities of daily living dependencies.
Kirkman S et al. Diabetes Care. 2012;35(12):2650–2664.

Case Study- What to do?Use our tools
• Interview patient in decision-making.
– MMSE
• Individualize Patient Goals
– Adjust target A1C based on chronic conditions, lifespan, mental capability
• Prioritize targets: BP, Lipids, A1C
• Customize treatment plan: meds, diet, exercise, caregiving

Inzucchi S E et al. Dia Care 2012;35:1364-1379
2nd TOOL:RANKING
More or less
stringent glucose control?
A1c

3rd TOOL: Priorities
Physiologic Parameter
Time to see benefit of tx
Outcome
Blood glucose 8 years Reduced microvascular disease
Reduced CV dx
Lipids 2-3 years Reduced stroke and MI morbidity and mortality
Blood pressure 2-3 years Reduced stroke and MI morbidity and mortality
Kirkman S et al. Diabetes Care. 2012;35(12):2650–2664.
Physiologic Parameter
Length of time needed to see benefit of tx
Outcome Research
Blood glucose 8 years 1. ↓ microvascular disease, mortality & MIs
2. Neutral CVD, MI stroke ↑𝑚𝑜𝑟𝑡𝑎𝑙𝑖𝑡𝑦
3. Neutral CVD, ↓ kidney disease
4. Neutral CVD, ↓𝑎𝑙𝑏𝑢𝑚𝑖𝑛𝑢𝑟𝑖𝑎
1. UKPDS
2. ACCORD (stop 3 yrs)
3. ADVANCE
4. VADT
Lipids 2-3 years Reduced stroke
mortality
No large trials
Meta-analysis of smaller studies
Blood pressure 2-3 years 1. Reduced stroke
2. Reduced mortality
1. ACCORD-BP
2. VADT
A1c 8..2%
LDL 128
BP 138/64

Recommendations for the Comprehensive Care of Older Patients With T2D: Consensus Panel Framework
Health Status Rationale
Reason-
able A1C
Goal
Fasting or
Preprandial
Glucose
(mg/dL)
Bedtime
Glucose
(mg/dL)
Blood
Pressure
(mm Hg) Lipids
Healthy Longer life expectancy <7.5% 90–130 90–150 <140/80
Statin (unless
contraindicated or
not tolerated)
Complex/
Intermediate
Health
Intermediate life
expectancy; high
treatment burden;
hypoglycemia
vulnerability; fall risk
<8.0% 90–150 100–180 <140/80
Statin (unless
contraindicated or
not tolerated)
Very
Complex/
Poor Health
Limited life expectancy;
treatment benefit
uncertain
<8.5% 100–180 110–200 <150/90
Consider benefit
with statin;
(secondary
prevention >
primary)
21
Healthy: few coexisting chronic illnesses, intact cognitive and functional status.Complex/Intermediate Health: multiple coexisting chronic illnesses, or 2+ instrumental ADL impairments, or mild to moderate cognitive impairment.Very Complex/Poor Health: long-term care or end-stage chronic illnesses or moderate to severe cognitive impairment or 2+ activities of daily living dependencies.
Kirkman S et al. Diabetes Care. 2012;35(12):2650–2664.

4th TOOL: Use the Medication Chart

Diabetes Medication
Target Population
Benefits Risks Dose Adjustment for CKD Stage 3-5Dialysis
COST
Sulfonylureas- glipizide, glyburide, glimeperide
T2DM < 5 years
↑ insulin secretion↓ 𝑚𝑖𝑐𝑟𝑜𝑣𝑎𝑠𝑐𝑢𝑙𝑎𝑟
(UKPDS)
More hypos; weight gain
Glimeperide: decrease dose; 1 mg/day recommendedGlipizide: no decrease in doseGlyburide: avoidDIALYSIS- GLIPIZIDE ONLY
LOW
Meglitinides-repaglinide,netaglinide
Recent diagnosisT2DM,Elevated PPG
Short acting, lesshypoglycemiqFlexible dosing based on size of meal,
More hyposWeight gainFrequent dosing
Repaglinide: no decrease in doseNateglinide: start at low dose of 60 mgDIALYSIS- REPAGLINIDE ONLY
MOD-HI
Biguanides-metformin, glucophage
Overweight, obese, IR
No wt gain, less hypoglycemia
↓ 𝐶𝑉𝐷 𝑒𝑣𝑒𝑛𝑡𝑠𝑈𝐾𝑃𝐷𝑆
GI side effects, rare lactic acidosis
Contraindicated: males SCr > 1.5 mg/dl; females: SCr> 1.4 mg/dl
Consider s crt 1.7/egfr<30 dose reductionDIALYSIS- AVOID
LOW
TZDs- ***rosiglitazone, pioglitazone
Overweight, obese, IR
↑ 𝑖𝑛𝑠𝑢𝑙𝑖𝑛𝑠𝑒𝑛𝑠𝑖𝑡𝑖𝑣𝑖𝑡𝑦
No hypos↑ 𝐻𝐷𝐿
Weight gain/fluidretention, slow onset, Bone fx
No dose adjustment for either med
DIALYSIS OK
LOW
DPP-4 ***SitagliptinSaxagliptinVildaliptinAlogliptinLinigliptin
↑ 𝑖𝑛𝑠𝑢𝑙𝑖𝑛↓ 𝑔𝑙𝑢𝑐𝑎𝑔𝑜𝑛
No hypoglycemia
Angioedema, urticarial,? Pancreatitis?HF
↓ 25% GFR 30-50↓ 50% GFR < 30 DIALYSIS OK
HI

Diabetes Medication
Target Population
Action/ Benefits Risks Dose Adjustment for CKD Stage 3-5 Dialysis
COST
GLP-1 RA ***Exenatide/ ERLiraglutideAbiglutideLixsenatideDulaglutide
Overweight,obese
No hypoglycemiaWt loss
↓ 𝑃𝑃 𝑔𝑙𝑢𝑐𝑜𝑠𝑒↓ 𝑠𝑜𝑚𝑒 𝐶𝑉 𝑟𝑖𝑠𝑘 𝑓𝑥
GI side effectsInjectablePancreatitis?Change thyroid tumors in animals
Avoid eGFR <30 HI
Alpha-glucosidase inhibitor-acarbose,miglitol
No hypoglycemia↓ 𝑃𝑃 𝑔𝑙𝑢𝑐𝑜𝑠𝑒 Elevated post meal glucoseSlow intestinal carbdigest/absorp
GI side effects, low impact of A1c Avoid SCr > 2 mg/Dl
DIALYSIS AVOID
MOD
SGLT2 inhibitors ***CanagliflozinDapagliflozinEmpagliflozin
Block glucosereabsorption
↑ 𝑔𝑙𝑦𝑐𝑜𝑠𝑢𝑟𝑖𝑎No hypos
↓ 𝑤𝑡↓ 𝐵𝑃
No hypos
Euglycemic DKA
GU infectionsPolyuriaHypotension/volume depletionDizziness
Adjust dose in egfr <59 Avoid in egfr < 30
HI
New Insulins HyposInjectable needs training
Adjust dose by 25-50% in patients with decreased kidney function
HI

Insulin & Older Adults
• US Public Health survelliance data of people ≥ 65 𝑦𝑒𝑎𝑟𝑠
– Insulin was one of top meds ADRs → ER visits
– 40% of these pts were hospitalized
– What do we learn?• careful selection of patients, training for insuln and smbg, regular follow up
– Budnitz et al. N Engl J Med. 2011:365:2002-2012

Case Study- Lifestyle Changes and Education
• Lifestyle changes– Exercise– Nutrition Education 1:1
• Blood Glucose Monitoring– Testing daily in the fasting state– 2 hour post meal testing after the largest meal
• Diabetes Core Classes– 10 hour program focusing on diabetes, meds, nutrition– ADA certified– Individualized Training. Bring a family member or caregiver.

Nutrition
• Older adults at risk for poor nutrition & weight loss– Causes: loss of smell, taste, hormonal changes that control satiety
• American Dietetics Association– Refer to RD for individualized care plan
– Involve patient, family, team members in choices
– Base on patient’s condition & life span
– Some changes may include:• Less restrictive diet
• More carbohydrate beverages
Position of the ADA Assoc; Ethical and legal issues in nutrition, hydration, and feeding.J Am Diet Assoc. 2008; 108:873-882

Research to support lifestyle changes
• DPP & Look AHEAD1
– Found wt loss & physical activity ↓ glucose – older adults had > wt loss & more physical activity than younger pts and not
associated with intensity of exercise. – So bottom line: don’t have to run a marathon or be on ‘Biggest Loser’ TV show
• Exercise & healthy eating for planned weight loss2
– Increases muscle mass– Improves functional status– Improves depression– ? decrease urinary incontinence– ? improve CV risk factors1. Espelnad et all. JAGS: 61:912-922, 2013. 2. American Heart Asso. 2014 . http://www.heart.org

Update Case Study 5 years later 87 yo
• Patient returns to clinic with A1c 9%.
– CABG with 2 vessel bypass, HTN, Hyperlipidemia, developing cognitive impairment
– Now living in ALF
• TREATMENT PLAN: changing the meaning of optimal ? Options?• Decreased risk of hypos with meds; changed target to A1c <8.5%• Added basal insulin in AM & stopped DPP4 due to $$$- ??? Now low dose TZD or NPH?• Continue metformin?• Add sulfonylurea?

Palliative Care Proposed Recs
Goals: comfort, symptom control, prevention of pain, hyperglycemia/hypoglycemia, dehydration; preservication of diginity and quality of life (1)
Patient has the right to refuse testing & treatment
Stable patient: focus on preventing hi/lo bgs (2)
Organ failure patient: focus on preventing bg lows; (2)tx highs with hydration as tolerated. T1DM require insulin but may simplify.T2DM my titrate off insulin.
• 1. J Am Med ir Assoc 2012, 13:497-502• 2. J Palliat Med 2011; 14:83-87

Summary
REMEMBER INDIVIDUALIZE DIABETES GOALS IN OLDER ADULTS
– USE TOOLS• Interview for patient priorities• Set medical priorities
– Lipids, BP, A1c• Set target A1c / bg control by using ranking scales• Use diabetes med chart • Add lifestyle changes• Re-evaluate routinely• Re-adjust diabetes goals based on patient / family priorities,
physical and mental condition, lifespan