Embed Size (px)
Citation preview

150 Sharma, Sharma
PREVENTIONThe US National Center for Infectious Dis-eases received reports of three adult deaths dueto chickenpox in the first three months of 1997,including two cases ofpneumonia in previouslyhealthy non-pregnant adults.28 Three controlstrategies were recommended, including uni-versal vaccination against varicella in childrenaged over 12 months and non-immune adults,after antibody testing in doubtful cases. Thevaccine was developed in Japan in 1972 and hasbeen available in North America since March1995. It is a live, attenuated virus preparationand therefore is unsuitable for immunosu-pressed persons and pregnant women. Uptakeof the vaccine has been poor even in designatedUS surveillance sites because of perceptionsthat chickenpox is mild and usually uncompli-cated and unjustified concerns over the efficacyand duration of immunity afforded by vaccina-tion. Other reasons advanced to account forpoor "hit rates" are the stringent storage andhandling regulations and matters of cost.Varicella is not included in currently availablevaccination schedules in the UK.The second strategy concerns varicella
zoster immune globulin (VZIG). It is availablefor post-exposure prophylaxis in susceptibleindividuals including pregnant women andimmunosuppressed persons and may be pre-scribed, on the advice of specialists in infec-tious disease, to non-immune health careworkers who may present to the emergencydepartment after occupational exposure to acase of chickenpox. VZIG should be given assoon as possible but it may be effective up to 96hours after exposure.
Finally, it was recommended that all adultcases of chickenpox should be treated with oralacicolvir, preferably within 24 hours of thedevelopment of the rash.
1 Gershon AA, Steinberg SP, Gelb L. Clinical reinfection withvaricella-zoster virus. J Infect Dis 1984;149:137-42.
2 Miller E, Marshall R, Vurdien J. Epidemiology, outcomeand control of varicella-zoster infection. Rev Med Microbiol1 993;4:222-30.
3 Haake DA, Zakowski PC, Haake DL, et al. Early treatmentwith acyclovir for varicella pneumonia in otherwise healthyadults: retrospective controlled study and review. Rev InfectDis 1990;12:788-98.
4 Wallace MR, Bowler WA, Murray NB, et al. Treatment ofadult varicella with oral acyclovir. A randomised, placebo-controlled trial. Ann Intern Med 1992;117:358-63.
5 Joseph CA, Noah ND. Epidemiology of chickenpox in Eng-land and Wales, 1976-85. BMJ 1988;296:673-6.
6 Fairley CK, Miller E. Varicella-zoster virus epidemiology-achanging scene ?JIlnfect Dis 1996;174(suppl 3):S314-19.
7 Mermelstein RH, Freireich AW. Varicella pneumonia. AnnIntern Med 1961;55:456-63.
8 Knyvett AF. The pulmonary lesions of chickenpox. QJ'Med1966;139:313-23.
9 Ellis ME, Neal KR, Webb AK. Is smoking a risk factor forpneumonia in adults with chickenpox ? BMJ 1987;294:1002-3.
10 Rose RM, Wasserman AS, Wyser WY, et al. Deficientresponse ofpulmonary macrophages from healthy smokersto antiviral lymphokines in vitro.3JInfect Dis 1986;154:61 1-18.
11 Waring JJ, Neubuerger K, Geever EF. Severe form of chick-enpox in adults. Arch Intern Med 1942;69:348-408.
12 Nillson A, Ortqvist A. Severe varicella pneumonia in adultsin Stockholm county 1980-1989. Scand J Infect Dis1996;28: 121-3.
13 Davidson RN, Lynn W, Savage P, et al. Chickenpoxpneumonia: experience with antiviral treatment. Thorax1988;43:627-30.
14 Weber DM, Pellecchia JA. Varicella pneumonia. Study ofprevalence in adult men. JAMA 1965;192:572-3.
15 Baren JM, Henneman PL, Lewis RJ. Primary varicella inadults: pneumonia, pregnancy and hospital admission. AnnEmerg Med 1996;28: 165-9.
16 Jackson MA, Burry VF, Olson LC. Complications ofvaricella requiring hospitalization in previously healthychildren. Pediatr Infect Dis J 1992;11:441-5.
17 Potgeiter PD, Hammond JMJ. Intensive care managementof varicella pneumonia. RespirMed 1997;91:207-12.
18 Weinstein L, Meade R. Respiratory manifestations of chick-enpox. Arch Intern Med 1956;98:91-9.
19 Picken G, Booth AJ, Williams MV. The pulmonary lesionsof chickenpox pneumonia revisited. Br J Radiol 1994;67:659-60.
20 Lee WA, Kolla S, Schreiner RJ, et al. Prolonged extracorpor-eal life support (ECLS) for varicella pneumonia. Crit CareMed 1997;25:977-82.
21 Whited RE. A prospective study of laryngotracheal sequelaein long-term intubation. Laryngoscope 1984;94:367-77.
22 Sugerman HJ, Wolfe L, Pasquale MD, et al. Multicenter,randomized, prospective trial of early tracheostomy. JTrauma 1997;43:741-7.
23 Gershon AA. Steroid therapy and varicella. J Pediatr1972;81:1034.
24 Smego RA, Asperills MO. Acyclovir for varicella pneumoniaduring pregnancy. Obstet Gynecol 1991;78: 1112-16.
25 Bean B. Antiviral therapy: new drugs and their uses. PostgradMed 1986;80:1 13-19
26 Laskin OL. Acyclovir: pharmacology and clinical experi-ence. Arch Intern Med 1984;144:387-8.
27 Broussard RC, Payne DK, George RB. Treatment with acy-clovir of varicella pneumonia in pregnancy. Chest 1991;99:1045-7.
28 Anonymous. Varicella-related deaths among adults-United States, 1997.JAAMA 1997;277:1754-5.
Management of laryngeal foreign bodies inchildren
Hari Shankar Sharma, Sanjay SharmaSchool ofMedicalSciences, UniversitySains Malaysia, 16150Kota Bharu, Kelantan,Malaysia:Department ofOtorhinolaryngologyH S Sharma
Department ofAnaesthesiologyS Sharma
Correspondence to:Dr Hari Shankar Sharma,Lecturer (e-mail:[email protected]).
Accepted 31 October 1998
AbstractForeign body aspiration is one ofthe lead-ing causes of accidental death in children.Food items are the most common itemsaspirated in infants and toddlers, whereasolder children are more likely to aspiratenon-food items. Laryngeal impaction of aforeign body is very rare as most aspiratedforeign bodies pass through the laryngealinlet and get lodged lower down in the air-way. Two rare cases of foreign body
aspiration with subglottic impaction invery young children (under 2 years of age)are described. In both the cases subglotticimpaction occurred consequent to at-tempted removal of foreign body by blindfinger sweeping. The clinical presentation,investigations, and management of theserare cases are discussed.(T Accid Emerg Med 1999;16: 150-153)
Keywords: foreign body; aspiration; larynx; children
on March 19, 2020 by guest. P
rotected by copyright.http://em
j.bmj.com
/J A
ccid Em
erg Med: first published as 10.1136/em
j.16.2.150 on 1 March 1999. D
ownloaded from

Laryngealforeign bodies in children
Aspiration of a foreign body occurs either withobjects that have been put into the mouth andaccidentally displaced posteriorly or withobjects that are unexpectedly encountered infood. In 1994, 3000 patients died fromsuffocation by ingested objects in the US mak-ing this the sixth leading cause of accidentaldeath.' As most aspirated foreign bodies enterthe bronchus after negotiating the glottis, thesubglottic impaction of aspirated foreign bodyis rare. However, the diagnosis becomes a chal-lenge when an object crosses the glottis andlodges in the subglottic region. Two cases ofsubglottic impaction of foreign bodies arediscussed.
Case reportsCASE 1A 1 year old boy choked after putting a smallfish bone into his mouth. His mother, who wit-nessed the incident, tried to remove the fishbone by putting her finger into the child'smouth, but was unsuccessful. The child thenhad a bout of coughing with blood tinged spu-tum and developed stridor. The child wastaken to a general practitioner for complaintsof noisy breathing and vomiting and oral ampi-cillin was prescribed. Three days later the childwas referred to the casualty department of ouruniversity hospital with the same complaints.On examination, the child was afebrile and hadminimal inspiratory stridor but no cyanosis.He refused oral feeds and had pooling of salivaand milk in the oral cavity. He also hadoccasional vomiting. The respiratory rate was22 breaths/min. There was no suprasternal orsubsternal recession. On auscultation there wasequal air entry in both the lungs with a roughinspiratory sound which was maximally heardover the trachea, but there was no palpatorytracheal thud (the impact of a moving trachealforeign body hitting against the wall of the tra-chea is felt by placing one finger on thetrachea). A radiograph of the soft tissue of theneck showed a radio-opaque shadow in thesubglottic region (fig 1). An emergency endos-copy was planned.Under all essential monitoring (electrocardio-
graphy, non-invasive blood pressure, and pulseoximeter), anaesthesia was induced with oxy-gen, nitrous oxide, and halothane. All prepara-tions were made to carry out tracheostomy orcricothyrotomy, if necessary. Once the childwas under anaesthesia direct laryngoscopy wasdone. No foreign body was found despite athorough direct laryngoscopic examination,therefore rigid bronchoscopy (using a 3.5 mmStorz bronchoscope) was used. Atropine 0.1mg and suxamethonium 10 mg were given tofacilitate introduction of the bronchoscope.
Ventilation was maintained by low frequencymanual jet ventilation (Sander's jet injector).Adequate depth of anaesthesia was maintainedwith entrainment of oxygen-halaothane mix-ture delivered through the breathing circuit(modified Ayer's T piece) connected to theventilation port of the bronchoscope. Musclerelaxation was maintained with atracurium.The sagittally impacted foreign body wasrevealed only when the bronchoscope was
Figure 1 Soft tissue radiograph of chest and the neckshowing radio-opaque shadow of the fish bone at subglotticregion in case 1.
I , .mmr-T 10 20 30
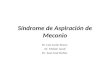
Figure 2 Subglottic foreign bodies:fish bone (case 1) andbroken tip ofplastic ball pen (case 2).
gently withdrawn and the left vocal cord wasretracted extremely laterally with the tip of thebronchoscope. The foreign body appeared likea "torn vocal cord" on end-on view through thebronchoscope. The fish bone, which wasdeeply embedded in the subglottic region, wasremoved with difficulty using forceps (fig 2).Check bronchoscopy showed oedema of thesubglottic region. The child was subsequentlyextubated and transferred to the intensive careunit for observation. Postoperatively the childwas treated with intravenous ampicillin anddexamethasone. Recovery was uneventful andthe child was discharged from the ward afterthree days. At follow up two weeks later, he wasasymptomatic and well.
CASE 2A 14 month old girl was brought to thecasualty department; she had been playingwith plastic toys, was knocked down by her sis-ter, and had then choked. The mother, whowitnessed the incident, suspected foreign bodyaspiration and explored the baby's mouth witha finger. She felt a sharp foreign body but wasunable to remove it. This manipulation re-sulted in blood stained vomiting followed bystridor. On examination the child had mildinspiratory and expiratory stridor but no
151
on March 19, 2020 by guest. P
rotected by copyright.http://em
j.bmj.com
/J A
ccid Em
erg Med: first published as 10.1136/em
j.16.2.150 on 1 March 1999. D
ownloaded from

Sharma, Sharma
cyanosis. The respiratory rate was 30 breaths/min. Auscultation of the chest showed bilateralconducted sounds. The child was taking foodorally. Radiography of the chest and soft tissueneck were normal. Under general anaesthesia(low frequency manual jet ventilation througha small catheter placed in the trachea) directlaryngoscopy did not show a foreign body. Arigid bronchoscopy (using 3.5 mm broncho-scope) revealed a greenish foreign body (aplastic tip of a ball pen) lying impacted at sub-glottic region; this was removed with forcepsafter dislodging and rotating it to the sagittalplane (fig 2). The anaesthetic technique usedwas the same as in the first case. A repeat bron-choscopy showed minimal subglottic oedema.Postoperatively the child was given ampicillinand dexamethasone and kept under observa-tion. She was sent home in good health aftertwo days.
DiscussionMost cases of foreign body aspiration occur inchildren less than 3 years of age.2A Childrentend to put objects impulsively into theirmouths and run the risk of aspiration. Mostaspirated foreign bodies cross the larynx andget lodged in the trachea or bronchus with anoccasional one remaining in the larynx. Thereported incidence of laryngeal lodgement ofaspirated foreign body varies from 2% to1 1%.58 Two kinds of foreign bodies may lodgein the larynx. One is a large object like a pieceof meat that may cause life threateningsupraglottic or glottic obstruction. This type ofaccident is more common in adults than inchildren and is not a diagnostic dilemma as itcauses complete laryngeal obstruction andsudden death. The National Safety Council inthe US has documented more than 240 deathsin children due to foreign body aspiration.'Nearly half (44%) of the cases of fatal chokingin childhood are due to aspiration of varioustypes of food (hot dogs 17%, candy 10%, nuts9%, and grapes 8%).9 The other kinds oflaryngeal foreign bodies are sharp and thinobjects. Such objects can get embedded easilyeither at the laryngeal inlet, usually gettinglodged between the vocal cords in the sagittalplane and causing non-fatal partial obstructionof the airways,'" or they can get embedded inthe subglottic region."The initial response to aspiration is choking
and coughing followed by stridor, sternalrecession, coughing, and hoarseness.'2 Themajority of aspirated foreign bodies caught inthe airways of children are spontaneouslyeliminated by coughing and at times laryngo-spasm may cause a brief period of cyanosis andtransient choking. Laryngeal foreign bodieswith sharp edges cause not only dyspnoea butalso odynophagia.1°
After passing the laryngeal inlet an aspiratedforeign body tends to be pushed upwards bythe protective cough reflex; sharp and flatobjects can get impacted in the subglotticregion, which is narrow and conical in shape."In neonates the larynx lies higher up at the levelof lower border of vertebral body of C4 anddoes not reach the adult position of C5-6 until
the age of 4 years.'4 In our patients parentsinstinctively attempted removal by blind fingersweeping, which probably pushed the thin andsharp foreign body deep into the subglotticregion. Therefore, blind finger sweeping shouldnever be done in infants and small children asthis manoeuvre can cause trauma and inducebleeding and what is initially a partial airwayobstruction may then become complete.'5Finger sweeping is rarely useful in adultchoking victims to remove foreign bodies lyingin the oral cavity or oropharynx before startingresuscitation. Instead, a properly performedHeimlich manoeuvre (with a combination ofabdominal thrusts and back blows to relievecomplete airway obstruction by a foreign body)is a much safer first aid procedure in youngnon-breathing, unconscious victims ofchoking.'6 This manoeuvre appears to beresponsible for many successful rescues result-ing in a marked decline in paediatric deathsfrom foreign body aspiration in the US.'
Several series have discussed non-lethallaryngeal obstruction8 "'. but none havespecially addressed subglottic foreign bodies.Recently Halvorson et al reported that subglot-tic foreign bodies pose a diagnostic challengeand in the majority of cases there is a delay indiagnosis.'3 Therefore, a high index of suspi-cion and specific questioning by the emergencydepartment physician should aid in differenti-ating patients with a laryngeal foreign bodyfrom acute epiglottitis, laryngotracheobronchi-tis, and asthma. Radiography of the soft tissueneck and chest may not show any abnormali-ties as only 10%-15% of aspirated foreignbodies are visualised radiologically.'8 In latepresentations the local response to the foreignobject is seen as a narrowing of the subglotticregion on radiography, which is definitive orsuggestive of foreign bodies.The removal of a laryngeal foreign body
under general anaesthesia is a potentially diffi-cult and hazardous operation especially in thecase of infants and young children.'3 '7 Adetailed preoperative assessment is essentialsince the anaesthesia, like the operative tech-nique, is determined by the site of the foreignbody and any secondary complications. Itrequires a team effort, which involves a skilledand experienced endoscopist and an equallyskilled and experienced anaesthetist and ascrub nurse. Close cooperation between theotolaryngologist and anaesthetist is essential tomaintain the airway at all times. The common-est method of removal of a foreign body in aspontaneously breathing patient is through arigid bronchoscope.2 '9 Muscle relaxation isusually advisable because the consequences ofa patient bucking violently during airwayinstrumentation, especially with a rigid bron-choscope, are severe, for example unnecessarybleeding and airway rupture.20 In smaller chil-dren a useful technique is to use the tip of arigid bronchoscope to retract the vocal cords.Thereby, a deeply embedded, subglottic, for-eign body is easily spotted. Complications afterbronchoscopy are uncommon, but laryngo-spasm and laryngeal oedema have been ob-served. Laryngospasm may be prevented by
152
on March 19, 2020 by guest. P
rotected by copyright.http://em
j.bmj.com
/J A
ccid Em
erg Med: first published as 10.1136/em
j.16.2.150 on 1 March 1999. D
ownloaded from

Painful elbow and von Willebrand's disease 153
adequate topical analgesia of the larynx andintravenous dexamethasone may help to re-duce laryngeal oedema.The emergency department physician
should, therefore, consider subglottic impac-tion of the aspirated foreign body in cases withsudden onset of dyspnoea with odynophagia.Soft tissue neck radiographs are the most use-ful investigation but should be done underproper supervision of the patient and in thepresence of a doctor capable of performing anemergency tracheostomy in a child. There isneed for a programme to educate the public inthe proper first aid measures when dealing withvictims of aspirated foreign bodies. This willprevent the kind of complications that wereseen in our cases.
1 National Safety Council. Accident facts. Itasca, IL: NationalSafety Council, 1995.
2 Banerjee A, Rao S, Khanna SK, et aL Laryngo-tracheo-bronchial foreign body in children. J Laryngol Otol1988;102: 1029-32.
3 Mu L, He P, Sun D. Inhalation of foreign bodies in Chinesechildren: a review of 400 cases. Laryngoscope 1991;lO1:657-60.
4 Svensson G. Foreign bodies in tracheobronchial tree.Special references to experience in 97 children. Int J Pedi-atr Otorhinolaryngol 1985;8:243-51.
5 Cohen SR, Lewis GB, Herbert WI, et al. Foreign bodies inairway. Ann Otol Rhinol Laryngol 1980;89:437-42.
6 Kim IG, Brummitt WH, Humphry A, et al. Foreign body inthe airway-a review of 202 cases. Laryngoscope 1973;83:347-54.
7 Krejovic B, Cvetkovic S, Popovic S. Les corps etrangers dularynx. journal Francais d'Oto-Rhino-Laryngologie 198 1;30:465-8.
8 Rothmann BF, Boeckman CR. Foreign bodies in the larynxand tracheobronchial tree in children. Ann Otol RhinolLaryngol 1980;89:434-6.
9 Harris CS, Baker SP, Smith GA, et al. Childhood asphyxia-tion by food-a national analysis and overview. JAMA1984;251:2231-5.
10 Darrow DH, Holinger LD. Foreign bodies of the larynx,trachea and bronchi. In: Bluestone CD, Stool S, KennaMA, eds. Paediatric otolaryngology. 3rd Ed. Philadelphia:WB Saunders, 1996:1394.
11 Brama I, Fearon B. Laryngeal foreign bodies in children. IntJf Pediatr Otorhinolaryngol 1982;4:259-65.
12 Esclamado RM, Richardson MA. Laryngotracheal foreignbodies in children. AmJDis Child 1987;141:259-62.
13 Halvorson D, Merritt RM, Mann C, et al. Management ofsubglottic foreign bodies. Ann Otol Rhinol Laryngol1996;105:541-4.
14 Battersby EF. Paediatric anaesthesia. Scott-Brown's otolaryn-gology. Volume 6. 5th Ed. London: Butterworth, 1987:503-26.
15 Standards and Guidelines for Cardiopulmonary Resuscita-tion (CPR) and Emergency Cardiac Care (ECC). NationalAcademy of Sciences-National Research Council. JAMA1986;255:2905-89.
16 Heimlich HJ. A life-saving maneuver to prevent food-choking. JAMA 1975;234:398-401.
17 Kent SE, Watson MG. Laryngeal foreign bodies. J LaryngolOtol 1990;104:131-3.
18 Moskowitz D, Gardiner U, Sasaki CT. Foreign body aspira-tion. Potential misdiagnosis. Arch Otolaryngol Head NeckSurg 1982;108:806-7.
19 McGuirt WF, Holmes KD, Feehs R, et al. Tracheobronchialforeign bodies. Laryngoscope 1988;98:615-8.
20 Woods A. Paediatric bronchoscopy, bronchography, andlarygoscopy. In: Berry FA, ed. Anaesthetic management ofdifficult and routine paediatic patients. New York: ChurchillLivingstone, 1986: 189-247.
An acutely painful elbow as a first presentation ofvon Willebrand's disease
H D M Poncia, J Ryan
Department ofAccident andEmergency Medicine,Royal Sussex CountyHospital, EasternRoad, BrightonBN2 5BEH D M PonciaJ Ryan
Correspondence to:Mr Ryan (e-mail:[email protected]).
Accepted 7 August 1998
AbstractA 26 year old woman presented to theaccident and emergency department witha painful right elbow. There had been nohistory of trauma. Clinical examinationsuggested an effusion, which was con-firmed on radiological examination. Herelbow was aspirated and revealed a hae-marthrosis. Subsequent investigations re-vealed a diagnosis of von Willebrand'sdisease (vWD). A spontaneously occur-ring effusion of the elbow may be due to ahaemarthrosis. Aspiration of blood in theabsence oftrauma may lead to a diagnosisof an occult coagulopathy in addition torelieving pain. The diagnosis and treat-ment ofvWD is discussed.(JAccid Emerg Med 1999;16:153-154)
Keywords: von Willebrand's disease; haemarthrosis;elbow
Case reportA 26 year old woman, normally fit and well,presented to the accident and emergency(A&E) department with a painful right elbow.Symptoms had developed spontaneously over-
night and she attributed them to sleeping in anawkward position. Her elbow was held in aflexed position. Flexion and extension wereboth restricted. Radiographs were taken whichshowed prominent anterior and posterior fatpads (fig 1 ). A synovial effusion was suspectedand her elbow was aspirated to providesymptomatic relief. Surprisingly, aspiration ofthe joint produced 7 ml of blood. She wasgiven a broad arm sling to rest her elbow. Oneweek later her elbow was much improved andfull extension was only limited by 10 degrees.At six weeks her elbow was back to normal.On further questioning the patient gave a
history of occasional bruising and heavyperiods during the previous 2-3 years. She wason no medication. Her mother also had ahistory of bruising. In view of this history andthe findings of a spontaneous haemarthrosis,she was referred for a haematological assess-ment.
Investigations revealed a normal full bloodcount, liver function, biochemistry, inter-national normalised ratio, and activated partialthromboplastin time ratio. However von Will-ebrand factor (vWF) antigen and vWF activitywere low, 31 IU/100 ml (50-200) and 29
on March 19, 2020 by guest. P
rotected by copyright.http://em
j.bmj.com
/J A
ccid Em
erg Med: first published as 10.1136/em
j.16.2.150 on 1 March 1999. D
ownloaded from