Embed Size (px)
Citation preview

Offloading the Diabetic Foot Ulcer
The Quest forCompliance and Efficient
Healing

“
Desmond Bell, DPM, CWSCo-Founder

First Coast CardiovascularInstitute, P.A.
Jacksonville, FL

Disclosures
• Organogenesis: Speaker’s Bureau• DermaSciences: Consultant• 3M: Consultant• Alliqua: Consultant

Offloading
• Goals of offloading areredistribution of focalpressure from onespecific area to a broadarea of dispersed force.
• This allows for thephases of wound healingto proceed withoutdisruption from groundreactive force or otherexternal source ofpressure.
Total Contact Cast

Offloading
• The first step inOffloading isdebridement
• “Edge effect”1• Macerated tissue
represents peak pressureand area of senescentcells, reduced mitoticactivity
• Must debrideaggressively
1. Armstrong DG, Athanasiou KA. “The edge effect: how and why wounds grow in size and depth”. Clin Pod Med Surg. 1998; 15 (1): 105-8

Offloading
• Wouldn’t send patientshome with a scalpel withinstructions to performself debridement
• For offloading to beoptimal, must be 24/7and tailored to meetneeds of patient
Example of “Soft” Total Contact Cast

Dr. Paul Brand
• First used TCC in theUnited States in 1965 inCarville, LA at theNational Hansen’s DiseaseCenter
• Long list of studiesdocumenting the successand utility of the TCC2,3
2. Birk, JA. The Contact Cast: an updated case study report. Wounds 2000; 12(2):26-313. Bell D: Evidence Based Rationale for Offloading Treatment Modalities. Surg Technology Int XVll. May 2008 113-117;

Total Contact Cast
The “Gold Standard”
Perceived as difficult to applyand time consuming
Must use caution in patientselection-not everyone is acandidate for TCC
CPT: 29445 use L or R modifierICD-9: use 707.15 or 250.8x when coding for ulcers

Total Contact Cast
• Despite efficacy andrecognition of its value,utilization remains low
• Diabetes Care in 2008,Stephanie Wu, DPM, etal, reported the results ofa survey of 901 clinicalpractices within theUnited States4
• This study revealed thatonly 1.7 percent of thecenters surveyed utilizedthe total contact cast
4. Wu SC, Jensen JL, Weber AK, Robinson DE, Armstrong DG. Use of pressure offloading devices in diabetic foot ulcers. do we practice what we preach? Diabetes Care. 2008; 31(11):2118–2119.

Total Contact Cast
• The USWR study,which included108,000 patientvisits in 18 woundcenters in 16states, revealedthat only 6% ofpatients with DFUswere treated withTCC.5 5. Fife CE, Carter MJ, Walker D: Why is it so hard to do the right thing in wound care? Wound Repair Regen 18: 154, 2010.

The Management of Diabetic Foot Ulcers through Optimal
Off-loading
Building Consensus Guidelines and PracticalRecommendations to Improve OutcomesJournal of the American Podiatric Medical
Association. Vol 104. No. 6. Nov/Dec 2014

Method
• The panelperformed aliterature search ofPubMed articles forevidence on off-loading.
• Inclusion criteriawere based uponthe support of theconsensusstatement.
• Fromapproximately 90selected studies, 64studies wereincluded in theevidence tables,along with 3additionalpublications knownby the authors butnot found in theliterature searches



Results
• Eight evidence-based consensus guidelinesand core recommendations resulted from thecollaborative work of the panel.
• Each statement references the level of theevidence and the strength of therecommendation - e.g., Moderate/Strong.


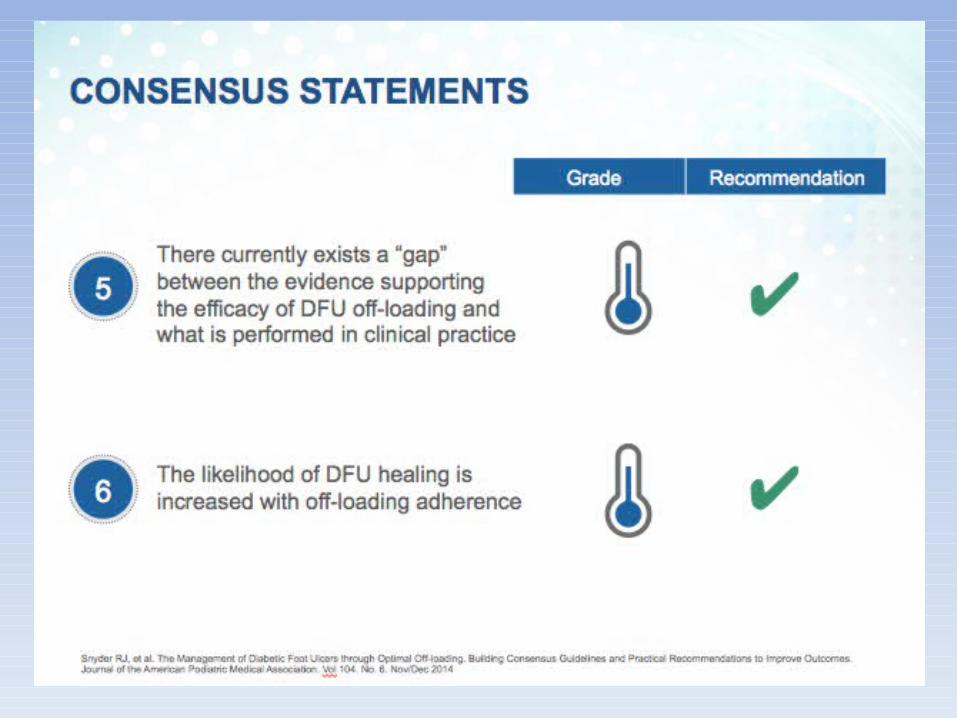






Consensus on Optimal DFU Offloading:Conclusions
• Likelihood ofhealing is increasedwith off-loadingadherence (whichis one of the reasonsthat TCC is soeffective andremains preferredstandard” of care).
• Evidenceconsistentlydemonstrated thatwhen off-loading isintegrated into thepatient encounterprocess andprovided at eachvisit, the likelihoodof healing a DFU isgreater and thechance forcomplications isreduced.
• Off-loading is alsoconfirmed to be acost-effectivetreatment forDFUs.
• There currentlyexists a gap betweenwhat the evidencesupports in regardto the efficacy ofDFU off-loadingand what isperformedin clinical practice.
• More education isneeded of both theclinician and thepatient to increaseoff-loading use.
• TCC remains thepreferred standardof care, but the useof devices renderedirremovable and/orthe i-TCC approachare supported byevidence to be aseffective as theconventionalapproach to TCC

Total Contact Cast
Contraindicated in:
Ischemic ulcers
Heavily exudative ulcers
Unsteady gait
Typically change onceweekly

Total Contact Cast
Indications• Chronic plantar ulcer of
foot or toe• Charcot arthropathy in
Acute or reparative phase
Contraindications• Infection• Significant vascular
disease• Highly exudative ulcer• Unsteady gait/concern
for falling• Claustrophobia

TCC would be Contraindicatedin this Particular Case
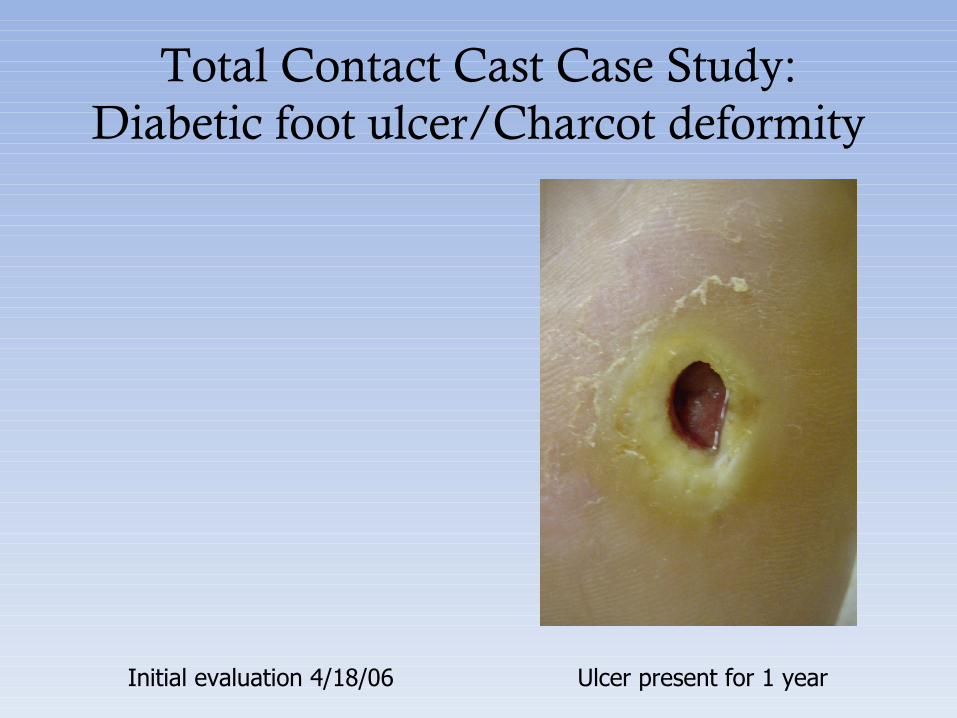
Total Contact Cast Case Study:Diabetic foot ulcer/Charcot deformity
Initial evaluation 4/18/06 Ulcer present for 1 year

Total Contact Cast Case Study:Diabetic foot ulcer/Charcot deformity
Apligraf application 4/25/06

Total Contact Cast Case Study:Diabetic foot ulcer/Charcot deformity
Resolved, 5/31/06
4/18/06

Utilization of Total Contact Cast to Treat Diabetic Foot Ulcerwith Charcot Deformity
Case Study #2• 47 year old white male• >17 month history of right
plantar ulcer• Prior treatment included
debridement, becaplermin gel:5 different clinicians
• Charcot foot with “Rockerbottom”
• Type 1 DM, HTN• Patient lost job as result of non-
healing wound

Utilization of Total Contact Cast to Treat Diabetic Foot Ulcerwith Charcot Deformity
Case Study #2

TCC-EZ® Cast System
• Quick application• Minimal learning curve• Non-removable• Indications and
contraindications as withtraditional TCC
Moderate Recommendation

Charcot Resistant Orthotic Walker
• Charcot Restraint Orthotic Walker
(CROW), a custom orthosis used intreating Charcot degeneration of thefoot and ankle.
• Custom-molded boot incorporates abivalve custom pretibial andposterior shell with rocker bottomsole that is designed to offload thefoot similarly to a total contact cast.
• Offers accommodation for eachpatient's particular needs.
• This product can also be used forpostsurgical protection andtransition following foot and anklereconstruction.
Removable
LOW Recommendation

Custom Ankle-Foot Orthoses (AFO’s)
• Use when pressure relief isrequired, but circumstancesmake use of more simplemethods impractical
• Requires custom molding forfitting of inner orthosis as wellas creation of custom boot
• Requires specialized fitting fromPedorthist or Orthotist
• Costly, >$1,000 per • Must be replaced periodically
LOW Recommendation

Bledsoe Boot
• Aluminum boot shell and uprightsystem that, unlike plastic boots,can be reformed to fit virtually anyleg or ankle shape.
• Can be removed for daily cleaning,dressing changes and medication.
• Triple density footbed comprised ofan auto-molding innersole and anew pre-molded dual densitymidsole is designed to evenlydistribute weight across the entirebottom surface of the foot, and upto one inch (2.5 cm) on all sides ofthe foot.
• The innersole molds itself to thefoot shape while the midsole isspecially designed to providemaximum perimeter loadingsuperior to a total contact cast.
Removable
LOW Recommendation

Active Offloading Walker
• Fleschli, et al found thedevice to have the lowestmean peak pressure undermetatarsal heads of alldevices tested, includingTCC4
• Contains hexagonal plugswhich act as a multi-density pressure reliefinsert
4. Fleschli JG, Lavery LA, Vela SA, et al. Comparisom of strategies for reducingPressure at the site of neuropathic ulcers. JAPMA 87 (10): 466-72, 1997
LOW Recommendation

DH Pressure Relief Walker
• Lavery, et al, found DHPressure Relief Walker tobe identical to TCC inpressure reduction at siteof ulcerations on sole5
• Removable
5. Lavery, LA, Vela, SA, Lavery, DC, Quebedeaux TL. Reducing dynamic foot pressuresIn high-risk diabetic subjects with foot ulcerations: a comparison of treatments. Diabetes Care 19 (8): 818-21, 1996
LOW Recommendation

CAM Walker
• Lavery, et al, found CAMWalkers reduce forefootplantar pressure bykeeping ankle at 90degrees, limits propulsion5
• Tested 4 different brands• Removable
5. Lavery, LA, Vela, SA, Lavery, DC, Quebedeaux TL. Reducing dynamicfoot pressuresIn high-risk diabetic subjects with foot ulcerations: a comparison oftreatments. Diabetes Care 19 (8): 818-21, 1996
Baseball Head Coach Cam Walker, Indian HillsCommunity College. Centerville, Iowa
LOW Level of Evidence

Instant Total Contact Cast
• Armstrong, et al devised theInstant TCC to address the issueof compliance6
• Combines benefit of reducedforefoot pressure from wearingCAM walker with inability toremove device of TCC
• Apply Cohesive bandage orPlaster of Paris over RemovableCAM walker
6. Armstrong, DG, Short B, , et al. Technique for fabrication of an “Instant TotalContact Cast” for treatment of neuropathic diabetic foot ulcers. JAPMA 92 (7):405-408, 2002.

“Half-Shoe”
• Darco originally created for postforefoot surgery
• Ortho-wedge, IPOS• Generally well tolerated• Alters gait, may cause
contralateral symptoms• Not recommended for patients
with unsteady gait• Fleschli, et al, found to be least
effective method in offloadingcomparison study7
7. Fleschli JG, Lavery LA, Vela SA, et al. Comparisom of strategies for reducingPressure at the site of neuropathic ulcers. JAPMA 87 (10): 466-72, 1997 VERY LOW Recommendation

OrthoWedge Shoe
• The OrthoWedge Shoe has beenclinically proven to effectively reduceweight bearing pressure from theforefoot to promote proper healing.
• Needleman and Lair found the device tobe useful in healing of ulcers, in separatestudies8,9
• Needleman also reported a 30%complication rate, including balanceproblems, falls and joint pain8
• Promotes healing by reducing weightfrom the forefoot and may be used forany condition from the metatarsal headsdistally in which it is desirable to reducebody weight such as ulcers, infections,trauma and surgery.
• 15º dorsi-angle shifts weight back to themidfoot and heel.
8. Needleman RL. Successes and pitfalls in the healing of neuropathic forefoot ulcerations With IPOS Postoperative shoe. Foot Ankle Int 18: 412-417. 1997
9. Lair c. Use of IPOS shoe in the management of patients with diabetes mellitus. Cleveland. Cleveland Clinic Foundation; 1992
LOW Recommendation

Freedom Leg Offloading Brace
• No personalexperience with thismethod
• No scholarly papersor reviews of theproduct

Roll-a-bout/Knee Walker
• Gaining widerutilization
• Easy to use• Rentals available• Some insurance
coverage• Ebay, Craig’s list,
etc.

External Fixation
• Advances in frametechnology ismaking externalfixation more userfriendly to patientand surgeon alike
• Patient mayambulate
• No wires throughleg Wright Medical Sidekick EZ Frame

“SOFT Total Contact Cast”
• “Real world” solution to offloading,addresses gait instability, reducesrisk of falling (safety) and providesFORCED COMPLIANCE
• Provides critical offloading in preand post skin substitute setting
• Quick application• Well tolerated• Reduction in inherent edema• Minimal disuse atrophy or hip
dysplasia over thousands ofapplications
• May use with half shoe ortraditional post-op shoe
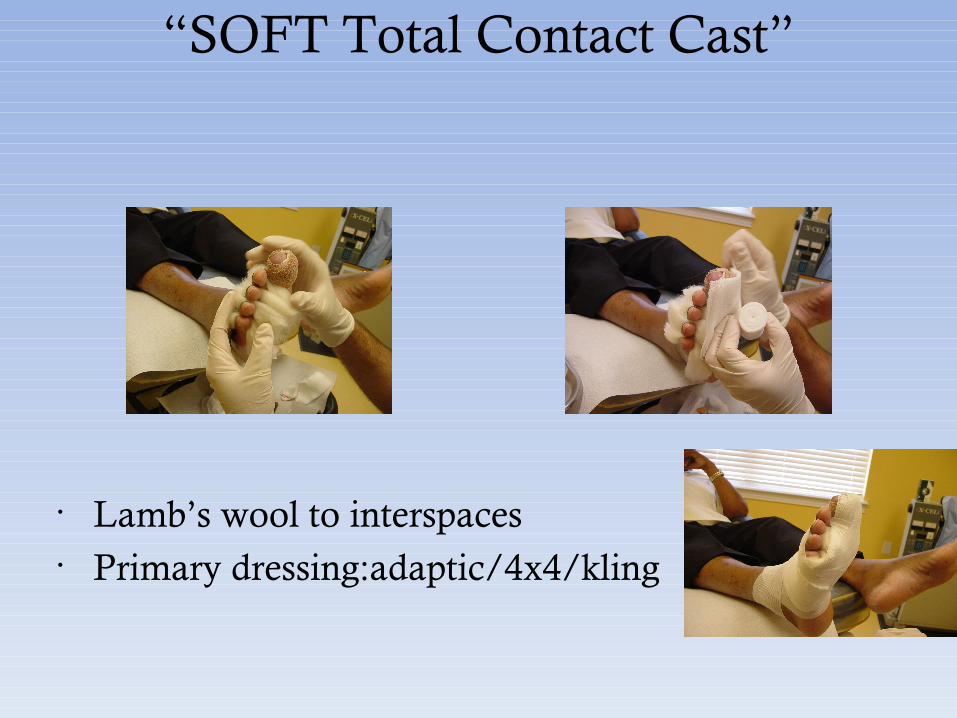
“SOFT Total Contact Cast”
• Lamb’s wool to interspaces• Primary dressing:adaptic/4x4/kling

“SOFT Total Contact Cast”
• Webril or cast padding applied • ¼” to ½” adhesive felt to area surrounding underlying ulcer• Pad arch area with additional folded 4x4 gauze

“SOFT Total Contact Cast”
• Secure adhesive felt with additional cast padding• Fashion a plantar plate from 1 roll of cast padding

“SOFT Total Contact Cast”
• Secure plantar platewith additional castpadding wrap

“SOFT Total Contact Cast”
• Apply paste bandage, i.e. Unna boot to secure padded layers (mayapply to ankle or below knee level)
• Cut out area at anterior ankle for improved comfort and to relievepressure from underlying neurovascular structures

“SOFT Total Contact Cast”

“SOFT Total Contact Cast”
Apply self adherent elastic wrap to complete cast; 1” between toes to reduce shifting

“SOFT Total Contact Cast”
• Contraindicated in:
Ischemic ulcers
Heavily exudative ulcers

Soft Total Contact Case Study:Diabetic Foot Ulcer
• Patient is a 72 year oldfemale with submetatarsalone diabetic foot ulcer, onsetfirst week of April 2003
• Hospitalized for cellulitis;osteomyelitis ruled out
• PMH: Type 2 DM, HTN,Hypothyroidism, Priordiabetic foot ulcers
May 9, 20031.6cm x 1.4cm

Soft Total Contact Case Study:Diabetic Foot Ulcer
• Soft total contact cast utilized for offloading ofApligraf application
• Bacterial burdencontrolled with silverdressing applied to ulcer inconjunction with soft totalcontact cast
• Soft total contact cast changed twice weekly
May 30, 20031.0cm x 0.8cm
Ulcer measured1.6cm x 1.4cm on May 9, 2003
Area of Newepithelialization

Soft Total Contact Case Study:Diabetic Foot Ulcer
• Apligraf applied on June6, 2003
• Steri-strips used to securegraft to ulcer
• Soft total contact cast used to offload
• Post-op shoe worn foradditional offloading
June 6, 20030.8cm x 0.8cm

Soft Total Contact Case Study:Diabetic Foot Ulcer
• Patient missed originallyscheduled “first dressingchange” appointment onJune 10, 2003
• Status post skinsubstitutemeasurements: June 16,2003 0.3cm x 0.3cm(first dressing change)
• Dressing change #2 onJune 20, 2003
• Soft total contact castutilized
June 20, 20030.1cm x 0.1cm

Soft Cast Information and Video
www.Fight4MyFeet.com

Thank You





























