Embed Size (px)
Citation preview

Ocular Toxicity in BRAF Mutant Cutaneous MelanomaPatients Treated With Vemurafenib
CHRISTINA H. CHOE, GRANT A. MCARTHUR, IVOR CARO, JOHN H. KEMPEN, AND RAVI K. AMARAVADI
� PURPOSE: To determine the frequency of ocularadverse effects associated with vemurafenib (PLX4032)treatment for metastatic cutaneous melanoma.� DESIGN: Retrospective review of the clinical study re-ports from the clinical pharmacology, phase 1, phase 2,and phase 3 trials of vemurafenib.� METHODS: The vemurafenib clinical trials were amulticenter series involving adult patients with histolog-ically confirmed, BRAFV600 mutation–positive, unre-sectable, stage IIIC or IV melanoma. A total of 855patients were enrolled in the trials: 568 patients weretreated with vemurafenib and 287 patients were treatedwith dacarbazine.� RESULTS: Among the 568 patients treated with vemur-afenib, ocular adverse effects developed in 22% (95%confidence interval [CI], 18.5–25.6). The most commonocular diagnosis was uveitis (4.0%; 95% CI, 2.6–6.0),followed by conjunctivitis (2.8%; 95% CI, 1.6–4.5)and dry eyes (2.0%; 95% CI, 1.1–3.7). All were success-fully managed while vemurafenib therapy was continued.� CONCLUSIONS: Ocular adverse events and symptomsmay be seen in more than one-fifth of patients beingtreated with vemurafenib. However, vemurafenib canbe continued while the ocular symptoms are beingmanaged. The pathogenesis of ocular symptoms in this pa-tient population is unclear; additional studies arenecessary. (Am J Ophthalmol 2014;-:-–-.� 2014 by Elsevier Inc. All rights reserved.)
METASTATIC CUTANEOUS MELANOMA HAS
historically been associated with a dismal prog-nosis. Despite advances in surgical, chemothera-
peutic, and radiation techniques, the overall survival rate
Accepted for publication Jul 3, 2014.From the Departments of Ophthalmology and the Scheie Eye Institute,
University of Pennsylvania Perelman School of Medicine, Philadelphia,Pennsylvania (C.H.C., J.H.K.); Peter MacCallum Cancer Centre, EastMelbourne, Victoria, Australia (G.A.M.); Genentech, South SanFrancisco, California (I.C.); Center for Clinical Epidemiology andBiostatistics and Department of Biostatistics and Epidemiology,University of Pennsylvania Perelman School of Medicine, Philadelphia,Pennsylvania (J.H.K.); and Department of Medicine, Abramson CancerCenter, University of Pennsylvania Perelman School of Medicine,Philadelphia, Pennsylvania (R.K.A.).
Christina H. Choe is currently affiliated with Carolina Ophthalmology,Asheville, North Carolina.
Inquiries to Ravi K. Amaravadi, Abramson Cancer Center, PerelmanCenter for Advanced Medicine, 3400 Civic Center Boulevard,Philadelphia, PA 19104; e-mail: [email protected]
0002-9394/$36.00http://dx.doi.org/10.1016/j.ajo.2014.07.003
� 2014 BY ELSEVIER INC.
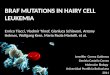
for metastatic cutaneous melanoma has remained largelyunchanged in the past 20 years.1 Recently, therapeutictargeting of the mitogen-activated protein kinase(MAPK) pathway (the RAS-RAF-MEK–extracellularregulated kinase [ERK] cascade) has shown significant suc-cess in improving clinical outcomes in patients withadvanced cutaneous melanoma (Figure 1).In 2002, Davies and associates made the landmark dis-
covery of activating V600 mutations in BRAF (v-raf mu-rine sarcoma viral oncogene homolog B1) in the MAPKpathway.2 This mutation most commonly is a single substi-tution of valine 600 to glutamic acid in the activating re-gion of the kinase domain (BRAFV600E). The BRAFV600E
and other BRAFV600 mutations are found in 40%–60% ofmelanomas and result in RAS-independent activation ofRAF kinase.2,3 This causes constitutive phosphorylationof downstream ERK, which leads to the transduction ofintracellular signals that promote cell proliferation andcancer development.Vemurafenib is a potent and specific oral BRAFV600 in-
hibitor that has produced more than a 50% objectiveresponse rate in phase 1 and 2 trials.4,5 In a randomizedphase 3 trial comparing vemurafenib and the alkylatingchemotherapy agent dacarbazine, vemurafenib had arelative reduction in the risk for death of 63%.6 This dis-covery led to agent approval by the US Food and DrugAdministration (FDA) and widespread clinical use aroundthe world. The adverse effects most commonly reportedwith vemurafenib therapy are cutaneous and includerash, alopecia, pruritus, hyperkeratosis, and an increasedincidence of keratoacanthoma and squamous cell carci-noma. Other common adverse effects include arthralgia,nausea, fatigue, diarrhea, headache, vomiting, lymphope-nia, and neutropenia.7
Little has been written in the literature about the ocularadverse effects of vemurafenib. Herein we describe the inci-dence of ocular adverse effects within the 4 published clin-ical trials of vemurafenib.
METHODS
CLINICAL STUDY REPORTS FROM CUTANEOUS MELANOMA
patients treated with therapeutic doses of vemurafenib(>240 mg orally 2 times daily) who were enrolled in anyof the following clinical trials—clinical pharmacology,phase 1 (PLX-06-02),4 phase 2 (BRAF Inhibitor in
1ALL RIGHTS RESERVED.

Receptor tyrosine kinase
vemurafenib
Nucleus
ERK
MEK
NRAS
CRAFmuBRAF
FIGURE 1. Mitogen-activated protein kinase (MAPK)pathway that is targeted in BRAF-mutant melanoma patientstreated with vemurafenib. ERK [ extracellular signal-regulated kinase; MEK [ MAPK kinase; muBRAF [ mutantB-raf.
TABLE 1. Incidence of Ocular Adverse Effects Observed in BRAF M
Clinical T
Trial CPS Phase 1
Drug Vem (n ¼ 52) Vem (n ¼ 4
Patients with >_1 ocular adverse effect, n (%) 3 (5.8) 25 (52.1
Diagnosis, n (%)
Uveitis 0 7 (14.6
Conjunctivitis 0 6 (12.5
Dry eyes 1 (1.9) 4 (8.3)
Episcleritis 0 0
Keratitis 0 1 (2.1)
Blepharitis 0 0
Retinal vein occlusion 0 0
Other eye disordersb 0 3 (6.25
Symptoms, n (%)
Blurred vision 0 4 (8.3)
Ocular discomfortc 1 (0.3) 2 (4.2)
Photophobia 0 7 (14.6
Ocular injection 1 (0.3) 0
Tearing 0 2 (4.2)
Periocular edema 0 0
Diplopia 0 1 (2.1)
Floaters 0 2 (4.2)
CPS ¼ clinical pharmacologic study; DTIC ¼ dacarbazine; Vem ¼ vemaThree patients in the phase 3 study experienced 2 occurrences of uvbOther reported ocular adverse events include asthenopia, discharge
subconjunctival hemorrhage, cataract, chalazion, scintillating scotoma,
irritation, reduced visual acuity, visual impairment, and vitreous floaters.cIncludes pain, irritation, and itching.
2 AMERICAN JOURNAL OF
Melanoma [BRIM-2]),5 and phase 3 (BRIM-3) studies,6
together with the 3-month safety update (for the clinicalpharmacology, BRIM-2, and BRIM-3 studies only [June2011])—were used to identify patients who had experi-enced ocular adverse events during treatment with vemur-afenib. For the BRIM-3 study, patients who received theactive comparator dacarbazine during the study and whoexperienced ocular adverse events were also identified.For all patients enrolled in these studies, ocular adverse ef-fects were recorded according to Common TerminologyCriteria for Adverse Events (CTCAE), version 3.0. Inparticular, the patient listings from each report were retro-spectively reviewed to identify all relevant patients. Proto-cols for the studies were approved by the appropriateinstitutional review boards at the time of the study;conformed to all country, federal, or state laws; and adheredto the tenets of the Declaration of Helsinki. (For the spe-cific review boards for each institution, refer to the reportsof the phase 1, 2, and 3 trials.4–6) All patients signedwritten informed consent prior to enrollment in theclinical trials. De-identified patient information thatconformed to Health Insurance Portability and Account-ability Act (HIPAA) guidelines was available for retro-spective analysis for this study; all patients enrolled in
utant Cutaneous Melanoma Patients Enrolled In Vemurafenib
rials
Phase 2 Phase 3 Total
8) Vem (n ¼ 132) Vem (n ¼ 336) DTIC (n ¼ 287) Vem (n ¼ 568)
) 35 (26.5) 62 (18.5) 10 (3.5) 125 (22.0)
) 7 (5.3) 9a (2.7) 0 23 (4.0)
) 0 10 (3.0) 1 (0.3) 16 (2.8)
1 (0.8) 6 (1.8) 0 12 (2.1)
3 (2.3) 0 0 3 (0.5)
0 1 (0.3) 0 2 (0.4)
0 3 (0.9) 0 3 (0.5)
1 (0.8) 0 0 1 (0.2)
) 7 (5.3) 4 (1.2) 12 (4.2) 14 (2.7)
8 (6.1) 9 (2.7) 2 (0.7) 21 (3.7)
2 (1.5) 15 (4.5) 5 (1.7) 20 (3.5)
) 4 (3.0) 6 (1.8) 2 (0.7) 17 (3.0)
4 (3.0) 11 (3.3) 1 (0.3) 16 (2.8)
3 (2.3) 6 (1.8) 0 11 (1.9)
3 (2.3) 4 (1.2) 0 7 (1.2)
2 (1.5) 2 (0.6) 1 (0.3) 5 (0.9)
0 2 (0.6) 1 (0.3) 4 (0.7)
urafenib.
eitis; therefore, there were 12 events among a total of 9 patients.
, ectropion, scleral cyst, mydriasis, retinal pigment epitheliopathy,
corneal lesion, eye pain, photophobia, blurred vision, diplopia, eye
--- 2014OPHTHALMOLOGY

TABLE 2. Demographics of BRAF Mutant Cutaneous Melanoma Patients in Whom Uveitis Developed During a Vemurafenib ClinicalTrial
Phase 1 Phase 2 Phase 3 Total
Uveitis (n ¼ 7) Uveitis (n ¼ 7) Uveitis (n ¼ 9)a Uveitis (n ¼ 23)
Median age (range) (y) 56 (22–68) 43 (24–72) 57 (41–76) 56 (22–76)
Male sex, n (%) 2 (29) 3 (43) 7 (78) 12 (52)
ECOG PS,b n (%)
0 5 (71) 6 (86) 7 (78) 18 (78)
1 2 (29) 1 (14) 2 (22) 5 (28)
Stage of metastatic melanoma,c n (%)
M1c 5 (71) 4 (57) 7 (78) 16 (70)
M1b 0 0 1 (11) 1 (4)
M1a 2 (29) 3 (43) 1 (11) 6 (26)
Unresectable IIIC 0 0 0 0
Prior therapies, n (%)
0 2 (28.6) 0 0 2 (8.7)
1 3 (42.9)d 4 (57.1) n/a 7 (30.4)
2 2 (28.6) 3 (42.9) n/a 5 (21.7)
>_3 0 0 n/a 0
Other vemurafenib-related toxicities, n (%)
Rash 6 (85.7) 2 (28.6) 4 (44.4) 12 (52.2)
Arthralgia 5 (71.4) 6 (85.7) 2 (22.2) 13 (56.5)
Fatigue 4 (57.1) 4 (57.1) 5 (55.6) 13 (56.5)
SCC/keratoacanthoma 4 (57.1) 1 (14.3) 3 (33.3) 8 (34.8)
ECOG PS ¼ Eastern Cooperative Oncology Group performance status; SCC ¼ squamous cell carcinoma.aThree patients in the phase 3 study experienced 2 occurrences of uveitis; therefore, there were 12 events among a total of 9 patients.bGrade 0¼ fully active, able to carry on all predisease performancewithout restriction; grade 1¼ restricted in physically strenuous activity but
ambulatory and able to carry out work of a light or sedentary nature (eg, light housework, office work).cM1a¼metastases to skin, subcutaneous, or distant lymph nodes; M1b¼metastases to lung; M1c¼metastases to all other visceral sites or
distant metastases to any site combined with an elevated serum lactate dehydrogenase; IIIC¼ clinically palpable lymph node, or unresectable
locally advanced disease. Staging criteria follow the American Joint Committee on Cancer (AJCC) TNM staging system.dOne patient required 2 consecutive courses of interleukin 2 therapy; however, this was counted as 1 therapy type.
the vemurafenib clinical trials consented to use of thisinformation. The clinical trials in this manuscript wereregistered with the National Institutes of Health and canbe found on the www.clinicaltrials.gov website with thefollowing identifiers: NCT00405587, NCT00949702,NCT01006980, and NCT01107418.
Uveitis was the most common ocular adverse event inthis study population; therefore, this subgroup wasanalyzed separately. The following preferred terms wereincluded in the definition of uveitis: uveitis, intermediateuveitis, iritis, iridocyclitis, and vitritis. After patients withuveitis were identified, key baseline characteristics of thestudy patients were compared and the treatment methodswere recorded.
RESULTS
AMONG 855 PATIENTS ENROLLED IN THE VEMURAFENIB
clinical trials, 568 were treated with vemurafenib and
VOL. -, NO. - UVEITIS ASSOCIATED WIT
287 were treated with dacarbazine (Table 1). An ocularadverse effect developed in 125 of the 568 patients(22.0%) who were treated with vemurafenib (95% confi-dence interval [CI], 18.5–25.6). Among the 287 patientstreated with dacarbazine, 10 (3.5%; 95% CI, 1.7–6.3)reported ocular adverse effects (Table 1).Of a total of 568 patients, uveitis (4.0%; 95% CI, 2.6–
6.0) was the most common ocular diagnosis associatedwith vemurafenib therapy, occurring in 23 patients,followed by conjunctivitis in 16 patients (2.8%; 95% CI,1.6–4.5) and dry eyes in 12 patients (2.0%; 95% CI, 1.1–3.7). Patients commonly reported blurred vision, oculardiscomfort, photophobia, redness, tearing, and edema—symptoms consistent with ocular inflammation.
� PATIENTS WITH VEMURAFENIB-ASSOCIATED UVEITIS:
Across the 4 clinical trials, 23 patients had uveitis duringthe study period. The clinical demographics of thispatient subset were similar to the demographics of thegeneral population of these clinical trials (Table 2).Mild to moderate uveitis (CTCAE grade 2 or 3) was
3H BRAF INHIBITION

Days on vemurafenib
6005004003002001000
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
Uve
itis
epis
ode
FIGURE 2. Time to uveitis episode in BRAF-mutant melanoma patients treated with vemurafenib. The number of days until onset ofsymptoms for each episode of uveitis experienced byBRAFmutant cutaneousmelanoma patients treated in vemurafenib clinical trials.
diagnosed a median of 117 days after initiation of vemur-afenib therapy (range, 7–550 days) (Figure 2 and Table 3).No cases of grade 4 uveitis (blindness) were observed.Recurrent uveitis developed in 4 patients during the studyperiod. All patients continued vemurafenib; however, in 6of the 23 patients (26%), the dose was reduced because ofthe diagnosis of uveitis. Uveitis was treated successfully inthe majority of patients by use of standard local therapies,including topical or periocular corticosteroids, cyclople-gic agents, and agents to lower intraocular pressure asneeded. In a subset of patients, intermittent systemic orintraocular steroids were used. In all cases of uveitis, itwas possible to continue vemurafenib.
� PATIENTS WITH OTHER SEVERE OCULAR ADVERSEEFFECTS: Only 3 patients discontinued vemurafenib dur-ing the study period because of ocular adverse effects: uni-lateral ischemic central retinal vein occlusion developedin 1 patient; double vision developed in 1 patient andresolved after discontinuation of the medication; and
4 AMERICAN JOURNAL OF
persistent ocular hyperemia and conjunctivitis developedin 1 patient and endured after discontinuation of the studymedication.
DISCUSSION
THESE RESULTS SHOWTHATOCULARADVERSE EVENTS ARE
commonly observed with vemurafenib therapy. Althoughmany of the ocular adverse events seen are not usually se-vere, uveitis is potentially blinding. However, cases of uve-itis in this study were manageable without cessation oftherapy in every instance; only 6 of 23 patients (26%)decreased or temporarily discontinued their dose. Therewere more cases of uveitis in the phase 1 trial of vemurafe-nib than in the other trials. The eligibility criteria for all ofthe trials and demographics of the population of patientswere similar except that the patients in the phase 1 trialwere, in general, more heavily pretreated than patients in
--- 2014OPHTHALMOLOGY

TABLE 3. BRAF Mutant Cutaneous Melanoma Patients With Vemurafenib-Associated Uveitis
Uveitis Case Trial Study Day–Onset of Uveitis Concomitant Treatment Dose Reduced?
1 Phase 1 7 Periocular corticosteroid injections,
corticosteroid drops
Yes
2 Phase 1 259 Corticosteroid drops No
3 Phase 1 117 Corticosteroid drops No
4 Phase 1 550 Corticosteroid drops, antibiotic ointment No
5 Phase 1 408 None reported No
6 Phase 1 229 Corticosteroid drops No
7 Phase 1 365 Corticosteroid drops No
1 Phase 2 68 and 81 Artificial tears, corticosteroid drops,
cycloplegic drops, glaucoma drops
No
2 Phase 2 127 Corticosteroid drops, cycloplegic drops No
3 Phase 2 86 Corticosteroid drops No
4 Phase 2 138 Corticosteroid drops No
5 Phase 2 240 Corticosteroid drops, cycloplegic drops Yes
6 Phase 2 55 Corticosteroid drops, cycloplegic drops,
antibiotic drops
No
7 Phase 2 51 Artificial tears No
1 Phase 3 106 and 117 Corticosteroid drops Yes
2 Phase 3 144 Corticosteroid drops No
3 Phase 3 98 Corticosteroid drops, cycloplegic drops No
4 Phase 3 178 Corticosteroid drops, artificial tears No
5 Phase 3 198 Corticosteroid/antibiotic drops No
6 Phase 3 144 Corticosteroid drops, cycloplegic drops Yes
7 Phase 3 97 and 145 Corticosteroid drops, cycloplegic drops Yes
8 Phase 3 49 Corticosteroid drops, cycloplegic drops Yes
9 Phase 3 49 and 107 Corticosteroid drops No
the other trials. We cannot exclude the possibility thatprior therapies, especially immunotherapies, could increasethe risk for uveitis from vemurafenib treatment.
Uveitis in the setting of vemurafenib therapy could beexplained by a number of possible mechanisms. One poten-tial explanation for the origin of the uveitis is direct vemur-afenib action on subclinical metastatic cells within the uvealtract. Choroid metastases from cutaneous melanoma arerare; the incidence is unknown and they are typically onlydetected when the metastases limit vision because of macu-lar edema or optic nerve infiltration.8 Wilmott and associ-ates showed that treatment with selective BRAF inhibitors(vemurafenib or dabrafenib) results in intra- and peritumoralinfiltration by CD4þ and CD8þ lymphocytes.9 Vemurafe-nib has been used to treat central nervous systemmetastases,indicating that vemurafenib is capable of crossing the blood-brain barrier and, therefore, the blood-retinal barrier.10
Hence, it is possible that uveitis occurred in certain patientsas a result of vemurafenib-induced lymphocytic infiltrationof subclinical uveal metastases.
The second possible mechanism is that the uveitis iscaused by an inflammatory response to antigens shared bymelanocytes in the melanoma and the choroid. Vogt-Koyanagi-Harada syndrome is a testament to the presenceof a shared melanocytic antigen between the choroid anddermis, and case reports show Vogt-Koyanagi-Harada syn-
VOL. -, NO. - UVEITIS ASSOCIATED WIT
drome occurring in patients who have undergone varioustreatments for metastatic melanoma.11–13 Boni andassociates found that melanoma cells exposed tovemurafenib undergo apoptosis, releasing melanocyte-derived antigens that then stimulate a T cell responseagainst other melanoma cells.14 One hypothesis is that,in some patients, these T cells might undergo degenerationand epitope spread, resulting in autoimmunity and uveitis.Although no cases of Vogt-Koyanagi-Harada syndromewere noted within this study population, it is possiblethat cases of vemurafenib-associated uveitis share a similarpathogenesis of shared antigen recognition.The third possibility is that the uveitis is a result of
direct inhibition of the downstream ERK by vemurafenibin ocular tissues. Broad inhibition of ERK is achievedwith MEK inhibitors; therefore, toxicity from MEK in-hibitors should reflect what highly toxic levels of vemur-afenib can achieve. Huang and associates showed thatorally administered MEK inhibitors within a rat modelincrease the expression of genes associated with oxida-tive stress within the retina, including a number ofacute-phase, prothrombotic, and inflammatory cyto-kines.15 It also resulted in breakdown of the blood-retinal barrier. Clinical studies of MEK inhibitors havenot reported any cases of uveitis; moreover, vemurafenibtypically activates ERK signaling in normal tissues,
5H BRAF INHIBITION

suggesting that although the ERK inhibition theory ispossible, it is unlikely.16,17
The final possibility is that the uveitis might be a result ofparadoxical activation of ERK. Although vemurafenib is aneffective inhibitor of BRAFV600, it has caused paradoxicalactivation of ERK in cell lines that develop another BRAFmutation.18 In these cases, it is theorized that selectiveBRAF inhibitors can bind with RAF family kinases (thatinclude the CRAF and ARAF serine/threonine kinases),causing dimerization of RAF kinases in these wild-typecells, ultimately activating ERK downstream.19,20 Thisphenomenon of paradoxical ERK activation is believed tobe the cause of new cases of melanoma and dysplastic neviin patients undergoing vemurafenib treatment.21,22 It alsois thought to be the reason behind the high incidence ofkeratoacanthoma and squamous cell carcinoma in patientstreated with vemurafenib.7
Although ERK activation along the MAPK pathway in-creases the risk for tumor proliferation, ERK activation alsostimulates T cell proliferation and interleukin 2 production.
6 AMERICAN JOURNAL OF
Its activity is modulated by cytotoxic lymphocyte antigen 4(CTLA4), a molecule found on the surface of activated Tlymphocytes. Anti-CTLA4 agents such as ipilimumab havebeen used in management of melanoma because they helpaugment the immune response of the body to melanoma. Itis no surprise that uveitis is a rare but well-known adverse re-action found with these agents.23,24 We propose that BRAF-selective inhibitors might share similar mechanisms withanti-CTLA4 agents in the pathogenesis of uveitis by causingERK activation in some patients.Our results show that vemurafenib, a vastly improved
therapeutic agent for management of metastatic BRAFmutant melanoma, is associated with a moderate risk forocular adverse effects, including the potentially blindingcondition uveitis. Notably, uveitis was controllable in allinstances without cessation of the potentially life-savingtherapy. Further research is necessary to identify the precisemechanisms involved in BRAF inhibitor–associated uve-itis, which might be relevant to drug design for anticancerdrugs that exploit related pathways.
ALL AUTHORS HAVE COMPLETED AND SUBMITTED THE ICMJE FORM FOR DISCLOSURE OF POTENTIAL CONFLICTS OF INTER-est. C.H.C. has received grants from Plexxikon, Roche, and Genentech for therapeutic clinical trials. G.A.M. received travel support from Roche. I.C.is employed by Genentech/Roche and has stock options. J.H.K. serves as a consultant for Alcon, Allergan, Can-Fite BioPharma, Clearside Biomedical,Lux Biosciences, and Xoma, and receives grant support from EyeGate. He receives grant funding from the National Eye Institute, the US Food andDrug Administration, and the Lions Club International Foundation, and has provided legal counseling/expert testimony for McCann & Geschke, PC.R.K.A. has received grants from Plexxikon, Roche, and Genentech for therapeutic clinical trials, and grants from the National Institutes of Health andGenentech to study a separate unrelated project. The study was supported by F. Hoffman-La Roche Ltd, Nutley, New Jersey, and Plexxikon Inc, Berke-ley, California. Additional funding was provided by Research to Prevent Blindness (New York, New York) and the Paul and Evanina Mackall Foun-dation Trust (New York, New York). The sponsors provided full data access to the authors, and authors who are employees of the sponsors wereinvolved in the collection, analysis, and interpretation of the data; and in the preparation, review, and approval of the manuscript. Contributionsof authors: conception, design, and conduct of study (C.H.C., G.A.M., I.C., J.H.K., R.K.A.); collection, analysis, and interpretation of data(C.H.C., J.H.K., R.K.A.); preparation, review, or approval of the manuscript (C.H.C., G.A.M., I.C., J.H.K., R.K.A). C.H.C., G.A.M., I.C., J.H.K.,and R.K.A. had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Support was provided by Roche for editorial/writing assistance.
8. Zografos L, Ducrey N, Beati D, et al. Metastatic melanoma in
REFERENCES1. Martinez SR, Tseng WH, Young SE. Outcomes for lymphnode-positive cutaneous melanoma over two decades. WorldJ Surg 2011;35(7):1567–1572.
2. Davies H, Bignell GR, Cox C, et al. Mutations of the BRAFgene in human cancer. Nature 2002;417(6892):949–954.
3. Long GV, Menzies AM, Nagrial AM, et al. Prognostic andclinicopathologic associations of oncogenic BRAF in meta-static melanoma. J Clin Oncol 2011;29(10):1239–1246.
4. Flaherty KT, Puzanov I, Kim KB, et al. Inhibition of mutated,activated BRAF in metastatic melanoma.N Engl J Med 2010;363(9):809–819.
5. Sosman JA, Kim KB, Schuchter L, et al. Survival in BRAFV600-mutant advanced melanoma treated with vemurafenib.N Engl J Med 2012;366(8):707–714.
6. Chapman PB, Hauschild A, Robert C, et al; BRIM-3 StudyGroup. Improved survival with vemurafenib in melanomawith BRAF V600E mutation. N Engl J Med 2011;364(26):2507–2516.
7. Heakal Y,KesterM,Savage S.Vemurafenib (PLX4032): an orallyavailable inhibitor of mutated BRAF for the treatment of meta-static melanoma. Ann Pharmacother 2011;45(11):1399–1405.
the eye and orbit. Ophthalmology 2003;110(11):2245–2256.9. Wilmott JS, Long GV, Howle JR, et al. Selective BRAF in-
hibitors induce marked T-cell infiltration into human meta-static melanoma. Clin Cancer Res 2012;18(5):1386–1394.
10. Rochet NM, Kottschade LA, Markovic SN. Vemurafenib formelanoma metastases to the brain. N Engl J Med 2011;365(25):2439–2441.
11. Aisenbrey S, Luke C, Ayertey HD, Grisanti S, Perniok A,Brunner R. Vogt-Koyanagi-Harada syndrome associatedwith cutaneous malignant melanoma: an 11-year follow-up.Graefes Arch Clin Exp Ophthalmol 2003;241(12):996–999.
12. Sober AJ, Haynes HA. Uveitis, poliosis, hypomelanosis, andalopecia in a patient with malignant melanoma. Arch Derma-tol 1978;114(3):439–441.
13. Yeh S, Karne NK, Kerkar SP, et al. Ocular and systemic auto-immunity after successful tumor-infiltrating lymphocyteimmunotherapy for recurrent, metastatic melanoma.Ophthal-mology 2009;116(5):981–989.
14. Boni A, Cogdill AP, Dang P, et al. Selective BRAFV600E in-hibition enhances T-cell recognition of melanoma withoutaffecting lymphocyte function. Cancer Res 2010;70(13):5213–5219.
--- 2014OPHTHALMOLOGY

15. Huang W, Yang AH, Matsumoto D, et al. PD0325901, amitogen-activated protein kinase kinase inhibitor, producesocular toxicity in a rabbit animal model of retinal vein occlu-sion. J Ocul Pharmacol Ther 2009;25(6):519–530.
16. Adjei AA, Cohen RB, Franklin W, et al. Phase I pharmacoki-netic and pharmacodynamic study of the oral, small-moleculemitogen-activated protein kinase kinase 1/2 inhibitorAZD6244 (ARRY-142886) in patients with advanced cancers.J Clin Oncol 2008;26(13):2139–2146.
17. Haura EB, Ricart AD, Larson TG, et al. A phase II study ofPD-0325901, an oral MEK inhibitor, in previously treated pa-tients with advanced non-small cell lung cancer. Clin CancerRes 2010;16(8):2450–2457.
18. Hatzivassiliou G, Song K, Yen I, et al. RAF inhibitors primewild-type RAF to activate the MAPK pathway and enhancegrowth. Nature 2010;464(7287):431–435.
19. Poulikakos PI, Zhang C, Bollag G, Shokat KM, Rosen N.RAF inhibitors transactivate RAF dimers and ERK signalling
VOL. -, NO. - UVEITIS ASSOCIATED WIT
in cells with wild-type BRAF. Nature 2010;464(7287):427–430.
20. Heidorn SJ,Milagre C,Whittaker S, et al. Kinase-dead BRAFand oncogenic RAS cooperate to drive tumor progressionthrough CRAF. Cell 2010;140(2):209–221.
21. Dalle S, Poulalhon N, Thomas L. Vemurafenib in melanomawith BRAF V600E mutation. N Engl J Med 2011;365(15):1448–1449.
22. Zimmer L, Vaubel J, Livingstone E, Schadendorf D. Side ef-fects of systemic oncological therapies in dermatology. J DtschDermatol Ges 2012;10(7):475–486.
23. Di Giacomo AM, Biagioli M, Maio M. The emerging toxicityprofiles of anti-CTLA-4 antibodies across clinical indica-tions. Semin Oncol 2010;37(5):499–507.
24. Robinson MR, Chan CC, Yang JC, et al. Cytotoxic Tlymphocyte-associated antigen 4 blockade in patients withmetastatic melanoma: a new cause of uveitis. J Immunother2004;27(6):478–479.
7H BRAF INHIBITION

Biosketch
Christina H. Choe, MD, completed her ophthalmology residency at the University of Michigan in Ann Arbor. She
subsequently completed a dual fellowship in oculoplastic and orbital surgery and ocular oncology at the University of
Pennsylvania, Philadelphia. Her research interests include thyroid eye disease, ocular surface disease, and ocular and
orbital oncology. She is currently in private practice in Asheville, North Carolina.
7.e1 --- 2014AMERICAN JOURNAL OF OPHTHALMOLOGY

Biosketch
Ravi K. Amaravadi, MD, is Assistant Professor of Medicine, Co-Leader of the Cancer Therapeutics Program, and a
practicing medical oncologist at Abramson Cancer Center at the University of Pennsylvania, Philadelphia.
Dr Amaravadi specializes in melanoma and phase 1 clinical trials and was involved with the early development of
BRAF inhibitors. His laboratory currently works on targeting autophagy to improve cancer therapy.
VOL. -, NO. - 7.e2UVEITIS ASSOCIATED WITH BRAF INHIBITION