Embed Size (px)
Citation preview

Plus: 2012 Salary Survey • Modifiers 50, 51, 59 • ASCs • Fractures
Oct
ober
20
12
Sarah W. Sebikari, MHA, CPC
Cover:Coding Colorectal ScreeningCover:Coding Colorectal Screening

Learn what you need to know for 2013 from the source of CPT®—the AMA!
Back by popular demand!ICD-10-CM Chicago WorkshopNov. 13-14, 2012, directly preceding the Symposium
Visit ama-assn.org/go/symposia or call (800) 621-8335 to learn more and register!
Nov. 14-16, 2012Marriott Chicago Magnificent Mile
© 2012 Thinkstock
2013 CPT® and RBRVS Annual Symposium
Register at ama-assn.org/go/symposia today!568
The number of CPT® code changes
for 2013. Get ready with the AMA experts!
The premier codingand reimbursement
event.

www.aapc.com October 2012 3
[contents] 7 Letter from the Vice President, Live Educational Events
9 Letter from Member Leadership
10 Letters to the Editor / Kudos
10 Coding News
12 AAPCCA: Recapture Your Chapter
13 Handbook Corner: Scholarship Fund
In Every Issue
20 Choose the Appropriate Surgical Modifier: 50, 51, or 59 NancyClark,CPC,CPMA,CPC-I
24 Slice and Dice Your Op Report WendyGrant,CPC
26 Cover: Consider All Factors when Coding Colonoscopies SarahW.Sebikari,MHA,CPC
28 Cover sidebar: Code an Incomplete Colonoscopy G.J.Verhovshek,MA,CPC
30 Medicare Risk Adjustment: Financial Incentives May Lead to Bad Practices
MaryA.Inman,JD,andTimothyP.McCormack,JD
34 Contracts Corner: Start by Gathering Data MarciaBrauchler,MPH,CPC,CPC-H,CPC-I,CPHQ
39 ASC Coding and Billing: Know What’s Important BrendaChidester-Palmer,CPC,CPC-I,CEMC,CASCC
44 Fractures 101: Let’s Cover the Basics CynthiaEverlith,BSHA,CPC,CMA
50 Diagnostic Specificity Is Key to Payment Accuracy for MA Plans HollyJ.Cassano,CPC
On the Cover: Standing next to River Sezibwa falls, Mukono District, Uganda, Sarah W. Sebikari, MHA, CPC, takes a break from coding colonoscopies to visit family. Cover photo by Sam Mwenkanya (www.smmoments.net).
Special Features
Education
Coming Up
Contents
October 2012
44
15 Hot Topic: Member Salary Survey
30 Auditing & Compliance
34 Billing & Practice Management
39 Facility
44 Coding & Billing
43 A&P Quiz
48 Newly Credentialed Members
Online Test Yourself – Earn 1 CEUGo to: www.aapc.com/resources/ publications/coding-edge/archive.aspx
39
• Modifier 57
• Suture Removal
• Advance E/M
• Compliance
• Outsourcing Billing
Features15
24
Salary Survey 2012
4 AAPCCodingEdge
Volume 23 Number 10 October 1, 2012
CodingEdge(ISSN:1941-5036)ispublishedmonthlybyAAPC,2480South3850West,SuiteB,SaltLakeCityUT84120-7208,foritspaidmembers.PeriodicalsPostagePaidatSaltLakeCityUTandatadditionalmailingoffice.POSTMASTER:Sendaddresschangesto:CodingEdgec/oAAPC,2480South3850West,SuiteB,SaltLakeCityUT84120-7208.
Serving 118,000 Members – Including You!
October 2012
adve
rtis
ing
inde
x Advanced Career Solutions, LLC ..................36www.CodingCert.com,www.CodingConferences.com
American Medical Association .......................2www.amabookstore.com
American Society of Anesthesiologists ........51www.asahg.org/Coding13
CaseCoder, LLC ............................................37www.casecoder.com
CMS ICD-10 ...................................................5Official CMS Industry Resources for ICD-10 Transition
www.cms.gov/ICD10
CodingWebU.com ..........................................17www.CodingWebU.com
Contexo Media ..............................................21www.contexomedia.com
HealthcareBusinessOffice, LLC ....................25www.HealthcareBusinessOffice.com
Ingenix is now OptumInsightTM, ...................33part of OptumTM www.optumcoding.com
Medicare Learning Network® (MLN) ............11Official CMS Information for Medicare Fee-For-Service Providers http://www.cms.gov/MLNGenInfo
NAMAS/DoctorsManagement ................. 8, 52www.NAMAS-auditing.com
The Coding Institute, LLC .............................41www.SuperCoder.com
ZHealth Publishing, LLC ...............................47www.zhealthpublishing.com
Be Green!Why should you sign up to receive Coding Edge in digital format?
Here are some great reasons:
• You will save a few trees.
• You won’t have to wait for issues to come in the mail.
• You can read Coding Edge on your computer, tablet, or other mobile device-anywhere, anytime.
• You will always know where your issues are.
• Digital issues take up a lot less room in your home or office than paper issues.
Go into your Profile on www.aapc.com and make the change!
Chairman and CEOReedE.Pew
Vice President of Finance and Strategic PlanningKorbMatosich
Vice President of MarketingBevanErickson
Vice President of ICD-10 Education and TrainingRhondaBuckholtz,CPC,CPMA,CPC-I,CGSC,COBGC,CPEDC,CENTC
Directors, Pre-Certification Education and ExamsRaemarieJimenez,CPC,CPMA,CPC-I,CANPC,CRHC
[email protected],CPC,CPMA,CPC-I,CMRS
Director of Member ServicesDanielleMontgomery
Director of PublishingBradEricson,MPC,CPC,COSC
Managing EditorJohnVerhovshek,MA,CPC
Executive Editors MichelleA.Dick,BS ReneeDustman,BS [email protected] [email protected]
Production Artists TinaM.Smith,AAS ReneeDustman,BS [email protected] [email protected]
Advertising/Exhibiting Sales ManagerJamieZayach,BS
Addressallinquires,contributionsandchangeofaddressnoticesto:
Coding EdgePO Box 704004
Salt Lake City, UT 84170(800) 626-CODE (2633)
©2012AAPC,CodingEdge.Allrightsreserved.Reproductioninwholeorinpart,inanyform,withoutwrittenpermissionfromAAPCisprohibited.Contributionsarewelcome.CodingEdgeisapublicationformembersofAAPC.StatementsoffactoropinionaretheresponsibilityoftheauthorsaloneanddonotrepresentanopinionofAAPC,orsponsoringorganizations.Cur-rentProceduralTerminology(CPT®)iscopyright2012AmericanMedicalAssociation.AllRightsReserved.Nofeeschedules,basicunits,relativevaluesorrelatedlistingsareincludedinCPT®.TheAMAassumesnoliabilityforthedatacontainedherein.
CPC®,CPC-H®,CPC-P®,CPCOTM,CPMA®andCIRCC®areregisteredtrademarksofAAPC.

The ICD-10 transition is coming October 1, 2014. The ICD-10 transition will change every part of how you provide care, from software upgrades, to patient registration and referrals, to clinical documentation, and billing. Work with your software vendor, clearinghouse, and billing service now to ensure you are ready when the time comes. ICD-10 is closer than it seems.
CMS can help. Visit the CMS website at www.cms.gov/ICD10 for resources to get your practice ready.
2014 COMPLIANCE DEADLINE FOR ICD-10
Official CMS Industry Resources for the ICD-10 Transitionwww.cms.gov/ICD10
NEWICD-10 DEADLINE:
OCT 1, 2014
CMS_ICD-10-Coding Edge.indd 1 8/31/12 3:44 PM


www.aapc.com October 2012 7
Certified members are always in search of the best education at the best val-ue when earning Continuing Educa-
tion Units (CEUs). And you don’t have to look far because AAPC’s Live Educational Events department offers a variety of quality educational events, enabling AAPC mem-bers to expand their coding competency in fun and affordable ways.
Coming Live and to a Location Near YouWe host national and regional conferences at least once per year, local classroom-style workshops each quarter, and online webi-nars weekly. Our live events team works vig-orously to provide year-round opportunities to earn both core and specialty CEUs.
Fulfill CEU Requirements with Regional ConferencesThe 2012 AAPC Regional Conference is scheduled for this month (Oct. 25-27) in Chicago. Regional conferences offer equiv-alent educational opportunities and almost the same number of CEUs as national con-ferences. They are just one day shorter, al-lowing essential education on a number of topics in less time. Nearly half of the attend-ees at regional conferences come from the host and adjoining states, which makes net-working with nearby coding industry pro-fessionals easier. Here are Chicago conference details:
• Earn up to 14 CEUs.• Members register for $350 and non-
members $550.• Explore the heart of Chicago, next to
the Magnificent Mile on Michigan Ave.• Comfortable accommodations are at
the Hyatt Hotel Chicago for $200 per night (taxes and fees inclusive).
Stay Tuned for National Conference PlansPlans are underway for the 2013 AAPC National Conference in Orlando, Fla. The conference will take place at the Coronado Springs Walt Disney World Resort in April. Registration will be $845 for members and $1,145 for non-members. Be sure to take ad-vantage of early-bird registration for a $100 discount.
50 Local Workshops Offer Up-to-date EducationTo make attending workshops convenient, each quarter we offer them in 50 cities around the country. Workshops provide a personal, hands-on opportunity to brush up your coding skills.Our fourth-quarter workshop topic is “2013 CPT® Coding Updates.” With more than 700 changes made to the CPT® codes for next year, this will be the perfect opportu-nity to learn not just what changes are being made, but also why. Taking place in multi-ple locations during the first week of De-cember, this workshop will be a great way to earn CEUs, network with local coders and, of course, LEARN!
Webinars: Featured Live or On DemandDo you need cost-effective CEUs for your entire office? Get the best value AAPC has to offer by subscribing to the 2013 webinar series. Registration for 2013 will open Dec. 1, 2012. Webinars are one of the most pop-ular methods to learn and earn necessary CEUs; since we began offering webinars in 2010, the number of registrants has nearly doubled because of webinars’ top-notch ed-ucational value.
Get the Most Bang for Your BuckIf you are in one physical location or regis-
tered for a corporate membership, your en-tire office can participate and earn CEUs for webinars. AAPC offers a full-year subscrip-tion; and beginning in June 2013, we will offer a half-year subscription, allowing reg-istrants to access webinars occurring in the last half of the year.
Suit Your Educational NeedsFor those who only need one webinar, we offer an individual-purchase subscription. And in the works for those who need more than one webinar but not quite an entire subscription, we are looking into providing you with exciting, discounted five-webinar bundles next year.Any of AAPC’s live educational events pro-vide value, education, and convenience. Browse through our offerings at www.aapc.
com and give us a try!Sincerely,
Bill Davies, MBA Vice President, Live Educational Events
Live Events Build CEU Excitement
LetterfromtheVicePresident,LiveEducationalEvents

Unsure of what direction to take in preparing for the CPMA® exam?
Let NAMAS Help!
Log onto www.NAMASinfo.com and take the SELF ASSESSMENT TEST
This test will suggest the training that is best suited for you based on your current auditing knowledge. Training suggestions may include: ◊ You are ready! Take the exam ◊ Self Study Guide only
◊ AAPC Online Training Program ◊ Live NAMAS Training Event
NAMAS proudly offers CPMA® training as well as additional educational opportunities.
Visit our website and check our calendar to see all of the exciting places NAMAS will be visiting!
NAMAS wants to help coders and auditors “Enhance Your Career Through Education”
We want to help propel your auditing career to the next level! Attend a NAMAS Training session in 2012 and you will be registered for the:
Auditor’s Career Kit
This kit will include: ◊ 2013 CPT®/ICD-9/HCPCS books ◊ 2013 Coding Updates Book ◊ NAMAS and AAPC paid memberships for 2013 ◊ Paid Admission to the NAMAS 5th Annual Auditing Conference ◊ Paid Admission to the 2013 AAPC Annual Conference ◊ A tablet for making you mobile and on-the-go EVERY educational session you attend increases your chance
of winning this auditors career kit!
www.NAMAS-Auditing.com 877-418-5564

www.aapc.com October 2012 9
This month brings my favorite holiday: Halloween! I am a haunted house enthusiast. I get a rush not know-
ing what is around the next spooky cor-ner, much like the excitement I feel when I think about the changes taking place to-day in health care. The unknown is never as frightful as our imagination leads us to be-lieve, however.
Eliminate Fright with Good InsightIn the seasonal television special, “It’s the Great Pumpkin, Charlie Brown,” Linus spends the entire night of Halloween wait-ing for the Great Pumpkin to arrive in a pumpkin patch. If he had just taken the ini-tiative to research the Great Pumpkin, he would have learned that his fictional hero did not exist. He could have spent all of his valuable time and energy more productively by strategically planning and learning how to get the most candy in the least amount of time while trick-or-treating.
Learn and Plan for Big ChangesNow that the Centers for Medicare & Med-icaid Services (CMS) has confirmed ICD-10-CM compliance for Oct. 1, 2014, it’s time to take implementation seriously and begin preparing for the changes the new code set will bring. AAPC has been en-couraging members to deepen anatomy and pathophysiology (A&P) knowledge for the past year. Do this now to help prepare you for the 69,000 ICD-10-CM codes, which include 251 code choices for diabetes alone. Training for the new code set is estimated to be approximately 16 to 24 hours for cod-ers (more for certain specialties like ortho-paedics). This estimate, however, is based on training coders who have a solid under-standing of A&P. To see how your ICD-10-CM A&P skills rank, take our quiz on page 43. Remember: Weakness in these areas will
increase the length of training needed and decrease post implementation productivity.
Treats to Forgo Last-minute TricksIt’s still too early for in-depth code set train-ing, but it isn’t too early to begin building interest for ICD-10-CM in your practice. At this stage, activities can be fun. Involve your entire practice by posting ICD-10-CM codes around the office, identifying condi-tions related to the area or object. For exam-ple, post E66.09 on the vending machine or H93.13 near scheduling. (I’m not tell-ing you what they are; you can find them on the CDC website at www.cdc.gov/nchs/icd/
icd10cm.htm. Use this site also to locate more codes to post within your practice.)
ICD-10-CM Halloween Coding FunIn the spirit of the upcoming holiday, a few of your fellow coders have assisted me in coming up with a few Halloween-themed ICD-10-CM codes to leave you with this month:
• Rash due to confrontation with a carnivorous plant—L24.7 Irritant contact dermatitis due to plants, except food
• Bitten by witch’s companion—W55.01xA Bitten by cat, initial encounter
• Swallowing witches brew—T65.91xA Toxic effect of unspecified substance, accidental (unintentional), initial encounter
• Wolfman transformation—L68.9 Hypertrichosis, unspecified
• Extreme reaction to sun exposure following vampire bite—L56 Other acute skin changes due to ultraviolet radiation and S11.95 Open bite of unspecified part of neck.
Until next month, happy haunting!
Cynthia Stewart, CPC, CPC-H, CPMA, CPC-I, CCS-PPresident, National Advisory Board
Turn ICD-10-CM Fear into Halloween Cheer
LetterfromMemberLeadership

10 AAPCCodingEdge
CodingNewsLetterstotheEditor
KUDOS
Kari Keller Promotes Coding Through TeachingKari Keller, CPC, CPC-I, CPMA, CCS, is an advocate for AAPC local chapters. As a professor at Lord Fairfax Community Col-lege (LFCC), she encourages her students to network by attending chapter meetings pri-or to becoming certified. During the past 10 years she has taught, she has recruited 20-30 students each year to join AAPC and at-tend chapter meetings. Keller says the Win-chester chapter was founded by one of her students and that 85-90 percent of chapter members are former students.One of Keller’s students, Suzanne M.
Lail, CPC, spoke of Keller’s dedication and how it has earned the respect of her students in so many ways. She said, “You can ask any of her students, she is always willing to help you in any way. Her professionalism and
compassion for people is incredible. She is brilliant!”The Winchester chapter gives schol-
arships to Keller’s students each year and those individuals become active members who “pay it forward.” This keeps the chapter flourishing for oth-ers to benefit from scholarships and other assistance in the future.Keller’s other accomplishments in-
clude holding past offices in the Win-chester chapter, volunteering for health screens at the local mall and being an American Cancer Society Relay for Life member. In the health field since the 1980s, Keller has been a certified physician assis-tant in orthopedics and a billing manager.Kudos to Kari Keller for her support!
KariKellerencourageshercodingstudents tobecomeactiveAAPCchaptermembers.
For m
ore
info
rmat
ion
and
to a
pply
on
line,
vis
it ht
tp:/
/www
.lfcc
.edu
un
der e
mpl
oym
ent o
ppor
tuni
ties.
For m
ore
info
rmat
ion
and
to a
pply
on
line,
vis
it ht
tp:/
/www
.lfcc
.edu
un
der e
mpl
oym
ent o
ppor
tuni
ties.
For m
ore
info
rmat
ion
and
to a
pply
on
line,
vis
it ht
tp:/
/www
.lfcc
.edu
un
der e
mpl
oym
ent o
ppor
tuni
ties.
For m
ore
info
rmat
ion
and
to a
pply
on
line,
vis
it ht
tp:/
/www
.lfcc
.edu
un
der e
mpl
oym
ent o
ppor
tuni
ties.
For m
ore
info
rmat
ion
and
to a
pply
on
line,
vis
it ht
tp:/
/www
.lfcc
.edu
un
der e
mpl
oym
ent o
ppor
tuni
ties.
For m
ore
info
rmat
ion
and
to a
pply
on
line,
vis
it ht
tp:/
/www
.lfcc
.edu
un
der e
mpl
oym
ent o
ppor
tuni
ties.
For m
ore
info
rmat
ion
and
to a
pply
on
line,
vis
it ht
tp:/
/www
.lfcc
.edu
un
der e
mpl
oym
ent o
ppor
tuni
ties.
For m
ore
info
rmat
ion
and
to a
pply
on
line,
vis
it ht
tp:/
/www
.lfcc
.edu
un
der e
mpl
oym
ent o
ppor
tuni
ties.
For m
ore
info
rmat
ion
and
to a
pply
on
line,
vis
it ht
tp:/
/www
.lfcc
.edu
un
der e
mpl
oym
ent o
ppor
tuni
ties.
Lord Fairfax Community College does not discriminate on the basis of race, sex, color, national origin, religion, sexual orientation, age, veteran status, political affiliation or disability in its programs or activities. Lord Fairfax Community College is accredited by the Commission on Colleges of the Southern Association of Colleges and Schools to award associate degrees. Contact the Commission on Colleges at 1866 Southern Lane, Decatur, Georgia 30033-4097 or call 404-679-4500 for questions about the accreditation of Lord Fairfax Community College. Revised May 4, 2009 | 09-LFCC-050
With flexible class scheduling,
you can earn extra money when it’s convenient
for you!
Teach aT LFcc!
We are seeking experienced professionals who would like to
teach on a part-time basis. All teaching disciplines are needed.
Positions require a master’s degree with 18-credit hours in teaching discipline.
To apply or find out more, please visit http://www.lfcc.edu.
EEO/AA EMPLOYER
LFCC has three convenient locations — the Fauquier and Middletown Campuses and
the Luray-Page County Center.
“ We must give our talents and expertise back to others. It is our duty to “mentor” the new workforce. By being an adjunct at LFCC I am giving my years of experience to help others understand the trade better and be successful.” – Kari M Keller, CCS, CPC-I PMCC
Instructor for AAPC-Medical Coding and Billing Curriculum Advisor, LFCC
Pleasesendyourletterstotheeditorto:[email protected]
Confirmed: CMS Pays Chiropractors Only for ManipulationI have a response to Evan M. Gwilliam’s, DC, CPC, CCPC, NCICS, CCCPC, very informative advice in August’s Letters to the Editor regarding the inability to find the Centers for Medicare & Medicaid Services (CMS) guidelines on separate evaluation and management (E/M) and chiropractic services (“Advice on Sepa-rate E/M and Chiropractic Services,” page 10). Although the CPT© book for 2012 states for codes 98940-98943, “Code also significant separately identifiable evaluation and management service (99201-99499 {99224, 99225, 99226}),” CMS only pays for the manipula-tion codes, not for any diagnostic or other services for chiropractors (See CMS Pub. 100-01, chapter 5, section 70.6 (definitions); CMS Pub. 100-02, chapter 15, section 240 (Chiropractic Services- Gener-al); and, CMS Pub. 100-03, section 150.1 (Manipulation)).The patient assessment, evaluation, re-evaluation, discharge, coun-seling, and consultation are bundled with the manipulation treat-ments and are NOT separately payable by Medicare, although they might be paid by other third-party payers (check with each for pol-icy rules).Lynn S. Berry, PT, CPC
PleasesendyourKudosto:[email protected]
ICD-10 Implementation? Oct. 1, 2014Two years from this month you will be using the ICD-10 code set to report diagnoses. A final rule published in the Federal Register confirms Oct. 1, 2014 as the ICD-10-CM implementation date. The final rule ends months of speculation spawned when the Centers for Medicare & Medicaid Services (CMS) released in April a proposed rule an-nouncing the possible delay. CMS accepted comments on the pro-posed implementation date until May 17.The final rule, which also sets dates for health plan and provider identifiers, emphasizes that providers and payers must adopt the code set by the 2014 date, and explains the reasons for one-year postponement.
• View the final rule at: www.ofr.gov/OFRUpload/OFRData/2012-21238_PI.pdf
• Review the fact sheet at: www.cms.gov/apps/media/fact_sheets.asp
AAPC provides ICD-10 implementation, documentation, and code set training opportunities and assistance. Go to www.aapc.com/
icd-10/index.aspx for an outline of available services.

The MLN –
free.
Visit the Medicare Learning Network® (MLN)Related Links Medicare Billing
Certificate Program Start learning now.
We help you understand the changes.
For additional content and timely updates Official CMS Information for
Medicare Fee-For-Service Providers
R
C
M
Y
CM
MY
CY
CMY
K
2B R3 Coding Edge, OCTOBER 2013 wSocial Icons.pdf 1 8/24/12 4:45 PM

12 AAPCCodingEdge
■ AAPCCA
Recapture Your ChapterWhen your chapter is on life support, look to the AAPCCA for a cure.
By Erin Andersen, CHC, CPC
Many chapters have different ailments. Some are struggling to find officers, others have members dropping like the temperature in December, and still others are just disconnected. The good news is that you can breathe new life into your chapter.
AAPC Chapter Association (AAPC-CA) Board of Directors has combed through their collective experienc-es throughout the country and inter-viewed chapters who were on life sup-port and are now thriving. Here are some tips to help revive your chapter.
Symptom: Low Member AttendanceDifferential Diagnosis: Life is busy! It’s hard to make time for a two-hour meeting each month.Treatment Plan:Members: Put the meeting on your schedule ASAP. It’s difficult to squeeze in a meeting at the last minute, so the sooner you have it on your calendar, the more likely you will attend. If your chapter’s meetings are held on a day or time that prohibits you from attending most meetings, talk with your chapter officers. They may be able to change the day or time if many people are un-able to attend for this reason.Officers: Find out why members do not attend. Understanding the attendance obstacles your members face will help you to restructure meet-ings to better serve your members.
Jennifer Kastner, CPC, CEMC, of Gaines-ville, Ga. suggests giving out a questionnaire when members vote for new officers. This pro-vides new officers with insight and direction for the year ahead.
My chapter (Rose City in Portland, Ore.) uses an online survey via Survey Monkey to collect data from members. Doing this at least once or twice a year will help you to stay up-to-date with your members’ needs.
Symptom: Trouble Finding New OfficersDifferential Diagnosis: Life is busy! Chapters have trouble finding officers because members can’t commit to proctoring at least one exam per year or do not have enough time to devote to of-
ficer duties. Treatment Plan:Members: Being an offi-cer takes less time than you think. On average, officers devote three to 10 hours per month (including meeting time) to fulfill their duties. Talk with current chapter of-ficers about the time you can reasonably devote to being an officer, and research which
office would suit you best. Enlist other coders in your circle for support in completing your of-ficer duties.
Although it may seem horrifying to give up a Saturday to proctor an exam for fellow coders, here are important things to consider:
• Generous coders gave up one of their Saturdays to help you start a career as a coder. You can do the same for the next generation of coders.
• Proctoring an exam is a great way to network. The flock of almost-minted coders who sit before you at the exam are most likely in need of a job and could be your next hire.
• Everyone needs six to seven hours of quiet time. Proctoring can give you time to read, work on knitting projects, plan a birthday party, etc., and is not lost time.
• In-laws coming to town? Imagine being able to tell your husband or wife, “Sorry honey, I have to proctor that day. You and your parents will just have to have fun at the Ear Wax Museum without me.”
Officers: Take a good look at your members. Newly certified coders may feel intimidated and think they don’t have enough experience to be an officer, or a shy coder who comes to all the meet-ings may be afraid to speak up and nominate herself. With a little encouragement, you might glean a new officer!
Inform members about officer benefits: dis-counts on AAPC regional and national confer-ences, networking, resume boosts, etc.
Don’t wait until September to find officers. Cultivate the idea months in advance. Start a dis-cussion in the Local Chapter Forums on AAPC’s website.
Symptom: Same People Run for Office Each YearDifferential Diagnosis: No one else volunteers to be an officer, so the same people must do it ev-ery year to keep the chapter going; or, perhaps no one else runs because they don’t think they will win the election.Treatment Plan: Members: Don’t be intimidated to run. If you want a change in your chapter’s direction, it’s likely other people do, too. Seeing your name on the ballot will be a welcome sight. Officers: You’ve been such an amazing officer for so many years; members think it would be im-possible to fill your shoes. It’s hard to walk away from long-held responsibilities, and you wonder if the chapter will collapse without your knowl-edge and guidance. If this is you, it’s time to mentor members so they feel confident to step into your role next year. You can pass on valu-able information to keep the chapter running smoothly.
Symptom: No NetworkingDifferential Diagnosis: You go to a meeting, locate your buddies, and sit down next to them. At the end of the meeting, you leave without talking to anyone outside of your circle.Treatment Plan:Members: Going to your first meeting can be scary and uncomfortable. How wonderful would it have felt if someone walked up to you and welcomed you at your first meeting? At your next meeting, talk to someone you don’t know. You may make a new friend, find a new resource for solving a coding dilemma, or just make someone feel good.Officers: Host a “Get to Know You” meeting. Roxanne Thames’, CPC, CEMC, York, Pa. chapter does this every year. Members partici-pate in an “Ice Breaker” exercise where coders interview one another. They also have a Face-book page for members to keep in touch with each other, post updates, and network the “new-fashioned” way.
Symptom: Stale MeetingsDifferential Diagnosis: It’s the same old thing month after month, year after year.

www.aapc.com October 2012 13
AAPCCA Extra
Treatment Plan: Members: Participation is not just for of-ficers. If things have become ho-hum in your chapter, talk with your officers about your ideas.
Officers: • Have contests. A goal provides purpose
and focus—things we all respond to. The Gainesville, Ga. chapter awards points to members for participation in the chapter. At the end of the year, prizes like a big screen television and a laptop are awarded to the top earners.
• Expand your horizons. Offer opportunities to participate outside of meetings. Host an annual coding seminar and/or coding classes to earn money for prizes, speakers, a better venue, or parties. Increasing your chapter’s income will open doors.
Symptom: Can’t Find SpeakersDifferential Diagnosis: You have tapped the shallow pool of speakers until it ran dry.Treatment Plan: Members: If you want a speaker for your specialty, then I nominate YOU. Let your officers know you’re open to speaking at a meeting. If you can’t fill an entire two-hour meeting, partner with other coders. If the thought of speaking to a group of people, even when pictured in their underwear, ter-rifies you, ask someone else to present (an employer, coworker, physician, etc.). Officers: Break out of the usual circle of speakers. Here are some meeting ideas to consider:
• Durable medical equipment (DME)
• How to write a resume (Core B)• How to interview for a job and dress for
success (Core B)• Coding roundtable• Non-traditional practitioners
(naturopaths, acupuncturists, herbalists, chiropractors, etc.)
• Compliance• Why being an officer is great!
Get fired up and begin resuscitating your chapter. Your ideas, participation, and pos-itive attitude are essential to making your chapter thrive.
Erin Andersen, CPC, CHC, has worked in cod-ing and compliance since 2003 at Oregon Health & Science University, performing chart audits and educating providers, coders, and staff about coding and billing. Ms. Andersen is the education officer in the Rose City chapter in
Portland, Ore. and a Region 8 representative on the AAPCCA Board of Directors.
If you want a change in your chapter’s direction, it’s likely other people do, too. Seeing your name
on the ballot will be a welcome sight.
AAPCCA
Generous Members Keep AAPCCA’s Hardship Scholarship Program Strong
By Judy A. Wilson, CPC, CPC-H, CPCO, CPC-P, CPC-I, CANPC
There are times when money is so tight members cannot pay the three-installment membership fees offered through AAPC and are in jeopardy of losing their credential. There is help for our members during these times.
Announced at 2012’s AAPC National Conference in Las Vegas, the AAPC Chapter Association’s (AAPCCA) Hardship Scholar-ship Program helps members maintain their membership and certi-fication during times of financial hardship. Unfortunately, we can’t help every member who requests financial assistance because funds are limited.
If each member were to donate just $1, however, we could help so many more members who are truly in need of financial assistance.
Chapters or members may donate to this great cause by mailing a check or money order, payable to the “AAPCCA Hardship Scholar-ship Program,” to:
AAPCCA Hardship Scholarship Program 2480 South 3850 West, Suite B Salt Lake City, UT 84120

For a complete list of all remaining boot camps, visit:aapc.com/2012bootcamps
1-800-626-CODE (2633)
If you have responsibility over your organization’s transition to ICD-10, CMS’ final rule date of October 1, 2014 gives you a little extra time to get back on track.
2-Day Boot Camp Curriculum:• Where to Begin – Organizing the Implementation Effort• Understanding the Information Technology Impact• What Needs to Change – Assessing Other Key Areas of Impact• Identifying Documentation Challenges• Building Your ICD-10 Action Plan• Budgeting for ICD-10• Planning Training Approaches and Resources• Successfully Measuring Outcomes• Introduction to ICD-10 Coding – Crosswalks and Mapping• Hands-on Coding Exercises and Documentation Case Studies• Templates, Tools, and Resources + Course Manual and ICD-10-CM Book
ICD-10 IMPLEMENTATION BOOT CAMPS
REGISTER TODAY!aapc.com/2012bootcamps800-626-CODE (2633)
$6952-Days | 16 CEUs
*Dates and locations subject to change
REMAINING IMPLEMENTATION BOOT CAMPS*DATE LOCATION
Oct 24 Chicago, Illinois
Oct 25 Los Angeles, California
Nov 1 Scottsdale, Arizona
Nov 8 Morgantown, West Virginia
Nov 15 Philadelphia, Pennsylvania
Nov 15 Arlington, Texas
Nov 29 Jacksonville, Florida
Nov 29 Manhattan, New York
DATE LOCATION
Dec 6 Seattle, Washington
Dec 6 Salt Lake City, Utah
Dec 13 Atlanta, Georgia
Jan 10 San Diego, California
Jan 17 Tulsa, Oklahoma
Jan 24 New Orleans, Louisiana
Jan 31 Hawaii

www.aapc.com October 2012 15
Snapshots are instant slices of our lives. Compare them from year to year while placing them side by side and our lives become stories.Every year, Coding Edge presents AAPC’s Salary Survey as an annual slice of data about our members’ welfare. This year, we decided to show you how the information trends through the years because it tells a very interesting story about our profession’s growth. The 2012 AAPC Health Care Salary Survey, which was open to health care business professionals online this summer, confirms coders, billers, practice managers, auditors, and educators are in a dy-namic environment. It is obvious the recession affected our industry, and for most members things are improving. But the unpredictable impact of market forces provides surprises.A lot has happened since 2008, when our trend lines begin. A deep recession, beginning in Decem-ber 2007, ended in 2009 with a slow recovery and rippling effect throughout the country. Changes to the mix of practice size and affiliation occurred. Major changes to the way federal and commercial payers could pay physicians evolved and were man-dated. And, as AAPC grew from 60,000 members in 2008 to nearly 120,000 now, our professional roles, expertise, locations, and educa-tion diversified unimaginably.A significant nod to the importance of our craft is that more than 25 percent of respondents said they have decision-making power in their work places, compared with less than 20 percent in previous years. This means AAPC members are gaining more credibili-ty for knowledge and expertise.
How Much We MakeThe 2012 average salary is $47,870, based on responses. This includes credentialed and non-credentialed members; but, when broken down by credential, the averages this year looks like this:
• Certified Professional Coder (CPC®) - $47,796 (up nearly $900 from 2011)• Certified Professional Coder – Hospital Outpatient (CPC-H®) - $56,466
(up nearly $1,800 from last year)• Certified Professional Coder – Payer (CPC-P®) - $55,255 (up nearly $3,800
from last year)• Certified Professional Medical Auditor (CPMA®) - $59,365 (up more than $3200 over last year)• Specialty credentials - $54,145• All AAPC credentials, avg. - $48,033
Taking all of the credential respondents’ salaries and averaging them, we see that in the last two years salaries are slowly growing.
Hot Topic ■
Salary Survey 2012: Trends Show Growth and DiversificationFive-year comparison indicates consistent progress in this health care sector.
By David Blackmer, BA, and Brad Ericson, MPC, CPC, COSC

16 AAPCCodingEdge
Hot Topic: Survey
Salary by Credentials
All credentials, average.
2012 2011 2010 2009 2008
% gain
Annual% gain
Annual % gain
Annual % gain
Annual Annual
2% $48,033 3% $46,925 1% $45,481 1% $45,185 $45,466
Average salary by workplace has increased from last year by 9.7 per-cent or more for those in smaller groups or practices. Those work-ing in facilities made more, but received less in raises comparative-ly, averaging between 4 and 5 percent. For example, as shown in the Salary by Workplace table, the average salary at a solo practice was $40,290 in 2010, $41,301 in 2011, and $45,312 in 2012 compared to the average salary in an outpatient hospital: $43,685 in 2010, $43,751 in 2011, and $45,399 in 2012.
Salary by Workplace
40,000
50,000
Hospital Inpatient
Large Group Practice
Hospital Outpatient
Solo Practice/Small Group Practice
Medium Group Practice
201020112012
48,000
46,000
44,000
42,000
As you can see in this next table, Salary by Job Responsibility, sala-ries are indeed affected by job responsibility, and educators are mak-ing the most money.
Salary by Job Responsibility
30,000
40,000
50,000
60,000Educating
Coding/Billing Manager
Practice/Office Manager
Auditing
Coding/Billing
20082009201020112012
Credentials, Education, and BenefitsCredentials and education impact our salaries. How much education and what certifications we hold factor in to where we sit financially.While slow, there is a definite trend toward employers requiring cre-dentials. As you can see in the Credential Required table, 54 per-cent of employers require certification today, compared to 47 per-cent in 2008.
Credential Required
0
10 %
20 %
30 %
40 %
50 %
60 %
No
Yes
20082009201020112012
We know now that the average years of experience of credentialed members are significant. In our survey, CPCs® have 12; CPMAs® and CPC-Hs® have 14; and Certified Professional Coder—Instructors (CPC-Is®) have 19 average years of experience. As shown in the Sala-ry by Experience table, salary reflects experience over the years, and salary increases follow suit.
Salary by Experience
30,000
40,000
50,000
60,000
70,000
80,000
2008
2009
2010
2011
2012
15+ years10 to 15 years5 to 9 years2 to 4 years0 to 1 years
It is discouraging to note that beginning coders’ salaries have not changed much in five years, while those with significant experience are seeing larger increases. Our education is less predictable from year to year. For example, sal-aries are larger depending on how much education a member has, but higher levels of education did not always see an increase in aver-age salary in past years. Fortunately, as shown in the Education ta-ble on the next page, this year showed improvement for everyone, es-pecially for those with a master’s degree or higher.

(484) 433-0495 www.CodingWebU.com
Tired of CD-Rom Courses that are out-of-date as soon as you take them?Tired of Audio Conferences where you cannot learn at your own pace?Tired of Online Courses you go through once and cannot access again?
If so, CodingWebU.com is your answer!We are the only program that provides interactive training incorporating audio, text and graphics to ensure you comprehend the information being taught. You will receive live updates as codes change and content is added.
You always have access to the most current information, even if you purchased the course three years ago.
We offer group discounts and reporting for larger customers.We can also create or host custom courses for your employees.
2012 Coding Scenarios ARE NOW AVAILABLE!!!2011 Annual CEU Coding Scenarios are also Available
Providing Quality Education at Affordable Prices
™CodingWebU.com
Over 70 Courses Approved for CEUs starting @ $30Pain Management Injections Emergency Department Coding Interventional RadiologyBurns, Lesions, and LacerationsBilling & ReimbursementGeneral Surgery CodingPhys. Pract. Revenue Mgm’tAdvanced Beneficiary Notices
AnatomyMedical TerminologyPhysiologyICD-10Chart AuditingRACCPT® & ICD-9 UpdatesE/M and OB/GYN
Specialty Coding ModifiersSleep DisordersMeaningful UseCompliance E|M CodingEHR...and more
CALL NOW to order your 2013 Coding Books!

18 AAPCCodingEdge
Hot Topic: Survey
Education
0
10,000
20,000
30,000
40,000
50,000
60,000
70,000
80,000
Master’s
Bachelor’s
Some/Associates
No college
20082009201020112012
$44,
941 $5
4,26
6
$41,
066
$79,
405
$40,
102
$51,
618 $6
1,94
6
$39,
643 $5
0,01
5
$62,
759
$39,
455
$51,
851
$65,
720
$39,
339
$51,
397
$71,
434
$43,
834
$42,
662
$42,
549
$42,
486
Those with an associate degree or some college make 9 percent more on average than those who have not attended college. Those who have a bachelor’s degree make 21 percent more on average than those with an associate degree or some college experience. Those who have a master’s degree or greater make 46 percent more on average than those who have a bachelor’s degree. Clearly education pays.We are an educated group, according to the breakdown of respon-dents’ education level in 2012, as shown in the Education Break-down table.
Education Breakdown
Master's degree and above
Bachelor's degree
Some college or Associate degree
Technical school
High school graduate53%
12%
11%6%
18%
We’ve seen growth in members with bachelor’s and master’s degrees. We believe that much of this gain is based on an increasing num-ber of providers becoming certified and members who are choos-ing this field as a second or third career. This led us to look at unem-ployment rates. As shown in the Unemployment table, the unem-ployment rate is up for CPCs® and those with AHIMA credentials, but still well below the national average of 8 percent. For apprentices (CPC-As®, CPC-H-As®, and CPC-P-As®) who are breaking into the field, employment has improved, but remains difficult, with rates close to 25 percent.
How much education and what certifications we hold factor in to where we sit financially.
CHICAGO, IL | OCT. 25-27, 2012AAPC REGIONAL CONFERENCE
3-Days | 14 CEUs | $350Come join us in Chicago!www.aapc.com/2012regional
2012 AAPC REGIONAL CONFERENCECHICAGO
Conference Sponsors

www.aapc.com October 2012 19
Unemployment
AHIMA Credentials
AAPC Credentials
CPC-A®, CPC-H-A®, CPC-P-A®
20112012
23.41% 25.45%
1.62%
2.71%5.08%
3.10%
We are seeing an upward trend towards facility employment, as shown in the Workplace table. This may be a reflection of many pro-viders’ decision to sell their practices to facilities.
Workplace
0
5%
10%
15%
20%
25%
Hospital Inpatient
Hospital Outpatient
Large Group Practice
Medium Group Practice
Solo Practice/Small Group Practice
201020112012
19.0
%
12.1
%
20.1
%
11.6
%
8.0%
19.7
%
13.4
%
20.2
%
11.3
%
6.7%
22.4
%
14.2
%
20.2
%
11.0
%
7.6%
What sort of benefits we receive fluctuates from year to year, as does the number of hours we work per week. More than half of respon-dents work an average of 31 to 40 hours a week. Around 40 percent work more than 40 hours per week. As shown in the Benefits table, employer-sponsored perks appear to be little changed over the past four years.
Benefits
40
60
80
100
Retirement Plan (401K, etc.)
Paid Vacation
Paid Sick Leave
Paid Holiday
Paid Professional Ass'n Dues
Paid Continuing Education
Health Insurance
2009201020112012
Where Do We Go from Here?Interestingly, most of us are alright staying exactly where we are. The highest percentage of respondents (44 percent) indicate coding/bill-ing was their long-term career goal. Auditing and practice manage-ment were the next top choices (about 16 percent each), with compli-ance and health information technology (HIT) trailing behind at 7 and 6 percent respectively.
Salary by RegionOne of the most interesting year-to-year comparisons is of average salary by region. It is easy to see how the recession has moved through regions and when. Most heartening, though, is that for respondents in 2012 in all regions, salaries are up. Only 19 percent of us work in
a rural area, while 37 percent work in a suburban location, and 44 percent work in an ur-ban setting. Overall, since the advent of the recession of 2008, members have slowly grown their com-pensation and continue to do so. For more data, go to www.
AAPC.com.
David Blackmer, BA, is marketing special-ist at AAPC; Brad Ericson, MPC, CPC, COSC, is director of Publishing and Ware-house at AAPC.
Pacific$54,980
Mountain$48,131
East North Central $45,258
New England $51,382
East South Central$41,709
South Atlantic$46,663
West South Central$47,230
Mid Atlantic$52,505
West North Central $44,464
Hot Topic: Survey
To discuss this article or topic, go to www.aapc.com

20 AAPCCodingEdge
Choose the Appropriate Surgical Modifier:
50, 51, or 59For proper modifier use, look to your resources for guidance.
By Nancy Clark, CPC, CPMA, CPC-I
Modifiers are crucial to telling the story of a claim by identifying procedures that have been altered, without changing the core mean-ing of the code(s) submitted. Let’s focus on proper application and instructive resources for surgical modifiers 50, 51, and 59.
Modifier 50Modifier 50 Bilateral procedure describes procedures/services that occur on identical, opposing structures (e.g., eyes, shoulder joints, breasts). Follow these rules for appropriate use:
✓ Do use modifier 50 on bilateral body organs, such as the kidneys, ureters, and hands.
✘ Do not append modifier 50 to procedures on the skin because the skin is one organ.
✓ Do use modifier 50 when the code description does not already state the procedure is bilateral.
✘ Do not use modifier 50 when “one or both” is in the code description.
When deciding whether to use modifier 50, it’s sometimes difficult to determine if the procedure is considered bilateral. An easy way to tell is to consult the Medicare Physician Fee Schedule (MPFS) (www.
cms.gov/apps/physician-fee-schedule). A table, similar to the condensed version shown in Table A, identifies which procedures Medicare
identifies as bilateral. Remember: Commercial carriers may follow their own guidelines.Example A in Table A indicates that code 68840 Probing of lacrimal canaliculi, with or without irrigation has a bilateral surgery indica-tor of 1. This denotes that the procedure is unilateral, as described in CPT®, and can be appropriately billed as a bilateral procedure with modifier 50 appended. Medicare will pay this procedure at 150 per-cent of the allowed amount, subject to the patient’s deductible and coinsurance. Be sure to increase the billed amount when the claim is submitted; Medicare will not increase this amount on its own. As an example, if the allowed amount for 68840 is $100, the coder should increase the billed amount to $150 on the claim form.Example B indicates code 60220 Total thyroid lobectomy, unilater-al; with or without isthmusectomy has a bilateral surgery indicator of 0. This procedure code cannot be billed as a bilateral procedure be-cause the thyroid is not a bilateral body part. When the indicator 0 is designated, it means that the physiology, anatomy, or the code de-scriptor specifically states the procedure is unilateral or there is an existing code for the bilateral procedure. Never append modifier 50 to these procedures. In Example C, code 58210 Radical abdominal hysterectomy, with bi-lateral total pelvic lymphadenectomy and para-aortic lymph node sam-pling (biopsy), with or without removal of tube(s), with or without re-
moval of ovary(s) has a bilateral in-dicator of 2. These procedures are considered “inherently bilateral,” which means the code descriptor or procedure specifically includes bilateral body parts. In this exam-ple, the code descriptor includes bilateral lymph nodes and, de-pendent on the extent of the pro-cedure, the fallopian tubes and ovaries. The allowed fee sched-ule for inherently bilateral proce-dures already includes payment
Table A: Physician Fee Schedule Search
Example CPT® Code Short Description
Bilateral Surgery Indicator
DefinitionUse Modifier 50?
A 68840 Explore/irrigate tear ducts 1Valid for bilateral; crite-ria does apply
YES
B 60220 Partial removal of thyroid 0 Bilateral does not apply NO
C 58210 Extensive hysterectomy 2Money is already estab-lished for bilateral
NO
Source: [adapted from] www.cms.gov/apps/physician-fee-schedule/?agree=yes&next=Accept
■ Feature
Annual
PROCEDURAL CODING CHANGES WORKSHOPS
Contexo Media | 4 Choke Cherry Road, 2nd Floor | Rockville, MD 20850 Tel: 1-800-334-5724 | [email protected] | www.codingbooks.com
www.codingbooks.com/conferences/pcc
Choose from four convenient locations, a live online workshop or an eLearning course:
5th Annual
Monday, December 3, 2012 Dallas, Texas
Tuesday, December 4, 2012 Boston, Massachusetts
Wednesday, December 5, 2012 Bethesda, Maryland
Friday, December 7, 2012 Orlando, Florida
Tuesday, December 11, 2012 Live Synchronous Online
On-Demand (available after Dec. 21) eLearning workshop
Contexo Media presents this year’s Procedural Coding Changes workshops to discuss the 2013 CPT® changes. The workshops are designed for medical coders, billers, payers and other healthcare administrative professionals whose primary role is to ensure that their practice or facility is keeping pace with proper and compliant reimbursement processes.
At the end of each workshop, you will earn 7 CEUs and be up-to-speed on the following important changes for 2013:
✔ Introduction and overview of 2013 CPT® changes: Added codes, Revised codes and Deleted codes
✔ Discussion of rationale and impacts of significant CPT® updates
✔ General changes including guidelines, modifiers and E/M codes
✔ Clarification of important specialty-specific CPT® coding changes
Visit www.coding books.com/ conferences/pcc or call 1-800-334-5724 to register.
CPT® is a registered trademark of the American Medical Association.
20685 PCC Workshops 2013 Full Ad_UP.indd 1 8/14/12 2:19 PM

22 AAPCCodingEdge
Feature: Modifiers
for a bilateral service, so modifier 50 should not be used and the billed amount should not be increased.A bilateral indicator of 3 (not shown here because it does not apply to surgery procedures) is considered “independently bilateral,” and usually applies to radiology procedures and diagnostic tests. These codes are considered bilateral if modifier 50 is present; and full pay-ment should be made for each procedure. One such code is 73080 Radiologic examination, elbow; complete, minimum of 3 views. For ex-ample, if this procedure is performed on both the left and right el-bows, and one procedure has an allowed amount of $100, the total allowed amount for 73080-50 would be $200.
Applying Modifier 50 to Claims FormsDifferent carriers require different reporting of bilateral procedures and offer different reimbursement methodologies. For examples of common carrier preferences, see Table B.Check your carriers’ online medical policy base or review your phy-sicians’ contracts for instructions on applying modifier 50 proper-ly on claims forms.
Modifier 51Modifier 51 Multiple procedures indicates that the same provider performed multiple procedures—other than E/M services—at the same session. You should list the most resource-intense (highest pay-ing) procedure first, and append modifier 51 to the second and sub-sequent procedures.Use modifier 51 to indicate:
• Same procedure, different sites• Multiple operation(s), same operative session• Procedure performed multiple times
Most payers apply a “multiple procedure discount” with modifier 51. This refers to the practice of reducing the reimbursement for subse-quent procedures because of shared resources when two or more pro-cedures are performed together. CPT® Appendix E lists codes that are exempt from modifier 51.The following is an example of multiple operations in the same op-erative session:
Scenario: The patient presents for removal of a 0.5 cm (as measured by CPT® guidelines) malignant skin lesion on the trunk. A layered closure of the resulting wound is performed in the same operative session. The appropriate coding is:12031 Repair, intermediate, wounds of scalp, axillae, trunk and/or ex-tremities (excluding hands and feet); 2.5 cm or less [typically 100 per-cent allowed reimbursement*]11600-51 Excision, malignant lesion including margins, trunk, arms, or legs; excised diameter 0.5 cm or less [typically reduced reimburse-ment*]*Dependent on carrier policy. You should also note that a few carri-ers may automatically order the procedure codes based on that car-rier’s fee schedules.
Modifier 59Modifier 59 Distinct procedural service is used to indicate a:
• Different session or encounter• Different procedure• Different site• Separate incision, excision, lesion, injury, or body part
Modifier 59 is frequently appended to those codes defined as “sepa-rate procedures” in CPT®. Designated separate procedures common-ly are carried out as an integral component of a more extensive proce-dure. Only when a procedure or service designated as a separate pro-cedure is carried out independently, and is considered to be unrelat-ed or distinct, may it be reported separately.For example, 29870 Arthroscopy, knee, diagnostic, with or without sy-novial biopsy (separate procedure) is a designated separate procedure. If this procedure is:
• Performed alone (e.g., on the left knee): Report 29870-LT.• Performed as an integral part of another procedure (e.g., a
diagnostic arthroscopy and surgical arthroscopy on the right knee): Do not bill the separate procedure. Code only the surgical arthroscopy 29866-RT Arthroscopy, knee, surgical; osteochondral autograft(s) (eg, mosaicplasty) (includes harvesting
of the autograft[s]).
Table B: Applying Modifier 50 to Claim Forms
Sample Carrier Preferred Format Example # of Units
Modifier 50 on one line Line 1: XXXXX-50 1 Unit
Procedure on two lines
Modifier 50 appended to the second procedure
Line 1: XXXXX
Line 2: XXXXX-50
1 Unit
1 Unit
LT/RT (Left side/Right side) modifiers
Appended to the procedure on one line
Billed as 2 units
Line 1: XXXXX-LT, RT 2 Units
Procedure listed twice
RT/LT modifiers appended
Modifier 59 on the second procedure
Line 1: XXXXX-LT
Line 2: XXXXX-59, RT
1 Unit
1 Unit

www.aapc.com October 2012 23
Feature: Modifiers
To discuss this article or topic, go to www.aapc.com
• Performed as a distinct procedure (e.g., a diagnostic arthroscopy on the left knee and a surgical arthroscopy on right knee in same surgical session): Report 29866-RT and 29870-59-LT. As with modifier 51, list first the more resource-intense procedure (in this case, the surgical approach).
In another example, the patient presents for an excision of a right arm skin lesion, which is benign, and a biopsy of a skin lesion on the left arm. These codes usually are not reported together because CPT® instructs, “the obtaining of tissue for pathology during the course of [surgical procedures in the integumentary system] is … not con-sidered a separate biopsy procedure and is not separately report-ed.” In this case, however, the procedures are performed on two dis-tinct body sites, and we are further instructed, “The use of a biop-sy procedure code (e.g., 11100, 11101) indicates that the procedure … was unrelated or distinct from other procedures/services provid-ed at that time.”The appropriate coding is:
• 11403 Excision, benign lesion including margins, except skin tag (unless listed elsewhere), trunk, arms or legs; excised diameter 2.1 to 3.0 cm for the right arm skin lesion excision, with ICD-9-CM code 216.6 Benign neoplasm of skin; skin of upper limb, including shoulder
• 11100-59 Biopsy of skin, subcutaneous tissue and/or mucous membrane (including simple closure), unless otherwise listed; single lesion for the left arm skin lesion biopsy, with ICD-9-CM code 238.2 Neoplasm of uncertain behavior of other and unspecified sites and tissues; skin
Once again, you should list first the more resource-intense proce-dure (the benign lesion excision). Follow that with the biopsy, ap-pending modifier 59 and linking it with the “uncertain behavior of neoplasm” diagnosis code.
The Great Debate: Modifier 51 vs. 59According to CPT®, when multiple procedures are performed at the same session by the same provider, you may identify the additional procedure(s) or service(s) by appending modifier 51. CPT®, howev-er, also instructs us to use modifier 59 to identify two procedures or services that are not usually submitted together, but are appropriate under the circumstances. CPT® further instructs us not to use mod-ifier 59 if another already established modifier is appropriate. This is how modifier 59 earned its nickname, “The modifier of last resort.”
When choosing between modifiers 51 and 59, payer policy may be the determining factor. Some payers, including Medicare contrac-tors, do not acknowledge modifier 51. And, though we should not code solely based on reimbursement, keep in mind that modifier 51 may trigger the multiple payment reduction. On the other hand, modifier 59 may trigger a front-end edit, and the payer may require documentation, which will inevitably delay claim reimbursement.A good reference are the National Correct Coding Initiative (NCCI) edits, which provide directions on when to appropriately “unbundle” procedure codes, as illustrated in Table C. NCCI edits are valid for Medicare only, but other payers are permitted to follow these guide-lines. You can find NCCI resources on the CMS website (www.cms.
gov/NationalCorrectCodInitEd/NCCIEP/list.asp).NCCI edits are referred to as Column 1 and Column 2 codes: Col-umn 1 is the reimbursable code; and column 2 is not payable unless a modifier is permitted and submitted. An edit of 1 in the first pair of codes indicates that the column 2 code is a component of the column 1 code, but can, at times, be billed sep-arately with modifier 59 appended. The first pair of codes in Table C relate to the example previously reviewed. In this example, the procedures were performed on different sites, so the use of modifi-er 59 is correct.The second set of codes, 11100 and 99149 Moderate sedation servic-es (other than those services described by codes 00100-01999), provided by a physician other than the health care professional performing the di-agnostic or therapeutic service that the sedation supports; age 5 years or older, first 30 minutes intra-service time are listed with a 0, which in-dicates that they cannot be billed together using any modifier. The last code pair, +11201 Removal of skin tags, multiple fibrocutane-ous tags, any area; each additional 10 lesions, or part thereof (List sepa-rately in addition to code for primary procedure) and the column 2 code of 10060 Incision and drainage of abscess (eg, carbuncle, suppurative hidradenitis, cutaneous or subcutaneous abscess, cyst, furuncle, or par-onychia); simple or single are assigned a 9 indicator. This means that an NCCI edit does not apply to this code pair. If the procedures were performed in the same operative session, use modifier 51 for multiple procedures on the column 2 code (10060), based on carrier policy.
Nancy Clark, CPC, CPMA, CPC-I, is a member of the 2011-2013 AAPC Nation-al Advisory Board (NAB). She is director of the Healthcare Business Resource Center in New Jersey. She is also a PMCC-approved instructor and a health care consultant. Ms. Clark participates in the Novitas Medicare Provider Outreach and Education Advisory Group.
Table C: Correct Coding Initiative
Column 1 Column 2
Modifier 0 = not allowed 1 = allowed 9 = not applicable
11403 11100 1
11100 99149 0
11201 10060 9
Modifier Trilogies: The Epic FinaleThis is the final article in our modifier confusion trilogy series. For information on modifiers 24, 25, and 57 use, see “Identify the Correct Global Period E/M Modifier” in August’s Coding Edge, pages 34-36. To clarify modifier 58, 78, or 79 use, see “Choose Which to Use: Mod-ifiers 58, 78, or 79?” in last month’s issue, pages 18-20.

24 AAPCCodingEdge
Coding & Billing
phot
obyi
Stoc
kpho
to©
Ivan
Ivano
v
Slice and Dice Your Op ReportTo accurately code surgical procedures, consider using a scalpel.
There is no quick way to code an operative (op) report. You must read and reread—think dissection—to be sure your coding reflects all the procedures and diagnoses performed.
Code from the Body of the ReportTo code only the “preoperative diagnosis, postoperative diagnosis, and operation per-formed,” listed at the beginning of the op re-port, would be incorrect. Additional proce-dures and diagnoses not shown at the top of the note may be identified in the body of the op report. By coding directly from the body, you can ensure your coding reflects what was actually performed, as well as the diag-noses related to the procedure(s).
Physicians don’t always specify the ap-proach used to perform the surgery. Look for key words to identify the approach. For instance, with abdominal procedures phy-sicians can perform either an open (several centimeter-long incision) or a laparoscopic approach (multiple small incisions). Even if
the physician indicates an approach at the beginning of the note, review the body of the op note to verify what he or she did.
Dissect the Procedure NoteThe largest section of the op report is the procedure note, which may be a few para-graphs to several pages long. This is where the physician documents the specifics of the procedure and how it was performed. The best way to dissect the note is to use the “slice-and-dice” technique, highlight-ing relevant information as you go, as shown in Example A.
The first “slice” in the op note shows the first element of the surgery. A cystotomy in-volved incising the ovarian cysts to drain them. This is coded with 49322 Laparosco-py, surgical; with aspiration of cavity or cyst (eg, ovarian cyst) (single or multiple).
The second “slice” in the op note shows the physician turned his attention to the hydrosalpinx. The portion of the fallopi-an tube that was filled with fluid was cau-terized and removed. This is coded using +58611 Ligation or transection of fallopian tube(s) when done at the time of cesarean de-livery or intra-abdominal surgery (not a sepa-rate procedure) (List separately in addition to code for primary procedure).
The third “slice” in the op note discusses the physician removing the appendix. This is reported using 44970 Laparoscopy, surgi-cal, appendectomy. Modifier 59 Distinct pro-cedural service is appended to this code to in-dicate that an additional organ was excised.
By Wendy Grant, CPC
Takeaways:
• Dissect your operative reports to glean the complete story.
• Code from the body of the report.
• Peel back the layers of the procedure.
• Clear physician documentation is key to accurate coding and billing.
Example A:Dissecttheprocedurenote.

www.aapc.com October 2012 25
Coding & Billing: Surgical Procedures
To discuss this article or topic, go to www.aapc.com
Even if the physician indicates an approach at the beginning of the note, review the body
of the op note to verify what he or she did.
Clear Physician Documentation Is KeyPhysicians should clearly document when they perform excisions, biopsies, lesions, re-moval of foreign bodies, placement and re-moval of drainage or feeding tubes, internal hardware used as part of repair, grafts, and the type of closure. The closure description should include enough detail to support any additional coding for an extensive repair.
What’s included or bundled? Pretty much anything that has to be done to accomplish the main procedure. The incision (or cre-ation of ports for laparoscopic instruments)
is included. The normal closure at the end of the procedure is always included, as well.
The physician should document any complications, as well as any abnormal find-ings: This is where the physician should document the time for procedures requir-ing additional work (for example, exten-sive bleeding or extensive scar tissue). If the surgeon documented significant additional work and/or time, over and above the usu-al time required to perform the surgery, you may be able to append modifier 22 Increased procedural services to request additional re-imbursement.
Regardless of the surgical procedure a
physician performs, you should always be on the lookout for certain elements in the documentation. Remember to read the complete op report and don’t code only from the summary or title of the proce-dure. Using the “slice and dice” technique can help easily identify multiple procedures within one op note.
Wendy Grant, CPC, has been in the coding and billing industry for 30+ years, with 22 of those years in clinic management. She is the accounts receivable manager for Health Man-agement Physician Network, Western Division, and analyzes coding and denials, and provides
coding education to maximize revenue. Ms. Grant has been on the AAPCCA Board of Directors since 2009 and served as sec-retary in 2011. She has been certified since 2002.
Be with the family and earn CEUs!
Continuing education. Any time. Any place. ℠
Need CEUs to renew your CPC®? Stay in town. At home. Use our CD-ROM courses anywhere, any time, any place. You won’t have to travel, and you can even work at home.
From the leading provider of interactive CD-ROM courses with preapproved CEUs
Finish at your own speed, quickly or leisurely Just 1 course earns as much as 18.0 CEUs Use any Windows® PC: home, office, laptop No Internet needed: no expiring passwords
Finish a CD in a couple of sittings, or take it a chapter a day — you choose. So visit our Web site to learn more about CEUs, the convenient way!
Our CD-ROM/CEU course line-up: E/M from A to Z (18 CEUs)
Primary Care Primer (18 CEUs) E/M Chart Auditing & Coding (16 CEUs) Demystifying the Modifiers (16 CEUs) Medical Coding Strategies (15 CEUs)
Walking Through the ASC Codes (15 CEUs) Elements of ED Coding (11 CEUs)
HealthcareBusinessOffice LLC: Toll free 800-515-3235 Email: [email protected] Web site: www.HealthcareBusinessOffice.com
Follow us on Twitter: twitter.com/hbollc
Easily affordable with EasyPayments! www.HealthcareBusinessOffice.com/easypay.htm
(Some courses also have CEU approval
from AHIMA. See our Web site.)

26 AAPCCodingEdge
■ Cover
Consider All Factors when Coding Colonoscopies
By Sarah W. Sebikari, MHA, CPC
Colorectal cancer is the second leading cause of death in the United States. Accord-ing to the American Cancer Society, if all adults 50 and older were screened for colon cancer, we could cut the death rate from this disease in half, saving approximately 25,000 lives each year.Colonoscopy is considered the gold stan-dard of screening for colorectal cancer. Coding for colorectal cancer screening is complicated by several factors, including findings, patient personal and family his-tory of gastrointestinal cancer, how far the scope was advanced, and therapeutic versus diagnostic procedures. In addition, the fol-lowing factors should be considered when coding colonoscopies:
• Procedures performed• Technique used• Instruments used
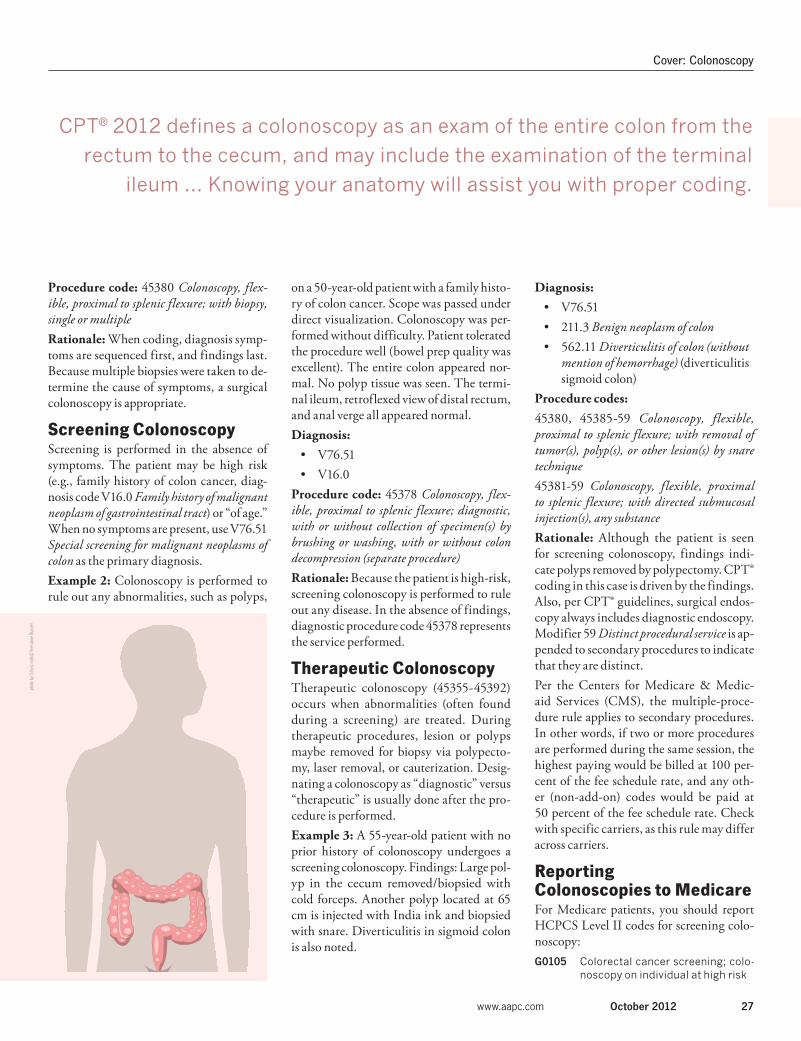
CPT® 2012 defines a colonoscopy as an exam of the entire colon from the rectum to the cecum, and may include the exami-nation of the terminal ileum. The colon in-cludes the rectum, sigmoid colon, descend-ing colon, splenic flexure, transverse colon, ascending colon and cecum. Knowing your anatomy will assist you with proper coding.
Diagnostic ColonoscopyA diagnostic colonoscopy allows the phy-sician to visualize the colon for any abnor-malities or to establish a diagnosis. The pa-tient may exhibit symptoms such as diar-rhea, blood in stool, abdominal pain, etc. Risk factors also play an important role in diagnosis coding.
Example 1: Patient has change in bow-el habits, abdominal pain, and diarrhea for the past two weeks. Colonoscopy is recom-mended. The scope is passed through the anal verge to the sigmoid colon where in-flammation is noted. Multiple biopsies of the sigmoid are taken. Further advancement of scope to the cecum confirms a normal column. The scope is withdrawn.Diagnosis:
• 789.00 Abdominal pain, unspecified site• 787.99 Other symptoms involving
digestive system (change in bowel habits)
• 787.91 Diarrhea not otherwise specified (NOS)
• 558.9 Other and unspecified noninfectious gastroenteritis and colitis (inflammation of sigmoid colon)
Takeaways:
• Coding for colorectal cancer screening is complicated by several factors, including findings, patient personal and family history of gastrointestinal cancer, how far the scope was advanced, and therapeutic versus diagnostic procedures.
• There are three types of colonoscopy with unique coding: diagnostic, screening, and therapeutic.
• Know your anatomy to code colonoscopies correctly.
Real cases help to distinguish between diagnostic, screening, and therapeutic services.
Transverse Colon
Descending Colon
Splenic Flexure
Hepatic Flexure
Sigmoid Colon
Ileum
Cecum
Ascending Colon
phot
obyi
Stoc
kpho
to©
Vadi
mm
mus
www.aapc.com October 2012 27
Cover: Colonoscopy
Procedure code: 45380 Colonoscopy, flex-ible, proximal to splenic flexure; with biopsy, single or multipleRationale: When coding, diagnosis symp-toms are sequenced first, and findings last. Because multiple biopsies were taken to de-termine the cause of symptoms, a surgical colonoscopy is appropriate.
Screening ColonoscopyScreening is performed in the absence of symptoms. The patient may be high risk (e.g., family history of colon cancer, diag-nosis code V16.0 Family history of malignant neoplasm of gastrointestinal tract) or “of age.” When no symptoms are present, use V76.51 Special screening for malignant neoplasms of colon as the primary diagnosis. Example 2: Colonoscopy is performed to rule out any abnormalities, such as polyps,
on a 50-year-old patient with a family histo-ry of colon cancer. Scope was passed under direct visualization. Colonoscopy was per-formed without difficulty. Patient tolerated the procedure well (bowel prep quality was excellent). The entire colon appeared nor-mal. No polyp tissue was seen. The termi-nal ileum, retroflexed view of distal rectum, and anal verge all appeared normal.Diagnosis:
• V76.51• V16.0
Procedure code: 45378 Colonoscopy, flex-ible, proximal to splenic flexure; diagnostic, with or without collection of specimen(s) by brushing or washing, with or without colon decompression (separate procedure)Rationale: Because the patient is high-risk, screening colonoscopy is performed to rule out any disease. In the absence of findings, diagnostic procedure code 45378 represents the service performed.
Therapeutic ColonoscopyTherapeutic colonoscopy (45355-45392) occurs when abnormalities (often found during a screening) are treated. During therapeutic procedures, lesion or polyps maybe removed for biopsy via polypecto-my, laser removal, or cauterization. Desig-nating a colonoscopy as “diagnostic” versus “therapeutic” is usually done after the pro-cedure is performed. Example 3: A 55-year-old patient with no prior history of colonoscopy undergoes a screening colonoscopy. Findings: Large pol-yp in the cecum removed/biopsied with cold forceps. Another polyp located at 65 cm is injected with India ink and biopsied with snare. Diverticulitis in sigmoid colon is also noted.
Diagnosis:• V76.51• 211.3 Benign neoplasm of colon • 562.11 Diverticulitis of colon (without
mention of hemorrhage) (diverticulitis sigmoid colon)
Procedure codes: 45380, 45385-59 Colonoscopy, flexible, proximal to splenic flexure; with removal of tumor(s), polyp(s), or other lesion(s) by snare technique45381-59 Colonoscopy, flexible, proximal to splenic flexure; with directed submucosal injection(s), any substanceRationale: Although the patient is seen for screening colonoscopy, findings indi-cate polyps removed by polypectomy. CPT® coding in this case is driven by the findings. Also, per CPT® guidelines, surgical endos-copy always includes diagnostic endoscopy. Modifier 59 Distinct procedural service is ap-pended to secondary procedures to indicate that they are distinct.Per the Centers for Medicare & Medic-aid Services (CMS), the multiple-proce-dure rule applies to secondary procedures. In other words, if two or more procedures are performed during the same session, the highest paying would be billed at 100 per-cent of the fee schedule rate, and any oth-er (non-add-on) codes would be paid at 50 percent of the fee schedule rate. Check with specific carriers, as this rule may differ across carriers.
Reporting Colonoscopies to MedicareFor Medicare patients, you should report HCPCS Level II codes for screening colo-noscopy:G0105 Colorectal cancer screening; colo-
noscopy on individual at high risk
CPT® 2012 defines a colonoscopy as an exam of the entire colon from the
rectum to the cecum, and may include the examination of the terminal
ileum … Knowing your anatomy will assist you with proper coding.
phot
obyi
Stoc
kpho
to©
Tere
sann
eRus
sell

28 AAPCCodingEdge
To discuss this article or topic, go to www.aapc.comCover: Colonoscopy
G0120 Colorectal cancer screening; alter-native to G0105, screening colo-noscopy, barium enema
G0121 Colorectal cancer screening; colo-noscopy on individual not meeting criteria for high risk
Per CMS guidelines, a patient is considered high risk if he or she meets one of the follow-ing criteria:
• A close relative (sibling, parent, or child) who has had colorectal cancer or an adenomatous polyp
• Family history of familial adenomatous polyposis
• Family history of hereditary non-polyposis colorectal cancer
• Personal history of adenomatous polyps
• Personal history of colorectal cancer
• Personal history of inflammatory bowel disease, including Crohn’s disease and ulcerative colitis
Colorectal cancer screening for a Medicare patient may be reported with the following HCPCS Level II codes: G0104 Colorectal cancer screening; flexi-
ble sigmoidoscopy
G0106 Colorectal cancer screening; al-ternative to G0104, screening sig-moidoscopy, barium enema
Example 4: Colonoscopy was performed to rule out any abnormalities, such as polyps, on a 65-year-old patient with personal his-tory of colon polyps. Scope was passed un-der direct visualization. Colonoscopy per-formed without difficulty. Patient tolerated the procedure well. The entire colon up to the terminal ileum appeared normal.
Diagnosis: • V76.51• V12.72 Personal history of colonic
polypsProcedure code:
• G0105Rationale: The patient is considered high risk per Medicare guidelines because he has a history of colon polyps, making G0105 the appropriate screening code.If findings are positive for additional pol-yps, CPT® codes 45380-45392 may be re-ported for Medicare. Consideration would be given to the technique used to remove the polyp to appropriately code the procedure (see example 3).
Sarah W. Sebikari, MHA, CPC, is senior coding analyst with Premier Health Care Ex-change, a health care cost management com-pany. She has been in the health care field for the past 11 years and a certified coder for the past nine years, with experience spanning from multiple-specialty physician to outpa-tient coding and reimbursement.
Code an Incomplete ColonoscopyMedicare rules for coding colonoscopy differ from American Medical
Association (AMA) rules, particularly with regard to “incomplete” colonoscopies.
For a Medicare patient undergoing a screening colonoscopy, if the sur-geon is able to advance the scope past the splenic flexure, consider the colonoscopy “complete” and report the appropriate code (e.g., screening
code G0105 Colorectal cancer screening; colonoscopy on individual at
high risk; or G0121 Colorectal cancer screening; colonoscopy on indi-vidual not meeting criteria for high risk, depending on the patient’s risk factors) with no modifier appended. In such a case, Medicare will pay the standard reimbursement rate for the coded procedure.
Medicare Guidance for “Incomplete”If the physician preps the patient for a screening colonoscopy but cannot advance the scope past the splenic flexure due to obstruction, patient discomfort, or other complications, append modifier 53 Reduced pro-cedural service to the appropriate code, per the Centers for Medicare & Medicaid Services’ (CMS) Program Memorandum, transmittal AB-03-114, change request (CR) 2822 (www.cms.hhs.gov/Transmittals/Downloads/AB03114.pdf).
“When a covered colonoscopy is attempted but cannot be completed because of extenuating circumstances … Medicare will pay for the interrupted colonoscopy at a rate consistent with that of a flexible sig-moidoscopy as long as coverage conditions are met for the incomplete procedure,” according to transmittal AB-03-114. Medicare expects the provider to maintain adequate information in the patient’s medical record in case it is needed by the contractor to document the incomplete procedure.
Reporting an incomplete screening should not trigger Medicare fre-quency limitations or affect your ability to collect appropriate reimburse-
ment for a subsequent complete examination. “It is not appropriate to count the incomplete colonoscopy toward the beneficiary’s frequency limit for a screening colonoscopy because that would preclude the beneficiary’s being able to obtain a covered completed colonoscopy,” instructs transmittal AB-03-114. The transmittal concludes, “If coverage conditions are met, Medicare pays for both the uncompleted colonoscopy and the completed colonoscopy whether the colonoscopy is screening in nature or diagnostic” [emphasis added].
Code It For example, one week after an attempted but unsuccessful screening exam, a high-risk patient returns for a second attempt. On this occa-sion, the physician successfully inserts the scope and fully visualizes the colon past the splenic flexure. The initial exam would have been reported G0105-53, for which the physician should receive reimbursement equiva-lent to that of a flexible sigmoidoscopy. For the second, successful exam, report G0105 once again, this time without a modifier. Medicare guide-lines dictate that your physician will be paid in full for the second exam at the standard fee schedule rate.
CPT® and Other Payer Instructions May DifferCPT®, in contrast to CMS rules, instructs, “For an incomplete colonos-copy, with full preparation for a colonoscopy, use a colonoscopy code with the modifier 52 [Reduced services] and provide documentation.”
Some non-Medicare payers may follow CMS guidelines for an incomplete colonoscopy (modifier 53), while others may adhere to CPT® instructions (modifier 52). Check with your individual third-party payers for their rec-ommendations.
G.J. Verhovshek, MA, CPC, is managing editor at AAPC.
By G.J. Verhovshek, MA, CPC

2013CODE BOOKS
ICD-9-CM & CPT® In-Stockand Shipping Now!
Pre-order Today!www.aapc.com/2013codebooks1-800-626-CODE (2633)
Physician Bundle 3 ICD-9 1 & 2 • HCPCS • Procedural Coding Expert
$304.85$124.95
Physician Bundle 1 ICD-9 1 & 2 • CPT® • HCPCS Level II
$304.85$169.95
Hospital Bundle 1 ICD-9 1-3 • CPT® • HCPCS Level II
$308.85$179.95
Physician Bundle 2 ICD-9 1 & 2 • HCPCS • CPT® • Procedural Coding Expert
$414.80$209.95
Hospital Bundle 2 ICD-9 1-3 • HCPCS • CPT® • Procedural Coding Expert
$418.80$219.95
Our Best Value!
Individual Books
LowestPrices
Anywhere
Bundles
AMA’s CPT® Professional
$109.95$94.95
ICD-9-CM Vol. 1-2
$99.95$54.95
HCPCS Level II
$94.95$54.95
ICD-9-CMVol. 1-3
$103.95$64.95
Procedural Coding Expert
$109.95$64.95
Ships in DecemberShips Now Ships in DecemberShips Now Ships Now

30 AAPCCodingEdge
Auditing & Compliance
By Mary A. Inman, JD, and Timothy P. McCormack, JD
Medicare Risk Adjustment:
Financial Incentives May Lead to Bad PracticesBe sure your model isn’t susceptible to fraud.
As Medicare-managed care health plans (Medicare Advantage (MA) plans) ex-
pand—especially in the past five years—providers are more regularly affected by “risk adjustment.” When done properly, the risk adjustment model has great potential to en-hance the quality of patient care. Unfortu-nately, risk adjustment is also susceptible to fraud by the proverbial “bad apple.”
Risk Adjustment BasicsRisk adjustment is a modified version of the traditional capitation system. Under tra-ditional capitation, a managed care orga-nization or provider group is paid a fixed amount per member per month (PMPM) to pay for all services the member requires dur-ing that period. Traditional capitation sets the PMPM rate based on demographic fac-tors such as the member’s age, gender, and geographic location. Risk adjustment enhances traditional capi-tation by adding payments for patients who are being actively treated for certain diseas-es and conditions known to be expensive to treat. Risk adjustment classifies patient sick-ness using hierarchical condition categories (HCCs), which are groups of related diagno-sis codes. HCCs are similar to diagnosis-re-lated groups (DRGs) or ambulatory payment classifications (APCs) used for hospital reim-bursement, but they are based on diagnosis codes rather than procedure codes. Individu-al patients may fall into multiple HCCs. For each additional HCC, the MA plan is paid an extra amount.Unlike traditional managed care, where there is a strong financial incentive to seek out only healthy members, the risk adjust-
ment model rewards managed care organi-zations and provider groups to care for sick members, as well. They can see a signifi-cant financial reward if they actively man-age those sick members to reduce health care costs.
Risk Adjustment Fraud: “Upcoding” DxCodesThe current design of the risk adjustment system largely relies on MA plans to police themselves. MA plans are responsible for de-termining which diagnosis codes its mem-bers were treated for in the prior year, us-ing a combination of traditional claims data and other medical documentation (such as the patients’ medical charts). The plan then submits the diagnosis codes to the Centers for Medicare & Medicaid Services (CMS) to get the increased risk adjustment capita-tion payments. Unethical MA plans and vendors take ad-vantage of the system’s structure to essen-tially “upcode” the diagnoses they submit to CMS. They do this by submitting a risk adjustment claim to CMS for a diagnosis the member either did not have or was not treated for in the year in question. In such cases, “risk adjustment” may be offered as
Takeaways:
• Risk adjustment is a modified version of the traditional capitation system.
• Unethical MA plans and vendors take advantage of the system’s structure to essentially “upcode” the diagnoses they submit to CMS.
• Be cautious and speak up when you see the warning signs of fraud.
phot
obyi
Stoc
kpho
to©
Anth
onyR
osen
berg

www.aapc.com October 2012 31
Auditing & Compliance: Risk
an explanation for why patient medical re-cords should be changed or “supplemented” (sometimes a year or more after the patient was treated). Or the MA plan, or its vendor, may suggest that a provider call a patient in for an office visit so certain diagnosis codes can be “captured” for “risk adjustment pur-poses” (regardless of whether the patient ac-tually needed any medical treatment).CMS rules are clear that a risk adjustment claim may be submitted only if the diagno-sis meets ICD-9-CM standards and there is documentation in the medical record that the member was treated face-to-face by a qualified provider in the year questioned.Common schemes used to upcode diagno-ses for risk adjustment purposes include the following:Coding from Problem Lists: CMS rules explicitly state that a “problem list” may be used only to code a diagnosis if it is “com-prehensive and show[s] evaluation and treat-ment for each condition that relates to an ICD-9-CM code on the date of service.” It is improper to submit risk adjustment claims for diagnoses that are merely mentioned in the member’s problem list if the diagnoses were not treated or considered by the provid-er during that visit.Improper Linkages: The risk adjustment system pays MA plans a higher capitation rate when certain conditions are “linked.” For example, a patient may have both dia-betes and nephropathy. CMS will pay the MA plan more if the diabetes caused the ne-phropathy because diabetes with renal com-plications is generally significantly more se-vere than diabetes without complications.
Diabetes without complications, which falls within HCC 19, has an average value of $1,500 per year. In contrast, diabetes with re-nal manifestations, which falls within HCC 15, is valued at over $4,500 per year.For an MA plan to submit a linked diagnosis code to CMS, the provider must document the linkage between the two conditions in the medical record. It is improper for an MA plan or vendor to assume the two conditions are linked.Coding from Test Results or Prescrip-tions: CMS prohibits the submission of risk adjustment claims based solely on laborato-ry or radiology test results, drug prescrip-tions associated with particular diagnoses, or durable medical equipment (DME) servic-es. Nonetheless, certain MA plans and ven-dors include diagnosis codes in their risk ad-justment submissions even though they ap-pear only on those invalid sources of docu-mentation.Chronic Conditions: While it is true that some conditions (such as Parkinson’s) nev-er go away, this does not mean that the diag-noses can be submitted to CMS every year. Risk adjustment rules explain that a condi-tion may only be submitted for reimburse-ment if it is actively treated (or affects oth-er treatment) in the year in question. It is not enough that the patient was diagnosed or treated for the condition at some point in the past. Targeted Coding: Some organizations pres-sure coders to focus on identifying high-val-ue diagnoses, rather than coding just what is in the medical record. Some common high-value targets include:
• Cachexia/Malnutrition (HCC 21) – value of $7,800 per year
• Old myocardial infarction (MI) (HCC 83) – $2,200 per year
• Diabetes with complications (HCC 15) – $4,600 per year
• Major depression (HCC 55) – $3,200 per year
Know the Red FlagsIf a coder involved in chart reviews or an au-dit related to risk adjustment sees any of these activities, there is a strong likelihood the coder is dealing with fraud. If someone tells a coder to use a diagnosis code that doesn’t meet ICD-9-CM standards and says it is OK because “risk adjustment coding is different than regular coding,” that is a major red flag indicating the health plan or vendor is en-gaged in fraud.At its core, risk adjustment coding is “regular coding,” but stricter. Even where a diagno-sis meets traditional ICD-9-CM standards, it may not be submitted for risk adjustment purposes unless the diagnosis is: (1) docu-mented by the provider in the medical record as having been treated or as affecting the pa-tient’s treatment; (2) made during a face-to-face encounter; (3) submitted to the MA plan from a qualified provider type; and (4) made during the specified calendar year.
Risk Adjustment Fraud and the False Claims ActAt a May 31, 2012 MA compliance confer-ence, federal prosecutor Robert Trusiak not-ed that MA fraud—in particular risk adjust-ment fraud—is a “hot button issue” for the
Unethical MA plans and vendors take advantage of the system’s structure to essentially “upcode” the
diagnoses they submit to CMS.

32 AAPCCodingEdge
To discuss this article or topic, go to www.aapc.comAuditing & Compliance: Riisk
Department of Justice (DOJ). Trusiak further noted that MA plans face potential liability under the federal False Claims Act (FCA) for false risk adjustment claims, even when the upcoding or other fraud was perpetrated by a vendor on the plan’s behalf.The FCA says any person who submits a false or fraudulent claim to the United States or causes someone else to submit a false or fraudu-lent claim may be liable for three times the amount of the false claim, plus an additional penalty of up to $11,000 for each false claim. To encourage whistleblowers to report fraud, the FCA contains a qui tam provision awarding whistleblowers 15-30 percent of what the government recovers as a result of whistleblower lawsuits they file against individuals and entities committing fraud.The government has already begun enforcement against unscrupu-lous MA plans attempting to game the risk adjustment system. In United States v. Janke, the government sued an MA plan under the FCA for submitting upcoded (or non-existent) diagnosis codes for risk adjustment payments. The DOJ settled with the MA plan and its owners for $22.6 million in November 2010.
Be Cautious and Speak UpAs Trusiak cautions, the FCA targets not only the person or organi-zation submitting a false claim, but also anyone who “causes the sub-
mission” of a false claim. This means that MA plans are not the only ones who face potential liability under the FCA for false or fraudu-lent risk adjustment claims. Hospitals or physician groups could be liable, as well, if they submit false information about their MA pa-tients’ diagnoses to MA plans and that false information is used to submit a false risk-adjustment claim to CMS.To avoid this risk, you should ask to review rules used by vendors when those vendors are identifying “new” diagnoses. Don’t hesitate to speak up if the standards being used by an outside reviewer don’t line up with the established CMS coding rules your organizations are using. Providers should insist on reviewing any code submissions made for their patients—especially when an MA plan or vendor has reviewed the providers’ medical record and identified new diagno-ses—to ensure the patient actually had that particular diagnosis and was treated for it during the visit. Coders, administrators, and pro-viders can all take steps to prevent or stop risk-adjustment fraud.
Mary A. Inman, JD, and Timothy P. McCormack, JD, are part-ners at Phillips & Cohen LLP, a law firm representing whistleblowers (www.phillipsandcohen.com). Whistleblower cases brought by the firm involving Medicare and Medicaid fraud, and other types of fraud against the government, have returned more than $8.5 billion in civil settlements and related criminal fines to federal, state, and local governments.
Take Your Career to the Next Level
To learn more about all of our credentials visit: www.aapc.com or call 1-800-626-CODE (2633)
CPMA®Certified Professional Medical AuditorMedical auditing is a critical piece to compliant and profitable physician practices. Whether it’s RAC audits, private payer denials, or just peace of mind, more physicians plan to have regular audits done. The risks are getting too big to not be compliant with documentation and coding. Prove your knowledge of coding and documentation guidelines and improve your practice’s revenue cycle.
Visit www.aapc.com/CPMA

Unparalleled content
No other conference offers such a robust curriculum headed by nationally
recognized experts on medical coding, billing, and compliance. Get inside — and
first-to-market — information on medical code updates, regulatory changes, and
compliance issues and gain the insight you need to keep your coding skills current
and relevant.
Complimentary ICD-10 assessment
Registered attendees will get a complimentary ICD-10 pre-assessment so you know
exactly where your organization stands in regards to the deadline. Once you know
what you need, you can tailor the courses you take to make the most of your
conference experience and take the right steps at the right time for a quick and
easy conversion.
Registration
Registration Fee: $675
Additional Half-day Workshop: $350
(Fees include sessions, breakfast, lunch, and snacks.)
Mention promo code 149963.
Register today
Visit: OptumCoding.com/Essentials
Call: 801.464.3649, Option 1
November 26–29, 2012 | Bellagio, Las Vegas
Optum Essentials Conference:All the coding, billing, and compliance insight you expect, plus the ICD-10 guidance you need.
Need more reasons to attend?This year’s Essential Conference will be
held at The Bellagio, with special
discount rates for attendees.
THE BELLAGIO® LAS VEGAS
Designed to induce a profound sense
of well-being, this AAA Five Diamond
Award-winning resort is both chic and
luxurious. Take a stroll through our
Conservatory & Botanical Gardens and
relax in the comfort of nature. From the
Dancing Fountains and Cirque du Soleil®
to the gallery of fine art, the Bellagio is
infused with graceful aesthetics inspired
by the natural wonders of the world.
The deadline for converting to ICD-10 is still looming. That’s why the content, structure, and price of this year’s Optum Essentials conference is designed to help you make a smooth transition to ICD-10 and streamline your day-to-day processes.
12-28812 OA100-8013 07/12 © 2012 Optum. All Rights Reserved.
November 26–29, 2012 | Bellagio, Las Vegas
Ingenix is now Optum®
—a leading health services business.

34 AAPCCodingEdge
■ Practice Management
Contracts: Start by Gathering DataPart 1: When negotiating contracts, use invaluable data to your advantage.
It’s always a good idea to know the details of your payer agreements. When renego-tiating your existing health plan agree-
ments, it’s essential. The time you spend un-derstanding your payer agreements will pay off continually during the many months it takes to renegotiate them. And the data you gather is an invaluable tool for the en-tire practice even after the contracting ef-forts are over.
Define Your Payer MarketFirst, define the payers who are available for contracting in your state and region. Instead of limiting your scope of possible payers to the existing contracts, look at the big picture and define all payers in your market. Some resources for your state would be:
• Health maintenance organizations (HMOs): Check with your state’s department of insurance, or similarly named government oversight agency, such as California’s Department of Managed Care. HMOs must report their membership numbers on a regular basis, so this information is readily available.
• Preferred provider organizations (PPOs): Your practice’s insurance broker might be able to provide you with key information, as would large
employer “watchdog” groups who keep an eye on the insurance market consolidation for its impact on employer health insurance premiums.
• Medicare Advantage: Look at the Medicare beneficiary website.
• Workers’ compensation (WC) carriers: Check with your state’s department of WC site.
• Independent practice associations (IPAs)/physician hospital organizations (PHOs): Look to your local hospital(s) website(s), under “Payers We Accept.”
Determine How Your Agreements Are HeldRenegotiating contracts is also a time for “housekeeping” your existing agreements. It is very complicated for a practice with multiple providers—and certainly for one with multiple practice locations—to be (and remain) loaded correctly and in the payer databases (online and hard-copy phy-sician directories). Look at payer directo-ries online to check how your practice is list-ed. You also can call payers’ toll-free num-bers to check which providers and locations are listed under your practice’s tax identifi-cation number. Consider also that if a physician has been a provider in the network for a long time, there may be multiple contracts attached to that provider. Payers will, most likely, de-fault the payment to the lowest fee schedule. This review with each payer of the demo-graphics for your group is a great beginning to a contract renegotiation. You might start by saying, “We noticed not all of our pro-viders are listed at South office on your web-site.” This is something a health plan should want to rectify because it gives the payer a
more robust network. Now that you’ve be-gun the conversation, you can follow with, “While you’re at it, perhaps you can review the rates that we have been receiving since 2005 without any improvement?”
Define Your PracticeHave a thorough understanding of what is important to your practice before con-tacting payers to renegotiate your existing agreements. With all of our clients, we start with a few reports that help us understand what is unique about the practice and the provider’s specialty. These reports are: Productivity by CPT®/HCPCS Level II code: Know your practice’s high-volume procedures. Your mix of evaluation and management (E/M) codes relative to proce-dures is good to know when payers offer fee schedules with different rates for office vis-its. Also know if the practice does consulta-tions, preventive exams, in-house labs, X-rays, injections, supplies, and other services that are valued outside the “traditional” Re-source-based Relative Value Scale (RBRVS) fee schedule before contacting any payer. Note: The procedure frequency count is essential to define for a given time (e.g., a month, quarter, or year). A list of only the CPT® and HCPCS Level II codes does not allow for the weighted analysis of fu-ture contract offers during the renegotia-tion phase. ICD-9-CM frequency: Generate a list of diagnoses with a frequency of use for each code for a period (e.g., month, quarter, year) to understand which diseases your practice treats. This helps you define your practice to the payers. It’s also good to see how well your practice is coding (red flags would be codes that end in “9,” or include “unspeci-fied,” “not otherwise specified” (NOS), or “not elsewhere classified” (NEC)). Espe-
By Marcia Brauchler, MPH, CPC, CPC-H, CPC-I, CPHQ
phot
obyi
Stoc
kpho
to©
Anth
iaC
umm
ing

www.aapc.com October 2012 35
Practice Management: Contracts
cially with payers that serve Medicare Ad-vantage members, the specificity of ICD-9-CM codes is increasingly taken into consid-eration when offering rate increases. Fee Schedule (charges by code for insur-ance and self-pay): Knowing your fees for each CPT® and HCPCS Level II service is important. We do a quick calculation of the fee relative to Medicare to evaluate exist-ing payer agreements. If your fees are set too low, for example, and you approach the pay-er for a rate increase, you won’t get it because the payer will know that you are already re-ceiving, for example, 90 percent or even 100 percent of your charge.
Define Your ProvidersWe find it helpful to have a “cheat sheet” of the salient credentialing items that define a practice, as well as each physician and non-physician practitioner. As shown in Figure A, this spreadsheet helps us to gather neces-sary items when completing payers’ creden-tialing applications. The “Group Info” col-umn is where information relevant to the practice should be entered. The “Physician Info” column should be repeated for each provider within the practice (doctor of med-icine (MD), doctor of osteopathy (DO), doctor of optometry (OD), physician assis-tant (PA), registered nurse (RN), etc.).
Define Your Payer ExperienceGather data on your practice’s experience with each payer before contacting the pay-er. Know how much volume the payer rep-resents to your practice, and have a sense of the payer’s “hassle factor” to your billers. In other words, you need to know if each payer pays you accurately and on time.
• Payer mix: Know the number of patients and/or volume of revenue
Info Group Info Physician Info
Last Name
N/A First Name
Degree
Initials
TIN/SSN
NPI Type 1: Type 2:
NPI Username
NPI Password
Medicare Provider #
Medicare ID Type
PECOS
UPIN
Medicaid
CAQH ID
N/A
CAQH Username
CAQH Password
State License #
License Obtained
License Issue
License Exp.
DEA #
DEA Issue
DEA Exp.
PLI #
PLI Carrier
PLI Limits
PLI Exp.
Board Cert.
N/A
Date Issue
Date Exp.
DOB
Birthplace
Taxonomies
Primary Office
Phone
Fax
Contact Name
Figure A:A“cheatsheet”ofthesalientcredentialingitemsthatdefineapracticehelpsgatheressentialinformation.

36 AAPCCodingEdge
Practice Management: Contracts
that each payer brings to the practice for a given period, (e.g., all of 2011). Prioritize those payers who deserve time and attention.
• Insurance accounts receivable (A/R) aging: This report allows you to monitor, at a glance, how timely your claims are being paid and the age of your outstanding accounts. This is the best way to identify issues with a given payer that may need to be addressed through a renegotiation.
• Clearinghouse reports: The summary data available from most claims’ clearinghouses is a quick way to see the volume of claims sent to each payer, and the adjudication of those claims (paid, denied, etc.).
• Contract allowable exception report: This report shows the exceptions if insurance pays incorrectly, bundles, or reduces payments.
• Denials detail and summary reports: These reports reflect which payers are causing denials. You should know the percentage of total receipts denied by payer. This can be leveraged in your renegotiations to quantify how bad the loss is to the practice.
Identify Online Payer Log-insIn a renegotiation, one of the first ques-tions our practices are asked by payer rep-resentatives is, “Do you have online access to our provider relations’ materials?” You want to answer “Yes,” which requires hav-ing online access to each payer’s web por-tal for providers. This sounds easy, but it actually took us 24 hours in one week to do the first time on behalf of one of our clients. Now that we know where to go for the registration, one of our practices can set up online payer access with most payers in about seven hours, which is still a long time.A great place to get started is with Navi-net (www.navinet.net/about/navinet-customers), which connects your practice, if you par-ticipate with each carrier, to its 30 insurer customers. Take the time to identify web portals and set up access for each payer with which your practice currently holds an agreement.This does, indeed, take time. But the more data you have gathered and organized, the easier the renegotiation process will be for you. And even if you don’t renegotiate, un-derstanding the payers that represent 100 percent of your practice’s revenue is always a worthwhile endeavor. In the next installment of this series on contracts, we look at how you can prepare your data to better understand your prac-tice, in anticipation of approaching your contracted payers.
Marcia Brauchler, MPH, CPC, CPC-H, CPC-I, CPHQ, is the founder and president of Physicians’ Ally, Inc., a health care con-sulting firm and concierge billing company for specialty physician practices. She works with physicians on managed care contracts, reimbursement, and practice administra-
tion. Her experience includes hospital, health plan, and inde-pendent practice association administration. Her firm sells updated HIPAA policies and procedures and online staff training. She is a published researcher and a frequent public speaker.
Know how much volume the payer represents to
your practice, and have a sense of the payer’s
“hassle factor” to your billers.
The only multi-specialty conference that will equip you with the tools you need in correcting codes from the start, avoiding claim denials, maximizing your productivity and increasing your practice’s bottom-line.
5th Annual 2013 Medical Coding Update and Reimbursement Conference
December 6-8, 2012 • Buena Vista Palace • Orlando, FL
Anesthesia • Ambulatory Surgery • Billing and Collection • Ob-Gyn • Orthopaedic • Otolaryngology • Pain Management • Pathology and Clinical Lab • Pediatrics • Urology
Earn asmuch as16 CEUs!
Type in AAPC195 as Promo Code to claim your exclusive $195 Price Off!
We're excitedly counting the months till we see you in Orlando, Florida for CodingCon’s 5th Annual 2013 Medical Coding Update and Reimbursement Conference happening on December 6-8, 2012 at the Buena Vista Palace, Orlando, Florida! This 2 ½ day event is the only multi-specialty conference that will equip you with the tools you need in correcting codes from the start, avoiding claim denials, maximizing your productivity and increasing your practice’s bottom-line. Call (866) 251-3060 or register at www.codingconferences.com today!
CODINGCON PLUS!Call 866-458-2962 and sign up for a three (3) day medical coding certi�cation training camp from CodingCert.com!December 6-8, 2012Buena Vista Palace, Orlando, FL
Spine Claims Auditing Technology to Revamp Your Revenue Cycle
www.casecoder.com888-337-8220 option 5
CaseCoderExtremeAd0112.indd 1 2/5/12 10:45 PM

Interactive and hands-on exercises with case studies
4-hours includes presentation and skill-building practice
Comprehensive workbook including presentation slides
Access on-demand recording after the live event
2013 CPT® CODING UPDATESUp to 6 CEUs | $149.95 | Author: Raemarie Jimenez, CPC, CPMA, CPC-I, CANPC, CRHC
Co-Author: G. John Verhovshek, CPC
Get prepared now for the 2013 CPT® code changes. Our half-day workshop available in 40+ cities will provide you with in-depth instruction and hands-on application of the coming changes.
You’ll Learn To:• Whichnew,deleted,andrevisedcodeswillaffectyourcodingandreimbursement
• The“why,”notjustthe“what”–includesrationalesforall majorchanges
• Howtostaycompliantwithnewcodechanges
• Learnhowtogetbuy-intoreduceunder-coding.
• Howtoapplytheupdatestocodingsituationsthrough hands-onexercises,ledbyexpertpresenters
700+CHANGES
AHEAD
Workshop Features
Find a workshop location near you and register today!
www.aapc.com/2013cpt1-800-626-CODE (2633)
WORKSHOPDECEMBER

www.aapc.com October 2012 39
Facility ■
ASC Coding and Billing: Know What’s Important
By Brenda Chidester-Palmer, CPC, CPC-I, CEMC, CASCC
The basics of ambulatory surgery center (ASC) coding and billing aren’t hard to master, but they do differ from physician and facili-ty requirements. The following overview will help you know what’s most important in the ASC setting.
Definition of ASCTo understand correct coding and billing for an ASC, you must first understand what an ASC is.The Medicare Carriers Manual, section 10.1, defines an ASC as a dis-tinct entity, operating exclusively to furnish outpatient surgical ser-vices. ASCs are not in the business of providing office visits, labora-tory services, diagnostic tests, etc.A hospital-operated facility may be considered by Medicare to be ei-ther an ASC or a provider-based department of the hospital, as de-fined in 42 CFR 413.65. To provide and bill services performed in an ASC, the ASC must enter into a participating provider agreement with the Centers for Medicare & Medicaid Services (CMS).
Basic Coding and BillingASCs use a combination of hospital and physician billing. Although ASCs use CPT® and HCPCS Level II codes to bill most of their ser-vices (as do physicians), some payers will allow an ASC to bill ICD-9-CM procedure codes (like a hospital). Some payers even base im-plant reimbursement on revenue code classification.It’s important to use the proper form when submitting claims. Medi-care pays for ASC services under Part B and requires the CMS-1500 claim form. Some third-party carriers will accept the CMS-1500 form, while others allow the UB04.
Approved List of Surgical ProceduresFor Medicare patients, you cannot perform just any procedure in the ASC setting. Medicare has an “approved” list of procedures for the ASC that CMS has determined not to pose a significant safety risk, and that are not expected to require an overnight stay follow-ing the surgical procedure. The list of approved procedures is based on the criteria: 1. They are NOT emergent or life threatening (for example, a
heart transplant or reattachment of a severed limb).
2. They CANNOT be per-formed safely in a physician’s office.
3. They can be elective.
4. They can be urgent.
Procedures also do not involve ma-jor blood vessels or result in major blood loss, and cannot involve pro-longed invasion of a body cavity.Medicare publishes this list of covered procedures annually. Up-dates are published quarterly, or as necessary. The file consists of two addenda listing approved surgical procedures and covered an-cillary services.Addendum AA (Final ASC-covered Surgical Procedures) includes comments, payment indicators, and final payment amounts for cov-ered surgical procedures. (See the Addendum AA example on the next page.)Addendum BB (Final Integral to Covered Surgical Procedures) cov-ers included and separately billable ancillary services. (See the Ad-dendum BB example on the next page.)Other addenda included in the file tell us how to interpret the com-ments and indicators listed on addenda AA and BB. You should have this file and refer to it frequently when billing CMS for ASC servic-es. These addenda are:
• Addendum DD1 – Final ASC Payment Indicators• Addendum DD2 – Final ASC Comment Indicators• Addendum EE – Surgical Procedures to Be Excluded from
Payment• Addendum EE is the “Excluded from Payment” list. If these
procedures are performed in the ASC, you may not be paid unless there were extenuating circumstances.
(See examples of Addendum DD1, Addendum DD2, and Adden-dum EE on the following pages.)
Nail down ASC basics and submit claims with confidence.

40 AAPCCodingEdge
Facility: ASC Coding and Billing
CPT® Code Short DescriptorSubject to Multiple Procedure Discounting
Final 2012 Comment Indicator
Final 2012 Payment Indicator
Final 2012 Payment Weight
Final 2012 Payment
10021 Fna w/o image Y P2 1.5259 $65.04
10022 Fna w/image Y G2 4.3315 $184.64
11312 Shave skin lesion Y CH P2 1.4194 $60.50
11313 Shave skin lesion Y P2 1.4194 $60.50
11400 Exc tr-ext b9+marg 0.5 < cm Y P3 $86.80
49082 Abd paracentesis Y NI G2 5.2152 $222.31
49083 Abd paracentesis w/imaging Y NI G2 5.2152 $222.31
Addenda AA example:
HCPCS Level II Code
Short DescriptorFinal 2012 Comment Indicator
Final 2012 Payment Indicator
Final 2012 Payment Weight
Final 2012 Payment
C1716 Brachytx, non-str, Gold-198 H2 $35.00
C1840 Telescopic intraocular lens NI J7
C8902 MRA w/o fol w/cont, abd Z2 7.2284 $308.13
J0696 Ceftriaxone sodium injection N1
J0800 Corticotropin injection K2 $2,516.22
70190 X-ray exam of eye sockets Z2 0.6064 $25.85
70200 X-ray exam of eye sockets Z2 0.6064 $25.85
Addenda BB example:
Indicator Payment Indicator Definition
A2 Surgical procedure on ASC list in 2007; payment based on Outpatient Prospective Payment System (OPPS) relative payment weight.
D5 Deleted/discontinued code; no payment made.
G2 Non office-based surgical procedure added in 2008 or later; payment based on OPPS relative payment weight.
H2 Brachytherapy source paid separately when provided integral to a surgical procedure on ASC list; payment based on OPPS rate.
J7 OPPS pass-through device paid separately when provided integral to a surgical procedure on ASC list; payment contractor-priced.
J8 Device-intensive procedure; paid at adjusted rate.
K2 Drugs and biologicals paid separately when provided integral to a surgical procedure on ASC list; payment based on OPPS rate.
K7 Unclassified drugs and biologicals; payment contractor-priced.
Addenda DD1 example:

www.aapc.com October 2012 41
Facility: ASC Coding & Billing
CI Comment Indicator Meanings
CH
Active HCPCS code in current year and next calendar year, payment indicator assignment has changed; active HCPCS code that is newly recognized as pay-able in ASC; or active HCPCS code that is discontinued at the end of the current calendar year.
NI
New code for the next calendar year or existing code with substantial revision to its code descriptor in the next calendar year, interim payment indicator assign-ment; comments will be accepted on the interim payment indicator for the new code.
HCPCS Short Description
11004 Debride genitalia and perineum
11005 Debride abdom wall
11006 Debride genit/per/abdom wall
11008 Remove mesh from abd wall
15756 Free myo/skin flap microvasc
15757 Free skin flap microvasc
15758 Free fascial flap microvasc
Addenda DD2 example: Addenda EE example:
Be aware of the supplies that have pass-through status: You do not
want to miss an opportunity to capture the correct reimbursement.

42 AAPCCodingEdge
Facility: ASC Coding and Billing
Packaged Services and Separate PaymentPayments to ASCs are “packaged,” which means related services are bundled together and paid in one lump sum. Examples of packaged items include:
Category
Medical and surgical supplies not on pass-through status
Implanted prosthetic devices not on pass-through status
Equipment Surgical dressings
Splints, casts, and related deviceDrugs, not on pass-through status
Supervision of the services of an anesthetist by the operating surgeon
Radiology services for which separate payment is not allowed under OPPS, and other diagnos-tic or interpretive services
Materials, including supplies/equipment for administration and monitoring of anesthesia
All administrative or housekeep-ing services
Some categories listed above include a note stating “not on pass-through status.” This means that even though payment is based on a package price, some items are “carved out,” or may be reported and paid in addition to the package price for the surgical procedure. Be aware of the supplies that have pass-through status: You do not want to miss an opportunity to capture the correct reimbursement. Other items that may be reported separately include brachytherapy sources, as well as certain items and services that CMS has designat-ed as contractor priced (e.g., procurement of corneal tissue).
Medicare Claims SubmissionsThere is a separate set of billing rules for ASCs. While some issues may be addressed by CMS, most billing guidelines are best obtained from your local carrier or intermediary. Some carriers/intermediaries issue very detailed guides (e.g., Trailblazer), while others may simply provide a list of links to the CMS website (e.g., Empire). To reiterate, an ASC must not report separate line items, HCPCS Level II codes, or any other charges for procedures, services, drugs, devices, or supplies that are packaged into the payment allowance for covered surgical procedures. The allowance for the surgical pro-cedure itself includes these other services or items.CMS does, however, strongly encourage billing for drug and biolog-icals that are eligible for separate payment. ASCs should report sup-plies with the correct HCPCS Level II code and correct number of units on the claim form.
Device Intensive ProceduresA modified (and somewhat confusing) payment methodology is used for device-intensive procedures (i.e., procedures done specifi-cally to insert a device, such as a pacemaker).The ASC will get paid for the device, but does not submit a separate line item for the device. The ASC would instead include the cost of
the device in the procedure code and submit one line item. ASCs are not allowed to base price on the allowable code from the Medicare Physician Fee Schedule (MPFS).For example, if a device intensive procedure is performed, and the formula is to bill the Medicare allowable plus 10 percent, you may be leaving money on the table. If the 10 percent increase does not cover the cost for the device, the money will not be recouped. It is impor-tant to know the cost to the ASC and add the cost of the device into the allowable. See Tables 1 and 2 for the right and wrong ways to bill a device intensive procedure.
Modifiers in the ASCSome modifiers used in the ASC are the same as those used by phy-sicians, while others are unique to the ASC facility. Modifiers recog-nized for ASC claim filing are (these are abbreviated descriptions):
• 52 Reduced services• 59 Distinct separate procedure• 73 Procedure discontinued after prep for surgery• 74 Procedure discontinued after anesthesia administered• RT Right side• LT Left side• TC Technical component• FB Device furnished at no cost/full credit• FC Device furnished at partial credit• PT Screening service converted to a diagnostic or
therapeutic service• PA Wrong body part• PB Surgery wrong patient• PC Wrong surgery on patient• GW Surgery not related to hospice patient’s terminal
conditionASCs have their own modifiers for a discontinued procedure. Mod-ifier 73 Discontinued outpatient hospital/ambulatory surgery center (ASC) procedure prior to the administration of anesthesia is used when preparation for surgery has begun, but anesthesia has not been ad-ministered. The patient is taken back to the “prep” area and has com-pleted paperwork, etc. The reasons may be the patient has a low grade temperature, or has eaten within the past four hours. The facility charges for the preparation, etc., but adds the modifier to show the procedure was not completed.Modifier 74 Discontinued outpatient hospital/ambulatory surgery cen-ters (ASC) procedure after administration of anesthesia is used when the procedure is terminated after anesthesia is administered. Plans can pay from 25 percent to 65 percent of the allowable amount, based on the modifier and documentation of how much of the service was performed.New modifier PT Colorectal cancer screening test; converted to diag-nostic test or other procedure designates that a screening colonoscopy was converted to a diagnostic or therapeutic service. For example, a patient presents to the ASC for a screening colonoscopy. He is not

www.aapc.com October 2012 43
To discuss this article or topic, go to www.aapc.com
high risk and has no symptoms or complaints. During the colonos-copy, a polyp is found in the sigmoid. The ASC reports 45380 Colo-noscopy, flexible, proximal to splenic flexure; with biopsy, single or mul-tiple instead of 45378 Colonoscopy, flexible, proximal to splenic flex-ure; diagnostic, with or without collection of specimen(s) by brushing or washing, with or without colon decompression (separate procedure) or G0121 Colorectal cancer screening; colonoscopy on individual not meet-ing criteria for high risk. Modifier PT designates the procedure was planned as a screening, but resulted as a diagnostic procedure. For Medicare patients, this allows the procedure to be paid as a screen-ing with no co-insurance.
Commercial PlansCommercial plans may or may not follow CMS policy for ASC claim filing. Check the carrier’s site for information on claim filing, and check your contract with the payer.
Brenda Chidester-Palmer, CPC, CPC-I, CEMC, CASCC, is the principal of Palmer Coding Consultant, providing audits and education to physicians in north-east Texas. She has 25 years experience in both single- and multi-specialty prac-tices. Brenda is the former coding compliance manager of Kelsey-Seybold Clinic, a 300 physician practice in Houston. She has spoken nationally at conferences and AAPC workshops, teaches PMCC curriculum, and is a former coding educator
at San Jacinto Junior College in Pasadena, Texas. Brenda was an officer of the Houston, Texas chapter and former AAPC National Advisory Board (NAB) member.
Example Code DescriptionPayment Indicator
Units Billed AmountMedicare ASC Allowed Amount
Medicare Payment to Provider
Beneficiary Payment to Provider
Claim should have one detail line, which includes the code for the surgical procedure with the cost for the procedure and the cost for the implanted device.
54405Insert multi-comp penis pros
J8 1 $16,000.00 $10,346.97 $8,277.58 $2,069.39
Example Code DescriptionPayment Indicator
Units Billed AmountMedicare ASC Allowed Amount
Medicare Payment to Provider
Beneficiary Payment to Provider
Incorrect 54405 Insert multi-comp penis pros J8 1 $5,000.00 $10,346.97 $4,000.00 (billed amount x 80%)
$1000.00 (billed amount x 20%)
C1813 Prosthesis, penile, inflatable N1 1 $11,000.00 $0.00 $0.00 $0.00
Table 1: The correct way to bill a device intensive procedure
Table 2: The incorrect way to bill a device intensive procedure
A&P Quiz
Think You Know A&P? Let’s See …Diverticulosis is a very common condition. Found in more than half of Americans over age 60, diverticulitis is small, bulging sacs or pouches of the inner lining of the intes-tine (diverticulosis) that become inflamed or infected.
Eating a low-fiber diet is one of the most likely causes. Constipation and hard stools cause people to strain when passing stools. This increases the pressure in the colon or intes-tines and may cause the pouches to form. When small pieces of stool become trapped
in these pouches it causes infection or inflam-mation.
Symptoms of diverticulitis often start sud-denly, and may become worse over a few days. Symptoms include tenderness usually in the left lower side of the abdomen, bloating or gas, fever and chills, nausea and vomiting, not feel-ing hungry, and not eating. Some people with diverticulosis have no symptoms at all.
Test yourself to find out where your A&P skills rank:
Where are the bulging sacs or pouches most often found?
A. Small intestine
B. Large intestine
C. Stomach
D. Rectum
Note: The answer to this quiz is on page 49.
Jackie Stack, BSHA, CPC, CPC-I, CEMC, CFPC, CIMC, CPEDC, CCP-P, is ICD-10 specialist at AAPC.
Facility: ASC Coding & Billing
By Jacqueline J. Stack, BSHA, CPC, CPC-I, CEMC, CFPC, CIMC, CPEDC, CCP-P

44 AAPCCodingEdge
■ Coding & Billing
Fractures 101: Let’s Cover the BasicsFrom types of fractures and their treatment to billing fractures, here are the answers you seek.
By Cynthia Everlith, BSHA, CPC, CMA
Fracture care may seem straightforward, but there are common misconceptions and confusion when it comes to the different types of fractures and how to bill for services. To set the record
straight, here’s everything you wanted to know about fractures, but were afraid to ask.
What Is a Fracture? Many people believe a fracture is a “hairline break,” or a certain type of broken bone. That is not true: A fracture and a broken bone are the same thing.
What Are the Different Kinds of Fractures?There are several types of fractures: transverse, oblique, spiral, angu-lated, displaced, and angulated, and displaced (see Figure 1).
How Many Types of Fractures Are There?An exhaustive list of precise fracture types would fill a book. A few examples include the following:Barton’s fracture: Fracture of the distal end of the radius into the wrist joint (ICD-9-CM 813.42 Other closed fractures of distal end of radius (alone)).Fissure fracture: A crack extending from a surface into, but not through, a long bone.Jefferson’s fracture: Fracture of the atlas (first cervical vertebra).Lead pipe fracture: The bone cortex is slightly compressed and
bulged on one side, with a slight crack on the other side of the bone.Parry fracture/Monteggia’s fracture: Fracture of the proximal half of the shaft of the ulna, with dislocation of the head of the radi-us (ICD-9-CM 813.03 Closed Monteggia’s fracture).Ping-pong fracture: A type of depressed skull fracture usually seen in young children, resembling the indentation that can be produced with the finger into a ping-pong ball; when elevated it resumes and retains its normal position.Pott’s fracture: Fracture of the lower part of the fibula, with serious injury of the lower tibial articulation, usually including chipping of the medial malleolus, or rupture of the medial ligament.Colles’ fracture: A fracture of the lower end of the radius, with the lower fragment displaced backward. If the lower fragment is dis-placed forward, it is a reverse Colles’ fracture (ICD-9-CM 813.41 Closed Colles’ fracture).These are just a few fracture types; the list is extensive. To help with coding when reviewing fracture documentation, have a medical dic-tionary or other resource on hand to look up unfamiliar terms.
Takeaways:
• There are numerous types of fractures and ways to code them.
• The AMA and AAOS are excellent resources for billing fracture fees.
• Guidance for billing fractures and their repairs is payer specific.
Figure 1:TypesofFractures

www.aapc.com October 2012 45
Coding & Billing: Fractures
How Do You Fix Fractures? Generally, bones heal best when immobilized, so treatment often involves casting the broken bone (or fracture), and may require sur-gery to set the bone in place. Prior to casting or fixation, the broken bone(s) must be returned to its proper position. This is referred to as “reduction.” “Closed” reduction is manipulation of a fracture without an inci-sion. “Open” reduction refers to manipulation of a fracture after in-cision into the fracture site. When coding fractures, you will need to know the type of reduction used, as well as which body part is affect-ed (leg, arm, finger, foot, etc.) and, in some instances, the precise lo-cation of the fracture (For instance, does the fracture affect the head or shaft of the femur?).As an example, consider the X-ray images in Figure 2. Each de-scribes a different type of fracture and fracture reduction.The X-ray on the left reveals a fracture on the third or long finger proximal phalanx (816.01 Closed fracture of middle or proximal pha-lanx or phalanges of hand). This fracture is minimally displaced, and could be an example of a closed treatment of a phalangeal fracture (CPT® 26720 Closed treatment of phalangeal shaft fracture, proximal or middle phalanx, finger or thumb; without manipulation, each) or closed treatment with manipulation (26725 Closed treatment of pha-langeal shaft fracture, proximal or middle phalanx, finger or thumb; with manipulation, with or without skin or skeletal traction, each), de-pending on what the provider documents.On film A, the short arrow shows a displaced fracture of the index finger (816.01), while the long arrow shows multiple finger metacar-pal fractures (815.03 Closed fracture of shaft of metacarpal bone(s)).On Film B, the short arrow points to a percutaneous pin fixation (CPT® 26727 Percutaneous skeletal fixation of unstable phalange-al shaft fracture, proximal or middle phalanx, finger or thumb, with manipulation, each) and the long arrow points to an internal fixa-tion with plates and screws (CPT® 26615 Open treatment of metacar-pal fracture, single, includes internal fixation, when performed, each bone). There are also types of internal fixation for fractures, such as rods and spheres.
How Do You Bill Fracture Fees?There are two common approaches when coding non-manipula-tive fracture care services. The American Academy of Orthopaedic Surgeons (AAOS) and the American Medical Association (AMA) support these two approaches. The AMA has published several ar-ticles in CPT® Assistant to reflect how these options work. The two options are:1. Fracture global fees2. Alternative method for fracture feesThe AAOS Guide to CPT® Coding for Orthopaedic Surgery definition of fracture global fees reporting method states:“Fracture global fees may include the hospital or office encounter in some payment areas. In others, CMS allows you to code an E/M ser-vice with a -57 modifier [Decision for surgery] within the global peri-od if the visit was the one in which the decision to perform the pro-cedure was made. The initial cast or splint is applied, and all revis-its, excluding radiographs that are obtained by the physician, should be included within a 90-day period from the time of the initial frac-ture. All recastings and or splinting are on an ‘encounter’ basis and are separately billed.”AAOS defines the alternative method as such:“Only when treatment of the fracture does not consist primarily of a ‘procedure’ (for example, closed treatment without manipulation), services may be itemized as if the problem were recognized as an of-fice encounter. Examples include an undisplaced fracture of the fifth metatarsal; a fracture of the pelvis, undisplaced or minimal-ly displaced; or a compression fracture of a vertebra. Office, hospi-tal, and emergency department encounters are coded as appropri-ate, as are all injections, supplies, casts, splints or treatment program necessities.”Be aware that this guidance is payer specific: When fracture care is performed in the office, the payer may want you to append modifier 25 Significant, separately identifiable evaluation and management ser-vice by the same physician on the same day of the procedure or other ser-vice to the evaluation and management (E/M) service.Your practice must decide whether to bill for treatment of a fracture or to itemize, depending on your scenario.
Figure 2: Examplesof fracturesandfracturereduction.
OnfilmA, theshortarrowshowsa displaced fracture of the indexfinger.
TheX-rayontheleftrevealsafrac-tureonthethirdorlongfingerprox-imalphalanx.
OnFilmB,theshortarrowpointstoapercutaneouspinfixationandthelongarrowpointstoaninternalfixa-tionwithplatesandscrews.

46 AAPCCodingEdge
To discuss this article or topic, go to www.aapc.comCoding & Billing: Fractures
Coding Example No. 1Closed reduction without manipulation vs. E/MIf you report closed reduction w/o manipulation:Cast/splint/strapping is included.X-ray and supplies may be separately reported.If you report an E/M service:
• Cast/splint application, X-ray, and supplies all may be separately reported.
The closed reduction, if you report it, includes a 90-day global package. The first casting, splinting, and strapping are included in the procedure, along with all post-op visits. Global treatment ex-cludes X-rays, durable medical equipment (DME), and any cast-ing or splinting supplies, all of which must be reported separately. The global package means that you are not allowed to charge for the post-operative portion of the procedure. In simple terms, you cannot charge for an office visit until after the global period.In such a case, proper coding would be:
• Procedure: 26725 • Do not code separately for cast or splint application.• Next visit: 99024 Postoperative follow-up visit, normally
included in the surgical package, to indicate that an evaluation and management service was performed during a postoperative period for a reason(s) related to the original procedure
• You cannot charge separately for related E/M services during the 90-day global period.
• You may report casting and/or splinting supply charges according to documentation.
Coding Example No. 2A patient comes into your office with a fractured clavicle. The frac-ture is not displaced and has good position. The patient is given a sling and told to follow up PRN (as needed). Can the office bill frac-ture care? Is this considered treatment if the patient is not to return? Remember: When charging for a fracture care code (or any surgical procedure), there is a formula that includes preoperative, operative, and postoperative portions. Physician reimbursement (approximate):
• 17 percent preoperative• 63 percent operative
• 20 percent postoperativeIn this example, there is no intent that the provider will follow up with the patient, which eliminates the postoperative portion of the formula. The argument could be made that billing the fracture treat-ment code would be incorrect. For instance, if an emergency depart-ment (ED) physician treats a fracture with no intent to follow up with the patient, it would be incorrect to bill a fracture care code. Rather, you would report an appropriate E/M service.Let’s consider a different scenario using fracture codes and how the reimbursement varies using the formula.
Coding Example No. 3A patient was injured on the slopes of Utah and lives in New Jersey. He has surgery in Utah and returns home, where he receives follow-up care. What happens to reimbursement?Ideally, the surgeon in Utah should get 17 percent for the preopera-tive portion and 63 percent for the operative or surgical portion. If the surgeon knows that the patient is not staying for postop care, he should apply modifier 54 Surgical care only to the billed fracture care code. He or she should call (and provide written documentation to) the patient’s orthopedist in New Jersey to transfer care. The ortho-pedist accepting care should bill the same surgery code with modifi-er 55 Postoperative care. The accepting orthopedist would receive 20 percent or the postoperative fee. In the real world, the billing is almost never as ideal as in our exam-ples. What surgeon wants to give up 20 percent of his surgery fee? What physician wants 20 percent payment to treat someone else’s work? In working in orthopedics for 25 years, I have not seen this happen. What can one do if faced with this similar scenario?You should make a call to the surgeon in Utah (or wherever the ini-tial treatment occurred) and plead your case. If the surgeon has al-ready filed a claim, but agrees to split the fee, a corrected claim would need to be filed. If there is no phone call placed, with no documenta-tion stating the transfer, you cannot bill for the postoperative care.
Cynthia Everlith, BSHA, CPC, CMA, is practice administrator for Arizona Hand and Wrist Specialists, a division of OSNA, PLLC. She has more than 25 years of ex-perience in orthopaedic coding and practice management, and 16 years with her current practice. She is actively involved in workers’ compensation legislation and has worked closely with the Industrial Commission of Arizona and the Arizona Medical Association in rules affecting physicians. She has presented nationally
and locally. She is a past American Association of Orthopaedic Executives (AAOE) Board of Direc-tors and past president of AAPC’s Grand Canyon Coders Phoenix chapter. She serves on the AAOE Communication Council and Technology Task Force, and is president of the Arizona AAOE Chapter.
When coding fractures, you will need to know the type of reduction used, as well as which body part is affected … and, in some instances, the precise location of the fracture …


48 AAPCCodingEdge
AbbyBruzzi, CPCAdrianaCoyne, CPCAlinaGissendaner, CPCAmandaIsaacson, CPCAmandaSunnycalb, CPCAngelaViveros, CPCAnnMarieKluxen, CPCAnneliseCairnLutz, CPCArleneRodgers, CPC,CPMA
AshlyVang, CPCAshwiniPradeepShirsat, CPCBeckyHannah, CPCBeckyPamGallegos, CPCBettinaCRuaro, CPCBobbiGannon, CPCBrandyCarter, CPCBrunetteHunt,CPC, CPC-HCarolynClifford, CPCCarolynHoward, CPCCatherineElizabethMcGee, CPC-HCatherineChouteau, CPCCharlotteDavis, CPCChristinaMarieHatten, CPCChristineSummers, CPC-PChristyEHouser, CPCColleenMTheobald,CPC, CPC-HCrystalRicket, CPCCynthiaDeniseHenderson, CPC-HCynthiaDianeKessens, CPCDanaColquitt, CPCDeborahMStrickler, CPCDeborahMiller, CPC-HDeborahMurphy, CPCDorothySalyer, CPCEileenMDavis,CPC, CPC-HElizabethBobbett, CPCElizabethRountree, CPCElizabethVenitaLyndall, CPCEmilyTin, CPCErwinDuran, CPCErynELukic,CPC, CPC-H,CEDC
FrankMarchese, CPCGailWeakley, CPCGloriaMadrigal, CPCHeatherGabriel, CPCIlhamHamideh, CPCIngaBurton, CPCIrmaPagan, CPCJacquelynADonley,CPC, CPC-HJadaKayWalker, CPCJanelleAdams, CPCJayaAnushaKrishnaMurthy, CPCJeanetteGrasso, CPCJenniferChambers, CPCJenniferMarieCadaval, CPCJennyDriessen, CPCJessicaSherouse, CPCJillianEBreece,CPC, CPC-HJohnYao, CPCJoleneMWentz, CPCJoyceBoanor, CPCJuliaKenney-Hall, CPCJulieDeer, CPCKarenBaird, CPCKarissaLynnLeFebvre, CPCKathleenJBacheldor, CPC-HKathyLarsen, CPCKatieDilling, CPCKellyRyan, CPCKennethDDickerson, CPCKeshiaPeters, CPCKimberlyReaySwift,CPC, CPC-HKristenViviano, CPC
KristinJayne, CPCKristinaMBlahovec,CPC, CPC-HLauraEsposito, CPCLilianaGFulchiero, CPCLisaKaeHayford, CPCLisaTompkins, CPCLoryleiSeda, CPCLucilleMarieFale,CPC, CPC-HMargueriteSpence,CPC, CPC-HMariamBaichoo, CPCMarieOverton, CPCMarthaEstherDelgado, CPC-H,CEDC
MaryJoChristiansen, CPCMaryLStewart, CPCMaryYang, CPCMelanieSebastian, CPCMelissaClifford, CPCMelissaDraper, CPCMelissaPitts, CPCMichelleDMartin, CPCMichelleDawnCole, CPCMichelleLPatarcity, CPCMoniqueD.Hill, CPCNagasreeGajjela, CPCNatashaDeniseBrown, CPCNicoleWilliamson, CPCO’ShandaYPablo, CPCPamelaAlisonMurray-Taylor, CPCPoonamVinodPanchal, CPCPreetiJungnuPatil,CPC, CPC-HPremalathaRRao, CPCPritiAnandPatil, CPCRajeeshaRaveendran, CPCRandyMyers, CPCRebeccaARitzinger, CPCReneeCook, CPCRitaAnnMead, CPCRolandGinnis, CPCRoseNSweet, CPCSalinaJohnsonGlover, CPCSandraJones, CPCSandraYudyUricochea, CPCSansannahSestokas, CPCSarahNunez, CPCSharonJudkins, CPCShelleeLewis, CPCShellyJRueckert, CPCSheriRice, CPCSherryCombs, CPCShiromanieMahabir, CPCTammyTechau, CPCTanishaBagaoisan, CPCTereseFerrante, CPCTheresaAZwart, CPCThereseEagle-Man, CPCToniHWinters, CPCTracyLynnBrockman, CPCTracyOrender, CPC-HUmayalRavi, CPCValarmathyManoharan, CPCVenkateshEthiraj,CPC, CPC-HYenDo, CPC
ApprenticesAbigailJaneLimEvangelista, CPC-AAbrahamBarabat, CPC-AAdrianSistozaManzano, CPC-AAgathaZandraCantada, CPC-AAgnesMarieSibugSira, CPC-AAimeeWagner, CPC-AAimerAlcalaMendoza, CPC-AAlainDaveDelosReyesCuizon, CPC-AAlexGutierrez, CPC-A
AliciaMouser, CPC-AAllisonCameron, CPC-AAlmasShaikh, CPC-AAlyssaANakamura-Ansary, CPC-AAlyssaBourne, CPC-AAmandaLBrown, CPC-AAmandaStapleton, CPC-AAmandaAcosta, CPC-AAmandaGrant, CPC-AAmandaJoyceHolt, CPC-AAmandaMiller, CPC-AAmandaPerson, CPC-AAmandaTarlton, CPC-AAmberDanielleBarlow, CPC-AAmberLoniGiles, CPC-AAmiPope, CPC-AAmirLjulja, CPC-AAmyBuchanan, CPC-AAmyEstill, CPC-AAmyHearley, CPC-AAmyLaGrange, CPC-AAmyLothes,CPC-A, CPC-H-AAmyScott, CPC-AAnaRolinaClaridades, CPC-AAnaTrujillo, CPC-AAnastasiaColleenBarnard, CPC-AAndreaLong, CPC-AAndreaUtterback, CPC-AAndrewCayboenMangamte, CPC-AAngelaMRakoczy, CPC-AAngelaMoore, CPC-AAngelaNeal, CPC-AAnnDowns, CPC-AAnneCatherineCeelen, CPC-AAnneHuntBarnes, CPC-AAnnettaMychelleKaufmann, CPC-AAnnieFerla, CPC-AAnnieRoseFrescoMagcalas, CPC-AAnthonyAndreuDihiansanMandigma, CPC-AAnujaAshokKalke, CPC-AAprilBeaman, CPC-AAprilMStevens, CPC-AAprilRodriguez, CPC-H-AArmandoBruegasMagampon, CPC-AAshleyGoldsmith, CPC-AAshleyMaleki, CPC-AAstridCaro, CPC-AAureliaDeJesusGonzales, CPC-AAyeshaShakiaWilson, CPC-ABarbSueHaskamp, CPC-ABarbaraBack, CPC-ABarbaraKivisto, CPC-ABarbaraNewport, CPC-ABarbaraPerry, CPC-ABeatrizMuñiz, CPC-ABeckyDupre, CPC-ABelmarieReyes, CPC-ABenedictB.Fabian, CPC-ABeverlyShienaEbilane, CPC-ABiancaMaxineBaluyot, CPC-ABillGurney, CPC-ABobbiJoThompson, CPC-ABrandiBorja, CPC-ABrandyHugo, CPC-ABrandyLeighBarnes,CPC-A, CPC-H-ABresha-AnneTiffanyKuuipoTabladillo, CPC-ABriannaMarieWolbert, CPC-ABudryJBlaise, CPC-ACadiAlbright, CPC-ACaleSommers, CPC-ACandaceKelson, CPC-ACandiCicala, CPC-ACandyNichols, CPC-ACariCarnell, CPC-ACarmenEstrella, CPC-A
CarolAnnOwens, CPC-ACarolSanderson, CPC-ACarrieJoCooley, CPC-ACaseyTolman, CPC-H-ACatalinaTheissen, CPC-ACatherineApostolos, CPC-ACatherineDillman, CPC-ACathiMartin, CPC-AChaliseBayletts, CPC-AChandrikiaMahadeo, CPC-AChericaNWright, CPC-ACherylAnnDeLaCruz, CPC-ACherylHetherington, CPC-ACherylLHess, CPC-ACherylSterling, CPC-AChristinaDeborahStallworth, CPC-AChristinaForgette, CPC-AChristinaJackson, CPC-AChristineAvery-Smith, CPC-AChristineBurns, CPC-AChristineHeffernan, CPC-AChristineVPalmer, CPC-AChristopherFranklynSigmon, CPC-AClarisseMargaretFesalbonFabic, CPC-ACodyDeerinwater, CPC-AColleenKeen, CPC-AConnieEastes, CPC-ACourtneyBoss, CPC-ACynthiaDiaz, CPC-ACynthiaGerwig, CPC-ACynthiaRHaas, CPC-ACynthiaSleeman, CPC-ADanaOrtega, CPC-ADanicaMills, CPC-ADanielleRager, CPC-ADavidBinstock, CPC-ADaviennaKiggins, CPC-ADeaneLMushlit, CPC-ADebiBrettAgcaoiliVicente, CPC-ADeborahKayEdwards, CPC-ADebraJohnson, CPC-H-ADeeFoss, CPC-ADeeAnnKayeCourtway, CPC-ADeepaliArunToke, CPC-ADenahShirey, CPC-ADeniceCrowsHeart, CPC-ADeniseBauman, CPC-ADeniseLundgren, CPC-ADennetteWelch, CPC-ADeonMichellePresley, CPC-ADesiraeSteenken, CPC-ADeslieManriquez, CPC-ADestinyTurner, CPC-ADianaWeber, CPC-ADianeLemm, CPC-ADileeshPaliyathilChandran, CPC-ADipakDubey, CPC-ADoloresHarris, CPC-ADondonClaveErazo, CPC-ADonnaBurcham, CPC-ADonnaGuray-Jurk, CPC-ADorothyPalmer, CPC-ADorothySReddinger, CPC-ADulceOrcajo, CPC-ADurgaprasadKotian, CPC-AElaineDicenVisaya, CPC-AElesaDonnoe, CPC-AElisabelNieves, CPC-AElishaAChilders, CPC-AElizabethAWilson, CPC-AElizabethCase, CPC-AElizabethDillonRogers, CPC-AEllenLee, CPC-AEnjoliMitchell, CPC-AEnnisMichaelStevenson, CPC-A
EricBaluyutHernandez, CPC-AErikaMaeRocheBenemerito, CPC-AErikaRushing, CPC-AEsperanzaPerez, CPC-AEstepanieCanariaNunez, CPC-AEuginaChanelTillman, CPC-AEvaClemens, CPC-AEvangelineKaku, CPC-AEvelynBakken, CPC-AFrancesVanCamp, CPC-AFrankGeorgeRobertson, CPC-AGajalakshmiViswanathan, CPC-AGeraldineAnneCummings, CPC-AGerardGeneMaynigo, CPC-AGiselleShollenberger, CPC-AGraceMagallanesBalag, CPC-AGreggRudes, CPC-AHannahMeddaugh, CPC-AHeatherBonetz, CPC-AHeatherBrewer, CPC-AHeatherPendleton, CPC-AHeatherShropshire, CPC-AHeatherUdell, CPC-AHemaliMehta, CPC-AHiediAprilleBuchholtz, CPC-AHollyKing, CPC-AIngridFrancescaNazarioGarcia, CPC-AIshkaCKershaw, CPC-AIvanRupertEPobre, CPC-AJackiCosner, CPC-AJacquelineEsposoEscota, CPC-AJamesGraziano, CPC-AJamiePilsbury, CPC-AJanetLoudin, CPC-AJanisWenger, CPC-H-AJasmineAlexandriaBrooks, CPC-AJasonKleinsorgen, CPC-AJayneAFisher, CPC-AJeanetteBoeckman-Vitalich, CPC-AJeceLynAbenirRosales, CPC-AJenelRamacieri, CPC-AJenniferCox, CPC-AJenniferHicks, CPC-AJenniferJones, CPC-AJenniferNorton, CPC-AJenniferOlsen, CPC-AJennyPrim, CPC-AJennyVega, CPC-AJennylynPerezDestreza, CPC-AJeremyRedd, CPC-AJerryGlennParrishJr, CPC-AJesicaSanchez, CPC-AJessicaKreider, CPC-AJessicaHolzberger, CPC-AJessicaProphete, CPC-AJessicaSpurlock, CPC-AJillMcMillin, CPC-AJillannHastay, CPC-AJoanWeaving, CPC-AJoannaHarrell, CPC-AJodieABrown, CPC-AJoEllenRivera, CPC-AJohnThaddeusMoralTan, CPC-AJosieLeighJohnson,CPC-A, CPC-H-AJuliaAHuslig, CPC-AJulieBurns, CPC-AJulieIllig, CPC-AJulieMJohnson, CPC-AJulieNewcomb, CPC-AJulieToledano, CPC-AJuliusLeoncioLaganzonDonor, CPC-AJunelMaximoAgliam, CPC-AKarenByrdy, CPC-AKarenMages, CPC-AKatherineCherylMiller, CPC-A
newly credentialed members

www.aapc.com October 2012 49
Newly Credentialed Members
KathleenJMason, CPC-AKatieSkinner-Davis, CPC-AKatlynMarieThayer, CPC-AKatrinaCartwright, CPC-P-AKayeAnnDeLaCruz, CPC-AKeitraWilkerson, CPC-AKelliBeard, CPC-AKellyCook, CPC-AKellyDavis, CPC-AKendallRasmussen, CPC-AKerrySpako, CPC-AKevinDurmala, CPC-AKhineOhn, CPC-AKilleenRyan, CPC-AKimHudson, CPC-AKimMareeLee, CPC-AKimTMinito, CPC-AKimberlyArmstrong, CPC-AKimberlyWilley, CPC-AKishorSatishJoshi, CPC-AKrisMichaelRocamora, CPC-AKristenKnox, CPC-AKristenMcCullough, CPC-AKristinDyer, CPC-AKristinaAntloga, CPC-AKristinaMeredith, CPC-AKurtEvanVillanueva, CPC-AKyraMunley, CPC-ALaDeanSpring, CPC-ALaNyahTriniceGeorge, CPC-ALathaPalraj, CPC-ALatishaEasterling, CPC-ALauraCross, CPC-H-ALaurieJMiller, CPC-ALaurieJohnson, CPC-H-ALaurieWaldman, CPC-ALeandraDay, CPC-ALeoPanergoMararac, CPC-ALeonellynPagsuyoinRollan, CPC-ALeslieHines,CPC-A, CPC-H-ALeslieKarenMacapusPiangco, CPC-ALindaTaylor, CPC-ALindaBecker, CPC-ALindaKDonovan, CPC-ALindaSBates, CPC-ALisaMichellePerry, CPC-ALissetteSuarez-Colon, CPC-ALolaElder, CPC-ALoraineAnneThompson, CPC-ALoriHoltgrefe, CPC-ALoriDeTurk, CPC-ALoriGlynn, CPC-ALoriJMarchbanks, CPC-ALorraineCarson, CPC-ALorraineScandia, CPC-ALucyPerez, CPC-ALuisClaroDiazBelocura, CPC-ALuzAOcon, CPC-ALydiaJoAnnYauger, CPC-ALyndseyGilmore, CPC-AMa.RenaflorAlmonte, CPC-AMadhuriNaik, CPC-AMarcelaCastro, CPC-AMarcelliniJoycePatricio, CPC-AMarciaSandraRiley, CPC-AMargaritaMontalvo, CPC-AMariaAnneGerona, CPC-AMariaBernadetteBKho, CPC-AMariaCalvelo, CPC-AMariaEloisaCavoto, CPC-AMariaLorenaCendejas, CPC-AMariaTeresaPenaranda, CPC-AMaribelRomero, CPC-AMaricruzRoman, CPC-AMarilynBartlett, CPC-AMarioRelojEngracial, CPC-AMarisolPena, CPC-AMarissaLynnTasker, CPC-AMaritesAEstreller, CPC-AMaritzaErinValadez, CPC-A
MarjorieJadaGritton, CPC-H-AMarkJaysonSCajayon, CPC-AMarkJosephLavadoCando, CPC-AMarthaKristinaCariagaBoladas, CPC-AMarthaWeiand, CPC-AMaryAHanson, CPC-AMaryamFakhrai, CPC-AMaryJaneGalmanSulit, CPC-AMauraCarlson, CPC-AMaureenBenbinenRosos, CPC-AMavisLee, CPC-AMeganLauraArgyle, CPC-AMeganMaxwell, CPC-AMeganParsons, CPC-AMeiHuiChen, CPC-AMelanieBSilver, CPC-AMelanieElliott, CPC-AMelissaHarris, CPC-AMelissaJarrard-Mahayni, CPC-AMelissaWilliams, CPC-AMelvinCarloGrimpola, CPC-AMichaelaLeonoraNarzolesBarit, CPC-AMicheleMullen, CPC-AMicheleZanella, CPC-AMichelleAndalNavarro, CPC-AMichelleAulbach, CPC-AMichelleJackman, CPC-AMichelleLynnBrown, CPC-AMichelleWade, CPC-AMickelLeeHamilton, CPC-AMilagrosEvangelinaCuelloGarrido, CPC-AMildredFlower, CPC-AMindiBandao, CPC-AMistyMcCormick, CPC-AMitchelleSaezVilla, CPC-AMollyMarieHansen, CPC-AMonaMahajan, CPC-AMonicaLMunguia, CPC-AMoniqueChante’Caldwell, CPC-AMuzammilHusainmiyaKhatib, CPC-ANancyKCook, CPC-ANariflorFlorendoBolo, CPC-ANatalieBloodsworth, CPC-ANicoleDunn, CPC-ANiveditaShankarTalele, CPC-ANorindaCruz, CPC-ANormaOffutt, CPC-ANusratSiddiqui, CPC-AOliverReyPateniaStoDomingo, CPC-APaigeRubio, CPC-APamelaCordoba, CPC-APamelaMarston, CPC-APatFrederick, CPC-A,CPC-H-A
PatriciaBooth, CPC-APatriciaLHenry, CPC-APatriciaShawler, CPC-APatriciaVictoriaCalope, CPC-APatriciaWhite, CPC-APatrickJayPatricioGuevarra, CPC-APatsiSawyer, CPC-APauletteMayLeynesSaludo, CPC-APaulineSheevaCatalan, CPC-APeggyMissall, CPC-APeggyWindle, CPC-APennyRenaeSummers, CPC-APhilipVelasquezSantos, CPC-APrajaktaAvinashRane, CPC-APreciousAnaMarieAispornaMartinez, CPC-APunamNath, CPC-ARachaelRees, CPC-ARachelAnnCRabena, CPC-ARachelEmilyMartineau, CPC-ARachelMaw, CPC-ARachelSpitzer, CPC-ARaelNonaCruzCatalan, CPC-ARahulBhalerao, CPC-ARakhiBhowmick, CPC-ARashmiKandalgaonkar, CPC-ARebekahAnaMaeCorreaBullecer, CPC-ARebekahVansandt, CPC-A
ReneeUnpingcoIoane, CPC-ARhowelaCapitleMansueto, CPC-ARichardCSimmons, CPC-ARichardGazzerro, CPC-ARichardHermosoGannaban, CPC-ARigobertoSanchez, CPC-ARinaMolina, CPC-ARitaNooney, CPC-H-ARitaLyman, CPC-ARitaNess, CPC-ARobinMFowler, CPC-ARomeliaRincon, CPC-ARonPauloStaAnaRico, CPC-ARonaldAllanLadiaAdriano, CPC-ARonnalieBaylonMacaraeg, CPC-ARonnetteLGonsowski, CPC-ARosellaARamos, CPC-ARoss-AnnMallillinSimangan, CPC-ARoyHisananAbdul, CPC-ARuelDPagayucan, CPC-ARupeshKadam, CPC-ASachinShankarSalve, CPC-ASamanthaRoberts, CPC-ASambandanBuddhaKavitha, CPC-ASandeshKadam, CPC-ASandraBennett, CPC-ASandraGMenne, CPC-ASandraRainey, CPC-ASaraJLuhning, CPC-ASarahEllenFredriksen,CPC-A, CPC-H-ASarahKrey, CPC-ASarahMeekhof, CPC-ASarahWolfe, CPC-H-ASarikaShingade, CPC-ASarojinideviMB, CPC-ASathishKumar, CPC-ASathyaAlagurajh, CPC-ASeethalakshmiIyer, CPC-AShaneCrouch, CPC-AShanellDelCorro, CPC-AShannonBoyd, CPC-AShannonMcClain, CPC-AShanthiDharuman, CPC-AShantriceScurry, CPC-ASharonAnton, CPC-ASharonPatriceHarris, CPC-ASharrieMercadoIlagan, CPC-AShawnMichaelHughes, CPC-AShawnaYost, CPC-ASheilaHudson, CPC-AShelleyWhitacre, CPC-ASherrilynMarieYoung, CPC-AShingarjitSandhu, CPC-AShrutiMaheshKoli, CPC-AShrutikaChandrakantKadam, CPC-ASiriBaker, CPC-ASmithaMahendraTarphe, CPC-ASnehaPrabhu, CPC-ASoniaJudd, CPC-ASonjaCrouch, CPC-ASpringMcKeown, CPC-AStaceyKeller, CPC-AStacyAnnMiles, CPC-AStacyMartin, CPC-AStefanieHager, CPC-AStephanieAnnParrish, CPC-AStephanieDAter, CPC-AStephanieMaldonado, CPC-ASteveJacobson, CPC-ASteveBurns, CPC-ASusanAgneessens, CPC-ASusanJewell, CPC-ASusanVanDaveer, CPC-ASuzannaBennett, CPC-ATabithaGeiger, CPC-ATahneeNSimpson, CPC-ATammiThompson, CPC-ATammyChereeTucker, CPC-ATammyMays, CPC-ATaniaOceguera, CPC-A
TanyaTamaraAngel, CPC-ATaraLipscomb, CPC-ATashaLynFord,CPC-A, CPC-H-ATaunyaSanders, CPC-ATeresaClifford, CPC-ATeriAdams, CPC-ATiffanyDabney, CPC-ATiffanyNicoleHansbury, CPC-ATiffanyStretton, CPC-ATimMecikalski, CPC-ATinaLeslie, CPC-ATommieWade, CPC-ATonyaLynnGreen, CPC-ATonyaMarieHarris, CPC-ATraciNacarato, CPC-ATracyAnneBonacci, CPC-ATralisaRaeKettner,CPC-A, CPC-H-ATrishaSelby, CPC-ATrudyABerkey, CPC-ATrudyKennedy, CPC-P-ATruptiNitinThube, CPC-AUjjawalaBVerma, CPC-AVaishnaviArunOtawkar, CPC-AVanessaJarabeReyes, CPC-AVickieChambers, CPC-AVictoriaKempe, CPC-AVidyaShankarBhuvad, CPC-AVirgilioJrAntonio, CPC-AWayneWilliamson, CPC-AWendyMDonahue, CPC-AWilliamAlfonsoMorales, CPC-AWilliamWAsbury, CPC-AWilliamWares, CPC-AWilroseAbiulDesabille, CPC-AYafenGromm, CPC-AYnaiciousKCrownie, CPC-AYogeshShantaramKadam, CPC-AYolimarZayas-Colon, CPC-AYvetteLawrence, CPC-AZyraMaeMenorNofuente, CPC-A
SpecialtiesAmyGTulip,CPC, CHONCAnaIBenitez-Marrero,CPC, CGSCAndreaBaskette,CPC, CEMCAngelaRMaxey,CPC, CEDCBayushKumssa,CPC, CEDCBradleyChapman, CPCOCarolePlowman,CPC, COBGCCarynSmith,CPC, CPMACathyThebeau,CPC, CPMACharleneJCihon,RN,CPC, CPMAChristopherT.Manion,CPC, CPMAConnieKayFullerton,CPC, CEMCDeniseGiliberti,CPC,CANPC, CGSCDonnaJMills,CPC, CCCDonnyFlores,CPC, CPCODorotheaWood,CPC-A, CCCFayeGGrile,CPC, CPCOFlorenceJohnson,CPC, CPMAGinaDBelafonte,CPC,CPC-H, CPMAJanStrattonLyon,CPC-P, CPMAJenniferEaster, CPMAJennyJeanWheaton,CPC, CPMAJillPaiva, CPCOJillRSank,CPC, CASCCJodyWegesin,CPC, CEDCJulieWilson,CGSC,COBGC, COSCKelliGuy,CPC, COSCKellieLKuhn,CPC, CEMCKevinMacaulay,CPC, CPMAKimberlyIvery, CPMALauraCornell,CPC, CPMALeighAnnRWhite,RN,CPC, CCCLisaWalters, CIRCCLoriAnnAnderson,CPC-A, CUCLoriWingo,CPC, CPMAMaryJuanitaGaljour,CPC,CEMC, CUC
MaryUnrue, CEDCMelindaBromberg,CPC, CPC-H,CPC-P,CCCMicheleWallace, CFPCNanetteIDuncan-Rodriguez,CPC, CCCNatalieRWilliams,CPC, CPMAPamelaKummer, CPCOPaulaJHayes,CPC, CPMAPedroMaestre,CPC, CPMAPetunaSelby, CPCOSandraSperrazza,CPC, CPMAShannonJackson,CPMA
StaceyABunk,CPC, CCCStacyLynnSeglem,CPC, CGICTerriWilmot,CPC, CPMATiffanyThuyT.Le,CPC, CPMATracyPalmer,CPC, CPPMTrishaAAchtziger,CPC, CPC-H,CPC-P,CCCTrishaLeavitt,CPC-A, CPMA,CASCC,CGICYvetteMatthews,CPC, CPMAZoeMantooth,CPC, CIRCC
Magna Cum LaudeAmyLove, CPCAndreaShaw, CPC-AAngelaMarieRolen, CPC-AAnnaEwaPianko,CPC-A, CPC-H-AArianneChristabelLacsonMaraan, CPC-ABasimaMahmoud, CPC-ACareyRussell, CPC-ACarlElexerCuyuganAno, CPC-ACheriStephenson, CPC-ACherylDenisePerez, CPC-AColleenDay, CPC-ADamaraArnold, CPCDavidDunn, MD,CPC-H,CIRCC,CCC,CCVTCDebraKutz, CPC-ADeniseReneeHitchcock, CPCEvelynMoreno, CPCGloriaBeatriceDesha, CPC-AJackieLynReginoAlcala, CPC-AJamesAngeloStevensVillaramaJavier, CPC-AJessicaTessman, CPCJustynaTaha, CPC-AKathleenRowell, CPC-ALindaKornacki, CPCLoriACox,CPC, CEMCMarisolLaxton, CPCMichelleCastilloVillar, CPC-AMichelleLynnGoatley, CPCMildredSjostrand, CPC-AOdemarisVelez, CPC-ARafaelaOrtiz, CPC-ARandiJoleneWidstrom, CPC-ASanjayMahadevMandavkar, CPC-ASheerinThasneemAbdulAzeez, CPC-AStephanieFlorence, CPC-ASusanJillMoore, CPC-HSusanMOwens,CPC, CGSCTaraDegroat, CPC-AVeronikaPetuhhova, CPC-AVinodPandurangSawant, CPC-AYolandaLafayeSimmons, CPC-A
A&P Quiz AnswerThe correct answer is B. Diverticulitis is small, bulging sacs or pouches of the inner lining of the intestine (diverticulosis) that become inflamed or infected. These pouches are most often in the large intestine (colon).

50 AAPCCodingEdge
■ Coding & Billing
To discuss this article or topic, go to www.aapc.com
Diagnostic Specificity Is Key to Payment Accuracy for MA PlansTake precautions when submitting more than eight diagnoses on a claim.
By Holly J. Cassano, CPC
Accurate payment under the Centers for Medicare & Medicaid Services (CMS) risk adjustment reimbursement model depends on diagnosis code specificity and reporting all current chronic conditions. A leading cause of incorrect and/or insufficient reim-bursement from Medicare Advantage (MA) plans is deficient hierarchal condition cate-gories (HCC) code reporting. CMS has been accepting up to eight diagno-sis codes since 2007. Unfortunately, many physician practices are either not aware of this, or their electronic health record (EHR) and/or clearinghouses allow only four to six diagnosis code entries for claims submis-sion. A practice can instruct its coders to submit all co-existing chronic diseases doc-umented at the time of service, but this is of no help if your EHR or clearinghouses won’t accept all of the diagnoses submitted.
Too Many Diagnosis Codes Cause ConfusionA Coding Edge reader—understanding the importance of reporting all active chronic conditions that co-exist at the time of ser-vice (TOS)—recently asked about proper processes for submitting diagnoses in the EHR, and what to do if you have to submit more than eight diagnoses on a claim form. Specifically, the reader asked, what happens if and when:
• The physician treats patients with 10 or more diagnoses addressed during a visit?
• Coders validate the first eight diagnoses listed in lieu of sequencing?
• Providers do not sequence the diagnosis codes while listing more than eight diagnoses?
Educate the Vendor and PayerFirst, contact your vendor and find out (ver-bally and in writing) the number of diag-nosis codes the vendor will accept electron-ically per claim. Find out also if the vendor and payer will accept CPT® 99080 Special reports such as insurance forms, more than the information conveyed in the usual medical communications or standard reporting form, which may be used as an adjunct to a regu-lar evaluation and management (E/M) of-fice visit code to submit additional diagno-sis codes for capturing chronic conditions.Contact all MA plans with which the prac-tice participates, and obtain in writing how many diagnosis codes each payer will ac-cept. If the number is less than eight, ask if the payer will accept 99080 for the addi-tional diagnosis codes (and get the reply in writing).Inquire how many codes any commercial carriers accept in your practice to prevent future claims issues with the adoption of
ICD-10, which will require even great-er due diligence and coding specificity.
Sequencing Is ImportantSequencing can have a dramatic effect on payments if the nature of the presenting problem (NOPP) and subsequent co-ex-
isting conditions are either under-reported or incorrectly reported to an MA plan. The key to successful sequencing begins with an assessment and a plan. For example:
• Determine the primary diagnosis by identifying the primary focus of care.
• Determine which of the other diagnoses affect treatment and coexist at the TOS. Be sure to report these diagnoses (linking to other services isn’t necessary if only an E/M service is provided).
• All pertinent diagnoses must be listed to justify the services rendered.
The CMS risk adjustment model was imple-mented to promote specificity and discour-age vague or unspecified coding. ICD-10 will promote this, as well. To ensure com-pliance and receipt of accurate payments through proper identification of chronic diseases, implement a strategy now. Be sure payers recognize all the diagnoses reported, so you don’t suffer potentially harmful con-sequences to your practice down the road.
Holly J. Cassano, CPC, has been involved in practice management, coding, auditing, teaching, and consulting for multiple special-ties for the past 16 years. She served two terms as an AAPC local chapter officer, main-tains an online column for Advance for Health Information Professionals, and writes for
Justcoding.com. She is the CEO of ACCUCODE Consulting, LLC and blogs for medicalcodingandbilling.org via Consumer Media Network (CMN). She works for Preferred Care Partners as a CDI specialist, based out of The Villages, Fla. You can reach her at [email protected] and follow her on Twit-ter@hollycassano.
Takeaways:
• Deficient HCC reporting is a leading cause of incorrect and/or insufficient reimbursement from MA plans.
• Claims with more than eight diagnoses may be problematic.
• Work with your vendor and payer to assure numerous diagnoses don’t derail your claims.
50 AAPCCodingEdge
phot
obyi
Stoc
kpho
to©
Dani
elR.
Bur
ch

RVG_Crosswalk 2013_CodingEdge Ad_04_5012.indd 1 4/2/12 9:47 AM
NAMAS 4th ANNUAL AUDITING CONFERENCE Monday and Tuesday Decem ber 3-4 Grove Park Inn Resor t , Asheville, NC
PLEASE JOIN US FOR A NATIONAL CONFERENCE BUILT EXCLUSIVELY FOR AUDITORS! Fall Special—Bring your physician for HALF PRICE!! When you register for the conference you can bring your physician for just $495
REGISTER NOW!
Features of the NAMAS 4th Annual Audit ing Conference
A comprehensive and diverse program of audit ing topics An extensive line-up of expert speakers from across many specialty f ields
Pre-conference audit ing w orkshop (Sunday December 2) w ith hands-on skill building w ith a box lunch provided
Optional tw o day training sessions available on Friday and Saturday (November 30 & December 1) covering CPMA® and more
Earn up to 20 CEUs w hen attending both the preconference and conference
2013 Coding Update Session w ill be included during the conference
w w w.NAMAS-Audit ing.com 877-418-5564
2012
Proudly Sponsored by:
![July 2011 - AAPCstatic.aapc.com/5548A1AF-4C9F-49A2-BFE0-BFA7D2344700/... July 2011 3 [contents] 7 Letter from the Chairman and CEO 8 Coding News 11 Letter from Member Leadership 12](https://img.dokumen.tips/doc/110x75/5b0b925e7f8b9a0c4b8e0bac/july-2011-july-2011-3-contents-7-letter-from-the-chairman-and-ceo-8-coding-news.jpg)










![July 2011 - Amazon Web Servicesaapcperfect.s3.amazonaws.com/5548A1AF-4C9F-49A2-BFE0-BFA... · 2011-06-08 · July 2011 3 [contents] 7 Letter from the Chairman and CEO 8 Coding News](https://img.dokumen.tips/doc/110x75/5e9fd39d88ad2465c54bb2f6/july-2011-amazon-web-servicesaapcperfects3-2011-06-08-july-2011-3-contents.jpg)






![HEALTHCARE - Amazon Web Servicesaapcperfect.s3.amazonaws.com/5548A1AF-4C9F-49A2-BFE0-BFA... · 2015-03-20 · April 2015 3 [contents] Coding/Billing Practice Management Auditing/Compliance](https://img.dokumen.tips/doc/110x75/5e754e5d2e9b37231c4b0b18/healthcare-amazon-web-servicesaapcperfects3-2015-03-20-april-2015-3-contents.jpg)









![CPT 2012 - AAPCstatic.aapc.com/5548A1AF-4C9F-49A2-BFE0-BFA7D... · CPT ® 2012 on the Horizon ® e. C M Y ... [contents] 7 Letter from the Chairman and CEO ... surf, and CPT® 2012](https://img.dokumen.tips/doc/110x75/5ae287877f8b9a595d8d553e/cpt-2012-2012-on-the-horizon-e-c-m-y-contents-7-letter-from-the-chairman.jpg)
