Embed Size (px)
Citation preview

See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/259704654
Occupational Therapists' Attitudes, Knowledge, and Implementation of
Evidence-Based Practice: A Systematic Review of Published Research
Article in British Journal of Occupational Therapy · January 2014
DOI: 10.4276/030802214X13887685335544
CITATIONS
58READS
2,088
4 authors, including:
Some of the authors of this publication are also working on these related projects:
Victims of Crime View project
Care farming in the UK View project
Dominic Upton
Charles Darwin University
197 PUBLICATIONS 2,874 CITATIONS
SEE PROFILE
Danielle Stephens
University of Worcester
12 PUBLICATIONS 113 CITATIONS
SEE PROFILE
Laura Scurlock-Evans
University of Worcester
28 PUBLICATIONS 265 CITATIONS
SEE PROFILE
All content following this page was uploaded by Dominic Upton on 15 November 2015.
The user has requested enhancement of the downloaded file.

24 British Journal of Occupational Therapy January 2014 77(1)
Critical review
IntroductionEvidence-based practice (EBP) is the procedure whereby clinicians incorpo-rate best research evidence, clinical expertise, and patient values, resultingin the presentation of the most appropriate and efficient services to theirpatients (Strauss et al 2010). EBP is conceived as a 5-step process involving:1) the development of a clinical question; 2) assimilation of the best availableevidence in order to answer the question; 3) systematic and critical appraisalof this evidence; 4) applying this evidence to a clinical problem; and 5)evaluation and revision of the previous steps in the process and identifyingany areas of change for future applications (Strauss et al 2010).
EBP provides a framework in which practitioners can consider clinicalproblem solving, allowing them to keep informed with current and bestpractice within their area (Upton and Upton 2006a). Due to the significantdemand for healthcare, which seems to be surpassing supply, EBP hasrecently been considered as a highly favourable approach which promises bothquality and efficiency in patient care (Oliver and McDaid 2002, Taylor 2007).Support for the adoption and implementation of EBP is apparent acrosshealth professions and internationally (Stergiou-Kita 2010). Additionally,EBP has been associated with improvement in patient outcomes and care,whilst also reducing associated healthcare costs (Melnyk et al 2010). Moreover,researchers have argued that the interventions used by therapists need to be
Occupational therapists’ attitudes, knowledge,and implementation of evidence-based practice:a systematic review of published researchDominic Upton,1 Danielle Stephens,2 Briony Williams,3 and Laura Scurlock-Evans4
Key words:Evidence-based practice,occupational therapy,knowledge, researchutilization.
Introduction: Evidence-based practice is the procedure whereby clinicians incorporatebest research evidence, clinical expertise, and patient values to provide best patient care.Recently, there has been a significant push towards occupational therapists’ adoptionof evidence-based practice. This systematic review aimed to determine occupationaltherapists’ attitudes, knowledge, and utilization of evidence-based practice.
Method: A search of literature published between 2000–12 was conducted inrelation to occupational therapists’ practice. Academic Search Complete, CumulativeIndex of Nursing and Allied Health Literature Plus, PsycARTICLES, Ingenta, Medline,Science Direct, and Journal Storage were systematically searched using MeSH andfree-text keywords. Google Scholar and reference lists were also searched.
Findings: Thirty-two papers were selected for review: 23 were quantitative, 8 were qualitative, and 1 used a mixed methods design. Studies demonstrated thatoccupational therapists hold positive attitudes towards evidence-based practice.However, these attitudes do not translate into practice, with research indicating alack of evidence-based practice utilization. Occupational therapists perceive a numberof barriers to evidence-based practice, including lack of time, lack of availabilityand accessibility of research, and having limited research skills.
Conclusion: It is essential that educational and training initiatives providetherapists with the tools and support they need to engage fully with researchevidence and its application within clinical care.
© The College of Occupational Therapists Ltd.Submitted: 2 May 2012.Accepted: 30 August 2013.
1Professor of Psychology, Faculty of Health,University of Canberra, Canberra, Australia.
2PhD student, Institute of Health and Society,University of Worcester, Worcester.
3Head of Academic Unit, Health and AppliedSocial Sciences, University of Worcester,Worcester.
4Psychology Assistant, Psychological Sciences,University of Worcester, Worcester.
Corresponding author:Laura Scurlock-Evans, Psychology Assistant,Psychological Sciences, University of Worcester,Henwick Grove, Worcester, WR2 6AJ. Email: [email protected] Twitter: @LScurlockEvans
Reference: Upton D, Stephens D, Williams B,Scurlock-Evans L (2014) Occupationaltherapists’ attitudes, knowledge, andimplementation of evidence-based practice:a systematic review of published research.British Journal of Occupational Therapy,77(1), 24–38.
DOI: 10.4276/030802214X13887685335544
by guest on November 4, 2015bjo.sagepub.comDownloaded from

25British Journal of Occupational Therapy January 2014 77(1)
Dominic Upton, Danielle Stephens, Briony Williams, and Laura Scurlock-Evans
both clinically and cost effective in order for occupationaltherapy to survive in the current healthcare climate (Taylor2007). Thus, there has been a significant push towardsoccupational therapists’ adoption of EBP within their dailyclinical care (Brown et al 2009).
Occupational therapy is a profession that reiterates theimportance of EBP implementation for both ensuring highquality care (College of Occupational Therapists [COT]2003, Crist 2010) and advancing the field (American Occu-pational Therapy Association [AOTA] 2007). The processof EBP implementation within occupational therapy is,essentially, based on the same principles of EBP for otherhealthcare disciplines (Bennett and Bennett 2000). However,despite the importance attributed to these principles, agap between practice and research within occupationaltherapy is frequently reported (Hu et al 2012, Salls et al2009). Although this problem is not unique to the field ofoccupational therapy (it has been observed with numerousother professional groups, such as nurses [Melnyk et al2004]), it is of concern. Research has indicated that occu-pational therapists may rely overly on personal clinicalexperience (Bennett et al 2003) and peer opinion (Döpp et al 2012). Furthermore, occupational therapists may neglectto develop and pursue information-seeking behaviours,such as learning to locate, access, evaluate, and utilize bestavailable evidence, that are considered vital for appropriateEBP implementation (Gilman 2011). However, it is impor-tant to realize that occupational therapists are faced withmultiple challenges within their daily practice, includinglimited organizational and structural systems, which maycontribute to their lack of EBP utilization (Caldwell et al2008). At a time of increasing accountability in the health-care professions (Prior et al 2010), it is essential that occu-pational therapy, as a profession, encourages the uptake ofeffective and relevant research to enhance the quality andconsistency of clinical decision making. This requires thatefficient initial EBP training and continuing educationalopportunities for developing and expanding EBP skills areavailable to therapists throughout their careers (Bennettand Bennett 2000). However, a thorough understanding ofthe factors affecting EBP implementation is first required toensure such training and support effectively meets the needsof the profession.
Aim of the reviewThe aim of this review was to synthesize research examin-ing occupational therapists’ attitudes, utilization, knowledge,and understanding of EBP. The findings of the review arethen considered in terms of how EBP implementation canbe increased and enhanced within clinical practice.
MethodDesignOwing to the heterogeneity of study designs and outcomemeasures, and inclusion of qualitative research, a meta-analysis
was rendered unfeasible. Therefore, the present systematicreview adopted a narrative analysis approach (using wordsand texts to summarize and explain findings of researchsynthesis), following the guidelines and reporting stan-dards identified by PRISMA (Moher et al 2009) and Greenet al (2006). This review framework was adopted due tothe flexibility it provides for synthesis of both quantitativeand qualitative study results.
Search strategyA search of the literature was conducted in relation tooccupational therapists’ current practice during the period2000–12. Free-text key words and MeSH (or equivalent)terms were used in combination (using Boolean operators)to systematically search the following databases: AcademicSearch Complete, Cumulative Index of Nursing and AlliedHealth Literature (CINAHL) Plus, American PsychologicalAssociation databases (e.g. Psych Articles), Ingenta, Medline,Science Direct, and Journal Storage (JSTOR). Specific key-words and phrases used included: ‘evidence-based practice’,‘occupational therapy’, ‘clinical practice’, ‘guidelines’, ‘barriers’,‘attitudes’, ‘knowledge’, ‘understanding’, ‘effectiveness’,‘implementation’, and ‘evidence’. Examples of specific MeSH(and equivalent) terms used included: ‘“Evidence-BasedPractice”[Mesh]’, ‘MH “Evidence-Based Practice+”’ and ‘MH“Occupational Therapy Practice, Evidence-Based”’. GoogleScholar was searched using the free-text keywords identifiedabove, and reference lists of retrieved articles were alsosearched for any additional articles meeting the criteria.
An example search strategy of one of the databases isavailable from the corresponding author upon request.
Quality appraisalStudies included in the review were quality appraised usingtools based on the guidelines developed by the McMasterUniversity Occupational Therapy Evidence-Based PracticeResearch Group (Law et al 1998, Letts et al 2007) andadapted by Alexandratos et al (2012). These tools werefurther modified to allow each article to be rated as strong,average, or poor, based upon the percentage of assessmentcriteria fulfilled (0–33%, 34–66% or 67%+). Articles wereappraised by two independent raters and disagreementsresolved by consensus.
Quality rating was not used as an inclusion criterionbut was used to help to inform the confidence with whichstudy results could be interpreted in the review synthesis.
Search outcomeThe studies were each reviewed initially in relation to thefollowing inclusion criteria:� English language publications between 2000 and 2012
(to ensure both breadth of coverage and currency ofinformation)
� Published within a peer-reviewed journal� Provided sufficiently detailed, extractable results for qual-
ified occupational therapists if more than one professionalgroup’s results were reported
by guest on November 4, 2015bjo.sagepub.comDownloaded from

26 British Journal of Occupational Therapy January 2014 77(1)
Occupational therapists’ attitudes, knowledge, and implementation of evidence-based practice: a systematic review of published research
� A focus was given to either one or all of the following:— Occupational therapists and perceived attitudes
towards EBP— Occupational therapists and perceived knowledge
or understanding of EBP — Occupational therapists and EBP implementation
(including barriers)
provided a summary of key findings for quantitative reports(Table 1), qualitative reports (Table 2), and mixed methodsreports (Table 3).
Of the reviewed articles, 14 were assigned a good qualityrating, 16 articles were assigned an average rating, and 2 wereassigned a poor rating.
Attitudes and values toward EBPAll studies demonstrated positive attitudes towards EBP tosome degree, and some suggested therapists valued EBP as ameans of enhancing the credibility of both the field and them-selves as professionals (Fänge and Ivanoff 2009, Karlssonand Törnquist 2007, Swedlove and Etcheverry 2012).
However, the research indicated a substantial proportionof therapists viewed EBP more negatively: for example,some practitioners perceived EBP as too complicated, andthe transition of research into practice as requiring toomuch effort (Döpp et al 2012). Furthermore, whilst manytherapists valued EBP and research utilization (RU) inprinciple (Bennett et al 2003, Brown et al 2009, Curtin andJaramazovi 2001, Humphris et al 2000, Heiwe et al 2011,Hu et al 2012, Lyons et al 2010, Lyons et al 2011), some feltensuring knowledge was up-to-date, rather than RU per se,was the priority (Karlsson and Törquist 2007), and othersconsidered active research to be unnecessary (Lyons et al2011). This suggests there is a potential issue concerningresearch generation, which may have an impact on theamount of practitioner-led contributions to research.
Research examining EBP attitudes across numerous dis-ciplines discovered that occupational therapists held positiveattitudes (which were at a similar level to professionals fromother disciplines), but reported greater levels of shared EBPlearning with colleagues (Caldwell et al 2007). However, theywere also less likely to report changes within their clinicalpractice due to research evidence (Caldwell et al 2007), indi-cating a disparity between attitudes and behaviour.
A range of factors may influence, or relate to, therapists’attitudes towards EBP. For example, Brown et al (2010) iden-tified higher occupational educational attainment as a strongpredictor of positive attitudes towards EBP, although Cameronet al (2005) found the opposite to be the case. However, slightdifferences in the demographics of the two studies’ samplesmay explain these contradictions. Nevertheless, Sweetland andCraik (2001) found that participants identified postgraduatecourses as playing an influential role in intervention choice.Döpp et al (2012) discovered that occupational therapistspracticing within an academic hospital held significantlymore positive perceptions of EBP than occupational thera-pists in other clinical settings. Furthermore, Bennett et al(2003) found that occupational therapists practicing withinrural areas were also found to hold more negative attitudestowards EBP, claiming that it was too demanding. However,this pattern failed to be replicated in other research (Hu et al2012). The differences between the two studies may reflectadvances within technological infrastructure in rural areas.
Additionally, therapists who had graduated more recentlyor had received prior EBP training appeared to hold more
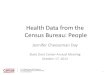
Fig. 1. PRISMA flowchart of the study retrieval and selection
process (Moher et al 2009).
Incl
uded
Elig
ibili
ty
Scre
enin
gId
enti
ficat
ion
Quantitativestudies included
(n = 23)
Records identified throughdatabase searching
(n = 12970)
Additional records identifiedthrough other sources
(n = 20)
Records after removal of duplicates publications(n = 10652)
Records screened using titleand abstract (n = 10652)
Mixed methodsstudies included
(n = 1)
Qualitativestudies included
(n = 8)
Full text articles assessedfor eligibility (n = 86)
Records excluded(n = 10568)
Full text articlesexcluded based oninclusion criteria
(n = 54)
In addition to the above, for quantitative studies an out-come measure was used to measure at least one of: attitudestowards EBP, knowledge of EBP, or implementation of EBP,and studies were reviewed in relation to these criteria.Qualitative studies were reviewed in relation to whetherthe study explored any or all of: perceived knowledge,understanding, attitudes, or implementation of EBP andwhether the study gave clear and accurate definitions ofthe research question and methodology adopted.
In total, 32 studies met the above inclusion criteria, ofwhich 23 were quantitative, 8 were qualitative, and 1 used amixed methods design. The PRISMA flowchart provides abreakdown of the assessment and exclusion of the abovearticles (Fig. 1).
FindingsAll 32 articles were summarized under the following headings:reference, sample, design, purpose, and results (Green et al2006). In addition, a quality rating was assigned to each article.
Study results were extracted from the abstract and fullarticle by one author and reviewed by a second author (toensure consistency and rigour), based upon the themes ofEBP attitudes, knowledge, and implementation. Study results
by guest on November 4, 2015bjo.sagepub.comDownloaded from

27British Journal of Occupational Therapy January 2014 77(1)
Dominic Upton, Danielle Stephens, Briony Williams, and Laura Scurlock-Evans
Table 1. Study characteristics and findings of quantitative reportsReference Sample Design Purpose Results Quality ratingHumphriset al 2000
Pollock et al 2000
Sweetlandand Craik2001
Dysart and Tomlin2002
Bennett et al 2003
McCluskey2003
Conveniencesample of 78occupationaltherapists fromthe UK (responserate = 78%).
Stroke rehabilitationprofessionals:physiotherapists(n = 27), occu-pational therapists(n = 26), nurses (n = 22), speechand languagetherapists (n = 6),others (n = 5).
Random sample of125 members ofthe NationalAssociation ofNeurologicalOccupationalTherapists work-ing with adultstroke patients.
Random sampleof 209 (responserate = 58%)Americanoccupationaltherapistmembers of theAmericanOccupationalTherapyAssociation.
Random sampleof 649 (responserate = 44%) occu-pational therapistscurrently membersof OccupationalTherapy AustraliaLimited (OTA,formerly OTAustralia).
Purposive sampleof 67 Australian(New South Wales)occupationaltherapists.
Cross-sectionalpostal survey(questionnairedeveloped bythe authors).
Focus groupresulting in thedevelopment ofa postalquestionnaire.
Postal surveydeveloped bythe authors.
Postal surveydesigned by theauthors.
Postal survey;modified versionof McColl et al(1998)questionnaire;evidence-basedmedicine.
Questionnairesurvey; modifica-tion of Upton andLewis (1998)survey concerningEBP and health-care professionals.
Explore factors that inhibitand facilitate the use ofresearch evidence byoccupational therapists.
Identify the barriers to EBPin stroke rehabilitation;examine differences ofperceived barriers betweenthe disciplines.
Identify the extent towhich EBP was used bytherapists working withadult stroke patients.
Explore how Americanoccupational therapistsaccess and use clinicallyrelevant research findings.
Determine practitioners’attitudes and perceptionsof EBP and their trainingneeds; perceived confidencein practitioners’ EBP skills;what EBP resources are reliedupon and what barrierspractitioners perceivetowards EBP utilization.
Determine therapists’ EBPknowledge and skill;participation in continuingEBP education; practitioners’perceived barriers towardsEBP utilization.
Many occupational therapists held positive attitudestowards the use of research in practice. Top threebarriers to EBP implementation were: workloadpressures, time limitations, and insufficient staffresources. Top three facilitators were: protected time,frequent educational sessions, and specific additionalstaff to enable research evidence implementation.
Key barrier in ability found to be lack of trainingin appraisal and interpretation of research results;occupational therapists expressed significantlyless confidence in their ability. Key barriers towardsEBP were found to be a lack of confidence in thevalidity of research and difficulties in applyingfindings to clinical practice. Majority of respondentsheld positive attitudes towards EBP (92%).Occupational therapists perceived more, orbigger, barriers than nurses.
Other therapists were identified as a key influentialfactor in intervention choice, alongside attendance atpostgraduate courses. Custom, practice, and expertopinion were identified as the most frequentlyapplied forms of evidence. Recently qualifiedprofessionals were more likely to report usinghigher levels of evidence in their practice. Otherimportant factors influencing practice included:relevance of research, time, knowledge, and support.
Occupational therapists occasionally accessedresearch information; 57% implemented 1–5 new,research-based treatment plans a year. A greaternumber of participants with 15 or more years ofclinical experience did not feel that researchconclusions usually translated into treatment planscompared to participants with less experience (p < 0.01). 59% of respondents had time providedfor training, but 45% felt there was no time toaccess research information. Barriers included:lack of time, education costs, lack of research skills,and placing less value on research evidence thanclinical experience.
Highly positive attitudes towards EBP (95.7%)and 56.0% reported using research in clinicaldecision making; however, practitioners rely onclinical experience in clinical decision making(96.3%); practitioners infrequently utilize EBPresources and lack confidence in their EBPrelated skills; lack of time and available evidenceperceived to be significant barriers.
Practitioners who had graduated in the previous5 years displayed more confidence in their EBPskills but lack confidence in critical appraisal ofevidence. Perceived barriers included lack of timeand large workloads.
Poor
Average
Average
Average
Strong
Average
by guest on November 4, 2015bjo.sagepub.comDownloaded from

28 British Journal of Occupational Therapy January 2014 77(1)
Occupational therapists’ attitudes, knowledge, and implementation of evidence-based practice: a systematic review of published research
Table 1 (continued)Reference Sample Design Purpose Results Quality ratingGosling andWestbrook2004
Cameron et al 2005
McKenna et al 2005
Upton and Upton2006b
Caldwell et al 2007
Random sample from 65 hospitals:physiotherapists (n = 228), socialworkers (n = 146),occupational therapists(n = 118), pharmacists(n = 84), dietitians (n = 78), speechpathologists (n = 77),clinical psychologists (n = 59).
Random sample ofoccupational therapistspracticing in theUnited States (USA)and Puerto Rico (n = 131).
Two random samplesof Australianoccupationaltherapists: nationalsample from membersof the Australianoccupational therapyassociation(Occupational TherapyAustralia) (n = 124),and State sample fromQueensland and NewSouth Wales (n = 89).
Stratified sample of1,000 UK allied healthprofessionals (responserate = 66.6%), 188being occupationaltherapists (responserate = 72.9%).
Random sample ofrecent graduates from 3 London-baseduniversities:occupational therapists(n = 29), nurses (n = 1),physiotherapists (n = 10), and socialworkers (n = 26).
A survey consist-ing of a 25-itemquestionnairecomprisingclose-endedquestions.
Postal surveyquestionnairebased on designby Humphris et al (2000).
Postal survey.
Postal survey.
Anonymouspostalquestionnaire.
Aimed to determinepractitioners’awareness of anonline evidencesystem; utilization ofthe evidence;perception of theevidence system onclinical practice; andperceived barrierspreventing utilization.
Examine USA occu-pational therapists’utilization of EBP;determine whetherEBP utilization differsbased on demo-graphics.
Explore therapists’uptake of OTseeker(an online EBPresource) and toexplore whether ithas had an impact ontheir clinical practice.
Explore allied healthprofessionals’practice andknowledge of EBP.
Explore relevance ofinitial training inrelation to EBP;explore practitioners’confidence inengaging with EBP.
A large proportion of respondents who hadheard of the online evidence resource utilized it(75%). Factors that affected utilization of theevidence resource included accessibility,perceived support, and computer skills. Lack oftraining in utilization of the online evidencesystem was perceived to be a significant barrier.
Large proportion of therapists held positiveattitudes towards EBP (98%). Very fewtherapists utilize EBP within their clinicalpractice (p < 0.01). Therapists with highereducational attainment held increasing views of the importance of EBP utilisation.
Most participants had heard of OTseeker (86%),whereas only over half of these had accessedthe resource (56.3%). Main barriers were foundto be lack of time. Only 13.6% of practitionersindicated that the resource had impacted theirclinical practice, although two-thirds reportedimproved knowledge due to accessing theinformation on OTseeker.
Occupational therapists reported greaterknowledge of EBP than podiatrists,radiographers, and orthoptists, but similarknowledge levels to physiotherapists, dieticians,speech and language therapists, andpsychologists. However, the majority ofoccupational therapists (41.7%) self-reportedtheir knowledge as low. Occupational therapists(and podiatrists) rated their awareness ofinformation sources lower than most othergroups, and (alongside pathology assistants andpharmacists) preferred to use evidence providedby colleagues. Barriers to EBP were similarbetween all health professionals, two keybarriers identified were lack of time and money.
Practitioners held positive attitudes towards EBP and research evidence; however,implementation of EBP by practitioners isinfrequent with limited utilization of researchresources.
Strong
Strong
Strong
Strong
Strong
by guest on November 4, 2015bjo.sagepub.comDownloaded from

29British Journal of Occupational Therapy January 2014 77(1)
Dominic Upton, Danielle Stephens, Briony Williams, and Laura Scurlock-Evans
Table 1 (continued)Reference Sample Design Purpose Results Quality ratingKarlsson andTörnquist2007
Welch andDawson2007
Brown et al2009
Salls et al2009
Brown et al2010
Lyons et al2010
425 Swedishoccupationaltherapists(response rate =74.4%) took partin a baselinequestionnaire and442 (responserate = 70.4%)took part in afollow-up survey.
24 senioroccupationaltherapistscurrentlypracticing withinthe NHS.
Conveniencesample; paediatricoccupationaltherapists fromAustralia, UnitedKingdom andTaiwan (n = 696,response rate = 56.6%).
Purposive sampleof occupationaltherapistspracticing inPennsylvania (n = 930).
ConvenienceSample;occupationaltherapists fromTaiwan (n = 413),Australia (n = 137), and theUnited Kingdom(n = 144).
Conveniencesample of 145 UK paediatricoccupationaltherapists(response rate = 30%).
Follow-up postalquestionnairedesign.
‘In-house’ self-administeredsurvey.
A postal survey;Edmonton ResearchOrientation Survey(EROS) (Pain et al1996); ResearchKnowledge, Attitudesand Practices ofResearch Survey(KAP Survey) (VanMullem et al 1999);Barriers to ResearchUtilization Scale(BARRIERS) (Funket al 1991).
Unpublished postalsurvey: adaptedfrom surveys byJette et al (2003)and Dysart andTomlin (2002).
A postal survey;EROS (Pain et al1996); KAP Survey(Van Mullem et al1999); BARRIERS(Funk et al 1991).
A postal survey;EROS (Pain et al1996); KAP Survey(Van Mullem et al1999); BARRIERS(Funk et al 1991).
Identify Swedishoccupational therapists’perceptions andattitudes of research-related activities, andengagement andplanned futureengagement withresearch.
Explore therapists’perceptions of EBP;identify demand forselected componentsconcerning EBP; andascertain preferredlearning strategies.
Investigate andcompare the perceivedknowledge, attitudes,practices, barriers, andorientation to EBP.
Examine occupationaltherapists’ attitudes,knowledge, andutilization of EBP.
Investigate the factorspredicting paediatricoccupationaltherapists’ attitudestowards EBP andresearch utilization.
Examine perceivedknowledge, attitudes,utilization, and barrierstowards EBP andresearch utilization.
Small differences were identified between thetwo surveys. Research was identified as importantto the development of the professional role andstatus. Reading research literature to updateknowledge identified as a priority, but applyingfindings to practice less so.
Therapists recognize a gap in their knowledgeand subsequent skills in utilizing publishedresearch. Staff need to improve skills pertainingto the appraisal and utilization of evidencewithin practice.
Occupational therapists were positive towardEBP but lacked confidence in their researchknowledge and practices. Differences betweencountries’ professionals were identified onratings of knowledge, practices, and attitudes.Although organizational factors were identifiedas key barriers to research utilization overall, UKand Taiwanese occupational therapists recordedorganization as the top barrier to EBP, whereasAustralian occupational therapists recordedcommunication as the greatest barrier.
Majority of respondents hold positive views ofEBP (96%); just over half of respondentsreported having learned about EBP during theireducation; very few therapists are using EBPwithin their clinical practice (12%); lack of timewas primary barrier.
Level of academic occupational therapyqualification was the most significant predictorof research utilization. Predictive factors towardsEBP included level of academic occupationaltherapy qualification and attitudes towardsestablishing current best practice.
Participants held positive views toward research,were willing to access new information andimplement findings into practice, but lackedconfidence in their research knowledge andpractices. Key barriers to utilization included:workplace/organizational factors, accessibility,and quality of research.
Strong
Average
Average
Strong
Strong
Average
by guest on November 4, 2015bjo.sagepub.comDownloaded from

30 British Journal of Occupational Therapy January 2014 77(1)
Occupational therapists’ attitudes, knowledge, and implementation of evidence-based practice: a systematic review of published research
Table 1 (continued)Reference Sample Design Purpose Results Quality ratingGilman2011
Heiwe et al2011
Lyons et al2011
Döpp et al2012
Hu et al2012
Lizarondoet al 2012
Recent graduatesfrom the PacificUniversity’s schoolof occupationaltherapy (n = 28).
Swedish UniversityHospital; dieticians(n = 41), occupa-tional therapists(n = 57),physiotherapists(n = 129).
Conveniencesample ofAustralianpaediatric occu-pational therapists(n = 138).
Random sampleof Dutch occupa-tional therapists(n = 100).
Conveniencesample of 64occupationaltherapists(response rate = 87.7%) in the UK.
Maximumvariation sampleof Australianoccupationaltherapists (n = 36), speechtherapists (n = 10),physiotherapists(n = 19), socialworkers (n = 15),and dietitians (n = 12).
Anonymous onlinesurvey; adaptedquestionnairedeveloped byPowell and Case-Smith (1991).
A cross-sectionalsurvey; translatedquestionnairedeveloped by Jetteet al (2003).
A postal survey;EROS (Pain et al1996); KAP Survey(Van Mullem et al1999); BARRIERS(Funk et al 1991).
Postal and online surveyquestionnaire.
Descriptive survey.
Pilot pre-post studydesign, using theEBPQ (Upton andUpton 2006b) andAdapted Fresnotest (McCluskeyand Bishop 2009).
Provide an understand-ing of recent PacificUniversity graduates’information-seekingbehaviours; contributeto the planning of theuniversity’s EBPcurriculum.
Explore dietitians’,occupationaltherapists’ andphysiotherapists’attitudes, beliefs,knowledge, andutilization of EBP.
Examine perceivedknowledge, attitudes,utilization, and barrierstowards EBP andresearch utilization.
Examine how Dutchoccupational therapistsperceive EBP, whatsources they rely on indecision making, andwhat barriers theyperceive whenimplementing EBP.
Explore the perception,involvement andparticipation of EBP ofoccupational therapistsin rural areas.
Explore the impact ofan iCAHE journal clubon practitioners’knowledge, attitudes,and use of EBP.
Barriers towards EBP included; limited searchskills, difficulty in accessing literature, and lack of available evidence.
All practitioners held overall positive attitudestowards EBP and its importance within clinicaldecision making; the majority of practitionersindicated having the skills and knowledgeneeded in interpreting and understandingresearch evidence; lack of time was perceived to be greatest barrier for all practitioners.
Therapists held overall positive attitudes towardsEBP and research utilization but indicated lack of knowledge and ability in performing researchactivities and engaging in conducting research.Therapists indicated moderate researchutilization. Article presentation and accessibilityof research were found to be greatest barriers to research utilization implementation.
Dutch therapists generally hold positive attitudestowards EBP; however, over half perceive it torequire too much effort (53%). Therapistsworking in academic hospitals held significantlymore positive attitudes (p < 0.01). Therapistsrelied on colleagues (79%) more often thanresearch evidence in clinical decision making.Most significant barrier was in evaluating thequality of research with 56.2% of therapistsperceiving research articles to be written in aninaccessible style.
No significant differences identified betweenrural and urban occupational therapists. Mostoccupational therapists held positive attitudestoward EBP, but owing to obstacles toimplementation low numbers had involvement in EBP related activities.
Occupational therapists demonstrated astatistically significant increase in EBPknowledge, but not attitude or self-reported use.Occupational therapists reported lowest levels ofEBP objective knowledge prior to theintervention, but no significant differences wereobserved on self-reported knowledge, attitudes,and use. Journal clubs may not be effectivemethods of enhancing EBP on their own, butcould be integrated with other strategies.
Average
Strong
Strong
Strong
Average
Good
by guest on November 4, 2015bjo.sagepub.comDownloaded from

31British Journal of Occupational Therapy January 2014 77(1)
Dominic Upton, Danielle Stephens, Briony Williams, and Laura Scurlock-Evans
Table 2. Study characteristics and findings of qualitative reportsReference Sample Design Purpose Results Quality ratingMcQueenet al 2006
Reagon et al 2008
Copley andAllen 2009
Fänge andIvanoff2009
Vachon et al 2010
Kristensenet al 2011
Conveniencesample of 7 UKNHS occupationaltherapists.
Purposive samplingof occupationaltherapists workingin the NHS andSocial Servicesdepartments (n = 21). Membersof staff observed(n = 90).
Australianoccupationaltherapists withina university-basedpaediatric clinic(n = 9).
Whole populationsample of Swedishlocal healthauthority occu-pational therapists(n = 15, responserate = 83%).
Purposive sampleof 8 Canadianoccupationaltherapists whohad attended a 4-day EBPworkshop.
Purposive sampleof 25 Danishoccupationaltherapists,working in threeclinical (strokerehabilitation)settings.Participants wereonly selected ifthey had morethan 2 years’clinicalexperience.
Pre-post studyanalysedqualitativelyusing contentanalysis.
Case studydesign; focusgroups, in-depthinterviews, andobservation.
Action Researchdesign; focusgroups.
Three focusgroup interviews(five differentoccupationaltherapists ineach).
Collaborativeresearchmethodologyover a period of 15 months,analysed usinggroundedtheory.
Phenomenologicalhermeneuticalresearchapproachincluding:participantobservation,focus groupdiscussions, and individualinterviews over20 months.AnalysedfollowingRicoeur’s (1976)approach.
To explore the impact of ajournal club on EBPbehaviours and attitudes.
Aims to uncover themeanings occupationaltherapists attribute to EBP.
To explore occupationaltherapists’ perception ofEBP and its utilization; toidentify strategies andresources that canincrease EBP utilization.
Identify and analyse theexperiences of Swedishoccupational therapists ofparticipation in andimplementation ofresearch.
Explore the clinicaldecisions makingprocesses used anddescribe the empowermentprocess they developed tobecome evidence-basedpractitioners.
Investigate facilitation ofevidence-based practice instroke rehabilitation(specifically in relation to five evidence-basedclinical guidelines), over aperiod of 20 months.
Participants’ responses following participation inthe journal club indicated greater awareness of EBP.
Four emerging themes including: perceptions ofEBP, functions of EBP, client-centred occupationaltherapy, and EBP. Tensions were discovered betweenconcepts of EBP and traditional client-centredness.
Therapists strongly support and accept the broaddefinition of EBP within their clinical practice.Therapists identified: that they used bothresearch-based and practice-based evidence toinform their clinical practice; the occupationalresearch base as being limited; a key limitationbeing the way research-evidence is generated(randomized controlled trials, etc.), which maynot be applicable to everyday clinical contexts.
One core category (feeling professionallycompetent) emerged from analysis, comprisingthree subcategories: perceiving congruencebetween research and practice, having thenecessary skills, and making a contribution.Engaging with research was seen to bring bothprofessional and personal gains.
Six different modes of decision making (whichaffected evidence utilization) were identified:defensive, repressed, cautious, autonomous,intuitive, and autonomous thoughtful. Reflectivelearning facilitated evidence utilization through astaged empowerment process: deliberateness,client-centredness, and system mindedness.
Learning processes became part of developingprofessional identities and resulted in greaterconfidence. ‘Facilitators’ (individuals in charge ofthe learning process) were identified asimportant to the change process. Being able tosee the purpose of integrating research evidenceinto practice was important to participants.Working in isolation was a barrier toimplementing standardized practice. Participationin the research process was identified asimportant, and having a critical attitude toclinical guidelines was seen as necessary whenadapting them to specific contexts. Moreexperienced therapists appeared to be able towork more flexibly through the process.
Poor
Average
Average
Average
Strong
Average
by guest on November 4, 2015bjo.sagepub.comDownloaded from

32 British Journal of Occupational Therapy January 2014 77(1)
Occupational therapists’ attitudes, knowledge, and implementation of evidence-based practice: a systematic review of published research
positive attitudes towards the use of EBP when comparedwith more experienced therapists (Bennett et al 2003, Dysartand Tomlin 2002, McCluskey 2003, Sweetland and Craik2001), and the number of jobs held since qualification wasassociated with a decrease in active research. However,Kristensen et al (2011) found that more experienced Danishoccupational therapists were able to work more flexiblythrough the process of EBP.
Research-based practice and traditionalmethodsTherapists may value different forms of evidence to those typ-ically placed at the top of the evidence pyramid (for example,systematic reviews of randomized control trials); a numberof studies identified colleagues (Döpp et al 2012, Dysart andTomlin 2000, Sweetland and Craik 2001) and personal clin-ical experience (Bennett et al 2003, Copley and Allen 2009,Sweetland and Craik 2001) as important in decision making.
Copley and Allen (2009) identified two differentiatedsources of evidence by which therapists make clinicaldecisions: evidence-based practice, and professional, practice-based knowledge. Although participants agreed upon theimportance of EBP and its significance within clinical care,
they found the restrictions of research in relation to sampleand interventions made findings inapplicable to practice.Consequently, therapists suggested a need to also take intoaccount their own clinical experience and evaluations ofcase-by-case outcomes. Similarly, Reagon et al (2008) foundthat occupational therapists, despite regarding EBP with someambivalence, associated EBP with some positive outcomes interms of demonstrating effectiveness of interventions, inform-ing knowledge gaps, and providing a cost-effective provisionof care. However, the therapists indicated the importance ofclient-centeredness within care and the tension often apparentbetween this and EBP. Hence, as the previous study illus-trated, the therapists believed EBP to be inadequate on itsown in relation to individual client care, suggesting theneed to incorporate multiple sources of evidence.
Therapists raised concerns regarding the relevance andapplicability of research evidence to clinical practice prob-lems (Copley and Allen 2009, Döpp et al 2012, Fänge andIvanoff 2009, Gilman 2011, Pollock et al 2000, Reagon et al2008, Sweetland and Craik 2001), with some questioningthe appropriateness of applying sterile ‘scientific evidence’(Reagon et al 2008) to ‘authentic practice’ (Copley and Allen2009). Hence, it would seem that there continues to be a
Table 2 (continued)Reference Sample Design Purpose Results Quality ratingBayley et al2012
SwedloveandEtcheverry2012
Conveniencesample ofCanadian occu-pational therapists(n = 23), nurses(n = 17), physicaltherapists (n = 23)and hospitalmanagers/directors(n = 16).
Conveniencesample of 10Canadian occu-pational therapistsfrom a largehealthcare facility.
Focus groups heldwithin 2–4 weeksof completion of a 6-monthimplementationproject. Focusgroups involved3–6 professionalsworking in thesame field.
Qualitative,exploratoryresearchinvolvinginterviews.
To describe barriers toimplementation ofevidence-basedrecommendations instroke rehabilitation.
Exploring perceptions ofthe value of research andfactors influencing theseperceptions.
Occupational therapists most frequently identifiedlack of time, team functioning and communication,patient/provider safety, and prioritizingtreatments as barriers to implementation ofevidence-based recommendations.
Participants valued research for informing practice,underpinning the profession, providing credibility,and economic justification for decisions. Perceptionswere influenced by experiences with research,resources, and practice culture.
Average
Average
Table 3. Study characteristics and findings of mixed methods reportsReference Sample Design Purpose Results Quality ratingCurtin andJaramazovi2001
Purposive sampleof UK senioroccupationaltherapists (n = 27).Conveniencesample of 653occupationaltherapists(response rate = 76.5%).
Mixed methods:interviewsfollowed byquestionnaires.
Explore the views andperceptions ofoccupational therapistsworking in Englandregarding EBP.
Occupational therapists held positive attitudestoward EBP, but identified lack of time, high staffturnover, and staff shortages as importantbarriers to implementation. Facilitators of EBPincluded: support from colleagues, personalmotivation, and access to resources.
Quantitative:average.Qualitative:average.Overall:average.
by guest on November 4, 2015bjo.sagepub.comDownloaded from

33British Journal of Occupational Therapy January 2014 77(1)
Dominic Upton, Danielle Stephens, Briony Williams, and Laura Scurlock-Evans
significant gap between the research base and its relevanceto interventions used on a daily basis and the clients treatedwithin actual clinical settings. However, participants inReagon et al’s (2008) study did agree that EBP is impor-tant within clinical practice, although in conjunction withclinical reasoning.
Perceiving congruence between research and practice(Fänge and Ivanoff 2009) and being able to see the purposeof integrating research evidence into practice (Kristensenet al 2011) have also been identified as important to prac-titioners, highlighting the need for clinically applicableresearch findings.
Education and knowledge surrounding EBPA large proportion of the research indicated some limits topractitioners’ EBP knowledge and skills. For instance, Döppet al (2012) discovered that Dutch occupational therapistsperceived their critical research appraisal skills to be lack-ing significantly, expressed difficulty with understandingstatistical analyses, and felt articles were written in aninaccessible style. Similar findings were identified by Dysartand Tomlin (2002), Lyons et al (2010), and Pollock et al(2000). Comparing the practices of different health profes-sionals, Upton and Upton (2006b) discovered that occupa-tional therapists reported equivalent knowledge of EBP tophysiotherapists, dieticians, speech and language therapists,and psychologists, and greater knowledge than podiatrists,radiographers, and orthoptists. However, the majority ofoccupational therapists (41%) still rated their knowledgeas low; furthermore, they rated their awareness of informa-tion sources as lower than most other allied health profes-sionals, and preferred evidence provided by colleagues.
Lacking confidence in research and knowledge processeswas a common theme in the literature (for example, Bennettet al 2003, Brown et al 2009, Lyons et al 2010). McCluskey(2003) found that therapists rated their ability as low inrelation to generating clinical questions, critical appraisalskills, and conducting literature searches, but that theyreported being confident in evaluating their own clinicalpractice, and their ability to change their practice based onnew evidence. Similarly, Caldwell et al (2007) discoveredthat just under two-thirds of their therapists reported beingconfident about their skills and knowledge. However,Heiwe et al (2011) and Salls et al (2009) found that over70% of their samples reported confidence in critically apprais-ing research and literature searching skills. Furthermore,Bennett et al (2003) discovered that their respondentsreported being most confident in literature searchingskills, although they were less confident in determiningclinical significance, study design, validity and usingspecific electronic databases. These results may be con-founded by level of academic preparation, as the relativelyhigh level of both Heiwe et al (2011) and Salls et al’s(2009) samples reported receiving formal EBP-associatedtraining and Bennett et al (2003) discovered that therapistsholding higher qualifications were found to be more con-fident in their EBP skills. In addition, Salls et al (2009)
identified that therapists who had been practicing for lessthan 5 years were more likely to report receiving EBPeducation during their academic preparation than thosewho had been practicing longer, potentially explainingdifferences in attitudes toward EBP observed betweenrecent graduates and more experienced professionals.
Studies revealed that therapists desired to improve theirknowledge and skills surrounding EBP (Brown et al 2010,Salls et al 2009) and in the use of an online evidenceretrieval system (Gosling et al 2004) in order improve theirimplementation of EBP within their everyday clinicalpractice. McCluskey (2003) also considered continuedEBP education, and discovered that a small proportion ofrespondents had attended EBP workshops, suggesting adesire to engage in continuing professional development.
Learning about EBP and associated skills has beenassociated with a number of benefits, including devel-oping professional identities and fostering confidence(Kristensen et al 2011). Furthermore, reflective learningwas found to facilitate RU through a staged empowermentprocess (Vachon et al 2010).
Two studies explored the impact of participation in ajournal club on EBP behaviours and attitudes; although whileMcQueen et al (2006) found participants demonstratedgreater awareness of EBP post-journal club, Lizarondo et al (2012) found that while occupational therapists’knowledge increased, they had not changed their attitudesor practice following participation. The researchers sug-gested that journal clubs may need to be integrated withother intervention strategies in order to be effective inenhancing EBP uptake.
Despite the benefits and interest in EBP, the timeconstraints associated with the occupational therapy rolemean that many practitioners are unable to attend EBPtraining sessions (McCluskey 2003). Welch and Dawson(2007) noted these time constraints in their study anddiscovered that, with regard to continual learning, therapistspreferred practice-based interactive strategies deliveredthrough ‘in-house’ forums, suggesting that such strategieswould bridge the knowledge gap while negating the timeconstraints associated with therapists’ workload.
Finally, issues surrounding a lack of perceived knowledgeand research skills also seem to be apparent when consid-ering therapists’ engagement with conducting research(Lyons et al 2011), suggesting a possible reason for thelack of practitioner involvement in research.
Implementation of EBPThe studies revealed consistent results in relation to a lackof utilization of EBP within occupational therapists’clinical practice. For example, Salls et al (2009) discoveredthat a meagre 12% of surveyed occupational therapistsreported frequent utilization of EBP. Lyons et al (2011)discovered that although therapists reported some imple-mentation of research, there was significant room forimprovement in terms of degree of implementation withineveryday clinical practice.
by guest on November 4, 2015bjo.sagepub.comDownloaded from

34 British Journal of Occupational Therapy January 2014 77(1)
Occupational therapists’ attitudes, knowledge, and implementation of evidence-based practice: a systematic review of published research
Worryingly, one of the most recent studies, conducted byDöpp et al (2012), indicated that despite positive attitudestowards EBP, therapists continually relied on colleagues asa source of clinical decision making, replicating the earlierfindings of Sweetland and Craik (2012). Of further concernwas the finding that 82.8% of therapists relied upon infor-mation from non-occupational therapists on a weekly basis.The authors indicated that journal articles and databaseswere the least frequently used sources of information.
Heiwe et al (2011) explored EBP implementation bydieticians, physiotherapists, and occupational therapistsand found a significant difference in RU between them:specifically, occupational therapists read and criticallyappraised significantly fewer articles. Similarly, Gosling et al (2004) considered the utilization of an online EBPresource and noted that although 86% of occupationaltherapists were aware of an online evidence resource, only79% of these individuals actually used it. The authors alsoindicated that compared to physiotherapists, occupationaltherapists used the resource less often, although this mayhave been confounded by differences in level of access tocomputers in patient-care areas. However, research byLizarondo et al (2012) revealed no significant differencesin the level of EBP use between occupational therapists,physiotherapists, dieticians, social workers, or speechpathologists prior to a journal club intervention.
Research also indicated differences in EBP utilizationin relation to level of academic attainment. For instance,Cameron et al (2005) discovered that the higher the thera-pist’s degree, the lower the EBP utilization. Surprisingly,the findings illustrated that occupational therapists with anundergraduate degree tended to rely on the research processmore than those with Master’s level qualifications, despitethe latter’s focus on research methodology. Additionally, itwas found that as the therapists’ years of clinical experienceincreased, the extent to which they implemented researchdecreased; this was a finding often found in relation toEBP utilization (McCluskey 2003).
Perceived limits and barriers to EBPimplementationThere was a general consensus across the studies regard-ing the dominant EBP barriers perceived by therapists. Asignificant barrier related to the accessibility of researchevidence in terms of accessing databases and the presen-tation of research articles (Bennett et al 2003, Dysart andTomlin 2002, Heiwe et al 2011, Lyons et al 2010, Lyons2011, Kristensen et al 2011, Salls et al 2009, Sweetlandand Craik 2001). Such communication barriers have beenevident across allied health professions (Metcalfe et al2001); however, it may be that occupational therapistsperceive the barriers to be of greater detriment towardsEBP implementation (Lyons et al 2011). Lack of time wasalso considered a significant barrier (Bayley et al 2012,Bennett et al 2003, Caldwell et al 2007, Copley and Allen2009, Dysart and Tomlin 2002, Heiwe at al 2011, Humphriset al 2000, Reagon et al 2008, Salls et al 2009, Sweetland
and Craik 2001, Upton and Upton 2006b), even in relationto the utilization of an online EBP resource designed toovercome this obstacle (McKenna et al 2005).
In addition, numerous studies reported that occupationaltherapists perceived the evidence base to be limited (Bennettet al 2003, Lyons et al 2011, McCluskey 2003), resultingin a lack of support in the implementation of appropriateinterventions. Furthermore, Pollock et al (2000) indicatedthat therapists had great difficulty in transferring the researchevidence into their clinical practice.
Table 4. Barriers to implementation of EBP and RU acrossquantitative and qualitative studies
Key barriers to EBP Studies identifiedWorkload pressures Curtin and Jaramazovi (2001), Humphris et al
(2000), McCluskey (2003).
Time pressures Bayley et al (2012), Bennett et al (2003), Dysart and Tomlin (2002), Heiwe et al (2011), Humphris et al (2000), Kristensen et al (2011),Lyons et al (2011), McCluskey (2003), McKennaet al (2005), Salls et al (2009), Sweetland and Craik (2001), Upton and Upton (2006b).
Insufficient staff/ Curtin and Jaramazovi (2001), Dysart andresources/finances Tomlin (2002), Humphris et al (2000), Upton
and Upton (2006b).
Lack of training/ Pollock et al (2000), Gosling and Westbrookknowledge (2004), Lyons et al (2011), Sweetland and
Craik (2001).
Lack of skills Döpp et al (2012), Dysart and Tomlin (2002), Fänge and Ivanoff (2009), Gilman (2011), Gosling and Westbrook (2004), Lyons et al (2011), Pollock et al (2000), Welch andDawson (2007).
Lack of support, Brown et al (2009), Cameron et al (2005), organizational Curtin and Jaramazovi (2001), Gosling andbarriers Westbrook (2004), Kristensen et al (2011),
Pollock et al (2000), Salls et al 2009, Lyons et al (2010), Sweetland and Craik (2001).
Relevance, applicability, Bennett et al (2003), Copley and Allen (2009),availability, quality of Döpp et al (2012), Dysart and Tomlin (2002), research evidence Fänge and Ivanoff (2009), Gosling and
Westbrook (2004), Gilman (2011), Lyons et al (2010), Lyons et al (2011), McCluskey 2003, Pollock et al (2000), Sweetland and Craik (2001).
Communication and Bayley et al (2012), Brown et al (2009). team functioning
Requiring too much Curtin and Jaramazovi (2001), Döpp et al (2012).effort or personalmotivation
Conflict with client- Reagon et al (2008).centred practice
Patient /provider safety Bayley et al (2012).and prioritizing treatments
by guest on November 4, 2015bjo.sagepub.comDownloaded from

35British Journal of Occupational Therapy January 2014 77(1)
Dominic Upton, Danielle Stephens, Briony Williams, and Laura Scurlock-Evans
A number of studies illustrated a perceived lack of demandand support for EBP from their reimbursement agencies oradministrators (Cameron et al 2005, Salls et al 2009), withGosling et al (2004) finding that occupational therapistsreported low levels of support in implementing an onlineEBP resource. Also, Pollock et al (2000) found that despite92% of their respondents perceiving EBP as highly importantwithin their practice, only 58% agreed that their departmentheld EBP as a priority. Finally, both Bayley et al (2012) andBrown et al (2009) discovered that the greatest perceivedbarriers toward EBP implementation were associated withorganizational factors. These findings are problematicwhen considered in the light of research suggesting thatperceived support from management and work colleaguesare associated with increased capability in, and utilization of,EBP (Döpp et al 2012, Sweetland and Craik 2001).
DiscussionLimitations of the reviewNarrative literature reviews are at risk of confirmation bias(Baumeister and Leary 1997). However, the adoption of asystematic review methodology (that is, systematic searchstrategy, quality appraisal, and data extraction procedures)and use of independent raters helped to mitigate this issue.
The review included only papers that had been publishedin peer-reviewed journals: although this ensured that allresearch had been through the rigour of the peer-reviewprocess, it introduced the potential for publication bias.Furthermore, only articles written in English were includedin the review, which may have led to the exclusion of otherrelevant research.
Strengths and limitations of the researchreviewedQuality assessment of the studies revealed that the majoritywere rated as either average or good, indicating that manystudies fulfilled at least 34% of quality criteria accordingto McMaster University’s guidelines. This suggests thatresearch is of a reasonable quality, but there is substantialroom for improvement.
A range of issues were identified as contributing to the‘average’ or ‘poor’ classifications, including issues in relationto the sampling methods employed in quantitative research.Specifically, a substantial proportion of studies recruitedrelatively small samples. Research surrounding practitioners’EBP utilization often reported significant time constraints onthe part of clinical practitioners (Metcalfe et al 2001), whichmay explain difficulties in recruitment. Furthermore, manystudies used convenience /opportunistic sampling; thispotentially limited the representativeness and generalizabilityof research findings.
All of the quantitative studies collected data via self-administered postal or online survey questionnaires. Althoughthese methods may be the most feasible means of collectingdata from occupational therapists (given their time constraints),
it has been argued that the use of self-report measures withinresearch can be highly problematic (Gawronski 2009). Forinstance, self-report measures have the tendency to be limitedin relation to introspection and are at risk of self-presentationbias and social desirability effects (Fisher 1993, Gawronski2009). None of the quantitative studies included a measureof socially desirable responding in order to mitigate this.
Additionally, although some studies adopted current ormodified published questionnaires, others relied upon thedevelopment of their own ‘in-house’ surveys (Welch andDawson 2007). Most of these surveys underwent pilotingin order to ensure construct validity, but many were lackingrigorous statistical measures in determining their reliabilityin measuring what they intended. Thus, the studies’ method-ological quality is undermined.
The qualitative studies reviewed adopted a range of datacollection methods, including focus groups, interviews, andobservation. Although many articles specified the approachadopted (for example, participatory action research), thiswas not always clear. Furthermore, although qualitativeresearch methodology is believed to reduce the risk of self-presentation bias (Gawronski 2009), issues surroundingresearch bias need to be considered in order to determinethe neutrality of research findings. Although some studiesdescribed decision trails, methods of triangulation, andpotential sources of researcher bias, this aspect was notalways specified clearly, making it difficult to ascertain thelevel of rigour in some studies.
Based upon discussion of these issues, generalizations andconclusions from this review’s synthesis should be tentative.However, despite this, a number of important implicationsthat may help to inform future practice and research doarise from the review’s findings.
Implications for practice, policy and researchThe research synthesis indicates that attitudes and practicemay be linked, but the relationship is not causal. Therefore,interventions should not focus heavily on this aspect inorder to enhance uptake of EBP. However, discrepanciesbetween attitudes toward and practice of EBP may be evidenceof socially desirable responding; future research should,therefore, aim to include a measure of social desirability tountangle this relationship.
Occupational therapists’ motivation to implement EBPwas both directly and indirectly identified as an importantfactor in EBP implementation by the research reviewed andmay represent a link between EBP attitudes and behaviour.Further research is required to explore methods of enhanc-ing individual and organizational motivation to implementEBP. In particular, identifying ways of making EBP personallyrelevant to practitioners (that is, how it benefits them andtheir clients directly) may help therapists to understand whyit is a beneficial framework to adopt.
Despite positive attitudes toward research, very few clin-icians were actively involved in research; for many, this maybe the result of workload and time pressures. Greater collab-orative working by practitioners with local higher education
by guest on November 4, 2015bjo.sagepub.comDownloaded from

36 British Journal of Occupational Therapy January 2014 77(1)
Occupational therapists’ attitudes, knowledge, and implementation of evidence-based practice: a systematic review of published research
(HE) institutions may be a means to both develop skills andensure research is grounded in clinically relevant terms.
Working in isolation and lack of support were identi-fied as important barriers to EBP. There is, therefore, a needto identify cost effective and time efficient interventions andsupport networks (which could have longevity). Journalclubs and the use of social media may provide mechanismsto produce research communities that allow research, bestpractice, and skills to be shared and disseminated, butthese must be embedded within an organizational culturethat promotes EBP and integrates it with other traininginitiatives. Developing dedicated staff roles, such as knowl-edge brokers, to help facilitate dissemination of up-to-dateresearch findings may promote EBP whilst addressing thetime-demands placed on many occupational therapists.
Although there are resource-demands that must beconsidered, mentoring may be another means of utilizingthe skills within a workforce (for instance, technologyskills of recent graduates and flexibility of experiencedtherapists), in a cost-effective manner. Mentoring furtherhighlights the need for assessment of training needs priorto any EBP intervention; some research reviewed indicatedthat the needs of experienced staff might differ from thoseof newly-qualified practitioners. Being aware of where thestrengths and needs of professionals lie will also help toensure that these individuals are being used to theirgreatest advantage. Ultimately, this may provide the oppor-tunity for professional enhancement for both the menteeand mentor in terms of career development.
Many participants identified the inaccessibility of researchas a barrier to implementing EBP: promoting open accessresources, whilst being mindful of the cost implications of this, may be an important goal in occupational therapyin future research. Furthermore, appropriate use of profes-sional alongside peer-reviewed publications may disseminateresearch to a wider audience. A preference for acquiringevidence from colleagues also suggests that knowledgebrokers may, for example, be an efficient means of dissemi-nating research.
Finally, the research reviewed indicated that many occu-pational therapists rely on personal clinical experience,which was viewed negatively by some authors. However,personal experience is not in itself incompatible with theoriginal conceptualisation of EBP (Taylor and Savin-Baden2001). Further research is therefore required to understandwhat occupational therapists mean and understand by theterm and how this could be used to increase the utility ofthe EBP approach within the field.
ConclusionThe results from all of the studies indicated that occupa-tional therapists tend to hold positive views towards EBP,its importance in clinical decision making and in providingthe most appropriate care for their patients. Despite this,occupational therapists implement EBP infrequently within
their day-to-day practice. This lack of RU was perceived tobe due to significant barriers within the therapists’ organi-zational structures, their current work load and subsequenttime constraints. Furthermore, many therapists’ perceivedthemselves to have a lack of knowledge with regards tocritically appraising research evidence, whilst perceivingarticles too inaccessible and difficult to translate into practice.Qualitative research demonstrated a perceived tensionbetween EBP and traditional client-centred approaches.Therefore, although many therapists realized the importanceand value of EBP, a substantial proportion of participantsvoiced concerns, or negative perceptions, of EBP. Thishighlights the need for good quality education for futureoccupational therapists, access to continual professionaldevelopment programmes, and organizational support forqualified practitioners. Combined, this may help the principlesof EBP to be implemented effectively within therapists’daily practice in a way which benefits both clients and theprofession as a whole.
Key findings� Despite occupational therapists holding generally positive attitudestoward EBP, a substantial proportion view EBP negatively.
� Occupational therapists have raised concerns about the relevanceand applicability of research evidence to clinical problems.
� Factors identified as barriers to EBP implementation and RU include:workload and time pressures, lack of training/knowledge/skills/personalmotivation, tension between EBP and traditional approaches, andorganisational barriers.
What the study has addedThis review of both quantitative and qualitative research has identifieda number of areas which could form the basis of interventions to encouragethe uptake, quality, and consistency of EBP implementation. Such areasinclude: making EBP personally relevant to practitioners, developing socialnetworks to support practitioners with EBP, mentoring, and encouragingpractitioner involvement in research through collaborative working withHE institutions.
Conflict of interest: None declared.Funding: This review received no specific grant support from any fundingagency in the public, commercial, or not-for-profit sectors.Research ethics: Ethics approval was not required for this review.
ReferencesAlexandratos K, Barnet F, Thomas Y (2012) The impact of exercise on the mental
health and quality of life of people with severe mental illness: a criticalreview. British Journal of Occupational Therapy, 75(2), 48–60.
American Occupational Therapy Association (2007) AOTA Centennial vision andexecutive summary. American Journal of Occupational Therapy, 61(6), 613–614.
Baumeister R, Leary M (1997) Writing narrative literature reviews. Review ofGeneral Psychology, 1(3), 311–320.
Bayley M, Hurdowar A, Richards C, Korner-Bitensky N, Wood-Daphinee S,Eng J … Graham I (2012) Barriers to implementation of stroke rehabilitationevidence: findings from a multi-site pilot project. Disability & Rehabilitation,34(19), 1633–1638.
by guest on November 4, 2015bjo.sagepub.comDownloaded from

37British Journal of Occupational Therapy January 2014 77(1)
Dominic Upton, Danielle Stephens, Briony Williams, and Laura Scurlock-Evans
Bennett S, Bennett JW (2000) The process of evidence-based practice inoccupational therapy: informing clinical decisions. Australian OccupationalTherapy Journal, 47(4), 171–180.
Bennett S, Tooth L, McKenna K, Rodger S, Strong J, Ziviani J, Mickan S, Gibson L(2003) Perception of evidence-based practice: a survey of Australianoccupational therapists. Australian Occupational Therapy Journal, 50(1),13–22.
Brown T, Tseng MH, Casey J, McDonald R, Lyons C (2009) Knowledge, attitudes,practice and barriers of pediatric occupational therapists to evidence-based practice and research utilization. WFOT Bulletin, 60, 38–48.
Brown T, Tseng HM, Casey J, McDonald R, Lyons C (2010) Predictors of researchutilization among pediatric occupational therapists. Occupation, Participationand Health, 30(4), 172–183.
Caldwell E, Whitehead M, Fleming J, Moes L (2008) Evidence-based practicein everyday clinical practice: strategies for change in a tertiary occupationaltherapy department. Australian Occupational Therapy Journal, 55(2),79–84.
Caldwell K, Coleman K, Copp G, Bell L, Ghazi F (2007) Preparing for professionalpractice: how well does professional training equip health and socialcare practitioners to engage in evidence-based practice? Nurse EducationToday, 27(6), 518–528.
Cameron KA, Ballantyne S, Kulbitsky A, Margolis-Gal M, Daugherty T, Ludwig F(2005) utilization of evidence based practice by registered occupationaltherapists. Occupational Therapy International, 12(3), 123–136.
College of Occupational Therapists (2003) Occupational Therapy ClinicalGuidelines for Rheumatology. Available at: https://www.cot.co.uk/sites/default/files/publications/public/Rheumatology0_0.pdf Accessed16.03.12.
Copley J, Allen S (2009) Using all the available evidence: perceptions of paediatricoccupational therapists about how to increase evidence-based practice.International Journal of Evidence Based Healthcare, 7(3), 193–200.
Crist P (2010) Adapting research instruction to support scholarship of practice:practice-scholar partnerships. Occupational Therapy in Healthcare, 24(1),39–55.
Curtin M, Jaramazovic E (2001) Occupational therapists’ views and perceptionsof evidence-based practice. British Journal of Occupational Therapy, 64(5),214–222.
Döpp CM, Steultjens EM, Radal J (2012) A survey of evidence-based practiseamong Dutch occupational therapists. Occupational Therapy International,19(1), 17–27.
Dysart A, Tomlin G (2002) Factors related to evidence-based practice amongUS occupational therapy clinicians. American Journal of OccupationalTherapy, 56(3), 275–284.
Fänge A, Ivanoff S (2009) Integrating research into practice: a challenge forlocal authority occupational therapy. Scandinavian Journal of OccupationalTherapy, 16(1), 40–48.
Fisher R (1993) Social desirability bias and the validity of indirect questioning.Journal of Consumer Research, 20(2), 303–315.
Gawronski B (2009) Ten frequently asked question about implicit measuresand their frequently supposed, but not entirely correct answers. CanadianPsychology, 50(3), 141–150.
Gilman PI (2011) Evidence-based information-seeking behaviours of occupationaltherapists: a survey of recent graduates. Journal of the Medical LibraryAssociation, 99(4), 307–310.
Gosling S, Westbrook J (2004) Allied health professionals’ use of online evidence:a survey of 790 staff working in the Australian public hospital system.International Journal of Medical Informatics, 73(4), 391–401.
Green NB, Johnson DC, Adams A (2006) Writing narrative literature reviewsfor peer-reviewed journals: secrets of the trade. Journal of ChiropracticMedicine 5(3), 101–117.
Heiwe S, Kajermo NK, Tyni-Lenne R, Guidetti S, Samuelsson M, Andersson I,Wengstrom Y (2011) Evidence-based practice: attitudes, knowledgeand behaviour among allied health care professionals. InternationalJournal for Quality in Health Care, 23(2), 198–209.
Hu D, Burke J, Aliki T (2012) Occupational therapists’ involvement views,and training needs of evidence-based practice: a rural perspective.International Journal of Therapy & Rehabilitation, 19(11), 618–628.
Humphris D, Littlejohns P, Victor C, O’Halloran P, Peacock J (2000) Implementingevidence-based practice: factors that influence the use of research evidenceby occupational therapists. British Journal of Occupational Therapy, 63(11),516–522.
Karlsson U, Törnquist K (2007) What do Swedish occupational therapists feelabout research? A survey of perceptions, attitudes, intentions and engagement.Scandinavian Journal of Occupational Therapy, 14(4), 221–229.
Kristensen H, Tove B, Lise H (2011) Facilitation of research-based evidencewithin occupational therapy in stroke rehabilitation. British Journal ofOccupational Therapy, 74(10), 473–483.
Law M, Stewart D, Pollock N, Letts L, Bosch J, Westmorland M (1998)Guidelines for Critical Review Form: Quantitative Studies. Available at:http://www.srs-mcmaster.ca/Portals/20/pdf/ebp/quanguidelines.pdf
Accessed 16.04.13.Letts L, Wilkins S, Law M, Stewart D, Bosch J, Westmorland M (2007)
Guidelines for critical review form: qualitative studies. Available at:http://www.srs-mcmaster.ca/Portals/20/pdf/.../qualguidelines_version
2.0.pdf Accessed 26.03.13.Lizarondo L, Grimmer-Somers K, Kumar S, Crockett A (2012) Does journal club
membership improve research evidence uptake in different allied healthdisciplines: a pre-post study. BMC Res Notes, 5, 588: Available at:http://www.biomedcentral.com/1756-0500/5/58/ Accessed 26.03.13.
Lyons C, Casey J, Brown T, Tseng Mei, McDonald R (2010) Research knowl-edge, attitudes, practices and barriers among paediatric occupationaltherapists in the UK. British Journal of Occupational Therapy, 73(5),200–209.
Lyons C, Brown T, Tseng HM, Casey J, McDonald R (2011) Evidence-basedpractice and research utilization: perceived research knowledge, attitudes,practices and barriers among Australian paediatric occupational therapists.Australian Occupational Therapy Journal, 58(3), 178–186.
McCluskey A (2003) Occupational therapists report low level of knowledge,skill and involvement in evidence-based practice. Australian OccupationalTherapy Journal, 50(1), 3–12.
McKenna K, Bennet S, Dierselhuis Z, Hoffmann T, Tooth L, McCluskey A (2005)Australian occupational therapists’ use of an online evidence-based practicedatabase (OTseeker). Health Information and Libraries Journal, 22(3),205–214.
McQueen J, Miller C, Nivison C, Husband V (2006) An investigation into theuse of a journal club for evidence-based practice. International Journalof Therapy and Rehabilitation, 13(7), 311–317.
Melnyk B, Fineout-Overholt E, Fischbeck Feinstein N, Li H, Small L, Wilcox L,Kraus R (2004) Nurses’ perceived knowledge, beliefs, skills, and needsregarding evidence-based practice: implications for accelerating theparadigm shift. Worldviews on Evidence Based Nursing, 1(3), 185–93.
Melnyk B, Fineout-Overholt E, Stillwell S, Williamson K (2010) Evidence-basedpractice: step by step: the seven steps of evidence-based practice. AmericanJournal of Nursing, 110(1), 51–53.
by guest on November 4, 2015bjo.sagepub.comDownloaded from

38 British Journal of Occupational Therapy January 2014 77(1)
Occupational therapists’ attitudes, knowledge, and implementation of evidence-based practice: a systematic review of published research
Metcalfe C, Lewin R, Wisher S, Perry S, Bannigan K, Moffett J (2001) Barriersto implementing the evidence base in four NHS therapies: dietitians,occupational therapists, physiotherapists, speech and language therapists.Physiotherapy, 87(8), 433–441.
Moher D, Liberati A, Tetzlaff J, Altman GD, The PRISMA Group (2009) Preferredreporting items for systematic reviews and meta-analyses: the PRISMAstatement. PLoS Medicine, 6(7), e1000097. doi:10.1371/journal.pmed.1000097.
Oliver A, McDaid D (2002) Evidence-based health care: benefits and barriers.Social Policy and Society, 1(3), 183–190.
Pollock SA, Legg L, Langhorne P, Sellars C (2000) Barriers to achieving evidence-based stroke rehabilitation. Clinical Rehabilitation, 14(6), 611–617.
Prior P, Wilkinson J, Neville S (2010) Practice Nurse use of evidence in clinicalpractice: a descriptive survey. Nursing Praxis in New Zealand, 26(2),14–25.
Reagon C, Bellin W, Boniface G (2008) Reconfiguring evidence-basedpractice for occupational therapists. International Journal of Therapy andRehabilitation, 15(10), 428–436.
Salls J, Dolhi C, Silverman L, Hansen M (2009) The use of evidence-basedpractice by occupational therapists. Occupational Therapy in Health Care,23(2), 134–145.
Stergiou-Kita M (2010) Implementing clinical practice guidelines in occupationaltherapy practice: recommendations form the research evidence. AustralianOccupational Therapy Journal, 57(2), 76–87.
Straus SE, Richardson WS, Glasziou P, Haynes RB (2011) Evidence-basedmedicine: how to practice and teach EBM (4th ed). Edinburgh, Scotland:Churchill Livingstone.
Swedlove F, Etcheverry E (2012) Occupational therapists’ perceptions of the valueof research. New Zealand Journal of Occupational Therapy, 59(1), 5–12.
Sweetland J, Craik C (2001) The use of evidence-based practice by occupationaltherapists who treat adult stroke patients. British Journal of OccupationalTherapy, 64(5), 256–260.
Taylor CM (2007) Evidence-based practice for occupational therapists (2nd ed).Oxford: Wiley-Blackwell.
Taylor CM, Savin-Baden M (2001) Whose ‘evidence’ are we applying? BritishJournal of Occupational Therapy, 64(5), 213.
Upton D, Upton P (2006a) Knowledge and use of evidence-based practiceof GPs and hospital doctors. Journal of Evaluation in Clinical Practice,12(3), 376–384.
Upton D, Upton P (2006b) Knowledge and use of evidence-based practiceby allied health and health science professionals in the United Kingdom.Journal of Allied Health, 35(3), 127–133.
Vachon B, Durand M, LeBlanc J (2010) Empowering occupational therapists tobecome evidence-based work rehabilitation practitioners. Work, 37(2),119–134.
Welch A, Dawson P (2007) Engaging occupational therapists in applyingevidence to practice: an action research project. International Journal ofTherapy and Rehabilitation, 14(10), 460–465.
Rheumatology practice in occupationaltherapy: promoting lifestyle manage-ment. Lynne Goodacre and MargaretMcArthur, eds. Wiley-Blackwell, 2013.£29.99. 240pp. ISBN: 978-0470655-160
This academic text book has muchfor every practicing rheumatology clin-ician to learn and use. It is divided into13 chapters on all aspects of occupa-tional therapy. Topics include Livingwith a Rheumatic Disease; Personal andTheoretical Perspectives; the Occupa-tional Therapy Perspective; Work; JointProtection; Pain; Independence; Splint-ing, and Maintaining a Sense of Self.
Each chapter has a detailed resourcessection. One or two chapters are verytheoretical, but most are practical andfull of research evidence and, if used,will change your practice to be moreevidence based.
One chapter provides the resourcesthat we need to develop local policy foroccupational therapy in the Rheuma-tology Service, linking it to the latestgovernment policy and research of long-term conditions. It provides guidance asto the evidence that we need to prove thatoccupational therapy has a role to playin a changing National Health Service.
My criticism of the book is that somesuggested interventions do not fit wellwith the limited resources available toclinicians with a busy case load.
This book has already changed myclinical practice with patients. I can alsosee it providing the basis for someexcellent training courses, includingRheumatology Occupational TherapyAssessment. Overall, it is easy to read andis a great book to ensure you are usingthe latest evidence-based approaches.
Christina Macleod, Occupational Therapist,Hampshire Hospitals NHS Foundation Trust.
Book review
by guest on November 4, 2015bjo.sagepub.comDownloaded from View publication statsView publication stats