Embed Size (px)
Citation preview

47 EuropEan Journal of paEdiatric dEntistry vol. 14/1-2013
G. Consoli, V. Luzzi, G. Ierardo, G.L. Sfasciotti, A. Polimeni*
“Sapienza” University of Rome, Italy
Department of Oral and Maxillofacial Sciences
*Head of the Unit of Paediatric Dentistry,
Head of Department of Oral and Maxillofacial Science
e-mail: [email protected]
Keywords Occlusal trauma; Occlusion; Periodontal disease.
abstract
Aim Controversy over the relationship between occlusion and the progression of periodontal destruction has been ongoing since the beginning of scientific studies of dental diseases. This paper reviews the literature and explores the relationship between trauma from occlusion with periodontal disease in children, presenting recommendations for clinical practice based on the available evidence.
Occlusal traumain mixed dentition: literature review
occlusal forces applied to a tooth or teeth with normal and healthy supporting tissues, while secondary occlusal trauma refers to changes that occur when normal or abnormal occlusal forces are applied to the attachment apparatus of a tooth or teeth with inadequate or reduced supporting tissues [Davies et al., 2001; Fu and Yap, 2007; Gher, 1998].
More usefully, occlusal trauma can also be described as acute or chronic. Acute trauma from occlusion occurs following an abrupt increase in occlusal load such as that resulting from biting unexpectedly on a hard object. Chronic trauma from occlusion is more common and has greater clinical significance [Davies et al., 2001].
Historical studiesConsiderable effort has been directed toward
determining whether or not occlusal trauma plays a role in the aetiology of periodontal disease, since trauma from occlusion might contribute to the pathogenesis of periodontal disease [Forabosco, 2006], which is considered to be a mixed infection caused by subgingival microorganisms that cause the destruction of deep periodontal tissues VSocransky, 1992; Asikainen,1995].
For more than a century, clinicians have postulated that there is a relationship between occlusal forces and the progression of periodontal disease, as described in the latest review of the literature by Harrel et al. [Harrel and Nunn, 2009; Harrel et al., 2006].
Also in the early 20th century, Stillman, one of the early pioneers of periodontal therapy, proposed that excessive occlusal stress was the cause of periodontal disease. He indicated that the successful treatment of periodontal disease requires the clinician to control the occlusal forces [Stillman 1917, 1926; Harrel and Nunn, 2009].
In the 1940s, Weinmann performed one of the first evaluations of the relationship between occlusion and periodontal disease at the cellular level. Based on his observations of human autopsy specimens, he considered that periodontal disease was related to the progression of an inflammatory process that began at the gingival attachment and spread into the surrounding bone, following the course of blood vessels. Weinmann did not find evidence that occlusion caused or influenced the progression of the inflammatory process [Orban & Weinman, 1933; Weinman, 1941; Harrel and Nunn, 2009].
Two decades later, Glickman and Smulow [1962, 1969] also examined human autopsy specimens and agreed that inflammation appeared to begin at the gingival attachment and subsequently progress into the surrounding periodontal supporting tissue. However, they suggested that there was evidence that the progression of inflammation varied depending on whether the teeth were undergoing occlusal trauma. They termed this different progression of periodontal disease an “altered pathway of destruction,” and the combined effects of occlusal trauma and inflammation
Introduction
The effect of occlusion on the periodontium has been long debated. However, the relationship between trauma from occlusion and the periodontium has not yet been convincingly verified [Fu and Yap, 2007]. The term “occlusal trauma” (i.e trauma resulting from occlusion) refers to the pathological or adaptive changes of the periodontium caused by the excessive occlusal force known as traumatogenic occlusion [Davies et al., 2001; Kemal Ustun et al., 2008]. In 1978, the World Health Organization defined occlusal trauma as damage to the periodontal region caused by stress on the teeth produced directly or indirectly by the teeth in the antagonist arch [Forabosco, 2006].
According to the American Academy of Periodontology (AAP) International Workshop for Classification of Periodontal Diseases (1999), trauma from occlusion can be classified as either primary or secondary [Fu and Yap, 2007]. Primary occlusal trauma results from excessive
art_Consoli_Polimeni occl_Trauma.indd 47 20/02/13 14:27

CONSOLI G. ET AL..
EuropEan Journal of paEdiatric dEntistry vol. 14/1-201348
as “codestructive factors” in periodontal disease [Harrel and Nunn, 2009; Harrel et al., 2006].
In the 1970s, Waerhaug, again evaluating human autopsy specimens, considered there there were no convincing evidence that occlusal forces play any role in periodontal destruction. Waerhaug’s conclusion was that occlusal trauma played no part in periodontal destruction, with plaque-related inflammation being the only cause of periodontal disease [Waerhaug 1979a, b; Harrel and Nunn, 2009; Harrel et al., 2006].
Most historical studies on the effect of occlusal forces on the progression of periodontal disease were aimed at demonstrating whether occlusion causes periodontal destruction. The desire to find a single cause of periodontal disease was rooted in the disease concepts of the late 19th century: the idea that a chronic process such as periodontal disease resulted from multiple risk factors did not fit the outlook of the first half of the 20th century. Glickman and Smulow’s view of a codestructive action between bacterial inflammation and occlusal trauma was a step toward the modern concept of multiple risk factors affecting the progression and severity of the disease process [Harrel et al., 2006].
Animal researchStarting in the 1930s, several animal research
projects were performed in an attempt to establish unequivocally whether a relationship between occlusion and periodontal disease exists [Harrel et al., 2006].
Some of the more prominent studies of the 1970s and 1980s were performed by two research groups: the University of Gothenburg in Sweden (Lindhe, Ericsson and Nyman) used beagle dogs, while the Eastman Dental Center of Manchester in New York (Polson and Zander) used squirrel monkeys. In these animal models the researchers artificially induced experimental periodontitis by using silk ligatures or by allowing the animals to accumulate plaque and calculus over a variable period of time (usually 6 months). They could then superimpose traumatic occlusion by using cap splints, and evaluate its effect on bone loss and attachment loss [Bhola et al., 2008].
Despite major differences in the animal models and the types of excessive occlusal forces applied, many similar results were obtained from these two studies.
The conclusion of both research groups was that without inflammation, occlusal trauma does not cause irreversible bone loss or loss of attachment. Thus, it appears that occlusal trauma in these animals is not a causative agent of periodontal disease [Harrel et al., 2006].
Human studiesHuman research on occlusion has yielded mixed
results [Harrel et al., 2006]. Pihlstrom et al. [1986] evaluated the association
between occlusal trauma and periodontitis by examining a series of clinical and radiographic
parameters of maxillary first molars. They concluded that the severity of periodontitis did not differ between teeth with occlusal contacts in working, balancing, and nonworking positions and those teeth without such contacts [Bhola et al., 2008].
Burgett et al. [1992] used a controlled clinical trial to evaluate the effect of treating the occlusion on healing outcomes after periodontal treatment. This well-controlled study demonstrated that in a group of patients with existing periodontal disease, there was improved healing if occlusal trauma was minimised by occlusal adjustment [Harrel et al., 2006].
As part of a large study into prognoses, McGuire and Nunn [1996] reviewed the change in prognosis and in the number of teeth lost by patients with periodontal disease who had parafunctional habits. That study found that treating occlusal trauma in patients with periodontal disease improved treatment outcomes, and that the absence of such treatment resulted in greater tooth loss [Harrel et al., 2006].
The consensus of the 1996 World Workshop in Periodontics was that there was inadequate information to determine whether a relationship existed between occlusion and the progression of periodontal disease [Gher, 1996; Harrel et al., 2006].
Another review article published in the mid-1990s stated a similar viewpoint [Svanberg et al., 1995; Harrel et al., 2006], while the 1999 Consensus Report on Periodontal Disease Classification agreed that occlusal trauma represented injury that results in tissue changes within the attachment apparatus as a result of occlusal forces. That report also agreed that excessive occlusal forces alone do not initiate plaque-induced gingival disease or the loss of connective tissue associated with periodontitis [Hallmon, 1999; Harrel et al., 2006].
To summarise, these human studies have provided some evidence of an association between trauma from occlusion and periodontal disease, but have not proved the presence of a cause-and-effect relationship. Data are still inconclusive regarding the effect of trauma from occlusion on the response to periodontal therapy [Bhola, 2008].
Discussion
More than 400 bacterial species may be cultured from the periodontal pockets of different individuals, and it is possible to recover 30-100 species (any one of which may be a pathogenic agent) from a single site. Many of the bacterial species present in the pockets are difficult to culture and identify. State-of-the-art molecular biology investigation methods (e.g., real-time polymerase chain reaction) now allow to identify periodontal pathogens with greater specificity and sensitivity than when using culture investigation methods, and to quantify them reliably [Forabosco et al., 2006; Kobayashi et al., 1998].
Bacterial species considered to be periodontopathic
art_Consoli_Polimeni occl_Trauma.indd 48 20/02/13 14:27

LITERATURE REVIEW ON OCCLUSAL TRAUMA
EuropEan Journal of paEdiatric dEntistry vol. 14/1-2013 49
are probably saprophytes, which are commonly present in the oral cavity and can live for years as perfectly compatible members of the microbial flora.
Environmental factors can influence the microorganisms and force them to express damaging factors that remain hidden for a long time, or select for the more virulent clonal varieties. Environmental stress, which creates a fertile breeding ground for the bacterial flora, may be induced by one of the various types of occlusal trauma [Forabosco et al., 2006; Kleinfelder and Ludwigt, 2002]. In fact, traumatic forces may be exerted on a tooth or group of teeth when they are subjected to noncentric precontact or interference during disclusive jaw movement, or following extractions that distort the dental alignment [Alkan et al., 2006; Forabosco et al., 2006; Serio and Hawlwy, 1999].
Angle, Case, Jackson, and many others have developed orthodontic diagnoses and therapeutics in the belief that malocclusions and malpositioned teeth are significant factors in the aetiology of periodontal disease [Alkan et al., 2006].
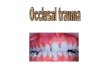
If it is accepted that increased occlusal forces could result in a further loss of attachment for teeth with an active inflammatory periodontitis, then it follows that a treatment plan aimed at preserving these teeth must address both problems. This does not mean that trauma from occlusion causes periodontitis; rather, it means that occlusal forces may exceed the “resistance threshold” of a compromised attachment apparatus, thereby exacerbating a pre-existing periodontal lesion [Alkan et al., 2006; Forabosco et al., 2006; Serio and Hawlwy, 1999]. It therefore follows that even though occlusal trauma is not a proven aetiological factor in periodontal disease, dentists must perform thorough occlusal examinations as part of their responsibility to maximize the health, comfort, and functioning of their patients’ teeth. Treatment aimed at reducing occlusal forces so that they fall within the adaptive capabilities of each patient’s dental attachment apparatus will be of benefit, particularly to those with or at future risk of periodontitis [Davies et al., 2001; Christensen, 2005, Polson, 1986]. Occlusal trauma is often caused by crowding of lower anterior teeth, anterior crossbite (Fig. 1), and thrusting of the mandible anteriorly on occlusion because of posterior occlusion and Class III malocclusion. Malocclusion and abnormal tooth position are now recognised as potential contributors to the disease process when they cause occlusal trauma.
Excessive functional stress may initiate inflammatory changes in the periodontium and thus enhance destructive bacterial processes. Occlusal trauma is able to extend the periodontal ligament space and hence encourage the apical migration of the bacteria and their proliferation [Asikainen et al., 1995; Bhola et al., 2008] (Fig. 2). Finally, Actinobacillus actinomycetemcomitans has been isolated in 53.3% of examined sites [Forabosco et al., 2006]. Although this is considered one of the
main periodontal pathogens, more-recent studies agree that A. actinomycetemcomitans plays a pathogenic role only in some subjects [Ximenez-Fyvie et al., 2000].
Localised gingival recession of the mandibular anterior teeth has been estimated to occur in about 7% of children. The reported incidence of severe gingival recession in young individuals in the literature is very low [Kemal Ustun et al., 2008; Ruiz, 2009].
Clinical diagnosis of trauma from occlusionIncreased tooth mobility is not always indicative of
trauma from occlusion. However, it is important that hypermobility, which does occur as a result of trauma from occlusion, is detected in patients with compromised periodontal attachment. The reason for this is that trauma from occlusion may accelerate further reductions in attachment in a patient with active periodontitis.
A definitive clinical diagnosis of occlusal trauma can only be made where progressive mobility can be identified through a series of repeated measurements over an extended period. This means that simple but reliable monitoring needs to be undertaken and a simple monitoring protocol is needed [Davies et al., 2001].
The common clinical signs of occlusal trauma are: increasing tooth mobility with migration or drifting, fremitus, and persistent discomfort on eating. The common radiographic signs of occlusal trauma are discontinuity and thickening of the lamina dura, widening of the periodontal ligament space (“funneling”
fig. 1 Anterior crossbite with occlusal trauma on tooth 31 in mixed dentition child.
fig. 2 Detail of occlusal trauma on tooth 41.
art_Consoli_Polimeni occl_Trauma.indd 49 20/02/13 14:27

CONSOLI G. ET AL..
EuropEan Journal of paEdiatric dEntistry vol. 14/1-201350
or “saucerisation”), and radiolucency and condensation of alveolar bone or root resorption [Davies et al., 2001].
Recommendations for the clinical practiceOcclusal trauma can precipitate migration of teeth,
pain during chewing, and patterns of increased mobility [Bayrak and Sen Tunc, 2008]. Incisor crossbite frequently results from abnormal retroclination of the anterior teeth of the maxilla. The occlusal trauma due to this condition and crowding can affect the periodontal health of the anterior teeth [Bayrak and Sen Tunc, 2008] (Fig. 1).
Various treatment methods have been proposed to correct anterior dental crossbite, such as bonded resin-composite slopes (Fig. 3) and removable acrylic appliances with finger springs [Strassler, 2009; Vitsentzos and Koidis, 1997] (Fig. 4). Short treatment times make these methods very attractive. Orthodontic treatment can often correct these problems, or at least prevent their progress [Seehra et al., 2009].
Conclusion
One of the chief objectives of paediatric dentistry is to guide the developing dentition to a state of normalcy in line with the stage of oral-facial growth and development. The period of mixed dentition offers the greatest opportunity for occlusal guidance and interception of malocclusion, since treatment may become more complicated if it is delayed to a later stage of maturity. Research involving humans has shown that occlusal discrepancies may be a significant risk factor for the progression of existing periodontal disease, and that the treatment of occlusal discrepancies significantly improves the outcome achieved with periodontal treatment [Harrel et al., 2006]. Removing the risk factor of occlusal discrepancies through selective grinding and/or occlusal appliances during periodontal therapy has been shown to produce significant changes in the progression of the disease and improve the results of treatment of the inflammatory component of the disease.
From this we conclude that the treatment of occlusal discrepancies should be considered as an integral part of the overall treatment of periodontal disease.
References
› Alkan A, Keskiner I, Arici S, Sato S. The effect of periodontitis on biting abilities. J Peridontol 2006 aug; 77(8): 1442-5.
› Asikainen S, Chen C, Slot SJ. Actinobacillus actinomycetemcomitans genotypes in relation to serotypes and periodontal status. Oral Microbiol and Immunol 1995; 10: 65-68.
› Bhola M, Cabanilla L, Kolhatkar S. Dental occlusion and periodontal disease: what is the real relationship?. J Calif Dent Assoc, 2008 Dec; 36(12): 924-30
› Davies SJ, Gray RJM, Linden GJ and James JA. Occlusal considerations in periodontics. Br Dent J 2001; 191(11): 597-604.
› Forabosco A, Grandi T, Vivoli R. Relationship between occlusal trauma and periodonthopatic flora. Clinical study with real-time PCR. Ann Stomatol 2006; 4(1): 16-22.
› Fu JH, Yap AU. Occlusion and periodontal disease. Where is the link?. Singapore Dent J 2007 Dec;29(1): 22-33 Review .
› Gher ME. Changing concepts. The effects of occlusion on periodontitis. Dent Clin North Am 1998 Apr; 42(2): 285-99.
› Harrel SK, Nunn ME. The association of occlusal contacts with the presence of increased periodontal probing depth. J Clin Periodontol 2009, 36:1035-1042
› Harrel SK, Nunn ME and Hallmon WW. Is there an association between occlusion and periodontal destruction?: yes-occlusal forces can contribute to periodontal destruction. J Am Dent Assoc 2006; 137: 1380-1392.
› Kemal Ustun, Zafer sari, Hasan Orocuglu, Ismet Duran and Sema S Hakki. Severe gingival recession caused by traumatic occlusion and mucogingival stress: a case report. Eur J Dent 2008; 2: 127-133.
› Kleinfelder JW, Ludwigt K. Maximal bite force in patients with reduced periodontal tissue support with and without splinting. J Periodontol 2002 Oct; 73(10): 1184-7.
› Kobayashi K, Kobayashi K, Soeda W, Watanable T. Gingival crevicular pH in experimental gingivitis and occlusal trauma in man. J Periodontol 1998 Sep; 69(9): 1036-43.
› Pihlstrom B, Anderson KA et al. Association between signs of trauma from occlusion and periodontitis. J Periodontol 1986; 57: 1-6, 1986.
› Polson AM. The relative importance of plaque and occlusion in periodontal disease. J Clin Periodontol 1986 Nov; 13(10): 923-7.
› Ruiz JL. Seven signs and symptoms of occlusal disease: the key to an easy diagnosis. Dent Today, 2009 Aug; 28(8): 112-3.
› Seehra J, Fleming PS, Di Biase AT. Orthodontic treatment of localized gingival recession associated with traumatic anterior crossbite. Aust Orthod J 2009 may; 25(1): 76-81.
› Serio FG, Hawlwy CE. Periodontal trauma and mobility. Diagnosis and treatment planning. Dent Clin North Am 1999 Jan; 43(1): 37-44.
› Strassler HE. Tooth stabilization improves periodontal progress: a case report. Dent Today 2009 Sep; 28(9): 88-92.
› Sule Bayrak and Emine Sen Tunc. Treatment of anterior dental crossbite using bonded resin-composite slopes: case reports. Eur J Dent 2008 Oct; 2: 303-306.
› Vitsentzos SI, Koidis PT. Facial approach to stabilization of mobile maxillary anterior teeth with steep vertical overlap and occlusal trauma. J Prosthet Dent 1997 May; 77(5): 550-2.
› Ximenez-Fyvie LA, Haffajee AD, Socransky SS. Comparison of the microbiota of supra- and subgingival plaque in health and periodontitis. J Clin Periodontol 2000; 27: 648-657.
fig. 3 Bonded resin-composite slopes on tooth 75 and 85.
fig. 4 Removable acrylic appliance with screw to procline tooth 11.
art_Consoli_Polimeni occl_Trauma.indd 50 20/02/13 14:27