Embed Size (px)
Citation preview

Received: 13 May 2002Published online: 19 November 2002© Springer-Verlag 2002
Abstract Case report: We report apediatric patient with encephalocele,lipomeningomyelocele, and Chiari Imalformation. Discussion: We alsoreview the extant medical literatureregarding associations between thesethree entities. We propose that thecombination of these three patholo-gies, which is reported here for thefirst time, is not serendipitous butrather a low-frequency association.Conclusions: After a literature re-view, we speculate that encephalo-cele and lipomeningomyelocele mostprobably occur by mechanisms simi-
lar to those that produce encephalo-cele and meningomyelocele and thatthe tonsillar ectopia in our patient isdue to an abnormally small posteriorcranial fossa resulting from the lackof neural tissue within the cranium atcritical times during development orhas its genesis, as some encephalo-celes may, in inappropriate paraxialmesoderm formation.
Keywords Cranium bifidum · Spinal dysraphism · Lipoma · Tonsillar ectopia · Hindbrain hernia
Childs Nerv Syst (2003) 19:50–53DOI 10.1007/s00381-002-0670-4 C A S E R E P O RT
R. Shane TubbsJohn C. Wellons IIIW. Jerry Oakes
Occipital encephalocele, lipomeningomyelocele, and Chiari I malformation: case report and review of the literature
Introduction
Encephaloceles of the cranium are presumably neuraltube defects; however, the association between concomi-tant defects of the skull and spina bifida occulta or apertais vague. We report a case of concurrent lumbar lipo-meningomyelocele, occipital encephalocele, and Chiari Imalformation in a newborn and review the extant medi-cal literature on these entities.
Case report
Our normal XY male patient was born at full term by cesareansection with no complications. The mother was Caucasian and thefather, Hispanic. At birth, the child was noted to have a large(12×8 cm) occipital encephalocele (Fig. 1) and a midline lumbarfatty mass measuring 5×6 cm (Fig. 2). The child was found on ex-amination to be able to move all extremities. MR imaging of thehead and lumbar spine revealed the encephalocele noted above(Fig. 3), Chiari I malformation, and lumbar lipomeningomyelocele(Fig. 4). The child had no cutaneous stigmata indicative of spinaldysraphism. The child underwent resection of the encephalocele,which had minimal parenchymal involvement. The anterior fonta-
R.S. Tubbs (✉)Department of Cell Biology, University of Alabama at Birmingham,Birmingham, Alabama, USAe-mail: [email protected].: +1-205-9396914Fax: +1-205-9399972
R.S. Tubbs · J.C. Wellons III · W.J. OakesPediatric Neurosurgery, Children’s Hospital, 1600 7th Avenue South Acc 400, Birmingham, AL 35233, USA
nel remained soft and sunken postoperatively, and serial imagingrevealed no hydrocephalus. The child’s lipomeningomyelocelewas operated without complications. To date, the child has not hada shunt placed, has no signs of either raised intracranial pressureor tonsillar ectopia, and moves both lower extremities well.
Discussion
The incidence of spinal lipomas is approximately 1 inevery 4,000 births [18]. In contrast, neural tube defectsoccur in 1–5 of every 1,000 live births, with encephalo-celes accounting for only about 5% of these [9] (70% ofwhich have occipital locations [10]). Encephaloceleshave been associated with both occult and nonoccultforms of spinal dysraphism. Meningomyeloceles arealso occasionally seen in association with encephalo-celes of both frontal and occipital origin [24]. “Double”neural tube defects are said to occur in approximately4–7% of live births [20, 26]. However, in a series of 623neural tube defects, Mealey et al. report that only 4 pa-tients had both encephalocele and meningomyelocele[19].

51
Diastematomyelia has occasionally been found in pa-tients with encephaloceles, and particularly in occipitalencephaloceles [24]. Naidich et al. report that 3% of oc-cipital encephaloceles will have an associated diastema-tomyelia [20]. Indeed, both encephalocele and spinaldysraphism have both been produced in rat models following exposure to vincristine or salicylates [7, 13].Vincristine, a vinca alkaloid, arrests cell division inmetaphase, whereas the teratogenic mechanisms of sali-cylates is unknown.
Many have assumed that these two entities, i.e., spinaldysraphism and cranium bifidum, are intuitively relatedas cephalad and caudal neural tube defects [24, 25].However, some authors have advocated categorizingcephaloceles in an independent category quite distinctfrom caudal neural tube malformation and with a sepa-rate dysembryology [6, 8, 21].
Lorber reports that in his series of 55 children bornwith occipital encephalocele, 1 had a lipoma of the caudaequina and 2 had a meningomyelocele [15]. It is of note
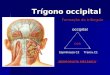
Fig. 2 Posterior view of lumbar region illustrating a subcutaneousfatty mass just superior to the intergluteal sulcus
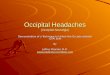
Fig. 3 Sagittal T1-weighted MRI of the brain illustrating the oc-cipital encephalocele. Tonsillar ectopia is mildly discernable
Fig. 4 Sagittal T1-weightedMRI of the lumbosacral regiondemonstrating the lipomenin-gomyelocele
Fig. 1 Lateral view of occipital encephalocele in our newborn pa-tient

52
that the Vater syndrome is associated with both occipitalencephalocele and spinal dysraphism [22]. Many patients with Knobloch syndrome have an associatedmeningocele as well as their occipital encephalocele [4].Associated findings in Goldenhar-Gorlin syndrome (oculo-auriculo-vertebral dysplasia) include occipital en-cephalocele, intracranial lipoma, and spinal dysraphism[1]. Curiously, Colombo et al. report a case of encepha-locele with congenital clubfoot in which no imaging ofthe lumbar spine was obtained [5].
Interestingly, encephaloceles are often associated withlipomas of the corpus callosum [16, 23]. It has been pro-posed that lipomas of both the corpus callosum and thelumbar spinal cord develop because fat-forming cells be-come abnormally trapped within areas of the anterior andposterior neuropore [16]. In fact, Fitz classifies both encephaloceles and lipomas of the corpus callosum asdisorders of closure [10]. However, this would need tooccur during primary neural tube closure, and the forma-tion of lipomeningomyelocele most probably occurs between gestational days 28 and 48 [11]. McLone hasproposed that a lipomeningomyelocele is formed whenthe neural tube detaches from the cutaneous ectodermprematurely, thereby allowing the folding neuroectodermto remain cleft dorsally, which could allow paraxial mes-enchyme access to the neural tube [18]. Giuffrè reports acase of intradural spinal lipoma of the cervical spinewith concurrent lipoma of the corpus callosum [12].There is a possible link between prenatal maternal expo-sure to valproic acid and lipomeningomyelocele forma-tion [3].
Tonsillar ectopia (Chiari I malformation) is seen in3–6% of patients with lipomeningomyelocele [2, 14]. Itis also known that the posterior cranial fossa tends to besmaller/distorted in this form of hindbrain herniation[17]. Therefore, could a decrease in intracranial nervoustissue and cerebrospinal fluid from an encephalocele al-low the developing posterior fossa to be smaller withoutthe expansile qualities of brain tissue and cerebrospinalfluid? It has been postulated that Chiari malformationand encephalocele are both forms of paraxial mesoderminsufficiency in the developing fetus [17].
Conclusions
Following a review of the literature on concomitant en-cephalocele, lipomeningomyelocele, and Chiari I malfor-mation, we believe our case report to be the first of itskind. However, there are several citations of associationsof encephaloceles and occult and nonoccult forms of spi-nal dysraphism, which were intraspinal “lipomas” in 2cases, and of encephalocele and hindbrain herniation tounderdevelopment of posterior cranial fossa paraxial me-soderm. In light of these findings, we hypothesize thatthe pathologic findings in our patient may be linked embryologically and are not spurious but rather low-fre-quency associations. These data will hopefully proveuseful to the clinician who may entertain the possibilitythat any one of these findings might be present in a pa-tient presenting with encephalocele, lipomeningomyelo-cele, or Chiari I malformation.
References
1. Aleksic S, Budzilovich G, Greco MA,McCarthy J, Reuben R, Margolis S,Epstein F, Feigin I, Pearson J (1984)Intracranial lipomas, hydrocephalus,and other CNS anomalies in oculoauriculo-vertebral dysplasia(Goldenhar-Gorlin syndrome). Childs Brain 11:285–297
2. Byrne RW, Hayes EA, George TM,McLone DG (1995) Operative resection of 100 spinal lipomas in infants less than 1 year of age. PediatrNeurosurg 23:182–187
3. Carter BS, Stewart JM (1989) Valproicacid prenatal exposure: associationwith lipomyelomeningocele. ClinPediatr (Phila) 28:81–85
4. Cohen MM, Lemire RJ (1982) Syndromes with cephaloceles. Teratology 25:161–172
5. Colombo P, Bianchi GA, Meregalli V(1996) Valutazioni patogenetiche circaun caso di encefalocele, rachischisi altae piede torto congenito non inquadra-bile in sindrome nota. Minerva Pediatr48:105–111
6. Curnes JT, Oakes WJ (1988) Parietalcephaloceles: radiographic and mag-netic resonance imaging evaluation.Pediatr Neurosci 14:71–76
7. DeMyer W (1965) Cleft lip and jaw induced in fetal rats by vincristine.Arch Anat Histol Embryol 48:180–186
8. DeSesso JM, Scialli AR, Holson JF(1999) Apparent lability of neural tubeclosure in laboratory animals and hu-mans. Am J Med Gen 87:143–162
9. Drugan A, Weisman A, Evans MI(2001) Screening for neural tube defects. Clin Perinatol 28:279–287
10. Fitz CR (1982) Midline anomalies ofthe brain and spine. Radiol Clin NorthAm 20:95–104
11. French BN (1996) Embryological aspects of the tethered cord syndromeand its relationship to spinal dysra-phism. In: Yamada S (ed) Tetheredcord syndrome. AANS, Park Ridge,pp 5–20
12. Giuffrè R (1966) Intradural spinal lipomas: review of the literature (99cases) and report of an additional case.Acta Neurochir (Wien) 14:69–95
13. Goldman AS, Yakovac WC (1963) Theenhancement of salicylate teratogeni-city by maternal immobilization in therat. J Pharmacol Exp Ther142:351–357
14. Grijalvo CA, Bank WO, Balériaux D,Imaña FJ, Szliwowski HB, Brotchi J(1993) Lipomyeloschisis associatedwith thoracic syringomyelia and ChiariI malformation. Neuroradiology35:375–377

53
15. Lorber J (1967) The prognosis of encephalocele. Dev Med Child Neurol
Suppl 13:75–8616. Macpherson RI, Holgate RC, Gudeman
SK (1987) Midline central nervous lipomas in children. J Can Assoc Radiol 38:264–270
17. Marín-Padilla M (1991) Cephalic axialskeletal-neural dysraphic disorders:embryology and pathology. Can JNeurol Sci 18:153–169
18. McLone DG (2000) Congenital malformations of the central nervoussystem. Clin Neurosurg 47:346–377
19. Mealey J, Dzenitis AJ, Hockey AA(1970) The prognosis of encephalo-celes. J Neurosurg 32:209–218
20. Naidich TP, Altman NR, Braffman BH,McLone D, Zimmerman RA (1992)Cephaloceles and related malforma-tions. AJNR Am J Neuroradiol13:655–690
21. Patterson RJ, Egelhoff JC, Crone KR,Ball WS (1998) Atretic parietal ceph-aloceles revisited: an enlarging clinicaland imaging spectrum. AJNR AmJ Neuroradiol 19:791–795
22. Raffel C, Litofsky S, McComb JG(1990–1991) Central nervous systemmalformations and the Vater associa-tion. Pediatr Neurosurg 16:170–173
23. Rao AS, Rao VRK, Mandalam KR,Gupta AK, Kumar S, Joseph S, Unni M(1990) Corpus callosum lipoma withfrontal encephalocele. Neuroradiology32:50–52
24. Reigel DH (1982) Encephaloceles. In:Section of Pediatric Neurosurgery ofthe American Association of Neurolog-ical Surgeons (eds) Pediatric neurosur-gery: surgery of the developing ner-vous system. Grune & Stratton, New York, pp 49–60
25. Stegmann K, Boecker J, Richter B,Capra V, Finnell RH, Ngo E, Strehl E,Ermert A, Kock MC (2001) A screenfor mutations in human homologues ofmice exencephaly genes Tfap2a andMsx2 in patients with neural tube defects. Teratology 63:167–175
26. Van Allen MI, Kalousek DK, ChernoffGF, Juriloff D, Harris M, McGillivrayBC, Yong SL, Langlois S, MacLeodPM, Chitayat D, Friedman JM, Wilson RD, McFadden D, Pantzar J,Ritchie S, Hall JG (1993) Evidence formulti-site closure of the neural tube inhumans. Am J Med Gen 47:723–743
![REVIEW Open Access...occipital (meningo) encephalocele of variable severity [1,34,41]. Ocular features The retina is one of the organs most frequently involved in JSRD, mostly in the](https://img.dokumen.tips/doc/110x75/60a8281e18acaf286a04b5cf/review-open-access-occipital-meningo-encephalocele-of-variable-severity-13441.jpg)