Embed Size (px)
Citation preview

Obstructed kidneys –
What to do?Des Sankar
Second Trimester Antenatal Surveillance
Detects a significant fetal anomaly in 1% of pregnancies
20 to 30% are genitourinary in origin
50% manifest as hydronephrosis
Incidence of ANH is 2-9/1000
Hydronephrosis implies obstruction
Better term – an increased Renal Pelvic Dilatation (RPD) as not all cases with
increased RPD are associated with obstruction
If not detected antenatally,
hydronephrosis can result in……
Pyelonephritis
Recurrent loin or abdominal pain
Renal calculi
Hypertension
End-stage renal disease
Aetiology of ANH
Transient/Physiological 50-70%
PelviUreteric Junction Obstruction 10-30%
Vesicoureteral reflux 10-40%
Uterovesical junction obstruction/megaureter 5-15%
Multicystic dysplastic kidney 2-5%
Posterior urethral valves 1-5%
Ureterocoele, ectopic ureter, duplex system Uncommon
Prune belly syndrome, polycystic kidney disease
Cysts
Nguyen et al.2010. The Society for Fetal Urology consensus statement on the evaluation and management of
Antenatal hydronephrosis. J Pediatr Urol 201;6:212-31
Antenatal Hydronephrosis (ANH)
Common 2 approaches of assessment
1. Anterior-posterior renal pelvic diameter
2. Society for Fetal Urology grading

AP Diameter
Second Trimester > 4mm
Third Trimester > 7mm
Based on published work of Lyn S Chitty and Douglas G Altman
94% of fetuses with an AP diameter of >20mm
50% with AP diameter of 10 to 15mm
3% with < 10mm
Required surgery or at least longterm monitoring for a significant urinary tract
lesion
Charts of fetal size:Kidney and renal pelvis measurements. Prenat Diag:2003Nov,23(11)891
Stocks A,et al: Correlation of prenatal renal pelvic anteroposterior diameter with outcome in infancy.
J Urol. Mar 1996;155(3):1050-2

AP Diameter
Second Trimester 7mm or more
Fetal Anomaly Screening Program (NHS)
Third Trimester >10mm
OR
Smaller diameters associated with Calyceal Dilatation
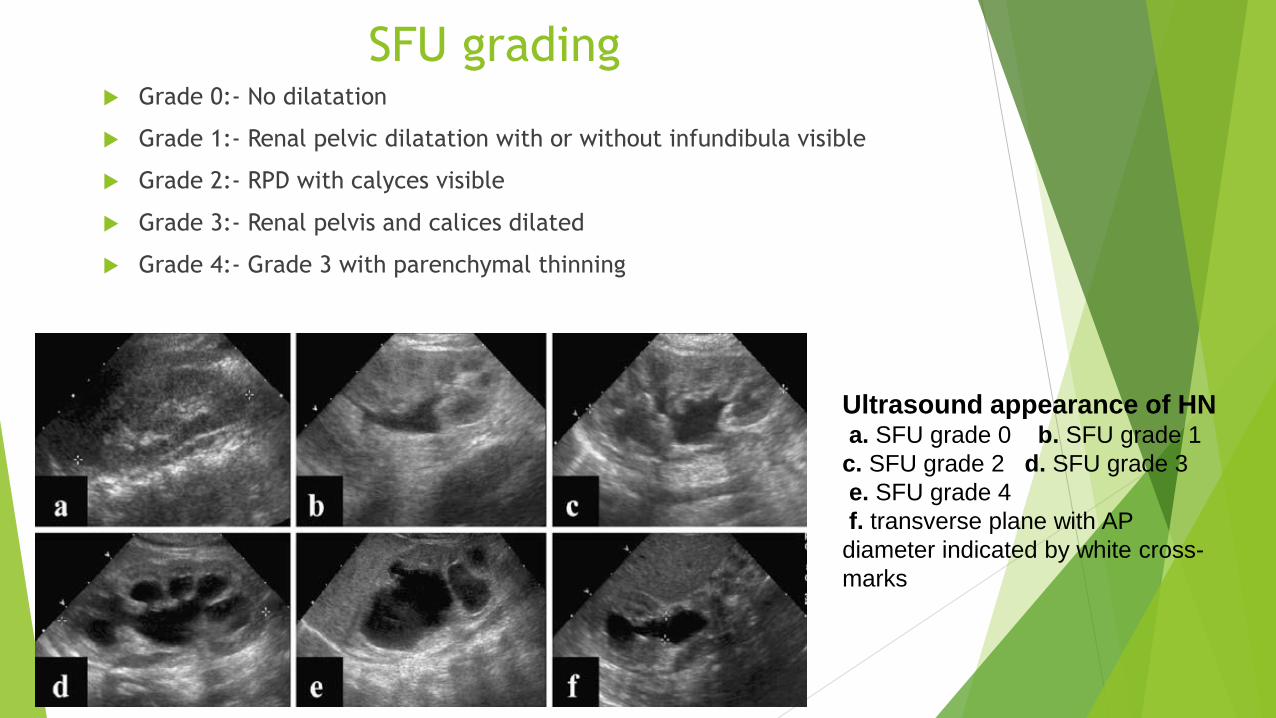
SFU grading Grade 0:- No dilatation
Grade 1:- Renal pelvic dilatation with or without infundibula visible
Grade 2:- RPD with calyces visible
Grade 3:- Renal pelvis and calices dilated
Grade 4:- Grade 3 with parenchymal thinning
Ultrasound appearance of HNa. SFU grade 0 b. SFU grade 1
c. SFU grade 2 d. SFU grade 3
e. SFU grade 4
f. transverse plane with AP
diameter indicated by white cross-
marks
SFU
Second trimester RPD
Mild 4 to <7mm
Moderate 7 to < 10mm
Severe > 10mm
Third Trimester RPD
Mild 7 to < 9mm
Moderate 9 to < 15mm
Severe > 15mm

Correlation with Outcomes
Larger the RPD……………………………..Caused by Obstructive Uropathy
The greater the risk of postnatal surgery
The lower the spontaneous resolution rate
Exception is with vesicoureteric reflux

Views that should be obtained
Spine AnteriorParasagittal for the length
Coronal for symmetry and echogenicity
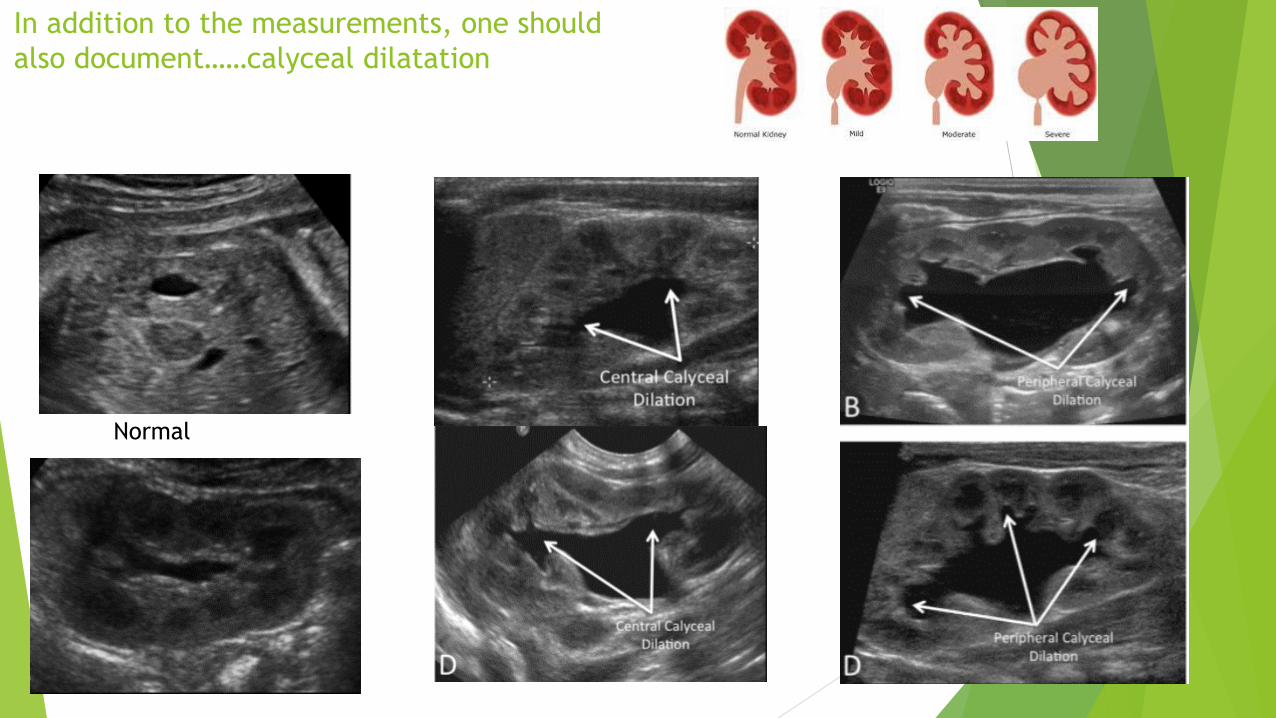
In addition to the measurements, one should
also document……calyceal dilatation
Normal

…..Parenchymal Thickness/Appearance
1. Thickness
2. Echogenicity
3. Cysts
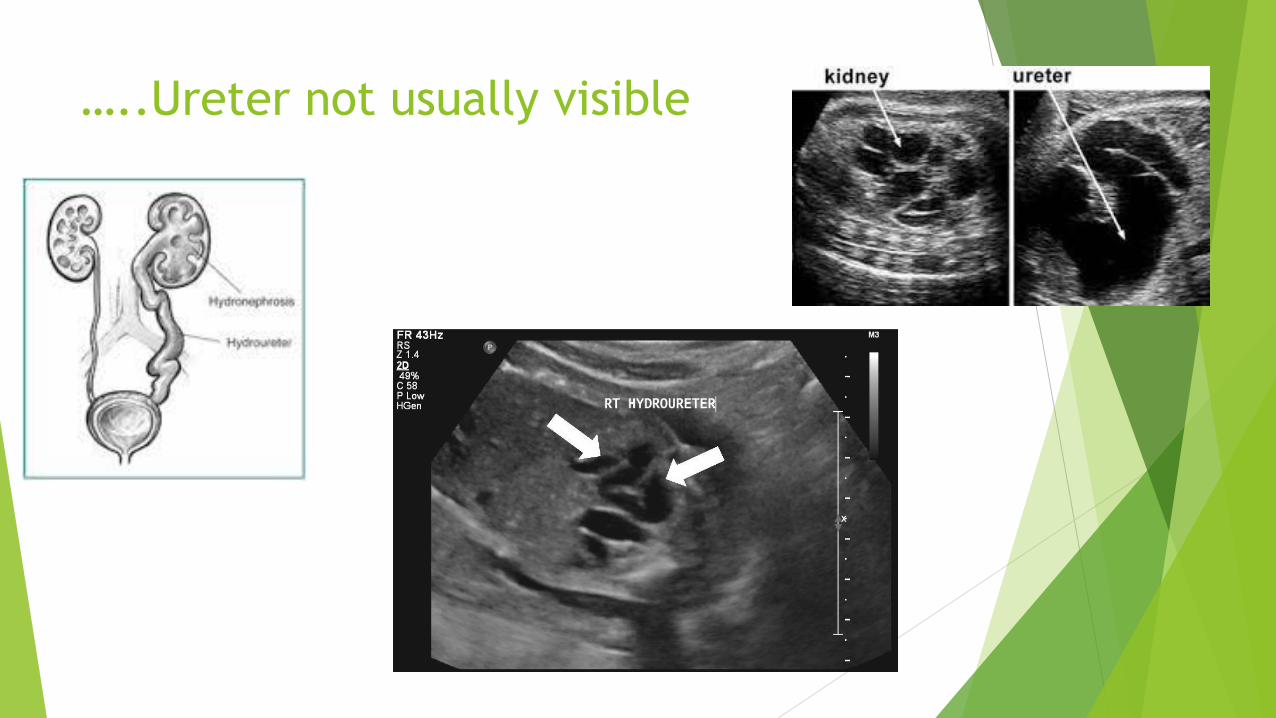
…..Ureter not usually visible
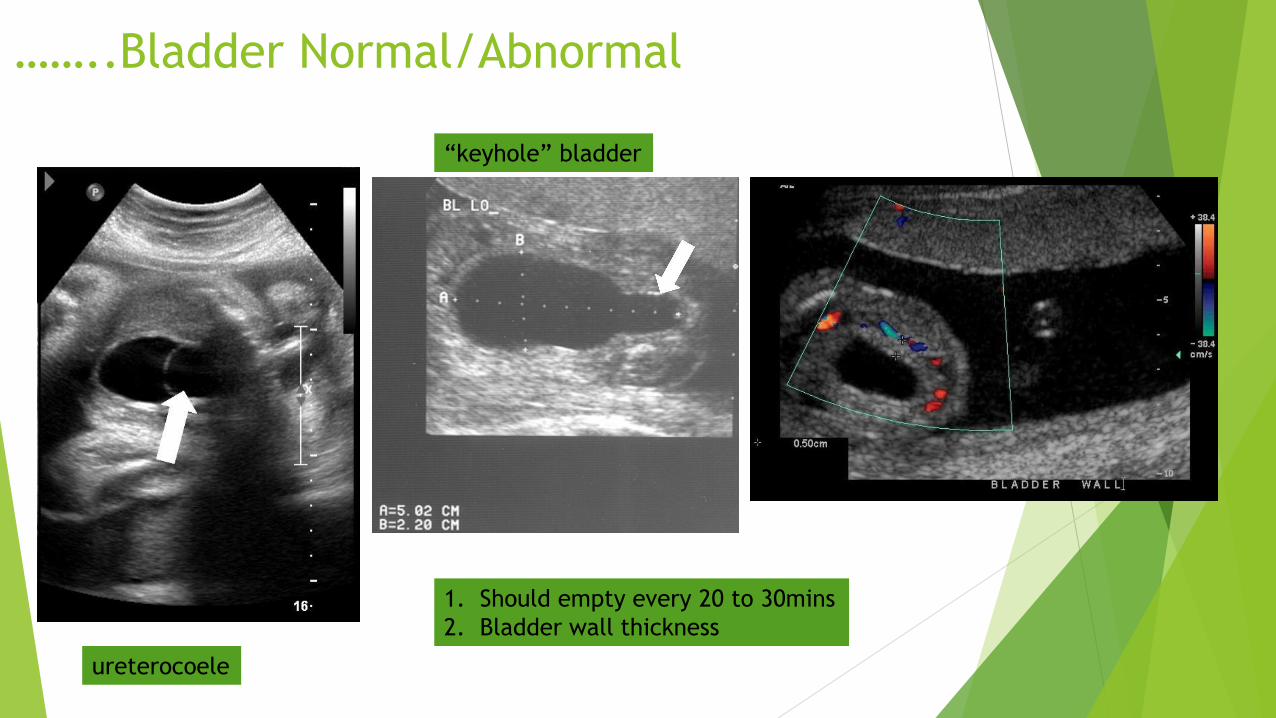
……..Bladder Normal/Abnormal
1. Should empty every 20 to 30mins
2. Bladder wall thickness
ureterocoele
“keyhole” bladder

………Amniotic fluid volume
Enquire about ruptured membranes
Aetiology of ANH
Transient/Physiological 50-70%
PelviUreteric Junction Obstruction 10-30%
Vesicoureteral reflux 10-40%
Uterovesical junction obstruction/megaureter 5-15%
Multicystic dysplstic kidney 2-5%
Posterior urethral valves 1-5%
Ureterocoele, ectopic ureter, duplex system Uncommon
Prune belly syndrome, polycystic kidney disease
Cysts
Nguyen et al.2010. The Society for Fetal Urology consensus statement on the evaluation and management of
Antenatal hydronephrosis. J Pediatr Urol 201;6:212-31
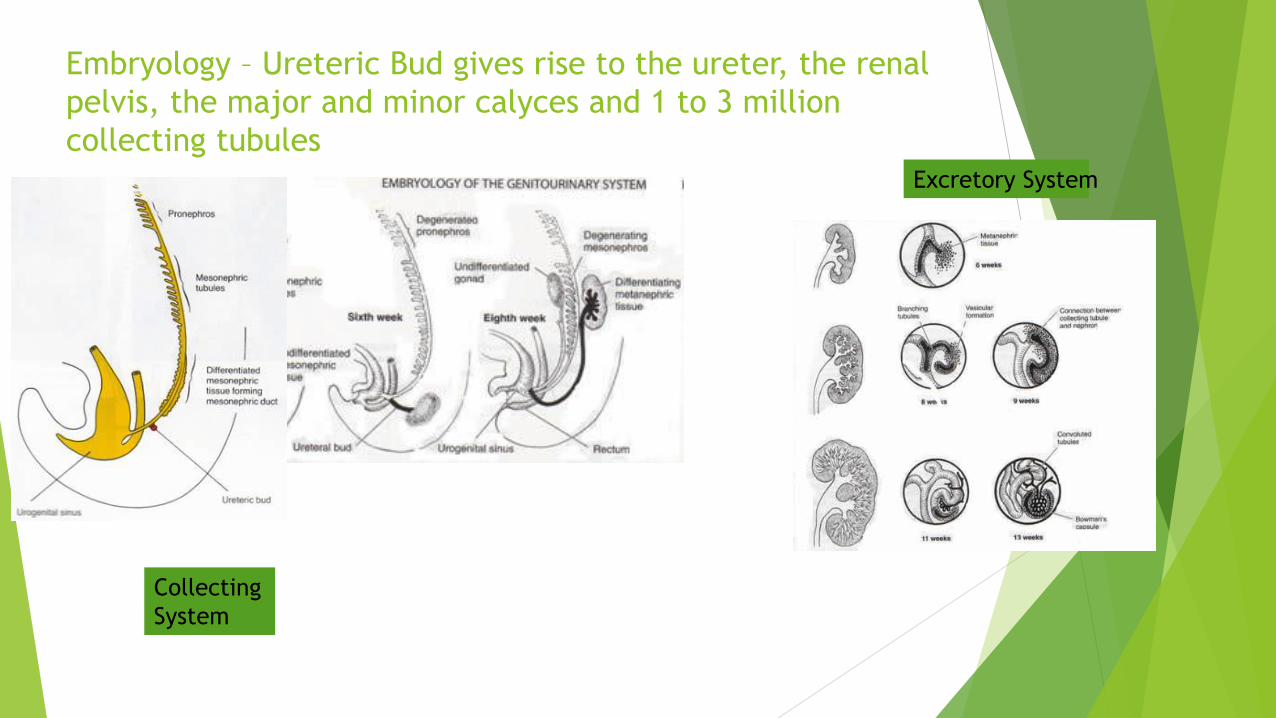
Embryology – Ureteric Bud gives rise to the ureter, the renal
pelvis, the major and minor calyces and 1 to 3 million
collecting tubules
Collecting
System
Excretory System

Physiological
Maternal overhydration
? Compression of the ureter by distended fetal bladder
70% of fetuses over a 2 hour period, exhibited both normal and abnormal
values (RPD <4mm to <10mm)
Striking findings concerning the variability in the measurement of the fetal renal
collecting system.
PersutteWH;et al UOG 2000;15:186-190
Delayed canalization of the ureter
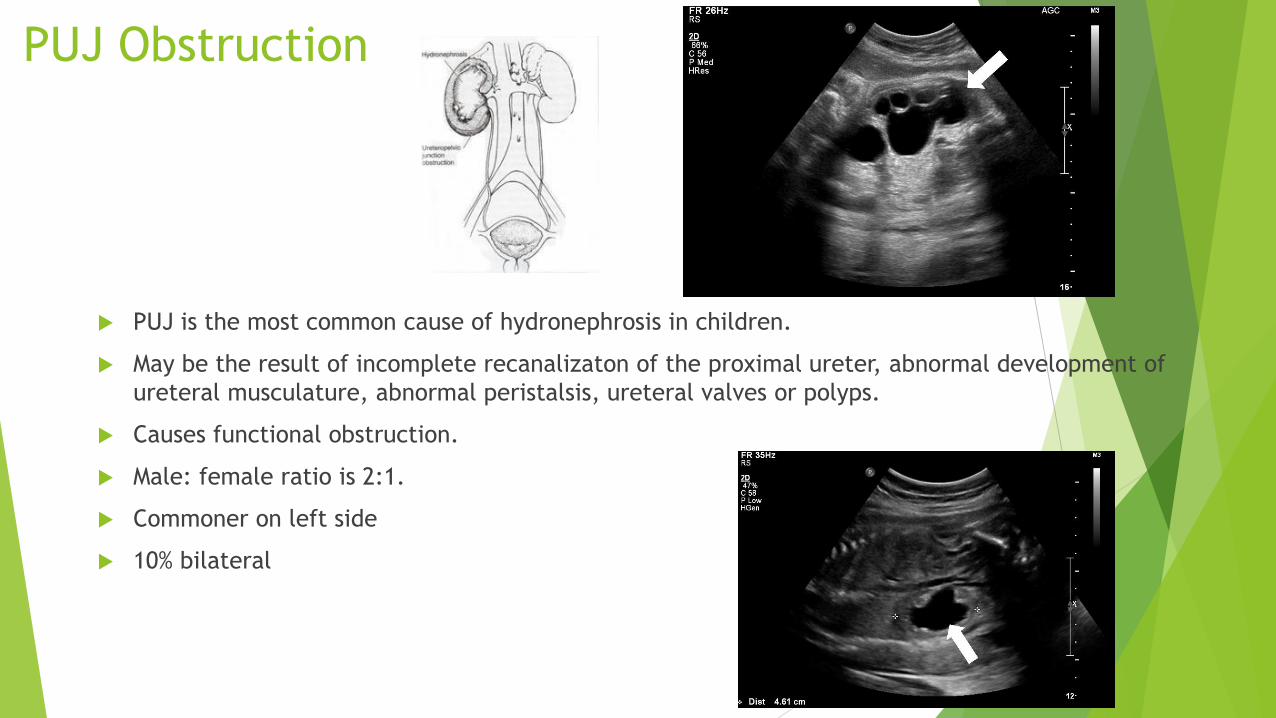
PUJ Obstruction
PUJ is the most common cause of hydronephrosis in children.
May be the result of incomplete recanalizaton of the proximal ureter, abnormal development of
ureteral musculature, abnormal peristalsis, ureteral valves or polyps.
Causes functional obstruction.
Male: female ratio is 2:1.
Commoner on left side
10% bilateral

Management
Antenatal follow-up scans & Generally deliver at term
Unilateral carries a good outcome
Bilateral hydronephrosis and oligohydramnios increased incidence of structural anomaly (cardiac, neurological and orthopaedic)
Post delivery
Mild unilateral or bilateral
No antibiotics
Renal tract US within 2w of birth
Reuss A, et al 1988

Moderate/severe or mild bilateral with
one other abnormality……………
Antibiotics
US in the first few days of life
Paediatric urology follow-up
VCU and MAG3 scans

Multicystic dysplastic kidney
MCDK
PUJODiscriminatory feature:- echogenic stroma

MCDK
Congenital maldevelopment in which the renal cortex is replaced by
numerous cysts of varying sizes
Usually unilateral and if very large, it can occasionally compress the
contralateral ureter
Bilateral – incompatible with life
Rarely associated with hypertension and malignancy
Needs paediatric follow-up
No antibiotics are required post delivery

Posterior Urethral Valves
Commonest cause of obstructive
megacystis
Abnormal congenital obstructing
membrane located in the posterior
urethra
Mechanical obstruction increases
voiding pressures and may alter
the development of the bladder
and kidneys
Symptoms – mild voiding disability
to severe – renal failure and
pulmonary hypoplasia
VCU :- dilated bladder with trabeculation,
diverticula and bilateral massive reflux
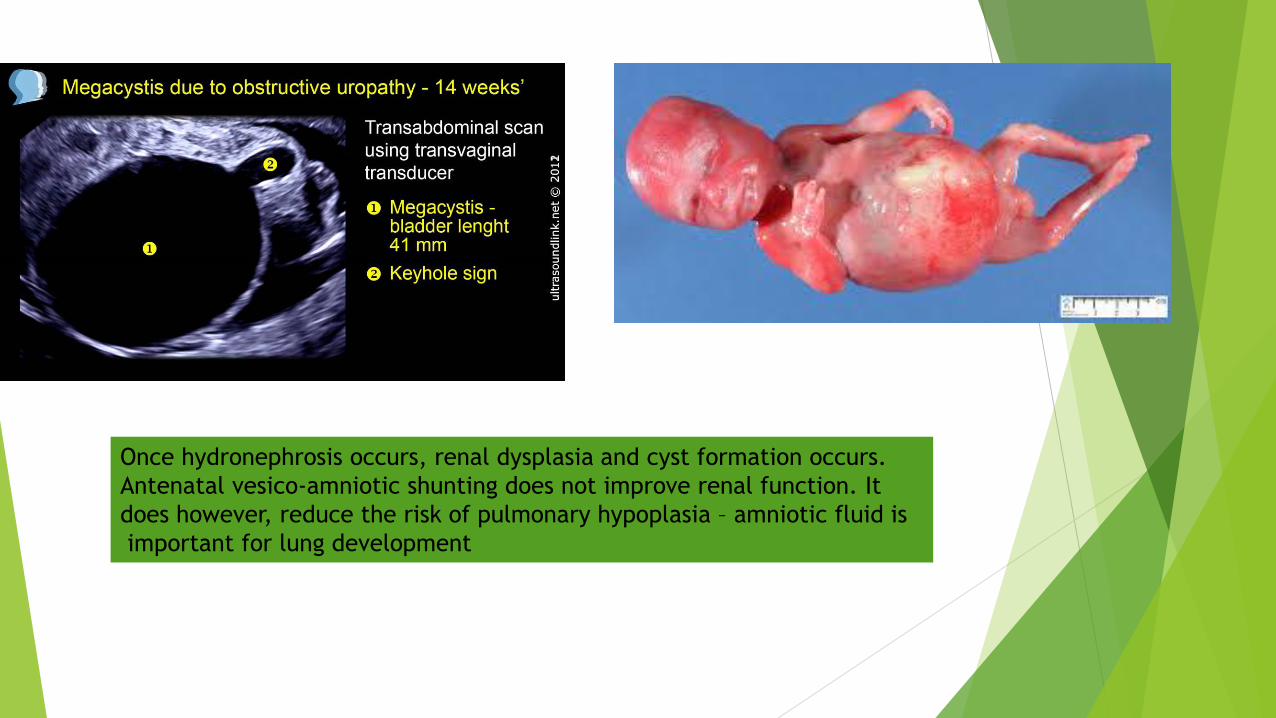
Once hydronephrosis occurs, renal dysplasia and cyst formation occurs.
Antenatal vesico-amniotic shunting does not improve renal function. It
does however, reduce the risk of pulmonary hypoplasia – amniotic fluid is
important for lung development
PUV delivery….
At 37 -38w
Might require ventilator support
In an institution with paediatric surgical expertise- immediate catherization
Survivors of the initial hurdle, will require early surgical intervention –
cystoscopy and ablation of the posterior valves
>30% will require renal transplant
Pregnancy interruption if detected early …… should be an option.

Pelviureteric Reflux
Post delivery VCU

In Summary
Renal Pelvic Dilatation is not uncommon
Once detected, assess the entire renal tract
Document the findings
Discuss findings (with available images) with the paediatric urologist and
paediatrician and formulate a plan of action