Embed Size (px)
Citation preview

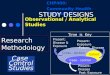
OBSERVATIONAL STUDY
Dr. Partha Sarkar (PGT, 2nd Yr)
Department of Pharmacology Medical College, Kolkata

STUDY DESIGN
Observational
Analytical Cross sectional Cohort Case control
Descriptive Case report Case series surveys
Experimental RCT QUASI

Study Design

Observational vs. Experimental Study
Observational studies The population is observed without any interference by the investigator
Experimental studies The investigator tries to control the environment in which the hypothesis is tested (the randomized, double-blind clinical trial is the gold standard)

Observational Study
• Non-experimental• Observational because there is no individual intervention• Treatment and exposures occur in a “non- controlled” environment• Individuals can be observed prospectively, retrospectively, or currently

Limitation of observational research: confounding
Confounding: Risk factors don’t happen in isolation, except in a controlled experiment.
Example Breastfeeding has been linked to higher IQ in infants, but the association could be due to confounding by socioeconomic status. Women who breastfeed tend to be better educated and have better prenatal care, which may explain the higher IQ in their infants.

Cause and Effect?
AtherosclerosisDepression in
elderly
?Biological changes
?Lack of exercise Poor Eating
Advancing Age

Why Observational Studies?
Cheaper Faster Can examine long-term effects Hypothesis-generating Sometimes, experimental studies are not ethical (e.g- Randomizing subjects to smoke)

Descriptive Studies

Good descriptive reporting answers five basic W questions: Who, what, why, when, where
Case report Case-series reports Surveillance studies
And a sixth: so what ?
Who has the disease in question ? What is the condition or disease being studied ? Why did the condition or disease arise ? Where does or does not the condition arise?
Descriptive studies

Case Report
Case Series
DescriptiveEpidemiology Study
One case of unusual findings
Multiple cases of findings
Population-based cases with denominator
Descriptive studies

Case Reports
Detailed presentation of a single case or handful of cases
Generally report a new or unique finding
e.g-
• previous undescribed diseas• unexpected link between diseas• unexpected new therapeutic effect• adverse events

Case Series
Experience of a group of patients with a similar diagnosis Assesses prevalent disease Cases may be identified from a single or multiple sources Generally report on new/unique condition May be only realistic design for rare disorders

Advantages• Useful for hypothesis generation• Informative for very rare disease with few established risk factors• Characterizes averages for disorder
Disadvantages• Cannot study cause and effect relationships• Cannot assess disease frequency
Case Series

Analytical Studies

Look to link exposure and disease What is the exposure? Who are the exposed? What are the potential health effects? What approach will you take to study the relationship
between exposure and effect?
Basic Question in Analytic Epidemiology

Basic Question in Analytic Epidemiology
Are exposure and disease linked?
Exposure Disease

Analytical Stdies

Analytical Stdies

Cross-sectional studies
An “observational” design that surveys exposures and disease status at a single point in time (a cross-section of the population)
timeStudy only exists at this point in time

Cross-sectional Design
time
Study only exists at this point in time
Studypopulation
No Disease
Disease
factor present
factor absent
factor present
factor absent

Cross-sectional Studies
Often used to study conditions that are relatively frequent with long duration of expression (nonfatal, chronic conditions) It measures prevalence, not incidence of disease Example: community surveys Not suitable for studying rare or highly fatal diseases or a disease with short duration of expression

Cross-sectional studies
Disadvantages Weakest observational design,(it measures prevalence,
not incidence of disease). Prevalent cases are survivors The temporal sequence of exposure and effect may be
difficult or impossible to determine Usually don’t know when disease occurred Rare events a problem. Quickly emerging diseases a
problem

Cross-sectional study
Relationship between atherosclerosis and late-life depression (Tiemeier et al. Arch Gen Psychiatry, 2004).
Methods Researchers measured the prevalence of coronary artery calcification (atherosclerosis) and the prevalence of depressive symptoms in a large cohort of elderly men and women in Rotterdam (n=1920).

Coronary calc >500 539
Coronary calc <=500 1381
81 1839 1920
Any depression
None
28 511
53 1328
2.19) (0.86, CI 95% ;37.1038.052.
RR
Risk Ratio
Interpretation: those with coronary calcification are 37% more likely to have depression (not significant).

Key difference
WHO IS BEING COMPARED?
COHORT: EXPOSED VS. UNEXPOSED
CASE-CONTROL: DISEASED VS. NON-DISEASED

Cohort studies
Sample on exposure status and track disease development (for rare exposures)
Marginal probabilities (and rates) of developing disease for exposure groups are valid.

Timeframe of Studies
Prospective Study Looks forward, looks to the future, examines future events, follows a condition, concern or disease into the future
time
Study begins here

Cohort Studies
Target population
Exposed
Not Exposed
Disease-free cohort
Disease
Disease-free
Disease
Disease-free
TIME

Types of cohort study

The Framingham Heart Study
The Framingham Heart Study was established in 1948, when 5209 residents of Framingham, Mass, aged 28 to 62 years, were enrolled in a prospective epidemiologic cohort study.
Health and lifestyle factors were measured (blood pressure, weight, exercise, etc.).
Interim cardiovascular events were ascertained from medical histories, physical examinations, ECGs, and review of interim medical record.

Measuring Risk
Cohort StudyWhat is the probability of getting diseased if you are
exposed as compared to unexposed?
Case-Control StudyWhat is the probability of having been exposed if
you have the disease compared to not having the disease?

Risk in Cohort Studies
Relative Risk (RR)
R R
A A BC C D
p ro b ab ility o f d isea se g iv en e x p o sedp ro b ab ility o f d isea se g iv en u n ex p o sed
/ ( )/ ( )
Disease Non-DiseasedExposed A B A+B
Unexposed C D C+DA+C B+D

400 400
1100 2600
0.23000/4001500/400 RR
Hypothetical Data
Normal BP
CHF
No CHF
1500 3000
High Systolic BP

Cohort Studies-Advantages/Limitations
Advantages Allows you to measure true rates and risks of disease for
the exposed and the unexposed groups. Temporality is correct (easier to infer cause and effect). Can be used to study multiple outcomes. Prevents bias in the ascertainment of exposure that may
occur after a person develops a disease.Disadvantages
Can be lengthy and costly! 60 years for Framingham. Loss to follow-up is a problem (if non-random) Selection Bias: Participation may be associated with
exposure status for some exposures

Case-Control Studies
Sample on disease status and ask retrospectively about exposures (for rare diseases)Marginal probabilities of exposure for cases and controls
are valid.
Doesn’t require knowledge of the absolute risks of disease
For rare diseases, can approximate relative risk

Timeframe of Studies
• Retrospective Study “to look back”, looks back in time to study events that have already occurred
time
Study begins here

Target population
Exposed in past
Not exposed
Exposed
Not Exposed
Case-Control Studies
Disease(Cases)
No Disease(Controls)

Case-control example
A study of the relation between body mass index and the incidence of age-related macular degeneration.
Methods Researchers compared 50 Iranian patients with confirmed age-related macular degeneration and 80 control subjects with respect to BMI, smoking habits, hypertension, and diabetes. The researchers were specifically interested in the relationship of BMI to age-related macular degeneration.

Results
Comparison of BMI in case and control groups
Case n = 50(%) Control n = 80 (%) p Value
Lean BMI <20 7 (14) 6 (7.5) NS
Normal 20 BMI <25 16 (32) 20 (25) NS
Overweight 25 BMI <30 21 (42) 36 (45) NS
Obese BMI 30 6 (12) 18 (22.5) NS
NS, not significant.

Overweight Normal
ARMD 27 23
No ARMD 54 26
What is the risk ratio here?
50
80
There is no risk ratio, because we cannot calculate the risk of disease!!
Corresponding 2x2 Table

Odds vs. Risk
We cannot calculate a risk ratio from a case-control study.
BUT, we can calculate a measure called the odds ratio…

Odds vs. Risk
If the risk is… Then the odds are…
½ (50%)
¾ (75%)
1/10 (10%)
1/100 (1%)
An odds is always higher than its corresponding probability, unless the probability is 100%
1:13:1
1:9
1:99

The proportion of cases and controls are set by the investigator; therefore, they do not represent the risk (probability) of developing disease.
bcad
dcba
dcddccbabbaa
ORDEP
DEPDEP
DEP
)/()/()/()/(
)~/(~)~/()/(~
)/(
Exposure (E) No Exposure (~E)
Disease (D) a b
No Disease (~D) c d
a+b=cases
c+d=controls
Odds of exposure in the cases
Odds of exposure in the controls
Odds Ratio

dbca
dcba
bcadOR
Exposure (E) No Exposure (~E)
Disease (D) a b
No Disease (~D) c d
Odds of disease for the exposed
Odds of exposure for the controls
Odds of exposure for the cases
Odds of disease for the unexposed
Odds Ratio

57.54*2326*27
26542327
OR
Overweight Normal
ARMD 27 23
No ARMD 54 26
Can be interpreted as: Overweight people have a 43% decrease in their ODDS of age-related macular degeneration. (not statistically significant here)
Odds Ratio

RROR
If the disease is rare (affecting <10% of the population)
WHY?
If the disease is rare, the probability of it NOT happening is close to 1, and the odds is close to the risk. Eg:
50.10:120/1
474.9/1
19/1
RR
OR
Odds Ratio
Good approximation of the risk ratio if the disease is rare

The Rare Disease Assumption
RROR EDPEDP
EDPEDPEDP
EDP
)~/()/(
)~/(~)~/()/(~
)/(
1
1
When a disease is rare: P(~D) = 1 - P(D) 1

The odds ratio vs. the risk ratio
1.0 (null)
Odds ratio
Risk ratio Risk ratio
Odds ratio
Odds ratio
Risk ratio Risk ratio
Odds ratio
Rare Outcome
Common Outcome
1.0 (null)

When is the OR is a good approximation of the RR?
General Rule of Thumb
“OR is a good approximation as long as the probability of the outcome in the unexposed is less than 10%”
Prevalence of age-related macular degeneration is about 6.5% in people over 40 in the US (according to a 2011 estimate). So, the OR is a reasonable approximation of the RR.

Case-control studiesAdvantages/Limitations:
• Advantages– Cheap and fast– Efficient for rare diseases
• Disadvantages– Getting comparable controls is often tricky– Temporality is a problem (did risk factor cause disease or
disease cause risk factor?– Recall bias

Nested case-control studies
A case-control study nested within a cohort study
Ideal for predictor variables that are expensive to measure and that can be assessed at the end of the study on subjects who develop the outcome during the study (cases) and on a sample of those who do not (controls)
Because the number of cases is probably fairly small, can match multiple controls to a given case to increase the power.

Why use a nested case-control study?
Removes recall bias because data collected before development of disease.
Allows for the time element to be included in the case- control. Therefore, if abnormal biologic characteristics were found years before the disease developed, these findings could now be attributed to risk factors for the disease rather than potential developments of early, subclinical disease. Often more cost-effective than a cohort. Not all samples
collected are tested. Rather they are stored until the disease has developed at which time analysis begins.

Table Size Test or measures of association
2x2 Risk ratio (cohort or cross-sectional studies)Odds ratio (case-control studies)Chi-squareDifference in proportionsFisher’s Exact test (cell size less than 5)
RxC Chi-squareFisher’s Exact test (expected cell size >5)
Summary of statistical tests for contingency tables

THANK YOU