Embed Size (px)
Citation preview

1
Methodist Hospital
Alcohol Withdrawal
Suggested Guidelines
S. Prizada Sattar, MD Teri L Gabel, Pharm.D.,BCPP
Sidney Kauzlarich, MD Subhash Bhatia, MD Mitzi Bollinger, RN
S. Prizada Sattar, MD 6-20-13
Rationale for the Suggested
Alcohol Withdrawal Scale and
Guidelines CIWA-AR
Developed by tested by experts in the treatment of alcohol withdrawal in detoxification units
Highly subjective scale
Time consuming
Alcohol Withdrawal Scale and Protocol Hybrid of the UNMC and CU Alcohol Withdrawal Scales and
Protocols
Other established and tested Alcohol Withdrawal Scales Australian Department of Veteran Affairs AWS
MINDS (Minnesota Detoxification Scale)
SAWS (Short Alcohol Withdrawal Scale) – Australian
Windsor Clinic Alcohol Withdrawal Scale – UK
Alcohol Withdrawal Scale - Wetterling et. al. 1997 and 2006
Adult Alcohol Withdrawal Scale – Stanley et.al. 2003, 2005, 2006
Purpose of the AWGs
Simplify Simple straight forward approach to treating alcohol
withdrawal
Unify Using the same process, minimizing confusion
Intensify Treat alcohol withdrawal sooner and more assertively
Prevent Prevent the onset of alcohol withdrawal and delirium
Treatment Comprehensive management of the patient in alcohol
withdrawal
Teri L Gabel, PharmD, BCPP 6-07
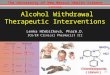
Time Course of Alcohol Withdrawal
Without Medication
Teri L Gabel, PharmD, BCPP 6-07
AW Symptom Onset
Symptoms Time to appearance
after last drink
Minor withdrawal symptoms: insomnia,
tremulousness, mild anxiety,
gastrointestinal upset, headache,
diaphoresis, palpitations, anorexia
6 – 12 hours
Alcoholic hallucinosis: visual, auditory, or
tactile hallucinations
12 – 24 hours *
Withdrawal seizures: generalized tonic-clonic
seizures
24 – 48 hours ¤
Alcohol withdrawal delirium (delirium tremens):
hallucinations (predominately visual),
disorientation, tachycardia, hypertension,
low-grade fever, agitation, diaphoresis
48 – 72 hours ¥
* Symptoms generally resolve in 48 hours
¤ Symptoms reported as early as two hours after last drink
¥ Symptoms peak in five days
Lorazepam
Teri L Gabel, PharmD, BCPP 6-07

2
Lorazepam Pharmacology
Acts at the level of the limbic, thalamic, and hypothalamic regions of the CNS, and can produce any level of CNS depression required including sedation, hypnosis, skeletal muscle relaxation, anticonvulsant activity, and coma
Lorazepam potentiates gamma-amino butyric acid (GABA)
Shorter elimination half-life than diazepam BUT it persists longer in the CNS
Teri L Gabel, PharmD, BCPP 6-07
Lorazepam Pharmacokinetics Absorption
Rapidly absorbed, onset of effect: 20-30 minutes (PO)
Bioavailability 90-93% (PO), 83-100% (IM), 100% (IV)
Distribution Protein Binding
70-90% (can see decreased binding in cirrhosis, chronic alcohol use, and renal insufficiency), Enterohepatic circulation, Brain concentration is approximately equal to the concentration of free drug in the plasma
3 Department Distribution Kinetics 1st distributes rapidly from the central compartment (blood stream) to the shallow peripheral compartment (brain) and then slowly from there to the deeper peripheral compartment (body fat).
Elimination Half-life: 6-12 hours
5 half-lives to steady state Teri L Gabel, PharmD, BCPP 6-07
Lorazepam Metabolism
www.occ-doc.net Teri L Gabel, PharmD, BCPP 6-07
Benzodiazepines
Side Effects
Sedation, dizziness, ataxia, confusion,
amnestic effects
Disinhibition
Delirium
Withdrawal
Activation: anxiety, tremor, agitation
Paresthesias: sensitivity to sound, light, touch
Seizures
Teri L Gabel, PharmD, BCPP 6-07
Alcohol Withdrawal Scale Scores 0 1 2 3
BP* Systolic < 140
Diastolic < 90
Systolic > 140-175
Diastolic > 90-100
Systolic > 175-200
Diastolic > 100-110
Systolic > 200
Diastolic > 110
Temperature < 99.1 F 99.1-100 F 100-101 F > 101.1 F
Pulse < 90 bpm 90-100 bpm 100-110 bpm >120 bpm
Sweating NONE Mild, Barely visible Moderate Marked, Betting and
Clothes are wet
Tremor NONE Felt/Not visible Mild Moderate/Visible
N/V NONE Upset stomach/nausea Vomiting Severe Vomiting /
Dry heaves
Agitation NONE Increased activity,
above normal
Restless, Fidgety Restless, pacing or
thrashing in bed
Hallucinations NONE Mild – no bother Moderate –
Bothersome
Marked, frightening,
overwhelming**
Sleeplessness NONE Inability to fall asleep
or remain asleep
for 2 hours
Unable to sleep after 4
hours
Not Applicable
* Use higher of the BPs (sBP or dBP) to score this item. ** Use of adjunct Antipsychotic medication recommended
Scoring the AWS Symptoms / Scores 0 1 2 3 Item Score
Patient BP
BP SBP < 140
DBP < 90
SBP > 140-175
DBP > 90-100 SBP > 175-200 DBP > 100-110
SBP > 200
DBP > 110 2
Patient Temp
Temperature < 99.1 F 99.1-100 F 100-101 F > 101.1 F 1
Patient Pulse
Pulse < 90 bpm 90-100 bpm 100-110 bpm >120 bpm 2
Sweating NONE Mild, Barely
visible
Moderate Marked, Betting
and Clothes
are wet
1
Tremor NONE Felt/Not visible Mild Moderate
Visible 1
N/V NONE Upset stomach /
nausea
Vomiting Severe Vomiting /
Dry heaves 1
Agitation NONE Increased activity,
above normal
Restless, Fidgety Restless, pacing or
thrashing in bed 1
Hallucinations NONE Mild – no bother Moderate –
Bothersome
Marked,
frightening
overwhelming*
0
Sleeplessness NONE Inability to fall asleep
or remain asleep for
2 hours
Unable to sleep after 4
hours
Not Applicable 0
Total
Score 9

3
In the Urgent Care Area
□ Initial NOW Dose: Lorazepam 2 mg PO/IM
Given IF the patient: Is NOT acutely intoxicated, e.g. no nystagmus or cerebellar ataxia Has elevated vital signs (BP >140/90 AND/OR pulse is >90bpm) BAL does NOT need to be zero to give lorazepam Is demonstrating signs and symptoms of alcohol withdrawal:
tremulousness, diaphoresis, confusion, irritability Has a known history of severe alcohol withdrawal Has a known history of alcohol withdrawal seizures Has a significant drop in Blood Alcohol Level
NOT given IF the patient: Is acutely intoxicated, e.g. presence of somnolence, nystagmus or
cerebellar ataxia
Teri L Gabel, PharmD, BCPP 6-07
In The ER Area
□ Repeat Dose: Lorazepam 2 mg PO/IM – in two hours If patient is still waiting for transfer
Previous parameters still apply
□ Initiate Alcohol Withdrawal Detoxification Guidelines Consider if patient will be in the ER for a
prolonged period of time
□ Thiamine 100mg PO/IM/IV X 1 PRIOR TO GIVING ANY IV GLUCOSE or Food
Teri L Gabel, PharmD, BCPP 6-07
On the Unit □ Initiate Alcohol Withdrawal Detoxification
Guidelines
If not already initiated in ER
□ Seizure Precautions
Vital Signs
□ Baseline
□ Q __ hour while awake
□ Other VS order
Teri L Gabel, PharmD, BCPP 6-07
On The Unit Standing Medications
□ Thiamine 100mg IM/IV X 1 (PRIOR TO GIVING
ANY IV GLUCOSE or Food), then 100mg PO for 1-4
days
□ Folic acid 1mg daily
□ Multivitamin/Minerals one daily
□ Magnesium Oxide 400mg BID or 1gram IM/IV once
(if magnesium levels are <1.5mg/dl)
□ Nicotine patch _____ (7mg, 14mg, or 21mg) – daily
to prevent nicotine withdrawal/craving
□ Any patient specific medications
Teri L Gabel, PharmD, BCPP 6-07
On the Unit
PRN Medications
□ Phenergan 25mg PO/IM every 4 hours PRN
nausea
□ Antacid 30mg PO every 4 hours PRN GI upset
□ Ibuprofen 600mg PO Q 4 hours PRN headache
□ Clonidine 0.1mg TID PRN for autonomic
hyperactivity
Other PRNS: Ranitidine, omeprazole, …
Teri L Gabel, PharmD, BCPP 6-07
On the Unit
Antipsychotic Medications – adjunct to lorazepam * For tactile, visual, auditory disturbances /
hallucinations, delusions, combativeness, and/or delirium interfering with medical care and safety and is unrelated to persistent elevation in BP, pulse, or persistent w/d tremors, diaphoresis.
□ Risperidone 1mg PO every 4 hours PRN
□ Haloperidol 2mg IV/IM every 4 hours PRN (when unable to take PO risperidone)
Please monitor for EPSEs.
□ Benztropine mesylate 1mg PO/IM PRN EPSE
No Olanzapine – interaction with lorazepam, and much higher lowering of seizure threshold
Teri L Gabel, PharmD, BCPP 6-07

4
AWS Based Lorazepam Dosing
□ Medication doses are to be HELD if patient is sedated or asleep.
□ Do not awaken a patient to perform the AWS or give them medication.
□ Use oral lorazepam when the patient is able to take oral medications
Lorazepam dose NOT TO EXCEED 24mg in 12 hours without a physician evaluation and order.
Maximum IV push rate: 2mg per minute This is not a dosing interval
□ IF AWS = 0 No medication is given
Teri L Gabel, PharmD, BCPP 6-07
AWS Based Lorazepam Dosing
Mild Alcohol Withdrawal
□ AWS checked every 6 hours for 24 hours
AWS < 5 AND VS <140/90 and pulse <99
□ Lorazepam 1mg PO every 6 hours PRN until patient is asymptomatic
Once consecutive assessments are < 5 over 24hours, discontinue AWS and medications
Teri L Gabel, PharmD, BCPP 6-07
AWS Based Lorazepam Dosing
Moderate Alcohol Withdrawal
□ AWS and VS checked every 2 hours
□ AWS < 5 BUT BP 140/90-175/100 AND/OR pulse is 100-110 bpm
OR
□ AWS 6-10 AND/OR BP 140/90-175/100 AND/OR pulse is 100-110bpm
□ Lorazepam 2mg PO/IM/IV every 2 hours
Once AWS < 6 OR VS have normalized, shift to Mild Alcohol Withdrawal dosing
Taper lorazepam when ready to DC
Teri L Gabel, PharmD, BCPP 6-07
AWS Based Lorazepam Dosing
Severe Alcohol Withdrawal
□ AWS and VS checked every 1 hour
□ AWS >10 AND/OR BP > 200/110 AND/OR Pulse > 120 bpm
□ Lorazepam 2mg PO/IM/IV every 1 hour
AWS < 10 AND/OR VS have normalized, then drop to mild or moderate alcohol dosing guidelines as indicated
AWS < 5 OR VS have normalized, drop to mild alcohol dosing guidelines
Taper lorazepam when ready to DC
Teri L Gabel, PharmD, BCPP 6-07
Flumazenil *REQUIRED If benzodiazepine is given IM or IV.
In case of over sedation with benzodiazepine:
□ Flumazenil 0.2 mg IV over 15 seconds then 0.2mg IV over 15 seconds if first dose ineffective after 45 seconds. An additional three doses may be given at 60 second intervals to a maximum total of 1mg. After the first 1mg, repeated doses may be given at 20-minute intervals if needed; For repeat treatment, no more than 1 mg (given as 0.5 mg/min) should be given at any one time and no more than 3 mg should be given in any one hour
*Monitor for desired level of consciousness and to prevent triggering alcohol withdrawal seizures
Teri L Gabel, PharmD, BCPP 6-07
Propylene Glycol Toxicity
Occurs with excessive use of IV
lorazepam
Symptoms of Propylene Glycol Toxicity
Unexplained anion gap, metabolic acidosis,
hyperosmolality, hemolysis, cardiac
arrhythmias, seizure, clinical deterioration,
coma
Teri L Gabel, PharmD, BCPP 6-07

5
AWS Guideline Fine Points Additional lorazepam doses beyond protocol - may
be given as NOW doses on physician electronic, written or verbal order only.
Multiple NOW orders should not be given simultaneously.
Set orders for PRN benzodiazepines are not allowed. Except as indicated in the guidelines.
Pharmacy will no longer honor orders for ranges of benzodiazepine doses.
Cases in which lorazepam doses vary from the established protocol will be evaluated.
Consider the judicious use of other PRN medications for specific symptoms not responding to lorazepam (clonidine, antipsychotics)
Teri L Gabel, PharmD, BCPP 6-07
Sample AWS Order
□ Seizure precautions
□ AWS and VS to be checked every 1
hour until AWS <10 then every 2 hours
until AWS < 6 then every 6 hours. Once
consecutive assessments are < 5 over
24hours, discontinue AWS and taper
medication.
□ Do not awaken patient for AWS or to
give medication.
Teri L Gabel, PharmD, BCPP 6-07
Sample AW Order
□ AWS = 0 = NO lorazepam is given
□ Lorazepam 1mg PO every 6 hours PRN AWS < 5 AND VS <140/90 and pulse <99
□ Lorazepam 2mg PO/IM/IV every 2 hours PRN AWS < 5 BUT BP 140/90-175/100 AND/OR pulse is 100-110 bpm OR AWS 6-10 AND/OR BP 140/90-175/100 AND/OR pulse is 100-110bpm
□ Lorazepam 2mg PO/IM/IV every 1 hour PRN NWI AWS >10 AND/OR BP > 200/110 AND/OR Pulse > 120 bpm
□ Flumazenil on unit
Teri L Gabel, PharmD, BCPP 6-07
Sample Lorazepam Tapers
A. If patient received <24mg/day
• Lorazepam 2mg every 6 hours x 24 hours
Lorazepam 2mg every 8 hours x 24 hours
Lorazepam 1mg every 8 hours x 24 hours,
then DC
B. If patient received >24mg/day
• Lorazepam 2mg every 4 hours x 24 hours
Lorazepam 2mg every 6 hours x 24 hours
Lorazepam 2mg every 8 hours x 24 hours
Lorazepam 1mg every 8 hours, then DC
Teri L Gabel, PharmD, BCPP 6-07
AW Fine Points
It is expected that patients will have some brief
periods of psychomotor agitation while in alcohol
withdrawal. No medication is required for these
brief episodes, instead, reassure the patient
verbally, decrease environmental stimuli, and
use soft restraints when appropriate.
Goal of medication is to PREVENT the onset of
withdrawal and to keep the patient calm or lightly
sedated patient, easily aroused but falls back to
sleep if left alone.
Teri L Gabel, PharmD, BCPP 6-07