Embed Size (px)
DESCRIPTION
Nutritional Problems. Lewis, S., Dirksen, S., Heitkemper,M., Bucher, L. & Camera,I.(2011). Medical Surgical NursinG. St Louis, MO:Mosby. Learning Objectives. Explain the essential components of a nutritionally good diet and their importance to health maintenance. - PowerPoint PPT Presentation
Citation preview
LEWIS, S., DIRKSEN, S., HEITKEMPER,M., BUCHER, L. & CAMERA,I.(2011). MEDICAL SURGICAL
NURSING. ST LOUIS, MO:MOSBY
Nutritional Problems
Learning Objectives
Explain the essential components of a nutritionally good diet and their importance to health maintenance.
Describe and analyze the common etiologic factors, clinical manifestations, and nursing and collaborative management of malnutrition.
Explain the indications for use, complications, and nursing management of enteral nutrition.
Identify the types of feeding tubes and related nursing management, inclusive of collaborative care. Define and evaluate using the clinical reasoning process the indications, complications, and nursing management related to parenteral nutrition.
Compare and analyze the etiologic factors, clinical manifestations,
and nursing management of eating disorders.
Nutrition- Carbohydrates
The process by which the body uses food for energy, growth, and maintenance of body tissues
Essential components: carbohydrates, fats, proteins, vitamins, and minerals
Average adult needs 20-35 calories per kilogram of weight/day
Carbohydrates = primary energy source: 45-60% of total caloric intake: protein sparing ingredient
SIMPLE Monosacharides = glucose and fructose [honey & fruit] Disacharides = complex; sucrose, maltose, lactose [sugar & milk]COMPLEX : starches [cereal, potatoes, legumes]
Carbohydrate
Carbohydrates
14 grams of dietary fiber from fruits, vegetables, and whole grains per 1000 calories/day
Healthy bowels and prevents constipationChoose food with little or no added sugar or
caloric sweeteners
Nutrition - Fats
Fats- 1 gram = 9 caloriesStored in the adipose tissue of the abdominal
cavityMajor source of energyAct as insulation, reduces body heat lossPadding and protection for vital organs in
abdomenCarriers of essential fatty acids and fat soluble
vitaminsSlow digestion = satiety; delays hunger36% of daily caloric intake in America= CONCERN
Should be 20 to less than 35%
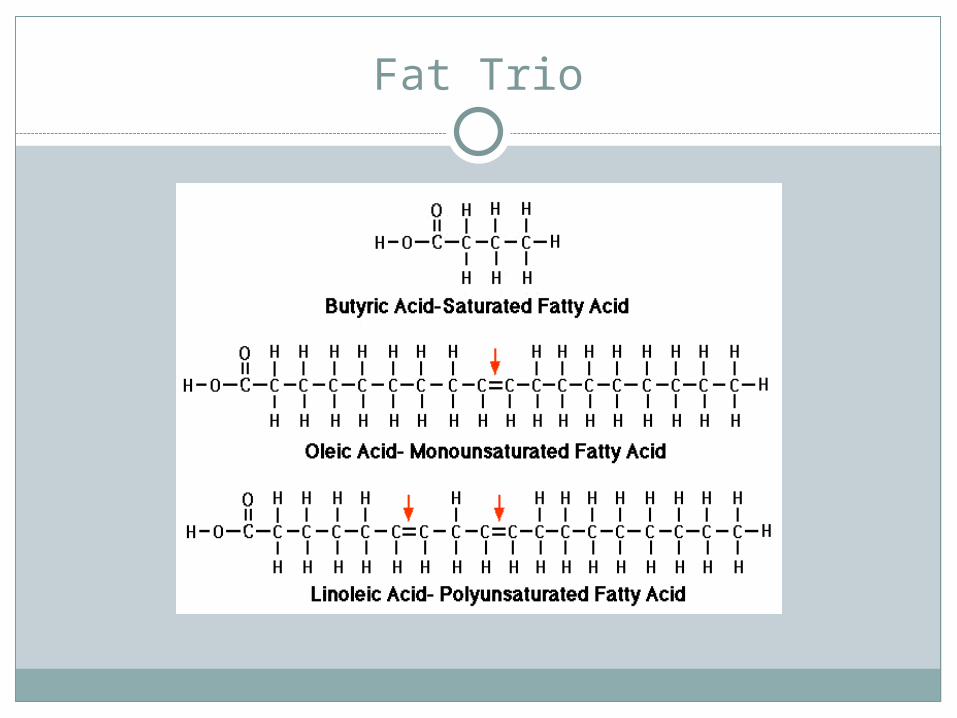
Fat Trio
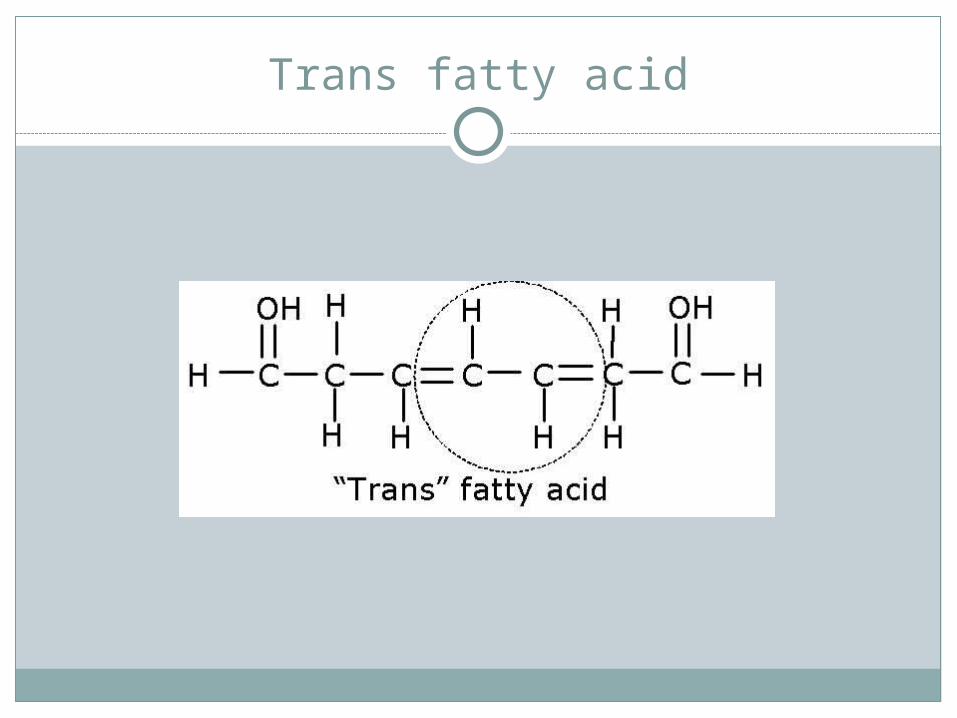
Trans fatty acid
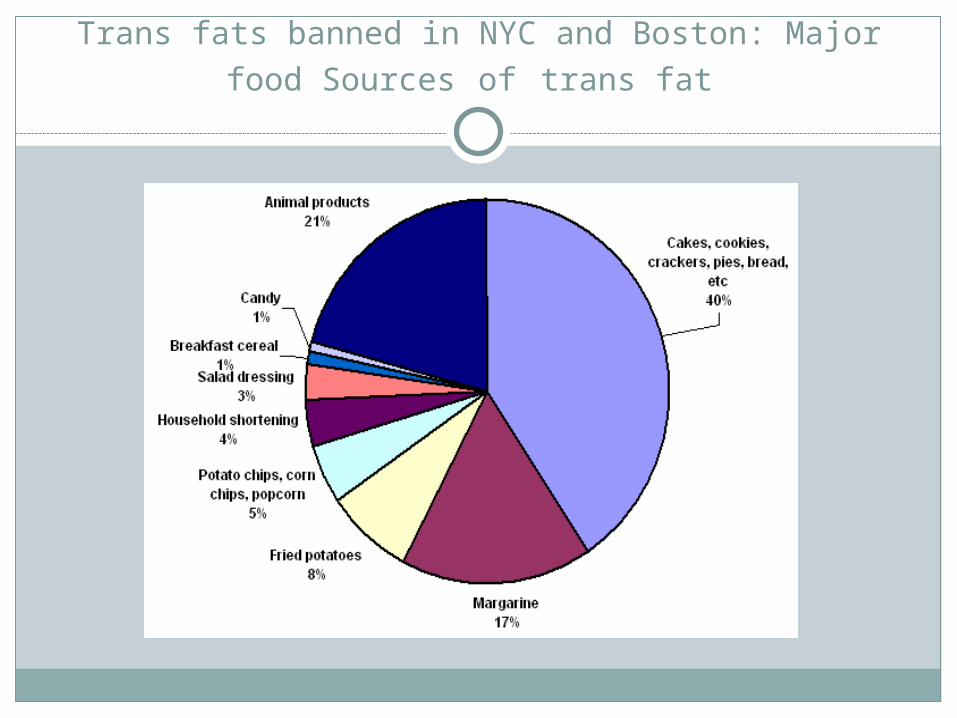
Trans fats banned in NYC and Boston: Major food Sources of trans fat
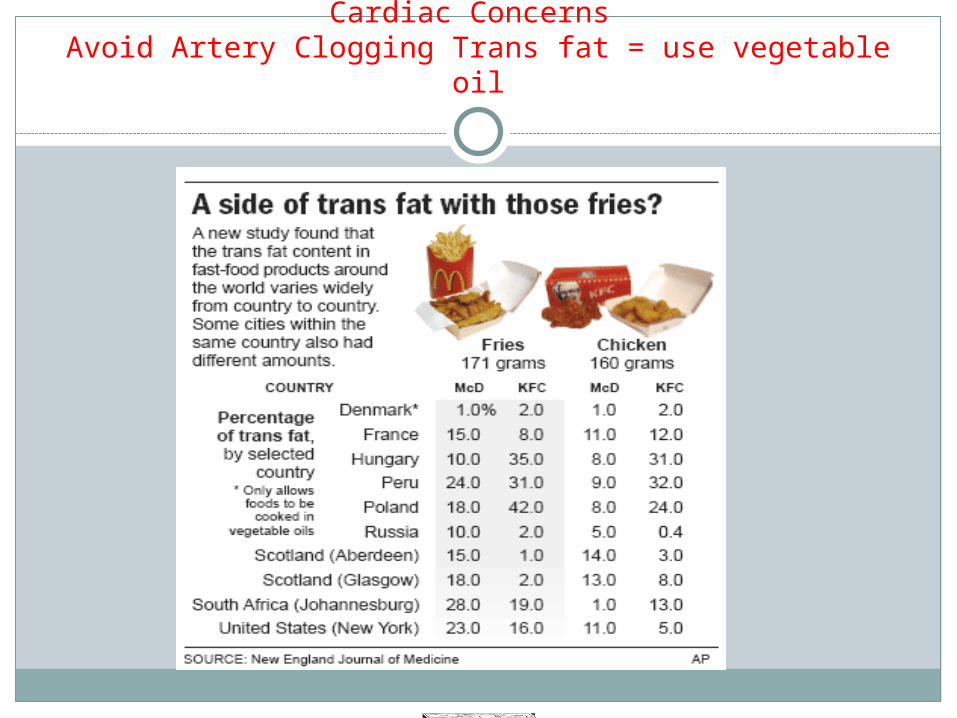
Cardiac Concerns Avoid Artery Clogging Trans fat = use vegetable oil
Trans fat and nursing education!
Trans fats
Nutrition - Proteins
Average adult needs = 20-35 calories per kilogram/day
Proteins should provide 15 -20% of caloric intakeProteins = tissue, body regulatory function, energyProteins are complex nitrogenous organic compounds:Amino acids are the fundamental unit of structure22 amino acids: 9 essential complete proteins
Availability depends on diet aloneand non-essential/incomplete proteins
Complete ProteinsComplete Proteins Incomplete ProteinsIncomplete Proteins
Milk and milk products
EggsFishMeatspoultry
GrainsLegumesNutsseeds
Protein Sources
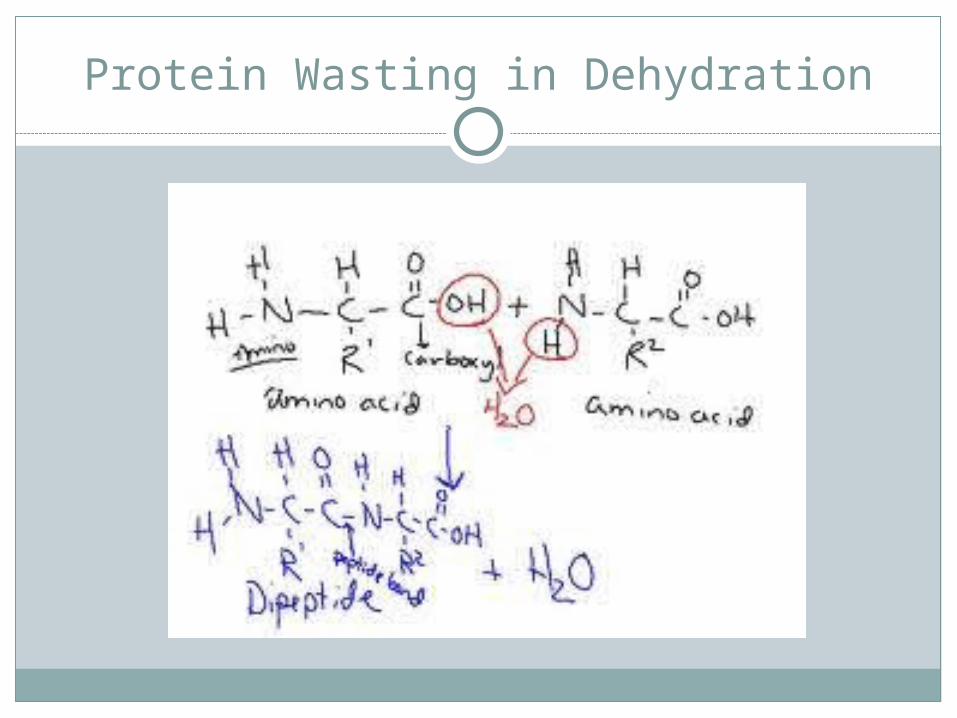
Protein Wasting in Dehydration
Vitamins
Organic compounds required in small amounts for metabolism
Catalysts for enzyme reactions that facilitate metabolism of carbohydrates, fats, and proteins
Two categories = fat or water solubleFat soluble: A, D, E, KWater soluble: B1, B6, Cobalamin B12, C,
Folate (folic acid)
Major MineralsMajor Minerals Trace ElementsTrace Elements
CalciumChlorideMagnesiumPhosphorusPotassiumSodiumsulfur
ChromiumCopper FluorideIodine [fish/shellfish]ManganeseMolybdenum-
chocolateSeleniumzinc
Major Minerals and Trace Elements
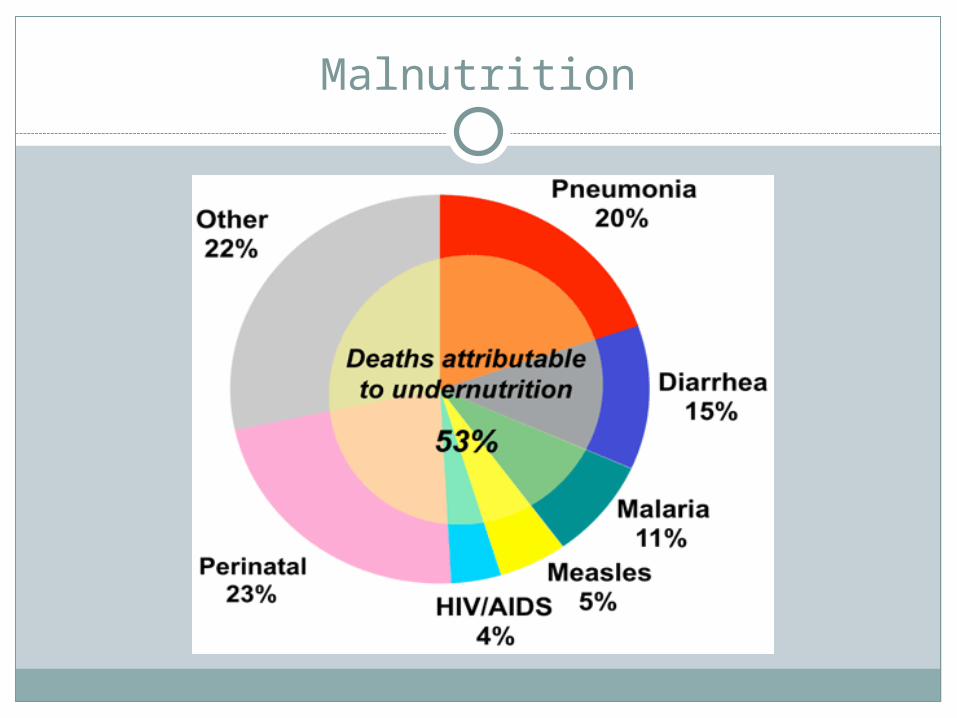
Malnutrition
Conditions that increase the risk for malnutrition
Dementia, depressionSocioeconomic factors- food insecurityChronic alcoholismExcessive dieting to lose weight, eating disordersSwallowing disordersDecreased ability to do ADLs, decreased mobilitydrugs: corticosteroids, antibioticsStressors: burns, trauma, fever, woundsNo oral intake or IV solutions for 10 days- 5 days
geriMalabsorption syndrome
Types of Malnutrition
Protein-calorie: most common formMarasmus: generalized loss of body fat and
muscle from protein and carbohydrate deficiency
Kwashiorkor: stress [GI obstruction, surgery, cancer, malabsorption, infectious disease] and protein deficiency S/S appear well nourished = low serum protein
levels
Malnutrition Lab value: prealbumin levels drop – normal = 20 low < 5
Starvation
97% of calories are from fat and protein is conserved
Fat stores used up in 4 – 6 weeksBody proteins in internal organs and plasma
are used; then rapidly decrease Causes liver dysfunction and loss of liver mass Causes shift in body fluids from the vascular fluid to the
interstitial spaces = edema in face and legs Skin appears dry and wrinkled Failure of the sodium potassium pump (20- 50% of all
ingested calories) as energy is needed / cells engorge Death will be rapid : CA patients on chemo Nursing measure; encourage eating!
FeverIncreases need for calories
due to the increase in the bodies metabolic rate [BMR]
1 degree = raises BMR 7%!
Thus without an increase in calories = a significant problem
Monitor serum protein levels: prealbumin is best
ANOREXIA NERVOSAANOREXIA NERVOSA BULEMIA NERVOSABULEMIA NERVOSA
Self-imposed wt lossMiddle-upper
class/whiteDeliberate starvationFear of wt gains/s = Hair loss,
sensitivity to cold, dry skin, constipation, elevated BUN, low K, body wasting and malnutrion
Binge and purgeWhiteLaxative/drug/
exercise abuseAnxiety, affective
disorders, conceal problem
s/s = dental problems, broken blood vessels in eyes, macerated knuckles
Eating Disorders
Clinical Manifestations of malnutrition
Muscles wasted and flabbyWeaknessIrritability/ confusionFatigueDelayed recovery and wound healingIncreased susceptibility to infectionRisk increases for anemiaLab analysis:Low serum prealbumin and lymphocyte
countElevated potassium and liver enzymes
Nursing Management/ Malnutrition
Nutritional screening: to determine need for a more thorough nutrition assessment
BMI = weight[kg] x height [squared in m]Nursing Dx
Imbalanced nutrition Self –care deficit Constipation or diarrhea Fluid volume deficit Risk for impaired skin integrity Non-compliance Activity intolerance
Interventions to prevent malnutrition
A key intervention is daily weight/ same time q day
Daily calorie countFrequent small mealsOral nutrition supplementsEnteral nutrition [tube feeding]Parenteral nutrition [PN] - procalamineTotal parenteral nutrition [TPN]
fat emulsion, dextrose, amino acids
Refeeding Syndrome
Can occur any time a malnourished patient is started on aggressive nutritional support
s/s: fluid retention, electrolyte imbalancesHypophosphatemia is the hallmark s/s dysrhythmias, respiratory arrest,
neurologic disturbances
NCLEX Question
A client receiving chemotherapy is experiencing persistent nausea and occasional vomiting. Based on these symptoms, which interventions should the nurse add to this client’s plan of care?
1.Change the clients diet to full liquid2.Offer small amounts of food frequently*3.Administer 4 mg zofran IV 1h prior to chemo*4.Encourage liquid consumption throughout the
day*5.Serve a big meal prior to chemo6.Offer foods that are mild smelling or odorless*
Nutrition Assessment for supplemental feedings
Functional GI tract:Yes = enteral nutrition
Long term = gastrostomy or jejunostomy tube Short term = nasogastric tube
NO = parenteral nutrition (PN)Short term = peripheral (PN) – procalamineLong term = central PN (TPN) Note- always keep TPN refrigerated until
use. Change bag, line, and filter every 24 hNever connect another line into TPN!!!!!
Indications for Tube Feedings
Anorexia patientsOrofacial fracturesHead and neck CANeurological or psychological conditions that
prevent oral intakeExtensive burnsChemotherapyEnteral nutrition is Safer than parenteral
nutrition
Nasogastric Tubes
Small diameter, soft and flexibleRadiopaque to assess position with X-raySmaller than standard decompression NG tubeAssess for patency as easily clogged, flush
regularly, *flush following medication administration
Administer meds one at a time Crush and mix all meds with water/sterile water is best* Flush after checking residual
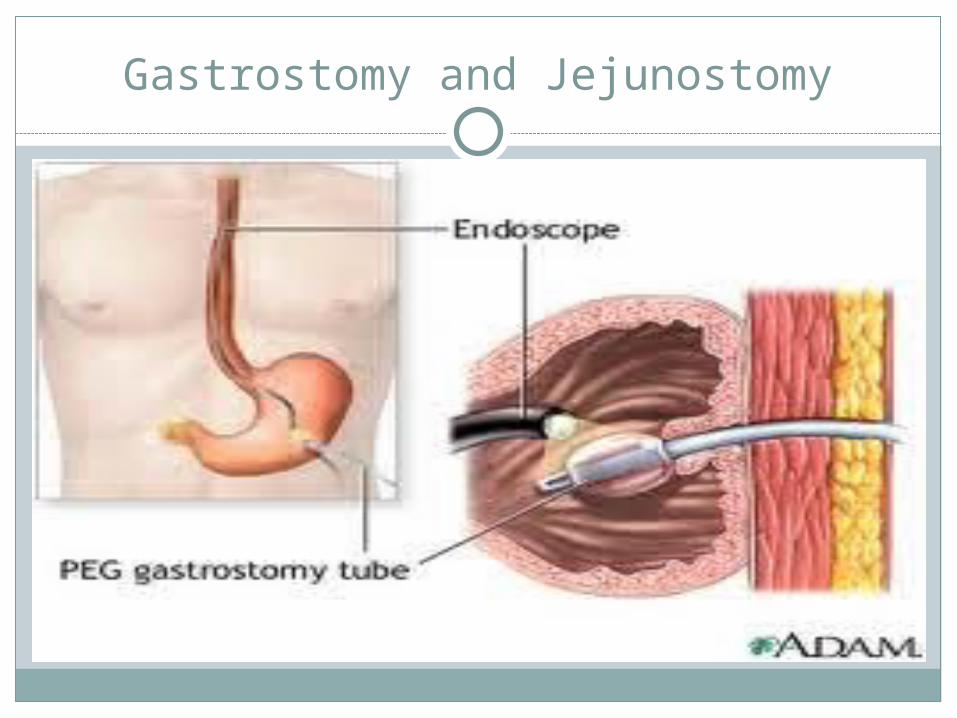
Gastrostomy and Jejunostomy

Long Term Enteral Nutrition
Percutaneous endoscopic gastrostomy (PEG)Always check placement before usingAssess for return of bowel sounds before
using- usually within 24 h of placement (water can be given within 2 h of placement)
Usually attached to a feeding pump for continuous feeding
Nursing Management of Feeding Tubes
Check placement before each feeding and medicationContinuous: start at a low rate and increase gradually for
24-48h to minimize side effectsAssess for bowel sounds before feeding. > or = 30ml
syringe Use liquid medications if possible/ crush pills thoroughly,
give one at a time, dissolve in H2O (sterile water is best)First stop enteral feeding - flush with 15ml prior to giving
medication and afterDilute viscous liquid medicationElevate HOB 30 – 45 degrees: and for 30- 60 min pDiscard feedings after 8 h. Change tubing q 24 hCheck residuals volumes and gastric emptying, flush p
check
Complications of Tube Feedings
Aspiration – too much feeding, too large a residual- delayed gastric emptying
Diarrhea- poor tolerance, too rapid, too cold (give at room temperature), fiber content too low
Abdominal distention – too much, too fast, or obstruction
Hyperglycemia – too high calorie for toleranceConstipation or impaction: to prevent - give water to
at regular intervalsDehydration: from diarrhea, vomiting, too little H2OResidual > 500 ml = hold next feeding for 1 h and
recheck; always reinstill aspirate ( if no other adverse s/s such as nausea, abdominal distention) and flush!
Nursing Diagnosis
Imbalanced nutrition less than body requirements related to . . .
Assess: weight/ height, Hct, muscle tone, food intake, hydration, bowel sounds, diarrhea, follow protocol
Collaborate with the dietician Risk for aspiration related to . . .Prevention: HOB elevated, check residuals, assess
tube placement, leave HOB elevated for 30-60 min p feeding
Assess for sensation of fullness, nausea, vomiting because these are signs of gastric retention
Nursing Diagnosis
Risk for aspirationCheck residual q4-6h for first 24h, then q 8 hoursHold tube feedings if residual is > 500 and
reassessElevate HOB 30-45 degrees during feedings and 30-60 min after feedingsAssess for gastric retention symptoms: sensation
of fullness, nausea, vomitingDiscontinue feedings 30-60 min before laying
patient supine
Gerontologic Considerations
More vulnerable to complications:More vulnerable to fluid and electrolyte
imbalancesDecreased perception of thirst Impaired cognition; ability to manage home careMore susceptible to hyperglycemiaMore susceptible to fluid overload due to poor
cardiac (CHF) or decreased renal functionDecreased ability to tolerate large fluid volumes
of feedingsIncreased risk for aspiration
Indications for Parenteral Nutrition
Chronic severe diarrhea or vomiting
Complicated surgery or trauma
GI obstructionGI anomalies or fistulasIntractable diarrheaSevere anorexia nervosaSevere malabsorptionShort bowel syndrome
Peripheral Parenteral Nutrition (PPN)
IV with large veinProcalamine: protein and caloriesShort term therapy nutritional supportTends to easily burn vein (vesicant) = assess
vein for redness, pain, irritation, and thrombophlebitis
Can cause fluid overload Monitor for jugular vein distention, elevated B/P,
crackles during lung auscultation, SOB
Total Parenteral Nutrition (TPN)
Hypertonic solution (vesicant) = glucose, crystalline amino acids, fat emulsion, minerals, vitamins
Adjusted per individual by MD every dayContains, Na, K, Cl, Mg, Ca, Phosphate and trace
elements as per pt needsOnly administered through a central line or PICC If need to wait for another bag of solution use 5-
10% dextrose IVNever D/C suddenly; taperMonitor blood glucose q 6h
Complications of Parenteral Nutrition
Risk for Infection: fungus, gram pos and neg bacteriaMetabolic problems: hyperglycemia, hypoglycemia, prerenal azotemia
(presence of nitrogen, urea, in the blood), essential fatty acid deficiency
electrolyte imbalances, mineral deficiencies, hyperlipidemia
= why TPN is reformulated every day by MDMechanical problems: During insertion = air embolus, pneumothorax,
hemorrhage Dislodgement Thrombus of vein Phlebitis
Catheter Related Infection
Assess site for : erythema, tenderness, exudate
Assess systemic: fever, chills, nausea, vomiting, malaise
Patient has s/s =Culture blood and tip of catheter: 2 blood
cultures - from catheter and peripherallyChest X-ray to detect change in pulmonary
statusAntibiotics if indicated
Nursing Diagnosis
Risk for infection related to central line placement . .
monitor for s/s of infection, assess and document site findings q 4-8h
Infection severity: fever, malaise, blood culture colonization, wound/ feeding culture colonization, WBC elevation (cancer patients may be difficult to assess due to poor immune response/low WBCs)
Infection control: maintain an aseptic environment: sterile dressing changes, change tubing and filter q 24h
Check lab values for s/s of infection: high WBC and increased neutrophil count
Nursing management of parenteral nutrition: Review
Assess VS q 4-8h and siteDaily weightKeep refrigerated until use- never add other
solutions to lineChange line, filter, and solution q 24hMake sure MD writes script for next dayIf not available hang 10% dextroseBS check q 6hMonitor for S/S of infection of site and of line (CA
pts)labs: glucose, electrolytes, urea nitrogen, CBC,
hepatic enzyme studies





























