Embed Size (px)
Citation preview

1
NURSING DOCUMENTATION
OBJECTIVES 1. The learner will be able to state 2
components of documentation that meet the ‘Standard of Care’
2. The learner will be able to identify 4 characteristics of a ‘complete skin assessment’
3. The learner will be able to identify 4 characteristics of a ‘complete wound assessment’
DOCUMENTATION IS…
Ø Something you learn in nursing school Ø Something you do everyday at work Ø How you record patient vitals, diet, meds…
THE permanent record of nursing assessment and care provided…
2
DOCUMENTATION
Ø ‘any written or electronically
generated information about a patient that describes the care or services provided to that patient’
SOME EXAMPLES…
‘Skin intact, red, and broken’ ‘The skin was moist and dry’ ‘Pulses are probably in both
feet’

3
‘Examination of genitalia reveals that he is circus-sized’
‘300cc PWISOTF’ (Plus what I spilled on the floor)
‘Patient found dead: felt cold,
blanket added, voiced no
complaints’
4
‘She has no rigors or shaking chills, but her husband states she was very hot in bed last night’
‘Large brown stool ambulating in the hall’
Documentation is the process of recording the patient assessment
and the care provided
It MUST demonstrate that the ‘Standard of Care’ has been met
5
STANDARD OF CARE
What is it and who decides?
STANDARD OF CARE Ø Guidelines used to determine what a nurse
should or should not do Ø Model of established practice that is
commonly accepted as correct Ø Basis for nursing care that draws on the
latest scientific data from nursing literature Ø Based on the premise that the registered
nurse is responsible for and accountable to the individual patient for the quality of nursing care he or she receives
STANDARD OF CARE The nurse has a professional responsibility,
and is held accountable to document patient data that accurately reflects:
Ø Nursing assessment Ø Plan of care Ø Appropriate interventions Ø Evaluation of the patient’s condition Standard of Care
ü Nursing Assess ü Plan of Care ü Interventions ü Eval / Re-Eval
6
STANDARD OF CARE Developed and implemented to define the ‘quality
of care provided’
Ø Federal / State laws, rules and regulations Ø Professional organizations establish norms for
the average practitioner Ø The ANA and Joint Commission on Accreditation
of Healthcare Organizations (JCAHO) have established nationally recognized ‘Standards of Care’
POLICY AND PROCEDURE
In addition- Ø Nurses must understand and
follow the policies and procedural guidelines of their individual facilities
LEGAL CONSIDERATIONS The healthcare industry can be a minefield of
litigation when patients Ø Don’t heal as expected Ø Develop unexpected complications or
infections which can lead to prolonged recovery or even death
Lawsuits often involve all those who cared for the patient, including the nurse
7
WOUND LITIGATION ON THE RISE
Ø Increasing elderly population Ø Regulatory climate Ø Misunderstanding by families as to the
cause of wounds Ø Perceived as ‘bad care’
Ø Public opinion that wound cases are an ‘easy target’
LEGAL CONSIDERATION
Ø Nursing documentation Ø often starting point in malpractice cases Ø can either deter a plaintiff from filing a lawsuit or
provide the leverage that is required to initiate one
Jurors and attorneys view what is written in
the patient record as the best evidence of what really occurred
PRESSURE ULCERS
The incidence of Hospital acquired pressure ulcers (HAPUs) is considered a ‘quality indicator’ of patient care
Ø ‘Quality care should not result in a HAPU’ Ø A ‘Never Event’ Ø High public awareness Ø Frequent involvement in litigation Ø Reimbursement issues

8
The reality is that not all pressure ulcers are
preventable…. The nurse MUST be able to show that all
appropriate assessments and interventions were done….
…That the ‘Standard of Care’ was met
DOCUMENTATION THAT MEETS THE STANDARD OF CARE
Ø Timely Ø Accurate Ø Comprehensive Ø Complete
Characteristics ü Timely ü Accurate ü Comprehensive ü Complete
Standard of Care ü Nursing Assess ü Plan of Care ü Interventions ü Eval / Re-Eval
DOCUMENTATION THAT MEETS THE STANDARD OF CARE
ASSESSMENT, ASSESSMENT, ASSESSMENT…..
ü SKIN ASSESSMENT ü WOUND ASSESSMENT ü RISK ASSESSMENT
Standard of Care ü Nursing Assess ü Plan of Care ü Interventions ü Eval / Re-Eval
Characteristics ü Timely ü Accurate ü Comprehensive ü Complete

9
SKIN ASSESSMENT
1. TIMELY ü ON ADMISSION ü EVERY SHIFT OR VISIT ü FOLLOW FACILITY POLICY
Characteristics ü Timely ü Accurate ü Comprehensive ü Complete
Standard of Care ü Nursing Assess ü Plan of Care ü Interventions ü Eval / Re-Eval
SKIN ASSESSMENT 2. ACCURATE / COMPREHENSIVE /
COMPLETE ü INTEGRITY- Alteration in Epidermis or Dermis ü COLOR- Erythema, Pallor, Cyanosis… ü TURGOR- Dehydration … ü MOISTURE STATUS- ü TEMPERATURE- ü HIGH RISK AREAS-
Characteristics ü Timely ü Accurate ü Comprehensive ü Complete
Standard of Care ü Nursing Assess ü Plan of Care ü Interventions ü Eval / Re-Eval
SKIN ASSESSMENT
DOCUMENT AND REPORT ABNORMALITIES
Characteristics ü Timely ü Accurate ü Comprehensive ü Complete
Standard of Care ü Nursing Assess ü Plan of Care ü Interventions ü Eval / Re-Eval

10
WOUND ASSESSMENT 1. TIMELY
ü ON ADMISSION ü EVERY SHIFT OR VISIT ü UPON TRANSFER / DISCHARGE ü PER FACILITY POLICY
Characteristics ü Timely ü Accurate ü Comprehensive ü Complete
Standard of Care ü Nursing Assess ü Plan of Care ü Interventions ü Eval / Re-Eval
WOUND ASSESSMENT 2. ACCURATE / COMPREHENSIVE /
COMPLETE ü Wound Type ü Location ü Measurement ü Undermining / Tunneling ü Wound Bed Appearance ü Drainage ü Odor ü Surrounding Skin
Characteristics ü Timely ü Accurate ü Comprehensive ü Complete
Standard of Care ü Nursing Assess ü Plan of Care ü Interventions ü Eval / Re-Eval
WOUND DOCUMENTATION Paints the picture & tells the story
SURROUNDING SKIN
ODOR
DRAINAGE
APPEARANCE
UNDERMINING TUNNELING
MEASUREMENT
LOCATION
WOUND TYPE
WOUND
Characteristics ü Timely ü Accurate ü Comprehensive ü Complete

11
WOUND TYPE FOR PRESSURE ULCERS: Ø If you know how to stage it-Do it! Ø If you are uncertain-Describe it!
SACRAL AREA
COCCYX
TROCHANTER ILIAC CREST
GLUTEAL FOLD ISCHUIM
LOCATION, LOCATION
Correctly identify wound location
Sacrum Coccyx
MEASUREMENT
LENGTH X WIDTH X DEPTH
Longest point Head to toe direction
90 degree angle Deepest point
Perpendicular to length Widest point
Document on Admission and per facility policy

12
UNDERMINING / TUNNELING
UNDERMINING TUNNELING
Document with measurement
APPEARANCE
GRANULATION TISSUE SLOUGH ESCHAR
Document tissue type or describe color
DRAINAGE
How much and what does it look like?
13
ODOR
Document presence of…
SURROUNDING SKIN
Document condition of skin surrounding wound
REALITY
Audits are enlightening… Ø Wrong location Ø Wrong wound type Ø Wrong pressure ulcer stage
Ø Ever changing pressure ulcer stage… Ø Missing assessment data Ø Inconsistencies from shift to shift
and day to day
14
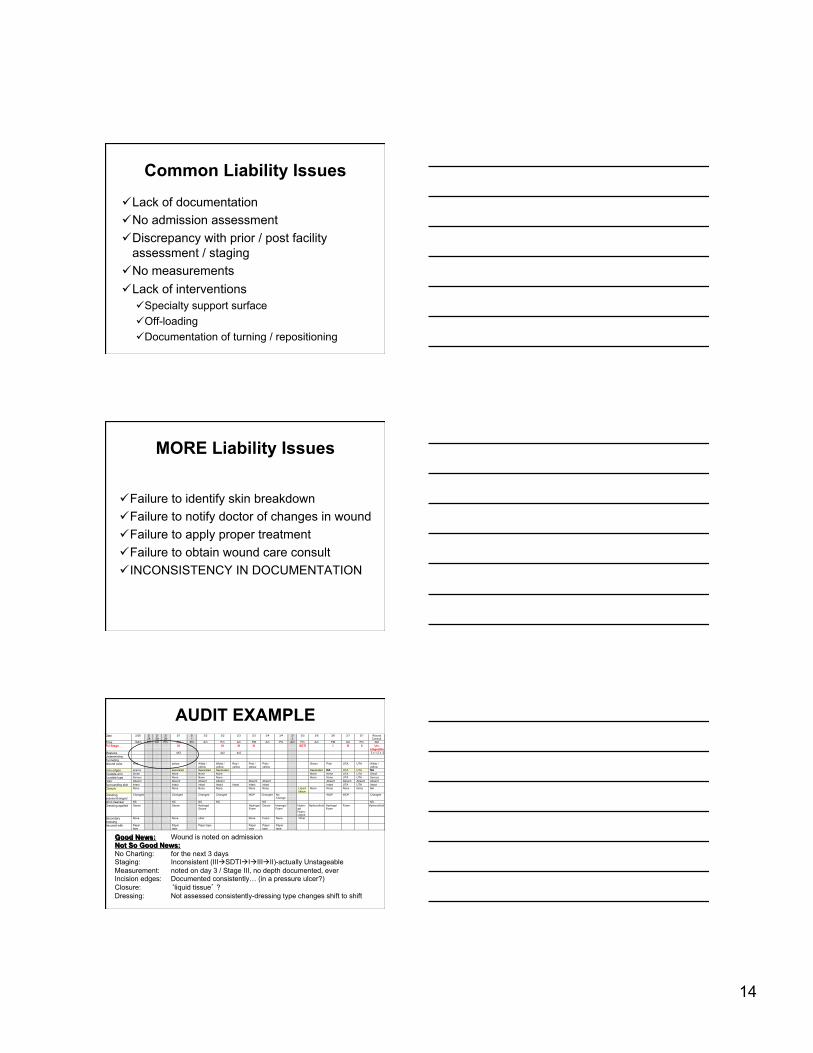
Common Liability Issues
ü Lack of documentation ü No admission assessment ü Discrepancy with prior / post facility
assessment / staging ü No measurements ü Lack of interventions
ü Specialty support surface ü Off-loading ü Documentation of turning / repositioning
MORE Liability Issues
ü Failure to identify skin breakdown ü Failure to notify doctor of changes in wound ü Failure to apply proper treatment ü Failure to obtain wound care consult ü INCONSISTENCY IN DOCUMENTATION
AUDIT EXAMPLE Date 2/28 2/
28 2/ 29
2/ 29
3/1 3/ 1
3/2 3/2 3/3 3/3 3/4 3/4 3/ 5
3/5 3/6 3/6 3/7 3/7 Wound Consult
Time 10Am Pm Am Pm AM Pm Am Pm Am PM Am Pm Am Pm Am PM Am Pm AM PU Stage III III III III SDTI I III II Un-
stageable Measure 4X2 4x2 4x2 3 x 1.2 x .2 Undermining Tunneling Wound color Pink yellow White /
yellow White / yellow
Red / yellow
Pink / yellow
Pink / yellow
Green Pink UTA UTA White / yellow
Incis edges approx separated Separated Separated Separated NA UTA UTA NA Exudate amt Small None None None None None UTA UTA Small Exudate type Serous None None None None None UTA UTA Serous Odor Absent Absent Absent Absent Absent Absent Absent Absent Absent Absent Surrounding skin Intact Intact Intact Intact Intact Intact Intact Intact UTA UTA Intact Closure None None None None None None Liquid
tissue None None None None NA
Dressing assess/changed
Changed Changed Changed Changed WDP Changed No Change
WDP WDP Changed
Wnd cleanser NS NS NS NS NS NS Dressing applied Gauze Gauze Hydrogel
Gauze Hydrogel
Foam Gauze Hydrogel
Foam Hydro-
gel Hydro- colloid
Hydrocolloid Hydrogel Foam
Foam Hydrocolloid
Secondary dressing
None None other None Foam None Other
Secured with Paper tape
Paper tape
Paper tape Paper tape
Paper tape
Paper tape
Good News: Wound is noted on admission Not So Good News: No Charting: for the next 3 days Staging: Inconsistent (IIIàSDTIàIàIIIàII)-actually Unstageable Measurement: noted on day 3 / Stage III, no depth documented, ever Incision edges: Documented consistently… (in a pressure ulcer?) Closure: ‘liquid tissue’ ? Dressing: Not assessed consistently-dressing type changes shift to shift
15
DOCUMENTATION TIPS
Documentation should include: Ø Data from Nursing Assessment Ø Nursing actions / interventions taken Ø Individuals notified about concerns / issues Ø Evaluation of actions
Standard of Care ü Nursing Assess ü Plan of Care ü Interventions ü Eval / Re-Eval
DOCUMENTATION TIPS Ø Document within timeframe outlined per
facility policy Ø Correctly identify LEFT and RIGHT Ø Correctly identify LOCATION, especially
Ø SACRAL Ø COCCYX
Ø Correctly stage all PRESSURE ULCERS Ø Do NOT stage wounds that are
NOT pressure ulcers Characteristics ü Timely ü Accurate ü Comprehensive ü Complete
GENERAL CAUTION Spell correctly: Ø “Fecal heart tones heard” Use appropriate words and grammar: Ø “The pelvic exam was done on the floor” Avoid inappropriate comments: Ø “Patient received insufficient care today
because nurse patient ratio was 1:7”
16
Don’t Forget RISK ASSESSMENT
ü Evidenced based tool: Braden / Norton ü Follow facility policy for frequency ü INTERPRET RESULTS
ü Implement appropriate interventions ü Use score to adjust the plan of care
Standard of Care ü Nursing Assess ü Plan of Care ü Interventions ü Eval / Re-Eval
IMPROVING COMPLIANCE
Ø Staff education and support related to
wound ID, pressure ulcer staging, wound assessment..
Ø Tools and visuals to assist staff in wound identification and staging
WOUND DOCUMENTATION
FORMAT SUGGESTIONS Ø Nurse ‘friendly’ Ø Contain all components necessary for ‘complete’ documentation Ø Improves probability of comprehensive doc
Ø Visual

17
EXAMPLE 1-INDICATE LOCATION OF WOUND (S) ON BODY DIAGRAM 2-DOCUMENTATION FOR: ALL WOUNDS EXCEPT INTACT SURGICAL WOUNDS
Wound #
Location Wound Type / Pressure Ulcer Stage
Wound Measurement
Appearance Drainage Odor Cleansed with
Dressing Applied
Click boxes for ‘smart
text’ options
1
Left ILIAC
PRESSURE ULCER STAGE
II 2 X 2 X .2cm RED SCANT
SEROUS ABSENT NS Hydrocolloid
3-DOCUMENTATION FOR INTACT SURGICAL WOUNDS ONLY A-Intact surgical incisions #___ through #___ (choose smart textà (1 / 2 / 3 / 4 / 5 / 6 / 7 / 8 / 9 / 10) B-Incision Appearance __________________________ (choose smart textà (clean / dry / well approximated / without erythema / without drainage / without odor) C-Closure ______________ (choose smart textà staple / sutures / glue / other / none)
‘SMART TEXT’ OPTIONS Wound# àchoose smart textà (1 / 2 / 3 / 4 / 5 / 6 / 7 / 8 / 9 / 10) Location àchoose smart textà (coccyx, ischial, scaral…) Wound Type / àchoose smart textà (arterial, diabetic, PU stage I, PU stage II, PU stage III…) Measurement àchoose smart textà (length 1 / 2 / 3…) (Width 1 / 2 / 3…) (Depth 1 / 2 / 3...) Appearance àchoose smart textà (red / pink / yellow / gray….) Drainage àchoose smart textà (none, scant, small…) Odor àchoose smart textà (absent, present) Cleansed with àchoose smart textà (NS, wound cleanser...) Dressing àchoose smart textà (Calcium alginate, gauze, hydrocolloid…)
X #1
BOTTOM LINE
Every nurse is responsible for the patient care provided and the DOCUMENTATION
to support it
SOME OPTIONS…

18
NURSING TOOLS
Ø Nurse ‘cheat sheet’ Ø Pressure ulcer staging analogy Ø PU staging algorithm Ø Musical wound assessment
‘Cheat Sheet’ for Nurses
Pressure Ulcer Analogy
Baker Pressure Ulcer Staging Tool
Nursing Tools
Musical Wound Assessment
Standard of Care ü Nursing Assess ü Plan of Care ü Interventions ü Eval / Re-Eval
Characteristics ü Timely ü Accurate ü Comprehensive ü Complete

19
Thank You
Wound Care Nursing





























