Embed Size (px)
Citation preview
MichiganHIVClinicalNursingConference
NursingCaseManagement:ImpactonAdherenceandCare
KathyForrest,MSN,MA,RNMay19,2017
1
Acknowledgements:GailDenkins,RN,BS;HIVHealthCoordinator,MDHHSandJenniferLangholz,BSN,RN;NurseCaseManager,MercyHealthPhysicianPartners-InfectiousDisease
Disclosure
Noconflictofinterestisdisclosedbytheauthorforthispresentation
2
LearningGoals
Attheconclusionofthispresentation,nurseswillbeableto:
• DescribethefoundationalprinciplesofnursecasemanagementanditsvalueinthecareofpatientswithHIVandSTDs
• Determineappropriateinterventionsforselectedclinicalexamplesusingconceptmappingwithcolleagues
• EvaluateconceptsandstrategiesforapplicationtopatientsinpracticewithHIVandSTDs
3
Foundational Principles of Nurse Case Management
4
Nurses’Role
• Centralroleinhealthcaredelivery• Uniquelypositionedtoassistpatientsandfamilieswithchroniccaremanagement
• Healthsystemshiftingtoemphasisonprimarycarewithcaredeliveredbyhighlyfunctioningteams
• RNleadingateam-based,patientcenteredapproachtocare
5MacyFoundation.2016.JosiahMacyAnnualReport.http://macyfoundation.org/docs/annual_reports/2016_Josiah_Macy_Annual_Report_Final.pdf
Whatiscasemanagement?
• Acollaborativeprocessofassessment,planning,facilitation,carecoordination,evaluation,andadvocacy foroptionsandservicestomeetanindividual’sandfamily’scomprehensivehealthneedsthroughcommunicationandavailableresourcestopromotequality,cost-effectiveoutcomes.
CaseManagementSocietyofAmerica(CMSA),2016:http://www.cmsa.org6
CommissionforCaseManagementCertification(CCMC)
• “Casemanagementisacollaborativeprocessthatassesses,plans,implements,coordinates,monitorsandevaluatestheoptionsandservicesrequiredtomeettheclient’shealthandhumanservicesneeds.Itischaracterizedbyadvocacy,communication,andresourcemanagementandpromotesqualityandcost-effectiveinterventionsandoutcomes.”(CommissiononCaseManagerCertification[CCMC],2010,p.3)
7
PhilosophyofCaseManagement
UnderlyingPremise:“Whenanindividualreachestheoptimumlevelofwellnessandfunctionalcapability,everyonebenefits:theindividual,theirsupportsystems,thehealthcaredeliverysystemandreimbursementsources”(cmsa.org).
Thecasemanageristhefacilitatoroftheprocess!
CaseManagementSocietyofAmerica(CMSA),2016:http://www.cmsa.org 8
CaseManagementBodyofKnowledge
• KnowledgeDomainsofCMSpecialtyPractice– Casemanagementconcepts– Principlesofpractice– Healthcaremanagementanddelivery– Healthcarereimbursement– Psychosocialaspectsofcare– Rehabilitation– Professionaldevelopmentandadvancement
9
CommissiononCaseManagerCertification[CCMC],(2017).Retrievedfromhttps://www.cmbodyofknowledge.com/content/case-management-knowledge-2
ACAandCaseManagementACA:intendedtobroadencoverageforallregardlessofpre-existingcondition;reduceMCRandMCAspending;reducehospitalcosts;reducereadmissionratestohospitals;improvepatientoutcomes;improvedqualityofcareandserviceCaseManagement:CoordinationandCollaborationofhealthcareservicesusingthecasemanagementprocess• Advocacyandeducation:insurancecasemanagervpatientcarecase
manager(CaseManagementAdvisor,2015)• Bridgingthegapbetweeneffectivecareandreimbursementchallenges• Educationtoincreaseawarenessofhealthplans,navigatehealthcare
system• Diagnosisrelatedstrategicplanningtoreducereadmissions• Guidingcaretopromoteself-management,smoothtransitions,and
coordinationofcare• Focusonhomecareservicestoreducehealthcarecosts• Valuedrivencaretransformation:CMsimproveclinicalcareoutcomes
andimprovepatients’experiences
Phillips&Fitzsimons(2015).TheAffordableCareAct:ImpactonCaseManagers10
HealthCareReform:CaseManager
• ExpandstheroleofCaseManagerUsingdata:
– Improvesclientconditionandoutcomes– Improvesfinancialpositionoforganization–Providesreturnoninvestment(ROI)
11CMSA,2015
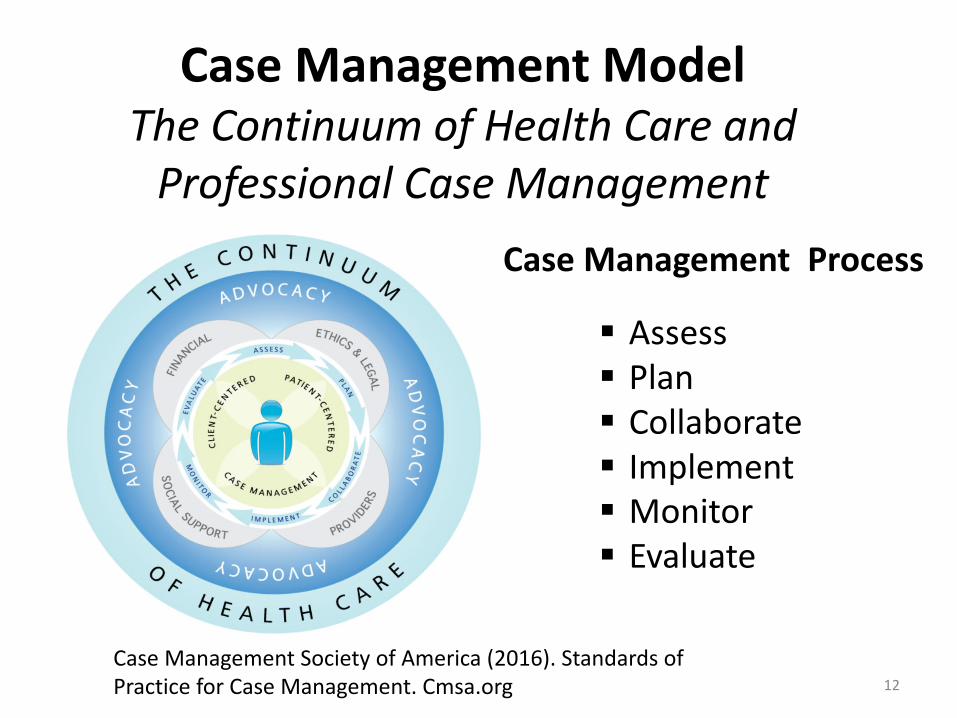
CaseManagementModelTheContinuumofHealthCareandProfessionalCaseManagement
CaseManagementProcess
§ Assess§ Plan§ Collaborate§ Implement§ Monitor§ Evaluate
12CaseManagementSocietyofAmerica(2016).StandardsofPracticeforCaseManagement.Cmsa.org
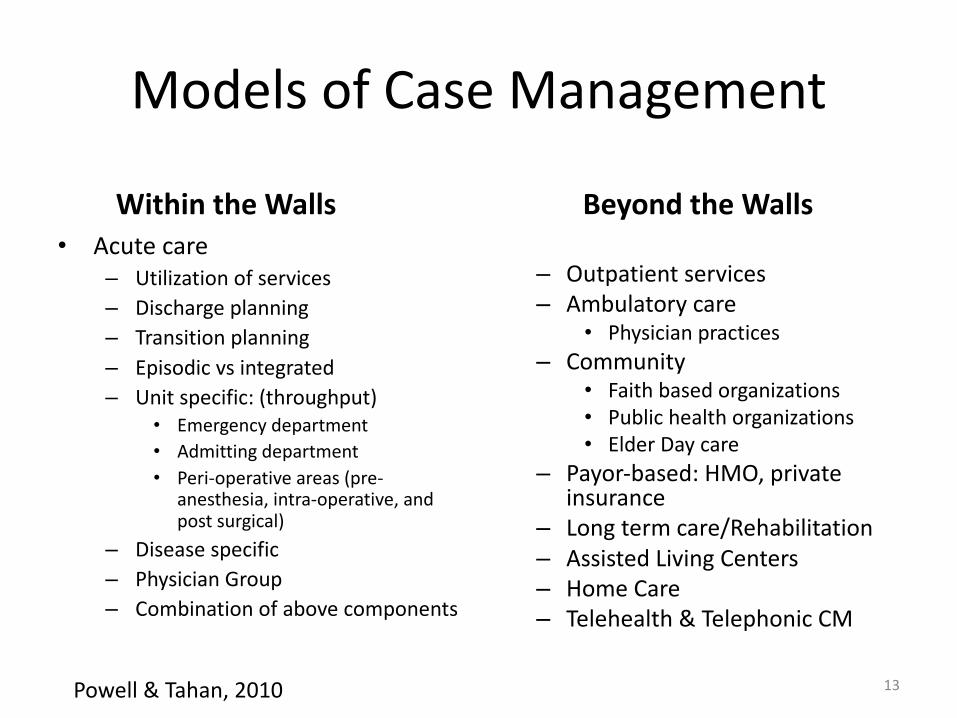
WithintheWalls BeyondtheWalls• Acutecare
– Utilizationofservices– Dischargeplanning– Transitionplanning– Episodicvsintegrated– Unitspecific:(throughput)
• Emergencydepartment• Admittingdepartment• Peri-operativeareas(pre-
anesthesia,intra-operative,andpostsurgical)
– Diseasespecific– PhysicianGroup– Combinationofabovecomponents
– Outpatientservices– Ambulatorycare
• Physicianpractices– Community
• Faithbasedorganizations• Publichealthorganizations• ElderDaycare
– Payor-based:HMO,privateinsurance
– Longtermcare/Rehabilitation– AssistedLivingCenters– HomeCare– Telehealth&TelephonicCM
ModelsofCaseManagement
13Powell&Tahan,2010
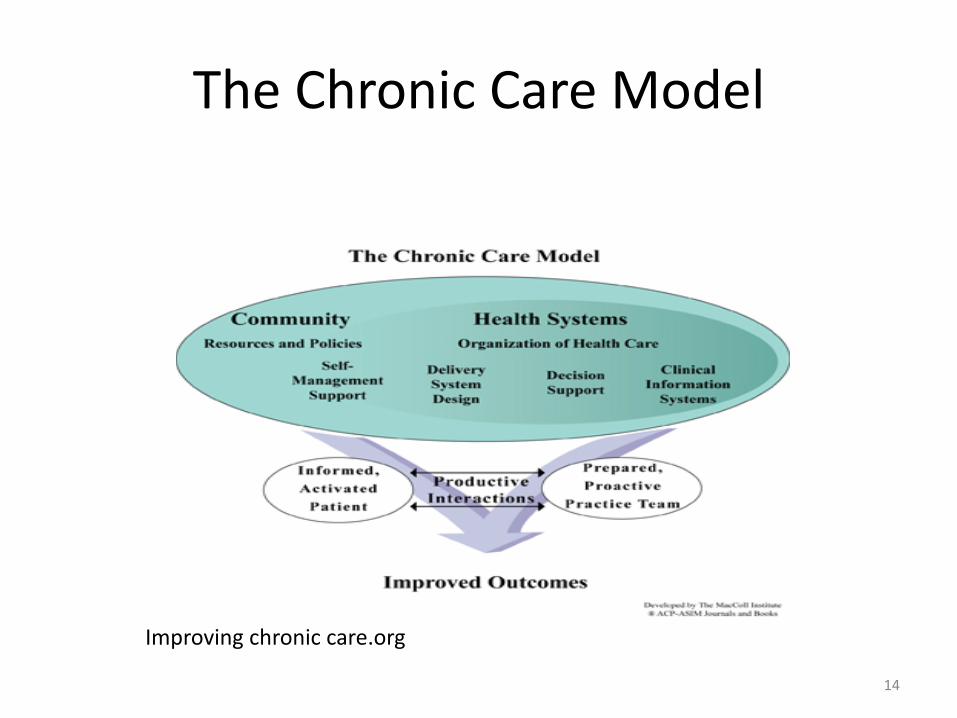
TheChronicCareModel
14
Improvingchroniccare.org
OutcomesofOptimalCMPractice• ThreeTargetGoals
– 1.Qualitycare/WellnessPromotion– 2.Accesstoappropriatehealthcareservices– 3.Costefficiency/financialresourceuse
• OutcomesoftheCaseManagementProcess– Qualityofcare– Collaborationamonghealthcareteammembers– Fiscalresponsibilities– Patientandfamilyadvocacy– Outpatient/community-basedcare– Professionalpractice
Source:Powell,S.andTahan,H.(2010).Essentialcasemanagementjobresponsibilitiesandskills.CaseManagement:APracticalGuideforEducationandPractice.(3rd ed.,p.35-68). 15
AdvantagesofCMPractice• AcrossalllevelsofcareCaseManagementhasseveraladvantages:– Focusonwellness, optimizingQOL,function,independenceandautonomy
– Preventivepracticestodetourorpreventproblems– Fewerhospitalreadmissions/preventadmissions– Lessacuityuponadmission– Resources tonavigatehealthcaresystem– FewerEDvisitsand911calls– Maximizereimbursement– Lowercostsofprovidingcare
Source:Powell,S.andTahan,H.(2010).OverviewofCasemanagement.CaseManagement:APracticalGuideforEducationandPractice.(3rd ed.,p.10). 16
RegardlessofCareorPracticeSetting
17
• CaseManagementincludes:– Outcomesorientedcaredelivery– Appropriateresourceallocation/utilization– Comprehensivecareplanning:assessment,interventionsand
linkingtoneededresources– Integrationandcoordinationofcaretoeliminatefragmentation– Collaborationacrosscareprovidersandsettings– Advocacy toensureneededservicesareobtained/outcomes
met– Useoflicensedprofessionalascasemanager– Compliancewithstandardsofaccreditationandregulatory
agencies– Effectivecommunicationacrossproviders,caresettingand
includingthepatient/family– Consumerandstaffsatisfaction
CategoriesandDomainsRoles,ResponsibilitiesandFunctions
• 5BroadCategories oftheCMRoles/Responsibilities– 1.ClinicalCareManagement– 2.ManagementandLeadership– 3.FinancialandResourceManagement– 4.InformationManagement– 5.ProfessionalResponsibilities
• 6Domains ofCMRolesandFunctions– 1.Casefindingandintake– 2.ProvidingCMservices– 3.OutcomesEvaluation/ClosingCase– 4.UtilizationManagement– 5.PsychosocialandEconomicIssues– 6.Vocationalconceptsandstrategies
18
CMCertification-CCM
• Nationalcertification• Demonstratesadherencetostandardsofcasemanagementpractice
• Validatesknowledge,educationandskillsinspecialtypractice
• Demonstratesprofessionalcompetence• Boostyourprofessionalcareer
19CommissionforCaseManagerCertification(CCMC):www.ccmcertification.org
TitleProtection
• CaseManagertitle- - advocacyworkunderway• PA499of2016
– RecognizesClinicalNurseSpecialistsinthePublicHealthCode,specialtycertification
– “Clinicalnursespecialist-certified”meansanindividualwhoislicensedasaregisteredprofessionalnurseandwhohasbeengrantedaspecialtycertificationasaclinicalnursespecialistbytheMichiganboardofnursing
– AllowsspecificAPRNactivities(prescribing;rounds;orders)
• Nurse(RN)versusmedicalassistant- -thinkofitintheseterms
20
PA0499:http://www.legislature.mi.gov/documents/2015-2016/publicact/pdf/2016-PA-0499.pdf

CASEMANAGEMENTVALUEINCAREOFPATIENTSWITHHIVANDSTDS
21
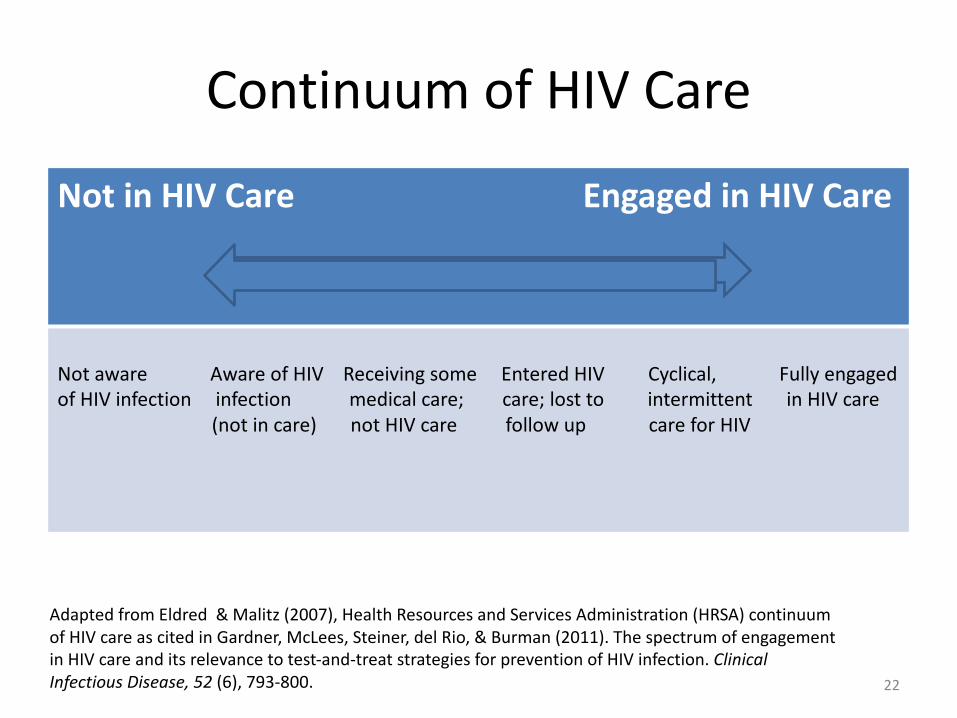
ContinuumofHIVCare
Not inHIVCareEngagedinHIVCare
NotawareAwareofHIV ReceivingsomeEnteredHIVCyclical,FullyengagedofHIVinfectioninfectionmedicalcare;care; losttointermittentinHIVcare
(notincare)notHIVcarefollow upcareforHIV
22
AdaptedfromEldred&Malitz(2007),HealthResourcesandServicesAdministration(HRSA)continuumofHIVcareascitedinGardner,McLees,Steiner,delRio,&Burman(2011).ThespectrumofengagementinHIVcareanditsrelevancetotest-and-treatstrategiesforpreventionofHIVinfection.ClinicalInfectiousDisease,52(6),793-800.
Known• Asof2015,1.2millionpeopleinUSwerelivingwithHIV:1in
8wereunaware(CDC,2017)• Duringtheperiodof2005-2014,theannualnumberofnew
HIVdiagnosesdeclined19%(CDC,2017)• Availabilityofpotentantiretroviraltherapy(ART)resultsin
remarkabledecreasesinHIV-relatedmorbidityandmortality(CDC,HIVSurveillance,2016);UNAIDS,2016)
• EntryintoHIVmedicalcareandretentioniscriticaltoprovisionofART
• AdherencetoARTisakeycomponenttodeterminesuccessfulHIVoutcomes
• IdentifyingpotentialgapsintheHIVcontinuumofcareandpreventingthemisimportanttoimprovedoutcomes
Thompsonetal,2012;CentersforDiseaseControlandPrevention[CDC],2017;CDC,2016;Gardneretal.,2011;UNAIDS,2016) 23
Statistics• 38%personswithHIVinU.S.achievedviralsuppression(UNAIDS,2016)
• OfthosewhoknewtheyhadHIV,69%linkedtocare;only59%retainedincare(ascitedinThompsonetal.,2012)
• Highlevelsofadherencerequiredtopreventresistantmutationsandvirologicfailure.Only62%ofpersonsachievedadherenceto90%ofdoses(ascitedinThompsonetal.,2012)
• Challenge:explorebestpracticestoimproveentryintocareandretainincare.
24
CoordinatedCare:PersonsLivingwithHIV• Accessto:
– Comprehensiveandholistichealthcare inamedicalhome
– Healthpromotionservicesandchronicdiseasemanagement
– Navigation assistance(healthcareandsocialservicesnetwork)
– Coordinatedlogistics (transportationorchildcare)– Governmentfundedbenefitsandprograms– Coordinatedhealthinformation(primarycare,specialistandotherteammembers)
– Strategiestoovercomebarriersofadherencetoantiretroviraltreatment(ART)
25HIVCareSectionCareCoordinationRFP2014
CareCoordination• PatientcareactivitiesareintentionallyorganizedwithallparticipantstobenefittheindividualwithHIVacrossthecontinuumofcare
• MostimportantaspectofHIVcare• Experts:knowledge,skills,experience• Usingcareguidelines- evidence-basedpractice• Sharedplanofcare- - clinicalinformationsharedinatransparentwaybyallcareproviders
• Patientsengagedandretainedincare=improvedhealthoutcomes,suppressedviralload
26HIVCareSectionCareCoordinationRFP2014
WhyisCareCoordinationsoDifficult?1.Accountability fortheprocessisshared,whichcontributestoambiguity astowhoisresponsibleformakingitworkwell.2.ManyPCPsnolongerhavethepersonalrelationshipswithconsultantsandhospitalsthatmakecommunicationeasier.3.Theaddedtimeandeffortrequiredtoachieveaneffectivereferral/consultationortransitionisgenerallynotreimbursed.4.Mostprimarycarepracticesdonot havethededicatedpersonnelorinformationinfrastructuretocoordinatecareeffective
27
CaliforniaHealthCareFoundation.(2008).ReducingCareFragmentation:AToolkitforCoordinatingCare.Retrievedfromhttp://www.improvingchroniccare.org/downloads/reducing_care_fragmentation.pdf
Recommendations:EntryIntoandRetentioninCare
#1Systematicallymonitorentry intocare- sharedresponsibility
#2Systematicallymonitorretention- biomarkers,visitadherence,gapsincare,visitsperinterval
#3Strengthbasedcasemanagement- newlydiagnosed(upto5visitsin90days)[motivationalinterviewing]
#4Intensiveoutreach toindividualsnotengagedinmedicalcarewithin6monthsofdiagnosis
#5Peer orparaprofessionalpatientnavigators-facilitateinteractionwithhealthcare;keepvisitsThompsonetal,2012 28
Recommendations:MonitoringARTAdherence
#6Selfreportedadherence- useshortinterval(oneweekvmonth)#7Pharmacyrefilldata-whenrefillsnotautosenttopatients#8Drugconcentrationsinbiologicalsamples- notrecommended.Toomuchvariation
#9Pillcountsbystafforpatientsnotrecommended(susceptibletopilldumping)
#10Electronic drugmonitors- impractical,burdensome(not recommended)
29
Recommendations:InterventionstoImproveARTAdherence
#11Oncedailyregimensarerecommended,iftoleratedfortreatmentnaïvepatients
#12Switchcomplexorpoorlytoleratedregimenstooncedailywithequivalentefficacy(experiencedpatients)
#13Fixeddosecombinationstodecreasepillburden
30
RecommendationsAdherenceToolsforPatients
#14Reminderdevices,communication(phonealarms,textmessages
#15Education/counseling onadherencetools#16Individualone-oneoneARTeducation#17Individualizedadherencesupport(one-on-one)#18Groupeducation/counseling#19Multidisciplinary education/counseling(recommended)
#20Peersupport-helpfulforsomepatients
31
RecommendationsHealthSystem&ServiceDelivery
#21Usingnurses andcommunitycounselor-basedcareapproachesimprovesadherence#22Casemanagementservicestoaddressfoodinsecurities,housing,andtransportation(recommended)#23Integratingmedication/pharmacymanagementsystems#24DirectlyadministeredARTisnotrecommendedforroutineclinicalcaresettings
32
Recommendations:SpecialPopulations
PregnantWomenSubstanceAbuseDisordersMentalHealthIncarcerationHomeless/MarginallyHousedChildrenandAdolescents
33
OtherConsiderations:MotivationalInterviewing
34
• Evidence-basedstrategytoassistpatientstofollowtreatmentrecommendations
• Usesdirective,client-centeredcounselingstyletoelicitbehaviorchangebyhelpingpatientexploreandresolveambivalence
• Acollaborativegoal-orientedstyleofcommunicatingwithparticularattentiontothelanguageofchange.Itisdesignedtostrengthenmotivationforancommitmenttoaspecificgoalbyelicitingandexploringtheperson’sownreasonsforchange inanatmosphereofacceptanceandcompassion
Levensky,Forcehimes,O’Donohue,Beitz,2007.;MillerandRollnick,2013
Motivationis• Fundamentaltochange
• Adynamicandfluctuatingstate
• Particularlysensitivetointerpersonalinteractionswithinfluentialothers
• Stronglyinfluencedbytheinterpersonalstyleofhelpingprofessionals—likenursesorotherhealthcareproviders(HCP)
35
TheproperquestionisnotWhyisn’tthispersonmotivated?
butrather,Forwhatisthispersonmotivated?
Source:MillerandRollnic
TheMotivationalPart
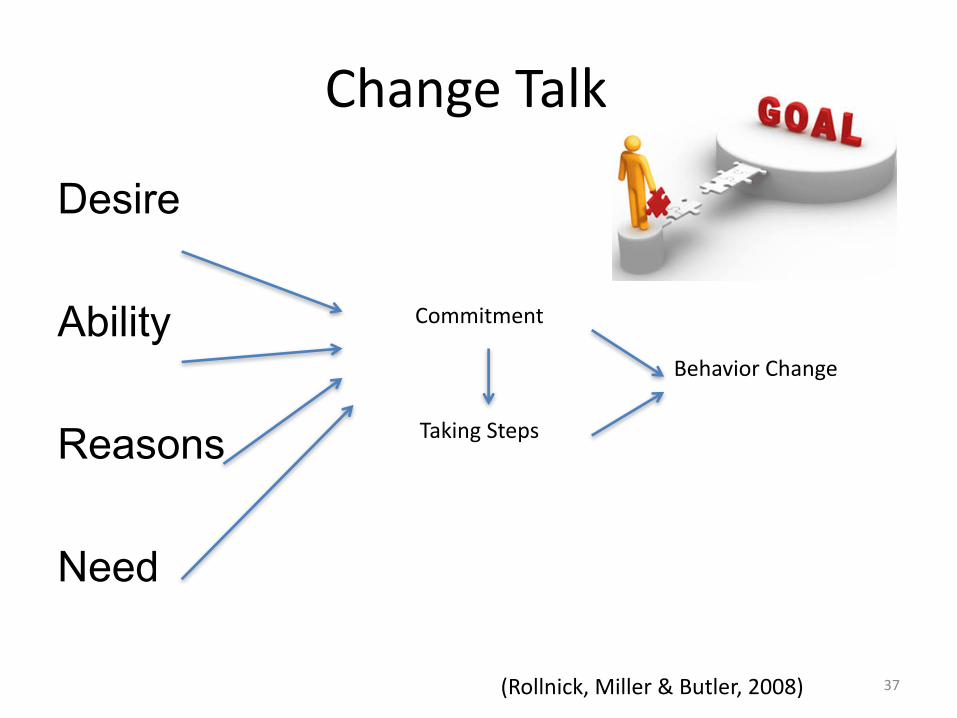
ChangeTalk
Desire
Ability
Reasons
Need
Commitment
TakingSteps
BehaviorChange
(Rollnick,Miller&Butler,2008) 37
OtherConsiderations:HumanTrafficking?
• HumanTraffickingOverview(sexandlabor)• 88%oftraffickedvictimsseekhealthcareserviceswhile
enslaved• HIVprophylaxis• Traumainformedcare• STDsasriskfactor/redflag• APP– downloadSexTraff apptoday!• MSUHumanTrafficking:CNEoffering:
http://nursing.msu.edu/Continuing%20Education/Online%20Offerings/default.htm
38
CapitalAreaHumanTrafficking2016ResourceGuide
Localresourcesbycategorywithcontactphonenumbers– LawEnforcement– LegalAid– Shelters– TransitionalHousing– ChildProtectiveServices– HealthCare– OutpatientandInpatientMentalHealthServices– FamilySupportResources– Transportation– EmploymentServices– FoodServices
http://wrc.msu.edu/_files/pdf/2016-resource-guide-CAATA.pdf39
AdditionalHelpinMichigan• MichiganHumanTraffickingTask
Force• CapitalAreaAnti-traffickingAlliance
(517)-574-5643• GeneseeCountyHumanTrafficking
TaskForce• KalamazooAnti-HumanTrafficking
Coalition(269)303-0725• KentCo.HumanTraffickingTask
ForceHotline:(616)726-7777Contact:616-426-3730
• Midland– (989)835-6771orK.Ade(989)-832-6818 [email protected] orNickiSmith [email protected]
• Mid-MichiganUndergroundRailroad,Inc.(989)399-0007x109or(989)996-0423
• NorthernMichiganCoalitiontoEndHumanTrafficking(231)846-8485
• Ottawa-AlleganCountyHumanTraffickingTaskForce
• SaginawCountyHumanTraffickingToolkit:https://www.saginawcountyms.com/human-trafficking-toolkit.html
• SoutheastMichiganHumanTraffickingTaskForce313-269-5490
• SouthernMichigan(517)266-8880or(517)918-8082
SouthwestMichiganTraffickingTaskForce:http://swmihumantrafficking.org/additional-help-in-michigan/ 40
PositiveSelf-ManagementProgramforHIV(PSMP)
• 2½hours,onceweekly,for6weeks• Facilitatedbytrainedleaders• LivingaHealthyLifewithHIV,4th ed.• Subjectscovered:
1. Howtointegratemedicationregimenintodailylife2. Dealingwithproblems(fear,frustration,fatigue,pain,isolation,etc)3. Appropriateexercisetomaintainandimprovestrength,flexibilityandendurance4. Communicatingwithfamily,friends,healthcareprofessionals5. Nutrition6. Evaluatingsymptoms7. Advanceddirectives8. Decisionmaking9. Sex,intimacyanddisclosure
• ProgramOutcomes– Improvedsymptommanagement– Significantlybettermedicationadherence(ofthoseusingART)– ImprovedHIVsuppressioninbloodafter6months– NoincreasedsideeffectsthannonPSMPparticipants
StanfordMedicine.(2017) 41
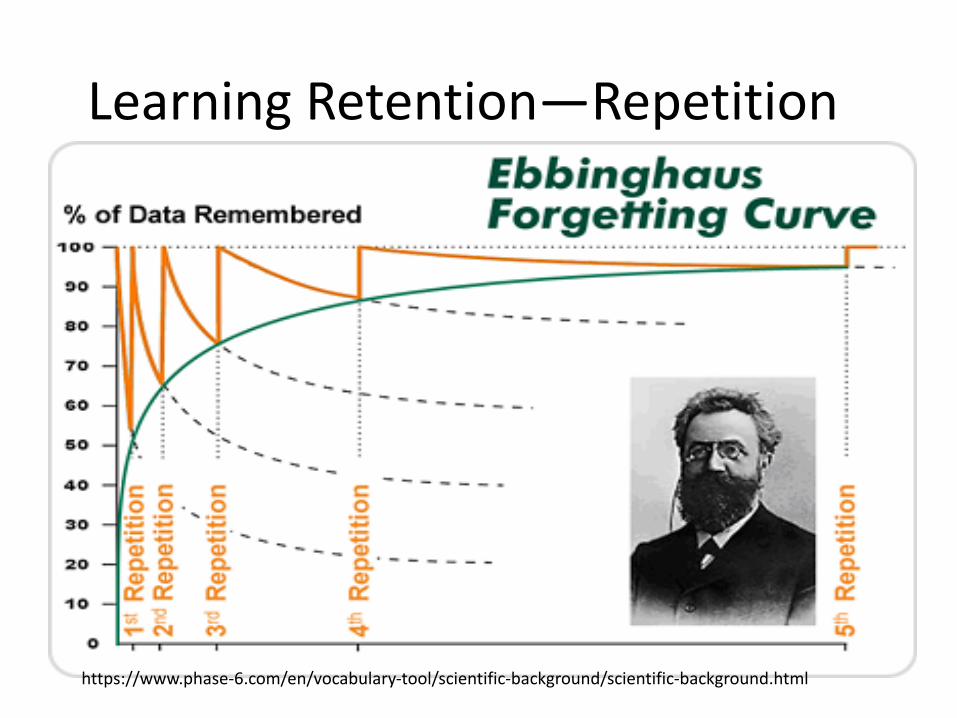
LearningRetention—Repetition
https://www.phase-6.com/en/vocabulary-tool/scientific-background/scientific-background.html

INTERVENTIONS:CAREMAPPING
43
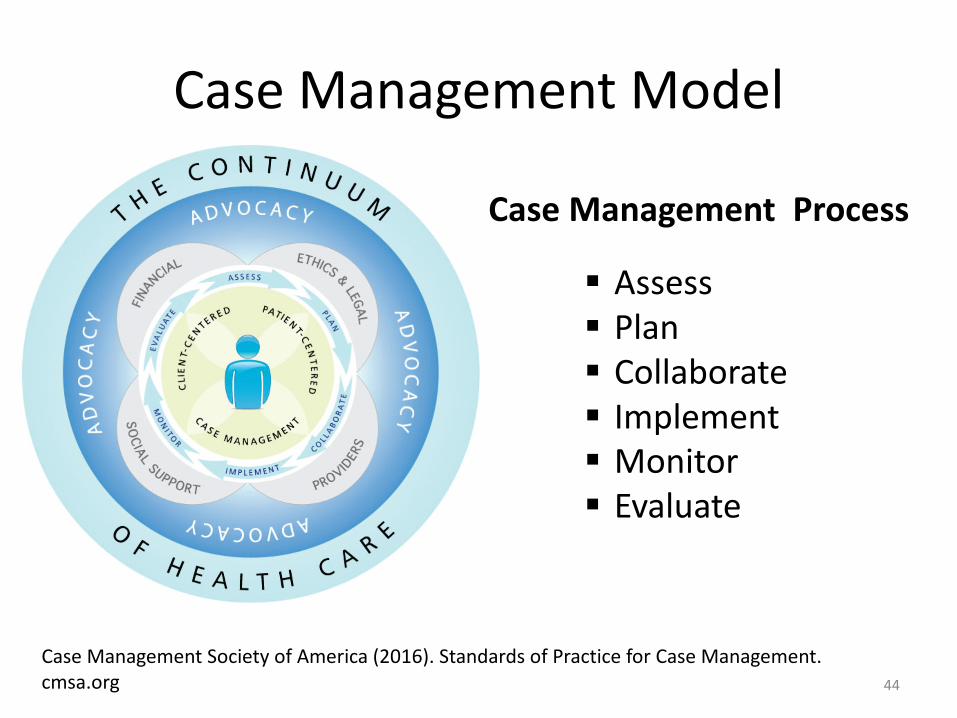
CaseManagementModel
CaseManagementProcess
§ Assess§ Plan§ Collaborate§ Implement§ Monitor§ Evaluate
44
CaseManagementSocietyofAmerica(2016).StandardsofPracticeforCaseManagement.cmsa.org
CareMapping
• Meanstolearn/sortcomplexconcepts,sub-conceptsandtheirinterrelationship
• Central concept/issueisinthecenterofthepage(patient/family)
• Relatedconcepts/issuessurroundthemainissue• Facilitatesteamengagementtoidentifyissuesandformulatecollaborateplansofcareandfollowup
Billings&Halstead(2012).TeachinginNursing:AGuideforFaculty45
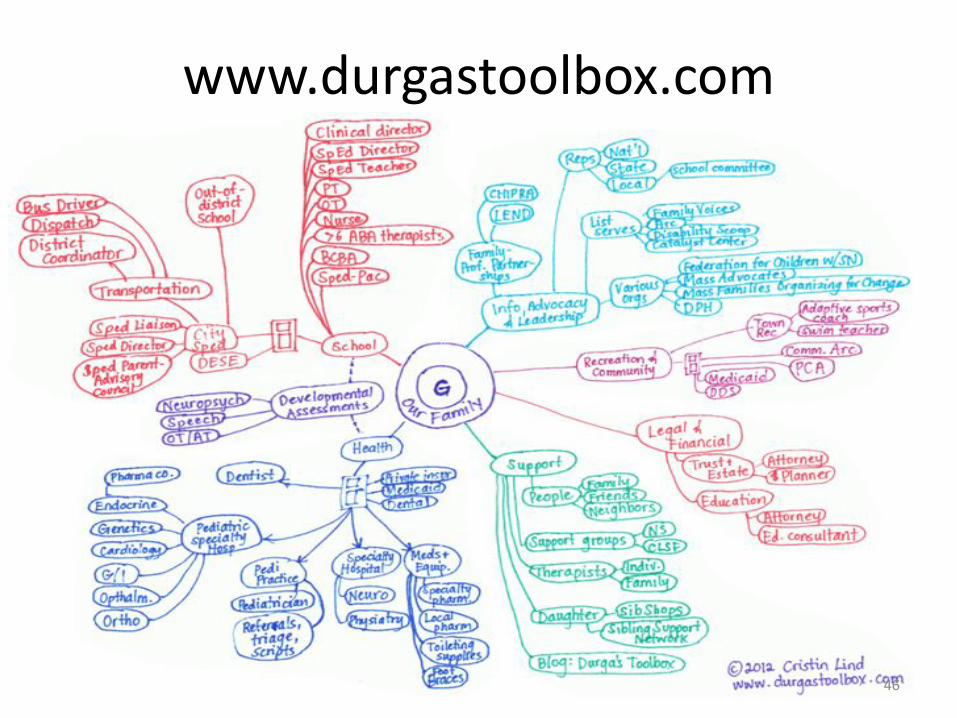
www.durgastoolbox.com
46
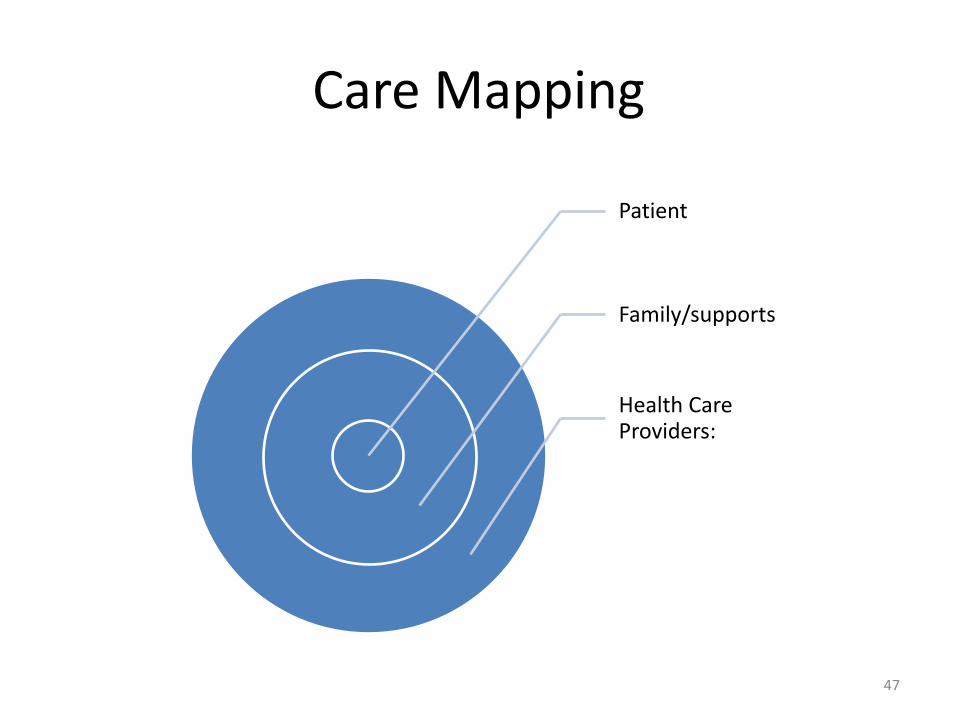
CareMapping
Patient
Family/supports
HealthCareProviders:
47
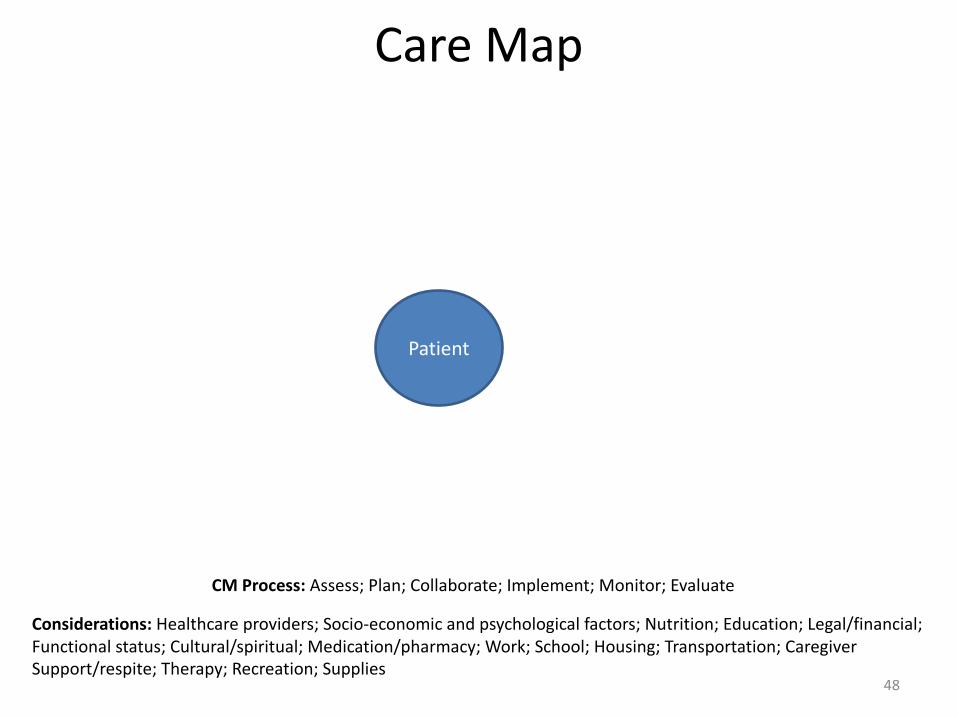
CareMap
Patient
Considerations:Healthcareproviders;Socio-economicandpsychologicalfactors;Nutrition;Education;Legal/financial;Functionalstatus;Cultural/spiritual;Medication/pharmacy;Work;School;Housing;Transportation;CaregiverSupport/respite;Therapy;Recreation;Supplies
CMProcess:Assess;Plan;Collaborate;Implement;Monitor;Evaluate
48
CaseStudy:Mrs.P.3monthfollowupvisittochecklabs/progress
• 42yoAfricanAmericanfemale
• HIV+for10years• Medicationadherent;samescripts2years• CD4countnormal;undetectableviralload
49
CaseStudy:Mrs.P.continued• “justdon’tfeelright”• Reportsincreasingfatiguesincelastvisit“alltuckeredout”
• Activitiesofdailylivingaffected:unabletogroceryshop“tootired”,admittedgettingfooditemsfromconveniencestore1blockaway,“that’sthebestIcoulddo”
• Unabletowalkstairsto2nd floorapartment;usestheelevator
50
CaseStudy:Mrs.P.continuedAssessmentfindings:Temp:97.2degreesF(oral)Pulse:60bpmRR:16bpmBP:116/78Ht:5feet,5inchesWt:115lbs (5lb weightlossinlast3months)Skin:pale,cooltotouchSaO2:96%(pulse-ox)(usually99%)
51
CareMap
Patient:Mrs.P.
Considerations:Healthcareproviders;Socio-economicandpsychologicalfactors;Nutrition;Education;Legal/financial;Functionalstatus;Cultural/spiritual;Medication/pharmacy;Work;School;Housing;Transportation;CaregiverSupport/respite;Therapy;Recreation;Supplies
CMProcess:Assess;Plan;Collaborate;Implement;Monitor;Evaluate
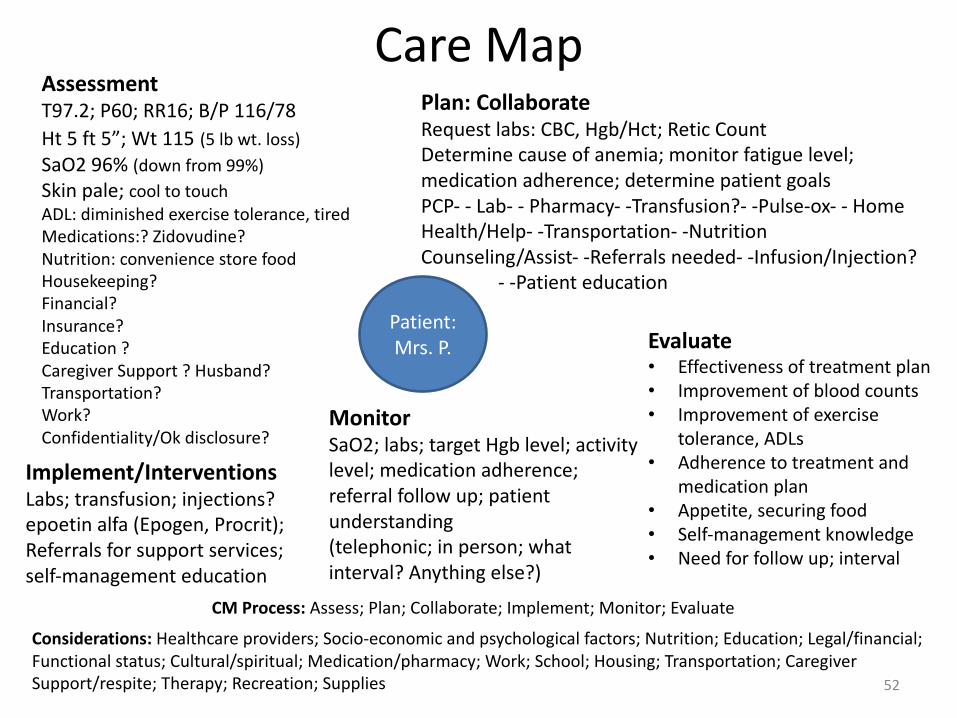
AssessmentT97.2;P60;RR16;B/P116/78Ht 5ft 5”;Wt 115 (5lb wt.loss)SaO296%(downfrom99%)Skinpale;cooltotouchADL:diminishedexercisetolerance,tiredMedications:?Zidovudine?Nutrition:conveniencestorefoodHousekeeping?Financial?Insurance?Education?CaregiverSupport?Husband?Transportation?Work?Confidentiality/Okdisclosure?
Plan:CollaborateRequestlabs:CBC,Hgb/Hct;Retic CountDeterminecauseofanemia;monitorfatiguelevel;medicationadherence;determinepatientgoalsPCP- - Lab- - Pharmacy- -Transfusion?- -Pulse-ox- - HomeHealth/Help- -Transportation- -NutritionCounseling/Assist- -Referralsneeded- -Infusion/Injection?
- -Patienteducation
Implement/InterventionsLabs;transfusion;injections?epoetin alfa (Epogen,Procrit);Referralsforsupportservices;self-managementeducation
MonitorSaO2;labs;targetHgb level;activitylevel;medicationadherence;referralfollowup;patientunderstanding(telephonic;inperson;whatinterval?Anythingelse?)
Evaluate• Effectivenessoftreatmentplan• Improvementofbloodcounts• Improvementofexercise
tolerance,ADLs• Adherencetotreatmentand
medicationplan• Appetite,securingfood• Self-managementknowledge• Needforfollowup;interval
52
YourTurn:CareMapActivity
Patient:Larry
Considerations:Healthcareproviders;Socio-economicandpsychologicalfactors;Nutrition;Education;Legal/financial;Functionalstatus;Cultural/spiritual;Medication/pharmacy;Work;School;Housing;Transportation;CaregiverSupport/respite;Therapy;Recreation;Supplies
CMProcess:Assess;Plan;Collaborate;Implement;Monitor;Evaluate
53
CaseStudy:Larry• 45yogayman;HIVdiagnosisin1987• Collegedegree;hasbeenemployedasCommunityCollegeinstructor
• Noopportunisticinfection• Experiencingwasting,depletionofCD4count,highviralload;failedallHAARTregimens
• Angry;despondentaboutfuture(verballyabusivetoclinicstaffandproviders)
• Malepartner(same)forover10years;couplestherapytoaddressangerissues
54
CaseStudy:LarrycontinuedRecentIssues:• Unabletoengageinenjoyableactivities(creativewriting,hiking,swimming,andreading)
• Reportsnoappetite,cannotsleep,feelsdepressedandsad;occasionallythinksofsuicide;withdrawnfromusualcircleoffriends;admittedhesometimesthinksofsuicide
• Watchestelevisionseatedinrecliner,dayandnight
55
CaseStudy:LarrycontinuedMoreInformation:
• Psychiatristinvolvedincareforafewyears;seesmentalhealthCNSregularlyinclinic
• Treatedwithbuproprion (Wellbutrin),sequentialtrialsofdifferentSSRIsandzolpidem (Ambien)totreatdepressionandsleepdisorder
• Patientreportssomerelieffromsymptoms(heattributestomedications)
• Patientiscoherent,insightfulabouthisfeelings,andabletoengageinplanningcare
56
YourTurn:CareMapActivity
Patient:Larry
Considerations:Healthcareproviders;Socio-economicandpsychologicalfactors;Nutrition;Education;Legal/financial;Functionalstatus;Cultural/spiritual;Medication/pharmacy;Work;School;Housing;Transportation;CaregiverSupport/respite;Therapy;Recreation;Supplies
CMProcess:Assess;Plan;Collaborate;Implement;Monitor;Evaluate
Assessment Plan/Collaborate Implement/Interventions
Monitor Evaluate
57
YourTurn:CareMapActivity
Patient:Larry
Considerations:Healthcareproviders;Socio-economicandpsychologicalfactors;Nutrition;Education;Legal/financial;Functionalstatus;Cultural/spiritual;Medication/pharmacy;Work;School;Housing;Transportation;CaregiverSupport/respite;Therapy;Recreation;Supplies
CMProcess:Assess;Plan;Collaborate;Implement;Monitor;Evaluate
Assessment Plan/Collaborate Implement/Interventions
Monitor Evaluate
58
EVALUATIONOFSTRATEGIES
59
QUESTIONS
• WhatisgoingonwiththisPatient?• WhatspecificconsiderationsdoyouhaveforLarry?
60
MOREQUESTIONS
• Canweassumeconfidentialitydisclosureisestablished?
• WhatareLarry’sgoals?Havetheybeenexplored?
• Whataboutendoflife?
61
62
ReferencesBillings&Halstead(2012).Teachinginnursing:Aguideforfaculty(4th ed.).StLouis,MO:Elsevier
CaliforniaHealthCareFoundation.(2008).ReducingCareFragmentation:AToolkitforCoordinatingCare.Retrievedfromhttp://www.improvingchroniccare.org/downloads/reducing_care_fragmentation.pdf
CaseManagementSocietyofAmerica.(2012).AdherenceGuidelines.Retrievedfromhttp://www.cmsa.org/Individual/Education/CaseManagementAdherenceGuidelines/tabid/253/Default.aspx
CaseManagementSocietyofAmerica.(2016).StandardsofPractice.Retrievedfromhttp://solutions.cmsa.org/acton/media/10442/standards-of-practice-for-case-management
CaseManagementSocietyofAmerica.(2016).[Website]Retrievedfromhttp://www.cmsa.org/
CentersforDiseaseControlandPrevention[CDC],(2017).HIVintheUnitedStates:AtaGlance.Retrievedfromhttps://www.cdc.gov/hiv/statistics/overview/ataglance.html
CentersforDiseaseControlandPrevention(2017).HIVGuidelines.Retrievedfromhttps://www.cdc.gov/hiv/guidelines/
CommissiononCaseManagementCertification[CCMC],(2017).Casemanagementknowledge.Retrievedfromhttps://www.cmbodyofknowledge.com/content/case-management-knowledge-2
Gardner,E.M.,McLees,M.P.Steiner,J.F.delRio,C.&Burman,W.J.(2011).ThespectrumofengagementinHIVcareanditsrelevancetotest-and-treatstrategiesforpreventionofHIVinfection.ClinicalInfectiousDisease,52(6),793-800.
Levensky,E.,Forcehimes,A.,O’Donohue,W.,&Beitz,K.(2007).Motivational interviewing:Anevidence-basedapproachtocounselinghelpspatientsfollowtreatmentrecommendations.AmericanJournalofNursing,107(10),50-58.
MacyFoundation.(2016).JosiahMacyAnnualReport.http://macyfoundation.org/docs/annual_reports/2016_Josiah_Macy_Annual_Report_Final.pdf
MichiganPublicHealthCode:Act368of1978http://www.legislature.mi.gov/(S(upi1k0w4n1kd1jxr5bjir1of))/mileg.aspx?page=getobject&objectname=mcl-act-368-of-1978
Miller, W. R., & Rollnick, S. (2013). Motivational interviewing: Helping people change, (3rd ed.). New York, NY: Guilford Press. 64
ReferencesNationalInstituteofAllergyandInfectiousDiseases,HIV/AIDStreatment.Retrievedfromhttps://www.niaid.nih.gov/diseases-conditions/hiv-treatment
NationalInstituteofHealth(2017).GuidelinesfortheuseofantiretroviralagentsinHIV-1Infectedadultsandadolescents.Retrievedfromhttps://aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf
PA0499:http://www.legislature.mi.gov/documents/2015-2016/publicact/pdf/2016-PA-0499.pdf
Phillips&Fitzsimons(2015).TheAffordableCareAct:Impactoncasemanagers.ProfessionalCaseManagement,20(6),323-327.
Powell,S.K.&Tahan,H.A.(2010).Casemanagement:Apracticalguideforeducationandpractice(3rd ed.).Philadelphia,PA:WoltersKluwerHealth.
Rollnick, S., Miller, W.R., Butler, C. (2008). Motivational interviewing in health care: Helping patients change behavior. New York, NY: Guilford Press.
StanfordMedicine.(2017).Positiveself-managementprogramforHIV(PSMP).Retrievedfromhttp://patienteducation.stanford.edu/programs/psmp.html
Tahan,H.M.&Treiger,T.M.(2017).CMSACorecurriculumforcasemanagement( 3rd ed.).Philadelphia,PA:WoltersKluwer.
Thompson,M.A.,Mugavero,M.J.,Amico,R.,Cargill,V.A.,Chang,L.W.,Gross,R.,…Nachega,J.B.(2012).GuidelinesforimprovingentryintoandretentionincareandantiretroviraladherenceforpersonswithHIV:Evidence-basedrecommendationsfromaninternationalassociationofphysiciansinAIDScarepanel.AnnalsofInternalMedicine,156(11),817-833.Retrievedfromhttp://annals.org/aim/article/1170890/guidelines-improving-entry-retention-care-antiretroviral-adherence-persons-hiv-evidence
UNAIDS.(2016).GlobalAIDSUpdate2016.Retrievedfromhttp://www.unaids.org/en/resources/documents/2016/Global-AIDS-update-2016
UNAIDS.(2016).PreventionGapReport.Retrievedfromhttp://www.unaids.org/en/resources/documents/2016/prevention-gap
U.S.DepartmentofHealthandHumanServices,CentersforDiseaseControlandPrevention[CDC].(2016).HIVCaseReportingandSurveillance.Retrievedfromhttps://www.cdc.gov/hiv/guidelines/reporting.html
U.S.PublicHealthServiceGuidelinesfortheManagementofOccupationalExposurestoHumanImmunodeficiencyVirusandRecommendationsforPostexposure Prophylaxis.Retrievedfromhttp://nccc.ucsf.edu/wp-content/uploads/2014/03/Updated_USPHS_Guidelines_Mgmt_Occupational_Exposures_HIV_Recommendations_PEP.pdf 65