Embed Size (px)
Citation preview

Nuove opportunità nel trattamento medico
ottimale della coronaropatia stabile
PL. Temporelli
Istituti Clinici Scientifici Maugeri
Divisione di Cardiologia Riabilitativa, Veruno

DISCLOSURE INFORMATION
• Temporelli Pier Luigi
negli ultimi due anni ho avuto i seguenti rapporti anche di finanziamento con soggetti portatori di interessi commerciali in campo sanitario:
Letture per:
Sigma-Tau
MSD
Menarini

A 62-year-old man has sustained an inferior ST segment-elevation MI. He has undergone successful primary angioplasty with implantation of a drug-eluting stent for acute occlusion of the right coronary artery.
There were no other significant coronary lesions, and the left ventricular ejection fraction at hospital discharge was 55%. Smoking was the sole cardiovascular risk factor and was stopped at time of MI.
Six months after MI, an exercise test was performed (80% of maximum predicted heart rate; negative).
At present, two years post-MI, the patient is asymptomatic and is
receiving optimal medical therapy for secondary prevention.
Case # 1




Solo due cose sono infinite: l’universo e la
stupidità umana…
E non sono sicuro della prima

L’insostenibile leggerezza della angioplastica nella
cardiopatia ischemica cronica

JAMA Intern Med. August 25, 2014

Metanalisi effetto PCI in pazienti con CAD stabile e documentazione ischemia
Stergiopoulos et al. JAMA Intern Med 2014;174:232-40
Morte IMA non fatale
Revasc Unplanned Angina in FU
CONCLUSIONS AND RELEVANCE:
In patients with stable CAD and objectively documented myocardial
ischemia, PCI with OMT was not associated with a reduction in
death, nonfatal MI, unplanned revascularization, or angina
compared with OMT alone.

Il ruolo irrinunciabile della terapia medica ottimale
nell’angina stabile

«Gestione terapeutica della cardiopatia ischemica cronica sintomatica"

Gestione terapeutica della cardiopatia ischemica cronica sintomatica"

Gestione terapeutica della cardiopatia ischemica cronica sintomatica"

…undergoing PCI, less than half were receiving OMT ….

Qual’è la terapia ottimale nell’angina stabile secondo
le Linee Guida?
Key points
Lifestyle changes are vital in the management of stable
angina, including smoking cessation, healthy diet, weight loss
and control of lipid levels
Associated conditions, such as hypertension and diabetes,
should be treated according to relevant guidance
Anti-anginal drugs should be titrated to the optimal licensed
dose to control symptoms
Revascularisation should be considered in selected patients

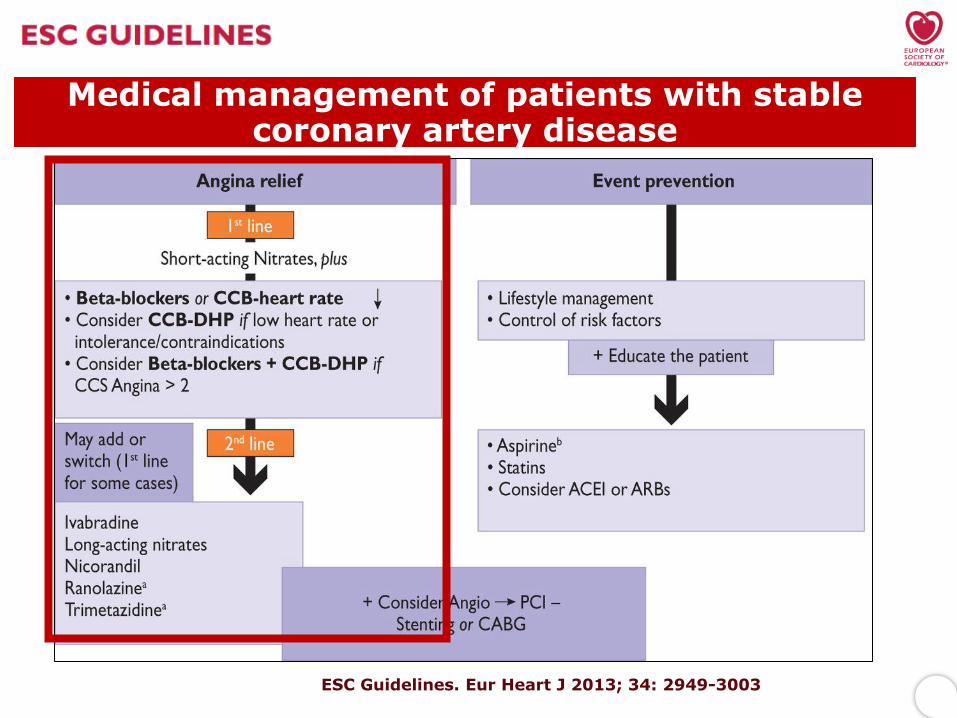
Medical management of patients with stable coronary artery disease
ESC Guidelines. Eur Heart J 2013; 34: 2949-3003

Medical management of patients with stable coronary artery disease
ESC Guidelines. Eur Heart J 2013; 34: 2949-3003
Medical management of patients with stable coronary artery disease
ESC Guidelines. Eur Heart J 2013; 34: 2949-3003 ESC Guidelines. Eur Heart J 2013; 34: 2949-3003

In the first-line setting, the major changes in the new guidelines are the
upgrading of calcium channel blockers, the distinction between
dihydropyridines and non-dihydropyridine calcium channel blockers, and the
presence of important statements regarding the combination of calcium
channel blockers with beta-blockers.

Adapted from Gibbons RJ, et al.
ACC/AHA 2002 Guideline Update for Chronic Stable Angina
Limitations
Comorbidity
Challenges
Side Effects
Beta Blockers Nitrates Calcium Antagonists
• COPD
• Bradycardia
• A-V conduction problems
• Peripheral Vascular Disease
• Sick Sinus Syndrome
• Left ventricular outflow
tract obstruction • Bradycardia
• Heart failure
• Left ventricular dysfunction
• Sick sinus syndrome
• A-V conduction problems
• Sexual dysfunction
• Fatigue
• Depression
• Hypotension
• Syncope
• Headache
• Syncope
• Tolerance
• Hypotension
• Flushing
• Dizziness
• Hypotension
• Edema
• Fatigue
Limitations of Conventional Antianginal Therapies
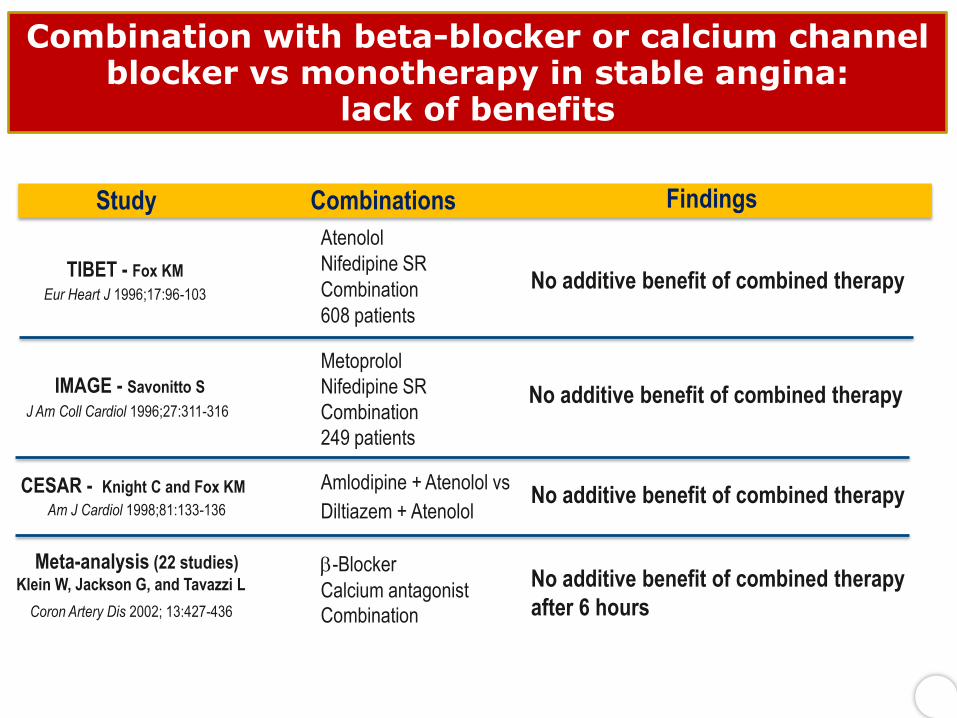
Findings Combinations Study
No additive benefit of combined therapy
Atenolol
Nifedipine SR
Combination
608 patients
TIBET - Fox KM
Eur Heart J 1996;17:96-103
No additive benefit of combined therapy
Metoprolol
Nifedipine SR
Combination
249 patients
IMAGE - Savonitto S
J Am Coll Cardiol 1996;27:311-316
No additive benefit of combined therapy Amlodipine + Atenolol vs
Diltiazem + Atenolol
CESAR - Knight C and Fox KM
Am J Cardiol 1998;81:133-136
No additive benefit of combined therapy
after 6 hours
-Blocker
Combination
Calcium antagonist Coron Artery Dis 2002; 13:427-436
Meta-analysis (22 studies) Klein W, Jackson G, and Tavazzi L
Combination with beta-blocker or calcium channel blocker vs monotherapy in stable angina:
lack of benefits

In the first-line setting, the major changes in the new guidelines are the
upgrading of calcium channel blockers, the distinction between dihydropyridines
and non-dihydropyridine calcium channel blockers, and the presence of
important statements regarding the combination of calcium channel blockers
with beta-blockers.
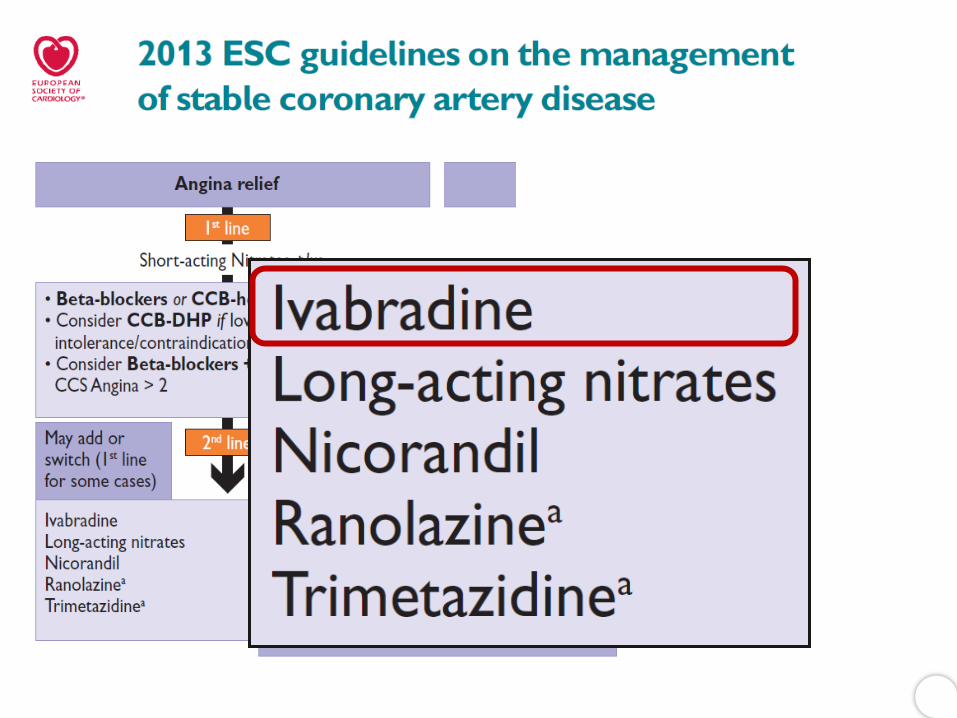
In the second-line setting, the 2013 ESC guidelines recommend the addition
of long-acting nitrates, ivabradine, nicorandil or ranolazine to first-line
agents. Trimetazidine may also be considered. However, no clear distinction
is made among different second-line drugs, despite different quality of
evidence in favour of these agents.

Eur Heart J , August 30, 2013

L’amore per i nitrati ai tempi del colera


Rassaf, Eur Heart J 2013

Nitrati «long-acting» e
funzione endoteliale
Long-acting nitrates induce or worsen oxidative stress by Increasing intracellular superoxide Inactivating nitric oxide and formation of peroxinitrite Inhibiting prostacyclin formation Stimulating endothelin expression Inhibiting the activity of soluble guanylate cyclase Long-acting nitrate drugs increase sympathetic activation and apocrine neurohormonal mechanisms by Increasing production of norepinephrine (also called noradrenalin) Increasing production of angiotensin II
It is known that none of the available long acting nitrates exerts 24-h antianginal and anti-ischemic therapeutic effects
Eur Heart J , August 30, 2013


Eur Heart J , August 30, 2013

Mega J, Circulation 2010
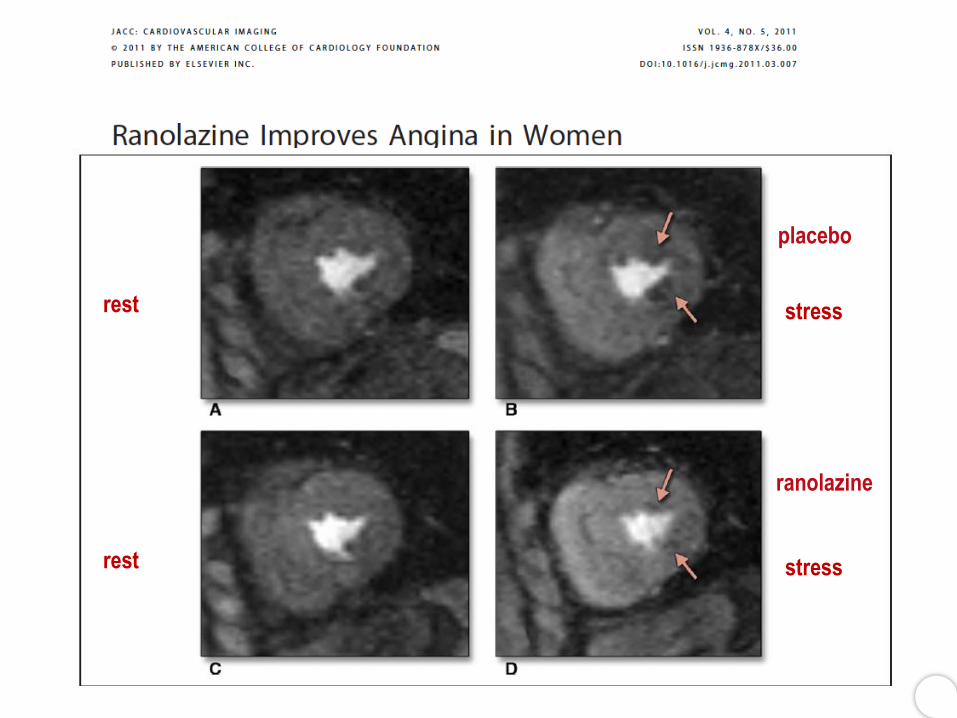
stress rest
stress rest
ranolazine
placebo




Facciamo così?
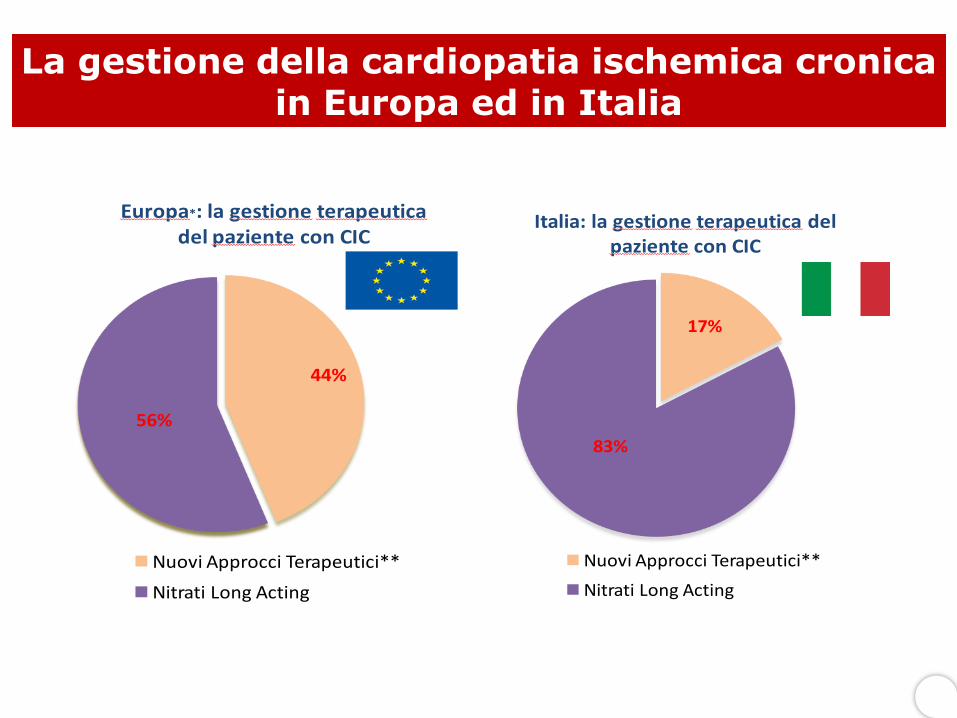
La gestione della cardiopatia ischemica cronica in Europa ed in Italia
44%
56%
Europa*: la gestione terapeuticadel paziente con CIC
Nuovi Approcci Terapeutici**
Nitrati Long Acting
17%
83%
Italia: la gestione terapeutica del paziente con CIC
Nuovi Approcci Terapeutici**
Nitrati Long Acting

E’ tempo di cambiare paradigma !


Algoritmo per l’ottimale gestione del trattamento sintomatico del paziente con
cardiopatia ischemica cronica stabile
Sintomi non controllati
Ivabradina *
Ranolazina
Associazione con:
Terapia di prima linea:
β –bloccante
Ca – antagonisti Nitrati LA
Trimetazidina
Da valutare:
Ca – antagonisti Nitrati LA
Trimetazidina
Da valutare:
Controindicazioni o intolleranza
Ranolazina
Ivabradina *
* In pz in RS, FC ≥70 bpm, FEVS≤40%

Alla luce delle evidenze cliniche la terapia medica ottimale dovrebbe essere il fondamento nella gestione del paziente con angina stabile Terapia medica ottimale non vuol dire assenza di rivascolarizzazione a priori, piuttosto la presenza di un intensivo approccio farmacologico e non Nell’ambito di un ottimale approccio farmacologico secondo le recenti Linee Guida internazionali e documenti di consenso nazionali le nuove molecole, in particolare ranolazina, occupano un ruolo di rilievo
Take Home Message


Ranolazina
Lo specialista (CAR-GER-DIA) in quasi l’80% dei casi ripete la prescrizione di nitrati a lunga durata
d’azione
La gestione del paziente in rivalutazione
Fonte dati Medical Audit 2013





























