Embed Size (px)
Citation preview

Sacramento, CA 95817
e Abstract—Recent world events have increased concernthat hospitals must be prepared for radiological emergencies.Emergency departments (EDs) must be ready to treat patientssuffering from injuries in combination with radiation expo-sure or contamination with radioactive material. Every hos-pital should have a Radiological Emergency Medical ResponsePlan, tested through periodic drills, which will allow effectivehandling of contaminated and injured patients. Treatment oflife-threatening or severe traumatic injuries must take prior-ity over radiation-related issues. The risk to ED staff fromradioactive contamination is minimal if universal precautionsare used. The likelihood of significant radiation exposure tostaff under most circumstances is small. Educating medicalstaff on the magnitude of the radiological hazards allows themto promptly and confidently provide the necessary patientcare. Measures must be taken to prevent the “worried well”and uninjured people with radioactive contamination fromoverwhelming the ED. © 2007 Elsevier Inc.
e Keywords—radiological emergency; radiological casual-ties; terrorism; dirty bombs; emergency planning
INTRODUCTION
The concern that emergency department (ED) personnelwill have to care for patients injured or contaminated by
a terrorist act involving radioactive material has in-creased dramatically since the end of the cold war in theearly 1990s. Sealed sources containing large amounts ofradioactive material suitable for use by a terrorist arewidely used in medicine and industry, and many largesealed sources have been lost from governmental over-sight, particularly in developing countries and states thatwere part of the former Soviet Union (1). This article isintended to assist hospitals and emergency departmentsin preparing for nuclear/radiological terrorism and foraccidents involving radiation injuries or radioactive con-tamination.
There are many possible terrorist radiation injury sce-narios, including: 1) covert placement of a sealed radio-active source in a public location, 2) the use of a radio-logical dispersal device (RDD), 3) an attack on orsabotage of a nuclear facility, and 4) detonation of anuclear weapon (atomic bomb), which is a remote butpossible threat (1,2). A sealed source may be covertlyplaced in a location that would expose many people untilthe presence of the source is discovered. Although manypeople could be exposed, it is unlikely that any would becontaminated. An RDD is not a nuclear weapon; instead,it is a device designed to spread radioactive material forthe purpose of terrorism. An RDD that uses a conven-
Selected Topics: Disaster Medicine is coordinated by Irving “Jake” Jacoby, MD, of the University of California SanDiego Medical Center, San Diego, California
RECEIVED: 1 February 2005; FINAL SUBMISSION RECEIVED: 26 September 2005;ACCEPTED: 11 May 2006
The Journal of Emergency Medicine, Vol. 32, No. 1, pp. 71–85, 2007Copyright © 2007 Elsevier Inc.
Printed in the USA. All rights reserved0736-4679/07 $–see front matter
71
doi:10.1016/j.jemermed.2006.05.034
Selected Topics:Disaster Medicine
NUCLEAR/RADIOLOGICAL TERRORISM: EMERGENCY DEPARTMENTMANAGEMENT OF RADIATION CASUALTIES
Jerrold T. Bushberg, PhD,*† Linda A. Kroger, MS,* Marcia B. Hartman, MS,*Edwin M. Leidholdt Jr, PhD,†§ Kenneth L. Miller, MS,� Robert Derlet, MD,‡ and Cheryl Wraa, RN‡
*Department of Environmental Health and Safety, †Department of Radiology, ‡Department of Emergency Medicine, University ofCalifornia Davis Health System, Sacramento, California, §US Department of Veterans Affairs National Health Physics Program, Mare
Island, California, and �Department of Radiology, Penn State Hershey Medical Center, Hershey, PennsylvaniaReprint Address: Jerrold T. Bushberg, PhD, University of California Davis Health System, 2315 Stockton Blvd., FSSB 2500,

tional explosive (e.g., dynamite or a plastic explosive) tospread the radioactive material is called a “dirty bomb.”Although the initial explosion may kill or injure thoseclosest to the bomb, the radioactive material that isdispersed will likely expose and contaminate survivorsand emergency responders. Due to the limited dispersionby such an explosion, it is unlikely that the exposure orcontamination of people outside the immediate blast areawill have any clinical effect beyond the psychologicalimpact from the fear of radiation and perhaps a slightlyincreased risk of cancer. To date, there has been no useof an RDD; however, the materials to produce an RDDhave been intercepted by law enforcement (3).
An attack on or sabotage of a nuclear facility, such asa commercial irradiation facility or a nuclear powerplant, could release large amounts of radioactive mate-rial. Detonation of a nuclear weapon (even one with arelatively low energy yield) in a populated area wouldresult in extensive loss of life and widespread contami-nation. The use of a stolen or improvised nuclear deviceis the least likely scenario, due to the strict securitycontrols over nuclear weapons and weapons-grade plu-tonium and uranium and the technical difficulty of con-structing such a weapon, but the potential number ofinjured people is many times greater than from the otherscenarios. In the case of a nuclear weapon detonation oran event resulting in the dispersion of used nuclearreactor fuel, the radioactive contamination will consist ofmany radionuclides, including radioactive isotopes ofiodine.
In all scenarios involving the release of radioactivematerial, radioactive contamination would be present atthe site of the event. There may also be deposition ofradioactive material by a downwind plume. The amountof contamination deposited by the plume would dependupon the nature of the event, the amount of radioactivematerial released, and atmospheric conditions such aswind speed.
There are several scenarios, other than those causedby terrorism, in which radiation emergencies may occur.Some examples include medical radiation therapy acci-dents; accidental overexposures from industrial irradia-tors; lost, stolen, or misused medical or industrial radio-active sources; accidents during the transportation ofradioactive material; and nuclear reactor accidents. TheRadiation Emergency Assistance Center Training Site(REAC/TS) recorded 428 major radiation accidentsworldwide between 1944 and 2005, resulting in 126radiation-related deaths (4). Although these accidentswere infrequent, heightened awareness of the potentialimpact from terrorist activity has prompted many hospi-tals to reassess their preparedness for radiological emer-gencies.
IONIZING RADIATION AND RADIOACTIVEMATERIAL DEFINITIONS
Ionizing Radiation
Ionizing radiation, such as X- and gamma rays as well asalpha and beta particles, has the ability to ionize matter,causing chemical changes that can modify DNA and killcells. Throughout this article, the term radiation willrefer only to ionizing radiation. Radiation is a naturalpart of the environment. People are constantly exposed toradiation from their surroundings, (e.g., the earth itself,building materials, air, and water) as well as from cosmicrays. On average, persons in the United States receiveabout 300 millirem (mrem) of radiation per year fromnatural sources (5). People are also exposed to manmaderadiation from medical imaging (e.g., radiology and nu-clear medicine studies), medical therapy (e.g., cancertreatment), industry (e.g., soil moisture density gaugesand nuclear power plants), and research.
Radioactive Material
Radioactive material consists of atoms with unstablenuclei. The traditional unit of activity is the curie, de-fined in Table 1. Contamination of people usually in-volves microcurie (�Ci; one millionth of a curie) tomillicurie (mCi; one thousandth of a curie) quantities.Nuclear Medicine patients are injected with �Ci to mCiquantities of short-lived radioactive material for routinediagnostic examinations. The amount of radioactivitycontinuously decreases with time, a phenomenon re-ferred to as radioactive decay. The physical half-life isthe time required for radioactive material to be reducedto half the initial amount by radioactive decay. Theeffective half-life combines the physical half-life withbiological elimination (e.g., urination, defecation, exha-lation, and sweating). Most of the radionuclides that areconsidered likely to be used in an RDD (see below) havephysical half-lives of 5 years or more.
Two common types of radioactive decay are alphaparticle emission and beta particle emission. Alpha par-ticles travel very short distances (� 0.1 mm) and there-fore, are only harmful when alpha-emitting radionuclidesare inhaled, swallowed, or present in a wound. Some betaparticles can travel up to 10 meters or more in air and acentimeter or more in soft tissue. Thus, most beta-emit-ting radioactive materials, if allowed to remain on theskin for a prolonged period of time, can cause skininjury. Beta-emitting contaminants may also be harmfulif deposited internally. Gamma radiation and X-rays arealso emitted by many radioactive materials and travelmany meters in air and many centimeters in living tissue.
72 J. T. Bushberg et al.
Layers of dense materials, such as lead, are commonlyused to shield against gamma radiation and X-rays. Someof the radioactive materials considered likely to be usedin an RDD are the beta emitters cesium-137 (Cs-137),cobalt-60 (Co-60), iridium-192 (Ir-192), strontium-90(Sr-90), and iodine-131 (I-131), and the alpha emittersamericium-241 (Am-241), californium-252 (Cf-252),and plutonium (Pu) (1,6).
Quantities and Units for Describing Ionizing Radiation
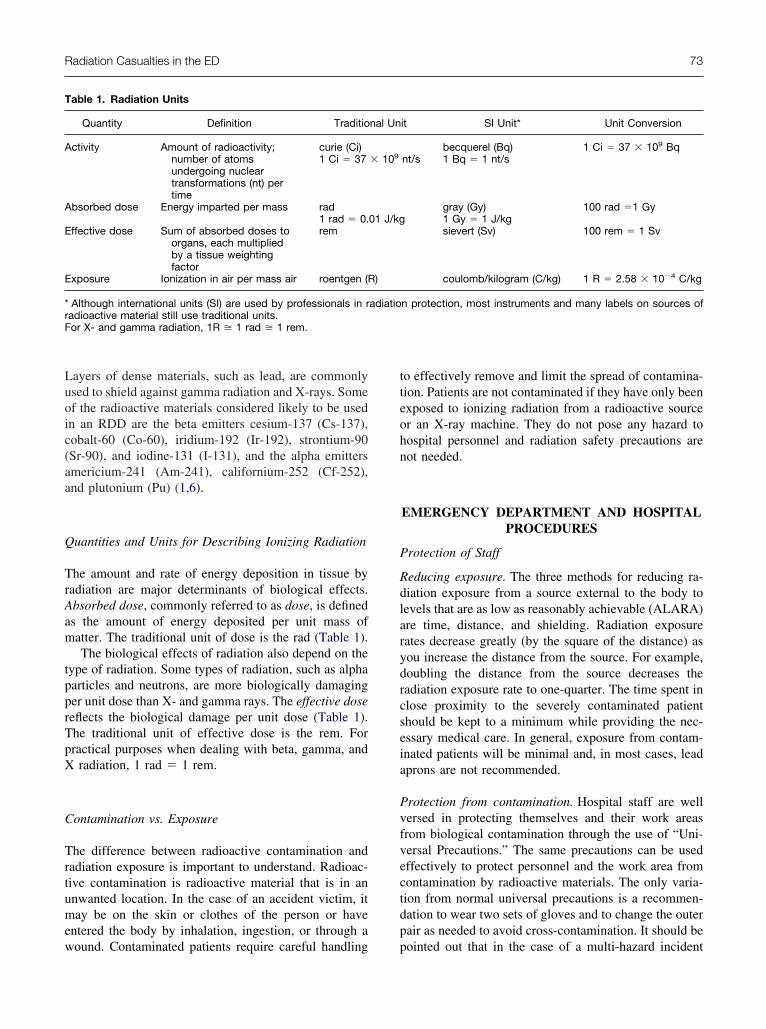
The amount and rate of energy deposition in tissue byradiation are major determinants of biological effects.Absorbed dose, commonly referred to as dose, is definedas the amount of energy deposited per unit mass ofmatter. The traditional unit of dose is the rad (Table 1).
The biological effects of radiation also depend on thetype of radiation. Some types of radiation, such as alphaparticles and neutrons, are more biologically damagingper unit dose than X- and gamma rays. The effective dosereflects the biological damage per unit dose (Table 1).The traditional unit of effective dose is the rem. Forpractical purposes when dealing with beta, gamma, andX radiation, 1 rad � 1 rem.
Contamination vs. Exposure
The difference between radioactive contamination andradiation exposure is important to understand. Radioac-tive contamination is radioactive material that is in anunwanted location. In the case of an accident victim, itmay be on the skin or clothes of the person or haveentered the body by inhalation, ingestion, or through awound. Contaminated patients require careful handling
to effectively remove and limit the spread of contamina-tion. Patients are not contaminated if they have only beenexposed to ionizing radiation from a radioactive sourceor an X-ray machine. They do not pose any hazard tohospital personnel and radiation safety precautions arenot needed.
EMERGENCY DEPARTMENT AND HOSPITALPROCEDURES
Protection of Staff
Reducing exposure. The three methods for reducing ra-diation exposure from a source external to the body tolevels that are as low as reasonably achievable (ALARA)are time, distance, and shielding. Radiation exposurerates decrease greatly (by the square of the distance) asyou increase the distance from the source. For example,doubling the distance from the source decreases theradiation exposure rate to one-quarter. The time spent inclose proximity to the severely contaminated patientshould be kept to a minimum while providing the nec-essary medical care. In general, exposure from contam-inated patients will be minimal and, in most cases, leadaprons are not recommended.
Protection from contamination. Hospital staff are wellversed in protecting themselves and their work areasfrom biological contamination through the use of “Uni-versal Precautions.” The same precautions can be usedeffectively to protect personnel and the work area fromcontamination by radioactive materials. The only varia-tion from normal universal precautions is a recommen-dation to wear two sets of gloves and to change the outerpair as needed to avoid cross-contamination. It should bepointed out that in the case of a multi-hazard incident
Table 1. Radiation Units
Quantity Definition Traditional Unit SI Unit* Unit Conversion
Activity Amount of radioactivity;number of atomsundergoing nucleartransformations (nt) pertime
curie (Ci)1 Ci � 37 � 109 nt/s
becquerel (Bq)1 Bq � 1 nt/s
1 Ci � 37 � 109 Bq
Absorbed dose Energy imparted per mass rad1 rad � 0.01 J/kg
gray (Gy)1 Gy � 1 J/kg
100 rad �1 Gy
Effective dose Sum of absorbed doses toorgans, each multipliedby a tissue weightingfactor
rem sievert (Sv) 100 rem � 1 Sv
Exposure Ionization in air per mass air roentgen (R) coulomb/kilogram (C/kg) 1 R � 2.58 � 10�4 C/kg
* Although international units (SI) are used by professionals in radiation protection, most instruments and many labels on sources ofradioactive material still use traditional units.For X- and gamma radiation, 1R � 1 rad � 1 rem.
Radiation Casualties in the ED 73

(e.g., radioactive materials and chemicals), higher levelsof personal protective equipment may be necessary.
Detection and measurement of radiation. Hospitals withNuclear Medicine or Radiation Oncology departmentshave radiation monitoring instruments. The ED shouldeither have its own or ready access to such instrumentsthat are properly maintained and calibrated. The EDtraining program should include instruction on instru-ment operation including the proper means of determin-ing the background levels. Background readings shouldbe taken in an area of the ED remote from the areas thatmay be contaminated. The most commonly used instru-ments to detect the presence of radioactive material andradiation are the Geiger-Mueller (GM) survey meter(also known as a Geiger counter) and the ionizationchamber survey meter (Figure 1). The GM survey meterwill detect small amounts of radioactive contaminationand typically has the capability of distinguishing be-tween alpha, beta, and gamma radiation. It is used toquickly determine if a person is contaminated and wherethe contamination is located. Ionization chamber surveymeters are used to measure exposure rates from low(mR/hr) to high (R/hr) levels of radiation. To determinethe exposure a person actually receives, the measuredexposure rate must be multiplied by the time that theperson was exposed. For example, if staff were caring for
a contaminated patient for 15 min and the ionizationchamber reading was 5 mR/hr, the staff would be ex-posed to 1.25 mR, less than the radiation exposure re-ceived from cosmic radiation during a cross-countryairplane flight (approximately 2.5 mrem). The averagenatural radiation dose to people living in the UnitedStates is 300 mrem per year. Other specialized equip-ment, such as multi-channel analyzers (MCA) that allowradionuclide identification, might only be available if thehospital has health physics or medical physics staff.
A personal dosimeter is a device that measures thedose of radiation received by the person wearing it. Filmbadge dosimeters must be sent for analysis so the radi-ation dose received is not known for several days. Self-reading dosimeters, although not as accurate as filmbadges, allow the wearer to see the total radiation dosethey have received at any time. Some of these areequipped with alarms that alert the wearer when a setpoint is exceeded. Ideally, both types of dosimetersshould be used by staff working directly with contami-nated patients.
Hospital Plan
The hospital should have a well-thought-out Radiologi-cal Emergency Medical Response Plan and should test itperiodically by drills. This may be part of the emergencymanagement plan required by the Joint Commission onAccreditation of Hospital Organizations (JCAHO) (7).There are several excellent documents that can assist inplan development (2,8–13). The plan should ensure thatthe medical care of the patient takes priority over decon-tamination. Resuscitation and stabilization are the pri-mary objectives, with decontamination efforts being sec-ondary. The plan should address contamination controlfor staff and facilities, including control and survey ofmaterials and personnel entering and leaving the contam-inated area (Table 2). Facility preparation depends on thetime available until patient arrival as well as the numberof patients expected. In situations involving other typesof hazardous materials, such as chemicals, decontamina-tion of the victims typically occurs before transportationto the ED. Although this approach may be appropriatefor some chemical and biological agents, it is unneces-sarily restrictive for radiological contamination, whichposes very little risk of harm to the emergency respond-ers. In addition, many casualties will likely self-refer tothe nearest hospital and therefore not be decontaminated.The hospital plan should specifically address the issueand provide for admission of critical patients directlyinto the ED or related services (e.g., CT, surgery) with-out decontamination if a delay would be life threatening.Emergency medical technicians should attempt to decon-
Figure 1. A GM survey meter (below) will detect smallamounts of radioactive contamination. It is useful in locatingcontamination and assessing the effectiveness of decon-tamination efforts. An ion chamber survey meter (above) willmeasure the exposure rate from X- and gamma radiation.
74 J. T. Bushberg et al.

trimri
awcOHatscpmswt
Eoctnpdfctroi
m
(ptsfebCohttctsitm
siitt(IsiaNilc
P
Qdvt(asrirb
T
A
P
C
Radiation Casualties in the ED 75
aminate the victims in the field if the patients are stable,emembering that medical management is the first prior-ty. Typically, 90% of radioactive contamination is re-
oved when the clothes are removed (14). What littleemains will likely stay in place if the patient is wrappedn a sheet and transported.
There should be a call list to notify the staff on duty,s well as to obtain additional staff and equipment thatill be needed. The additional support for the ED could
ome from hospital staff in Nuclear Medicine, Radiationncology, Diagnostic Radiology, and Radiation Safety/ealth Physics. If radiation safety personnel are avail-
ble, they will be a valuable asset in the management ofhe flow of people through the ED. They can performurveys of the accident victims, assist in contaminationontrol, and provide radiation dose assessment (15). Thelan should address where to obtain radiation surveyeters. Diligent use of survey meters by staff (e.g.,
urvey gloves and change as necessary, survey shoeshen leaving, etc.) will help prevent the spread of con-
amination (Figure 1).The plan should designate a triage area outside the
D. In this area, assessment can be made as to whetherr not a person needs to be seen in the ED (2,16). A massasualty incident involving radioactive material is likelyo generate large numbers of frightened people who doot require acute medical care (2,14). The plan shouldrovide for centers for assessment of minor injuries,econtamination, and counseling of these persons awayrom the ED so that the ED is not inundated. Theseenters should be staffed by physicians with radiologicalraining, health physicists or other staff trained to useadiation survey instruments, and psychological counsel-rs. The hospital should also plan to provide psycholog-cal support to patients and hospital staff.
Patient flow in the ED should be established in a
able 2. Facility Management of Radiological Emergencies
ctivate hospital planObtain radiation survey meters.Call for additional support; staff from Nuclear Medicine,
Radiation Oncology, Radiation Safety (Health Physics).Establish triage area.Establish area for decontamination of uninjured persons.
rotect staff from contaminationUse universal precautions and double glove.Survey hands and clothing with radiation survey meter.Replace gloves and gowns if contaminated and between
patients.Keep areas outside the treatment area free from
contamination.ontrol contaminationInstruct staff to use universal precautions.Provide multiple containers for contaminated waste.Protect the floor with covering if time permits.
anner that will control the spread of contamination N
Figure 2) (9,16,17). Several methods to consider are:lacing a floor covering on one side of the hallway fromhe ED entrance to the treatment room; designating aeparate entrance for contaminated patients; and trans-erring the contaminated patient to a clean gurney beforentering the ED. Ideally, the treatment room floor shoulde covered, but only if time allows for such an activity.ontainers for waste should be set up to limit the spreadf contamination. Compared to chemical and biologicalazards, one advantage of radioactive contamination ishe ease with which it can be detected. Frequent use ofhe GM survey meter can alert personnel of the need tohange their gloves or clothing when they become con-aminated and to identify when contamination is beingpread so that cleanup and extra precautions can bemplemented. Contamination in the ED may occur, buthis should not preclude the continued use of the treat-ent areas or equipment during the event.The plan should identify a laboratory that can assay
amples collected to assess external and internal contam-nation (Table 3). The laboratory should be capable ofdentifying the radionuclide(s) involved and estimatinghe amounts of radioactive material in the samples, par-icularly in regards to possible internal contaminationdiscussed below under “Assessment and Therapy fornternal Contamination”). A gamma-ray spectroscopyystem with an MCA is particularly useful for identify-ng radionuclides. A medical center with full time radi-tion safety staff will likely have this capability and auclear Medicine department can develop this capabil-
ty. Arrangements should be made in advance so that theaboratory can calibrate its equipment for the radionu-lides likely to be encountered and provide staff training.
PATIENT ASSESSMENT AND MANAGEMENTOF RADIOACTIVE MATERIAL
CONTAMINATION AND RADIATIONINJURIES
atient Assessment
uestions about the circumstances surrounding the inci-ent as well as a GM survey of the patient will providealuable patient management information and will fur-her assist in predicting the extent of radiation injury9,13,18). Although contamination surveys are second-ry to patient stabilization, they should be conducted asoon as possible. In the case of an RDD, very high doseates could exist if embedded shrapnel from the RDD isntensely radioactive, which is easily determined withadiation survey equipment. This type of shrapnel shoulde transferred to lead containers (readily available from
uclear Medicine departments and commonly referred
tcfccoa
tnovAf
Fu llow fo
76 J. T. Bushberg et al.
o as “pigs”) and placed distant from staff. Specimensollected for medical assessment can yield valuable in-ormation for treatment planning (Table 3). Samplesollected to assess contamination should be placed inontainers and labeled with the patient’s name, date, timef collection, and sample location. ED staff should be
igure 2. Patient flow through the ED. Familiarization of the Ese of periodic drills will maximize their effectiveness and a
ware that elevated radiation measurements from a pa- s
ient may be caused by radioactive material from a recentuclear medicine or radiation oncology procedure insteadf radioactive contamination from an event. Nausea andomiting are signs of exposure to a high radiation dose (seecute Radiation Syndrome section below), but such a dose
rom terrorist activities is unlikely. Consequently, if such
f to the hospital’s Emergency Management Plan through ther optimal care of the patients being seen.
D staf
ymptoms are present, they may be psychological in nature.

D
Dorwctrtuoeimawcc
ag
ftaerducTswri
ocftpEt
T
IB
B
U
WN
W
WU
F
A Site (Rp
Radiation Casualties in the ED 77
econtamination
econtamination should not delay or impede stabilizationf the patient (Table 4). Removal of clothing generallyeduces contamination on the patient by 90% (14). Usualashing methods are effective for removal of radioactive
ontamination. Non-contaminated wounds should be pro-ected with waterproof dressings to minimize uptake ofadioactive material during decontamination efforts. Con-aminated waste water need not be contained if it willnduly complicate the treatment of the patient or if it istherwise determined to be impractical. Decontaminationfforts should not cause the skin to become abraded. Open-ngs in the skin allow increased absorption of radioactiveaterial. If an area of contaminated skin persists, cover the
rea with gauze and a glove or plastic to promote sweating,hich can remove radioactive material from pores. Remove
ontaminated hair, if necessary, using scissors or electriclippers. To avoid cutting the skin, do not shave.
To decontaminate wounds, irrigate with tepid waternd gently wash with soap and a surgical sponge or
able 3. Specimens to be Collected for Medical Assessmen
Specimen/Type of Analysis Reason
n All Cases of Suspected Radiation Injurylood: CBC with differential lymphocytecount, repeated every 6 h for 48 h ifpossibility of total body irradiation.
To establish achange overdecrease inan early preddose. See Ta
lood: Chromosomal analysis Chromosomalmost accurathe radiationlabs are requtake several
rine: Routine urinalysis Determine normand baselineconstituents;important if icontaminatio
hen External Contamination is Suspectedose, ear, mouth: Swab body orifices.Analyze with GM probe, gamma orliquid scintillation counter, ormultichannel analyzer if available.
Assess the poscontaminatioradionuclide.
ounds: Samples from dressings orswabs of wounds. Analyze with GMprobe, gamma or liquid scintillationcounter, or multichannel analyzer ifavailable.
Assess if wouncontaminatedradionuclide.
hen Internal Contamination is Suspectedrine bioassay: 24-h specimen; repeat for4 days
Body excreta mradionuclidescontaminatio
eces bioassay: 24-h specimen; repeat for4 days
dapted from Radiation Emergency Assistance Center/Trainingatient, 2002, http://www.orau.gov/reacts/emergency.htm.
auze pad. Normal wound debridement can be per- b
ormed. Excision around wounds solely to remove con-amination should be performed only in extreme casesnd upon the advice of radiological emergency medicalxperts. Contaminated thermal burns can be gentlyinsed, but should not be scrubbed, to prevent furtheramage to the skin. Often, radioactive material will ex-de from wounds into gauze dressings, so frequenthanging of dressings may aid wound decontamination.he dressing also serves to keep the contamination frompreading. Cease decontamination of the skin andounds when the area is less than twice the background
eading on the GM survey meter or if there is no signif-cant reduction between washes.
Under no circumstances should emergency surgery orther necessary medical procedures be delayed due toontaminated skin or wounds. Staff will be protectedrom becoming contaminated by using universal precau-ions. Sheets and dressings will keep contamination inlace. When the patient is ready to be moved from theD to other areas of the hospital, the patient can be
ransferred to a clean gurney. The clean gurney can be
Patient Exposed to Radiation
taining Mechanism for Obtaining
e and assesssignificant
cyte count isf radiation
Veni-puncture in uncontaminated skin areainto purple top tube containing EDTA;cover puncture site.
s are theof estimatingSpecializedd resultsee Table 7
Veni-puncture in uncontaminated skin areainto lithium heparin tube; if that is notavailable, use an EDTA tube. Coverpuncture site.
ney functionnaryially
spected.
Avoid contamination when collectingsample. Label sample with date andtime of collection.
of internalidentify the
Use separate saline or water moistenedswabs to wipe the inside of each nostril,ear, and mouth. Label and bagseparately.
dentify theSave dressings as they are changed. Use
swabs to sample the secretions fromwounds. If foreign objects or debris areremoved from the wound or skin,transfer it to lead containers (pigs).
ntainrnaloccurred.
Use standard specimen containers.
EAC/TS) (4): Hospital emergency care of the radiation accident
t of a
for Ob
baselintime. A
lymphoictor oble 7
analysete waydose.ired andays. Sal kidfor uriespec
nternaln is su
sibilityn and
ds areand i
ay coif inte
n has
rought into the contaminated treatment room by rolling

iflwbr
A
DiiiotcrpfplFpgpppecbttn
satattfdeatpmmPcGdaDciRRpticDacg
T
12345
6
78911
11
78 J. T. Bushberg et al.
t over clean paper or other clean material placed on theoor. After the patient is transferred onto the gurney,rap a clean sheet around the patient and he or she cane transported throughout the hospital without spreadingadioactive contamination.
ssessment and Therapy for Internal Contamination
eposition of radioactive materials in the body (i.e.,nternal contamination), is a time-dependent, physiolog-cal phenomenon related to both the physical and chem-cal natures of the contaminant. Internal contaminationccurs mainly by inhalation, ingestion, or absorptionhrough wounds, although percutaneous absorption oc-urs with some radioactive materials. The fraction of theadioactive material that is absorbed into the body de-ends upon the radionuclide, chemical and physicalorm, and route into the body. For example, solublelutonium is readily absorbed into the body through theungs or a wound, but only very slightly if ingested.urthermore, the amount of radioactive material thatoses a significant threat if taken into the body variesreatly with radionuclide and chemical form. For exam-le, 100 �Ci of Cs-137 chloride in the body would notose a significant threat, but less than 1 �Ci of solublelutonium would. In many cases, early treatment is nec-ssary if it is to have much effect. Thus, time can beritical and treatment decisions may need to be madeased on preliminary information. If internal contamina-ion is suspected, plan for 24-h urine and fecal collec-ions (Table 3), but the decision to treat suspected inter-
able 4. Step-By-Step Patient Decontamination
. Do not delay surgery or other necessary medical procedures
. Carefully remove and bag patient’s clothing and personal be
. Survey patient and, if practical, collect samples.
. Handle foreign objects with care until proven non-radioactive
. PrioritiesA. Decontaminate wounds first then intact skin.B. Start with the highest levels of contamination.C. Protect non-contaminated wounds with water-proof dreD. Irrigate and gently scrub contaminated wounds with a sE. Extend wound debridement for removal of contaminationF. Change dressings frequently.
. Decontaminate thermal burns by gently rinsing. Aggressive wwill be removed when dressings are changed.
. Decontaminate intact skin and hair by washing with soap and
. Remove stubborn contamination on hair by cutting with sciss
. Promote sweating for residual skin contamination.0. Avoid overly aggressive decontamination.1. Cease decontamination of skin and wounds:
A. When the area is less than twice background, orB. When there is no significant reduction between deconta
2. Change outer gloves frequently to minimize spread of conta3. Use survey meter to monitor progress of decontamination.
al contamination should not be delayed until these a
amples are collected or analyzed (19). If an MCA isvailable, it will be a valuable tool to expedite the de-ermination of which decorporation therapy is appropri-te based on the radionuclide(s) present. Also, if inhala-ion of radioactive material is suspected, immediatelyake nasal swabs. A separate swab should be obtainedrom each nostril and placed in its own container. Ra-ioactivity on both nasal swabs should be consideredvidence of inhalation of radioactivity, but lack of radio-ctivity on the swabs should not lead to the presumptionhat such material was not inhaled. Several methods ofreventing incorporation (e.g., catharsis, gastric lavage)ight be applicable, depending on the type of radioactiveaterial present. NCRP (National Council on Radiationrotection) Report No. 65, Management of Persons Ac-identally Contaminated with Radionuclides (17), theuidebook for the Treatment of Accidental Internal Ra-ionuclide Contamination of Workers (20), and Guid-nce for Industry, Internal Radioactive Contamination—evelopment of Decorporation Agents (21) provide
linical guidance on the management of internal contam-nation. The NCRP is currently working on an update toeport No. 65 that will contain additional information.EAC/TS has medical experts on call 24 h a day torovide assistance with issues such as decorporation andreatment of exposed individuals (4). Some of the med-cations or preparations used in decorporation (trisodiumalcium-diethylenetriaminepentaacetate [Ca-DTPA], Zn-TPA, Prussian Blue, etc.) might not be available locally
nd should be stocked (or a source identified in theommunity) as part of the hospital’s Radiological Emer-ency Medical Response Plan (Table 5). The U.S. Food
minations; residual contamination can be controlled.s (typically removes 90% of contamination).
radiation survey meter.
sponge.in extreme cases and upon expert advice.
may increase the severity of injury. Additional contamination
r.electric clippers.
n efforts, and before the skin becomes abraded.on.
or exalonging
with a
ssings.urgical
only
ashing
wateors or
minatiominati
nd Drug Administration has stated that Prussian Blue is

s1fapitturt
A
Anpotmaw(rvtat(aayrpfei
fmDabtimmraapew
Sfepdt
igesfdtmMFpm
amsrbawic
L
Ri2esoattbbn
SpJT
Radiation Casualties in the ED 79
afe and effective in treating people exposed to cesium-37 and that Ca-DTPA and Zn-DTPA are safe and ef-ective for treatment of internally deposited plutonium,mericium, and curium (21). If it is suspected that theatient may have been exposed to radioiodine, potassiumodide (KI) should be administered to help protect thehyroid gland (Table 6) (17,20,22,23). It should be notedhat with the exception of KI, which is very effective ifsed early after exposure to radioiodines, most decorpo-ation agents will reduce the effective dose from radia-ion to the patient by a factor of only 3 or less.
cute Radiation Syndrome
cute radiation syndrome (ARS) (i.e., radiation sick-ess) is rare but may present as an acute illness inatients after exposure to very large doses (� 100 rem)f radiation. ARS is extremely unlikely to occur in staffreating patients who are contaminated with radioactiveaterial. ARS follows a roughly predictable course overperiod of time ranging from a few hours to severaleeks (Table 7) and is described in many references
9,14,24). The severity of the syndrome increases withadiation dose, amount of the body exposed (whole bodys. partial body exposure), and the penetrating ability ofhe radiation. The severity is also affected by factors suchs age, genetics, and medical conditions. If it is believedhat the victim may have received a high radiation dosee.g., � 50 rem), a complete blood cell count withbsolute lymphocyte count should be taken initially andbout every 6 h thereafter (Table 3). Chromosomal anal-ses of lymphocytes are performed by specialized labo-atories and typically require days for results to be re-orted. REAC/TS can assist with locating the appropriateacilities (4). Results of these tests may be used tostimate the radiation dose and the severity of radiationnjury.
The signs and symptoms that develop in ARS occur inour distinct phases: prodromal (initial), latent period,anifest illness stage, and recovery or death (Table 7).uring the prodromal phase, symptoms including loss of
ppetite, nausea, vomiting, fatigue, and diarrhea shoulde treated in a routine clinical manner. The severity andime of onset of symptoms should be recorded. For dosesn the range of 100–800 rem to most of the body, theanifest illness stage begins in less than 2 weeks and isainly caused by damage to the hematopoietic system,
esulting in decreased blood concentrations of leukocytesnd platelets, which cause an increased risk of infectionnd bleeding. For doses above about 800 rem, the latenteriod is on the order of 1 to 3 days and the primaryffects are due to damage to the lining of the intestines,
ith diarrhea, fever, sepsis, and electrolyte disturbances. turvival, even with medical treatment, is highly unlikelyor doses above about 1000 rem. For even higher doses,xceeding about 3000 rem, there is little or no latenteriod. The patient soon becomes confused, with severeiarrhea and hypotension, and death occurs in a day orwo.
Treatment of ARS should focus on prevention ofnfection. Antibiotics for neutropenia and fever should beuided by the recommendations of the Infectious Dis-ases Society of America (25). Routine gut prophylaxishould not be administered (24). Hematopoietic growthactors should be given within the first 24–48 h and thenaily. Patients with severe ARS will require hospitaliza-ion. Several books and papers provide guidance on theanagement of ARS (2,9,14,24). REAC/TS and theedical Radiobiology Assistance Team of the Armed
orces Radiobiology Research Institute (AFRRI) canrovide guidance 24 h a day on patient assessment andanagement of ARS (Table 8).Patients who have suffered trauma combined with an
cute high-level radiation exposure will have increasedorbidity as compared to patients who have received the
ame dose of radiation without trauma. If a patient haseceived an acute radiation dose � 100 rem, efforts muste made to close wounds, cover burns, reduce fractures,nd perform surgical stabilizing and definitive treatmentsithin the first 48 h after injury. After 48 h, surgical
nterventions should be delayed until hematopoietic re-overy has occurred.
ocal Radiation Injury
adiation exposure to parts of the body can cause local-zed effects if the dose is sufficiently high, typically �00 rem. The patient may not be aware that he or she wasxposed. Such a patient may have localized burn-likekin injuries without a history of heat exposure. Epilationf the exposed area may occur. These symptoms do notppear immediately but rather days after exposure. Aendency to bleed, nausea and vomiting or other symp-oms of ARS may be present. If a patient presents withurns immediately after a terrorist event, such as a dirtyomb, it is more likely that the burns are thermal burns,ot radiation burns.
OTHER HEALTH EFFECTS OF RADIATION
tudies of animals and epidemiologic studies of humans,articularly the survivors of the atomic bombings inapan, have shown that radiation is a weak carcinogen.he International Commission on Radiological Protec-
ion has estimated the lifetime risk of fatal cancer, for

Table 5. Substances Suitable for Decorporation Treatment
Medication Trade Name Elements Dosage Schedule*
RelativeEffectiveness with
Time Principle of Action Side Effects Contraindications
DTPA (diethylenetriaminepentaaceticacid, Ca or Zn) (21)
N/A Am, Cf, Cm, Pu Adults: 1 g/d by slowi.v. push orinfusion in 250 mL5% glucose.Inhalation in anebulizer: 1 g/d
Should be started assoon as possible.Efficacy greatestwithin 6 h ofexposure.
Chelation Monitor blood pressureduring infusion.Monitor for kidneyfunction, liverenzymes and signsof intestinal damage.Can be used forwound cleaning. Mayneed trace metalsupplements forprolonged therapy.
Ca-DTPAcontraindicated forpatients withkidney, intestinalor hematopoeiticdisorders,pregnant womenand minors.
Pediatrics (� 12years): 14 mg/kg/dby slow i.v. pushor infusion in 250mL 5% glucose
Ca-DTPA for initialtreatment (24 h)followed by Zn-DTPA forprotracted therapy.
KI (potassium iodide) Thyroblock, Iostatand others
I 130 mg/day oral† 50% effective at 6 h.Only 7% effectiveif given at 24h.
Blocking Angioedema ifsensitive to I; Treatw/ perchlorate, 1 �200 mg, then 100mg every 5 h.
Caution with goiterorhyperthyroidosis;Do not treat theelderly.
Prussian Blue (ferrichexacyanoferrate)(21)
Radiogardase Cs Adults andadolescents: 3grams orally threetimes daily.Pediatrics (2–12years): 1 gramorally three timesdaily.
Most effective whengiven promptly butcontinues to beeffective inpreventingrecycling ofradionuclide in theintestine.
Adsorption Constipation. Mayaffect absorption ofother medicationsincludingtetracycline.
Only effective if GImotility is intact.
A) Aluminumphosphates
A) Aluminumcontainingantacids
Sr A) 100 mL gel (13 g)oral
A & B) Mosteffective if givenimmediately.
A & B) Adsorption A&B) Constipation.Possible interactionswith othermedicationsincludingtetracycline.
A&B) Diabetics: Maycontain glucose.
B) Alginates B) Gaviscon B) 10 g oral then 4 gper day
C) NH4Cl (ammoniumchloride) plusCalcium gluconate
C) 1–2 g NH4Cl every6 h oral plus 500mg Ca gluconatein 500 mL 5%glucose in waterover 4 h i.v.
C) Still effective upto 2 wks afterexposure.
C) De-mineralization C) Gastric irritation. C) Ca gluconateshould not begiven to patientswith heartconditions.
80J.T.B
ushbergetal.

wbtr
brsalat0n1
n(ctoo(irDcbaa(
TltsaaMdphabEatsrb
le5.
(Co
ntin
ued
)
Med
icat
ion
Trad
eN
ame
Ele
men
tsD
osag
eS
ched
ule*
Rel
ativ
eE
ffec
tiven
ess
with
Tim
eP
rinci
ple
ofA
ctio
nS
ide
Eff
ects
Con
trai
ndic
atio
ns
HC
O3
(sod
ium
icar
bon
ate)
N/A
U4
gor
alin
itial
ly;
2g
ever
y4
hun
tilur
ine
pH
of8–
9is
mai
ntai
ned
.
Com
ple
xatio
nN
one
nici
llam
ine
Cup
rimin
e,D
epen
Hea
vyM
etal
sin
clud
ing
Cu,
Fe,
Hg,
Pb
,A
u,P
o
250–
1500
mg
ever
y8
hor
alC
hela
tion
Mac
ulop
apul
aror
eryt
hem
atou
sra
sh,
mar
row
sup
pre
ssio
n,ki
dne
yfu
nctio
n,im
mun
e-re
late
dd
isea
ses.
onsu
ltR
EA
C/T
S(4
)or
the
Phy
sici
ans
Des
kR
efer
ence
(PD
R)
for
info
rmat
ion
onp
edia
tric
dos
ages
not
pro
vid
ed.
eeTa
ble
6fo
rad
diti
onal
info
rmat
ion.
Radiation Casualties in the ED 81
orking age adults exposed to low doses of radiation, toe about 5 � 10�4 deaths per rem (26). For doses likelyo be received by staff in the ED (� 1 rem), the increasedisk of cancer is minimal.
Radiation-induced hereditary (genetic) effects haveeen demonstrated in animals, but direct evidence ofadiation-induced hereditary effects has not been ob-erved in any of the studies of humans exposed to radi-tion, even after high doses of radiation (27). For dosesikely to be received by staff, the risk is minimal. Usingtheoretical model, the increased risk of genetic effects
o children of young emergency responders would be �.02% from 5 rem and � 0.2% from 50 rem (27). Theatural incidence of genetic disease and malformations atto 2 years of age is 6–10% (28).Studies of animals and humans have shown that pre-
atal radiation exposure can cause teratogenic effects27,29–31). However, there is no evidence of an in-reased incidence of such effects for doses � 10 rem tohe embryo or fetus. Also, some epidemiological studiesf humans indicate that radiation-exposure to the embryor fetus may increase the incidence of post-natal cancer29). Although it is quite unlikely that someone provid-ng care for a radioactively contaminated patient wouldeceive a large dose, as a precaution, the Centers forisease Control and Prevention (CDC) recommends ex-
luding pregnant staff from such cases whenever possi-le (8). Fetal doses would have to be � 10 rem beforebortions were considered and, then, only on advice fromphysician with expertise on radiation and pregnancy
32).
RADIATION DOSE LIMITS FOREMERGENCY WORKERS
here are several recommendations for radiation doseimits to emergency workers performing lifesaving ac-ions. Although the U.S. Nuclear Regulatory Commis-ion does not have a limit for emergency lifesavingctions (i.e., immediate response to a life or death situ-tion), the National Council on Radiation Protection andeasurements (5) and the International Council on Ra-
iation Protection (26) recommend that doses can ap-roach or exceed 50 rem. Although this dose is 10 timesigher than annual occupational dose limit, it representsmodest increase in cancer risk compared to the large
enefit to the recipients of the lifesaving measures.mergency workers should perform these lifesavingctivities voluntarily and with prior training regardinghe risks of exposure. It is unlikely that the dose to EDtaff would approach these levels. The doses ED staffeceived after the Chernobyl accident were � 1 rem
(12).Ta
Na b
Pe
*C
†S

IciAmfnatpowNFbbnpgbnrp
IttnpuAci
M
oo(jptumssriaaqaeSRpbpi
dtarEtpIidd
ss
T
AAPAC1B
*i 130 m† the full
82 J. T. Bushberg et al.
FACILITY RECOVERY
f the efforts made during facility preparation were suc-essful, facility recovery should be relatively easy. Dur-ng facility recovery, employee exposures should be keptLARA. If available, an in-house radiation safety staffember will supervise decontamination efforts. Waste
rom the ED and triage area should be taken to a desig-ated holding location until it can be surveyed for radio-ctive material before disposal. Some facilities have por-al radiation monitors to survey hospital trash. Theyrovide a quick method that can replace hand surveyingf each bag of waste. A radiation survey of the facilityill identify any surfaces that require decontamination.ormal cleaning methods are typically very effective.acilities should be decontaminated to the extent possi-le. Gloves, shoe covers, and coveralls should be worny people decontaminating the area. For some contami-ated items, replacement may be more cost effective andractical than decontamination. The decontaminationoal for surfaces is to have less than twice the normalackground reading. Areas that cannot be decontami-ated to this level should be referred to health physics oradiation safety specialists. There are companies that canerform decontamination services.
SUMMARY
n a radiological emergency, medical stabilization andreatment of the patient take priority over decontamina-ion efforts. Radiation exposure and contamination areot likely to be significant hazards to staff. Staff canrotect themselves from radioactive contamination bysing universal precautions while treating these patients.s opposed to patients who arrive contaminated with
hemical or biological agents, radioactive contaminations easy to detect.
Every hospital should have a Radiological Emergency
able 6. Thyroid Radioiodine Predicted Dose Threshold for
Predicted ThyroidDose (rad) KI Dose
dults over 40 years �500 13dults 18–40 years �10 13regnant or lactating women �5 13dolescents 12–18 years† �5 6hildren 3–12 years �5 6mo–3 years �5 3irth–1 month �5 1
Take tablet or fraction of tablet orally once a day. Crush for sman place of tablets. SSKI contains 1 gm of KI per mL of solution.
Adolescents approaching adult size (� 70 kg) should receive
edical Response Plan that will allow effective handling r
f contaminated and injured patients. JCAHO requiresrganizations to have an emergency management plan7). There are many resources available including books,ournal articles, and internet sites that will be useful inreparing a hospital emergency plan (Table 8). Testinghe plan through periodic drills (e.g., annually) and thetilization of an effective training program (Table 8)inimizes the potential for apprehension and panic
hould activation of the plan ever be needed. The planhould address patient assessment and management ofadioactive contamination and radiation injuries. Train-ng should emphasize that resuscitation and stabilizationre the most important aspects of treating the radiationccident victim(s). Preparations should ensure that ade-uate supplies and radiation survey instruments arevailable. Non-ED staff who can assist in a radiologicalmergency should be identified and trained in advance.taff from Nuclear Medicine, Radiation Oncology, andadiation Safety have expertise in radiation protectionractices and the use of survey meters. Measures shoulde taken to prevent the “worried well” and uninjuredeople with radioactive contamination from overwhelm-ng the ED and hindering patient care.
Most victims of a mass casualty event involving ra-ioactive material will arrive at the ED with little con-amination. ED staff are likely to receive far less than thennual occupational dose limit of 5 rem. The long-termisks from radiation exposures of � 5 rem are very low.ven in an extreme case involving radiation casualties,
he Chernobyl nuclear reactor accident in 1986, medicalersonnel working on the victims received � 1 rem (12).n the case of an RDD, very high dose rates could existf embedded shrapnel from the RDD was intensely ra-ioactive. This unlikely possibility would be easy toetermine with radiation survey instruments.
Most victims of radiation accidents will show no signs orymptoms of radiation exposure due to their small expo-ures. In the rare instance when victims have received large
istration of KI for Different Risk Groups (22)
Number of 130 mg Tablets* Number of 65 mg Tablets*
1 21 21 2
1/2 11/2 11/4 1/21/8 1/4
ren. Saturated Solution of Potassium Iodide (SSKI) can be usedg of SSKI � 0.13 mL, or approximately 3 drops. Dilute in juice.adult dose (130 mg).
Admin
(mg)
0005526
ll child
adiation doses, early signs and symptoms and their inten-

Table 7. Phases of Acute Radiation Syndrome
Phase ofSyndrome Feature
Effects of whole-body irradiation, from external radiation or internal absorption, by dose range in rad (1 rad � 1cGy; 100 rad � 1Gy)
0–100 100–200 200–600 600–800 800–3000 � 3000
Prodromal Nausea, vomiting None 5–50% 50–100% 75–100% 90–100% 100%Time of onset 3–6 h 2–4 h 1–2 h � 1 h MinutesDuration � 24 h � 24 h � 48 h � 48 h N/ALymphocyte count Unaffected Minimally decreased � 1000 at 24 h � 500 at 24 h Decreases within
hoursDecreases within hours
CNS function No impairment No impairment Routine task performance Simple, routine taskperformance
Rapid incapacitation
Cognitive impairment for6–20 h
Cognitiveimpairment for �24 h
May have a lucid interval of several hours
Latent No symptoms � 2 weeks 7–15 days 0–7 days 0–2 days NoneManifest illness Signs, symptoms None Moderate
leukopeniaSevere leukopenia, purpura, hemorrhage,
pneumonia, hair loss over 300 radDiarrhea, fever,
electrolytedisturbance
Convulsions, ataxia,tremor, lethargy
Time of onset � 2 weeks 2 days–2 weeks 1–3 daysCritical period None 4–6 wk; greatest potential for effective medical
intervention2–14 d 1–48 h
Organ system None Hematopoietic, respiratory (mucosal) systems GI tract, Mucosalsystems
CNS
HospitalizationDuration
0% � 5% 45–60 days 90% 60–90 days 100% 90� days 100% Weeks tomonths
100% Days to weeks
Mortality None Minimal Low with aggressivetherapy
High Very high; significant neurological symptomsindicate lethal dose
From (14): Military Medical Operations Armed Forces Radiobiology Research Institute. Medical Management of Radiological Casualties Handbook, 2nd edn. April 2003. Available at:http://www.afrri.usuhs.mil.
Radiation
Casualties
inthe
ED
83

sicArscv
Al
1
1
1
T
O
B
B
84 J. T. Bushberg et al.
ities will be an indication of the severity of the radiationnjury. The first 24 h after an incident will be the mosthallenging for those involved in the emergency response.fter the first day, there will likely be many additional
esources arriving from state and federal agencies. Under-tanding basic radiation protection principles will aid theare providers in effectively and efficiently managing theictims of radiation accidents.
cknowledgments—We thank Fred A. Mettler, Jr, MD and Wil-iam E. Dickerson, MD for their reviews of this manuscript.
REFERENCES
1. Ferguson, CD, Potter WC. In: Donohoe LS, ed. The four faces ofnuclear terrorism. Monterey, CA: Monterey Institute of Interna-tional Studies; 2004:10–12.
2. National Council on Radiation Protection and Measurements. Re-port No. 138. Management of terrorist events involving radioactivematerials. Bethesda, MD: NCRP Publications; 2001.
3. Center for Nonproliferation Studies at the Monterey Institute ofInternational Studies. Radiological terrorist tutorial: history of ra-diological terrorism. Available at: http://www.nti.org/h_learnmore/
able 8. Resources
rganizationsRadiation Emergency Assistance Center/ Training Site (REACCenters for Disease Control (CDC)
Medical Radiobiology Advisory Team (MRAT) of the ArmedForces Radiobiology Research Institute (AFRRI)
ooksMedical Management of Radiation Accidents. Gusev, GuskovMedical Effects of Ionizing Radiation. Mettler and Upton, SauThe Medical Basis for Radiation-Accident Preparedness. REANational Council on Radiation Protection and Measurements.Distribution and Administration of Potassium Iodide in the Ev
(http://books.nap.edu/catalog/10868.html). 2004.ooklets/articlesDisaster Preparedness for Radiology Professionals, Response
Preparedness Primer)Guidebook for the Treatment of Accidental Internal RadionucDepartment of Health and Human Services, Food and Drug A
Contamination—Development of Decorporation Agents, MaDepartment of Homeland Security Working Group on Radiolo
docs/Radiologic_Medical_Countermeasures_051403.pdf), 2Interim Guidelines for Hospital Response from a Radiological
(http://www.bt.cdc.gov/radiation/pdf/MassCasualtiesGuidelMajor radiation exposure—what to expect and how to responMedical management of the acute radiation syndrome: recom
group. Waselenko JK, MacVittie TJ, Blakely WF, et al. AnnMedical Management of Radiological Casualties Handbook, (OSHA Best Practices for Hospital-Based First Receivers of V
Hazardous Substances, http://www.osha.gov/dts/osta/bestTraining programEmergency department management of radiation casualties.
2004.
radtutorial/chapter03_01.html. Accessed May 22, 2006.4. Oak Ridge Institute for Science and Education. Radiation Emer-
1
gency Assistance Center/Training Site (REAC/TS). Available at:www.orau.gov/reacts/ Accessed May 22, 2006.
5. National Council on Radiation Protection and Measurements. Re-port No. 116. Limitation of exposure to ionizing radiation. Be-thesda, MD: NCRP Publications; 1993.
6. Centers for Disease Control and Prevention, Department of Healthand Human Services. Radioactive isotopes. Available at: http://www.bt.cdc.gov/radiation/isotopes/. Accessed May 22, 2006.
7. Joint Commission on Accreditation of Healthcare Organizations.The 2004 Joint Commission accreditation manual for hospitals.Oakbrook Terrace, IL. Joint Commission on Accreditation ofHealthcare Organizations; 2004.
8. Centers for Disease Control and Prevention, Department of Healthand Human Services. Interim guidelines for hospital response tomass casualties from a radiological incident. Available at: www.bt.cdc.gov/radiation/pdf/masscasualtiesguidelines.pdf. AccessedMay 22, 2006.
9. Mettler FA. In: Gusev IA, Guskova AK, Mettler FA, eds. Medicalmanagement of radiation accidents, 2nd edn. Boca Raton, FL: CRCPress; 2001:425–35.
0. Bushberg JT, Miller, KL. Hospital responses to radiation casual-ties. In: Brodsky A, Johnson RHJr, Goans RE, eds. Public protec-tion from nuclear, chemical and biological terrorism. Madison, WI:Medical Physics Publishing; 2004:445–60.
1. Occupational Safety and Health Administration. OSHA bestpractices for hospital-based first receivers of victims from masscasualty incidents involving the release of hazardous sub-stances. Available at: http://www.osha.gov/dts/osta/bestpractices/firstreceivers_hospital.html. Accessed May 22, 2006.
2. Mettler FA, Voelz GL. Major radiation exposure—what to expectand how to respond. N Engl J Med 2002;346:1554–61.
(865) 576-1005 www.orau.gov/reacts(888) 246-2675 www.bt.cdc.gov/radiation/links.asp(888) 246-2857 (Spanish)
(301) 295-0530 www.afrri.usuhs.mil
Mettler, CRC Press, 2001.1995.onference, 2002.
t Nos. 65 and 138.Nuclear Incident, National Academy of Sciences
diological Terrorism (http://www.acr.org and search Disaster
ntamination of Workers. Radiation Dosimetry, 41:1–49, 1992.tration, Guidance for Industry Internal Radioactive06 (http://www.fda.gov/cder/guidance/index.htm)ispersal Device Preparedness, (http://www1.va.gov/emshg/
nt,f), 2003.tler FA, Voelz GL. N Engl J Med 2002;346:1554–61.tions of the strategic national stockpile radiation working
Med 2004;140:1037–51.ww.afrri.usuhs.mil), 2003.
from Mass Casualty Incidents Involving the Release ofes/firstreceivers_hospital.html), 2004.
rg JT, et al. (http://hps.org/hsc/documents/emergency.ppt),
/TS)
a andnders,C/TS CRepor
ent of a
to Ra
lide Codminisrch 20gical D003.Incideines.pdd. MetmendaInternhttp://wictimspractic
Bushbe
3. International Atomic Energy Agency and World Health Organization.Generic procedures for medical response during a nuclear or radio-

1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
Radiation Casualties in the ED 85
logical emergency. Available at: http://www-pub.iaea.org/MTCD/publications/PDF/EPR-MEDICAL-2005_web.pdf. Accessed May 22,2006.
4. Armed Forces Radiobiology Research Institute. Medical manage-ment of radiological casualties, 2nd edn. Bethesda, MD: ArmedForces Radiobiology Research Institute; 2003. Available at: www.afrri.usuhs.mil. Accessed May 22, 2006.
5. Toohey RE. Role of the health physicist in dose assessment. In:Ricks RC, Berger ME, O’Hara, Jr. FM, eds. Medical basis forradiation-accident preparedness. New York: The Parthenon Pub-lishing Group, Inc.; 2002:33–43.
6. Miller KL. The regional approach to management of radiationaccident victims. In: Vince MA, ed. Coping with radiation acci-dents. Ravenna: Envirotox Management, Inc.; 1990:121–30.
7. National Council on Radiation Protection and Measurements. Re-port No. 65. Management of persons accidentally contaminatedwith radionuclides. Bethesda, MD: NCRP Publications; 1979.
8. Miller KL, DeMuth WE. Handling radiation emergencies: no needto fear. J Emerg Nurs 1983;9:3141–4.
9. Berger ME, Jones OW, Ricks RC, Garrett S. Decontaminating thenasal passages. Health Phys 2003:84(5 Suppl):S80–2.
0. Gerber GB, Thomas RG, eds. Guidebook for the treatment ofaccidental internal radionuclide contamination of workers. RadiatProt Dosimetry 1992:41:5–49.
1. U.S. Department of Health and Human Services, Food and DrugAdministration. Guidance for industry, internal radioactive con-tamination—development of decorporation agents. Available at:http://www.fda.gov/cder/guidance/6983fnl.htm. Accessed May 22,2006.
2. U.S. Department of Health and Human Services, Food and Drug
Administration. Guidance: potassium iodide as a thyroid blockingagent in radiation emergencies. Available at: http://www.fda.gov/cder/guidance/4825fnl.htm. Accessed May 22, 2006.
3. National Research Council of the National Academies. Distribu-tion and administration of potassium iodide in the event of anuclear incident. Washington, DC: The National Academies Press;2004.
4. Waselenko JK, MacVittie TJ, Blakely WF, et al. Medical manage-ment of the acute radiation syndrome: recommendations of thestrategic national stockpile radiation working group. Ann InternMed 2004;140:1037–51.
5. Hughes WT, Armstrong D, Bodey GP, et al. 1997 Guidelines forthe use of antimicrobial agents in neutropenic patients with unex-plained fever. Clin Infect Dis 1997;25:551–73.
6. International Commission on Radiological Protection. Publication60: 1990 Recommendations of the international commission onradiological protection. New York: Elsevier Science; 1990.
7. United Nations Scientific Committee on the Effects of AtomicRadiation (UNSCEAR). Hereditary effects of radiation, report tothe General Assembly, with scientific annexes No. E.01.1X.2. NewYork. United Nations; 2001:1–2.
8. Mossman KL, Hill LT. Radiation risks in pregnancy. Obstet Gy-necol 1982;60:237–42.
9. Doll R, Wakeford F. Risk of childhood cancer from fetal irradia-tion. Br J Radiol 1997;70:130–9.
0. Hall EJ. Radiobiology for the radiologist, 5th edn. Philadelphia:Lippincott Williams & Wilkins; 2000:189–91.
1. Mettler FA, Upton AC. Medical effects of ionizing radiation, 2nd
edn. Philadelphia: WB Saunders, 1995:329.2. Annals of the International Commission on Radiological Protec-
tion. Publication 84. Pregnancy and medical radiation. Tarrytown,
NY: Elsevier Science Inc.; 2000.