Embed Size (px)
Citation preview

1
NSW Institute of Trauma and Injury Management
NSW Major Trauma Retrieval
& Transfers
Consensus guidelines

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines ii
1
AGENCY FOR CLINICAL INNOVATION 2
Level 4, Sage Building 3 67 Albert Avenue 4 Chatswood NSW 2067 5
PO Box 699 Chatswood NSW 2057 6 T +61 2 9464 4666 | F +61 2 9464 4728 7 E [email protected] | www.aci.health.nsw.gov.au 8
SHPN (ACI) XXXXX, ISBN XXX-X-XXXXX-XXX-X. 9
Produced by: Institute of Trauma and Injury Management. 10
Further copies of this publication can be obtained from 11 the Agency for Clinical Innovation website at www.aci.health.nsw.gov.au 12
Suggested citation: NSW Institute of Trauma and Injury Management. NSW Major Trauma Retrieval and Transfers: 13 Consensus Guidelines. Sydney: NSW Agency for Clinical Innovation, 2017. 14
Disclaimer: Content within this publication was accurate at the time of publication. This work is copyright. It may be 15 reproduced in whole or part for study or training purposes subject to the inclusion of an acknowledgement of the source. 16 It may not be reproduced for commercial usage or sale. Reproduction for purposes other than those indicated above 17 requires written permission from the Agency for Clinical Innovation. 18
Version: 01 Trim: ACI/D16/5910 19
Date Amended: XX/XX/XXXX 20
© Agency for Clinical Innovation 201X 21
The Agency for Clinical Innovation (ACI) works with clinicians, consumers and managers to design and promote better healthcare for NSW. It does this by:
service redesign and evaluation – applying redesign methodology to assist healthcare providers and consumers to review and improve the quality, effectiveness and efficiency of services
specialist advice on healthcare innovation – advising on the development, evaluation and adoption of healthcare innovations from optimal use through to disinvestment
initiatives including guidelines and models of care – developing a range of evidence-based healthcare improvement initiatives to benefit the NSW health system
implementation support – working with ACI Networks, consumers and healthcare providers to assist delivery of healthcare innovations into practice across metropolitan and rural NSW
knowledge sharing – partnering with healthcare providers to support collaboration, learning capability and knowledge sharing on healthcare innovation and improvement
continuous capability building – working with healthcare providers to build capability in redesign, project management and change management through the Centre for Healthcare Redesign.
ACI Clinical Networks, Taskforces and Institutes provide a unique forum for people to collaborate across clinical specialties and regional and service boundaries to develop successful healthcare innovations.
A priority for the ACI is identifying unwarranted variation in clinical practice and working in partnership with healthcare providers to develop mechanisms to improve clinical practice and patient care.
www.aci.health.nsw.gov.au

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines iii
Prelude 1
The NSW Major Trauma Retrieval and Transfers consensus guidelines have been developed to 2
assist clinicians in providing a more selective, evidence-based approach to the management of 3
major trauma patients. 4
These consensus guidelines aim to provide all hospitals with a standardised set of criteria to 5
support transfer agreements within their networks for the identification and transfer of trauma 6
patients as necessary. This document sets out suggested criteria for early consultation and 7
transfer; however, these may vary with the level of clinical services available at individual hospitals 8
These guidelines are intended for use by staff involved in the care and/or coordination of adult and 9
paediatric major trauma patients requiring inter-hospital retrieval or transfer during the acute phase 10
of trauma management. 11
12

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines iv
Algorithm 1
Any time urgent
critical trauma transfer
criteria?
Contact ACC/NETS within 30mins of arrival for time urgent medical consult or retrieval to the
nearest appropriate Trauma Service
Any non-time urgent
critical trauma transfer criteria?
Complete initial trauma assessment
Any high risk
mechanism of injury or comorbities?
No
Provide required care at local hospital. Reassess need for transfer.
Early consult as required
Conduct primary survey
Consult with networked Trauma Service / Patient Flow Units or the ACC/NETS for non-time
urgent medical retrieval to the nearest appropriate Trauma Service
Medical Retrieval team to consider activation of Code Crimson pathway
Yes
No
Perform complete trauma assessment and observe. If any clinical deterioration, early consult with
networked Trauma Service / Patient Flow Units for potential transfer to nearest appropriate Trauma
Service
Interhospital Transfer of Major Trauma Patients
Yes
No
ACC*: 1800 650 004
NETS#: 1300 36 2500
Perform complete trauma assessment and observe. If any clinical deterioration, early consult with
networked Trauma Service / Patient Flow Units for potential time urgent transfer to nearest
appropriate Trauma Service
Currently at a Regional Trauma Service?
Yes
No
Any time urgent
critical trauma transfer
criteria?
Contact networked Trauma Service, and ACC/NETS for time urgent consultation or medical retrieval to
the nearest appropriate Trauma Service within 30mins of arrival.
Medical Retrieval team to consider activation of Code Crimson pathway
Yes
No
Currently at a Major Trauma Service?
Provide required care. Consider need for transfer for specialty care
including burns, spinal and paediatrics. Early consult as required
Yes
No
Any non-time urgent
critical trauma transfer Criteria or high risk
mechanism of injury or comorbities?
Yes
Perform complete trauma assessment and observe. If any clinical deterioration, early consult with
networked Trauma Service / Patient Flow Units for potential transfer to nearest appropriate Trauma
Service
No
Provide required care. Consider need for transfer for specialty care
including burns, spinal and paediatrics. Early consult as required
Yes
Aeromedical Control Centre*
Newborn and paediatric Emergency Transport Service#
2

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines v
Time Urgent Critical trauma consult and/or transfer criteria 1
SIGNS AND SYMPTOMS (AFTER INITIAL ASSESSMENT, TREATMENT, CLINICAL DETERIORATION OR SYMPTOMS NOT IMPROVING)
AIRWAY:
Requiring Intubation At risk airway,
hoarseness, stridor
BREATHING:
Respiratory compromise
Hypoxia, cyanosis Pa02 <60 or PaC02
>60 or pH < 7.2 or BE <-5
CIRCULATION:
Severe haemorrhage Haemodynamic
instability Requiring blood
transfusion for resuscitation
Ongoing significant bleeding
DISABILITY:
Lateralising signs Falling GCS Paralysis/sensory
deficit
AGE TERM – 3M 4 – 12 MTHS 1 – 4 YRS 5 – 12 YRS 12+ YRS ADULT
HR <100 or >180 <100 or >180 <90 or >160 <80 or >140 <60 or >130 <40 or >140
RR >60 >50 >40 >30 >30 <10 or >30
BP SYS <50 <60 <70 <80 <90 <90
SPO2 <90% <90%
GCS <15 <13
INJURIES (SUSPECTED OR ACTUAL)
PENETRATING INJURIES
Serious Penetrating injuries to the head, neck, torso or abdomen
HEAD (REQUIRING URGENT NEUROSURGICAL CONSULTATION)
Intracranial FB / Open Fracture Depressed or complex skull fracture Lateralising signs Traumatic intracranial haemorrhage
NECK / SPINAL CORD / VERTEBRAL COLUMN
Unstable vertebral column injury Spinal cord injury (to spinal cord injury unit as per SSCIS)
Peripheral neurological deficit in suspected spinal cord or vertebral column injury Aerodigestive injury (larynx, trachea, oesophagus) Major vascular injury (carotid artery, vertebral artery, internal jugular vein)
CHEST
Any injury involving mediastinum or great vessels Major thoracic cage injury e.g. flail chest Massive haemothorax (>1,000ml)
ABDOMEN / PELVIS
Complex or open pelvic fracture Severe or complex solid organ or hollow viscous injury suspected Haemoperitoneum on FAST Urogenital injury
LIMBS / EXTREMITIES
Major limb amputation Major crush injury Fracture/dislocation with neurovascular compromise Penetrating limb injury with neurovascular compromise
BURNS
Severe Burns (refer to State-wide burns transfer guidelines)
SECONDARY DETERIORATION
Deteriorating condition requiring prolonged ICU e.g. sepsis with multiple injury Organ failure: single or multiple Major tissue necrosis

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines vi
Non-Time Urgent critical trauma consult and/or transfer criteria 1
INJURIES (SUSPECTED OR ACTUAL)
PENETRATING INJURIES
Penetrating injuries to the limbs (excluding isolated minor injury to hands or feet)
HEAD (REQUIRING URGENT CT SCAN)
Loss of consciousness or persistent amnesia (failed A-WPTAS after 4 hours) Signs or suspicion of signs of base of skull fracture or skull fracture
2 or more vomits or a seizure
NECK / SPINE
Stable vertebral injury (single column injury) Swelling, bruising, haematoma, hoarseness or stridor
CHEST
Seatbelt abrasions / contusions Pneumothorax/haemothorax 3 or more rib fractures or flail segment ECG changes
ABDOMEN / PELVIS
Seatbelt abrasions / contusions Severe pain, rigidity, swelling, Pelvic fracture Solid organ injury (AAST Grade I, II or III liver, spleen, pancreas or kidneys)
LIMBS / EXTREMITIES
2 or more proximal long bone fractures Open fracture of long bone
MULTIPLE SYSTEM
Injury to >2 body systems (minor)
OTHER TRAUMA TRANSFER CRITERIA
Head or torso and pelvic injuries without evidence of time critical or complex features (above)
High-risk mechanism of injury or comorbidities 2
HIGH-RISK MECHANISM OF INJURY
BLUNT TRANSPORT INCIDENT
Death in same vehicle Steering wheel deformity Vehicle vs. pedestrian/cyclist/motor bike Ejection from vehicle Entrapment with compression
BLUNT OTHER INCIDENTS
Focal blunt trauma to head or torso Falls > 3m or paediatrics twice the child’s height High voltage injury Crush injury Drowning
COMORBIDITY FACTORS ASSOCIATED WITH ANY INJURY
Patients <16 years of age Patients >65 years of age Obstetric patients >20 weeks gestation Patients on anticoagulants Immunosuppression Cardio, respiratory or chronic disease Morbid obesity
Alcohol or Illicit Drug use
3 4
NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines vii
Acknowledgements 1
NSW Institute of Trauma and Injury Management (ITIM) 2
Assoc. Prof. Michael Dinh, Clinical Director 3 Ms Christine Lassen, Manager 4 Mr Glenn Sisson, Project Officer 5 Ms Kelly Dee, Clinical Review Officer 6 Dr Pooria Sarrami, Research Officer 7 Mr Hardeep Singh, Data Manager 8 Mr Benjamin Hall, Project Officer 9 10
NSW Trauma Innovation Committee 11
Dr Yashvi Wimalasena - Co-chair 12 Mr Dwight Robinson - Co-chair 13 Mr Adam Parker 14 Dr Alan Garner 15 Mr Alex Peters 16 Mr Christopher Ennis 17 Ms Gayle Van Zyl 18 Mr Giles Buchanan 19 Dr Jason Bendall 20 Ms Jessica Keady 21 Ms Julie Friendship 22 Dr Matthew Oliver 23 Dr Negin Sedaghat 24 Mr Nick Cockrell 25 Dr Torgrim (Tom) Soeyland 26 27
Supporting documents 28
Selected Speciality and Statewide Service Plans, NSW Trauma Services Number Six, 2009 29 Critical Care Tertiary Referral Networks & Transfer of Care (Adults) 2017 – PD2017_XXX 30 Critical Care Tertiary Referral Networks (Paediatrics) 2010 – PD2010_030 31 Care Coordination: Planning from Admission to Transfer of Care in NSW Public Hospitals 2011 – 32 PD2011_015 33 Inter-facility Transfer Process for Adults Requiring Specialist Care 2011 – PD2011_031 34 Recognition and Management of Patients who are Clinically Deteriorating 2013 – PD2013_049 35 CEC Patient Safety report – Retrieval and Inter-hospital transfer 2013 36 NSW Ambulance Protocols and Pharmacology 2014 37 38
Trauma Services 39
The development and contents for these guidelines were adapted from NSW, Australian and 40
International Trauma Services transfer guidelines. 41

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines viii
Glossary 1
Aeromedical Control Centre The Aeromedical Control Centre (ACC) coordinates all Medical 2
Retrievals throughout NSW, excluding those in far-west NSW (west 3
of the Darling River) which are managed by the Royal Flying Doctor 4
Service). The ACC is the central control facility of the Aeromedical 5
Services and manages all requests for air rescue, aeromedical 6
transport and adult medical retrieval. 7
Conference call “One phone call” referral where possible to connect the referring 8
clinician, medical retrieval consultant and receiving clinician. 9
Critically injured A patient whose injuries or physiologic instability constitutes a 10
significant and imminent threat to their life without appropriate 11
resuscitation and support. Patients may be classified as Time 12
Urgent or Non-Time Urgent 13
Definitive treatment Definitive treatment is defined as the hospital providing the highest 14
level of care to meet all the clinical needs of the patient. Many 15
patients receive definitive care at Regional Trauma Services, but a 16
small number of patients are transferred to a Major Trauma Service 17
(higher level) for specialised care. 18
Designated Trauma Service A facility that has been designated as a trauma service by NSW 19
Health. A designated trauma service comprises a multidisciplinary 20
structure including staff and resources necessary to ensure the 21
appropriate and efficient provision of trauma care to injured patients. 22
This includes access to relevant sub specialties and coordinated 23
multidisciplinary care. Designated Trauma Services comprise Major 24
Trauma Services, Regional Trauma Services and Paediatric 25
Trauma Services. 26
Inter-hospital retrieval Movement of critically injured and/or unwell patients from one 27
hospital to another hospital by a medical retrieval team. 28
Inter-hospital transfer Movement of patients from one hospital to another requiring access 29
to specialised care. 30
Local Hospital Local hospitals play a part in the trauma system but are not 31
designated trauma services. These may be tertiary hospitals, while 32
others are hospitals serving predominantly local communities in 33
metropolitan or rural areas. As part of the NSW Ambulance Protocol 34
T1, local hospitals will be bypassed for major trauma where possible. 35
Local hospitals will, however, continue to receive minor to moderate 36
trauma cases. 37
Major Trauma A major trauma is defined as any patient who meets the trauma 38
triage tool in the pre hospital setting or any patient who has 39
sustained serious injuries to two or more body regions and/or meets 40
the transfer criteria as outlined in this document. 41
42

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines ix
Major Trauma Service A Major Trauma Service can provide the full spectrum of care for 1
major and moderately injured patients, across the trauma care 2
continuum from initial resuscitation through to rehabilitation and 3
discharge. These hospitals provide a full range of specialist services. 4
This includes Adult Major Trauma Services (MTS) and Paediatric 5
Major Trauma Services (PTS) 6
NETS Newborn and paediatric Emergency Transport Service. A medical 7
retrieval service for babies and children who require intensive care. 8
Non-Time Urgent Patient that is stabilised requiring transfer for a higher level of 9
definitive critical care or clinical specialty, but whose transfer is not 10
time- urgent requiring transfer within 24-72 hoursThis is facilitated 11
by the LHD Patient Flow Unit or Critical Care Advisory Service in 12
consultation with the patient’s clinical management team. 13
Paediatric Trauma Service A Paediatric Trauma Service can provide the full spectrum of care 14
for major and moderately injured paediatric patients, across the 15
trauma care continuum from initial resuscitation through to 16
rehabilitation and discharge. These hospitals provide a full range of 17
specialist paediatric services. 18
Patient Flow Unit Responsible for managing patient flow within a given facility 19
Risk of critical deterioration A patient who has suffered a significant injury or illness who may 20
appear to be stable but whose condition may quickly deteriorate 21
requiring constant monitoring and early transfer for definitive care. 22
Primary cases In the prehospital setting these cases are taken to a designated 23
trauma or specialty services from the scene of injury by road 24
ambulance or medical retrieval team 25
Protocol T1 / T1 Protocol NSW Ambulance Trauma Protocol: Pre-Hospital Management of 26
Major Trauma (commonly referred to as Protocol T1). Protocol T1 27
states any major trauma patient meeting the set criteria for (or 28
potential) major trauma must be transferred from scene to the 29
highest level trauma service with one hour travel time. This ensures 30
that critically injured patients are brought as quickly as possible to 31
the highest level of trauma care for the greatest chance of early 32
survival and recovery. 33
Regional Trauma Service A Regional Trauma Service can provide a high level of care to the 34
injured patient. Definitive trauma care can be provided to a limited 35
number of major trauma patients in collaboration with the major 36
trauma service and can provide all aspects of care to people with 37
moderate and minor trauma. 38
Serious Penetrating Injury Penetrating injury to the head, neck, torso or abdomen involving or 39
likely to involve injury to deep or underlying structures. 40
Specialist Burn Injury Unit Three units in NSW located at Concord Repatriation General 41
Hospital, Royal North Shore Hospital and The Children’s Hospital at 42
Westmead and are part of the Statewide Burn Injury Service (SBIS). 43
Spinal Cord Injury Unit Four units in NSW located at Royal North Shore Hospital, Prince of 44
Wales Hospital, Sydney Children’s Hospital and The Children’s 45

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines x
Hospital at Westmead part of the NSW State Spinal Cord Injury 1
Service (SSCIS). 2
T1 preferred hospital T1 preferred destinations (hospitals) are NSW Ambulance 3
nominated hospitals and whilst these generally have more 4
resources than a local hospital, they are limited in their capacity to 5
manage a major trauma patient. 6
Time Urgent A patient whose injuries requires emergency care at the closest 7
appropriate hospital in the shortest time possible to achieve early 8
intervention and stabilisation and definitive care. This includes 9
physiologic signs or symptoms that constitutes a significant and 10
imminent threat to the patient’s life without appropriate resuscitation 11
and support. 12
Unstable vertebral injury Disruption of two or more columns through fracture, dislocation or 13
ligamentous injuries. 14
15

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines xi
Acronyms 1
AAST American Association for the Surgery of Trauma 2
ACC Aeromedical Control Centre 3
ACI Agency for Clinical Innovation 4
A-WPTAS Abbreviated Westmead post traumatic Amnesia Scale 5
BE Base Excess 6
BP Blood Pressure 7
CEC Clinical Excellence Commission 8
ETA Estimated Time of Arrival 9
GCS Glasgow Coma Scale 10
HR Heart rate 11
ISBAR Identification, Situation, Background, Assessment, Reccomendation 12
ITIM Institute of Trauma and Injury Management 13
LHD Local Health District/s 14
M Months 15
mmHg Millimetre of mercury 16
MTS Major Trauma Service 17
NETS Newborn and Paediatric Emergency Transport Service 18
NSW New South Wales 19
PaCO2 Partial pressure of carbon dioxide 20
PaO2 Partial pressure of oxygen 21
pH Potential of hydrogen 22
PFU Patient Flow Unit 23
PTS Paediatric Trauma Service 24
RR Respiratory Rate 25
RTS Regional Trauma Service 26
SBIS Statewide Burn Injury Service 27
SBIU Specialist Burn Injury Unit 28
SCIU Spinal Cord Injury Unit 29
SpO2 Saturation of Peripheral Oxygen 30
SSCIS State Spinal Cord Injury Service 31
SYS Systolic 32
T1 Trauma protocol 1 33
TBSA Total Body Surface Area 34
< Less than 35
> Greater than 36
% Percentage 37

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines xii
Prelude ......................................................................................................................................... iii 1
Algorithm ...................................................................................................................................... iv 2
Time Urgent Critical trauma consult and/or transfer criteria ..................................................... v 3
Non-Time Urgent critical trauma consult and/or transfer criteria ............................................. vi 4
High-risk mechanism of injury or comorbidities ....................................................................... vi 5
Acknowledgements .................................................................................................................... vii 6
Glossary ..................................................................................................................................... viii 7
Acronyms ..................................................................................................................................... xi 8
Tables ......................................................................................................................................... xiii 9
1. Introduction .......................................................................................................................... 1 10
2. Scope of guidelines ............................................................................................................. 1 11
3. NSW Trauma Services ......................................................................................................... 2 12
4. NSW Trauma Networks ....................................................................................................... 3 13
5. Interstate referral locations ................................................................................................. 4 14
6. Inter-hospital trauma transfer guidelines ........................................................................... 5 15
7. Transfer of a burn injury.................................................................................................... 11 16
8. Transfer of an acute spinal cord injury ............................................................................ 13 17
9. Handover of patient information ....................................................................................... 14 18
10. Preparation for transfer ..................................................................................................... 15 19
11. Inter-hospital transport providers .................................................................................... 15 20
12. Roles and Responsibilities ............................................................................................... 16 21
13. Endorsement ...................................................................................................................... 17 22
14. Appendices ........................................................................................................................ 18 23
24
25
Contents

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines xiii
Tables 1
Table 1: NSW Trauma Services .................................................................................................... 2 2
Table 2: NSW T1 preferred hospitals ........................................................................................... 2 3
Table 3: NSW Trauma networks ................................................................................................... 3 4
Table 4: Interstate trauma referral patterns ................................................................................ 4 5
Table 5: Signs and symptoms of Time Urgent Critical major trauma ....................................... 7 6
Table 6: Time Urgent Critical Injury criteria for inter-hospital trauma transfer ........................ 7 7
Table 7: Non-Time Urgent Critical Injury criteria for inter-hospital trauma transfer ................ 9 8
Table 8: High-risk mechanism of injury and comorbidities factors ........................................ 10 9
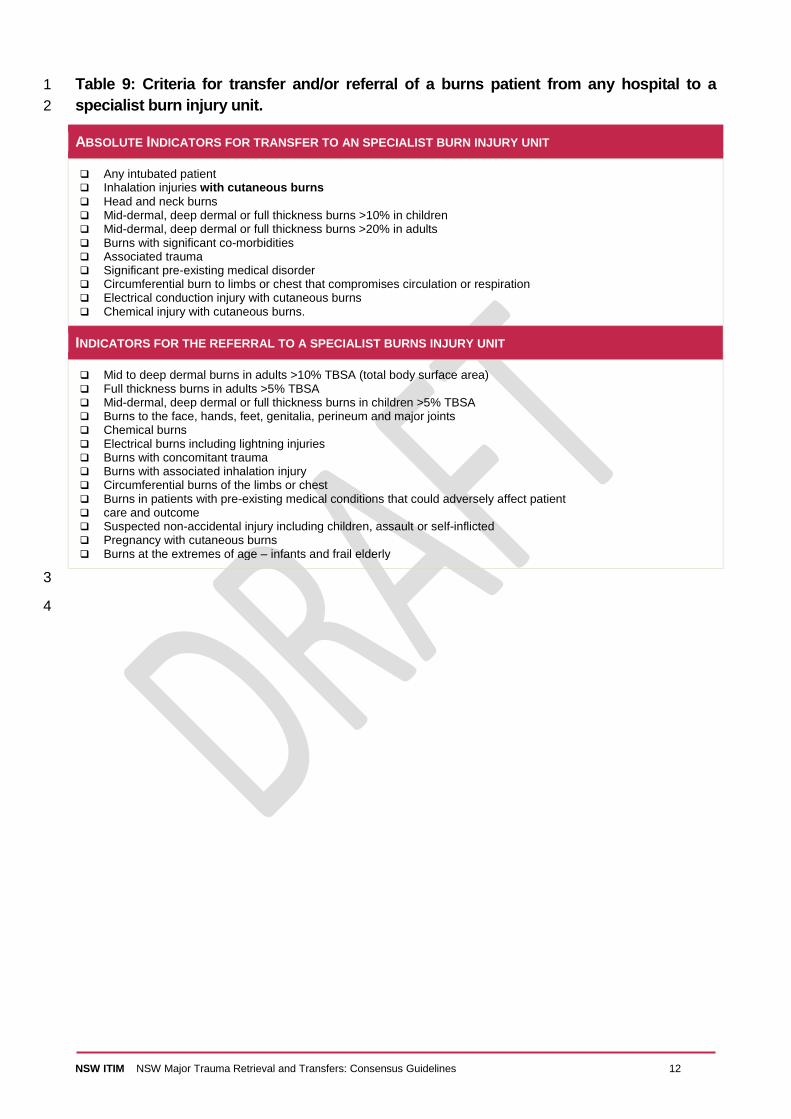
Table 9: Criteria for transfer and/or referral of a burns patient from any hospital to a 10
specialist burn injury unit. .......................................................................................... 12 11
Table 10: Criteria for transfer and/or referral of an acute spinal cord injury patient from any 12
hospital to a State Spinal Cord Injury Unit ................................................................. 13 13
Table 11: ISBAR handover guide ............................................................................................... 14 14
15

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines 1
1. Introduction 1
The NSW trauma system currently operates as a series of networks, mostly driven by local 2
decisions and requirements. Currently, although the NSW Trauma model of care is followed at the 3
highest level, there is high variability with how each network functions. 4
Across NSW Health over 900 major trauma patients require referral and transfer to a designated 5
trauma service each year1. Whilst vital, transfers prolong the time before the definitive care can be 6
provided, such as specialised surgery, interventional radiology or paediatric services. The overall 7
median time to definitive care in NSW in 2015 was 660 minutes1. This median time is considered 8
excessive and is thought to be having a direct impact on patient outcomes. 9
Recently there has been an emerging trend of unwarranted clinical variation in the identification, 10
referral and transfer of major trauma patients. Overall, these variations in referral and transfer of 11
patients were apparent across all Major Trauma Service (MTS), Regional Trauma Service (RTS) 12
and Paediatric Trauma Service (PTS) during the NSW Trauma Patient Outcome Evaluation2 and 13
Clinical Excellence Commission (CEC) Patient Safety Report titled Retrieval and Inter-hospital 14
Transfer Patient Safety Report3. 15
These consensus guidelines aim to provide all hospitals with a standardised set of criteria to 16
support transfer agreements within their networks for the identification and transfer of trauma 17
patients as necessary. This document sets out suggested criteria for early consultation and 18
transfer; however, these may vary with the level of clinical services available at individual hospitals. 19
2. Scope of guidelines 20
The NSW Major Trauma Retrieval and Transfers consensus guidelines have been developed to 21
assist clinicians in providing a more selective, evidence-based approach to the management of 22
major trauma patients. They are not intended to replace senior clinical decision-making. The 23
authors appreciate the heterogeneity of the patient population and their signs and symptoms and 24
the need to often modify management in light of a patient’s co-morbidities. The guidelines rely on 25
individual clinicians to interpret the needs of individual patients. 26
These guidelines are intended for use by staff involved in the care and/or coordination of adult and 27
paediatric major trauma patients requiring inter-hospital retrieval or transfer during the acute phase 28
of trauma management. 29
The information provided is based on the best available information at the time of writing, which is 30
January 2017. These guidelines will, therefore, be updated every 3 years and consider new 31
evidence as it becomes available. 32
33
1 NSW Institute of Trauma and Injury Management. Major Trauma in NSW 2015. Sydney: NSW Agency for Clinical Innovation, 2016.
2 NSW Institute of Trauma and Injury Management. Trauma Patient Outcome Evaluation: Qualitative Report. Sydney: NSW Agency for Clinical Innovation, 2016.
3 Clinical Excellence Commission Patient Safety report – Retrieval and Inter-hospital transfer 2013

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines 2
3. NSW Trauma Services 1
The trauma services of NSW provide expert care for injured patients, coordinating the 2
multidisciplinary teams and advocating for patients, both within the acute and rehabilitative phases. 3
A major trauma service (MTS/PTS) can provide the full spectrum of care for major and moderately 4
injured patients, from initial resuscitation through to rehabilitation and discharge. There are 5
currently seven adult and three paediatric designated MTSs in NSW. 6
A RTS can provide all aspects of care to patients with moderate to minor trauma and definitive 7
care to a limited number of major trauma patients in collaboration with the MTS. A RTS provides 8
initial assessment, stabilisation, definitive care and initiate transfer to an MTS when a patient 9
requires services not available at the RTS. There are currently 10 designated RTSs in NSW. 10
Table 1: NSW Trauma Services 11
Adult Major Trauma
Services
Paediatric Major Trauma
Services Regional Trauma Services
John Hunter Hospital John Hunter Children’s Hospital Coffs Harbour Health Campus
Liverpool Hospital Sydney Children’s Hospital Gosford Base Hospital
Royal North Shore Hospital Children’s Hospital at Westmead Lismore Base Hospital
Royal Prince Alfred Hospital
Nepean Hospital
St George Hospital Orange Health Service
St Vincent's Hospital Port Macquarie Base Hospital
Westmead Hospital Tamworth Rural Referral Hospital
The Tweed Hospital
Wagga Wagga Rural Referral
Hospital
Wollongong Base Hospital
12
T1 preferred hospitals (destinations) are NSW Ambulance nominated hospitals and whilst these 13
generally have more resources than a local hospital, they are limited in their capacity to manage a 14
major trauma patient. 15
Table 2: NSW T1 preferred hospitals 16
NSW T1 PREFERRED HOSPITALS
Armidale Rural Referral Hospital Bathurst Base Hospital South East Regional Hospital (Bega)
Broken Hill Base Hospital Dubbo Base Hospital Griffith Base Hospital
Goulburn Base Hospital Manning Rural Referral Hospital (Taree)
Shoalhaven District Memorial Hospital (Nowra)
17

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines 3
4. NSW Trauma Networks 1
Trauma networks are closely aligned with the NSW Critical Care Tertiary Referral Networks, define 2
the links between Local Health Districts (LHD) and tertiary referral hospitals, and are largely 3
determined by the location of the MTS and the imperative to achieve early clinical intervention for 4
seriously injured patients. The networks take into account established clinical referral relationships 5
which may include referral patterns across LHD boundaries and cross jurisdictional border 6
arrangements. Details of the MTS, PTS, RTS and their networked LHD are outlined in Table 3. 7
Table 3: NSW Trauma networks 8
NSW TRAUMA SERVICE NETWORKS
MTS PTS RTS REFERRING LHD
John Hunter Hospital John Hunter Children’s Hospital
Coffs Harbour Health Service Lismore* Port Macquarie Tamworth Tweed Heads*
Northern NSW*
Mid North Coast Hunter New England
Liverpool Hospital Children’s Hospital at Westmead
N/A South West Sydney
Royal North Shore Hospital Sydney Children’s Hospital Gosford Central Coast Northern Sydney
Royal Prince Alfred Hospital Sydney Children’s Hospital N/A Sydney
St George Hospital Sydney Children’s Hospital Wollongong Wagga Wagga
Illawarra and Shoalhaven
Murrumbidgee*
South East Sydney*
Southern NSW
St Vincent's Hospital Sydney Children’s Hospital N/A N/A
Westmead Hospital Children’s Hospital at Westmead
Nepean Orange
Nepean Blue Mountains
Far West*
Western Sydney Western NSW
9
*Due to proximity the following LHD/ hospitals maintain referral networks to Interstate referral locations 10
11

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines 4
5. Interstate referral locations 1
Owing to proximity, some facilities may refer major trauma patients to an interstate trauma service 2
or specialty service. 3
Table 4: Interstate trauma referral patterns 4
INTERSTATE TRAUMA REFERRAL PATTERNS
MTS PTS REFERRING FACILITIES/LHD
Gold Coast University Hospital Lady Cilento Children’s Hospital Northern NSW
The Canberra Hospital Sydney Children’s Hospital Southern NSW Batlow/Adelong Multi Purpose Service Boroowa Multi Purpose Service Murrumburrah-Harden Hospital Tumut Hospital Young Hospital
The Alfred Hospital Royal Melbourne Hospital
Royal Children’s Hospital Barham Health Service Deniliquin Health Service Finley Hospital Tocumwal Multi Purpose Service Berrigan Health Service Corowa Health Service Holbrook Health Service Culcairn Multi Purpose Service
Royal Adelaide Hospital Women’s and Children’s Hospital Far West
5

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines 5
6. Inter-hospital trauma transfer guidelines 1
GUIDELINES
T1 Preferred or Local Hospital
Where a patient has any of the Time Urgent Critical criteria of potential major trauma, the senior treating
clinician should consult with ACC/NETS as per local procedure in order to arrange a time critical medical
retrieval to the nearest appropriate Trauma Service. This should occur as soon as possible, but no later
than 30 minutes of the patient’s arrival or identification of criteria being met.
Where a patient meets any of the Non-Time Urgent Critical criteria, the senior treating clinician should
consult with their local networked trauma service and/or Patient Flow Units (PFU) as per local procedure in
order to arrange transfer to the nearest appropriate Trauma Service (Regional or Major). This should
occur as soon as possible, but no later than 30 minutes of the patient’s arrival.
Where a patient does not meet any of the inter-hospital trauma consult and or transfer criteria but does meet
any of the High-risk mechanism of injury or comorbidities criteria, a complete trauma assessment and
observation is required due to the high risk of deterioration. If any clinical deterioration is observed, the
senior treating clinician should consult with their networked trauma service and/or Patient Flow Units as per
local procedure in order to arrange potential transfer to the nearest appropriate Trauma Service (Regional
or Major).
Regional Trauma Service
Where a patient is being assessed at a Regional Trauma Service and has injuries meeting Time Urgent
Critical criteria, the senior treating clinician should consult with their networked Major Trauma Service
and/or Patient Flow Units and the ACC/NETS as per local policy in order to arrange a time critical medical
retrieval to the nearest appropriate Major Trauma Service. This should occur as soon as possible, but
no later than 30 minutes of the patient’s arrival or identification of criteria being met.
Where a patient is being assessed at a Regional Trauma Service and does not meet any of time urgent
critical criteria but does meet any of the Non-Time Urgent Critical criteria or High-risk mechanism of
injury or comorbidities criteria, a complete trauma assessment and observation is required due to the high
risk of deterioration. If any clinical deterioration is observed, the senior treating clinician should consult
with their networked trauma service and/or Patient Flow Unit as per local procedure in order to arrange
consultation and potential transfer to the nearest appropriate Major Trauma Service.
Other
Where a direct transfer to a Major Trauma Service is indicated but not achievable, patients should be
transported to the nearest Trauma Service for initial assessment and resuscitation with a view to further
transfer onto a Major Trauma Service as required.
In certain circumstances, trauma patients who do not meet the outlined trauma transfer criteria may still be
transferred to the local networked trauma service to ensure an adequate standard of care, including when
the resources at a metropolitan or rural hospital are overwhelmed.
Where a patient meets specialist burn or spinal cord injury criteria, where clinically indicated, patients may be
transported directly to the networked Specialist Burn Injury Unit (SBIU) or Spinal Cord Injury Unit (SCIU)
after consultation with the service and ACC/NETS.
2
3

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines 6
Inter-hospital Trauma Transfers 1
The aim of the NSW Trauma Plan is to concentrate trauma care in major and regional trauma 2
centres, transporting the right patient to the right hospital as soon as possible. Criteria for inter-3
hospital trauma transfer are reflective of signs and symptoms, specific injury patterns and the 4
resources available at the local hospital. The decision to transfer trauma patients to a higher level 5
of care should be made on clinical grounds by senior clinicians in consultation with networked 6
Trauma Service, PFU or the ACC/NETS. Availability of an intensive care unit (ICU) bed or other 7
resources at the receiving facility is not to delay the acceptance of time critical patients for 8
emergency care. 9
Once the need for transfer has been recognised, arrangements for transfer should be expedited. 10
They should not be delayed for diagnostic procedures that have no impact on resuscitation or the 11
transfer process and do not change the immediate plan of care. Once contacted, the ACC or NETS 12
will coordinate the retrieval of the patient. 13
The destination of the secondary transport cases, which are cases requiring transfer to a higher 14
level trauma service, will be the responsibility of the networked trauma service. These are outlined 15
in: 16
NSW Policy Directive PD20xx_xxx Critical Care Tertiary Referral Networks & Transfer of 17
Care (Adults) 18
NSW Policy Directive PD2010_030 Critical Care Tertiary Referral Networks (Paediatrics) 19
NSW Policy Directive PD2011_031 Inter-facility Transfer Process for Adults Requiring 20
Specialist Care 21
Signs and symptoms of Time Urgent Critical major trauma 22
The first step in identifying patients with potential major trauma is to assess their vital signs and 23
symptoms. If the trauma patient meets any of the criteria in Table 5 below, they may have 24
sustained major trauma. The senior treating clinician should consult as soon as possible with the 25
ACC/NETS as per local procedure. For RTSs this includes consultation with the networked trauma 26
service and/or Patient Flow Unit. 27
28

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines 7
Table 5: Signs and symptoms of Time Urgent Critical major trauma 1
SIGNS AND SYMPTOMS (AFTER INITIAL ASSESSMENT, TREATMENT, CLINICAL DETERIORATION OR SYMPTOMS NOT IMPROVING)
AIRWAY:
Requiring Intubation At risk airway,
hoarseness, stridor
BREATHING:
Respiratory compromise
Hypoxia, cyanosis Pa02 <60mmHg or
PaC02 >60mmHg or pH < 7.2 or BE <-5
CIRCULATION:
Severe haemorrhage Haemodynamic
instability Requiring blood
transfusion for resuscitation
Ongoing significant bleeding
DISABILITY:
Lateralising signs Falling GCS Paralysis/sensory
deficit
AGE TERM – 3M 4 – 12 M 1 – 4 YEARS 5 – 12 YEARS 12+ YEARS ADULT
HR <100 or >180 <100 or >180 <90 or >160 <80 or >140 <60 or >130 <40 or >140
RR >60 >50 >40 >30 >30 <10 or >30
BP SYS <50 <60 <70 <80 <90 <90
SPO2 <90% <90%
GCS <15 <13
PaO2 = partial pressure of oxygen, < = Less than, mmHg = millimeter of mercury, > = greater than, PaCO2 = partial pressure of carbon 2 dioxide, pH = potential of hydrogen, BE = Base Excess, GCS = Glasgow Coma Scale, M = Months, HR = Heart rate, RR = Respiratory 3 Rate, BP = Blood Pressure, SYS = Systolic, SpO2 = Saturation of Peripheral Oxygen, % = Percentage 4
Specific injuries of Time Urgent Critical major trauma 5
The presence of any suspected or actual injuries as outlined in Table 6 indicates they may have 6
sustained major trauma should be transferred to the nearest appropriate Trauma Service. The 7
senior treating clinician should consult as soon as possible with the ACC/NETS as per local 8
procedure. For RTSs this includes consultation with the networked trauma service and/or Patient 9
Flow Unit. 10
Table 6: Time Urgent Critical Injury criteria for inter-hospital trauma transfer 11
INJURIES (SUSPECTED OR ACTUAL)
PENETRATING INJURIES
Serious penetrating injuries to the head or torso
HEAD (REQUIRING URGENT NEUROSURGICAL CONSULTATION)
Penetrating injury / Intracranial Foreign Body / Open Fracture Depressed, complex skull fracture Lateralising signs Traumatic intracranial haemorrhage
NECK / SPINAL CORD / VERTEBRAL COLUMN
Unstable vertebral column injury Spinal cord injury (to spinal cord injury unit as per SSCIS) Peripheral neurological deficit in suspected spinal cord or vertebral column injury Aerodigestive injury (larynx, trachea, oesophagus) Major vascular injury (carotid artery, vertebral artery, internal jugular vein)
CHEST
Any injury involving mediastinum or great vessels Major thoracic cage injury e.g. flail chest Massive haemothorax (>1,000ml)
ABDOMEN / PELVIS
Complex or open pelvic fracture Severe or complex solid organ or hollow viscous injury suspected Haemoperitoneum on FAST Urogenital injury

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines 8
LIMBS / EXTREMITIES
Major limb amputation Major crush injury Fracture/dislocation with neurovascular compromise Penetrating limb injury with neurovascular compromise
BURNS
Severe Burns (refer to State-wide burns transfer guidelines – Section 7)
SECONDARY DETERIORATION
Deteriorating condition requiring prolonged ICU e.g. sepsis with multiple injury Organ failure: single or multiple Major tissue necrosis
1
2

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines 9
Specific injuries of Non-Time Urgent Critical major trauma 1
The presence of any suspected or actual injuries as outlined in Table 7 as moderate or major 2
trauma should be transferred to the nearest appropriate trauma service (Regional or Major). The 3
senior treating clinician should consult as soon as possible with the networked trauma service 4
and/or Patient Flow Unit or ACC/NETS as per local procedure. For RTSs this includes consultation 5
with the networked trauma service and/or Patient Flow Unit if any clinical deterioration or additional 6
time urgent critical criteria is identified. 7
Table 7: Non-Time Urgent Critical Injury criteria for inter-hospital trauma transfer 8
INJURIES (SUSPECTED OR ACTUAL)
PENETRATING INJURIES
Penetrating injuries to the limbs (excluding isolated minor injury to hands or feet)
HEAD (REQUIRING URGENT CT SCAN)
Loss of consciousness or persistent amnesia (failed A-WPTAS# after 4 hours) Signs or suspicion of base of skull fracture or skull fracture
2 or more vomits or a seizure
NECK/SPINE
Stable vertebral injury (single column injury) Swelling, bruising, haematoma, hoarseness or stridor
CHEST
Seatbelt abrasions / contusions Pneumothorax/haemothorax 3 or more rib fractures or flail segment ECG changes
ABDOMEN / PELVIS
Seatbelt abrasions / contusions Severe pain, rigidity, swelling Pelvic fracture Solid organ injury (AAST* Grade I, II or III liver, spleen, pancreas or kidneys)
LIMBS / EXTREMITIES
2 or more proximal long bone fractures Open fracture of long bone
MULTIPLE SYSTEM
Injury to >2 body systems (minor)
OTHER TRAUMA TRANSFER CRITERIA
Head or torso and pelvic injuries without evidence of time critical or complex features (above)
# Abbreviated Westmead Post Traumatic Amnesic Scale 9 * American Association for the Surgery of Trauma 10
11

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines 10
High-risk mechanism of injury and comorbidities 1
The high-risk mechanisms of injury and comorbidity factors listed in Table 7 below should be 2
considered when assessing all trauma patients. Whilst patients meeting these criteria only (no 3
signs and symptoms or injuries requiring inter-hospital trauma consultation or transfer) are not 4
considered as major trauma requiring inter-hospital trauma transfer to a designated trauma service, 5
this cohort of patients are at high risk of deterioration. As such, they should receive a thorough 6
trauma assessment and be observed. 7
If any clinical deterioration is observed, the senior treating clinician should consult with their local 8
networked trauma service and/or Patient Flow Unit as per local procedure in order to arrange 9
potential transfer to the nearest appropriate Trauma Service (Regional or Major). 10
Table 8: High-risk mechanism of injury and comorbidities factors 11
HIGH-RISK MECHANISM OF INJURY
BLUNT TRANSPORT INCIDENT
Death in same vehicle Steering wheel deformity Vehicle vs. pedestrian/cyclist/motor bike Ejection from vehicle Entrapment with compression
BLUNT OTHER INCIDENTS
Focal blunt trauma to head or torso Falls > 3m or paediatrics twice the child’s height High voltage injury Crush injury Drowning
COMORBIDITY FACTORS
Patients <16 years of age Patients >65 years of age Obstetric patients >20 weeks gestation Patients on anticoagulants Immunosuppression Cardio, respiratory or chronic disease Morbid obesity Alcohol or Illicit Drug use
12
13

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines 11
7. Transfer of a burn injury 1
GUIDELINES
Patients meeting the criteria for inter-hospital transfer of burns patients as outlined in Table 8 below must be
referred and/or transferred to a specialist burns injury unit (SBIU) as a trauma burns transfer as per the
SBIS.
In certain circumstances, patients who have suffered a burn injury but do not meet the criteria set out in
Table 8 may also be transferred to the networked SBIU to ensure an adequate standard of care, including
when the resources at a referring hospital are overwhelmed.
Adult cases of severe burn injury without combined trauma may be transported to Concord 2
Repatriation General Hospital or appropriate interstate facility. 3
All adult cases of combined severe trauma and burn injury should be transported to Royal North 4
Shore Hospital or appropriate interstate facility following discussion with their networked trauma 5
service. 6
All paediatric burns patients, including combination paediatric trauma patients, should be 7
transferred to the Children’s Hospital at Westmead or appropriate interstate facility. 8
If the referring practitioner is unsure or seeking advice they should contact the ACC for guidance 9
on best management of the patient. 10
Please refer to the ACI Statewide Burn Injury Service NSW Burn Transfer Guidelines for Criteria 11
for transfer and/or referral of a burns patient from any hospital to a Severe Burn Injury Service and 12
NSW Policy Directive PD20xx_xxx Critical Care Tertiary Referral Networks & Transfer of Care 13
(Adults) and NSW Policy Directive PD2010_030 Critical Care Tertiary Referral Networks 14
(Paediatrics). 15
Statewide specialist severe burn injury services and contact numbers are: 16
Royal North Shore Hospital – 02 9463 2111 17
Concord Repatriation General Hospital – 02 9767 7776 18
Children’s Hospital at Westmead – 02 9845 1114 19
20
NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines 12
Table 9: Criteria for transfer and/or referral of a burns patient from any hospital to a 1
specialist burn injury unit. 2
ABSOLUTE INDICATORS FOR TRANSFER TO AN SPECIALIST BURN INJURY UNIT
Any intubated patient Inhalation injuries with cutaneous burns
Head and neck burns Mid-dermal, deep dermal or full thickness burns >10% in children Mid-dermal, deep dermal or full thickness burns >20% in adults Burns with significant co-morbidities Associated trauma Significant pre-existing medical disorder Circumferential burn to limbs or chest that compromises circulation or respiration Electrical conduction injury with cutaneous burns Chemical injury with cutaneous burns.
INDICATORS FOR THE REFERRAL TO A SPECIALIST BURNS INJURY UNIT
Mid to deep dermal burns in adults >10% TBSA (total body surface area) Full thickness burns in adults >5% TBSA Mid-dermal, deep dermal or full thickness burns in children >5% TBSA Burns to the face, hands, feet, genitalia, perineum and major joints Chemical burns Electrical burns including lightning injuries Burns with concomitant trauma Burns with associated inhalation injury Circumferential burns of the limbs or chest Burns in patients with pre-existing medical conditions that could adversely affect patient care and outcome Suspected non-accidental injury including children, assault or self-inflicted Pregnancy with cutaneous burns Burns at the extremes of age – infants and frail elderly
3
4

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines 13
8. Transfer of an acute spinal cord injury 1
GUIDELINES
Patients meeting the criteria for inter-hospital transfer of spinal cord patients as outlined in Table 9
below must be referred and/or transferred to a spinal cord injury unit (SCIU).
In certain circumstances, patients who have suffered a spinal cord injury but do not meet the
criteria set out in Table 9 may also be transferred to the networked SCIU to ensure an adequate
standard of care, including when the resources at a referring hospital are overwhelmed.
In cases of an isolated acute spinal cord injury, where clinically indicated, patients may be referred 2
and transported directly to the relevant specialist spinal cord injury unit. Spinal cord and spinal 3
column imaging may not be required prior to referral or transfer; advice on this should be sought 4
from the referral SCIU. 5
In cases of combined severe trauma and acute spinal cord injury patients should be transported to 6
Royal North Shore Hospital, the Children’s Hospital at Westmead, the Sydney Children’s Hospital 7
or appropriate interstate facility following discussion with their networked trauma service. 8
If the referring practitioner is unsure or seeking advice they should contact the ACC for guidance 9
on best management of the patient. 10
Please refer to NSW Policy Directive PD20xx_xxx Critical Care Tertiary Referral Networks & 11
Transfer of Care (Adults) and NSW Policy Directive PD2010_030 Critical Care Tertiary Referral 12
Networks (Paediatrics). 13
State Spinal Cord Injury Units and contact numbers are: 14
Royal North Shore Hospital - 02 9926 7111 15
Prince of Wales Hospital - 02 9382 2222 16
Children’s Hospital at Westmead – 02 9845 0000 pg 82399 17
Sydney Children’s Hospital – 02 9382 1000 18
Table 10: Criteria for transfer and/or referral of an acute spinal cord injury patient from 19
any hospital to a State Spinal Cord Injury Unit 20
ABSOLUTE INDICATORS FOR REFERRAL/TRANSFER TO A SPECIALIST ACUTE SPINAL CORD INJURY SERVICE
Sudden onset of neurological deficit affecting spinal segments from C1 to S5 following trauma
Complete or Incomplete spinal cord injury
Cauda equina
Neurogenic shock
21
22

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines 14
9. Handover of patient information 1
GUIDELINE
Referring clinicians are encouraged to provide handover to the receiving clinician for all patients using the
standardised mnemonic ISBAR (Identification, Situation, Background, Assessment, Recommendation) to
improve quality and safety in the transfer of critical information.
The information in Table 10 below will be required by the receiving hospital and the ACC. It is 2
encouraged to have as much information at hand before calling. 3
Table 11: ISBAR handover guide 4
ISBAR INFORMATION
IDENTIFICATION Clinician’s name Clinician’s role/position Clinician’s ward/unit/hospital Identify the patient including name, age, sex and MRN
SITUATION Injuries sustained / Preliminary diagnosis
BACKGROUND Mechanism of injury / Presenting problem Include time of event
ASSESSMENT Signs and Symptoms o Include pre-hospital and current vital signs and trends
Primary Survey assessment o Airway & c-spine (e.g. neck pain) o Breathing & ventilation (e.g. pneumothorax) o Circulation & haemorrhage control (e.g. arterial laceration) o Disability (GCS) (e.g. closed head injury) o Environment (temperature) (e.g. hypothermia)
Treatment given and effect Diagnostic tests and results Other (Secondary survey assessment and interventions if time has permitted)
RECOMMENDATION Care plan Level of specialist care required Level of urgency Confirmation of handover and transfer
5
6
7

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines 15
10. Preparation for transfer 1
GUIDELINES
The patient’s airway, breathing and circulation should be stabilised prior to transfer. All efforts should be
made to control significant haemorrhage prior to transfer. If such control cannot be achieved, advice should
be sought from the senior trauma clinician at the networked MTS or ACC Consultant.
A senior trauma clinician from the networked MTS, ACC Consultant or Retrieval Specialist should advise the
referring hospital regarding patient management and preparation for transfer using the established
processes.
Wherever practicable, all patients identified as requiring inter-hospital trauma transfer should be seen by the
most senior clinician prior to leaving the referring hospital whilst not delaying the transfer process.
Where available, telemedicine should be utilised during this process to connect the patient and clinicians with
the remote specialists and improve accuracy of advice regarding patient management, stabilisation,
treatment, critical decisions
The use of a transfer checklist may assist in streamlining the preparation of the trauma patient for safe
transfer (see Appendix 1).
11. Inter-hospital transport providers 2
NSW Aeromedical Control Centre (ACC) 3
The need for physician-assisted transfer is determined by the ACC in consultation with the 4
receiving facility. Transfer will generally require medically supervised transport which may be via 5
ACC. 6
Cases requiring complex decision making may warrant a teleconference involving the referring 7
(treating) service, ACC and the receiving facility trauma and/or specialty services. 8
For non-time urgent transfers ACC should be contacted on 1800 650 004 by the referring hospital, 9
once the patient has been accepted by the referral trauma service, to facilitate timely medical 10
retrieval. 11
http://www.ambulance.nsw.gov.au/about-us/aeromedical.html 12
Paediatric trauma 13
Children, less than 16 years of age should be transferred to a paediatric MTS. For clinical guidance, 14
transport and patient acceptance at a paediatric MTS please contact NETS retrieval: 1300 36 2500. 15
For further information refer to NSW Policy Directive PD2010_030 Critical Care Tertiary Referral 16
Networks (Paediatrics) and NSW Policy Directive PD2005_157 Emergency Paediatric Referrals – 17
Policy 18
19

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines 16
12. Roles and Responsibilities 1
Referring facility clinicians 2
Referring clinicians are encouraged to: 3
Refer trauma cases to their networked trauma service or ACC/NETS without delay. It is not 4
necessary to have made a diagnosis nor have stabilised the injured patient prior to 5
contacting the referring trauma service. 6
Call the ACC as soon as the treating physician ascertains that the patient has severe 7
trauma related injuries that meet criteria or exceed the local institutional capabilities. This 8
should occur within 30 minutes of arrival or identification of meeting criteria. 9
Seek advice via the ACC if uncertain of the appropriateness of referral or are seeking 10
guidance regarding the medical treatment of the patient. 11
Both referring and receiving clinicians should be encouraged to discuss over telemedicine if 12
the technology is available. 13
Receiving facility clinicians 14
Receiving clinicians are encouraged to: 15
Accept call and handover from referring clinicians. 16
Request details of the Primary Survey to provide appropriate medical advice. 17
Provide advice for management and stabilisation of patient regardless of if accepting the 18
transfer of the patient. 19
Inform referring clinician to contact ACC to arrange transfer. 20
Inform the Emergency Department, Surgeon on call, Bed Manager, ICU (if required) and 21
other specialties of incoming trauma transfer and the patient’s estimated time of arrival 22
(ETA) as required. 23
Where necessary, facilitate direct transfer of the patient to the operating theatre if required 24
(see Trauma ‘Code Crimson’ pathway). 25
Retrieval Services 26
Aeromedical Control Centre (ACC): 27
Upon being contacted by referring hospital ACC will arrange appropriate transportation of 28
the patient/s to the receiving trauma service. 29
Provide advice for interim management or confirmation of management plan via 30
teleconference if required. 31
Newborn and paediatric Emergency Transport Service (NETS): 32
Upon being contacted by either ACC or referring hospital NETS will arrange appropriate 33
transportation of the patient/s to the accepting trauma service. 34
Provide advice for interim management or confirmation of management plan via 35
teleconference if required. 36

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines 17
13. Endorsement 1
These guidelines have been reviewed and endorsed by XXX committee/s and approved by the 2
NSW ITIM Executive Committee. 3
4

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines 18
14. Appendices 1
Appendix 1: ECI Inter-hospital Adult Retrieval Checklist 2
3
4

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines 19
1 2
3

NSW ITIM NSW Major Trauma Retrieval and Transfers: Consensus Guidelines 20
1 2
3

Collaboration. Innovation. Better Healthcare.
1