Embed Size (px)
Citation preview

Vaccine
Research
Center
National Institute of Allergy and Infectious Diseases
National Institutes of Health Department of Health and Human
Services
For more information:
1-866-833-LIFE
vrc.nih.gov
Novel RSV Vaccines Under
Development
Barney S. Graham, M.D., Ph.D.
Achievements and Future Challenges in the
Surveillance of Respiratory Viruses
San Jose, Costa Rica
January 30, 2013

plasma
membrane
150 nm
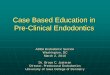
nonstructural
NS1 (139)
NS2 (124)
- inhibit Type I IFN induction - inhibit Type I IFN signaling - activate PI3K and NF-B - inhibit apoptosis
- viral transcription - RNA replication
M2-2 (90)
regulatory
inner envelope face
- assembly M (256) -
nucleocapsid-associated
M2-1 (194) - transcription processivity factor
- RNA-binding
- phosphoprotein
- polymerase
N (391)
P (241)
L (2165)
envelope spikes
G (298) - attachment
- neutralization and protective
antigen
- antibody decoy (secreted G)
- fractalkine mimic
- TLR antagonist
SH (64) - putative viroporin
- inhibits apoptosis
- fusion and entry
- neutralization and protective
antigen
- TLR4 agonist
F (574)
NS2 NS1 M2-1 M2-2
3´
G F SH M N P L
le
6 8 0 2 4 10 15 kb
tr
15,222 nt total
RSV Genome Organization and
Protein Functions
2

Disease Severity is Greatest in
Children <2.5 Months of Age
Boyce TG et al J Pediatr. 2000; 137:865
Other disease (23%)
CHD (5%)
BPD (3%)
Prematurity (12%)
Low-risk (53%)
0
10
20
30
40
50
60
Ja
n
Feb
Ma
r
Ap
r
Ma
y
Ju
n
Ju
l
Au
g
Se
p
Oct
No
v
De
c
Month of Birth
RS
V H
os
pit
ali
zati
on
s
pe
r 1
00
Ch
ild
ren
BPD
CHD
Other disease
<=28 wk
29-<33 wk
33-<36 wk
Low-risk
Biological challenges for vaccination
• Relatively weak induction of cellular responses
• Reduced capacity for somatic mutation of antibody
• Presence of maternal antibody
• Frequent reinfection
• Legacy of vaccine-enhanced disease 3

Biological Factors Associated
with Difficult Vaccine Targets
• Infection is not easily controlled by natural immunity – High frequency of severe disease (filoviruses)
– Persistent infection (HSV, HIV, HCV)
– Reinfection is common (RSV, HIV)
• Alteration or evasion of host immune response – Interference with innate and adaptive immunity
– Integration, sequestration, and immune sanctuaries
• Significant genetic variation or multiple serotypes
• Site of initial infection is major target organ for disease
• Animal models do no recapitulate pathogenesis of human disease
• Critical role for T cell-mediated immunity (HIV, HCV)
• Delay between infection and induction of cellular immunity (HCV)
Graham & Walker in The Immune Response to Infection, 2011 4

Biological Factors Associated
with Difficult Vaccine Targets
• Infection is not easily controlled by natural immunity – High frequency of severe disease (filoviruses)
– Persistent infection (HSV, HIV, HCV)
– Reinfection is common (RSV, HIV)
• Alteration or evasion of host immune response – Interference with innate and adaptive immunity
– Integration, sequestration, and immune sanctuaries
• Significant genetic variation or multiple serotypes
• Site of initial infection is major target organ for disease
• Animal models do no recapitulate pathogenesis of human disease
• Critical role for T cell-mediated immunity (HIV, HCV)
• Delay between infection and induction of cellular immunity (HCV)
5 Graham & Walker in The Immune Response to Infection, 2011

Factors that Diminish Incentives for
Industrial Vaccine Development
• Concern about safety
– RSV
• Concern about achieving efficacy – HIV, RSV
• Sporadic or biodefense threats without a dependable
commercial market – Ebola/Marburg
– New emerging viral diseases
Graham et al. Clinical Pharmacology and Therapeutics 2009 6

Factors that Diminish Incentives for
Industrial Vaccine Development
• Concern about safety
– RSV
• Concern about achieving efficacy – HIV, RSV
• Sporadic or biodefense threats without a dependable
commercial market – Ebola/Marburg
– New emerging viral diseases
7 Graham et al. Clinical Pharmacology and Therapeutics 2009

No Efficacy –
Serious Adverse
Effects
Low/No Efficacy –
No Immediate
Safety Concerns
No Efficacy –
Inappropriate
Immune Response
Efficacy unknown –
Currently in
Clinical Testing
Efficacious
Formalin-inactivated
alum-precipitated
whole virus
Subunit vaccine
G protein –
streptococcal
conjugate
Subunit vaccine
F glycoprotein in
alum in adults
Various live
attenuated RSV
nasally in children
Live virus vaccine
delivered IM in
children
BPIV-RSV live
chimeric virus nasally
None
Overview of RSV
Vaccine Clinical Development
8
Live attenuated RSV
nasally in children
rA2cp248/404/1030/ΔSH
ΔM2-2
Post-fusion F Rosettes

FI-RSV Vaccine-Enhanced Disease
Vaccine n Infected (%) Hospitalized (%) Deaths
FI- RSV 31 20 (65) 16 (80) 2
FI-PIV-1 40 21 (53) 1 (5) 0
Kim et al. Am J Epidemiol 1969;89:422 9

Correlates of FI-RSV
Vaccine-Enhanced Illness
Johnson et al. J Virol 2004; 78:6024
% E
os
ino
ph
ils
in
BA
L
0
5
10
15
20
25
30
35
40
45
FI-Vero FI-rRSV wt
FI-rRSV
DG
FI-rRSV Gep-
FI-r RSV
DSH Graham et al. JI 1993;151:2032
Tang et al. Vaccine 1997;15:597
Properties to Avoid
• Antibodies with poor NT activity → Immune complex deposition
• CD4+ Th2-biased response → Allergic inflammation
Polack et al. J Exp Med 2002; 196:859
10

Options for Vaccine Evaluation
F
G
SH
Internal
Multiple
Neonate (<2 mo) Infants and children (>6 mo) • Sero-negative • Sero-positive
Siblings and parents of neonates Young adult women • Pregnant women • Women of child-bearing age
Elderly (>65 yr)
Live-attenuated • RSV • chimeric paramyxovirus vectors
Gene-based vectors • Nucleic acid – DNA or RNA • Replication defective • Replication competent
Subunit or particle-based • Purified protein • Virus-like particle • Virosome • Nanoparticle • Peptides
Whole-inactivated RSV
Platforms Antigens Delivery Target Populations
11
Respiratory tract Parenteral Other mucosal site
11

Considerations for Immunizing
RSV-Naïve Infants
• Opportunity to prevent or delay first RSV infection – Reduced primary morbidity
– Reduced childhood wheezing
• Opportunity to establish future immune response patterns (antibody specificity and T cell phenotype) – Improved immunity against reinfection
• Target age is critical – Peak age of hospitalization ~2.5 mo
– ~50% of hospitalization occur >6 mo
– If incidence is ~60% in first year, ~70% are RSV-naïve at 6 mo
12 12

Selecting Target Age for
Initiating Vaccination
<4 mo >6 mo
Efficacy
Somatic mutation - ++
Dendritic cell and APC maturation - ++
Clearance of maternally-derived antibody - ++
No longer breast-feeding - +
Safety
Idiosyncratic apnea and other rare adverse events + -
Small airway size ++ -
Relative Th2 bias ++ -
13 13

RSV Vaccine Pipeline
Product Sponsor Type of Vaccine Target Antigen Target population Phase
Sanofi RSV vaccine Sanofi Subunit F, G, M protein Elderly patients Phase II
BBG2na Queen’s Univ Belfast Subunit G n/a Phase II
MEDI-559 MedImmune Live-attenuated Whole virus Infants and children Phase I-IIa
MEDI-534 MedImmune Live chimeric F Protein Infants Phase I-IIa
MEDI ΔM2-2 & others NIAID +/- MedImmune Live-attenuated Whole virus Adults, infants and children Phase I
Novavax RSV Novavax Nanoparticle F Protein n/a Phase I
Sendai-RSV chimera St. Jude’s Live chimeric F n/a Pre-clinical
RSV vaccine Merck/Nobilon Single-cycle Whole virus n/a Pre-clinical
NanoBio RSV Nanobio/Merck Inactivated Whole virus n/a Pre-clinical
MVA-BN RSV Bavarian Nordic Vector Subunit Adult high risk patients Pre-clinical
GenVec RSV GenVec Vector F Children and infants Pre-clinical
Universal RSV Crucell/J&J Vector Subunit Infants and elderly Pre-clinical
RSV vac_Oka Okairos Vector F-N-M2-1 n/a Pre-clinical
VEE-F Alphavax Vector F n/a Pre-clinical
RNA replicon Novartis Vector-RNA F n/a Pre-clinical
Mymetics RSV Mymetics VLP-Virosome Multiple Elderly patients Pre-clinical
TechnoVax Technovax VLP Multiple n/a Pre-clinical
SynGem Mucosis VLP-lactococcus F n/a Pre-clinical
RSV VLP Vac LigoCyte VLP F n/a Pre-clinical
F protein Novartis Subunit F n/a Pre-clinical
RSV vaccine GSK Subunit F Pediatric Pre-clinical
AMV601 / RespiVac AmVac Subunit n/a Pre-clinical
PEV4 Pevion Subunit F n/a Pre-clinical
Epitope-scaffold U. Wash/ TSRI) Epitope-scaffold F epitope Pediatric and at-risk adults Pre-clinical
SHe Ghent/Immunovaccine Subunit SH n/a Pre-clinical
T4-214 TI Pharma n/a Pre-clinical
TWi RSV vaccine TWi Biotech n/a Pre-clinical
Sources: Company Website, Fierce Vaccines, RSV 2012 Symposium, Clinicaltrials.gov
14

Whole-inactivated virus
WT or attenuated virus
Naked
DNA or RNA
Vectors
VLPs or
virosomes
Comparing Product Concepts Based on
Immunological Concepts
15
Native F or G
MHC pathway
CD8 T cell induction
IL-4 Delivery
route Replication competence
- II - ++ IM -
++/- II - +/- IM -
++ II +/- I +/- -/+ IM -
++ I & II ++ - IM or nasal - or +
++ I & II + - IM -
++ I & II + - nasal +
++ I & II + - nasal or IM +
Recombinant,
or chimeric
viruses
Protein subunits

Passive Prophylaxis with Synagis
•Humanized mouse monoclonal antibody
•Monthly injections reduce hospitalizations by 50%
•Licensed for select high-risk infants
•Demonstrates neutralizing antibodies against the F glycoprotein are protective
Shane Storey, Nat Rev Drug Discovery (2010) 9, 15-16 16

Vaccine Antigen Selection:
Rationale for Choosing F
Reasons for choosing F:
• Target of Synagis
• Higher sequence conservation than G
• Unlike G, F is absolutely required for virus entry
Prefusion
Receptor
Delivery of nucleocapsid and genome
Postfusion
Prehairpin
Target cell cytoplasm
17

*
* HR2 TM FP HR1
Organization of RSV F Glycoprotein
• Type I integral membrane protein essential for RSV entry and cell-to-cell fusion
• Primary target for neutralizing antibody.
• pH-independent class I viral fusion protein
• Multiple furin cleavage sites
• Two heptad repeat regions that form an anti-parallel six-helix bundle in post-fusion state.
• F1 has a cysteine-rich domain. C-linked palmitylation
Disulfide bond
Cysteine
Infection inhibiting peptide
Unique to RSV
Heptad repeat
Transmembrane domain
*
Known or potential furin cleavage site
Signal peptide
F1 F2
69 212 313 322 333 343 358 367 382 393 416 422 439 550 1 574 37 21
70 116 126 500 27
Fusion peptide
N-linked glycosylation
Neutralizing antibody epitope
18

New Technologies Have Made an RSV
Vaccine Possible
Discovery of immunity Molecular
biology
10
12
14
16
0
2
4
6
8
1800 1820 1840 1860 1880 1900 2020 2040 1920 1940 1960 1980 2000 2060
Animal Models
B & T cell biology
Delivery devices
Genomics
Glycobiology
Informatics
Manufacturing
Nanobiology
Proteomics
Structural Biology
Vector biology
2080
Potential areas for new
technical advances
HPV
Rotavirus
Varicella
Japanese
encephalitis
Hepatitis A
Hepatitis B
Rubella
Mumps
Adenovirus
Measles
Poliovirus
Influenza
Yellow fever
Rabies
Smallpox
Major Conceptual and Technological Advances Viral Vaccines
Cell culture
19
RSV ?

Summary
• There is a robust pipeline of candidate RSV vaccines and antigen design is being facilitated by atomic structure
• We need RSV-devoted NGO involvement for advocacy, advancing candidates, and coordination of public-private partnerships
• Developing clinical trial infrastructure through North-South partnerships would facilitate clinical development
• The regulatory process will be facilitated if we avoid generic terms for new vaccine platforms and describe them by immunological and biophysical properties
• For RSV-naïve infants it may be best to achieve licensure first in children >6 mo of age
– Expand safety database
– Perform studies to evaluate herd (neonatal) immunity
– Develop mathematical transmission models to refine timing and schedule for vaccination
– Consider passive-active approaches
20

Viral Pathogenesis Laboratory
21
Sung-Han Kim, Syed Moin, Barney Graham, Kaitlyn Morabito, Azad Kumar, Kevin Graepel, Kayvon
Modjarrad, Man Chen, Tracy Ruckwardt, Allison Malloy, Jason McLellan, Jie Liu, Erez Bar-Haim

Questions
22