Embed Size (px)
Citation preview

NUCLEAR CARDIOLOGY (V DILSIZIAN, SECTION EDITOR)
Novel Molecular Angiotensin Converting Enzymeand Angiotensin Receptor Imaging Techniques
Jamshid Shirani & Vasken Dilsizian
# Springer Science+Business Media New York 2014
Abstract Angiotensin II (AII), an octapeptide member of therenin-angiotensin system (RAS), is formed by the enzymeangiotensin converting enzyme (ACE) and exerts adversecellular effects through an interaction with its type 1 receptor(AT1R). Both ACE inhibitors and angiotensin receptorblockers (ARB) mitigate the vasoconstrictive, proliferative,proinflammatory, proapoptotic, and profibrotic effects of AIIand are widely used as effective anti-remodeling agents inclinical practice. Prediction of individual response to theseagents, however, remains problematic and is influenced bymany factors including race, gender, and genotype. In addi-tion, systemic and tissue RAS activity do not correlate closely.This report summarizes the results of on-going attempts tononinvasively determine tissue ACE activity and AT1R ex-pression using novel nuclear tracers. It is hoped that theavailability of such imaging techniques improve treatment ofheart failure through more selective pharmacologic interven-tion and better dose titration of available drugs.
Keywords Molecular imaging . Cardiovascular imaging .
Angiotensin II .Angiotensinconvertingenzyme .Angiotensinreceptors . Left ventricular remodeling . Left ventricularsystolic dysfunction . Congestive heart failure . Angiotensinconvertingenzymeinhibitors .Angiotensin receptorblockers .
Imaging
AbbreviationsACE Angiotensin Converting EnzymeAII Angiotensin IIARB Angiotensin Receptor Blocker(s)AT1R Angiotensin II Type-1 ReceptorCHF Congestive Heart FailureCT Computerized TomographyLV Left Ventricle (Ventricular)PET Positron Emission TomographyRAS Renin-Angiotensin SystemSPECT Single Photon Emission Computed Tomography
Introduction
Activation of the systemic and particularly of the tissue com-ponents of the renin-angiotensin system (RAS) is a majorcontributor to the pathogenesis and progression of left ven-tricular (LV) remodeling and congestive heart failure (CHF)[1••, 2••]. Much of the adverse influence of RAS on LVremodeling is mediated through the interaction of the primaryeffector molecule of RAS, angiotensin II (AII), with its type-1receptor (AT1R) at the cellular level [1••, 2••]. Pharmacologicinterventions that reduce the production of AII (angiotensin-converting-enzyme [ACE] inhibitors) or inhibit its interactionwith AT1R (angiotensin receptor blockers [ARB]) have beenshown to ameliorate LV remodeling and improve outcome ofpatients with LV systolic dysfunction in randomized clinicaltrials [3••]. However, individual responses to these medica-tions have varied widely and have been influenced by manyfactors including race [4], gender [5•], and genotype [6]. Inaddition, the presence of a complex array of receptors,byproducts of AII metabolism, and alternative pathways ofAII production makes prediction of the AII activity in indi-vidual patient difficult. Inadequate RAS suppression is
This article is part of the Topical Collection on Nuclear Cardiology
J. Shirani (*)Department of Cardiology, St. Luke’s University Health Network,801 Ostrum Street, Bethlehem, PA 18015, USAe-mail: [email protected]
V. DilsizianDepartment of Diagnostic Radiology and Nuclear Medicine,University of Maryland School of Medicine, Baltimore, MD, USA
Curr Cardiol Rep (2014) 16:466DOI 10.1007/s11886-014-0466-7

associated with adverse outcomes [7•] and while some pa-tients may benefit from combined ACE inhibitor and ARBtherapy such a regimen is associated with higher risk of sideeffects [8]. For all these reasons, accurate assessment of tissueACE activity and AT1R expression is of utmost clinical inter-est and has stimulated a concerted effort for developing non-invasive imaging techniques that target these clinically rele-vant components of RAS (Fig. 1). This historical perspectivereviews the milestones in development of novel ACE andAT1R imaging techniques.
Imaging ACE
Molecular Structure and Function of ACE
ACE (kininase II) is a zinc-dependent (2 zinc atoms permolecule) polypeptide dicarboxypeptidase that produces AIIby cleaving the carbonyl-terminal histidyl-leucine of its pre-cursor angiotensin I [9•]. AII is the primary effector peptide ofRAAS that is responsible for the vasoconstrictive, profibrotic,proinflammatory, proapoptotic, and proliferative actions ofRAS. ACE is highly expressed on vascular endothelium andis locally produced in many organs including the heart. Al-though alternative pathways (such as chymase) to AII produc-tion exist, ACE is responsible for more than 90 % of AIIproduced locally in the heart in the absence of ACE inhibitors.The enzyme contains 2 homologous extracellular catalytic
domains with different biologic functions. Binding of ACEto vascular endothelium is through its C terminal hydrophobictransmembrane region while ACE inhibitors bind to the ex-tracellular binding sites of the enzyme. Serum ACE activity isin general measured by tripeptide substrates, most commonlythe hippuryl-his-leu; however, nearly 90 % of ACE activityoccurs within the tissue component that is not accessible tosuch assays. The study of the distribution and magnitude ofACE expression in various organs has been greatly facilitatedby the development of radiolabeled ACE inhibitors (Table 1).
Radiolabeled Captopril
The first attempts at radiolabeling angiotensin-converting en-zyme (ACE) inhibitors were made to study selective in vitrobinding to membrane-bound ACE using liquid scintillationchromatography. Early studies using [3H]-captopril demon-strated that regional distribution of the radiotracer paralleledclosely those of the ACE enzymatic activity in various tissuesincluding the heart [10]. Further in vitro studies demonstratedthat the high affinity ligand binding occurred atone [3H]-captopril site per ACE molecule [11]. The radiotracer wasthen used to study the distribution and activity of vascularendothelial (pulmonary and mesenteric) and tissue ACE invarious models of systemic hypertension in rats [12]. Impor-tantly, it was shown that vascular and tissue enzyme activitydid not always parallel each other [12]. The tracer was even-tually abandoned because it was unstable and was found to
Fig. 1 Diagrammaticrepresentation of myocardial celland potential targets of radiotracerimaging and mapping of thesurface renin-angiotensin system.ACE angiotensin-convertingenzyme, AGT angiotensinogen,Ang II angiotensin II, AT1Rangiotensin II type 1 receptor,AT2R angiotensin II type 2receptor, mRNA messenger RNA.Reproduced with permission from:Schindler TH, Dilsizian V. Cardiacpositron emission tomography/computed tomography imaging ofthe renin-angiotensin system inhumans holds promise for image-guided approach to heart failuretherapy. J Am Coll Cardiol.2012;5:1269–84 [48]
466, Page 2 of 8 Curr Cardiol Rep (2014) 16:466

attach substantially to sites other than ACE. The first positron-labelled ACE-inhibitor that was tested in vitro was thefluorine-18-fluorocaptopril (18FCAP) [13]. In vivo bio-distribution was first assessed in rats and showed high uptakesin organs known to have high ACE activity such as lungs,kidneys, and the aorta [13]. It was also noted that the clearanceof the radiotracer was faster for lungs and kidneys, comparedwith the aorta. Competitive inhibition of ACE by co-injectingunlabeled 4-cis-fluorocaptopril (SQ 25750) resulted inmarked decrease in 18FCAP uptake in the lungs and thekidneys [13].18FCAP was also administered to a healthyhuman volunteer, and displaceable uptake was observed inthe lungs and the kidneys. The results demonstrated thefeasibility of probing ACE in vivo using PET. In anotherhuman study of healthy volunteers and 5 patients withpulmonary hypertension,18FCAP PET was able to safelyand reproducibly measure total mass of pulmonary ACEand determine the efficacy of treatment with the ACEinhibitor enalapril [14]. These landmark proof-of-conceptobservations demonstrated that radiolabeled ACE inhibitorscould be used in vivo (in rats and humans) to monitorACE. However, 18FCAP had several shortcomings. Capto-pril contained a sulfhydryl group that tended to formcaptopril disulfide dimers or mixed dimers of captopril andendogenous sulfhydryl compounds (such as L-cysteine, glu-tathione, and methionine) producing high nonspecific binding[15]. Also, in vivo conformational changes resulted in cis andtrans isomers of 18FCAP with potentially different kinetic rateconstants [16]. Finally, captopril was shown to have a higheraffinity for vascular compared with tissue ACE and thus, wasthought to be less suited for examination of tissue ACEactivity [17] compared with more tissue specific ACE inhib-itors such as lisinopril.
Radiolabeled Zofenoprilat
Zofenopril is another sulfhydryl containing ACE inhibitorpro-drug that requires systemic conversion to its active me-tabolite, zofenoprilat. The drug is much more potent thancaptopril as an ACE inhibitor. A radioligand of zofenoprilat
was synthesized after labeling with 11C [18]. The positronemission tomographic tracer, [11C]-zofenoprilat was then test-ed in human volunteers and was shown to accumulate inorgans known to have high ACE levels such as lungs andkidneys [18]. Activity was also noted in the heart.
Radiolabeled MK351A
The next group of radiolabeled ACE inhibitors belonged tothe decarboxylase group (including lisinopril) that had nosulfhydryl moiety and had more affinity for tissue ACE. Atyrosyl derivative of enalaprilic acid, MK351A, was labeledwith 125I and was used to measure serum ACE activity inpatients with sarcoidosis with reliable and reproducible resultscompared with standard enzyme kinetic assay [19]. The tech-nique was then used as a binding assay to measure ACEactivity in tissue preparations from rats [20]. This was advan-tageous over the available enzyme kinetic assays that failed toassess tissue ACE activity and could allow establishing phar-macokinetic and pharmacodynamics profiles of ACE inhibi-tors [21]. Using quantitative in vitro autoradiography, detaileddistribution of myocardial ACEwas demonstrated [22] and anincreased expression of myocardial ACE following acutemyocardial infarction was shown in rats [23]. Also, the effectsof vasopeptidase inhibitor omapatrilat on tissue ACE andneutral endopeptidase activity could be evaluated in rats using[125I]-MK351A and [125I]-RB104, a neutral endopeptidaseinhibitor ligand [24, 25]. Vasopeptidase inhibitors simulta-neously inhibit ACE and neutral endopeptidase, the majorenzyme that degrades natriuretic peptides. Although [125I]-MK351A was not used in any human study, it did establishitself as the standard radioligand for ACE affinity assays.
Radiolabeled Lisinopril
The next dicarboxylate ACE inhibitor used as a radioligandwas radiolabeled lisinopril. It had several important advan-tages over 18FCAP, [11C]-zofenoprilat and [125I]-MK351A:(1) it was an ACE inhibitor in wide clinical use and with anestablished safety record for human use; (2) although a lysineanalog of enalapril, unlike the parent drug did not requiresystemic conversion to an active metabolite for its pharmaco-logic effect; (3) exhibited relatively high affinity for tissueACE with more predictable dissociation compared with lipo-philic avid ligands such as quinapril and ramipril; and that the(4) binding of lisinopril to the active site of ACE was wellcharacterized [26]. The higher affinity of lisinopril for tissueACEwas also felt to improve image resolution compared withcaptopril. Finally, a unique feature of lisinopril was that themolecule could be modified substantially during the labelingprocess without compromising its pharmacologic properties[27]. Thus, [18F]fluorobenzoyl-lisinopril (18FBL) was devel-oped by investigators at the National Institutes of Health by
Table 1 Molecular radiotracers that target the renin-angiotensin system
Angiotensin converting enzyme Angiotensin II type 1 receptor
18F-fluorocaptopril 125I-[Sar1, Ile8]AII11C-zofenoprilat 11C-MK-996125I-MK351A 11C-L-159884125I-iodotyrosyl-lisinopril 11C-KR3117318F-fluorobenzoyl-lisinopril 99mTc-losartan-Leu-Diglycoloyl-
PEG(4)-Tetraamine99mTc-(CO)3D(C8)-lisinopril
11C-losartan11C-methyl-candesartan
Curr Cardiol Rep (2014) 16:466 Page 3 of 8, 466

radiolabeling benzoic acid active ester with 18F and reactingthat with the epsilon-amino group of lisinopril for positronemission tomography [28]. The radioligand was then testedfor determining the magnitude and distribution of tissue ACEin myocardial sections of explanted human hearts of patientswith ischemic cardiomyopathy [29••]. In vitro autoradiogra-phy demonstrated excellent concordance between 18FBL up-take and immunohistochemical evidence of ACE distributionwith the highest uptake in the periphery of the infarctedmyocardial segments [29••]. The study provided direct evi-dence for specific binding of the radioligand to myocardialACE. It was felt that high resolution and the highly specificbinding of the radioligand to myocardial ACE could poten-tially be used to assess enzyme activity in vivo with thepotential to improve risk to benefit ratio of RAS modulation,monitor drug efficacy, and titrate dosage in heart failure.
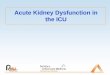
One of the major potential limitations of 18FBL for use inhuman is the lack of wide spread availability of PET. Otherimaging techniques, such as single-positron emission comput-ed tomography (SPECT) or SPECT-computed tomography(CT) [SPECT-CT] may be more readily available and, thus,parallel efforts were made to also develop technetium (Tc)-based radiotracers for use in conjunction with SPECT imaging[30]. One such tracer, 99mTc-Lisinopril, was studied forin vivo imaging of myocardial ACE activity in transgenic ratmodel [31••].Micro SPECT-CT imaging was performed at 10,30, 60, and 120minutes after radiotracer injection. In vivo andex-vivo specific binding of 99mTc-Lisinopril to myocardialACE was verified with pre-treatment with unlabeledlisinopril, enzyme-linked immunosorbent assay for ACE ac-tivity and with ACE messenger ribonucleic acid expression(Fig. 2). Overall, at 120 minutes, 99mTc-Lisinopril myocardialuptake was 5-fold higher in transgenic rats compared withcontrol animals. This study provided a new evidence for thepotential role of imaging in studying pharmacokinetics andpharmacodynamics of ACE inhibition in the intact animalwith a potential for human application [32].
Imaging the AT1R
Molecular Structure and Function of AT1R
AT1R is a 359 amino acid G protein-coupled receptor that isthe principal mediator of the adverse cellular effects of AII[33]. The receptor is activated in the presence of AII bytransmembrane displacement that allows binding of AII tospecific extracellular binding sites. Receptor activation thenleads to a cascade of intracellular events that culminates inproduction of growth factors and proinflammatory cytokines.AT1R has, thus, been the target of research that has led to thedevelopment of a highly effective class of anti-remodelingagents, the angiotensin-receptor blockers (ARB). Similar to
ACE, characterization of the structure and function of AT1Rhas been highly facilitated by the development of selectiveradiolabeled ligands (Table 1).
Radiolabeled AII
The initial effort characterize AII binding sites includedin vitro receptor binding assays using [125I]-AII [34]. Theearly studies demonstrated that AII had 2 distinct receptors(initially designated as A and B) that could be identified bycompetitive displacement of the radioligand by specificnonlabeled antagonists [35]. Both [3H]-AII and [125I]-AIIhave been used to study AII-AT1R interaction in vitro [36]and for identification of new potent antagonists of AT1R [37].
Radiolabeled ARB
The discovery and synthesis of selective ARB and their per-ceived significance in treatment of systemic hypertensionheightened the interest in the study of AT1R receptor. Thesignificance of in vivo imaging of these receptors was recog-nized early and lead to the application of [Sar1, Ile8]AII, apeptide antagonist of AT1R, as a radiotracer for in vivo imag-ing of rat and Rhesus monkeys [38]. Although the experimentwas successful in demonstrating high uptake of the radiotracerin the liver and the kidney, image resolution was poor, and thehigh uptake by the liver and subsequent biliary excretionobscured imaging of the kidneys [38]. In general, the shortduration of action and the partial agonist properties of peptideantagonists were thought to be limiting to their use as effectiveradioligands. The introduction of the nonpeptide ARB pre-sented an opportunity for development of new tracers forselective AT1R imaging. The first such radiotracer was the[11C]-MK-996 for PET imaging [39]. The radiotracer waseffectively used in dogs but was abandoned in favor of itsmethoxy analog, L-159884, due to difficulties in synthesis ofthe former [40]. In vivo imaging demonstrated binding of the[11C]-L-159884 to AT1R in mouse kidneys, lungs, and theheart [41] as well as the renal cortex in a canine model [42].Concerns, however, existed regarding the usefulness of [11C]-L-159884 as a clinical imaging tool due to its rapid metabolismand potential for nonspecific binding. The search for optimalcandidates for human studies led to the development ofradiolabeled 2-Butyl-5-methoxymethyl-6-(1-oxopyridin-2-yl)-3-[[2’-(1H-tetrazol-5-yl)biphenyl-4-yl]methyl]-3H-imidazo[4,5-b]pyridine {[11C] KR31173}from the potent AT1Rantagonist SK-1080 [43]. The radiotracer was produced bycoupling a tetrazole-protected hydroxyl precursor with [11C]-methyl iodide and subsequently removing the protecting groupby acid hydrolysis [43]. The presence and time course ofregional myocardial upregulation of AT1R was then studiedusing in vivo micro-PET [11C]-KR31173 imaging in a ratmodel of myocardial ischemia-reperfusion [44]. Injection of
466, Page 4 of 8 Curr Cardiol Rep (2014) 16:466

the radioligand following 20–25 minutes of coronary ligationresulted in detectable increase in uptake of the tracer in theinfarct area. The specific binding of the tracer to AT1R wasvalidated with ex vivo autoradiography and with immunohis-tochemical staining [44]. Comprehensive evaluation of thisradiotracer has also shown the feasibility and suitability of thisagent for in vivo imaging using PET and PET-CT in largeranimals [45, 46]. It was shown that the uptake and retention ofthe radioligand correlated with the AT1R distribution (high inthe adrenal gland, kidney, lung, and heart) with a high organ to
blood ratio [45]. Importantly, the myocardium was shown todemonstrate high specific binding (96 %), which appearedpromising for the future application of this tracer in cardiacimaging [46]. The quality of PET images was also found to beexcellent in the studied dogs [45] and pigs [46] with clearvisualization of various organs including kidneys and the heart.
In 2012, Fukushima et al presented the first-in-man appli-cation of receptor ligand [11C]-KR31173 combined with PET/CT that confirmed the presence of local tissue RAS in humanhearts, proved to be safe, and that the signal was high enough
Fig. 2 Noninvasivemicro-SPECT/micro-CT Imaging of ACE-1 activity.Micro SPECT-CT imaging provides simultaneous scintigraphic andmorphologic localization of Tc-Lis uptake, 60 minutes after traceradministration, in a control animal (left), ACE-1 overexpressingtransgenic animal (middle) and a transgenic animal after cold-lisinopril administration (right). White arrowhead demonstrates intenselung uptake and yellow arrows point to myocardial ACE-1 activity.White arrows suggest a substantial reduction in tracer uptake after
pretreatment with nonradiolabeled lisinopril administration. Despitethe several-fold lower lung-to-heart ratio in the transgenic animalswhen compared with the control animals, the lung uptake may stillbe visualized, and more importantly may contribute spill over countsto the myocardium, which can be corrected for. Reproduced withpermission from: Dilsizian V, et al. Molecular imaging of humanACE-1 expression in transgenic rats. J Am Coll Cardiol Img.2012;5:409–418 [31••]
Fig. 3 PET/CT of Myocardial AT1R in a Healthy human patient.Transaxial fusion images through the mid-cardiac region are shown.Baseline images show regionally homogeneous uptake of the angiotensinII type 1 receptor (AT1R) ligand [11C]-KR31173 in left ventricularmyocardium (left). Repeat imaging 3 hours after an oral (p.o.) dose of40mg olmesartan for specific blocking of AT1R shows complete absence
of myocardial [11C]-KR31173 uptake, confirming tracer specificityfor the receptor. Tracer is only present in the blood pool of atria andventricles. Reproduced with permission from: Fukushima K, et al.Molecular hybrid positron emission tomography/computed tomogra-phy imaging of cardiac angiotensin II type 1 receptors. J Am CollCardiol. 2012:60:2527–34 [47••]
Curr Cardiol Rep (2014) 16:466 Page 5 of 8, 466

to allow external imaging with PET (Fig. 3) [47••]. Myocardialretention of [11C]-KR31173 was visually detectable in 4healthy volunteers, which was homogenously distributed inthe myocardium and stable over time. However, myocardialretention of KR31173 in these healthy human subjects wassignificantly lower (nearly 4-fold) than those in normal healthypigs, and only 54 % of the receptors were blocked after pre-treatment with olmesartan (AT1R blocking agent), suggestinglimited specificity [48]. Additional experiments performed inyoung farm pigs under healthy conditions and 3–4 weeks aftermyocardial infarction showed AT1R upregulation in the in-farcted area when compared with remote myocardium [47••].Moreover, the retention of KR31173 in infarcted and remotemyocardium was significantly higher than in the myocardiumof healthy pigs. In postmortem immunohistochemistry analy-sis, anti-AT1R antibody binding was localized to spindle-shaped cells, presumably myofibroblasts, in the infarct region,while there was also significant binding to cardiomyocytes inremote areas [48]. These findings in pigs are similar to thoseobserved in experimental mouse model of postinfarction heartfailure where in vivo AT1R imaging was accomplished withTc-99 m losartan micro SPECT-CT and immunohistochemicalanalysis showed binding of the radiotracer almost exclusivelyin the myofibroblast rather than cardiomyocytes [49]. Thus,while the [11C]-KR31173 imaging signal identifies AT1R ex-pression in the myocardium, it does not differentiate betweenmyofibroblast and cardiomyocyte cell types and with 54 % ofthe receptors blocked after pre-treatment with an AT-1 blocker,it has limited specificity [48].
Losartan, the first ARB that was used clinically, has alsobeen radiolabeled and used in experimental settings. Thechelate-coupled losartan-Leu-Diglycoloyl-PEG(4)-tetraamine,with higher affinity for AT1R compared with the parent drug,was radiolabeled with 99mTc and used for cardiac imaging in amouse model of acute myocardial infarction [49]. In vivomicro SPECT-CTshowed an increase uptake within the infarctregion 3 weeks after coronary ligation. The specific binding ofthe tracer to AT1R receptor was verified with immunohisto-chemical studies. The potential use of 99mTc-losartan in clinicalstudies is encouraged by the fact that the radiotracer can besynthesized rapidly and effectively at a high radiochemicalyield and high uptake in the heart when studied in the mouse[50]. Radiolabeling of losartan for PET imaging ([11C]-losartan) has also been successfully done at high radiochemicalpurity [51].
Finally, candesartan, a more lipophilic ARB than the pro-totype drug losartan, has been successfully labeled with [11C]as a potential PET tracer and is shown to specifically andcompetitively bind to AT1R [52]. The radiotracer was origi-nally made with the hope that the high lipophilicity wouldallow the agent to cross the blood brain barrier and provide ameans for imaging intracerebral AT1R. However, in practice,it did not cross into the brain in sufficient amount to allow
detection of the receptors in the brain. Preliminary evaluationof this PET radioligand ([11C]-methyl-candesartan) has shownpromising results for in vivo detection of changes in AT1Rreceptor density in the rat kidney [53].
Conclusions and Future Directions
RAS is a system of ever-increasing complexity with numerousbiologically active components often with opposing cellulareffects [54••]. In clinical management of patients with leftventricular systolic dysfunction, however, the activities of sev-eral components of the system appear to have themost profoundeffects on systemic and tissue response to injury and persistentabnormal stimuli [55•]. Among these, AII and aldosteroneappear to be the most influential and have been the primarytargets of established and novel pharmacologic interventionsaimed at amelioration of adverse cardiac remodeling [55•, 56,57]. RAS blockade in heart failure, however, remains challeng-ing due to the absence of reliable clinical markers of adequatetarget inhibition and potential for serious side effects that maylimit clinical benefits and affect outcomes [58]. Dose titration,dual RAS blockade, alternative therapy, and identification ofreactivation of the system through alternative pathways aresome of the important clinical questions that are largely unan-swered at this time [59]. Molecular imaging is well poised toprovide important insights into these clinically relevant ques-tions through application of advanced imaging techniques andsophisticated molecular probes [60, 61]. Combined assessmentand serial evaluation of myocardial ACE activity and AT1Rholds great promise for the most efficacious modulation ofRAS in patients with left ventricular systolic function.
Compliance with Ethics Guidelines
Conflict of Interest Jamshid Shirani declares that he has no conflict ofinterest. Vasken Dilsizian declares that he has no conflict of interest.
Human and Animal Rights and Informed Consent This article doesnot contain any studies with human or animal subjects performed by anyof the authors.
References
Papers of particular interest, published recently, have beenhighlighted as:• Of importance•• Of major importance
1.•• Burchfield JS, XieM, Hill JA. Pathological ventricular remodeling:mechanisms: part 1 of 2. Circulation. 2013;128:388–400. Seereference 2.
466, Page 6 of 8 Curr Cardiol Rep (2014) 16:466

2.•• XieM, Burchfield JS, Hill JA. Pathological ventricular remodeling:therapies: part 2 of 2. Circulation. 2013;128:1021–130. This 2-partmanuscript is an in-depth up-to-date review of cellular and molec-ular aspects of left ventricular remodeling and anti-remodelingtherapies in various cardiac diseases.
3.•• Lang CC, Struthers AD. Targeting the renin-angiotensin-aldosteronesystem in heart failure. Nat Rev Cardiol. 2013;10:125–34. Thisreview article discusses new indications for established inhibitorsof the renin-angiotensin system as well as novel pharmacologicapproaches to various components of this system with higherefficacy.
4. Ishizawar D, Yancy C. Racial differences in heart failure therapeu-tics. Heart Fail Clin. 2010;6:65–74.
5.• Hilliard LM, Sampson AK, Brown RD, Denton KM. The "his andhers" of the renin-angiotensin system. Curr Hypertens Rep.2013;15:71–9. This is a comprehensive review of the gender differ-ences in the biologic function of the renin-angiotensin system withparticular reference to the effects of the sex hormones.
6. Davis HM, Johnson JA. Heart failure pharmacogenetics: past,present, and future. Curr Cardiol Rep. 2011;13:175–84.
7.• Gregori M, Tocci G, Marra A, et al. Inadequate RAAS suppressionis associated with excessive left ventricular mass and systo-diastolicdysfunction. Clin Res Cardiol. 2013;102:725–33. In this study of115 newly diagnosed hypertensive patients, inadequate suppressionof plasma renin activity, and aldosterone level was associated withhigher echocardiographic left ventricular mass and Doppler evi-dence of myocardial performance abnormalities.
8. Mallat SG. Dual renin-angiotensin system inhibition for preventionof renal and cardiovascular events: do the latest trials challengeexisting evidence? Cardiovasc Diabetol. 2013;12:1–12.
9.• Bernstein KE, Ong FS, BlackwellWL, et al. Amodern understandingof the traditional and nontraditional biological functions ofangiotensin-converting enzyme. Pharmacol Rev. 2012;65:1–46. Thisis an interesting historical perspective on the angiotensin convertingenzyme with an up-to-date discussion of its diverse biologic actionsparticularly in reference to the 2 homologous catalytic domains.
10. Strittmatter SM, Kapiloff MS, Snyder SH. [3H]Captopril binding tomembrane associated angiotensin converting enzyme. BiochemBiophys Res Commun. 1983;112:1027–33.
11. Strittmatter SM, Snyder SH. Characterization of angiotensinconverting enzyme by [3H]captopril binding. Mol Pharmacol.1986;29:142–8.
12. Wilson SK, Lynch DR, Snyder SH. Angiotensin-converting en-zyme labeled with [3H]captopril. Tissue localizations and changesin different models of hypertension in the rat. J Clin Invest.1987;80:841–51.
13. Hwang DR, Eckelman WC, Mathias CJ, et al. Positron-labeledangiotensin-converting enzyme (ACE) inhibitor: fluorine-18-fluorocaptopril. Probing the ACE activity in vivo by positronemission tomography. J Nucl Med. 1991;32:1730–7.
14. Qing F, McCarthy TJ, Markham J, Schuster DP. Pulmonaryangiotensin-converting enzyme (ACE) binding and inhibition inhumans. A positron emission tomography study. Am J Respir CritCare Med. 2000;161:2019–25.
15. Markham J, McCarthy TJ, Welch MJ, Schuster DP. In vivo mea-surements of pulmonary angiotensin-converting enzyme kinetics. I.Theory and error analysis. J Appl Physiol. 1995;78:1158–68.
16. Schuster DP, McCarthy TJ, Welch MJ, et al. In vivo measure-ments of pulmonary angiotensin-converting enzyme kinetics. II.Implementation and application. J Appl Physiol. 1995;78:1169–678.
17. Abadir PM, Walston JD, Carey RM. Subcellular characteristics offunctional intracellular renin-angiotensin systems. Peptides. 2012;38:437–45.
18. Matarrese M, Salimbeni A, Turolla EA, et al. 11C-Radiosynthesisand preliminary human evaluation of the disposition of the ACEinhibitor [11C]zofenoprilat. Bioorg Med Chem. 2004;12:603–11.
19. Jackson B, Cubela R, Johnston CI. Angiotensin-converting enzyme(ACE) measurement in human serum using radioinhibitor ligandbinding. Aust J Exp Biol Med Sci. 1986;64:149–55.
20. Jackson B, Cubela R, Johnston C. Angiotensin converting enzyme(ACE), characterization by 125I-MK351A binding studies of plas-ma and tissue ACE during variation of salt status in the rat. JHypertens. 1986;4:759–65.
21. Johnston CI, Cubela R, Sakaguchi K, Jackson B. Angiotensinconverting enzyme inhibition in plasma and tissues. Clin ExpHypertens [A]. 1987;9:307–21.
22. Yamada H, Fabris B, Allen AM, et al. Localization of angiotensinconverting enzyme in rat heart. Circ Res. 1991;68:141–9.
23. Kohzuki M, Kanazawa M, Yoshida K, et al. Cardiac angiotensinconverting enzyme and endothelin receptor in rats with chronicmyocardial infarction. Jpn Circ J. 1996;60:972–80.
24. Burrell LM, Droogh J, Man in't Veld O, et al. Antihypertensive andantihypertrophic effects of omapatrilat in SHR. Am J Hypertens.2000;13:1110–6.
25. Kubota E, Dean RG, Hubner RA, et al. Differential tissue andenzyme inhibitory effects of the vasopeptidase inhibitor omapatrilatin the rat. Clin Sci. 2003;105:339–45.
26. Natesh R, Schwager SL, Sturrock ED, Acharya KR. Crystal struc-ture of the human angiotensin-converting enzyme-lisinopril com-plex. Nature. 2003;421:551–4.
27. Pandurangi RS, Lusiak P, Kuntz R, Sun Y, Weber KT. Chemicaland photochemical modification of angiotensin converting enzymeinhibitors: implications in the development of cardiac radionuclideimaging agents. Bioorg Chem. 1997;25:77–87.
28. Lee YHC, Kiesewetter DO, Lang L, et al. Synthesis of 4-[18F]fluorobenzoyllisinopril: a radioligand for angiotensinconverting enzyme (ACE) imaging with positron emission tomog-raphy. J Label Compd Radiopharm. 2001;44:S268–70.
29.•• Dilsizian V, Eckelman WC, Loredo ML, Jagoda EM, Shirani J.Evidence for tissue angiotensin-converting enzyme in explantedhearts of ischemic cardiomyopathy using targeted radiotracer tech-nique. J Nucl Med. 2007;48:182–7. High-affinity F-18 labeledfluorobenzoyl-lisinopril was shown to specifically localize in ex vivomyocardial samples obtained from explanted cardiomyopathic heartsin cardiac allograft recipients by autoradiography.
30. Femia FJ, Maresca KP, Hillier SM, et al. Synthesis and evaluationof a series of 99mTc(CO)3+ lisinopril complexes for in vivo imag-ing of angiotensin-converting enzyme expression. J Nucl Med.2008;49:970–7.
31.•• Dilsizian V, Zynda TK, Petrov A, et al. Molecular imaging ofhuman ACE-1 expression in transgenic rats. J Am Coll CardiolImg. 2012;5:409–18. In human ACE-1 over-expressing transgenicrats, technetium-99m-labeled lisinopril was shown to provide asignal intensity that is sufficiently high to allow external microSPECT-CT imaging.
32. Yancy CW, Lee DC. Personalized medicine in heart failure: are wethere yet? J Am Coll Cardiol Img. 2012;5:419–21.
33. Fillion D, Cabana J, Guillemette G, et al. Structure of the humanangiotensin II type 1 (AT1) receptor bound to angiotensin II frommultiple chemoselective photoprobe contacts reveals a unique pep-tide binding mode. J Biol Chem. 2013;288:8187–97.
34. Chang RS, Lotti VJ. Two distinct angiotensin II receptor bindingsites in rat adrenal revealed by new selective nonpeptide ligands.Mol Pharmacol. 1990;37:347–51.
35. Whitebread S, Mele M, Kamber B, de Gasparo M. Preliminarybiochemical characterization of two angiotensin II receptor sub-types. Biochem Biophys Res Commun. 1989;163:284–91.
36. Martin RP, Rodrigues ES, PachecoNA, et al. Distinct bindingmodeof 125I-AngII to AT1 receptor without the Cys18-Cys274 disulfidebridge. Regul Pept. 2009;158:14–8.
37. Caballero-George C, Vanderheyden PM,DeBruyne T, et al. In vitroinhibition of [3H]-angiotensin II binding on the humanAT1 receptor
Curr Cardiol Rep (2014) 16:466 Page 7 of 8, 466

by proanthocyanidins from Guazumaulmifolia bark. Planta Med.2002;68:1066–71.
38. Gibson RE, Beauchamp HT, Fioravanti C, Brenner N, Burns HD.Receptor binding radiotracers for the angiotensin II receptor:radioiodinated [Sar1, Ile8]Angiotensin II. Nucl Med Biol.1994;21:593–600.
39. Mathews WB, Burns HD, Dannals RF, Ravert HT, Naylor MN.Carbon-11 labeling of the potent nonpeptide angiotensin-II antag-onist MK-996. J Label Compd Radiopharm. 1995;36:729–37.
40. Hamill TG, Burns HD, Dannals RF, et al. Development of [11C]L-159,884: a radiolabelled, nonpeptide angiotensin II antagonist thatis useful for angiotensin II, AT1 receptor imaging. Appl Radiat Isot.1996;47:211–8.
41. Kim SE, Scheffel U, Szabo Z, et al. In vivo labeling of angiotensinII receptors with a carbon-11-labeled selective nonpeptide antago-nist. J Nucl Med. 1996;37:307–11.
42. Szabo Z, Kao PF, Burns HD, et al. Investigation of angiotensin II/AT1 receptors with carbon-11-L-159,884: a selective AT1 antago-nist. J Nucl Med. 1998;39:1209–13.
43. Mathews WB, Yoo SE, Lee SH, et al. A novel radioligand forimaging the AT1 angiotensin receptor with PET. Nucl Med Biol.2004;31:571–4.
44. Higuchi T, Fukushima K, Xia J, et al. Radionuclide imaging ofangiotensin II type 1 receptor upregulation after myocardialischemia-reperfusion injury. J Nucl Med. 2010;51:1956–1961.
45. Zober TG, Mathews WB, Seckin E, et al. PET Imaging of the AT1receptor with [11C]KR31173. Nucl Med Biol. 2006;33:5–13.
46. Gulaldi NC, Xia J, Feng T, et al. Modeling of the renal kinetics ofthe AT1 receptor specific PET radioligand[ 11 C]KR31173.Biomed Res Int. 2013;2013:1–12.
47.•• Fukushima K, Bravo PE, Higuchi T, et al. Molecular hybrid posi-tron emission tomography/computed tomography imaging of car-diac angiotensin II type 1 receptors. J Am Coll Cardiol. 2012:60:2527–34. The first-in-man application of receptor ligand [11C]-KR31173 combined with PET/CT that confirmed the presence oflocal tissue RAS in human hearts, proved to be safe and that thesignal was high enough to allow external imaging with PET.
48. Schindler TH, Dilsizian V. Cardiac positron emission tomography/computed tomography imaging of the renin-angiotensin system inhumans holds promise for image-guided approach to heart failuretherapy. J Am Coll Cardiol. 2012;5:1269–84.
49. Verjans JW, Lovhaug D, Narula N, et al. Noninvasive imaging ofangiotensin receptors after myocardial infarction. J Am CollCardiol Img. 2008;1:354–62.
50. Ibrahim IT, Sanad MH. Radiolabeling and biological evaluation oflosartan as a possible cardiac imaging agent. Radiochemistry.2013;55:336–40.
51. Hadizad T, Collins J, Antoun RE, Beanlands RS, DaSilva JN.[11C]Methyl-losartan as a potential ligand for PET imagingangiotensin II AT1 receptors. J Label Compd Radiopharm.2011;54:754–7.
52. Hadizad T, Kirkpatrick SA, Mason S, et al. Novel O-[(11)C]methylated derivatives of candesartan as angiotensin IIAT(1) receptor imaging ligands: radiosynthesis and ex vivo evalu-ation in rats. Bioorg Med Chem. 2009;17:7971–7.
53. Lortie M, DaSilva JN, Kirkpatrick SA, et al. Analysis of[11C]methyl-candesartan kinetics in the rat kidney for the assess-ment of angiotensin II type 1 receptor density in vivo with PET.Nucl Med Biol. 2013;40:252–61.
54.•• Santos RA, Ferreira AJ, Verano-Braga T, Bader M. Angiotensin-converting enzyme 2, angiotensin-(1-7) and Mas: new players ofthe renin-angiotensin system. J Endocrinol. 2013;216:R1–R17.This manuscript thoroughly explores the role of newly identifiedcomponents in the overall biologic function of the renin-angiotensinsystem.
55.• McMurray JJ. CONSENSUS to EMPHASIS: the overwhelmingevidence which makes blockade of the renin-angiotensin-aldosteronesystem the cornerstone of therapy for systolic heart failure. Eur J HeartFail. 2011;13:929–36. This is an excellent expert review of theestablished clinical benefits of renin-angiotensin system inhibition inleft ventricular systolic dysfunction.
56. Pitt B, Filippatos G, Gheorghiade M, et al. Rationale and design ofARTS: a randomized, double-blind study of BAY 94-8862 inpatients with chronic heart failure and mild or moderate chronickidney disease. Eur J Heart Fail. 2012;14:668–75.
57. Pitt B, Kober L, Ponikowski P, Gheorghiade M, et al. Safety andtolerability of the novel nonsteroidal mineralocorticoid receptorantagonist BAY 94-8862 in patients with chronic heart failure andmild or moderate chronic kidney disease: a randomized, double-blind trial. Eur Heart J. 2013;34:2453–563.
58. Kiernan MS, Wentworth D, Francis G, et al. Predicting adverseevents during angiotensin receptor blocker treatment in heartfailure: results from the HEAAL trial. Eur J Heart Fail.2012;14:1401–9.
59. Horiuchi M, Iwanami J, Mogi M. Regulation of angiotensin IIreceptors beyond the classical pathway. Clin Sci (Lond). 2012;123:193–203.
60. Dilsizian V, Taillefer R. Journey in evolution of nuclear cardiology:will there be another quantum leap with the F-18 labeled myocar-dial perfusion tracers? J Am Coll Cardiol Img. 2012;5:1269–84.
61. Buxton DB, Antman M, Danthi N, et al. Report of the NationalHeart, Lung, and Blood Institute Working Group on thetranslation of cardiovascular molecular imaging. Circulation.2011;123:2157–63.
466, Page 8 of 8 Curr Cardiol Rep (2014) 16:466