Embed Size (px)
Citation preview

Review
10.1517/13543780903241615 © 2009 Informa UK Ltd ISSN 1354-3784 1619All rights reserved: reproduction in whole or in part not permitted
NovelinvestigationaladenosineA2AreceptorantagonistsforParkinson’sdiseaseAnnalisa PinnaNational Research Council CNR, Institute of Neuroscience – Cagliari. c/o Department of Toxicology, University of Cagliari, Via Ospedale 72, 09124 Cagliari, Italy
The development of non-dopaminergic therapies for Parkinson’s disease (PD) has attracted much interest in recent years. Among new classes of drugs, adenosine A2A antagonists have emerged as the best candidates. BIIB014, preladenant and ST-1535 are new adenosine A2A antagonists currently in Phase I and II clinical trials for evaluation of their efficacy in patients with PD. All these compounds have been proven safe and well tolerated. Moreover, results from Phase II trials also demonstrate that BIIB014 and preladenant are effective in reducing the waking time spent in OFF state in patients at the late stage of PD treated with L-DOPA. BIIB014 is also efficacious as monotherapy in patients at the early stage of PD. Finally, ST-1535, at this time, displays a very promising potential in experimental models of PD and a safe profile in clinical studies. This review summarizes pharmacological data available on these three A2A antagonists, their effects in animal models of PD and their profiles in clinical trials.
Keywords: adenosine A2A receptor antagonists, BIIB014, clinical trials, Parkinson’s disease, preladenant, ST-1535
Expert Opin. Investig. Drugs (2009) 18(11):1619-1631
1. Generaloverview
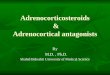
Parkinson’s disease (PD) is an age-related chronic neurological disorder characterized by rest tremor, bradykinesia, rigidity, gait and postural instability and a variety of non-motor symptoms (including sleep disturbance, depression and decline in cognition) [1,2]. The pathophysiological hallmark of PD is a progressive loss of dopaminergic neurons in the substantia nigra pars-compacta (SNc). This leads to a deficiency of the neurotransmitter dopamine in the caudate-putamen (CPu, also named striatum), which results in alterations in the activity of neural circuits within the basal ganglia (BG) that regulate movement (Figure 1) [1].
The cause of neurodegeneration in PD is unknown, but growing evidence suggests that it might be multifactorial in terms of both etiology and pathogenesis. A combination of environmental and genetic factors, toxins, genetic susceptibility and the aging process may accent for PD etiology [3]. Furthermore, several ascer-tained contributing factors to PD pathogenesis are oxidative stress, mitochondrial dysfunction, excitotoxicity and altered proteolysis [4].
The disease is found in all ethnic groups, but with geographical differences in prevalence. As PD is mainly an illness of aged people, it is more common in devel-oped countries where people live longer such as the US and Europe [5,6]. Early onset of sporadic PD is rare, as about 4% of patients develop clinical signs of the disease before an age of 50 years [7]. PD affects 1 – 2% of the population > 65 years and increases to 3 – 5% in people aged 85 year and older [8]. Recently, a prevalence projection report suggested that number of individuals afflicted by PD is expected to double by 2030, in line with the increase in aging population and life
1. General overview
2. Adenosine A2A receptor
antagonists
3. BIIB014
4. Preladenant
5. ST-1535
6. Conclusions
7. Expert opinion
Exp
ert O
pin.
Inv
estig
. Dru
gs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Hon
g K
ong
on 0
5/13
/13
For
pers
onal
use
onl
y.

NovelinvestigationaladenosineA2AreceptorantagonistsforParkinson’sdisease
1620 ExpertOpin.Investig.Drugs(2009) 18(11)
expectancy [9]. PD is not considered a ‘fatal’ disease, but mortality in PD patients is generally higher than that of the general population, regardless of L-DOPA or other therapy [8]. Death is typically caused by secondary complications of the disease; pneumonia is the most common, followed by cardio-vascular events (including stroke) and cancer [2,8]. PD is asso-ciated with an enormous economic burden in the US and other countries [8]. Estimates of annual direct costs of care in the US vary considerably from < $2000 to > $15,000 per patient. Cost burden is particularly evident in advanced PD
with severe symptoms, where the poorer quality of life caused by health problems, reduced productivity and even greater need for healthcare services drive up both direct and indirect costs [10]. Moreover, direct costs for drug therapy increase sig-nificantly with clinical progression of symptoms [10]. More effective management of PD, especially development of drugs that could slow down the disease progression, might potentially reduce healthcare resource utilization and associated costs [10].
The total economic burden of PD in the US was projected to be $23 billion annually. Almost 70% of this burden was
B.
A2A
DYN
SP
GABA
ENK
GABA
D1 D2
GABA
Glu
Th
Cortex
GABA
A2A
Glu
GP
SNr
CPuCPu
STh
A.
Glu
DYN
SP
GABA
ENK
GABA
D1 D2 A2A
GABA
Glu
Th
Cortex
GABA
A2A
GP
SNr
CPuCPu
STh
Figure1.Schematicrepresentationofregional(coronalsectionsofratbrain)andcellularlocalizationofA2AreceptorsintheCPuprovidingthebasisofanti-ParkinsonianactionofA2Aantagonists. As shown in both panels representing the two major CPu GABA-containing output pathways, A2A receptors are largely restricted to GABA-containing neurons that express dopamine D2 receptors and ENK and project to the GP. By contrast, GABA-containing neurons projecting directly to SNr are rich in D1 receptors, DYN and SP with no appreciable expression of A2A receptors. A. Parkinson’s disease. Dopamine depletion occurring in CPu produces a reduced stimulation of both dopamine D1 and D2 receptors resulting in a decrease in inhibition of GABA-containing CPu-GP neurons and an attenuated excitation of direct GABA-containing pathway which leads to a reduction of inhibitory control on the SNr. The attenuated inhibition of GP neurons disinhibits the excitatory Glu transmission of the STh. The resulting imbalance between the activity of the two pathways leads to a marked increase of inhibitory output from the SNr and excessive inhibition of Th-cortex neurons resulting in reduction of movements. B. A2A receptor blockade in Parkinson’s disease should mitigate overactivity of striatopallidal and STh-SNr neurons, thus, restoring some balance between the indirect and the direct pathways. A2A antagonist coadministered with a low dose of L-DOPA (which increases dopamine levels that stimulate both D1 and D2 receptors) would facilitate the inhibitory cellular action of D2 receptors on striatopallidal neurons and, in turn, through the basal ganglia circuit, may indirectly facilitate activation of the striatonigral pathway stimulated by D1 receptors.CPu: Caudate-putamen; DYN: Dynorphin; ENK: Enkephalin; Glu: Glutamatergic; GP: Globus pallidus; SNr: Substantia nigra reticulata; SP: Substance P;
STh: Subthalamic nucleus; Th-cortex: Thalamo-cortical.
Exp
ert O
pin.
Inv
estig
. Dru
gs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Hon
g K
ong
on 0
5/13
/13
For
pers
onal
use
onl
y.

Pinna
ExpertOpin.Investig.Drugs(2009) 18(11) 1621
estimated to depend on indirect costs in terms of productivity loss, provision of uncompensated care by family and house-hold members; while the 4% of the total burden was the estimated value of the global market for PD medications [8]. Current drug therapy of PD is symptomatic and primarily aimed at restoring dopaminergic function in the CPu, usually by the administration of the dopamine precursor L-DOPA (in combination with a peripheral decarboxilase inhibitor), which is still the most efficacious treatment. Besides its proven efficacy, L-DOPA is well tolerated, easy to administer and relatively inexpensive. However, disabling complications, such as motor fluctuations (wearing off and on–off phenomena) and dyskinesia, are frequent after several years of L-DOPA therapy in the majority of PD patients [11]. Accordingly, L-DOPA is habitually administered in association with other drugs, including direct dopamine agonists, anticholinergics and agents capable of delaying the dopamine catabolism (MAO-B and COMT inhibitors), to reduce the dose of L-DOPA required to counteract PD motor disabilities. Recently, treat-ment during the early stage of PD has evolved, and evidence suggests that dopamine agonist monotherapy may prevent the response fluctuations that are associated with disease progression [12]. Moreover, treatment during the advanced stage focuses on improving control of a number of specific clinical problems. Successful management of motor response fluctuations, dyskinesias and of psychiatric problems is often possible with specific treatment strategies [13]. However, drugs currently administered with L-DOPA either elicit adverse effects (AEs), limiting their therapeutic usage, or display an inadequate effectiveness on Parkinsonian motor disabilities, often restricted to the early stages of the disease. Furthermore, although deep brain stimulation or lesion surgery are effective in improving motor function and motor-related complica-tions in PD, these surgical treatments are an option restricted to a defined patient population [14,15]. Therefore, if quality of life is to be maintained and the socio-economic burden is to be reduced, more effective anti-Parkinsonian therapies need to be developed for use over a longer portion of the illness duration. This requires new pharmacological approaches to PD management.
2. AdenosineA2Areceptorantagonists
The inadequacies and AEs of drugs that target the dopaminergic system have prompted a search for alternative or adjunctive non-dopaminergic approaches that can modulate BG motor circuit with a reduced risk of side effects.
In the field of newly developed drugs, antagonists of adenosine A2A receptors have recently emerged as the best candidate class of non-dopaminergic antiparkinsonian agents, based in part on their peculiar enrichment in CPu, whose functionality is critically compromised in PD (Figure 1) [16,17]. Moreover, within the Cpu, adenosine A2A receptors are largely restricted to the striatopallidal neurons, where they are co-expressed with dopamine D2 receptors (Figure 1) [18,19].
This discreet anatomical localization reduces the liability of A2A antagonists for adverse CNS effects, such as those that limit the usefulness of current non-dopaminergic (anti-cholinergic and anti-glutamatergic) agents in PD. Furthermore, A2A antag-onists consistently reverse Parkinsonian motor deficits in all preclinical models of PD, and do so without inducing or exacerbating dyskinesias in non-human primate models [17,20]. Concerning the mechanism by means of which A2A antagonists reverse motor disability in PD animal models, solid evidence accounts for a crucial role of the opposite interactions between A2A and dopamine D2 receptors. Hence, A2A receptor antag-onists, by acting at the striatopallidal neuronal level, enhance D2-mediated effects (Figure 1). Furthermore, A2A receptor blockade indirectly increases the effects induced by activa-tion of D1 receptors present in the striatonigral neurons (Figure 1) [21,22]. Therefore, A2A antagonists exert a facili-tatory action on dopamine transmission that may result in motor activation, clarifying the beneficial effect of these drugs on Parkinsonian motor deficits (Figure 1) [17,20,23]. Other potential mechanisms of action may, however, exist [17,20,23]. Moreover, the recent discovery that the A2A receptor can form functional heteromeric complexes with other GPCR, such as D2 and mGlu5 receptors, has suggested new opportunities for modulating the multiple potential anti-Parkinsonian benefits of A2A antagonists [24]. Additionally, the A2A antago-nists might have some neuroprotective effects, potentially slowing down the disease progression. Epidemiological data that connected the consumption of caffeine (a non-selective adenosine antagonist) with a reduced risk of developing PD converge with laboratory studies showing that caffeine and more selective A2A antagonists protect against dopaminergic neuron toxicity in rodent models of Parkinsonian neurode-generation [17,23,25-27]. These data suggested a preventive action of A2A antagonists on PD onset and development [17,20,23,28]. The mechanism by which A2A receptor blockade mediates neuroprotection in PD is still unclear; however, several studies have suggested that neuroinflammation may play an active role in the pathogenesis of neurodegeneration in PD, because reactive astrogliosis and microgliosis, have been described in the SNc of PD patients and 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP)-treated primates [29-31]. Further-more, blockade of microglia reactivity in mice recovered dopamine neurons from acute MPTP toxicity [32] and pre-treatment with A2A antagonists resulted in dopamine neurons neuroprotection and inhibition of astroglial response in the CPu [33] or microglia activation in SNc [34], suggesting a causal relation between the two events (for a review see [28,35]). Finally, recent results hypothesize a critical modulation of cognition by adenosine A2A receptors, and A2A antagonists have proven to ameliorate cognitive dysfunction in different experimental paradigms, including dopamine-depleted rats [36]. On the basis of these considerations, several A2A antagonists, both xantine and non-xantine derivatives, have been pro-duced and some of them are being tested as treatment for Parkinsonian patients in several clinical trials.
Exp
ert O
pin.
Inv
estig
. Dru
gs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Hon
g K
ong
on 0
5/13
/13
For
pers
onal
use
onl
y.

NovelinvestigationaladenosineA2AreceptorantagonistsforParkinson’sdisease
1622 ExpertOpin.Investig.Drugs(2009) 18(11)
The extensively studied A2A antagonist appears to be istradefylline (also known as KW-6002) a xanthine derivative that recently completed clinical trials in which it proved capable of alleviating symptoms associated with PD [23,37,38]. However, this compound did not receive the approval by the FDA in 2008, as the agency expressed concern whether the results in clinical trials supported the clinical utility for istradefylline and asked for more thorough clinical investigations [39]. Additional reports have disclosed further matters that may have implications for the clinical utility of this compound, including metabolic issues and poor photostability in both solid form and solution [40].
At the same time, a number of pharmaceutical companies have progressed A2A antagonists into clinical trials including BIIB014 (V2006; 3-(4-amino-3-methylbenzyl)-7-(2-furyl)-3H-[1,2,3]triazolo[4,5-d]pyrimidine-5-amine) from Vernalis plc-Biogen Idec (Figure 2), preladenant (SCH-420814; 2-(furan-2-yl)-7-[2-[4-[4-(2-methoxyethoxy)phenyl]piperazin- 1-yl]ethyl]-7H-pyrazolo[4,3-e][1,2,4]triazolo[1,5-c]pyrimidin- 5-amine) from Schering-Plough Corp. (Figure 3) and ST-1535 (2-butyl-9-methyl-8-(2H-1,2,3-triazol 2-yl)-9 H-purin-6-ylamine) from Sigma-Tau (Figure 4). This review focuses on data available on these three A2A antagonists that at this time are in progress in their clinical evaluation (Phase II for BIIB014 and preladenant; Phase I for ST-1535). Currently, other companies working in this field include Adenosine Thera-peutics, Neurocrine Biosciences and Almirall Prodesfarma, although little is known about their development candidates at this stage [38,41].
3. BIIB014
3.1 Chemical,pharmacodynamicandpharmacokineticstudiesRecently, Weiss et al. (2003) [42] reported that during a program investigating the biochemical basis of side effects
associated with the antimalarial drug mefloquine, it was discovered that the (-)-(R,S)-enantiomer of the drug is a potent and moderately selective antagonist of A2A receptors [42]. The efforts to optimize this non-xantine compound, and a number of related derivatives, in order to find a candidate compound with a suitable profile for clinical development led to the discovery of BIIB014 (also known as V2006), a small molecule with appropriate characteristics for clinical anti-Parkinsonian evaluation (Figure 2) [43].
BIIB014 is a triazolo[4,5-d]pyrimidine derivative (manufac-tured by Vernalis plc which entered into an agreement with Biogen Idec to develop and commercialize it) that displays high affinity for A2A receptor, with a Ki value of 1.3 nM, and selectivity for the A2A receptor subtype (> 50-fold versus A1 and A2B receptors and > 1000-fold versus A3 receptor) (Table 1) [43,44]. Further examination of possible off-target effects of BIIB014 demonstrated selectivity for A2A receptors greater than 500-fold with respect to all the other 75 targets investigated [43]. Functional activity determined in cells by assessing Ca2+ mobilization using a fluorescence imaging plate reader demonstrated that BIIB014 acts as a functional antago-nist of A2A receptor in good agreement with the radioligand binding assay. This study also demonstrated that BIIB014 is devoid of any intrinsic agonist activity [43].
In vitro metabolic studies indicate that BIIB014 is metab-olized by multiple CYP isoforms, suggesting a low propensity for drug–drug interactions or variable pharmacokinetics due to CYP polymorphisms. Furthermore, the compound showed a low potential for inhibition or induction of the major CYP isoforms [43,45].
In absorption, distribution, metabolism and elimination studies with [14C]-BIIB014 in rats and cynomolgus monkeys, the compound was found to be eliminated predominantly in feces, with BIIB014 being the major component in this matrix [45]. No sex-differences were observed in the rate and route of elimination of BIIB014. Quantitative whole body auto-radiography studies in the rat indicated that [14C]-BIIB014 was widely distributed throughout the body following both intravenous and oral dosing [45].
Moreover, in vivo pharmacokinetic studies in rats and cynomolgus monkey show that BIIB014 possesses good oral bioavailability, a long plasma half-life and good brain pene-tration. Specifically, rat pharmacokinetics demonstrated an esti-mated half-life of 2 – 6 h and an oral bioavailability of about 35%. A measured brain uptake of 57% indicates good penetration of the compound from plasma into the whole brain and cerebrospinal fluid [43,45]. The cross species metabolic profile of BIIB014 was qualitatively similar, with the cynomolgus monkey being most similar to humans. As a consequence, the cynomolgus monkey was chosen as the non-rodent toxicology species for BIIB014. The plasma protein binding of BIIB014 was the highest in humans and cynomolgus monkey and lower in rat, rabbit and mouse, respectively [45].
Pharmacokinetic studies in healthy young and elderly humans demonstrated that BIIB014 plasma concentrations
N
N
O
N
N
N NH2
H2N
Me
BIIB014 (V6002)
Figure2.ChemicalstructureofBIIB014.
Exp
ert O
pin.
Inv
estig
. Dru
gs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Hon
g K
ong
on 0
5/13
/13
For
pers
onal
use
onl
y.

Pinna
ExpertOpin.Investig.Drugs(2009) 18(11) 1623
were measurable after all doses (5, 10, 15, 25, 50 and 100 mg) used. In particular, absorption was rapid (tmax 2 – 4 h), and dose proportionally seen up to 15 mg (fasted). Exposure between 15 and 100 mg increased but less-than-dose pro-portionally. Food improved absorption, increasing maximum concentration (Cmax) (not AUC) after a 10 mg dose, and this effect could be observed proportionally up to doses of 50 mg [45]. BIIB014 had a moderate apparent clearance and a low to moderate apparent volume of distribution giving a half-life of 10 – 25 h, allowing single daily dosing. There was slight accumulation on repeated dosing but no evidence of self-induction or inhibition. Time to steady-state was 5 days, consistent with half-life. Although advanced age (≥ 65 years old) influenced disposition of BIIB014 at high doses, steady-state was still achieved by day 5 and dose reductions are not required in this population. Moreover, BIIB014 did not display mutual pharmacokinetic interaction with L-DOPA–carbidopa combination (Sinemet® 10/100) [46]. Therefore, pharmacoki-netics of BIIB014 in healthy subjects is appropriate for further development of this compound as a single daily treatment [46].
In addition, an open-label positron emission tomography (PET) study with a multiple dose of BIIB014 (administered orally for 8 – 12 consecutive days) was made to evaluate the occupancy of A2A receptors in the brain (CPu, nucleus accum-bens, thalamus and cerebellum) of healthy male volunteers [47]. The radiotracer used was [11C]SCH-442416 that exhibited high affinity (Ki = 0.048 nM) and selectivity (> 20,000-fold versus A1, A2A and A3) for A2A receptors [48]. The results of this PET study are not yet published.
N N
N
N O
N
NH2
N
N NO
OCH3
Preladenant (SCH-420814)
Figure3.Chemicalstructureofpreladenant.
N
N N
N
N
N
N
NH2
ST-1535
Figure4.ChemicalstructureofST-1535.
3.2 PreclinicalstudiesinexperimentalmodelsofPDSeveral preclinical studies examining BIIB014 in PD exper-imental models have been performed in order to evaluate the in vivo activity as an anti-Parkinsonian drug before its clinical investigation.
First of all, the in vivo activity of BIIB014 was tested in the mouse and rat models of haloperidol-induced hypoloco-motion, demonstrating a minimal effective dose of just 0.1 or 1 mg/kg by mouth (p.o.), respectively [43,49]. By comparison, istradefylline demonstrated activity at 0.3 mg/kg p.o. in the mouse model of haloperidol-induced hypolocomotion and 1 mg/kg p.o. in the corresponding rat model [43]. Moreover, BIIB014, at doses of 3 and 10 mg/kg p.o., administered in combination with a sub-threshold dose of the dopamine agonist apomorphine, increased the number of contralateral turns in unilaterally 6-hydroxydopamine (6-OHDA)-lesioned rats compared to apomorphine alone [49]. Afterwards, the efficacy of BIIB014 on reversal of PD symptoms in dyskinetic MPTP-lesioned marmosets pretreated with L-DOPA was eval-uated. In this study, BIIB014 produced the same magnitude of anti-Parkinsonian effect as L-DOPA did against disability, with an equivalent duration of action, but less dyskinesia [49].
3.3 Clinicalefficacy:PhaseIIThe pharmacological efficacy and safety of BIIB014 as anti-Parkinsonian drug were investigated by two clinical Phase II trials. The first study was a double-blind, placebo-controlled randomized trial of single and repeated doses of BIIB014 (administered orally once a day for 8 weeks) in association with habitual L-DOPA treatment in patients with moderate-to-severe PD [50]. Efficacy of BIIB014 was evaluated by using part III (motor) of the Unified Parkinson’s Disease Rating Scale (UPDRS) and by examination of change in waking time spent in OFF state (OFF Time) and in ON state (ON Time), change in time with troublesome dyskinesia and by Clinical Global Improvement [50]. The second Phase II study was a double-blind, placebo-controlled randomized, dose-ranging trial of BIIB014 monotherapy in patients with early-stage PD [51]. The interim results of these two clinical trials reported by Biogen Idec demonstrated that BIIB014 was well tolerated and showed dose-dependent clinically relevant effects in both early- and late-stage PD patients [52].
Exp
ert O
pin.
Inv
estig
. Dru
gs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Hon
g K
ong
on 0
5/13
/13
For
pers
onal
use
onl
y.

NovelinvestigationaladenosineA2AreceptorantagonistsforParkinson’sdisease
1624 ExpertOpin.Investig.Drugs(2009) 18(11)
In particular, BIIB014 was efficacious, in a dose-dependent manner, as adjunct therapy in late-stage PD patients, decreasing the OFF Time and increasing the ON Time [52]. Furthermore, the effectiveness of this compound was demonstrated also in the monotherapy study where B11B014 dose-dependently decreased UPDRS Part III (motor) in early-stage PD patients [52].
3.4 Safetyandtolerability3.4.1 Preclinical/Phase ISafety pharmacology studies in animals have not revealed any effects that diverge from the intended CNS activity of BIIB014. This compound was not genotoxic in standard tests. Repeated dose toxicity studies in rats and monkeys have demonstrated that high systemic exposures (300-fold higher than the minimal effective dose in haloperidol model) of BIIB014 are tolerated without commonly observed AEs [43].
Safety and tolerability of BIIB014 have also been assessed by five studies in human subjects. These studies, in healthy young and elderly, used a double-blind, randomized, placebo-controlled design and showed that BIIB014 was well tolerated in healthy males and females in which it was administered in single oral doses up to 100 mg, and repeated dosing up to 50 mg/day for 10 days. Moreover, no clinically significant abnormalities were seen in vital signs, electrocardiography (ECG), safety laboratory or cognitive function tests [46,53].
3.4.2 Phase IIBiogen Idec reported that BIIB014 was well tolerated in both clinical trials in Phase II: in combination with L-DOPA, in late-stage PD patients, and as monotherapy in early-stage PD patients. Both studies have evaluated the number and proportion of subjects displaying AEs as well as clinical laboratory and ECG parameters and vital signs [50-52].
4. Preladenant
4.1 Chemical,pharmacodynamicandpharmacokineticstudiesPreladenant (also named SCH-420814) is an adenosine A2A antagonist, currently under development by Schering-Plough
Corp. for treatment of PD. It was derived from the known SCH-58261 (pyrazolo[4,3-e]-1,2,4-triazolo[1,5-c]pyrimidine), a pharmacological tool used to characterize the A2A receptor subtype [54]. The SCH-58261 is a high-affinity A2A receptor antagonist (Ki = 0.6 nM) and shows potent in vivo activity in several animal models of PD (Table 1) [55-61]. However, SCH-58261 is only moderately selective for A2A receptors over A1 receptors, possesses very poor water solubility and fails to show activity after oral administration (Table 1) [55]. In an attempt to improve the pharmacological properties of SCH-58261, the derivative SCH-412348 was developed by modifying the phenethyl side chain of SCH-58261. SCH-412348 is a potent and selective A2A antagonist (versus A1 receptors), which is also orally active in the rat haloperidol-induced catalepsy model. Further optimization of the latter molecule led to the methoxyethoxyethyl ether, preladenant which shows high A2A receptor selectivity, good pharmacokinetic properties and excellent in vivo activity against Parkinsonian symptoms (Figure 3) [54].
Preladenant exhibits high affinity for both rat and human A2A receptors, with Ki values of 2.5 and 1.1 nM, respectively (Table 1). Moreover, the compound is > 1000-fold selective for human A2A receptors over A1, A2B and A3 receptors with Ki values at human A1, A2B and A3 receptors of > 1000, > 1700 and > 1000 nM, respectively (Table 1). In cell-based assays, preladenant inhibits increases in cAMP mediated by the A2A agonist CGS-21680 with Kb values of 0.7 nM (rat) and 1.3 nM (human), confirming that preladenant acts as an antagonist at A2A receptors. In line with its selectivity, preladenant did not show significant binding against a panel of 59 unrelated receptors, enzymes and ion channels [54].
In the rat, preladenant displays pharmacokinetic properties characterized by a relatively short half-life, moderate clearance, a high steady-state volume of distribution and a brain:plasma ratio of 1. When administered to rats as the hydrochloride salt, the compound was well absorbed, with a measured oral bioavailability of 57%. In several species, a major metabolite was the O-desmethyl compound [54].
A human pharmacokinetic study in healthy males and females, divided in two age groups (18 – 45 and > 65 years),
Table1.AdenosineA2Aantagonistsandtheiraffinityforhumanadenosinereceptors.
A2Aantagonists
Pharmaceuticalcompany KiA2A(nM) KiA1(nM) KiA2B(nM) KiA3(nM) Phaseofclinicaldevelopment
Ref.
SCH-58261 Schering-Plough Corp. 0.6 287 5000 > 10,000 Research tool [55]
Istradefylline Kyowa Hakko Kogyo Co. Ltd 9.12 > 287 N.D > 681 Phase III [93]
BIIB014 Vernalis plc Biogen Idec 1.3 68 63 1005 Phase II [43]
Preladenat Schering-Plough Corp. 1.1 > 1000 >1700 > 1000 Phase II [55]
ST-1535 Sigma-Tau 6.6 71.8 352.3 > 1000 Phase I [72]
The table shows the affinity of different A2A antagonists towards the subtypes of human adenosine receptors, and the phase of clinical development for each
compound. SCH-58261 is reported as a comparison with newly synthesized derivatives.
Exp
ert O
pin.
Inv
estig
. Dru
gs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Hon
g K
ong
on 0
5/13
/13
For
pers
onal
use
onl
y.

Pinna
ExpertOpin.Investig.Drugs(2009) 18(11) 1625
showed that after preladenant administration (25 mg p.o.), the exposure was 38% higher in females than in males; however, no significant differences in exposure were observed on the basis of age [62]. Preladenant was rapidly absorbed and plasma concentration (AUC and Cmax) showed high inter-subject variability. However, although elderly females showed the highest preladenant exposure, they reported only two AEs, suggesting that increased exposure following a single dose did not affect safety profile of preladenant [62]. Moreover, a PET study was undertaken to correlate plasma concentration of preladenant (after 10, 50 and 200 mg p.o.) and receptor occupancy, using the radiotracer [11C]SCH-442416 in healthy humans [63]. This Phase I study showed that A2A receptor occupancy by preladenant increased rapidly, reached the 50% at preladenant plasma concentration of only 6 ng/ml and achieved a maximum at a relatively low plasma concentration of 50 ng/ml. A2A receptor occupancy duration was augmented with increasing doses of prelad-enant. On this basis, low dose of preladenant (5 mg), given twice a day (b.i.d.), 8 h apart, is estimated to provide ≥ 50% A2A receptor occupancy for 12 h/day in about 75% of the population [63].
4.2 PreclinicalstudiesinexperimentalmodelsofPDPreladenant was investigated in several rodent (catalepsy, 6-OHDA etc.) and primate (catalepsy, MPTP etc.) models of PD. In line with studies with the pharmacological tool SCH-58261, preladenant improved motor function in Parkinsonian rodent and non-human primate, but with the notable advantage, with respect to SCH-58261, of being orally active [21,56-61]. Specifically, oral administration of preladenant, dose-dependently attenuated CGS-21680-induced hypolocomotion and produced a reversal of haloperidol-induced catalepsy in rats and mice, with significant effects at doses of 0.1 – 1 mg/kg [64]. Ex vivo binding studies demonstrated that ∼ 70% receptor occupancy is required within the CPu for preladenant to produce marked anti-cataleptic activity [64]. Acute preladenant potentiated L-DOPA-induced contralateral turning in 6-OHDA-lesioned rats at doses of 0.1 – 3 mg/kg. Moreover, in chronic studies, preladenant co-administered daily with a threshold dose of L-DOPA, in contrast to a full dose of L-DOPA alone, did not induce behavioral sensitization, which suggests a low dyskinetic potential of this drug treatment [64]. In contrast to L-DOPA, preladenant (1 and 3 mg/kg, p.o.) produced a dose-dependent improvement in motor function without eliciting dyskinesia in the MPTP cynomolgus monkey. A more pronounced effect was observed in animals with mild-to-moderate disease. In animals bearing severe disease, potentia-tion of L-DOPA by preladenant showed an improvement in motor function with a significant increase in the ON Time [65]. Interestingly, preladenant also exhibited an antidepressant-like profile in models of behavioral despair, such as mouse tail suspension test and rodent forced swim test [64].
4.3 Clinicalefficacy:PhaseIIThe efficacy of preladenant was initially investigated in two Phase IIa studies which used a short-term administration of this compound (b.i.d., dosing over 1 – 3 days), concomitantly to L-DOPA, in PD patients. Motor function was measured using the UPDRS Part III. Results of these Phase IIa studies demonstrated that in PD patients, short-term treatment with preladenant plus L-DOPA produced an improvement in motor function [65].
The more extensive dose-finding study on preladenant was a randomized, placebo-controlled, double-blind, multi-center, international Phase II clinical trial (P04501) that evaluated the efficacy and safety of four different doses (1, 2, 5 or 10 mg b.i.d.) of preladenant compared to placebo in the treatment of patients with moderate-to-severe PD displaying motor fluctuations and dyskinesia [66,67]. All patients were on a stable regimen of standard treatments with L-DOPA and other adjunctive treatments, such as dopamine agonists and/or entacapone, but they were still experiencing motor fluctua-tions and dyskinesia. The ongoing treatment was continued throughout the trial, in which the medication investigated was given as an adjunctive therapy. A total of 253 patients were randomized into five groups (1 mg group n = 49; 2 mg group n = 49; 5 mg group n = 57; 10 mg group n = 49; placebo group n = 49), and the treatment lasted 12 weeks. Results showed that preladenant, at doses of 5 and 10 mg b.i.d. was significantly more effective in reducing the OFF Time than placebo (-1.6 (p = 0.049) and -1.7 h/day (p = 0.019), respectively, versus -0.5 h/day). In addition, preladenant, at the same doses of 5 and 10 mg b.i.d. significantly increased the ON Time with respect to placebo (+1.4 (p = 0.024) and +1.3 h/day (p = 0.049), respectively, versus +0.2 h/day) [67]. Another important result of this clinical study was the lack of association between the enhancement of the ON Time produced by preladenant and a proportional overall increase in any dyskinesia (troublesome and non-troublesome) compared to placebo [68].
A further Phase II, 36 week open-label extension (P05175) to P04501 trial is underway to assess the long-term safety of preladenant, at the dose of 5 mg b.i.d., in combination with L-DOPA or dopamine agonists, (completion is expected by September 2009), in moderate-to-severe PD patients who should have participated in the main study (P04501) [69].
A new Phase II clinical trial (P05550) is being organized to investigate the effects of single doses of preladenant or placebo on the anti-Parkinsonian activity and dyskinetic effects of L-DOPA infusion in PD patients. This study will examine the low dose of 10 mg or the high dose of 100 mg of prelad-enant, given as a single, oral administration in conjunction with intravenous L-DOPA infusion and oral carbidopa [70].
4.4 Safetyandtolerability4.4.1 Preclinical/Phase IIn the clinic, preladenant was first investigated for safety in rising single and multiple dose studies in healthy volunteers.
Exp
ert O
pin.
Inv
estig
. Dru
gs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Hon
g K
ong
on 0
5/13
/13
For
pers
onal
use
onl
y.

NovelinvestigationaladenosineA2AreceptorantagonistsforParkinson’sdisease
1626 ExpertOpin.Investig.Drugs(2009) 18(11)
In these Phase I studies, preladenant was found to be well tolerated with all AEs being nonspecific and of mild intensity and self-limiting. The profile of preladenant was quite different from that of a dopaminergic agent, as nausea, vomiting, hypotension or any CNS events were not recorded up to the maximal dose tested [65].
4.4.2 Phase IIIn the 12 week Phase II trial study (P04501), preladenant was also evaluated for its safety at all doses tested (1, 2, 5 and 10 mg) in moderate-to-severe PD patients. To this aim, the number and proportion of subjects who reported AEs, serious AEs, as well as vital signs, clinical laboratory and ECG param-eters of patients were assessed [71]. Preladenant was found to be safe and well tolerated at all four doses tested. The inci-dence of AEs was similar between preladenant- and placebo-treated groups. Discontinuation rates attributed to AEs among patients receiving therapeutic doses (5 and 10 mg) of prelad-enant (29; 14%) were comparable to those observed in patients receiving placebo (7; 14%) [71]. The most frequently reported AEs were Parkinsonism, dyskinesia and somnolence, which occurred with approximately the same frequency in prelad-enant and placebo groups. There was no clinically significant drug effect on pulse, respiration, lab and ECG parameters. Nevertheless, after the first administration of preladenant, the occurrence of a non-clinically significant, small, transient and dose-independent elevation in systolic and diastolic blood pressure devoid of corresponding increase in pulse rate was noted [71].
5. ST-1535
5.1 ChemicalstudiesThe development of ST-1535 by Sigma-Tau began with a study aimed at generating new A2A antagonists on the basis of the available structure–activity knowledge for A2A receptor ligands [72]. The ST-1535 is a 9H-purine derivative with an alkyl chain useful in modulating selectivity versus A2A subtype receptor, and a 1,2,3 triazole ring useful for improving the solubility profile and for providing one more H-bond acceptor relative to furan (Figure 4) [72]. Besides, the elevated affinity of this compound, with respect to other derivatives with an adenine-type structure, denotes that 2-substitution of the adenine ring system with relatively long (CH2)n-CH3 (N > 2) alkyl chains favors affinity toward the A2A receptor with respect to what substituted with short (N = 2) or branched alkyl chains do [72].
ST-1535 displayed a preferential affinity to human A2A adenosine receptors (Ki = 6.6 nM) with respect to human A1 adenosine receptors, in addition to showing a 12-fold selectivity for A2A receptors versus A1 receptors and no appreciable affinity for more than other 30 different receptors (Table 1) [72]. It is worth noting that this compound competitively antago-nized modification of cAMP production induced in CHA cells, by agonists of A2A and A1 adenosine receptors, and to
a lesser extent of A2B receptors; while it did not have any antagonistic effect on A3 adenosine receptors [73].
5.2 PreclinicalstudiesinexperimentalmodelsofPDST-1535 showed a good anti-Parkinsonian activity in different experimental models of PD in rodent and non-human primates. The oral administration of ST-1535 reversed CGS-21680 (administered i.c.v.) or haloperidol-induced-catalepsy in mice and potentiated L-DOPA effects in reducing haloperidol-elicited catalepsy [73]. In addition, ST-1535 increased spontaneous locomotor activity in mice [73]. Moreover, acute administration of ST-1535 dose-dependently potentiated contralateral turning behavior induced by a threshold dose of L-DOPA in 6-OHDA-lesioned rats [74,75]. Another impor-tant report showed that ST-1535 was effective, although with a lower intensity with respect to SCH-58261, in antagonizing specific motor deficits induced by dopamine neuron degenera-tion, such as latency of step initiation and sensory-motor integration deficits, even without L-DOPA combined administration, suggesting that this drug would be effective as a monotherapy in the PD treatment [61]. Additionally, acute administration of ST-1535 proved capable of reducing tremulous jaw movements in the tacrine model of PD tremor [75]. Subchronic behavioral data supported by biochemical studies in unilateral 6-OHDA-lesioned rats demonstrated that ST-1535, in association with a low dose of L-DOPA, displayed anti-Parkinsonian activity similar to that produced by a full dose of L-DOPA without exacerbating its abnormal motor side effects [75].
Consistent with rodents studies, ST-1535 administered alone to MPTP-treated marmosets produced a dose-related increase in locomotor activity and tended to reverse motor disability. Furthermore, when co-administered with L-DOPA, this com-pound enhanced the intensity and duration of L-DOPA-induced reversal of motor deficits in MPTP-treated marmosets [76]. More recently, the potential neuroprotective profile of ST-1535 was explored by evaluating whether this compound prevented quinolinic acid-induced glutamate outflow in the rat CPu, a reliable index of neuroprotective activity in vivo. ST-1535, at both behaviorally active and inactive doses, significantly prevented quinolinic acid-induced glutamate outflow in the CPu [77].
Finally, unlike the A2A antagonist istradefylline (3 mg/kg), ST-1535 (20 mg/kg) also reduced the passive avoidance induced by the A1 agonist CPA, suggesting that ST-1535 might be effective also on cognitive aspects of PD [78]. Therefore, ST-1535, being able to block the functionality of both A2A and A1 receptors, ameliorates the cognitive function in an animal model. The antagonism of A1 receptors by ST-1535, besides, might improve the dopamine release that progressively is reduced in PD patients.
5.3 Clinicaltrials:safetyandtolerability(PhaseI)In order to ascertain the safety, tolerability and to collect human pharmacokinetic data of single oral ascending doses
Exp
ert O
pin.
Inv
estig
. Dru
gs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Hon
g K
ong
on 0
5/13
/13
For
pers
onal
use
onl
y.

Pinna
ExpertOpin.Investig.Drugs(2009) 18(11) 1627
(50, 100, 200, 300 and 450 mg) of ST-1535, a first randomized, double-blind, study in healthy humans was performed. Forty healthy males, subdivided in six cohorts, were included in the study. All subjects were in good physical and mental health at study entry as determined by the medical history and physical examination, baseline vital signs, ECGs and laboratory findings. In five cohorts, six subjects were treated with one single oral administration of ST-1535 at five ascending doses of 50, 100, 200, 300 and 450 mg. The other 10 subjects received placebo under the same conditions. ST-1535 administered as a single dose up to 450 mg was generally well tolerated. There were no hematological, biochemical or urinary laboratory abnormalities of clinical concern [79].
On the base of the results of this Phase I trial study, it was planned to test ST-1535 at multiple doses of 50, 100, 150 and 200 mg, which resulted to be more tolerable than the higher doses of 300 and 450 mg. This study is ongoing [79]. The primary goal of the study is to provide evidence about the safety profile of ST-1535 in the repeated dose administra-tion in male healthy volunteers; the secondary objective is to establish the PK profile of ST-1535 in healthy male subjects following a repeated dose treatment orally administered, for 2 weeks [79].
6. Conclusions
Drug treatment of PD is accompanied by a progressive loss of drug efficacy, the onset of motor complications, negligible effects on non-motor symptoms and a failure to delay disease progression. Therefore, novel approaches to therapy are required, and the unique expression of adenosine A2A receptors in BG circuit, specifically on striatopallidal neurons, confer them a high potential as non-dopaminergic therapeutic targets for PD [16,17,20,23]. Three new A2A antagonists are undergoing clinical evaluation for PD treatment: BIIB014, preladenant and ST-1535. All three compounds display an encouraging pharmacological and safety profile, in line with their very good anti-Parkinsonian activity shown in rodent and non-human primate models of PD. Additionally, in Phase II clinical trials, both BIIB014 and preladenant, given as adjunctive therapy, showed dose-dependent clinically relevant effects in patients with moderate-to-severe PD. Specifically, both A2A antagonists reduced the OFF Time in PD patients with respect to placebo group, being also safe and well tolerated. Moreover, BIIB014 resulted also as effective monotherapy in early-stage PD patients. Phase II extension trials with both preladenant and BIIB014 are in progress, and Schering-Plough Corp. is preparing Phase III clinical development program of preladenant in PD [52,80]. Concerning ST-1535, although its efficacy in PD patients is still to be evaluated, preclinical reports suggest that this A2A antagonist could be a potential strategy in PD therapy in early as well as in late stage of the disease [61,73-77]. Moreover, specific experiments in animals suggest that ST-1535 could be useful also against cognitive deficits of
PD, and, additionally, its neuroprotective potential might delay the dopaminergic neurodegeneration underlying the disease [77,78].
7. Expertopinion
In the field of non-dopaminergic approaches to PD therapy, the development of A2A antagonists is intensively being pur-sued, even though the clinical progress of the A2A antagonist istradefylline has received a slow down by the FDA rejection in 2008 [16,17,20,23,39]. Therefore, there is a realistic hope that new A2A antagonists such as BIIB014, preladenant, ST-1535 or even istradefylline, after a further and thorough investiga-tion, would reach the market in the short to mid term. To optimize the clinical efficacy of A2A antagonists, it might be considered to narrow both clinical trials and future therapy to PD patients with mild-to-moderate degree of illness. In fact, A2A antagonists could be less effective in PD patients with severe degree of the disease, who most likely display a more marked dopaminergic degeneration. Indeed, it may be hypothesized that residual endogenous dopamine might be essential in achieving the complete expression of the anti-Parkinsonian properties of A2A receptor antagonists, thus, clarifying why istradefylline displays a moderate efficacy when administered in combination with L-DOPA, as declared by the FDA. Moreover, further clinical evaluation of A2A antagonists is also needed in combination with sub-optimal doses of L-DOPA, instead of optimal doses used of L-DOPA, as suggested by preclinical studies.
Furthermore, istradefylline monotherapy failed to reverse Parkinsonian disabilities in humans, in conflict with data observed in PD animal models, in which several A2A antago-nists counteract motor deficits when administered without L-DOPA [61,81-85]. This discrepancy may be explained by the low doses of istradefylline used so far in clinical trials. Hence, higher doses of istradefylline could elicit beneficial effects on Parkinsonian symptoms when administered alone, suggesting the need for a thorough dose-range investigation when performing clinical trials with A2A antagonists. In line with this hypothesis, recent clinical data reported that BIIB014 in monotherapy was effective in reducing the UPDRS Part III in early-stage PD patients [52]. To date, no clinical trials have been already performed using preladenant as monotherapy. Nevertheless, although, the clinical results achieved by this compound as adjunctive therapy in moderate-to-severe PD patients make it, so far, a very good potential candidate for PD therapy.
Moreover, several preclinical pieces of evidence concerning the effects of A2A receptor blockade on cognition-related functions, together with symptomatological and neuropathological features of cognitive deficits in PD, suggest the suitability of A2A receptor antagonists as a potential therapeutic approach for use in the treatment of Parkinsonian cognitive decline [17,20,36]. A more detailed evaluation of the mnemonic-enhancing effects exerted by A2A antagonists by means of selective
Exp
ert O
pin.
Inv
estig
. Dru
gs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Hon
g K
ong
on 0
5/13
/13
For
pers
onal
use
onl
y.

NovelinvestigationaladenosineA2AreceptorantagonistsforParkinson’sdisease
1628 ExpertOpin.Investig.Drugs(2009) 18(11)
preclinical or clinical tests assessing cognitive function should be performed to determine a more thorough therapeutic profile for these agents on PD-related cognitive deficits. A further potentially positive effect produced by A2A antagonists might be on PD-associated depressive symptoms, another major non-motor feature of the pathology [86]. No clinical study has yet addressed this issue, but such an effect could be hypothesized based on investigations showing the effec-tiveness of several A2A antagonists, including preladenant, in animal models of depression [64,87]. Finally, another important feature of A2A antagonists is neuroprotection. Indeed, a number of preclinical reports from rodent models of Parkinsonian neurodegeneration and data obtained in epidemiological studies suggest how blockade of A2A receptors might be capable of counteracting progression of the dopaminergic neuronal degeneration occurring in PD [17,20,23,28,35]. This finding envisions A2A antagonists as agents, substantially capable of preventing onset and/or worsening of both Parkinsonian motor and non-motor symptoms. Moreover, regarding inflammation, it is important to consider the role of the A2A receptors in the periphery. In fact, the A2A recep-tors are widely distributed in blood cells such as neutrophils, lymphocytes and platelets where they regulate inflammatory reactions and mediate platelet aggregation [28,88,89]. It is worth noting that in several peripheral organs such as liver
and lung, sub-threshold doses of an inflammatory stimulus that generated minimal tissue damage in wild-type mice were sufficient to create extensive tissue damage, more pro-longed and higher levels of pro-inflammatory cytokines and death of animals in A2A receptor knockout mice [90-92]. Based on these findings, A2A receptors have been proposed as endog-enous breakers that inhibit inflammation and limit tissue damage [90-92]. Hence, long-term therapy of the A2A antago-nists in patients with PD could exacerbate inflammatory damages in the periphery organs; further toxicological and pharmacological studies on A2A antagonists in brain as well as peripheral organs are required to clarify these potential effects on peripheral organs in the development of the A2A antagonists for PD treatment [28,89].
To conclude, data reported in the present review depict A2A antagonists as extremely promising drugs for use in the treatment of PD. Their potential is largely represented by the clear efficacy demonstrated in palliating PD motor symptoms, together with their potential ability in preventing onset and progression of the disease and ameliorating cognitive decline.
Declarationofinterest
The author states no conflict of interest and has received no payment in preparation of this manuscript.
Bibliography1. Obeso JA, Rodriguez-Oroz MC,
Rodriguez M, et al. Pathophysiology of the basal ganglia in Parkinson’s disease. Trends Neurosci 2000;23:S8-19
2. Chaudhuri KR, Healy DG, Schapira AH; National Institute for Clinical Excellence. Non-motor symptoms of Parkinson’s disease: diagnosis and management. Lancet Neurol 2006;5(3):235-45
3. Alves G, Forsaa EB, Pedersen KF, et al. Epidemiology of Parkinson’s disease. J Neurol 2008;255(Suppl 5):18-32
4. Jenner P, Olanow CW. The pathogenesis of cell death in Parkinson’s disease. Neurology 2006;66:S24-36
5. Twelves D, Perkins KS, Counsell C. Systematic review of incidence studies of Parkinson’s disease. Mov Disord 2003;18(1):19-31
6. von Campenhausen S, Bornschein B, Wick R, et al. Prevalence and incidence of Parkinson’s disease in Europe. Eur Neuropsychopharmacol 2005;15(4):473-90
7. Van Den Eeden SK, Tanner CM, Bernstein AL, et al. Incidence of Parkinson’s disease: variation by age,
gender, and race/ethnicity. Am J Epidemiol 2003;157(11):1015-22
8. Weintraub D, Comella CL, Horn S. Parkinson’s disease–Part 1: pathophysiology, symptoms, burden, diagnosis, and assessment. Am J Manag Care 2008;14:S40-8
9. Dorsey ER, Constantinescu R, Thompson JP, et al. Projected number of people with Parkinson disease in the most populous nations, 2005 through 2030. Neurology 2007;68:384-86
10. Dowding CH, Shenton CL, Salek SS. A review of the health-related quality of life and economic impact of Parkinson’s disease. Drugs Aging 2006;23(9):693-721
11. Olanow CW, Agid Y, Mizuno Y, et al. Levodopa in the treatment of Parkinson’s disease: current controversies. Mov Disord 2004;19(9):997-1005
12. Horstink M, Tolosa E, Bonuccelli U, et al. Review of the therapeutic management of Parkinson’s disease. Report of a joint task force of the European Federation of Neurological Societies and the Movement Disorder Society-European Section. Part I:
early (uncomplicated) Parkinson’s disease. Eur J Neurol 2006;13(11):1170-85
• Goodreviewoftherapeuticmanagement ofearly-stagePDpatients.
13. Horstink M, Tolosa E, Bonuccelli U, et al. Review of the therapeutic management of Parkinson’s disease. Report of a joint task force of the European Federation of Neurological Societies (EFNS) and the Movement Disorder Society-European Section (MDS-ES). Part II: late (complicated) Parkinson’s disease. Eur J Neurol 2006;13(11):1186-202
• Goodreviewoftherapeuticmanagement oflate-stagePDpatients.
14. Guttman M, Kish SJ, Furukawa Y. Current concepts in the diagnosis and management of Parkinson’s disease. CMAJ 2003;168(3):293-301
15. Goetz CG, Poewe W, Rascol O, Sampaio C. Evidence-based medical review update: pharmacological and surgical treatments of Parkinson’s disease: 2001 to 2004. Mov Disord 2005;20(5):523-39
16. Morelli M, Di Paolo T, Wardas J, et al. Role of adenosine A2A receptors in parkinsonian motor impairment and l-DOPA-induced motor complications. Prog Neurobiol 2007;83(5):293-309
Exp
ert O
pin.
Inv
estig
. Dru
gs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Hon
g K
ong
on 0
5/13
/13
For
pers
onal
use
onl
y.

Pinna
ExpertOpin.Investig.Drugs(2009) 18(11) 1629
17. Xu K, Bastia E, Schwarzschild M. Therapeutic potential of adenosine A(2A) receptor antagonists in Parkinson’s disease. Pharmacol Ther 2005;105:267-310
•• VerygoodreviewofA2Aantagonists, theirmechanismsonmotorbehaviorandtheirpotentialtherapeuticefficacyinParkinson’sdisease
18. Schiffmann SN, Vanderhaeghen JJ. Adenosine A2 receptors regulate the gene expression of striatopallidal and striatonigral neurons. J Neurosci 1993;13:1080-7
19. Svenningsson P, Le Moine C, Aubert I, et al. Cellular distribution of adenosine A2A receptor mRNA in the primate striatum. J Comp Neurol 1998;399:229-40
20. Simola N, Morelli M, Pinna A. Adenosine A2A receptor antagonists and Parkinson’s disease: state of the art and future directions. Curr Pharm Des 2008;14(15):1475-89
21. Pinna A, Di Chiara G, Wardas J, Morelli M. Blockade of A2A adenosine receptors positively modulates turning behaviour and c-fos expression induced by D1 agonists in dopamine-denervated rats. Eur J Neurosci 1996;8:1176-81
22. Pollack AE, Fink JS. Synergistic interaction between an adenosine antagonist and a D1 dopamine agonist on rotational behaviour and striatal c-Fos induction in 6-hydroxydopamine-lesioned rats. Brain Res 1996;743:124-30
23. Jenner P, Mori A, Hauser R, et al. Adenosine, adenosine A(2A) antagonists, and Parkinson’s disease. Parkinsonism Relat Disord 2009, May 13. PubMed PMID: 19446490. [Epub ahead of print]
•• VerygoodreviewofA2Aantagonists,theirinfluenceonbasalgangliaandtheirpotentialefficacyasnon-dopaminergictherapyinParkinson’sdisease.
24. Fuxe K, Marcellino D, Genedani S, Agnati L. Adenosine A(2A) receptors, dopamine D(2) receptors and their interactions in Parkinson’s disease. Mov Disord 2007;22(14):1990-2017
•• VerygoodreviewconcerningheteromericreceptorcomplexesandtheirroleinParkinson’sdisease.
25. Ross GW, Abbott RD, Petrovitch H, et al. Association of coffee and caffeine intake with the risk of Parkinson disease. JAMA 2000;283:2674-9
26. Ascherio A, Zhang SM, Hernán MA, et al. Prospective study of caffeine consumption and risk of Parkinson’s disease in men and women. Ann Neurol 2001;50:56-63
27. Chen JF, Xu K, Petzer JP, et al. Neuroprotection by caffeine and A(2A) adenosine receptor inactivation in a model of Parkinson’s disease. J Neurosci 2001;21:RC143
28. Kalda A, Yu L, Oztas E, Chen JF. Novel neuroprotection by caffeine and adenosine A(2A) receptor antagonists in animal models of Parkinson’s disease. J Neurol Sci 2006;248(1-2):9-15
29. Barcia C, Sánchez Bahillo A, Fernández-Villalba E, et al. Evidence of active microglia in substantia nigra pars compacta of parkinsonian monkeys 1 year after MPTP exposure. Glia 2004;46:402-9
30. Hunot S, Hirsch EC. Neuroinflammatory processes in Parkinson’s disease. Ann Neurol 2003;53:S49-58
31. McGeer PL, Itagaki S, Boyes BE, McGeer EG. Reactive microglia are positive for HLA-DR in the substantia nigra of Parkinson’s and Alzheimer’s disease brains. Neurology 1988;38:1285-91
32. Wu DC, Jackson-Lewis V, Vila M, et al. Blockade of microglial activation is neuroprotective in the 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine mouse model of Parkinson disease. J Neurosci 2002;22:1763-71
33. Ikeda K, Kurokawa M, Aoyama S, Kuwana Y. Neuroprotection by adenosine A2A receptor blockade in experimental models of Parkinson’s disease. J Neurochem 2002;80:262-70
34. Pierri M, Vaudano E, Sager T, Englund U. KW-6002 protects from MPTP induced dopaminergic toxicity in the mouse. Neuropharmacology 2005;48:517-24
35. Chen JF, Sonsalla PK, Pedata F, et al. Adenosine A2A receptors and brain injury: broad spectrum of neuroprotection, multifaceted actions and “fine tuning” modulation. Prog Neurobiol 2007;83(5):310-31
•• VerygoodreviewaboutA2Areceptors andtheirneuroprotectiverole.
36. Takahashi RN, Pamplona FA, Prediger RD. Adenosine receptor antagonists for cognitive dysfunction: a review of animal studies. Front Biosci 2008;13:2614-32
• Goodreviewoftheinfluenceofadenosineantagonistsincognitivedysfunction.
37. Kase H, Aoyama S, Ichimura M, et al. Progress in pursuit of therapeutic A2A antagonists: the adenosine A2A receptor selective antagonist KW6002: research and development toward a novel nondopaminergic therapy for Parkinson’s disease. Neurology 2003;61(11Suppl 6):S97-100
38. Jenner P. Istradefylline, a novel adenosine A2A receptor antagonist, for the treatment of Parkinson’s disease. Expert Opin Investig Drugs 2005;14:729-38
• Goodreviewofistradefyllineasanti-Parkinsoniandrugandpieceofevidenceinclinicaltrials.
39. FDA Issues Not Approvable Letter for Istradefylline. Available from: http://www.drugs.com/nda/kw_6002_080228.html [Last accessed 16 June 2009]
40. Hockemeyer J, Burbiel JC, Mueller CE. Multigram-scale syntheses, stability, and photoreactions of A2A adenosine receptor antagonists with 8-styrylxanthine structure: potential drugs for Parkinson’s disease. J Org Chem 2004;69(10):3308-18
41. Johnston TH, Brotchie JM. Drug in development for Parkinson’s disease: an update. Curr Opin Investig Drugs 2006;7(1):25-32
42. Weiss SM, Benwell K, Cliffe IA, et al. Discovery of nonxanthine adenosine A2A receptor antagonists for the treatment of Parkinson’s disease. Neurology 2003;61(11 Suppl 6):S101-6
43. Gillespie RJ, Bamford SJ, Botting R, et al. Antagonists of the Human A2A Adenosine Receptor. 4. Design, Synthesis, and Preclinical Evaluation of 7-Aryltriazolo[4,5-d]pyrimidines. J Med Chem 2009;52(1):33-47
• Manuscriptregardingthechemical andpharmacologicalcharacterization ofBIIB014.
44. Product Pipeline of Vernalis. Parkinson’s Disease: V2006. Available from: http://www.vernalis.com/ver/rdc2/neurology/v2006/ [Last accessed 16 June 2009]
45. Padfield A, Denny S, Merrett A, et al. Pre-clinical drug metabolism and pharmacokinetic studies with BIIB014/V2006. Presented at International research conference “Targeting adenosine A2A receptors in PD and other CNS Disorders”, Boston, USA (17-19 May 2006). Available
Exp
ert O
pin.
Inv
estig
. Dru
gs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Hon
g K
ong
on 0
5/13
/13
For
pers
onal
use
onl
y.

NovelinvestigationaladenosineA2AreceptorantagonistsforParkinson’sdisease
1630 ExpertOpin.Investig.Drugs(2009) 18(11)
from: http://handle.dtic.mil/100.2/ADA452764 [Last accessed 16 June 2009]
46. Wade A, Bakhtyari A, Thomas R, et al. BIIB014/V2006: Pharmacokinetics in young and elderly healthy subjects. Presented at International research conference “Targeting adenosine A2A receptors in PD and other CNS Disorders”, Boston, USA (17-19 May 2006). Available from: http://handle.dtic.mil/100.2/ADA452764 [Last accessed 16 June 2009]
47. An Open-Label, Positron Emission Tomography Study to Assess Adenosine A2A Brain Receptor Occupancy of BIIB014 at Multiple Dose Levels in Healthy Male Volunteers. ClinicalTrials.gov. NCT00531193. Available from: http://clinicaltrials.gov/ct2/show/NCT00531193 [Last accessed 16 June 2009]
48. Moresco RM, Todde S, Belloli S, et al. In vivo imaging of adenosine A2A receptors in rat and primate brain using [11C]SCH442416. Eur J Nucl Med Mol Imaging 2005;32(4):405-13
49. Lightowler S, Knight AR, Upton R, et al. Pharmacology of BIIB014/V2006, an A2A antagonist for the treatment of PD. Presented at International research conference “Targeting adenosine A2A receptors in PD and other CNS Disorders”, Boston, USA (17-19 May 2006). Available from: http://handle.dtic.mil/100.2/ADA452764 [Last accessed 16 June 2009]
50. A Randomized, Double-Blind, Placebo-Controlled, Dose Escalation Study of Single and Multiple Oral Dose Administration of BIIB014 in Subjects With Moderate to Late Stage Parkinson’s Disease Who Are Also Receiving Treatment With Levodopa ClinicalTrials.gov. NCT00438607. Available from: http://clinicaltrials.gov/ct2/show/NCT00438607 [Last accessed 16 June 2009]
51. A Randomized, Double-Blind, Placebo-Controlled, Dose Escalation Study of Multiple Doses of BIIB014 Administered Orally in Subjects With Early Parkinson’s Disease. ClinicalTrials.gov. NCT00442780. Available from: http://clinicaltrials.gov/ct2/show/NCT00442780 [Last accessed 16 June 2009]
52. Biogen Idec reports favourable data from Phase IIa Parkinson’s Disease studies of BIIB014 (licensed from Vernalis). Available
from: http://www.vernalis.com/ver/nc/latestreleases/releases2009/2009-03-27/ [Last accessed 16 June 2009]; Access the Biogen IDEC results of presentation from: http://library.corporate-ir.net/library/14/148/148682/items/329869/503E91BE-5BE4-47F0-A030-17858A19C307_6_BIIB014v2.pdf [Last accessed 16 June 2009]
53. Lightowler S. Progressing the A2A antagonist BIIB014/V2006 to the clinic for the treatment of PD. Presented at International research conference “Targeting adenosine A2A receptors in PD and other CNS Disorders”, Boston, USA (17-19 May 2006). Available from: http://handle.dtic.mil/100.2/ADA452764 [Last accessed 16 June 2009]
54. Neustadt BR, Hao J, Lindo N, et al. Potent, selective, and orally active adenosine A2A receptor antagonists: Arylpiperazine derivatives of pyrazolo[4,3-e]-1,2,4-triazolo[1,5-c]pyrimidines. Bioorg Med Chem Lett 2007;17:1376-80
• Manuscriptregardingthechemicalcharacterizationofpreladenant.
55. Ongini E, Dionisotti S, Gessi S, et al. Comparison of CGS 15943, ZM 241385 and SCH 58261 as antagonists at human adenosine receptors. Naunyn Schmiedebergs Arch Pharmacol 1999;359(1):7-10
56. Fenu S, Pinna A, Ongini E, Morelli M. Adenosine A2A receptor antagonism potentiates L-DOPA induced turning behavior and c-fos expression in 6-hydroxydopamine-lesioned rats. Eur J Pharmacol 1997;321:143-47
57. Svenningsson P, Nomikos GG, Ongini E, Fredholm BB. Antagonism of adenosine A2A receptors underlies the behavioural activating effect of caffeine and is associated with reduced expression of messenger RNA for NGFI-A and NGFI-B in caudate-putamen and nucleus accumbens. Neuroscience 1997;79(3):753-64
58. Wardas J, Konieczny J, Lorenc-Koci E. SCH 58261, an A(2A) adenosine receptor antagonist, counteracts parkinsonian-like muscle rigidity in rats. Synapse 2001;41(2):160-71
59. Carta AR, Pinna A, Tronci E, Morelli M. Adenosine A2A and dopamine receptor interactions in basal ganglia of dopamine denervated rats. Neurology 2003;61:S39-43
60. Simola N, Fenu S, Baraldi PG, et al. Blockade of adenosine A2A receptors antagonizes parkinsonian tremor in the rat tacrine model by an action on specific striatal regions. Exp Neurol 2004;189:182-8
61. Pinna A, Pontis S, Borsini F, Morelli M. Adenosine A2A receptor antagonists improve deficits in initiation of movement and sensory motor integration in the unilateral 6-hydroxydopamine rat model of Parkinson’s disease. Synapse 2007;61:606-14
62. Cutler DL, Tendolkar A, Hunter J. Effects of age and gender on preladenant pharmacokinetics in healthy subjects. Presented at Movement Disorder Society’s 13th International Congress of Parkinson’s Disease and Movements Disorders, Paris, France (7-11 June 2009). Abstract Mo-194
63. Brooks DJ, Warrington S, Tendolkar A, et al. Positron emission tomography (PET) study of preladenant in healthy male subjects. Presented at Movement Disorder Society’s 13th International Congress of Parkinson’s Disease and Movements Disorders, Paris, France (7-11 June 2009). Abstract Mo-187
64. Hodgson RA, Bertorelli R, Varty GB, et al. Characterization of the Potent and Highly Selective A2A Receptor Antagonists Preladenant and SCH 412348 in Rodent Models of Movement Disorders and Depression. J Pharmacol Exp Ther 2009 Mar 30. PubMed PMID: 19332567. [Epub ahead of print]
65. Hunter J. SCH 420814: a novel Adenosine A2a antagonist. Exploring Parkinson’s Disease and beyond. Presented at International research conference “Targeting adenosine A2A receptors in PD and other CNS Disorders”, Boston, USA (17-19 May 2006). Available from: http://handle.dtic.mil/100.2/ADA452764
66. Phase 2, 12-Week, Double-Blind, Dose-Finding, Placebo-Controlled Study to Assess the Efficacy and Safety of a Range of SCH 420814 Doses in Subjects With Moderate to Severe Parkinson’s Disease Experiencing Motor Fluctuations and Dyskinesias. ClinicalTrials.gov. NCT00406029. Available from: http://clinicaltrials.gov/ct2/show/NCT00406029 [Last accessed 18 June 2009]
67. Hauser RA, Pourcher E, Micheli F, et al. Efficacy of preladenant, a novel A2A antagonist, as an adjunct to levodopa for the treatment of Parkinson’s disease.
Exp
ert O
pin.
Inv
estig
. Dru
gs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Hon
g K
ong
on 0
5/13
/13
For
pers
onal
use
onl
y.

Pinna
ExpertOpin.Investig.Drugs(2009) 18(11) 1631
Presented at Movement Disorder Society’s 13th International Congress of Parkinson’s Disease and Movements Disorders, Paris, France (7-11 June 2009). Abstract Tu-185
68. Huyck SB, Wolski K, Cantillon M. Impact of A2A receptor antagonist preladenant on dyskinesia in moderate to severe Parkinson’s disease: Post-hoc analysis of dose-finding study. Presented at Movement Disorder Society’s 13th International Congress of Parkinson’s Disease and Movements Disorders, Paris, France (7-11 June 2009). Abstract Tu-187
69. A Phase 2, 36-Week, Open-Label, Uncontrolled Safety Follow-up Study Assessing SCH 420814 5 mg BID (Protocol No. P05175). ClinicalTrials.gov. NCT00406029. Available from: http://clinicaltrials.gov/ct2/show/NCT00537017 [Last accessed 18 June 2009]
70. Acute Effects of SCH 420814 on Dyskinesia and Parkinsonism in Levodopa Treated Patients. ClinicalTrials.gov. NCT00845000. Available from: http://clinicaltrials.gov/ct2/show/NCT00845000 [Last accessed 18 June 2009]
71. Pourcher E, Micheli F, Mok V, et al. Safety and tolerability profile of preladenant as an adjunct to L-dopa in patients with Parkinson’s disease. Presented at Movement Disorder Society’s 13th International Congress of Parkinson’s Disease and Movements Disorders, Paris, France (7-11 June 2009). Abstract We-187
72. Minetti P, Tinti MA, Carminati P, et al. 2-n-Butyl-9-8-[1,2,3] triazol-2-yl-9H-purin-6-ylamine and analogues as A2A adenosine receptor antagonists. Design, synthesis, and pharmacological characterization. J Med Chem 2005;48:6887-96
• ManuscriptregardingthechemicalcharacterizationofST-1535.
73. Stasi MA, Borsini F, Varani K, et al. ST1535: A preferential A2a adenosine receptor antagonist. Int J Neuropsychopharm 2006;9(5):575-84
74. Rose S, Ramsay Croft N, Jenner P. The novel adenosine A2a antagonist ST1535 potentiates the effects of a threshold dose of l-dopa in unilaterally 6-OHDA-lesioned rats. Brain Res 2007;1133:110-14
75. Tronci E, Simola N, Borsini F, et al. Characterization of the antiparkinsonian effects of the new adenosine A2A receptor antagonist ST1535: acute and subchronic studies in rats. Eur J Pharmacol 2007;566:94-102
76. Rose S, Jackson MJ, Smith LA, et al. The novel adenosine A2a antagonist ST1535 potentiates the effects of a threshold dose of L-dopa in MPTP treated common marmosets. Eur J Pharmacol 2006;546(1-3):82-7
77. Galluzzo M, Pintor A, Pèzzola A, et al. Behavioural and neurochemical characterization of the adenosine A2A receptor antagonist ST1535. Eur J Pharmacol 2008;579(1-3):149-52
78. Di Serio S, Danese V, Guaraldi D, et al. The novel adenosine A2A receptor antagonist 2-butyl-9-methyl-8-(2H-1,2, 3-triazol-2-yl)-9H-purin-6-ylamine (ST1535) ameliorates memory disruption mediated by adenosine A1 receptor stimulation. Presented at 13th European Behavioural Pharmacology Society Biennial Meeting, Rome, Italy (4-7 September 2009)
79. Sigma-Tau communication about development of ST-1535. Available from: http://www.sigma-tau.it/eng/fasidisviluppo.asp [Last accessed 18 June 2009] with specific piece of information provide by Sigma-Tau Company
80. Schering Plough Corp. communication about preladenant clinical development program in PD. Available from: http://www.medicalnewstoday.com/articles/130623.php [Last accessed 18 June 2009]
81. Kanda T, Tashiro T, Kuwana Y, Jenner P. Adenosine A2A receptors modify motor function in MPTP-treated common marmosets. Neuroreport 1998;9:2857-60
82. Kanda T, Jackson MJ, Smith LA, et al. Combined use of the adenosine A(2A) antagonist KW-6002 with L-DOPA or with selective D1 or D2 dopamine agonists increases antiparkinsonian activity but not dyskinesia in MPTP-treated monkeys. Exp Neurol 2000;162:321-27
83. Grondin R, Bedard PJ, Hadj Tahar A, et al. Antiparkinsonian effect of a new selective adenosine A2A receptor antagonist in MPTP-treated monkeys. Neurology 1999;52:1673-7
84. Shiozaki S, Ichikawa S, Nakamura J, et al. Actions of adenosine A2A receptor antagonist KW-6002 on drug-induced catalepsy and hypokinesia caused by reserpine or MPTP. Psychopharmacology 1999;147:90-5
85. Bara-Jimenez W, Sherzai A, Dimitrova T, et al. Adenosine A(2A) receptor antagonist
treatment of Parkinson’s disease. Neurology 2003;61:293-6
86. Levin BE, Katzen HL. Early cognitive changes and nondementing behavioral abnormalities in Parkinson’s disease. Adv Neurol 2005;96:84-94
87. El Yacoubi M, Ledent C, Parmentier M, et al. Adenosine A2A receptor antagonists are potential antidepressants: evidence based on pharmacology and A2A receptor knockout mice. Br J Pharmacol 2001;134:68-77
88. Gessi S, Varani K, Merighi S, et al. A(2A) adenosine receptors in human peripheral blood cells. Br J Pharmacol 2000;129:2-11
89. Haskó G, Pacher P. A2A receptors in inflammation and injury: lessons learned from transgenic animals. J Leukoc Biol 2008;83(3):447-55
•• VerygoodreviewaboutA2Areceptors andinflammation.
90. Ohta A, Sitkovsky M. Role of G-protein-coupled adenosine receptors in down regulation of inflammation and protection from tissue damage. Nature 2001;414:916-20
91. Ohta A, Lukashev D, Jackson EK, et al. 1,3,7-trimethylxanthine (caffeine) may exacerbate acute inflammatory liver injury by weakening the physiological immunosuppressive mechanism. J Immunol 2007;179(11):7431-8
92. Thiel M, Chouker A, Ohta A, et al. Oxygenation inhibits the physiological tissue-protecting mechanism and thereby exacerbates acute inflammatory lung injury. PLoS Biol 2005;3(6):e174
93. Mihara T, Mihara K, Yarimizu J, et al. Pharmacological characterization of a novel, potent adenosine A1 and A2A receptor dual antagonist, 5-[5-amino-3-(4-fluorophenyl)pyrazin- 2-yl]-1-isopropylpyridine-2(1H)-one(ASP5854), in models of Parkinson’s disease and cognition. J Pharmacol Exp Ther 2007;323(2):708-19
AffiliationAnnalisa PinnaNational Research Council CNR, Institute of Neuroscience – Cagliari. c/o Department of Toxicology, University of Cagliari, Via Ospedale 72, 09124 Cagliari, Italy Tel: +39 070 6758662; Fax: +39 070 6758665; E-mail: [email protected]
Exp
ert O
pin.
Inv
estig
. Dru
gs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Hon
g K
ong
on 0
5/13
/13
For
pers
onal
use
onl
y.

Exp
ert O
pin.
Inv
estig
. Dru
gs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Hon
g K
ong
on 0
5/13
/13
For
pers
onal
use
onl
y.