Embed Size (px)
Citation preview

NOVEL INDICATIONS:
Experiences from a Study in MDD with Mixed Features (Mixed Depression)
Josephine Cucchiaro, PhD
Vice President Clinical Operations & Project Management
Sunovion Pharmaceuticals
11 APRIL 2013

Disclosures
I am a full time employee of Sunovion Pharmaceuticals

Overview 1. MDD with mixed features (mixed depression)
2. Lurasidone development programs have provided insight into potential new indications – PEARL schizophrenia
– PREVAIL bipolar depression
3. RESOLVE Study in mixed depression
– Definition and characterization of the diagnosis
– Baseline characteristics of enrolled patients

WHAT IS MIXED DEPRESSION?

The majority of bipolar depressive episodes have symptoms of mania
Goldberg et al AJP 2009
Number of DSM-IV Manic Symptoms During an Index Episode of Bipolar Depression in STEP-BD (N=1,380)

6
Epidemiology of Mixed Depression • Large-scale studies have confirmed high rates of concomitant sub-
syndromal hypomania among MDD population (~40-50%) (P. Zimmerman et al., Arch.Gen Psych. 2009; T. Suppes et al. Arch. Gen Psych 2005; J. Angst et al. AJP 2010; J. Goldberg et al., Am J Psych 2009, Benazzi et al., 2007, 2008; M. Frye et al., Am J Psych 2009; Benazzi and Akiskal, 2006)
• Prevalence of mixed depression (7-9%) approaches that observed for MDD alone (10%) (J. Angst et al. AJP 2010; P. Zimmerman et al., Arch.Gen Psych. 2009)
• Compared with MDD patients, mixed depression patients display higher rates of comorbidity with:
– Substance abuse disorders (P. Zimmerman et al., Arch.Gen Psych. 2009; Dodd et al., J Aff Dis 2010)
– Behavioral problems and criminal acts (P. Zimmerman et al., Arch.Gen Psych. 2009; Angst et al., 2010)
– Panic disorder (Zimmerman et al., 2009)
– Suicidality (Balazs et al., 2006; Angst et al., 2010; Goldberg et al., 1998; Judd and Akiskal, 2003)
– Overrepresented in women (Suppes et al., 2005, Akiskal and Benazzi, 2003)
• Associated with poorer long-term clinical outcomes compared with pure MDD (Dodd et al., 2010, Angst et al., 2010)

7
DSM-5: Major Depressive Episode With Mixed Features
• Full criteria for a major depressive episode and at least 3 of the following symptoms are present nearly every day during the episode:
– Elevated, expansive mood
– Inflated self-esteem or grandiosity
– Flight of ideas or subjective experience that thoughts are racing
– More talkative than usual or pressure to keep talking
– Increase in energy or goal-directed activity (either socially, at work or school, or sexually)
– Increased or excessive involvement in activities that have a high potential for painful consequences (eg, engaging in unrestrained buying sprees, sexual indiscretions, or foolish business investments)
– Decreased need for sleep (feeling rested despite sleeping less than usual [to be contrasted from insomnia])
• Symptoms of mood elevation excluded from core defining symptoms:
– Irritability, psychomotor agitation, distractibility, insomnia

Translational evidence from late phase studies – Can this be achieved?
Considerations:
• Pharmacological profile
• Clinical data in schizophrenia and bipolar depression

Schizophrenia Program: Depressive Symptom Change - Pooled Dataa
Anxiety Depression
PANSS Items Anxiety/Depression MADRS
Placebo 80mg
Baseline: Anxiety – Placebo 3.67, Lurasidone 3.83, Depression – Placebo 2.90, Lurasidone 3.04
Baseline: Placebo 14.5, Lurasidone 14.2
* *
*
N=83 N=86 N=135 N=135 N=181 N=181
LOCF at end point *p<0.05 using ANCOVA aStudies 006, 196 – ECNP 2005
LOCF at end point *p<0.05 using ANCOVA aStudy 196 – ECNP 2005
-1.0
-0.5
0.0
Mea
n C
hang
e fr
om B
asel
ine
-4
-3
-2
-1
0
Mea
n C
hang
e fr
om B
asel
ine
Nakamura et al, (2009) J Clin Psych; Ogasa et al (2013) Psychopharmacology

PREVAIL Studies in Bipolar Depression MADRS: Primary Endpoint
*
*
**
*** ***
**
**
***
*** ***
-18
-14
-10
-6
-2
Baseline 1 2 3 4 5 6
Week
Effect size (MMRM): Lurasidone 20-60 mg: 0.51 Lurasidone 80-120 mg: 0.51
-10.7
-15.4 -15.4
*P≤0.05; **P≤0.01; ***P≤0.001. Loebel A, et al., Am J Psych, in press 2013..
Placebo (n=162)
Lurasidone 20-60 mg (n=161)
Lurasidone 80-120 mg (n=162)
Baseline mean 30.5 30.3 30.6
LS M
ean
Cha
nge
from
Bas
elin
e
Placebo + Li/VPA (n=161)
Lurasidone + Li/VPA (n=179)
-13.5
-17.1 LS
Mea
n C
hang
e fr
om B
asel
ine
Baseline mean 30.8 30.6
Effect size (MMRM): Lurasidone + Li/VPA: 0.34
PREVAIL Monotherapy PREVAIL Adjunctive Therapy

Post hoc analysis: MADRS Change for Subjects With and Without Subthreshold Hypomania
11
Group 1: patients above or below the median Baseline YMRS score of 4
PREVAIL Monotherapy

12
RESOLVE Study: Operational Criteria for Mixed Depression Diagnosis
• Full criteria for a Major Depressive Episode (at least 2 weeks in duration)
AND • 2-3 manic symptoms occurring nearly every day
(present for at least the past 2 weeks) • Manic symptoms to be consistent with DSM 5
list (non-specific symptoms of irritability, distractibility and psychomotor agitation are excluded)
Convincing management to fund a novel program
• Opinion of academic experts and the relevant literature on high unmet medical need for this population
• Stressed rationale for use of lurasidone as a potential treatment
• Advocated for the position that this study, while being high risk, would contribute to a better understanding of this population
• Study could provide insights for future product development programs

14
RESOLVE Study Design
6 weeks
Extension Study
Placebo
Lurasidone 20-80 mg/d
Screening
Bas
elin
e
3-14 days
Day 0
Double Blind
6 months
Open Label

15
• 18 to 75 years of age
• Diagnosed with an MDE (diagnosed by DSM-IV-TR, and confirmed by the modified SCID-CT)
• MADRS total score of ≥ 26 at both screening and baseline visits
• 2-3 manic symptoms to be consistent with DSM 5 list (non-specific symptoms of irritability, distractibility and psychomotor agitation are excluded)
Key Entry Criteria
DO INVESTIGATORS UNDERSTAND THE POPULATION UNDER STUDY?

Ensuring accurate diagnosis
• Thorough discussion of the diagnosis at Investigator’s Meetings
• Measures to validate and confirm the diagnosis included in trial procedures
• Modified SCID-CT (to include assessment of mixed features)

Objections to the Diagnosis
• The proposed diagnosis does not exist or is very rare
• Patients with this clinical presentation are bipolar spectrum patients
• Recruitment will be very difficult

I understand the criteria for diagnosis of a major depressive episode with mixed features (subthreshold hypomanic symptoms)
57%35%5%3% 1) I have no understanding of this diagnosis
2) I have limited understanding of this diagnosis
3) I have a moderate to good understanding of this diagnosis
4) I fully understand this diagnosis

How often do you see patients with an episode of major depressive disorder with mixed features (subthreshold hypomanic symptoms) in clinical practice?
1%39%48%11% 1) I rarely observe this condition (~2-3 cases/year)
2) I sometimes observe this condition (~1 case/month)
3) I often observe this condition (~1 case/week)
4) I never observe this condition
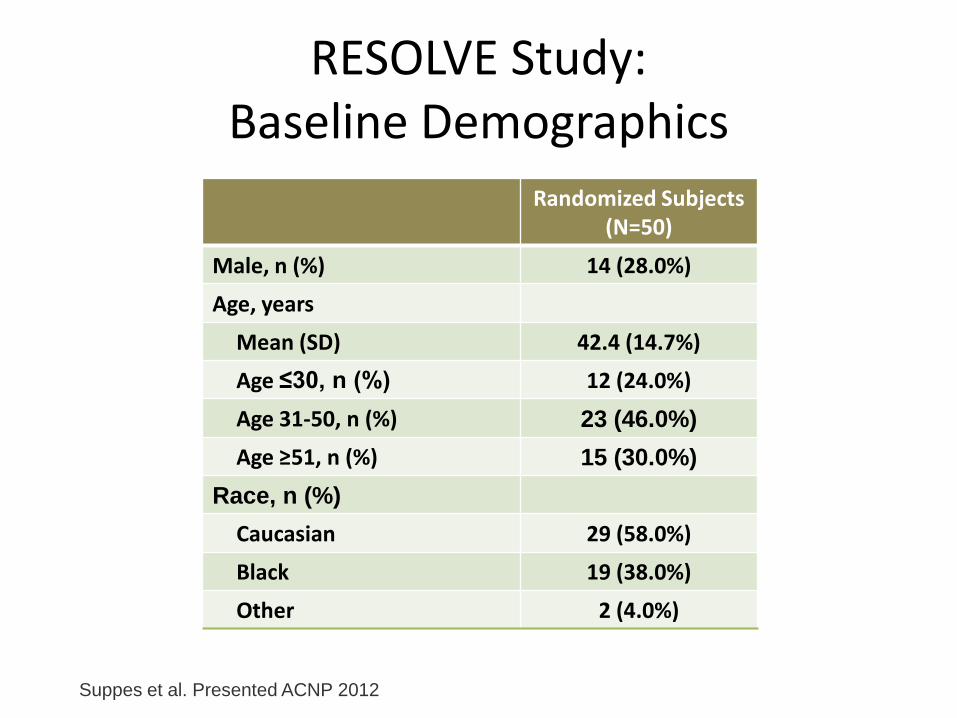
RESOLVE Study: Baseline Demographics
Randomized Subjects (N=50)
Male, n (%) 14 (28.0%) Age, years
Mean (SD) 42.4 (14.7%) Age ≤30, n (%) 12 (24.0%) Age 31-50, n (%) 23 (46.0%) Age ≥51, n (%) 15 (30.0%)
Race, n (%) Caucasian 29 (58.0%) Black 19 (38.0%) Other 2 (4.0%)
Suppes et al. Presented ACNP 2012

RESOLVE Study: Baseline Clinical Characteristics
Mean (SD)
Number of Lifetime Major Depressive Episodes
Total Number 6.1 (6.4)
Number with Mixed Features 4.6 (5.9)
Duration of Current Episode, months
Major Depressive Features 4.6 (3.2)
Concurrent Mixed Features 3.7 (3.3)
MADRS Score 33.2 (4.8)
CGI-S Score 4.6 (0.7)
YMRS Score 12.7 (5.0)
HAM-A Total Score 16.6 (6.9)
Sheehan Disability Scale Total Score 19.1 (6.3)
Suppes et al. Presented ACNP 2012

RESOLVE Study: Baseline Manic Symptoms
Proportion Reporting Manic Symptoms, % (N=50)
Total Manic Symptoms = 3
Total Manic Symptoms = 2
Decreased Need for Sleep
Increased or Excessive Involvement in Risky Activities
Increased Energy or Goal-Directed Activity
Flight of Ideas or Racing Thoughts
More Talkative or Pressure to Keep Talking
Inflated Self-esteem, Grandiosity
Elevated, Expansive Mood
Suppes et al. Presented ACNP 2012

RESOLVE Study: Excluded Manic Symptoms
Frequency of manic symptoms occurring on most days in the past 2 weeks that are not included in the study or DSM-5 criteria for mixed depression
Proportion Reporting, %
Suppes et al. Presented ACNP 2012

25
RESOLVE Study: Psychiatric Family History
Perc
enta
ge
N=18
Maternal
6%0%
6%11%
72%
11%
0%0%
20%
40%
60%
80%
100%
Schizophrenia BipolarDisorder
Depression Anxiety Alcoholism SubstanceAbuse
Other

26
RESOLVE Study: Psychiatric Family History
N=19
Paternal
0%
11%
37%
0%
37%
5%11%
0%
20%
40%
60%
80%
100%
Schizophrenia BipolarDisorder
Depression Anxiety Alcoholism SubstanceAbuse
Other
Perc
enta
ge

Conclusions
• Innovative drug development within established drug classes can be pursued
• Requires thorough understanding of the pharmacologic and clinical profile of the molecule
• Education and discussion with investigators and other key stakeholders is needed





























