Embed Size (px)
Citation preview

Novel Humanitarian Aid Program: The GlivecInternational Patient Assistance Program—Lessons Learned From Providing Access toBreakthrough Targeted Oncology Treatmentin Low- and Middle-Income Countries
Pat Garcia-Gonzalez,
Paula Boultbee
and David Epstein
Pat Garcia-Gonzale , TheMax Foundation; PaulaBoultbee, PTBConsulting LLC, Seattle,WA; and David Epstein,NovartisPharmaceuticals, EastHanover, NJ.Corresponding author:Pat Garcia-Gonzalez,MS, The MaxFoundation, 200 NEPacific St, Suite 103,Seattle, WA 98105;e-mail: [email protected].
Imatinib was the first targeted therapy approved for the treatment of cancer. With its approval, it was immediately clear toNovartis that this breakthrough therapy would require an innovative approach to worldwide access, with special considerationof low- and middle-income countries. Lack of government reimbursement, universal health care, or health insurancecoverage, few trained specialty physicians or diagnostic services, and poor health care infrastructure were, and continue tobe, contributing barriers to access to treatment in low- and middle-income countries. The Glivec International PatientAssistance Program (GIPAP) is an international drug donation program established by Novartis Pharma AG and implementedin partnership with The Max Foundation, a nonprofit, nongovernmental organization. GIPAP was established in 2001,essentially in parallel with the first approval of imatinib for chronic myeloid leukemia. Since 2001, GIPAP has made imatinibaccessible to all medically and financially eligible patients within 80 countries on an ongoing basis as long as theirphysicians prescribe it and no other means of access exists. To date, more than 49,000 patients have benefited from GIPAP,and 2.3 million monthly doses of imatinib have been approved through the program. GIPAP represents an innovative drugdonation model that has set the standard for access programs for other targeted or innovative therapies. The purpose of thisarticle is to describe the structure of GIPAP, as well as important lessons that have contributed to the success of the program.This article may assist other companies with the development of successful and far-reaching patient assistance programs inthe future.
INTRODUCTION
Chronic myeloid leukemia (CML) is a hematologicmalignancy that annually affects between one and1.6 of 100,000 people worldwide.1 One of therarest forms of leukemia in terms of annual inci-dence, CML is expected to become the mostprevalent hematologic malignancy in the world by2020.2-4 Once an acutely life-threatening conditionwith a median survival of often fewer than 5years,2,3 CML has been considered a chronicillness since the advent of targeted therapies.5-9
Imatinib (Glivec, Gleevec; Novartis Pharmaceuti-cals, East Hanover, NJ) was the first targetedtherapy to be developed and approved for thetreatment of a cancer. Imatinib was approved forthe treatment of accelerated- and blast-phase Phil-adelphia chromosome (Ph) –positive CML in May2001 in United States and for the first-line treat-ment of Ph-positive CML in January 2002 in boththe United States and Europe. It was subsequentlyapproved for the treatment of GI stromal tumor(GIST) in 2002.5
Despite advances in the treatment of cancer andother diseases like HIV, hepatitis C virus, andmalaria, patient access to lifesaving medications inlow- and middle-income countries (LMICs) is often
challenging for both financial and logistic rea-sons.10,11 Lack of reimbursement or health insur-ance coverage, inadequate infrastructure, pooraccess to trained specialty physicians or diagnosticservices, and insufficient patient health educationare all contributing factors to poorer patient out-comes in LMICs.12 It is estimated that in manyLMICs, more than 80% of pharmaceuticals mustbe purchased by patients directly (private payersystems).13,14 The international community hasresponded to this unmet need by establishinghumanitarian donation programs of varying sizeand scope. There are many examples of suchdonation programs that have historically fallen preyto organized theft and corruption, leading to theillegal selling of often substandard medicines onthe black market; in other instances, these medi-cines have been mishandled and rendered inef-fective and have ultimately never made it to theintended patient population.15 These challengesfaced by the international community have led tothe development of manufacturer-led internationaldonation programs as well as WHO guidelines fordrug donations to ensure broad and equitabledistribution of lifesaving therapies to patients inneed worldwide.16
specialarticle
executivesum
mary
jgo.ascopubs.org JGO – Journal of Global Oncology Volume 1, Issue 1, October 2015 37
© 2015 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License AA
z

The Glivec International Patient Assistance Pro-gram (GIPAP) is an international donation programestablished by Novartis Pharma AG in partnershipwith The Max Foundation, a nonprofit, nongovern-mental organization (NGO) that serves as the pro-gram administrator.16 The remit of the program isto facilitate access to and distribution of imatinib topatients in LMICs, who meet specific programcriteria. Following the WHO guidelines for drug
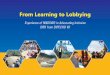
donations,17 Novartis provides imatinib at no costto eligible patients with CML or GIST, the approvedindications for the drug, in participating countries.Eighty LMICs in Africa, Asia, Eastern Europe, LatinAmerica, and the Caribbean that have no compre-hensive drug reimbursement system or availablegenerics have participated in GIPAP. To date,49,477 patients from 80 countries (Patient Assis-tance Tracking System [PATS database]) have
Albania Botswana Ecuador Honduras Mali Nigeria Saint Lucia Thailand
ArgentinaBurkina
FasoEl Salvador India Mauritius Pakistan Senegal Togo
Armenia Cambodia Ethiopia Indonesia Mexico Panama Seychelles Turkey
Azerbaijan Cameroon Fiji Jamaica MoldovaPapua New
GuineaSingapore Uganda
Bahamas Chile Gabon Kazakhstan Mongolia ParaguaySolomon Islands
Uruguay
Bangladesh China Georgia Kenya Morocco Peru South Africa Uzbekistan
Belarus Colombia Ghana Kyrgyzstan Namibia Philippines Sri Lanka Venezuela
Benin Cote d’Ivoire Guatemala Madagascar NepalRepublic of
CongoSudan Vietnam
BhutanDominican Republic
Guinea Malawi Nicaragua Russia Surinam Zambia
Bolivia East Timor Haiti Malaysia Niger Rwanda Tanzania Zimbabwe
Figure 1 –Glivec InternationalPatient AssistanceProgram country mapand list.
38 Volume 1, Issue 1, October 2015 jgo.ascopubs.org JGO – Journal of Global Oncology

benefited from GIPAP since the inception of theprogram in late 2001 (Fig 1), and more than 2million 1-month supplies of treatment have beenapproved for donation.18
The development of a drug donation program for atargeted cancer therapy was uncharted territory in2001. The path to the growth of this program waspeppered with successes but riddled with majorhurdles along the way. Each hurdle led to keylearning and subsequent adjustments that helpedthe program mature and evolve into a robustexample of best practice and the most compre-hensive and far-reaching access program devel-oped for an oncology drug, one that to this day stillprofoundly affects patients and communitiesworldwide. The purpose of this article is to describethe partnership between the donor company, No-vartis, and The Max Foundation, the NGO thatadministers the program, as well as to describe thecurrent structure of GIPAP, highlighting the novelcharacteristics that were implemented by trial anderror, to enable others to draw parallels and benefitfrom this collective experience.
HISTORY AND INITIATION OF GIPAP
The GIPAP partnership between Novartis and TheMax Foundation was initiated in late 2001, at atime when imatinib had been newly approved forCML based on the results of the IRIS (InternationalRandomized Study of Interferon Versus STI571)trial.19 Immediately after the first approval of ima-tinib, it was clear to Novartis that many patientsworldwide would benefit from access to this ther-apy. Still, given the novel type of cancer therapy,one allowing patients to be treated on an outpatientbasis but requiring chronic treatment and regularmonitoring indefinitely, there were many difficultquestions to answer before embarking on a drugdonation initiative. For example:
● How many patients would be properly diag-nosed and thus eligible for a patient assis-tance program, and what infrastructurewould be required to fairly provide imatinib tothese patients consistently?
● How could a patient assistance program en-sure that requests for imatinib would comeonly from hematologists and oncologists withexperience and qualifications to safely mon-itor their patients’ treatment?
● How could this program ensure that onlyappropriate, eligible patients gained accessto imatinib? Given the robust global presscoverage of imatinib, including a Time mag-azine cover (May 28, 2001) hailing it as amagic bullet for cancer, might some eagerhealth care providers attempt to treat othercancers with the donated drug, possibly en-dangering the lives of their patients withcancer?
● How would Novartis identify a suitable part-ner to administer the imatinib drug donationprogram?
The model proposed by Novartis for this donationprogram required identifying individual diagnosedpatients and guiding them through the program.This led Novartis to the decision to seek an NGOwith a patient-focused approach. The search for apartner that could serve as the administrator of theprogram was a critical step in implementing GIPAPand beginning to address these challenges. Largeorganizations with a focus on cancer as well asorganizations that focused on hematologic malig-nancies specifically were considered. Novartissought a unique NGO with a vested interest inspecifically fighting CML, because focus on andawareness of this rare disease were minimalamong other larger foundations with broader inter-est in hematologic malignancies or cancers expe-rienced by a larger number of patients. The Max
Table 1 – GIPAP Patient and Physician Approvals
Year
GIPAP Patients by Disease Type(n � 49,484) No. of GIPAP Physicians
(n � 1,502)CML GIST Other�
2001 13 — — †
2002 740 32 — †
2003 2,146 130 — †
2004 4,705 387 — †
2005 4,335 583 — 205
2006 5,264 1,021 — 142
2007 5,863 1,426 17 171
2008 5,672 1,398 41 158
2009 2,136 454 37 46
2010 1,676 404 63 38
2011 1,827 502 67 42
2012 1,815 588 62 33
2013 1,838 616 66 53
2014 1,825 644 95 32
2015‡ 688 239 33 22
Total 40,577 8,426 481 1,502
Abbreviations: CML, chronic myeloid leukemia; GIPAP, Glivec International Patient AssistanceProgram; GIST, GI stromal tumor.�Other includes: Philadelphia chromosome–positive acute lymphoblastic leukemia, myelodysplasticand myeloproliferative diseases, systemic mastocytosis, hypereosinophilic syndrome and/or chroniceosinophilic leukemia, and dermatofibrosarcoma protuberans.†Data not available in annual increments before 2005. Total No. of physicians from 2001 to 2004 was560.‡As of May 25, 2015.
jgo.ascopubs.org JGO – Journal of Global Oncology Volume 1, Issue 1, October 2015 39

Foundation, founded in 1997 in the memory ofMaximiliano (Max) Rivarola, who tragically suc-cumbed to CML at the age of 17 years, was chosennot only for its clear and pointed focus on CML, butalso because of its grassroots efforts and strongemotional connection to patients with CML. Theorganization had a deep commitment to the bet-terment of patients and a global scope with focuson LMICs. For these reasons, The Max Foundationwas an obvious choice as partner in the GIPAPinitiative, but its small size and relatively newstanding in the NGO landscape presented chal-lenges. The Max Foundation was faced with theherculean effort of administering an internationaldonation program for a novel, targeted cancertherapy. This included identifying and verifying theidentity and eligibility of patients across manyregions of the world and liaising with health careproviders for each specific patient, including thosein regions where Internet access and communica-tions were extremely limited. The logistics oflaunching a donation program of this scope couldbe daunting. For example, because donated med-icines maintain high market values, which mayresult in high import taxes, tax exemptions must beconsidered and obtained in each country.
Despite these major hurdles, the GIPAP partner-ship was formally established in 2001, just monthsafter US Food and Drug Administration approval ofimatinib for CML.20,21 Just as imatinib was the firsttargeted therapy for CML, GIPAP was the firstpatient assistance program for a targeted therapy,making The Max Foundation and Novartis pio-neers in this field. Since its launch, GIPAP hasexpanded its reach from a total of 13 patientsapproved in 2001 to more than 49,000 patients by2015, with more than 20,000 of them still activelyreceiving donated product (Table 1). The scope ofGIPAP as a function of time includes approxi-mately 2,340,000 months of imatinib treatmentapproved for donation to date (PATS database).
GIPAP MODEL
What differentiates GIPAP from other large inter-national drug donation efforts is its direct-to-patientapproach. The Max Foundation identifies and ver-ifies the eligibility of each individual patient andrequests a product donation from Novartis at aspecific dose as prescribed by that patient’s phy-sician in 3-month intervals. In this way, the orga-nization ensures that only properly diagnosed,eligible patients gain access to imatinib. The orga-nization carefully tracks the time and consumptionneed for resupply of each patient. The Max Foun-dation plays a key role in the protection of the
privacy of patients by assigning a unique identifierto each patient to be used in all communicationswith Novartis.
In setting up GIPAP, and as the program owner,Novartis is tasked with identifying the appropriatecountries in which to implement the program andestablishing the medical and financial eligibilitycriteria. Although there were no direct-to-patientdonation programs before GIPAP, the WHO guide-lines for drug donations have provided the basicfoundation for the medical criteria of the program,which accepts only patients with a confirmeddiagnosis of an approved indication for imatinib.17
Novartis is responsible for delivering the drug to thetreating cancer institution at the requested doseand amount for each specific patient, labelingimatinib supply for GIPAP with a “for patientassistance” sticker to deter product diversion andsupport appropriate use, as well as to ease theprocess of obtaining tax waivers. In countrieswhere Novartis does not have the necessary infra-structure to support drug importation, the com-pany contracts with Axios International to aid inthese logistics. The selection of qualified institu-tions and physicians is performed in collaborationbetween Novartis and The Max Foundation.
Participation of physicians and nurses in GIPAP isvoluntary, but their commitment has greatly con-tributed to the successful treatment of their pa-tients. The physicians and nurses at GIPAP sitescomply with the demanding data entry needs ofthe program, in many cases support importationand tax exemption processes, and personally con-tact patients with appointment reminders andother important information. These interactionsfoster strong peer-to-peer support and patientgroup development. As the program has ultimatelyhelped increase the prevalence of CML in thesecommunities, the number of living patients withCML under the care of each physician has growndramatically in the program.
The company, the program administrator, and thephysician work in close communication to ensurethat each patient receives needed product on aperiodic basis without interruptions in treatment(Fig 2). This is a critical aspect of this new model,because identifying each individual patient anddelivering drug in accordance with specific needprevent drug stockpiling. A donation program suchas GIPAP requires a significant investment of re-sources from the donor company and can have animportant impact on drug production. As an exam-ple, in 2014, approximately 30% of all imatinibproduced by Novartis was for donation, with a large
40 Volume 1, Issue 1, October 2015 jgo.ascopubs.org JGO – Journal of Global Oncology

part of it supporting GIPAP (data on file, Novartis,East Hanover, NJ).
A challenge of donating tyrosine kinase inhibitorssuch as imatinib is the chronic and outpatientnature of this treatment. It has been shown thatachieving optimal clinical outcomes for patientsreceiving imatinib is strongly linked to patient ad-herence to treatment.22-25 As a patient-focusedorganization, The Max Foundation is able to offerdirect support services to patients in GIPAP acrossmany countries.16 These support services, al-though not part of the program itself, holisticallycontribute to the successful long-term participationof patients in GIPAP and are vital to the environ-ment within which the program operates. Collec-tively, for The Max Foundation, the averagenumber of one-on-one patient contacts per monthin 2013 was more 10,000 across countries.18
IMPACT OF GIPAP PARTNERSHIP ON CREATIONOF SUSTAINABLE LOCAL RESOURCES
To further provide support services to patients withCML and GIST, over the past 14 years, The MaxFoundation has diligently worked to identify localpatient leaders in the GIPAP countries and to-gether with them has embarked on the establish-ment of patient organizations. In partnership withthese patient organizations, The Max Foundationprovides peer-to-peer support, facilitating diseaseeducation and supporting adherence to prescribedtherapies. The Max Foundation has been directlyengaged in the establishment of 35 local patientsupport organizations and currently supports atotal of 68 organizations in 58 countries throughthe Max Global Network.16
Novartis, along with other companies with interestin CML and GIST, continues to support educationalinitiatives and awareness campaigns initiated byThe Max Foundation and its partner organizations.One such global campaign entitled “What is myPCR?” helps both physicians and patients betterunderstand a diagnosis and how best to optimally
manage their disease.26 These independent ele-ments collectively contribute to the success ofGIPAP (Fig 3).
CASE STUDY IN INDIA
India has the largest number of GIPAP recipients(12,668 patients helped), representing 25% of allprogram recipients, and has been an active GIPAPcountry since 2002. To support physicians andhelp patients navigate the program verification andapproval process in India, The Max Foundationexpanded its team to include a local cancer careprovider in 2002 and formally established the firstIndia MaxStation. MaxStations, as designated byThe Max Foundation, are local advocates withexperience in cancer support that facilitate com-munications and data transfer among all programstakeholders. MaxStations are a core componentof the internal structure of The Max Foundation.Outside of their role as GIPAP program adminis-trators, all MaxStations dedicate 20% of their timeto providing support services to patients. In May2002, when the first MaxStation was incorporatedin India, there were 22 active patients in GIPAP inthe country. One year later, with 620 patientsactive in GIPAP in India, The Max Foundationlaunched a new patient support initiative, Friendsof Max, in partnership with local patient leaders.Friends of Max was launched in five cities in May2003 as the patient support arm of The MaxFoundation in India. Through Friends of Max, TheMax Foundation provides disease education, anti-stigma campaigns, adherence programs, andother support initiatives to patients with CML andGIST in India.
In the past 14 years, The Max Foundation hasestablished MaxStations in 13 countries to supportGIPAP. Furthermore, the organization has en-gaged with patient organizations, treating physi-cians, and patient leaders in other GIPAP countriesto support the delivery of support services aroundpatients.
LESSONS LEARNED FROM GIPAP
● It is possible to safely and consistently delivertargeted therapies to patients in any region ofthe world.
Through GIPAP, it has been demonstrated thatwith the right partnerships and true commitment ofall parties, it is possible to safely provide access totargeted cancer treatment for patients in any cor-ner of the world. Moreover, in countries with limitedresources to treat a specific cancer, starting with acommitment to access to therapies can be a
Reapproval Cycle
Physician confirmsdiagnosis andprescribes imatinib
Patient is assessedand approved inGIPAP
Novartis generatessupply and distributesto local institution
The Max Foundation notifiesNovartis of ongoing supplyneeds for individual patients
The Max Foundationtracks patient progresswith the physician
PRESCRIBES APPROVES
ONGOING
SUPPLY
PROGRESS
Figure 2 –Glivec InternationalPatient AssistanceProgram (GIPAP) drugdonation flow.
jgo.ascopubs.org JGO – Journal of Global Oncology Volume 1, Issue 1, October 2015 41

catalyst to improving the health care infrastructurenecessary to treat the disease, as well as to devel-oping sustainable local resources such as patientsupport organizations. For example, access to mo-lecular monitoring, a core component of effectiveCML therapy, was essentially nonexistent in mostGIPAP countries in 2001. Access to imatinibthrough GIPAP led The Max Foundation, Novartis,and others with interest in CML to develop initia-tives to improve access to reliable diagnostics inLMICs. In 2011, the first molecular test to measureBCR-ABL in Sub-Saharan Africa was performed inBlack Lion Hospital, Addis Ababa, Ethiopia. Acces-sibility of diagnostics had a profound impact on thesuccess of the program, with an increase of 30% inthe annual accrual of patients in Ethiopia (Fig 4).Today, similar resources are available for diagnos-ing and monitoring CML in many GIPAP countries.
● Forecasting drug supply and complying withpharmacovigilance regulations are key chal-lenges of the model.
Assessing the drug supply needs of each countryand providing adequate supply in a timely fashionto all patients have been major challenges through-out the implementation of GIPAP. Time for produc-tion and importation must be taken into account, aprocess that ranges from 6 to 8 weeks dependingon the location. The likelihood of changes in lawsand personnel regulating importation of donatedproducts in LMICs poses threats to the capacity ofthe program partners to prevent treatment inter-ruptions. Although certain circumstances are un-avoidable, a lesson learned from the GIPAPexperience is the need to engage and educatelocal stakeholders regarding the initiative to ensure
an efficient drug importation process and day-to-day running of the program. This process hasevolved since the inception of GIPAP. When GI-PAP was initially established, there was an urgencyto provide potentially lifesaving therapy to seriouslyill patients without options as soon as possible.Thus, the program was initiated as what could beperceived as a vertical donation program, andthere was little time available to engage with keylocal stakeholders broadly. With the maturity of theprogram, a concerted effort has been made toattend to the role of important local stakeholderswho can help facilitate the smooth and consistentimplementation of the program long term.
Furthermore, pharmacovigilance, although a mostnecessary practice to protect the safety of patients,is one of the most challenging aspects of theGIPAP model. Pharmacovigilance is a requirementof all health authorities to ensure the safety ofpatients receiving treatment, and companies arethus required to report all adverse events thatoccur in their patient-oriented programs, includingany drug donation program. As a proxy of thecompany, The Max Foundation team must reportall adverse events of which they become awareoccurring in GIPAP. GIPAP captures a high vol-ume of adverse events thanks to the large numberof participants, their length of time receiving treat-ment, and regular interaction by The Max Founda-tion with people in the program. The MaxFoundation had to provide a solution to managethis significant and important administrative bur-den. To do so, The Max Foundation expanded itsstaff and quickly developed the necessary struc-tures for tracking all adverse event reports. PATS,developed by The Max Foundation to support andcoordinate all organizational activities in GIPAP,today includes an adverse event reporting tool thatensures high-quality and timely reporting. Whilecomplying with the mandates of safety reporting,The Max Foundation continues to protect patientconfidentiality by submitting the reports using thepersonal unique identifiers assigned to each pa-tient. The Max Foundation is required to report theevents to the Novartis safety team, which mustwork with each treating physician to complete theinformation required and subsequently submit it tothe health authorities as per regulatory require-ments. Perhaps the heaviest burden of this pro-cess lies with the health care providers. BecauseGIPAP operates in the real world, and physiciansare often overburdened, the addition of this re-quirement is yet another stress on their time andresources.
GIPAP
Individual Patient Support(The Max Foundation)
Formation and supportof patient organizations
(The Max Foundation)
Figure 3 –The Max Foundationpatient assistance andsupport model. GIPAP,Glivec InternationalPatient AssistanceProgram.
42 Volume 1, Issue 1, October 2015 jgo.ascopubs.org JGO – Journal of Global Oncology

PATS is a smart Web engine that also serves topropel the life cycle of patients in the program, afeature without which the program would not suc-ceed. With case-by-case management capacity,PATS alerts The Max Foundation team of the timeto start the resupply process for each patient.Moreover, the system allows health care providersto input needed information regarding each patientin real time to generate resupply requests to No-vartis. PATS thus facilitates real-time logistics alongwith facilitating pharmacovigilance.
● Drug donation and patient assistance pro-grams must be tailored to unique and chang-ing country-specific needs.
One of the challenges of establishing a long-termdrug access program is being able to evolve overtime as the natural environment changes. Somecountries, where a program like GIPAP madesense in 2001, presented different characteristicsa decade later. In 2009, Novartis unveiled theNovartis Oncology Access (NOA) program as anexpansion of GIPAP. NOA has been implementedin countries where factors such as a growingmiddle class, development of universal health caresystems, or otherwise improved affordability ofmedicines have created the opportunity to engagelocal stakeholders in sharing the responsibility ofproviding access to imatinib. Under NOA, Novartisshares the cost of imatinib either with governmenthealth care systems, charities, and other payers ordirectly with patients without health care coveragewho are unable to pay for the full cost of theirmedication but can pay it in part under a copaymodel. In some countries such as India, a third-party financial institution conducts the financialassessment of patients, while working closely withThe Max Foundation to ensure continued supportfrom the broad physician network, patient engage-ment services, and uninterrupted delivery of med-icines. Since its launch in 2009, NOA India has
further expanded access to imatinib by providingtreatment to 17,000 additional patients (PATSdatabase).
● GIPAP improves our understanding of dis-ease in LMICs.
Important information about the diagnosis andtreatment duration of patients with rare diseases inLMICs may be gleaned through programs likeGIPAP. In a recent analysis of GIPAP data, the ageat diagnosis was shown to be significantly loweramong patients treated with imatinib in LMICs; acorrelation was also demonstrated between thetime from diagnosis to treatment with overall sur-vival rates in those countries.27 Since time fromdiagnosis to tyrosine kinase inhibitor treatment is avariable that can be improved through educationand access to proper diagnostics, this analysishelped identify an area that could be indepen-dently targeted to improve patient outcomes. An-other recent analysis of GIPAP data demonstratedthat the outcomes of pediatric patients with CMLtreated with imatinib in LMICs, an area poorlyunderstood previously, are similar to those of pe-diatric patients in the United States, as long asaccess to therapy is provided promptly and con-sistently.28 Similar findings were demonstratedwith adult patients in GIPAP.29 Factors that con-tribute to successful GIPAP enrollment and patientoutcomes within participating GIPAP sites havealso been analyzed. It was found that GIPAP siteswith at least one hematologist/oncologist and withdiagnostic and research capabilities were associ-ated with higher patient enrollment numbers andbetter patient outcomes versus sites without one ofthese factors.30 These findings have assisted withthe selection of new centers and institutions withwhich to partner as GIPAP has expanded world-wide. These analyses, made possible through anal-ysis of GIPAP data, address a critical deficit in thestudy of CML by providing data on treatmentpatterns and outcomes in LMICs that were largelyunknown.
DISCUSSION
In the past 14 years, GIPAP has provided approx-imately 2.3 million monthly doses of imatinib tomore than 49,000 patients in LMICs, representinga large humanitarian effort of unprecedentedscope and impact. One of the most significantfindings throughout the evolution of GIPAP is thatproviding access to targeted cancer therapies canbe a catalyst for the subsequent development ofresources and improvement of health care sys-tems, as opposed to the more common strategy ofsome sponsors in supporting capacity building
GIPAP Ethiopia Patient Accrual Over Time
0 0 110
28
6167
7468
100 97
81
108
48
No.
of P
atie
nts
Enro
lled
Year
120
100
80
60
40
20
0
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
*
Figure 4 –Glivec InternationalPatient AssistanceProgram (GIPAP)Ethiopia patient accrualover time. (*) As ofJune 1, 2015.
jgo.ascopubs.org JGO – Journal of Global Oncology Volume 1, Issue 1, October 2015 43

efforts but excluding access to drugs. In addition,cooperation with key local stakeholders and align-ment with local authorities at early stages shouldbe sought. The model itself—partnering with anNGO such as The Max Foundation for tracking thetreatment and drug consumption of each individ-ual patient and offering wraparound patient sup-port services—greatly contributes to overcomingshortfalls from bulk international humanitarian do-nations, minimizing drug diversion, and improvingtreatment compliance. Companies developing life-saving medicines to treat noncommunicable dis-eases such as cancer should strongly considerimplementing global access strategies with apatient-centered approach such as the one usedfor GIPAP. There will always be a role in the area ofglobal oncology for international donations ofdrugs, and this program provides an exampleof how access to innovative cancer treatment inLMICs is both possible and beneficial to the globalcommunity as well as individual patients.
There are many known barriers to access to inno-vative cancer therapies in LMICs, affordability be-ing commonly cited as one. In the GIPAP example,the program removes the variable of affordability;no quotas on the number of patients have everbeen imposed by Novartis, and all applications
submitted by approved physicians in GIPAP opencountries have been and will continue to be eval-uated on their own merit. Still, lack of access todiagnostics, favorable socioeconomic conditions,and viable health care infrastructure may preventpatients from accessing otherwise available treat-ments. As such, the program has shed light on theneed for a broader approach to finding solutions tothe complex causes of lack of access to treatment.Collectively, our findings from GIPAP are impor-tant, because the GIPAP population comes fromcountries where it is estimated that 70% of all newcancer diagnoses will be made31; the findingshighlight that robust partnerships between NGOsand pharmaceutical companies for programs sim-ilar to GIPAP could serve as a tool to improvepatient access, research, and outcomes. GIPAP isan example of how to effectively provide patientassistance in countries where little or no healthinsurance or prescription drug coverage exists.This model demonstrates that such initiativescan work in concert with existing local healthcare structures to treat life-threatening condi-tions worldwide.
DOI: 10.1200/JGO.2015.000570published online ahead of print at jgo.acsopubs.org onSeptember 23, 2015
AUTHOR CONTRIBUTIONSManuscript writing: All authorsFinal approval of manuscript: All authors
AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTSOF INTERESTThe following represents disclosure information providedby authors of this manuscript. All relationships areconsidered compensated. Relationships are self-heldunless noted. I � Immediate Family Member, Inst � MyInstitution. Relationships may not relate to the subjectmatter of this manuscript. For more information aboutASCO’s conflict of interest policy, please refer to www.asco.org/rwc or jco.ascopubs.org/site/ifc.
Pat Garcia-GonzalezConsulting or Advisory Role: GlaxoSmithKline (Inst)Travel, Accommodations, Expenses: GlaxoSmithKline,Asuragen
Paula BoultbeeEmployment: Pharmacyclics, Pharmacyclics (I)Leadership: Pharmacyclics, Pharmacyclics (I)
Stock or Other Ownership: Pharmacyclics, Pharmacyclics(I)Consulting or Advisory Role: Pharmacyclics, VersartisTravel, Accommodations, Expenses: Pharmacyclics, Phar-macyclics (I)David EpsteinEmployment: Novartis AGLeadership: Novartis AGStock or Other Ownership: Novartis AG
ACKNOWLEDGMENTWe thank all the patients and their families for theircommitment to the Glivec International Patient AssistanceProgram (GIPAP) as well as to their own treatment. We alsothank physicians for their participation in GIPAP andcountless individuals involved at Novartis, Axios, and otherpartners, as well as The Max Foundation teams, whodedicate great effort to ensuring that patients directly benefitfrom this program. We acknowledge Michael Wrigglesworth,who created the Patient Assistance Tracking System (PATS)and provided the data reported from the PATS database forthis article. We acknowledge Michael Mandola, PhD, foreditorial assistance with this article.
REFERENCES
1 Arias E: United States life tables, 2006. Natl Vital Stat Rep 58:1-40, 2010
2 Interferon alfa-2a as compared with conventional chemotherapy for the treatment of chronic myeloid leukemia:The Italian Cooperative Study Group on Chronic Myeloid Leukemia. N Engl J Med 330:820-825, 1994
3 Hehlmann R, Heimpel H, Hasford J, et al: Randomized comparison of interferon-alpha with busulfan andhydroxyurea in chronic myelogenous leukemia: The German CML Study Group. Blood 84:4064-4077, 1994
44 Volume 1, Issue 1, October 2015 jgo.ascopubs.org JGO – Journal of Global Oncology

4 Huang X, Cortes J, Kantarjian H: Estimations of the increasing prevalence and plateau prevalence of chronicmyeloid leukemia in the era of tyrosine kinase inhibitor therapy. Cancer 118:3123-3127, 2012
5 Glivec (imatinib) summary of product characteristics. Basel, Switzerland, Novartis Pharma AG, 2014
6 TASIGNA (nilotinib) summary of product characteristics. Basel, Switzerland, Novartis Pharma AG, 2014
7 Sprycel (dasatinib) summary of product characteristics. Uxbridge, United Kingdom, Bristol-Myers Squibb Pharma, 2014
8 BOSULIF (bosutinib) product monograph. Kirkland, Quebec, Canada, Pfizer Canada, 2014
9 Iclusig (ponatinib) summary of product characteristics. Weybridge, United Kingdom, Ariad Pharma, 2014
10 Ford N, Singh K, Cooke GS, et al: Expanding access to treatment for hepatitis C in resource-limited settings:Lessons from HIV/AIDS. Clin Infect Dis 54:1465-1472, 2012
11 Tougher S, Ye Y, Amuasi JH, et al: Effect of the Affordable Medicines Facility–malaria (AMFm) on theavailability, price, and market share of quality-assured artemisinin-based combination therapies in sevencountries: A before-and-after analysis of outlet survey data. Lancet 380:1916-1926, 2012
12 CanTreat International. Scaling up cancer diagnosis and treatment in developing countries: What can we learnfrom the HIV/AIDS epidemic? Ann Oncol 21:680-682, 2010
13 Hovhannisyan SG, Tragakes E, Lessof S, et al: Health Care Systems in Transition: Armenia. Brussels, Belgium,European Observatory on Health Care Systems, 2001
14 Cohen JC, Cercone JA, Macaya R: Improving Transparency in Pharmaceutical Systems: Strengthening CriticalDecision Points Against Corruption. Washington, DC, World Bank Group, 2002
15 Faucon B, Bariyo N, Whalen J: Thieves hijacking malaria drugs in Africa. http://www.wsj.com/articles/SB10001424052702304672404579181632935636414
16 The Max Foundation. http://www.themaxfoundation.org
17 World Health Organization: Guidelines for Medicine Donations (revised 2010). http://www.who.int/medicines/publications/med_donationsguide2011/en
18 The Max Foundation: Glivec International Patient Assistance Program (GIPAP). http://www.themaxfoundation.org/gipap/Default.aspx
19 O’Brien SG, Guilhot F, Larson RA, et al: Imatinib compared with interferon and low-dose cytarabine for newlydiagnosed chronic-phase chronic myeloid leukemia. N Engl J Med 348:994-1004, 2003
20 Cohen MH, Moses ML, Pazdur R: Gleevec for the treatment of chronic myelogenous leukemia: US Food andDrug Administration regulatory mechanisms, accelerated approval, and orphan drug status. Oncologist 7:390-392, 2002
21 Cohen MH, Williams G, Johnson JR, et al: Approval summary for imatinib mesylate capsules in the treatmentof chronic myelogenous leukemia. Clin Cancer Res 8:935-942, 2002
22 Breccia M, Efficace F, Alimena G: Adherence to treatment is a complex and multifaceted issue that cansubstantially alter the outcome of chronic myeloid leukemia patients treated with tyrosine kinase inhibitors.Leuk Res 36:804-805, 2012
23 Sharf G, Hoffman V, Bombaci F, et al: Non-adherence in chronic myeloid leukemia: Results of a global surveyof 2546 CML patients in 79 countries. Haematologica 98:453, 2013 (abstr S1104)
24 Ibrahim AR, Eliasson L, Apperley JF, et al: Poor adherence is the main reason for loss of CCyR and imatinibfailure for chronic myeloid leukemia patients on long-term therapy. Blood 117:3733-3736, 2011
25 Marin D, Bazeos A, Mahon FX, et al: Adherence is the critical factor for achieving molecular responses inpatients with chronic myeloid leukemia who achieve complete cytogenetic responses on imatinib. J Clin Oncol28:2381-2388, 2010
26 What is my PCR? http://www.whatismypcr.org/
27 Mendizabal AM, Garcia-Gonzalez P, Levine PH: Regional variations in age at diagnosis and overall survivalamong patients with chronic myeloid leukemia from low and middle income countries. Cancer Epidemiol 37:247-254, 2013
28 Sadak KT, Fultz K, Mendizabal A, et al: International patterns of childhood chronic myeloid leukemia: Comparisonsbetween the United States and resource-restricted nations. Pediatr Blood Cancer 61:1774-1778, 2014
29 Kanavos P, Vandoros S, Garcia-Gonzalez P: Benefits of global partnerships to facilitate access to medicines indeveloping countries: A multi-country analysis of patients and patient outcomes in GIPAP. Global Health 5:19, 2009
30 Tekinturhan E, Audureau E, Tavolacci MP, et al: Improving access to care in low and middle-incomecountries: Institutional factors related to enrollment and patient outcome in a cancer drug access program.BMC Health Serv Res 13:304, 2013
31 Farmer P, Frenk J, Knaul FM, et al: Expansion of cancer care and control in countries of low and middleincome: A call to action. Lancet 376:1186-1193, 2010
jgo.ascopubs.org JGO – Journal of Global Oncology Volume 1, Issue 1, October 2015 45