Embed Size (px)
Citation preview

Norwalk Little League
2021
Coaches Book & Safety Manual
Safety Officer: Bryan Ennis
845-527-1240
Safety Code For Norwalk Little League
Our Goal: Injury Prevention
► The Norwalk National Little League follows the safety policies
and procedures of "Little League Baseball" in Williamsport, PA.
Our program focuses on providing coaches and managers with
proper first aid training and direction on the prevention of
injury to players. We welcome the participation of parents in
these efforts.
► The Safety Officer will be a Board Member, versed in Little
League safety procedures and charged with developing and
maintaining a safety program for the league that fosters safe
and injury-free practices.
► Norwalk Little League follows the Concussion Protocol of the
City of Norwalk and all League Coaches and Field Level
Volunteers are required to take CDC Heads Up Concussion
training as well as follow City Protocol which includes training
for players and parents, diligence in watching for any signs of
concussion among players, notification of parents and league of
potential concussion incidents and keeping potentially concussed
players out of practice or play until cleared by a medical
professional to return. All managers and coaches will take the
online Concussion Training Course located at the following URL:"
http://www.cdc.gov/concussion/HeadsUp/online training.html . Once this is
complete, a copy of the printable completion certificate should
be forwarded to their Division Commissioner and League Safety
Officer

► Arrangements will be made to have emergency medical
supplies available at each game or practice. First Aid Kits are
provided for each field and can be found in the field lock
boxes. These kits will be checked and replenished regularly by
the League Safety Officer.
► Managers and coaches shall be trained in First Aid and
Basic Life support, such training to be provided by the League.
Time and place of training will be March 22nd at 7pm via Zoom.
► All games and practices will-be-suspended when weather
does not permit a safe player environment.
► Field conditions will be inspected by both teams' coaches
prior. to any game or practice.
► All dugouts will be policed by the occupying teams before
and after each game or practice to ensure that they are kept
free of debris.
► Only players, managers, coaches, league officials and
umpires are allowed on the playing area and within dugouts
during games and practices.
► Foul balls that are off the playing area will be retrieved
by someone designated by the coach or umpire.
► All players should be kept attentive to game action and alert to
potential harm from flying balls and/or equipment. Likewise all
players should be instructed against any throwing of equipment or swinging of bats anywhere other than the batters box or
designated "on-deck" area.
► Equipment will be maintained in proper working order and
regularly inspected for problems. Any problems should be
brought to the immediate attention of the League Equipment Manager.
► All players will wear all safety equipment as listed in the "Little League Safety Code".
► "Horse play" is not allowed in or near any playing area.
► No head-first sliding will be permitted on initial attainment of
a base. Exception will be made for a player returning to a base
in either a pick-off situation or following a base over-run.
► Players who are required to wear glasses should be encouraged to wear "Safety Glasses" during games and practices.
► Players will not wear watches, rings, pins other jewelry or metallic items while playing.
► Copies of team medical clearance forms are to be kept on-site with coach or manager during games and practices.

► Catchers must wear catcher's helmet, mask, throat
guard, long model chest protector, shin guards and protective
cup with athletic supporter (males) for all games and
practices. NO EXCEPTIONS. Managers should encourage all
male players to wear protective cups and supporters for all
games and practices.
► Coaches are not allowed to catch pitchers (rule# 3.09),
including acting as informal catcher during warm-ups or
batting practices:
► All Managers, coaches and players must remain in the
dugout when not on the field playing or as a base coach during
the game and may not leave without the permission of the
umpire. No "on-deck" batter is allowed in any level of baseball
from Majors or below. The player must go directly from the
dugout to the batter's box. Parents or other children are not
allowed to mingle around the dugout and talk to the players or
offer them food or drink. The batting team is allowed a coach
in the first base coaches' box and a coach in the third base
coaches' box. Any other coach or manager entering the field
of play is an automatic time out and should be done only with
the permission of the umpire.
► All managers and coaches are required to attend training
on March 22nd at 7pm via Zoom. Training will take place via
zoom.

Emergency Numbers:
Dial : 911
Norwalk Police: 854-3000
Norwalk Fire: 866 -3312
Carry Cell Phone
Make arrangements to have a
cellular phone available at your
games and practices (Especially on
fields where public phone access is
unavailable)Um
Remember: Some fields are located right next door to a Fire Station
which contains trained emergency personnel. As you begin First Aid
and/or dial 911, send someone to the Fire Station to request helpH
When To Call 911
If the injured person is unconscious, call 911 immediately. If the victim is
conscious but has any of the following symptoms, call 911 and request a paramedic:
► Trouble breathing or is breathing in a strange way. ► Has chest pain or pressure. ► Is bleeding sever ely. ► Has pressure or pajn in the abdomen that does not go away. ► Is vomiting or pass ing blood. ► Has seizures, severe headache or slurred speech. ► Appears to have been poisoned. ► Has injuries to the head, neck or back. ► Has possible broken bones
911 Protocol :
► Location of emer gency. Tell Them where you are and how to find you..
► Callers Name and Phone Number from which call is being made.
► What Happened: describe the nature of the accident.
► How many people inj ur ed.
► Nature of the injuries.
► What First Aid is being given.
Do not hang up until dispatcher does. Appoint someone to go to the street
and guide ambulance to your precise location. Continue First Aiduntil help
arrives.
Emergency Medical Procedures

Emergency Numbers
Emergency: 911
Norwalk Police: 203-866-4414 Non Emergency
Norwalk Fire: 203-866-3312 Non Emergency
Poison Contro1: l-800-343-2TI2
League Offical Contact Information
Officer Type(s) League President League Secretary League Treasurer League Safety Officer League Baseball Vice President League Other Officer League Other Officer League Coaching Coordinator League Marketing/PR Manager League Other Officer League Other Officer, League Player Agent League Challenger Vice President League Umpire-in-Chief League Other Officer
Norwalk Little League
P.O. Box367
Norwalk, CT 06852-0367
Phone: 203-219-6333
Email: [email protected]
Name Email Day Phone Michael Inzitari [email protected] 203-912-6121 Francis Norris-Oliva [email protected] 203-644-5602 Brian Goddard [email protected] 978-273-6146 Bryan Ennis [email protected] 8455271240 Dan Balliett Doug Dobrydnio
[email protected] 203-856-1808 [email protected] 9143162550
Tyler Fairbairn [email protected] 2034179911 Kirk Gordon [email protected] 203-223-6079 Jessica Herlihy [email protected] 914-409-6691 Russ Miller [email protected] 203-223-1561 Rob Ridell [email protected] 2035555555 Guy Taccone [email protected] 203-838-3326 Greg Vetter [email protected] 2032470929 Jon Zurkowski [email protected] 2036671152

This volunteer application should only be used if a league is manually entering information into JDP 7. Have you ever been refused participation in any other youth programs and/or listed on the SafeSport Centralized or an outside background check provider that meets the standards of Little League Regulations 1(c)9. Disciplinary Database or USA Baseball Ineligible List? Yes No THIS FORM SHOULD NOT BE COMPLETED IF A LEAGUE IS UTILIZING THE JDP QUICKAPP. Visit LittleLeague.org/localBGcheck for more information.
A COPY OF VALID GOVERNMENT ISSUED PHOTO IDENTIFICATION MUST BE ATTACHED TO COMPLETE THIS APPLICATION.
All RED fields are required.
If yes, explain:
(If volunteer answered yes to Question 7, the local league must contact the Little League Security Manager.)
In which of the following would you like to participate? (Check one or more.)
Name
First Middle Name or Initial Last
Date
League Official
Coach
Umpire
Field Maintenance
Manager
Scorekeeper
Concession Stand
Other
Address
City State Zip
Please list three references, at least one of which has knowledge of your participation as a volunteer in a youth program:
Name/Phone
Social Security # (mandatory)
Cell Phone Business Phone
Home Phone: E-mail Address:
Date of Birth
Occupation
Employer
Address
Special professional training, skills, hobbies:
Community affiliations (Clubs, Service Organizations, etc.):
Previous volunteer experience (including baseball/softball and year):
IF YOU LIVE IN A STATE THAT REQUIRES A SEPARATE BACKGROUND CHECK BY LAW, PLEASE ATTACH A COPY OF THAT STATE’S
BACKGROUND CHECK. FOR MORE INFORMATION ON STATE LAWS, VISIT OUR WEBSITE: LittleLeague.org/BgStateLaws
AS A CONDITION OF VOLUNTEERING, I give permission for the Little League organization to conduct background check(s) on
me now and as long as I continue to be active with the organization, which may include a review of sex offender registries (some of
which contain name only searches which may result in a report being generated that may or may not be me), child abuse and criminal
history records. I understand that, if appointed, my position is conditional upon the league receiving no inappropriate information on my
background. I hereby release and agree to hold harmless from liability the local Little League, Little League Baseball, Incorporated, the officers, employees and volunteers thereof, or any other person or organization that may provide such information. I also understand
that, regardless of previous appointments, Little League is not obligated to appoint me to a volunteer position. If appointed, I understand
that, prior to the expiration of my term, I am subject to suspension by the President and removal by the Board of Directors for violation
of Little League policies or principles.
1. Do you have children in the program?
Yes
No
Applicant Signature
If Minor/Parent Signature
Date
Date
If yes, list full name and what level? Applicant Name (please print or type)
2. Special Certification (CPR, Medical, etc.)? If yes, list:
3. Do you have a valid driver’s license?
Yes
Yes
No
No
NOTE: The local Little League and Little League Baseball, Incorporated will not discriminate against any person on the basis of race,
creed, color, national origin, marital status, gender, sexual orientation or disability.
Driver’s License#: State
4. Have you ever been charged with, convicted of, plead no contest, or guilty to any crime(s) involving or against a
minor, or of a sexual nature?
If yes, describe each in full: Yes No
(If volunteer answered yes to Question 4, the local league must contact the Little League Security Manager.)
5. Have you ever been convicted of or plead no contest or guilty to any crime(s)?
Yes
No
If yes, describe each in full:
(Answering yes to Question 5, does not automatically disqualify you as a volunteer.)
6. Do you have any criminal charges pending against you regarding any crime(s)? Yes No
If yes, describe each in full:
(Answering yes to Question 6, does not automatically disqualify you as a volunteer.)
Last Updated: 10/28/2020
Little League® Volunteer Application – 2021 Do not use forms from past years. Use extra paper to complete if additional space is required.
LOCAL LEAGUE USE ONLY: Background check completed by league officer on
System(s) used for background check (minimum of one must be checked): Review the Little League Regulation 1(c)(9) for all background check requirements
JDP (Includes review of the SafeSport Centralized Disciplinary and USA Baseball Ineligible List)*
OR
National Criminal Database check
National Sex Offender Registry
SafeSport Centralized Disciplinary Database and/or USA Baseball Ineligible List Sex Offender
*Please be advised that if you use JDP and there is a name match in the few states where only name match searches can be performed you should notify volunteers that they will receive a letter or email directly from JDP in compliance with the Fair Credit Reporting Act containing information regarding all the criminal records associated with the name, which may not necessarily be the league volunteer.
Only attach to this application copies of background check reports that reveal convictions of this application.

ACCIDENT REPORTING PROCEDURE
What to report -
An incident that causes any player, manager, coach, umpire, or
volunteer to receive medical treatment and/or first aid must be
reported to the NLL Safety Officer.
When to report -
All such incidents described above must be reported to the NLL
Safety Officer within 24 hours of the incident. The NLL Safety
Officer, Bryan Ennis can be reached at the following:
Cell: 845-527-1240
Email: lake98rs@gmail. c-om
Address: 20 Bobwhite Drive Norwalk CT 06851
How to make a report
Reporting incidents can come in a variety of forms. Most typically, they
begin with a telephone conversation followed by filing of the accident
reporting form.. At a minimum, the following information must be
provided:
• The name and phone number of the individual involved.
• The date, time, and location of the incident.
• As detailed a description of the incident as possible.
• The preliminary estimation of the extent of any injuries.
• The name and phone number of the person reporting the incident.
Potential Concussion Reporting
If you have removed a player from play due to symptoms reported by
them or symptoms noticed by you or another coach, you will need to
share the Potential Concussion Notification form, share it with the
parent when they pick up their child, have them sign the bottom
portion, tear off the bottom portion and provide that signed portion to

the League Safety Officer. You should then follow Concussion Protocol
pertaining to return of activity, which includes signed permission from
a Medical Professional.
NLL Safety Officer's Responsibilities -
With in 24 hours of receiving the NLL Accident Investigation Form, the
Safety Officer will contact the injured party or the party's parents
and;
_ verify the information received;
_ obtain any other information deemed necessary;
_ check on the status of the injured party; and
_ in the event that the injured party required other medical treatment
(i.e., Emergency Room visit, doctor's visit, et.) will advise the parent
or guardian of the League's insurance coverage and the provision for
submitting any claims.
If the extent of the injuries are more than minor in nature, the
/------· Safety Officer shall periodically call the injured party to:
_ Check on the status of any injuries, and
_ Check if any other assistance is necessary in areas such as
submission of insurance forms, etc., until such time as the incident is
considered "closed" (i.e., no further claims are expected and/or the
individual is participating in the League again).

Regulation III(d) Note 3 has been amended to read, in part:
Applies to: All Divisions
NOTE 3: If a medical professional, Umpire in Chief, the player's coach, the player's
manager or the player's parent has determined a player sustains a possible concussion, the
player must be, at a minimum, removed from the game and/or practice for the remainder
of that day. The league must also be aware of its respective state/ provincial/municipal
laws with regards to concussions and impose any additional requirements as necessary.
His/her return to full participation is subject to:
I. The league's adherence to its respective state/provincial/municipal laws,
2. An evaluation and a written clearance from a physician or other accredited
medical provider and
3. Written acknowledgement of the parents
Little League International strongly encourages all leagues and teams to not only comply
with any applicable state/provincial/municipal laws, but also, to review the information
and training materials on concussions that are available free of charge on the Centers For
Disease Control website, accessible from the link below. This link provides concussion
information from all 50 states: State Concussion Info
, .,.,........
Summary and Implementation: For the 2013 season, language was added regarding the
recommended procedure a league should follow when a player sustains a possible
concuss10n.

·
·• :i\.·.·<'
./ . ;_:·
IN YOUTH SPORTS
WHAT SHOULD YOU DO IF YOU THINK
YOUR CHILD HAS A CONCUSSION?
1. Seek medical attention right away. A health care
professional wil l be able to decide how serious the
concussion is and when it is safe for your child to
return to sports.
2. Keep your child out of play. Concussions take time
to heal. Don't let your child return to pla y until a
health care prof essiona l says it's OK. Chi ldren who
return to play too soon-while the brain is still
hea li ng- ris k a greater chance of having a second
concussion. Second or later concussio ns can be very
serious. They can cause permanent bra in damage,
affecting your child for a lifetime.
3. Tell your child's coach about any recent
concussion. Coaches should know if your child had
a recent concussion. Your chi ld' s coach may not know
about a concussion your child received in another
sport or activity unless you te l l the coach.
IMPORTANT PHONE NUMBERS
FILL TN THE NAME AND NUMBER OF YOUR LOCAL
HOSPIT AU SJ BELOW:
Hosp i tal Name: _ _ _ _ _ _ _ _ _ _ _ _ _
Ho spi ta l P hone_: _ _ _ _ _ _ _ _ _ _ _ _
Hosp rui l Name_: _ _ _ _ _ _ _ _ _ _
Hosp rui l P hone: _ _ _ _ _ _ _ _ _
For immediate attention. CALL 911
For more information and to order additional materials free-o f-charge, visit:
www.cdc.gov/ConcussionlnYouthSports

1
· .r .c
o "' IN YOUTH SPORTS
Concussion Training for Coaches
INTRODUCTION
Each day in ou r nation, hundreds of thousands of young athletes head out
to fields, ice and gymnasiums to practice and compete in a wide variety of
sports. There's no doubt that these sports are a great way for kids and teens
to stay healthy, as well as learn impor t ant leadership and team-bu ildi ng skill s.
But medical researchers have discovered young athletes1 especially kids and
teens1 often don't recognize their own limi t ations; especial ly when they have
a concussion.
Youth concussion can have long term impacts on young athletes such as their
healt h, memor y, learning and even their su rviva l. This has lead to a new effort to
improve preven t ion, recognition and response to sport s-re lated concussion .
That1s where you come in. I t' s your responsibi lit y as a coach, to help recognize
and make the cal l to pull an athlet e off the field, ice, or court if you t hink that
player might have a co nc ussio n.

LESSON 1
All concussions are se1-io us.
Concussions can happen in any sport or recreational activity.
Recognizing and responding properly to concussions when they first occur can help
prevent further injury or even death.
Understanding Concussion
A concussion is a type of traumatic brain injury
or TBI-caused by a bump, blow, or jolt to the
head or by a hit to the body that causes your head
and brain to move rapidly back and forth.
This sudden movement can literally cause the
brain to bounce around or twist in the skull,
stretching and damaging the brain cells and
creating chemical changes in the brain.
What you might not know is that these chemi -
cal changes make the brain more vulnerable to
further injury. During this window of vulnerability
the brain is more sensitive to any increased stress
or injury, until it fully recovers.
Unlike a broken arm, or other injuries that you
can feel with your hands or see on an x-ray, you
can't see a concussion. It is a disruption of how
the brain works. It is not a "bruise to the brain."
That is why brain CAT scans and MRls are
normal with most concussions.
Causes of Concussion A knock to the head from a fall ...
A jolt to the torso from a collision ...
A hit to the head from a stick or ball ...
A concussion can occur from any type of contact
such as colliding with a player, a goalpost, the
ground, or another obstacle. Concussions can also
occur outside of sports, ranging from bumping
your head on a door to being in a car crash.
Don't be fooled! Even what may seem like a mild
bump to the head can actually be serious.
Potential Consequences
of a Concussion
Concussions affect people differently. While most
athletes with a concussion recover quickly and
fully, some will have symptoms that last for days,
or even weeks. A more serious concussion can last
for months or longer.
Not giving the brain enough recovery time after a
concussion can be dangerous. A repeat concussion
that occurs before the brain recovers from the
first-usually within a short time period (hours,
days, weeks)-can slow recovery or increase the
chances for long-term problems. In rare cases,
repeat concussions can result in brain swelling or
permanent brain damage. It can even be fatal.
Yes, while rare, permanent brain damage and
death are two potential consequences of not
identifying and responding to a concussion in a
proper or timely manner.
That's why is it incredibly important for you to
pull an athlete from play if you suspect he or she
has a co ncussion.
Did You !<now?
• Most concussions occur without loss
of consciousness.
• Athletes who have, at any point in
their lives, had a concussion have an
increased ri sk for another concussio n.
• Young child r en and teens are more
likely to get a concussion and take
longer to recover than adult s.

LESSON 2
What to Watch for As a coach you're the first defel'lse, ready to jump
i11 to he'ip if something seems " off" -even when
an athlete d0esn't know it or want to admit it.
Remember, you can' t see a concuss.ion, Hke you
can see a broken a;rm, and there is n0 one sing:le
ind k ator for concussron. Instead, rec09r:dzin9 a
concussi0n requires watchi,ng for different ty:pes
of signs or symptoms.
So to help recognize a concussion, you sh0u,ld
watch for and ask others to report the folfowing
t wo t h-ings amQng you r atMe tes:
(\?S?\ A forceful bump, blow, or j,olt to the head
o:r body that results in rapid movement of
the head.
-and-
@m0A· ny co:ncuss.,o.n signs or symptoms, such as a
change in th e athlete's beha vi0 r, th!nldnlll,, 0 r
physical functioning..
I<eep the following list 0f signs and symptoms 0n
hand. Athletes who exhib+t or report one ar more
of the signs and symptoms listecl below, or simply
say they just " don' t feel right" after a bump, b4.ow,
or j1:,:lt to the head or body, may have a concussion.
Signs and symptoms of concussion genera .lfy show
u1!) s o.on after the ,i rn jury. But the fu H effect of the
lnj:ury may not be notlcea:ble at first and smme
sy.mptoms may not show up for hmurs or days. For
example, il'l the first few minutes the atl11ete might
be sltghtly confused o:r appear a little bit dazed,
but an hour later th€y can't reca.fl c.oming to the
pracHce, game, o•r event.
S0 asses the player, then assess th€ i,i:layer
again. Make sure that the athlete is supervised
for at least o:ne or two hours after y0u susll)ect
a C.O:F1Ct1ss ion. Also, talk tm the athlete's parents
about wa,tch:ing for symptoms at home and when
the athlete returns t0 school.
The key is to keep a list of concussi:on signs
and symptoms in your cli pbo ard, and t0 use
ft wh He repeatedly checking on your athlete
with a suspected concussion. You can order CDC' s
free ' Heads Up" materials with concussion signs
and symptoms to place on your clipboard for all
practices and games, and post ln the l0cker rooms.
SIGNS OBSERVED BY COACHING STAFF SYMPTOMS REPORTED BY ATHLETES
Appears dazed or stunned
1s•..q fiis d o giiis 1 Jr·8dsHt6fr > i• i\
Fm.rgets an instruction
....··r.sJnsufoof 9 :e;scb& ot·JJ tirie i: Moves clumsily
H,eadache er "pressure" in head
·.··.• Afwis ers :qtle t16ns) l ,l j <
Lmses cmnscio1:.1sness (even briefly)
.··.·•·.··S.frdwms·•: ood,:hefui i b'r:·8 f!;O'rl li1:y"••i:h aAi ·, •••• ••• >•.·•:·•>·¢ n#; t1¥ratldri••i:sl
i½ Mitil'Y Pf6:bi ffis{,\>·.•·:··•·:·•·. : .•···•.
Can't recall events prior to hit oer fal·I
· · t an1i+e2J1fev.J,¼:f k# rhHibf fain Confusion
. : i:ci /}ti 1f i i H' ti:?: · etf fl.fh
d••
r r/ ••• ·•-·: •-•··• ·

Danger Signs
If the signs or symptoms get worse, you need to consider it a medical emergency.
In rare cases, a dangerous blood clot may form on the brain in an athlete with a
concussion and squeeze the brain against the skull. Call 9-1-1 or take the athlete to
the emergency department right away if after a bump, blow, or jolt to the head or body,
he or she exhibits one or more of the following danger signs:
One pupil larger than the other
Drowsiness or inability to wake up
A headache that gets worse and does
not go away
e- Weakness, numbness, or decreased
coordination
Repeated vomiting or nausea
Slurred speech
LESSON 3
When You Suspect a Concussion
Pulling someone out of the middle of a practice,
game, or event is never an easy thing, especially if
an athlete tells you that nothing is wrong.
But we know that your top priority is keeping your
athletes safe and preparing them for the future
both on and off the field.
That's why we encourage you to follow these
steps, which are part of CDC's 11 Heads Up" four
step action plan:
(i) Remove the athlete from play. Look for the
signs and symptoms of a concussion, if your
athlete has experienced a bump or blow to the
head or body. When in doubt, sit them out.
Convulsions or seizures
Inability to recognize people or places
Increasing confusion, restlessness, or
agitation
Unusual behavior
Loss of consciousness (even a brief
loss of consciousness should be taken
seriously!
(€) Ensure that the athlete is evaluated by a
health care professional experienced in
evaluating for concussion. Do not try to
judge the severity of the injury yourself. Health
care professionals have a nu.mber of methods
that they can use to assess the severity of
concussions. As a coach, recording the following
information can help health care professionals
in assessing the athlete after the injury:
Cause of the injury and force of the hit or
blow to the head or body
Any loss of consciousness (passed out/
knocked out) and if so, for how long
Any memory loss immediately following
the injury
Any seizures immediately following the
injury
Number of previous concussions (if any)

(D Inform the athlete's parents or guardians
about the possible concussion and give
them the CDC fact sheet on concussion
for parents. This fact sheet can help parents
monitO'r the athlete for sign or symptems that
appear or get worse once the athlete is at
home or returns to school.
(D Keep the athlete out of play the day of the
injury and until a health care professional,
experienced in evaluating for concussion,
says it's OK for the athlete to return. In
the case of suspected concussion, the decision
about when to return to practice or play is a
medical decision.
LESSON 4
Why Take a Time Out? Resting after a concussion is critical because it
helps the brain recover.
Remember those brain cells we talked ab0ut ear
lier that aren't working properly? Well, they need
t he body's energy to heal. So, if an athlete with a
concussion spends that energy exercising , tryin111 to
score a goal, or doing other recreational activities,
that means there's less energy available to help
the brain repair itself.
That's why ignoring concussion symptoms and
trying to "tough it out" often makes symptoms
worse and can make recovery take longer,
sometimes for months. Even activities that involve
learning and concentration,such as studying,
working on the computer, or playing video games,
can cause concussion symptoms to reapl!)ear or
get worse.
It's up to a healthcare profess.ional to determine if
an injured athlete' s concussion sympt oms have been
reduced significantly, and when he or she should
slowly and gradually return to daily activities.
"Toughing it Out" isn't Strong
It's Dangerous Sometimes people believe that it shows strength
and co1;1rage to play when you're injured. Not only
is that belief wrong, it can put a young athlete at
risk for serious injury.
Don't let others- fans, parents, or teammates
pressure you or the injured athlete to continue
!!)l ayin g. As you've probably experienced, some
athletes may try telling you thats/he is "just fine"
or thats/he can 11t0ugh it out."
Tell them that taking a time out is not a sign
of weakness, and that playing with a concussion
is dangerous. Don't shy away from sharing
this information with parents and other team
supporters, either.
Both physical and cognit ive act ivit ies- such
as concentration and learning- should be
carefully managed and monitored by a health
care rm, !lf essi0nal until they give you and your
athlete the t1ireen light.
At fi.rst, be prepared for your player to offer
resistance-the player might feel frustrated, sad,
or even angry abQUt hav ing to sit out .
• Talk to them about it.
• Be honest about the risks of getting put back
into play too soon.
Offer your supl!)ort and encouragement.
• Tell them that as the days go by, they'II feel
better.
Progressive Return to Activity Program
Back to Sports
An athlete should return to sports practicesunder
the supervi sion of an appropriate health care
profess.ional. When available, be sure to work
closely with your team's cert ifi ed athletic t rainer.

There are five gradual steps that you and the
health care professional should follow to help
safely return an athlete to play. Remember, this
is a gradual process. These steps should not be
completed in one day, but instead over days,
weeks, or months.
Step l Begin with light aer obic exercise, but
only to increase an athlete's heart rat e.
This translates into 5 to 10 minutes
on an exercise bike, walking, or light
jogging. There should be no weight lifting,
jumping or hard running at this point.
Step 2 Add activities that increase an athlete's
heart rate, and incorporate limited
body or head movement. This includes
moderate jogging, brief running,
moderate-intensity stationary biking,
and moderate-intensity weightlifting
(reduced time and/or reduced weight
from your typ ical rout ine).
Step 3 Bump it up a notch to heavy, non-contact
physical activity. This includes sprinting/
running, high-intensity stationary biking, ·
the player's regular wei ght li ft ing routine,
and non-contact sport-specific dl'ills On
3 planes of movement).
Step 4 Reintegrate the athlete in practice
sessions, even full contact in controlled
practice if appropriate for the sport.
Step 5 Put him or her back into play.
During each step, keep your eyes open for
returning symptoms, including fuzzy thinking
and concentration. Any symptoms need to be
reported to the athlete's health care professional. If
an athlete's symptoms come back, ors/he exhibits
new symptoms with this increased activity, stop
these activities and take it as a sign that the
athlete is pushing him/herself too hard.
After additional rest, and an ok from their health
care professional, the athlete may start over again
at Step 1.
The athlete should on{>'graduate to the next level
of act ivity ifs/he does not experience concussion
symptoms.
Back to the Books
Supporting a student recovering from a
concussion requires a collaborative approach
among school professionals, health care
professionals (including a cer ti fied athletic
trainer), parent s, and st udents.
Not on ly can they help ease the transition, and
make accommodations for a student if needed,
they can also keep an eye out for problems like
inability to pay attention, remember or learn new
information; inappropriate or impulsive behavior
dur ing class; or other concussion symptoms such
as fatigue or headaches.
Students who return to school after a concussion
may need to:
Take rest breaks as needed,
Spend hours at school,
Be given more time to take tests or complete
assignments,
Receive help with schoolwork, and/or
Spend less time on the computer, reading,
or writing.
As the student's symptoms decrease, the extra
help or support can be gradually removed.
Remember
Concussions affect people differ en t ly.
While most athletes wit h a concussion
1· ecovei- quickly and fully, some will have
symptoms that last for days, or even
weeks. A more serious concussion can
last for mont hs or lon ger.

LESSON 5
By taking th,is training-and taking concussions
serio.usly-y0u've shown your dedicaUon to you-r
athletes and their safety.
Now, it's time to take what you've lea.:rned
to your coaching staff, team, parents, school
p·rofess.i:onals and community. GeneraHng the
support you'll need when it comes to identify
ing a-nd respondJng to a concussion now wiJI
help later when )'<)U need to pull out an athlete
because you suspect a concussi:o:n
Use the following preparedness checklists to
gu.ide you throwgh pre- , mid- , and post-seasons.
Pre-season Checklist Check with your lea9ue, scha,,.J, or district
about concussion p0lfr:i.es.
Concussion policy statements should include
the sch.D'ol or J.ea.gue's commitment to
sa-fety, a brief descri:ptio-n of concuss.klfl,
and information on when athletes can safely
return to play. Parents and athletes should
si.gn the concussion poHcy statement at the
beg'inning of each sports season.
Win the support and involvement of
other schoo,I or league rrfficials-stich as
p:rincipa!s1 certified ath:!etic:: trainers, other
coaches, schoo1 nurses, and pa-rent-teacher
associations-to help ensure that school
rules and concussi,on pol-ides are in p-Iace
before the first praetice.
Create a concussion action plan.
To ensure that concussiuns are identified
ear-ly and managed co:rrectJy, have an acUOfl
plan in place before the season starts. You
can use the ''Heads Up"fou-r-step action
plan and include it in your league, school, or
district's concuss-ion po-Hey.
Educate athletes, parents, and other
coaches about concussion.
Dedicate a team meeting to talk about
concussion and before the first practice,
talk to ath,letes, parents, other coaches,
and league and school officials about
the dangers of concussion; potential
f.c:ing-term consequences of concuss.ion;
and yotr.r concerns as weH as your
expectations of safe pl.ay.
Show rnncessi,on videos available on CDC's
website. Pass out concussion fad sheets for
athletes and for parents at the beginn,ng of
the sea5on, and again if a concuss-ion occu,rs.
Remind ath,letes to immediately tell the
coaching staff if they suspect that they
have a concussion o-r that a teammate has
a concuss.ion..
Monitor the health of your athletes.
Review the signs and symptoms of
concussion, and keep the,., Heads Up''
four-step action plan with you at games
a:fil:d practkes. (Carry the" Heads Up"
clfpboard with you and fill out the
pocket card or cl:i,pboard sti,cker so that
infonnati:an about si ns, symptoms, and
emergency contacts is readHy avai.labl,e.l
Make su,re to ask if an athlete has ever had
a concussie-n, and insist that your athletes
be medkally evaluated and in good condition
to partidpate.
Pri-Or to the first pracUce, determine whether
your school or league has or would consider
conducting p.re-season, baseline testing. Also
known a5 neu.roco,gnitive tests, these tests
hefp assess bra,n function <including learning
and memory skHls, ability to pay attention or
concentrate, and how q·uick!y someone can
think and solve problems) and can be used
a9a,i,n during the season if an athlete has
a concuss-ion, to identify the effects of the
inj,u,ry. Identify the appropriate health care
p,rofessional to run tills program.

Mid-season Checklist
Insist that safety comes first.
Teach and remind athletes of safe-playing
techniques. Encourage them to follow the
rules of play; to practice good sportsmanship
at all times; and to consistently wear the
right protective equipment (that fits properly,
is well-maintained, and worn correctly) for
their activity.
Teach your athletes that it's not smart to play
with a concussion.
Remind your athletes and everyone who
influences them-teammates, fans, parents,
fellow students-playing with a concussion
is dangerous.
Work closely with other league or school
officials-
Be sure that appropriate staff is available for
injury assessment and referrals for further
medical care.
Enlist certified athletic trainers, school nurses,
or appropriate school or league officials to
monitor any changes in the athlete's behavior
or school work that could indicate that the
student has a concussion. Ask them to report
concussions that occurred during the season.
This will help in monitoring injured athletes
who participate in multiple sports throughout
the year.
Post-season Checklist
Keep a concussion log.
Work with a certified athletic trainer, school
nurses, and other school or league staff to
review injuries that occurred during the season.
Discuss with other staff any needs for better
concussion prevention or response preparations.
Review your concussion policy and action plan.
Discuss any need for improvements to
your concussion policy or action plan with
appropriate health care professionals and
league or school staff, especially in light of
what your log reveals.
SUMMARY
We hope, through this module, that you've come to better understand the impact sports
related concussion can have on youth athletes. If we, as coaches and parents, come to better
understand this impact, become mo,-e focused on its recognition, and more resolved to pull
athletes from the game when there is a possibility of concussion, we will have come a long
way towards reducing the impact of this all too common injury.
And always remember - When in Doubt, Sit them Out!
To learn more about concussion or to order concussion educational materials
free-of-charge-contact the CDC at 1-800-CIIC-INFO or visit:www.cdc.gov/Concussion.

0
Final Quiz for Coaches
(0 A concussion is a:
A. type of traumatic brain injury (or TBil caused by a bump, blow, or jolt to the head or by
a hit to the body that causes the head and brain to move rapidly back and forth.
B. a brain bruise.
C. loud sound heard from far away.
( When can concussions occur?
A. Only when playing full contact sports.
B. Only when the individual who was hit or jolted loses consciousness.
C. I n any organized or unorganized recreational sport or activity and most occur without
loss of consciousness.
(3) How do you identify a concussion?
A. By looking at CT or MRI scans of an individual's brain.
B. By watching for different types of signs or symptoms, such as a change in the athlete's
behavior, thinking, or physical functioning .
C. Asking an athlete if they had their "bell rung" in the last hit.
( Which of the following are signs of a concussion that you as a coach may identify?
A. The athlete appears stunned, is unsure of the game, score, or opponent, is confused about
their assignment or position, and is answering questions slowly.
B. The athlete follows the rules for safety and the rules of the sport, practices good sport s
manship, and uses the proper equipment for the sport.
C. The athlete looks pale, their tongue is white, and after gently pinching the skin, it does not
immediately snap back into place.
( Which of the following are symptoms of a concussion that an athlete may describe?
A. The athlete complains of shoulder pain that radiates down the arm to a tingling feeling in
the fingers.
B. The athlete feels weak, tired, and has stopped sweating.
C. The athlete states the lights hurt their eyes, they feel confused,"not right", and complains
of an odd headache with "pressure" in their head.
---
I
1\ H -:';
· ;,
--

CD If an athlete has had a previous concussion they:
A. are more likely to sustain another concussion, especially if the first concussion has not had
time to heal.
B. wil I never have another concussion.
C. will not sustain another concussion from a similar blow or jolt.
(j) What is the first thing you should do as a coach when one of your players has sustained a bump or blow to the head or body and isn't acting right?
A. Immediately rush an athlete to the hospital-even if none of the Danger Signs are present.
B. Allow the athlete to finish out the quarter/period/half, etc. and then take the athlete for a
medical examination.
C. Remove the athlete from play and look for signs or symptoms of a concussion-even those
that may appear hours later.
CD Which of the following would be considered Danger Signs of a severe concussion and
require rushing an athlete to the emergency department immediately?
A. The athlete seems slightly off balance, complains of a headache, did not lose consciousness,
but just "isn't feeling right."
B. The athlete lost consciousness, has slightly slurred speech, and seems to become increasing
more confused and restless.
C. The athlete complains of a headache and appears slightly dazed or stunned.
Cv When can an athlete return to play after a concussion?
A. As soon as they are feeling better.
B. After being evaluated by a health care professional.
C. After being cleared by a health care professional and after a five step process in which the
athlete's activity level is slowly increased over a period of days, weeks, or months depending
on the athlete's response to the increasingly challenging activities.
0°V When should you talk to the athlete's parents about the possible concussion he/she may have had?
A. The evening of the event or the following day.
B. Immediately following the game or practice-before allowing the child to go home.
Information should be given to the parents regarding the signs and symptoms of concussion,
encouragement to see a health care professional, and follow-up with parents regarding the
status of the athlete.
C. Before the next game/match/event so as to make sure the child is cleared for play.
0".0 How can you help prevent concussions?
A. By ensuring that all athletes wear properly fitted gear, play with good sportsmanship at all
times, and obey the rules of safety.
B. By working with parents, athletes, and school and club administrators to spread awareness
about concussions all year: pre-season, during the season, and post season.
C. Both A and B.

..---.
s ort P rent ode f Conduct
C
..--...
We the-------:------:------:---= ---- =- Little League, ha;e implemented the following Spo1t Parent Code of
Conduct for the important message it holds about the
proper role of parents in supporting their child in sports.
Parents should read, understand and sign this form prior
to their children participating in our league.
Any parent guilty of improper conduct at any game or
practice will be asked to leave the sports facility and be
suspended from the following game. Repeat violations
may cause a multip.le game suspension, or the season
forfeiture of the privilege of attending all games.
Preamble
The essential elements of character-building and ethics
in sports are embodied in the concept of sportsmanship
and six core principles:
• Trustworthiness,
• Respect,
• Responsibility,
• Fairness,
• Caring, and
• Good Citizenship.
The highest potential of sports is achieved when
competition reflects these "six pillars of character."
I therefore agree:
l. I will not force my child to participate in sports.
2. I will remember that children participate to have fun
and that the game is for youth, not adults.
3. I will inform the coach of any physical disability or
ailment th.at may affect the safety of my child or the
safety of others.
4. I will learn the rules of the game and the policies of
the league.
5. I (and my guests) wi11 be a positive role model for my
child and encourage sportsmanship by showing
respect and courtesy, and by demonstrating positive
support for all players, coaches, officials and specta
tors at every game, practice or other sporting event.
6. I (and my guests) will not engage in any kind of
unsportsmanlike conduct with any official, coach,
player, or parent such as booing and taunting; refus
ing to shake hands; or using profane language or gestures.
7. I will not encourage any behaviors or practices
that would endanger the health and well being of
the athletes.
8. I will teach my child to play by the mies and to
resolve conflicts without resorting to hostility
or violence.
9. I will demand that my child treat other players,
coaches, officials and spectators with respect
regardless of race, creed, color, sex or ability.
1O. I will teach my child that doing one's best is more
important than winning, so that my child will never
feel defeated by the outcome of a game or
his/her perfom1ance.
11. I will praise my child for competing fairly and
trying bard, and make my child feel like a winner
every time.
12. I will never ridicule or yell at my child or other
participants for making a mistake or losing a
competition.
13. r will emphasize skill development and practices and
how they benefit my child over winning. I will also
de-emphasize games and competition in the lower
age groups.
14. I will promote the emotional and physical well
being of the athletes ahead of any personal desire
I may have for my child to win.
15. I will respect the officials and their authority during
games and will never question, discuss, or confront
coaches at the game field, and wilt take time to
speak with coaches at an agreed upon time
and place.
I 6. I will demand a sports environment for my child that
is free from dmgs, tobacco, and alcohol and I will
refrain from their use at all sports events.
17. I will refrain from coaching my child or other
players during games and practices, unless I am
one of the official coaches of the team.
Parent/Guardian Signature
I\ L _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _,

CDC - Heads Up Online Training Course - Concussion - Traumatic Bra... http://www.cdc.gov/concussion/HeadsUp/online_training.html
Centers for Disease Control and Prevention CDC 2 7:&,,.,;ng u,es. Prot.,ettni;i Poop!<>. Sovlng Mon,,ythroui;ih Preventoo.
AKE THE.FREE NLINE CONCUSSIO RAINING .... -rCoaches ·
(/concussion/HeadsUp/Training
/HeadsUpConcussion.html) Heads Up Online Training Course
Get prepared for the new season in less than 30 minutes
Heads Up: Concussion in Youth Sports is a free, online course available to coaches, parents, and
others helping to keep athletes safe from concussion. It features interviews with leading experts,
dynamic graphics and interactive exercises, and compelling storytelling to help you recognize a
concussion and know how to respond if you think that your athlete might have a concussion.
Once you complete the training and quiz, you can print out a certificate, making it easy to show your league or school you are ready for the season.
What You Will Learn This course will help you:
• Understand a concussion and the potential consequences of this injury, • Recognize concussion signs and symptoms and how to respond, • Learn about steps for returning to activity (play and school) after a concussion, and • Focus on prevention and preparedness to help keep athletes safe season-to-season.
We can help athletes stay active and healthy by knowing the facts about concussion and when it is safe for athletes to return to play.

CDC - Heads Up Online Training Course - Concussion - Traumatic Bra... http://www.cdc.gov/concussion/HeadsUp/online_training.html
(/24-7/SavingLives/Concussions/)
Take the Training > > (/concussion/HeadsUp/Training
/Heads UpConcussion.html)
Cole's Story: CDC Heads Up! Concussion Training Saved My Life! ((24-7/SavingLives
I Concussions/)
Read how CDC's online coaches' training helped a coach to recognize and respond to
concussion in a young athlete.
Download the Course Script and Quiz:
• English: script (/concussion/headsup/pdf/Heads Up Concussion rn Sports Script-a.pelf) and quiz (/concussion/headsup/pdf/Heads Up 0uiz-a.pdf)
• Spanish: script ((concussion/headsup /pdf/Heads Up Concussion in Sports Script SPANISH-a.pd£) and quiz (/concussion /headsup/pdf/Heads Up Quiz Spanish-a.pd£)
CDC's Heads Up online course for youth sports coaches is now available in a CD-ROM format for
use at events, training sessions, and conferences. Please contact [email protected]
(mailto:[email protected]) to obtain a copy of the CD-ROM.
Order or Download the Parent and Athlete Information Sheet:
• English: Parent/Athlete Information Sheet-,:, (/concussion/headsup /pelf/Parent Athlete Info Sheet-a.pd£)
• Order (http://wwwn.cdc.gov/pubs/ncipc.aspx#tbi4)
Learn More:
• Concussion in Sports (http://www.cdc.gov/concussion/sports/index.html) • Resources for High School Sports ChttJ>://www.cdc.gov/concussion/HeadsUp/high school.html)
• Resources for Youth Sports (http://www.cdc.gov/concussion/HeadsUp/youth.html)
• Resources for School Professionals (http://www.cdc.gov/concussion/HeadsUp/schools.html)
• Resources for Health Care Professionals (http://www.cdc.gov/concussion/clinician.html)

CDC - Heads Up Online Training Cmrrse - Concussion - Traumatic Bra... http://www.cdc.gov/ concussion/HeadsUp/online_training.html
Follow us on Facebook@ {http://www.facebook.com/cdcheadsup) and share your experiences and learn about new CDC's resources to help parents and coaches
address concussion in sports.
Page last reviewed : July 26, 2011
Page last updated: July 26, 2011
Content source: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control
Centers for Disease Control and Prevention 1600 Clifton Rd. Atlanta, GA 30333,
USA 800-CDC-INFO (800-232-4636) TIT: (888) 232-6348, New Hours of Operation
8am-8pm ET/Monday-Friday
Closed Holidays - [email protected]

[INSERT YOUR LOGO]
Concussion, a type of traumatic brain injury, is caused by a bump, blow, or jolt to the head. Concussions can also occur from a blow to the body that causes the head and brain to
move rapidly back and forth-literally causing the brain to bounce around or twist within the skull.
This sudden movement of the brain causes stretching and tearing of brain cells, damaging the cells and creating chemical changes in the brain.
HOW CAN I RECOGNIZE A POSSIBLE CONCUSSION?
Concussions can result from a fall or from athletes colliding with each other, the ground, or with an obstacle, such as a goalpost. Even a "ding," "getting your bell rung," or what seems to be a mild bump or blow to the head can be serious.
As a coach you are on the front line in identifying an athlete with a suspected concussion. You know your athletes well and can recognize when something is off-even when the athlete doesn't know it or doesn't want to admit it.
So to help spot a conc ussi on, you should watch for and ask others to report the following two things:
1. A forceful bump, blow, or jolt to the head or body that results in rapid movement of the head.
AND
2. Any concussion signs or symptoms, such as a change in
the athlete's behavior, thinking, or physical functioning.
Signs and symptoms of concussion generally show up soon after the injury. But the full effect of the injury may not be noticeable at first. For example, in the first few minutes the athlete might be slightly confused or appear a little bit
dazed, but an hour later they can't recall coming to the practice or game.
You should repeatedly check for signs of concussion and
also tell parents what to watch out for at home. Any worsening of concussion signs or symptoms indicates a medical emergency.
SIGNS AND SYMPTOMS
Athletes who experience one or more of the signs and symptoms listed below, or who report that they just ''don't feel right,'' after a bump, blow, or jolt to the head or body, may have a concussion.
SYMPTOMS REPORTED BY ATHLETE: • Headache or "pressure" in head • Nausea or vomiting • Balance problems or dizziness • Double or blurry vision • Sensitivity to light • Sensitivity to noise • Feeling sluggish, hazy, foggy, or groggy • Concentration or memory problems • Confusion • Just not "feeling right" or is "feeling down"
SIGNS OBSERVED BY COACHING STAFF: • Appears dazed or stunned • Is confused about assignment or position • Forgets an instruction • Is unsure of game, score, or opponent • Moves clumsily • Answers questions slowly • Loses consciousness (even briefly) • Shows mood, behavior, or personality changes
• Can't recall events prior to hit or fall • Can't recall events after hit or fall
WHAT IS A CONCUSSION?

WHAT ARE CONCUSSION DANGER SIGNS?
. . ......-.. :. .--··..- ,:· .·. .' -... :, ..·.· . ·.......,.·:::._.:,.•. ,•, •...,..
In rare cases, a dangerous blood clot may form on the brain in an athlete with a concussion and crowd the brain against the skull. Call 9-1-1 or take the athlete to the emergency department right away if after a bump, blow, or jolt to the head or body the athlete exhibits one or more of the following danger signs:
• One pupil larger than the other • Is drowsy or cannot be awakened • A headache that gets worse • Weakness, numbness, or decreased coordination • Repeated vomiting or nausea • SIurred speech • Convulsions or seizures • Cannot recognize people or places • Becomes increasingly confused, restless, or agitated • Has unusual behavior • Loses consciousness {even a brief loss of consciousness
should be taken seriously)
FACTS
Sometimes people wrongly believe that it shows strength and courage to play injured. Some athletes may also try to hide their symptoms.
Don't let your athlete convince you that he or she is "just fine" or that he or she can '\tough it oul" Discourage others from pressuring injured athletes to play. Emphasize to athletes and parents that playing with a concussion is dangerous.
WHAT SHOULD I DO IF A CONCUSSION IS SUSPECTED?
No matter whether the athlete is a key member of the team or the game is about to end, an athlete with a suspected concussion should be immediately removed from play. To help you know how to respond, follow the Heads Up four step action plan:
1. REMOVE THE ATHLETE FROM PLAY.
Look for signs and symptoms of a concussion if your athlete has experienced a bump or blow to the head or body. When in doubt, sit them out!
2. ENSURE THAT THE ATHLETE IS EVALUATED BY AN APPROPRIATE HEALTH CARE PROFESSIONAL.
Do not try to judge the severity of the injury yourself. Health care professionals have a number of methods that they can use to assess the severity of concussions. As a coach, recording the following information can help health care professionals in assessing the athlete after the injury:
• Cause of the injury and force of the hit or blow to the head or body
• Any loss of consciousness {passed out/knocked out) and if so, for how long
• Any memory loss immediately following the injury • Any seizures immediately following the injury • Number of previous concussions (if any)
3. INFORM THE ATHLETE'S PARENTS OR
GUARDIANS. Let them know about the possible concussion and give them the Heads Up fact sheet for parents. This fact sheet can help parents monitor the athlete for sign or symptoms that appear or get worse once the athlete is at home or returns to school.
4. KEEP THE ATHLETE OUT OF PLAY.
An athlete should be removed from play the day of the injury and until an appropriate health care professional says they are symptom-free and it's OK to return to play. After you remove an athlete with a suspected concussion from practice or play, the decision about return to practice or play is a medical decision.
JOIN THE CONVERSATION

WHY SHOULD I BE CONCERNED ABOUT CONCUSSIONS?
Most athletes with a concussion will recover quickly and
fully. But for some athletes, signs and symptoms of
concussion can last for days, weeks, or longer.
If an athlete has a concussion, his or her brain needs time to
heal. A repeat concussion that occurs before the brain
recovers from the first-usually within a short time period
(hours, days, weeks)-can slow recovery or increase the
chances for long-term problems. In rare cases, repeat
concussions can result in brain swelling or permanent brain
damage. It can even be fatal.
DID YOU l<NOW?
• Young children and teens are more likely to get a
concussion and take longer to recover than
adults.
• Athletes who have ever had a concussion are at
increased risk for another concussio.n
• All concussions are serious.
• Recognition and proper responsed to concussions
when they first occur can help prevent further
injury or even death.
HOW CAN I HELP ATHLETES TO RETURN TO PLAY GRADUALLY?
An athlete should return to sports practices under the
supervision of an appropriate health care professional.
When available, be sure to work closely with your team's
certified athletic trainer.
Below are five gradual steps that you and the health care
professional should follow to help safely return an athlete to
play. Remember, this is a gradual process. These steps
should not be completed in one day, but insteadover days,
weeks, or months.
BASELINE: Athletes should not have any concussion symptoms. Athletes
should only progress to the next level of exertion if they do
not have any symptoms at the current step.
STEP 1: Begin with light aerobic exercise only to increase an
athlete's heart rate. This means about 5 to 10 minutes on
an exercise bike, walking, or light jogging. No weight lifting
at this point.
STEP 2: Continue with activities to increase an athlete's heart rate
with body or head movement. This includes moderate
jogging, brief running, moderate-intensity stationary biking,
moderate-intensity weightlifting (reduced time and/or
reduced weight from your typical routine).
STEP 3: Add heavy non-contact physical activity, such as sprinting/
running, high-intensity stationary biking, regular
weightlifting routine, non-contact sport-specific drills (in 3
planes of movement).
STEP 4: Athlete may return to practice and full contact (if
appropriate for the sport) in controlled practice.
STEP 5: Athlete may return to competition.
If an athlete's symptoms come back or she or he gets new
symptoms when becoming more active at any step, this is a
sign that the athlete is pushing him or herself too hard. The athlete should stop these activities and the athlete's health
care provider should be contacted. After more rest and no
concussion symptoms, the athlete should begin at the
previous step.

HOW CAN I HELP PREVENT CONCUSSIONS OR OTHER SERIOUS BRAIN INJURIES?
Insist that safety comes first To help minimize the risks for concussion or other serious brain injuries:
• Ensure that athletes follow the rules for safety and the rules of the sport.
• Encourage them to practice good sportsmanship at all times.
• Make sure the athlete wears the right protective equipment for their activity. Protective equipment should fit properly, be well maintained, and be worn consistently and correctly.
• Wearing a helmet is a must to reduce the risk of severe brain injury and skull fracture. However, a helmet doesn't make an athlete immune to concussion. There is no "concussion-proof" helmet
Check with your league, school, or district about concussion policies. Concussion policy statements can be developed to include: • The school or league's commitment to safety • A brief description of concussion • Information on when athletes can safely return to school
and play.
Parents and athletes should sign the concussion policy statement at the beginning of the season.
"WHEN IN DOUBT, SIT THEM OUT!"
[ INSERT YOUR LOGO J

Field Safety Checklist
Field Conditions
Backstop Repair
Home Plate Repair
Bases
Pitcher's Mound
Batter's Box Level
Batter's Box Marked
Grass Cut
Holes In Field
Outfield Fence Repair
Foul Lines Marked
Dirt Needed
Dugouts
Fences Broken
Bench Needs Repair
Roof Needs Repair
Trash Cans In Place
Clean Up Needed
Safety Equipment
Catcher's Equipment Safe
Helmets Safe
Protective Wear Safe
Jewelry Removed
Bats Inspected
Shoes Checked
First Aid Kits In Place and Complete
Problem:
Circle the problem area, write a brief description of repair that is needed and
submit to Safety Officer or League President.

Regular Season Pitching Rules - Baseball
VI - PITCHERS
(a) Any player on a regular season team may pitch. {NOTE: There is no limit to the number
of pitchers a team may use in a game.)
(b) A pitcher once removed from the mound cannot return as a pitcher. Junior, Senior, and Big League
Divisions only: A pitcher remaining in the game, but moving to a different position, can return as a
pitcher anytime in the remainder of the game, but only once per game.
(c) The manager must remove the pitcher when said pitcher reaches the limit for his/her age
group as noted below, but the pitcher may remain in the game at another position:
League Age 1 7-18 105 pitches per day
13 -16 95 pitches per day
11 -12 85 pitches per day
9-10 75 pitches per day
7-8 50 pitches per day
Exception: Exception: If a pitcher reaches the limit imposed in Regulation VI (c) for
his/her league age while facing a batter, the pitcher may continue to pitch until any one
of the following conditions occurs: 1. That batter reaches base; 2.That batter is put out;
3. The third out is made to complete the half-inning. Note 1: A pitcher who delivers 41
or more pitches in a game cannot play the position of catcher for the remainder of
that day.
(d) Pitchers league age 14 and under must adhere to the following rest requirements:
• If a player pitches 66 or more pitches in a day, four (4) calendar days of rest must
be observed.
• If a player pitches 51 - 65 pitches in a day, three (3) calendar days of rest must be
observed.
• If a player pitches 36 - SO pitches in a day, two (2) calendar days of rest must be
observed.
• If a player pitches 21- 35 pitches in a day, one (1) calendar days of rest must be
observed.
• If a player pitches 1-20 pitches in a day, no (0) calendar day of rest is required.
Pitchers league age 15-18 must adhere to the following rest requirements:
• If a player pitches 76 or more pitches in a day, four (4) calendar days of rest must
be observed.
• If a player pitches 61 - 75 pitches in a day, three (3) calendar days of rest must be
observed.
• If a player pitches 46 - 60 pitches in a day, two (2) calendar days of rest must be
observed.
• If a player pitches 31 -45 pitches in a day, one (1) calendar days of rest must be
observed.
• If a player pitches 1-30 pitches in a day, no (0) calendar day of rest is required.
(e) Each league must designate the scorekeeper or another game official as the official pitch
count recorder.

(f) The pitch count recorder must provide the current pitch count for any pitcher when
requested by either manager or any umpire. However, the manager is responsible for
knowing when his/her pit ch er.must be removed.
(g} The official pitch count recorder should inform the umpire-in-chief when a pitcher has
delivered his/her maximum limit of pitches for the game, as noted in Regulation VI (c).
The umpire-in-chief will inform the pitcher's managerthatthe pitcher must be removed
in accordance with Regulation VI (c}. However, the failure by the pitch count recorder to
notify the umpire-in-chief,and/or the failure of the umpire-in -chief to notify the manager,
does not relieve the manager of his/her responsibility to remove a pitcher when that pitcher
is no longer eligible.
(h} Violation of any section of this regulation can result.in protest of the game in which it
occurs. Protest shall be made in accordance with Playing Rule 4.19.
(j} A player who has attained the league age of twelve (12) is not eligible to pitch in the Minor
league. (See Regulation V - Selection of Players)
(k) A player may not pitch iri more than one game in a day. (Exception: In the Big league
Division, a player may be used as a pitcher in up to two games in a day.)
NOTES:
1. The withdrawal of an ineligible pitcher after that pitcher is announced, or after a
warm-up pitch is delivered, but before that player has pitched a ball to a batter, shall
not be considered a violation. little League officials are urged to take precautions to
prevent protests. When a protest situation is imminent, the potential offender should
be notified immediately.
2. Pitches delivered in games declared "Regulation Tie Games" or "Suspended Games"
shall be charged against pitcher's eligibility.
3. In suspended games resumed on another day, the pitchers of record at the time the
game was halted may continue to pitch to the extent of their eligibility for that day,
provided said pitcher has observed the required days of rest.
Example 1: A league age 12 pitcher delivers 70 pitches in a game on Monday when
the game is suspended. The game resumes on the following Thursday. The pitcher is
not eligible to pitch in the resumption of the game because he/she has not observed the
required days of rest.
Example 2: A league age 12 pitcher delivers 70 pitches in a game on Monday when the •
game is suspended. The game resumes on Saturday. The pitcher is eligible to pitch up to
85 more pitches in the resumption of the game because he/she has observed the required
days of rest.
Example 3: A league age 12 pitcher delivers 70 pitches in a game on Monday when the
game is suspended. The game resumes two weeks later. The pitcher is eligible to pitch
up to 85 more pitches in the resumption of the game, provided he/she is eligible based
on his/her pitching record during the previous four days.
Note: The use of this regulation negates the concept of the "calendar week" with regard
to pitching eligibility.
cu

Regulation VI (d) has been amended to read, in part:
Applies to: Baseball & Challenger Rule Books
EXCEPTION: If a pitcher reaches a day(s) ofrest threshold while facing a batter, the
pitcher may continue to pitch until any one of the following conditions occurs: I. That
batter reaches base; 2. That batter is retired; 3. The third out is made to complete the half
inning. The pitcher will only be required to observe the calendar day(s) of rest for the
threshold he/she reached during that at-bat, provided that pitcher is removed before
delivering a pitch to another batter.
Summary and Implementation: For the 2013 season, wording was revised allowing a
pitcher who reaches his/her imposed days of rest threshold while facing a batter to
continue to pitch until the current batter has been retired or reaches base.

Regulation VI (d) has been amended to read, in part:
Applies to: Baseball & Challenger Rule Books
E.XCEYf'IUN: lf a pitcher reaches a day(s) of rest threshold while facing a bart.er, the
pitcher may continue to pitch until any one of the following conditions occurs: 1. That
batter reaches base; 2. That batter is retired; 3. The tlilid out is made to complete the half
inning. The pitcher will only be required to observe the calendar day(s) ofrest for the
threshold he/she reached during that at-bat, provided that pitcher is removed before
delivering a pitch to another batter.
Summary and Implementation: For the 2013 season, wording was revised allowing a
pitcher who reaches his/her imposed days of rest threshold while facing a batter to
continue to pitch until the current batter has been retired or reaches base.
Tournament Rule 4(e) has been amended to read, in part:
Applies to: Baseball Rule Book
EXCEPTION: If a pitcher reaches the limit imposed above for his/her league age whiie
facing a batter, the pitcher may continue to pitch until any one of the following conditions
occurs: l. 1 hat bar..er reaches base; 2. rnat barter is retired; 3. The third out is made to
complete the half-inning. The pitcher will only be required to observe the calendar day(s)
of rest for the threshold he/she reached during that at-bat, provided that pitcher is
removed before delivering a pitch to another batter.
Summary and Implementation: For the 2013 International Tournament, revised
wording allowing a pitcher who reaches his/ her imposed days of rest threshold while
facing a batter to continue to pitch until the current batter has been retired or reaches base.

PITCHING
PITCH COUNT
Pitch count does matt er. Remember, in the major leagues, a pitcher is
removed after approximately 100 pitches. .A child cannot be expected
to perform like an adult! Little League managers and coaches are
usually quick to teach their pitchers how to get movement on the qall.
Unfortunately the technique that older players use is not appropriate
for children thirteen (13) years and younger. The snapping of the arm
used to develop this technique will most probably lead to serious
injuries to the child as he/she mat ures.
Arm stress during the acceleration phase of throwing affects both
the inside and the outside of the growing elbow. On the inside, the
structures are subjected to distraction f or ces, causing them to pull
apart . On the outside, the forces are compressive in nature with
different and potentially more serious consequence. s
The key structures on the inside (or medial) aspect of the elbow
include the tendons of the muscles that allow the wrist to flex and the
growth plate of the medial epicondyle ("Knobby" bone on the inside of
the elbow). The forces generated during throwing can cause this
growth plate to pull away (avulse) from the main bone. If the distance
between the growth plate and main bone is great enough, surgery is
the only option to fix it.
This growth plate does not fully adhere to the main bone until age 15!
Similarly, on the outside (or lateral) aspect of the elbow,the two bony
surfaces can be damaged by compressive forces during throwing. This
scenario can lead to a condition called Avascular Necrosis or Bone Cell
Death as a result of compromise of the local blood flow to that area.
'· '-. ,/

,,.-.._,
·, ;t . \, , ./
This disorder is permanent and often leads to fragments of the bone
breaking away (loose bodies) which float in the joint and can cause
early arthritis. This loss of elbow motion and function often
precludes further participation.
Studies have demonstrated that curveballs cause most problems
at the inside of the elbow due to the sudden contractive forces
of the wrist musculature. Fastballs, on the other hand, place more
f or ce· at the outside of the elbow. Sidearm delivery, in one study,
fed to elbow injuries in 74% of pitchers compared with 27% in
pitchers with a vertical delivery st yle.
Dr . Glenn Fleisig at the American Sports Medicine Institute is
· in the process of finalizing the results of a study funded by
USA Baseball that evaluated pitch counts in skeletally
immature athletes as they relate to both elbow and shoulder
inj uries. The study included 500 athletes, ages 9-14, from the
Birmingham, Alabama area. Each child who pitched in a game
was called after the game and interviewed over the phone. The
investigators were able to conduct over 3000 interviews.
Approximately 200 of the 500 pitchers had videotape of their
mechanci s.
PRELIMINARY DATA HAVE DEMONSTRATED THE FOLLOWING:
1) A significantly higher risk of elbow injury occurred after
pitchers reached 50 pitches/outing.
2) A significantly higher risk of shoulder injury occurred
after pitchers reached 75 pitches/outing.
3) In one season, a total of 450 pitches or more led to
cumulative injury to the elbow and the shoulder .
4) The mechanics, whether good or bad, did not lead to an
increased incidence of arm injuries.
5) The preliminary data suggest that throwing curveballs
increases risk of injury to the shoulder more so than the
elbow: however, subset analysis is being undertaken to
investigate whether or not the older children were the
pitchers throwing the curve.
6) The pitchers who limited their pitching repertoire to the
fastball and change-up had the lowest rate of injury to
their throwing arm.
7) A slider increased the risk of both elbow and shoulder
problems.
Based on the data, a recommendation can be made to reduce the
number of pitches per outing to 50-60 for the 8-12 age groups
and 50-75 for the 13 and 14 year olds.
If a curveball is taught, the Manager should instruct the child to
throw the curveball like a football without snapping the arm or
the wrist. Once these pitch counts are reached, we recommend
replacing the pitcher. Should that player be inserted back into
the lineup, we recommend against the position of catcher as the
number of throws required mirrors that of the pitcher.
Children should not be encouraged to· ''play through pain." Pain
is a warning sign of injury. Ignoring it can lead to greate

.,,,.--.. CUrveballs, Catchers and Fatigue
Research needs to continue on
links between overuse injuries and
two hottest topics.
New research suggests that curveballs
aren't as dangerous as some in the
medical field have suggested, with
stresses similar between the curveball
and fastball. But let's not be so quick
to accept curveballs for youngsters,
warns Dr. James Andrews,
orthopaedic surgeon and baseball
injuries researcher. Add to that
concern that catchers are joining
the growing trend of patients
seeing orthopaedic
surgeons needing
to repair their
injured arms.
Dr. Andrews stated
that while the most
recent studies "can't
show in the lab that the
curveball causes more
damage" than the
fastball or other
pitches, he does
not advocate
teaching or
throwing
curveballs
until a
player's arm
is close to
fully
developed,
at age
13 to 15.
Fatigue Still the Key Risi< ''We still believe the two major
pitches to throw... are the fastball and
the change-up," Dr. Andrews said.
"My personal opinion is fatigue is ...
the highest risk factor in youth
baseball related to injuries. If you can
prevent fatigue, then you will have
done 95% of what you can do to keep
these kids healthy."
"So how does the curveball interact
with fatigue? If you are playing
competitively... they want to win, and
the curveball is a major factor" in winning games, Dr. Andrews said.
"Fatigue comes from the inability of a
young player to throw the curveball
properly with good mechanics. That's
the whole key."
Dr. Andrews stated he does not call
curveballs "safe" for younger players.
"However, if you throw the curveball
with good mechanics, there are no
greater forces on the shoulder or
elbow than throwing the fastball,
apparently, from what we can
measure in the lab."
He also explained that throwing a
curveball requires a great deal of
control, and "is not an easy pitch to
throw, and certainly not everyone can
throw it properly."
Teach Proper Curveball Mechanics And teaching good curveball
mechanics is important, no matter
what age, he said. "Do we have
knowledgeable coaches teaching these
kids the curveball?" Dr. Andrews
asked. ''We' ve got to be really
careful. When you put a kid in
a competitive situation, a
championship series, and call
for 70% curveballs, what's
that going to do to the fatigue
factor? Remember, it's a highly
neurologically controlled pitch: if
the mechanics get off because
you' re fatigued, and throwing 70% curves, then we' re in trouble. So be
careful throwing curveballs."
Dr. Andrews repeated the caution
from the position statement, that
"throwing curveballs too early may
be counterproductive, leading to arm
fatigue as well as limiting the youth's
ability to master fastball mechanics,"
he said. ''Intheory, don't throw
curves till you can shave."
Catchers at Increasing Risk When the most talented and athletic
players are catchers, a coach's
natural desire is to make that player a
pitcher, too. But Dr. Andrews warned
that catchers, good catchers who are
mirroring every throw from the
pitcher as well as being asked to
throw long, fast, accurate throws to
first, second and third bases are at
increased risk of arm fatigue and
subsequent injury.
' 'We're seeing a lot of injuries with
catchers. I had a catcher come in
from Atlanta, and I did surgery on
him. I asked him how he got hurt.
He's 15 years of age, and he's not
supposed to have an injury [at that
age]; but believe me, they're out
there all over the place in that age
group," Dr. Andrews stated.
He said the player was at a showcase
and was asked to throw 100 throws
in 200 seconds. Throwing a ball from
home to second in 2 seconds is a
good throw; and the organizers were
timing the catchers on the total they
could throw down in 200 seconds.
"So he would throw as hard as he
could throw, and then reach and
they'd put a ball in his hand and do it
again, to see how he fell off, what
kind of stamina he had," Dr.
Andrews related. "And about the 50th
throw, he tore his ligament.
" Now that particular situation was
almost criminal, and unfortunately
what might happen down the road is
it might become a criminal offense,"
he added. "So the timing is right to
get this under control, before the
fedt:ral courts and tht: statt: courts
and the lawyers get it under control."

Youth Baseball Pitching Study Shows Overuse is
Primary Cause of Arm Injuries
No Proof Curve Balls are More Dangerous than Other
Pitches
By Communications Division
SOUTH WILLIAMSPORT, Pa.
August 3, 2011
A five-year study, recently concluded by the Department of Exercise and Sport Science at
the University of North Carolina, found that the primary cause of arm injuries in youth
baseball players was overuse. It also failed to show an increased risk of arm injury due to
breaking pitches, such as curve balls.
"Some within the baseball community have advocated for a ban on curveballs," Stephen
D. Keener, President and Chief Executive Officer for Little League Baseball and Softball,
said. "However, the study conclusions do not clearly support such a ban.
"Furthermore, a ban on breaking balls would not be simple to put into practice," Mr.
Keener said. "With such a wide range of aptitude and ability, it's practically impossible
to judge if any youth pitcher intended to throw a curveball or if that's just how the ball
came out of the pitcher's hand. To task our dedicated volunteers with judging the type of
pitch thrown is not only unfair, it would be impractical."
Little League Baseball and Softball, the largest youth sports organization in the world, in
collaboration with USA Baseball, the governing body of amateur baseball in the United
States, and the Department of Exercise and Sport Science at the University of North
Carolina in Chapel Hill, conducted the study of pitching arm injuries in youth baseball.
Funding for the five-year study, which begin in 2006, was provided through a grant from
the Yawkey Foundations.
"We are proud to support this study and recognize the need to further our understanding
of the causes of arm injuries in youth baseball and the importance of protecting the health
and wellbeing of its players," James Healey, President of the Yawkey Foundations, said.
"Little League's ability to provide healthy opportunities for youth is important to the
future of the sport and the Yawkey Foundations are pleased to be involved."
An extensive overview of the study can be found at the Little League International web site at: http://www.littleleague.org/Assets/forms pubs/media/UNCStudy.pdf.

The aim of the study, the first substantive research done in this area, was to describe the
incidence and prevalence of pitching arm injuries and examine the risk factors.
The study used three different test groups - Little League pitchers (ages 8-13); high
school-aged pitchers; and college-aged pitchers. The Little League test group consisted of
410 players who were followed for four years between 2006 and 2010. The test group
from the high school level was made up of 293 players who were recruited in 2007 and
followed for additional years. The college test group consisted of 629 players that were
followed for two years beginning in 2008.
The pitchers were surveyed each year to assess their pitching methods, techniques, pain
presence and injury occurrence. The factors acquired from the surveys were then
analyzed to assess which of those factors influenced pitching injury risk.
The study produced several findings including the following: 1. The relationship between
age, type of pitch and injury risk is complex, but there was no clear evidence that
throwing breaking pitches at an early age was an injury risk factor; and; 2. The data
showed the primary cause of arm injuries is overuse, not the type of pitch.
The study's principal investigators were: Frederick 0. Mueller, Ph.D., Dept. of Exercise
and Sport Science, University ofNorth Carolina; Stephen W. Marshall, Ph.D.,
Department of Epidemiology, University ofNorth Carolina; and the late Dr. Barry
Goldberg, a former member of the Little League International Board of Directors, and
Director of Sports Medicine for Yale University's Health Services, who championed this
study.
In 2008, Little League Baseball became the first national youth baseball organization to
adopt the pitch count, instead of the number of innings pitched, as the basis for its
pitching rules.
"Even if Little League were to find a practical way to ban curveballs in our program, they
would remain a part of the game for children playing outside our program, as they have
been for decades," Mr. Keener, a Little League graduate, said. "For coaches and parents,
armed with the information in this report, the decision on when and how to teach the
curveball is a matter of preference and education."
Little League has relied on the expert advice and counsel of Dr. James Andrews, Founder
and Medical Director of the American Sports Medicine Institute (ASMI); and Dr. Glenn
Fleisig, Research Director at ASMI for the development of its groundbreaking pitch
count rules. Dr. Andrews, who currently serves on the Little League International Board
of Directors, and Dr. Fleisig are two of the world's most knowledgeable and respected
authorities on pitching injuries.

When should you teach youth pitchers how to throw
a curveball?
Posted on September 21, 2012 by coachdeck
By Dan Gazaway, Owner of The Pitching Academy
This has been a debatable topic for many years now and there are many theories as to
when a youth pitcher should learn how to throw a curveball. The fact is that there is no
magical age to start teaching the pitch. Here is my take on youth pitchers who learn how
to throw a curveball .
First and foremost, a pitcher should not mess around with any other pitch until they learn
proper fastball mechanics. When one of my pitchers can throw a decent fastball, the first
pitch I will teach them is an effective changeup. Change of speed and location (hitting
your spots) is important and before a pitcher reaches the high school level he can be very
successful with just two pitches; if they are great pitches of course.
There are many dangers if youth pitchers don't understand a few key points about
throwing the curveball. Here are a few of them:
• They don't know how to throw a curveball properly.
• They fall in love with the pitch, because they have found success with it and they
tend to overuse it. A curveball, even at the major league level, should not be
thrown more than 20% of the time.
• The curveball, regardless if it is thrown correctly, will put more stress on your
throwing arm than a fastball because of wrist and forearm angle at the release of
the pitch.
• Youth pitchers who have not hit puberty haven't developed enough in their bones
and connective tissues like tendons and ligaments that help support larger muscle
groups; therefore, increasing the risk of injury.
• Youth pitchers hands and fingers are short so most of them have problems with
the pitching grip affecting the proper release of the baseball which can also lead to
IIlJUiy.
What is the solution? Educate yourself on the proper mechanics of the
curveball. Understand the risks that are associated with the curve. Also, don't be too
hesitant to teach the curveball; it is a very effective pitch to have in your arsenal. If you
wait too long to learn the curveball, you may not have time to throw a "great" curveball.
Teach the proper pitching grip first, then wrist and forearm angle at release of the
baseball. It is important not to teach a pitcher that they have to snap or twist their wrist a
certain way at release of the baseball.
I have all of my pitchers practice gripping and throwing the curveball on their knees,
throwing the pitch to a net much closer than they would off a mound. You reduce the

risk of injury this way because you have taken the momentum out of the pitch (they are
not exploding to foot strike). This way, with the knee drill, they will be able to throw
more curveballs, learning the pitch much faster than they would throwing off a mound or
on their feet on flat ground. In conclusion, before you learn how to throw a curveball,
learn proper pitching mechanics first.
Dan Gazaway is Owner and Founder of The Pitching Academy
(yvww.thepitchingacademy.net). He has instructed over 2,000 pitchers in the last seven
years and received a Bachelor's Degree as a Health Education Specialist at Utah State
University. He is a motivational speaker for topics ranging from attitude, goal-setting
and leadership and be contacted at [email protected].

G---.1 LITTLE LEAGUE® BASEBALL AND SOFTBALL
ACCIDENT NOTIFICATION FORM _ INSTRUCTIONS
Accident & Health (U.S.)
1. This form must be completed by parents 0f claimant is under 19 years of age) and a league official and forwarded to Little League
Headquarters within 20 days after the accident. A photocopy of this form should be made and kept by the claimant/parent. Initial medical/
dental treatment must be rendered within 30 days of the Little League accident.
2. Itemized bills including description of service, date of service, procedure and diagnosis codes for medical services/supplies and/or other
documentation related to claim for benefits are to be provided within 90 days after the accident date. In no event shall such proof be
furnished later than 12 months from the date the medical expense was incurred.
3. 1/Vhen other insurance is present, parents or claimant must forward copies of the Explanation of Benefits or Notice/Letter of Denial for
each charge directly to Little League Headquarters, even if the charges do not exceed the deductible of the primary insurance program.
4. Policy provides benefits for eligible medical expenses incurred within 52 weeks of the accident, subject to Excess Coverage and
Exclusion provisions of the plan.
5. Limited deferred medical/dental benefits may be available for necessary treatment incurred after 52 weeks. Refer to insurance brochure
provided to the league president, or contact Little League Headquarters within the year of injury.
6. Accident Claim Form must be fully completed - including Social Security Number (SSN) - for processing.
League Name
N ame of Injured Person/Claimant SSN
PART 1
League I.D.
I Date of Birth (MM/DD/YY) Age Sex
I I I D Female
D Male
Name of Parent/Guardian, if Claimant is a Minor Home Phone (Inc. Area Code) Bus. Phone (Inc. Area Code)
( ) ( )
Address of Claimant Address of Parent/Guardian, if different
----=ie Little League Master Accident Policy provides benefits in excess of benefits from other insurance programs subject to a $50 deductible r injury. "Other insurance programs" include family's personal insurance, student insurance through a school or insurance through an
..,mployerfor employees and family members. Please CHECK the appropriate boxes below. If YES, follow instruction 3 above.
Does the insured Person/Parent/Guardian have any insurance through: Employer Plan □Yes □No School Plan □Yes □No
Individual Plan OYes □No Dental Plan □Yes □No
Date of Accident Time of Accident Type of Injury
DAM □PM!
Describe exactly how accident happened, including playing position at the time of accident:
Check all applicable responses in each column:
D BASEBALL D CHALLENGER (4-1 8) □ PLAYER D D SOFTBALL □ T-BALL (4-7) □ MANAGER, COACH D
TRYOUTS
PRACTICE
□ SPECIAL EVENT (NOT GAMES)
D CHALLENGER □ MINOR (6-12 ) □ VOLUNTEER UMPIRE D
0 TAD (2ND SEASON) D LITTLE LEAGUE(9-12) D PLAYER AGENT 0 0 INTERMEDIATE (50/70) (11-13) 0 OFFICIAL SCOREKEEPER 0
□ JUNIOR (12 -1 4) D SAFETY OFFICER D
□ SENIOR (13 -16) D VOLUNTEER WORKER D
D BIG (14-18)
SCHEDULED GAME □ TRAVEL TO
TRAVEL FROM
TOURNAMENT
OTHER (Describe)
SPECIAL GAME(S) (Submit a copy of your approval from Little League Incorporated)
I hereby certify that I have read the answers to all parts of this form and to the best of my knowledge and belief the information contained is
complete and correct as herein given.
I understand that it is a crime for any person to intentionally attempt to defraud or knowingly facilitate a fraud against an insurer by
submitting an application or filing a claim containing a false or deceptive statement(s). See Remarks section on reverse side of form.
I hereby authorize any physician, hospital or other medically related facility, insurance company or other organization, institution or person
that has any records or knowledge of me, and/or the above named claimant, or our health, to disclose, whenever requested to do so by Little League and/or National Union Fire Insurance Company of Pittsburgh, Pa. A photostatic copy of this authorization shall be considered
effective and valid as the original.
.1te Claimant/Parent/Guardian Signature (In a two parent household, both parents must sign this form.)
Date Claimant/Parent/Guardian Signature
Send Completed Form To: Little League® International 539 US Route 15 Hwy, PO Box 3485 Williamsport PA 17701-0485 Accident Claim Contact Numbers: Phone: 570-327-1674 Fax: 570-326-9280
-A1 - J

□ □ □
□ □ □ □ □ □
For Residents of California: Any person who knowingly presents a false or fraudulent claim for the payment of a loss is guilty of a crime and may be subject to fines and confinement in state prison.
For Residents of New York:
.,..-4..,;iy person who knowingly and with the intent to defraud any insurance company or other person files an application for insurance or tement of claim containing any materially false information, or conceals for the purpose of misleading, information concerning any
ct material thereto, commits a fraudulent insurance act, which is a crime, and shall also be subject to a civil penalty not to exceed five thousand dollars and the stated value of the claim for each such violation.
For Residents of Pennsylvania: Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance or statement of claim containing any materially false information or conceals for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime and subjects such person to criminal and civil penalties.
For Residents of All Other States: Any person who knowingly presents a false or fraudulent claim for payment of a loss or benefit or knowingly presents false information in an application for insurance is guilty of a crime and may be subject to fines and confinement in prison.
Name of League
PART 2 - LEAGUE STATEMENT (Other than Parent or Claimant)
Name of Injured Person/Claimant League I.D. Number
Name of League Official Position in League
Address of League Official Telephone Numbers (Inc. Area Codes) Residence: ( ) Business: ( ) Fax: ( ) □ □
Provide names and addresses of any known witnesses to the reported accident.
--"-1-teck the boxes for all appropriate items below. At least one item in each column must be selected.
OSITION WHEN INJURED
01 1ST 02 2ND 03 3RD 04 BATTER 05 BENCH 06 BULLPEN 07 CATCHER 08 COACH 09 COACHING BOX
10 DUGOUT 11 MANAGER 12 ON DECK 13 OUTFIELD 14 PITCHER 15 RUNNER 16 SCOREKEEPER 17 SHORTSTOP 18 TO/FROM GAME 19 UMPIRE
20 OTHER 21 UNKNOWN 22 WARMING UP
INJURY
01 ABRASION 02 BITES 03 CONCUSSION 04 CONTUSION 05 DENTAL 06 DISLOCATION 07 DISMEMBERMENT 08 EPIPHYSES 09 FATALITY 10 FRACTURE 11 HEMATOMA 12 HEMORRHAGE 13 LACERATION 14 PUNCTURE 15 RUPTURE 16 SPRAIN 17 SUNSTROKE 18 OTHER 19 UNKNOWN
20 PARALYSIS/ PARAPLEGIC
PART OF BODY □ 01 ABDOMEN □ 02 ANKLE □ 03 ARM
□ 04 BACK □ 05 CHEST □ 06 EAR □ 07 ELBOW □ 08 EYE □ 09 FACE □ 10 FATALITY □ 11 FOOT □ 12 HAND □ 13 HEAD □ 14 HIP
□ 15 KNEE □ 16 LEG □ 17 LIPS □ 18 MOUTH □ 19 NECK □ 20 NOSE □ 21 SHOULDER □ 22 SIDE □ 23 TEETH □ 24 TESTICLE □ 25 WRIST □ 26 UNKNOWN □ 27 FINGER
CAUSE OF INJURY 01 BATTED BALL
□ 02 BATTING □ 03 CATCHING
□ 04 COLLIDING D 05 COLLIDING WITH FENCE
06 FALLING 07 HIT BY BAT 08 HORSEPLAY 09 PITCHED BALL 10 RUNNING 11 SHARP OBJECT
□ 12 SLIDING □ 13 TAGGING □ 14 THROWING
□ 15 THROWN BALL D 16 OTHER D 17 UNKNOWN
Does your league use batting heimets with attached face guards? DYES □NO
_.. YES , are they □Mandatory or □Optional At what levels are they used?
,ereby certify that the above named claimant was injured while covered by the Little League Baseball Accident Insurance Policy at the time of the reported accident. I also certify that the information contained in the Claimant's Notification is true and correct as stated, to the best of my knowledge.
Date League Official Signature
□ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □
□ □ □ □ .□ □ □ □ □ □ □ □ □ □ □ □ □ □ □

little League® Baseball & Softball
CLAIM FORM INSTRUCTIONS
WARNING - It is important that parents/guardians and players note that: Protective equipment cannot
prc:vent all injuries a player might receive while participating in baseball/softball
To expedite league personnel's reporting ofinjuries, we have prepared guidelines to nse as a checklist in completing
reports. It will save time -- and speed your payment of claims.
The National Unim Fire Insurance Company ofpittsbw-gh, Pa (NUFIC) Accident Master Policy acquired through
Little League® contains an "Excess Coverage Provisim" whereby all personal and/or group insw-ance shall be nsed
first
The Accident ClaimFormmnst be fiillycompleted, inclndmg a SocialSecurity Number, :fur processing
To help explain insw-ance coverage to parents/guardians refer to What Parents Should Know on the internet that
should be reproduced on your league's lettemead and distributed to parents/guardians of all participants at
registration time.
Ifiitjuries occur, initially it is necessary to determine whether claimant's parents/guardians or the claimant has other
insw-ance such as group, employer, Blue Cross and Blue Shield, etc., whlchpays benefits. (This in:rormationshould
be obtained at the time of registration prior to tryouts.) If such coverage is provided, the claim mnst be filed first
with1he primary company under which1he parent/guardian or claimant is insw-ed.
When filing a claim, all medical costs should be fiilly itemized and :rorwarded to Little Leagne International If no
other insurance is in eflect, a letter Jromthe parent/gnardian or claimant's employer explaining the lack of group or
employer insw-ance should accompany1he claim :form
The NUFIC Accident Policy is acquired by leagnes, not parents, and provides comprehensive coverage at an
a.:flordable cost Accident coverage is underwritten by NationalUnion Fire Insurance Company ofFittsburgh, a
Pennsylvania Insurance company, with its principalplace ofbnsiness at 175 Water Stteet, 181h Floor, New York,
NY 10038. It is currently authorized to transact business in all states and the District ofColumbia. NAIC Number
19445.This is a briefdescription of the coverage available under 1he policy. The policy will contain linritations,
exdusims, and termination provisions. Fulldetails of the coverage are contained in1he Poli:y. Ifthere are any
conilicts between this document and the Policy, the Policy shall govern
The current insurance rates would not be possible without yow- help in stressmg safety programs at the locallevel
The ASAP manual, League Safety Officer Program Kit, is recommended :for use byyour Safety Oflicer.
TREAJMENT OF DENTAL INJURIES
De:ferred Dental Treatment ror claims or injuries occurr:ingin 2002 and beyond:If the insured incurs Il!iury to solllld,
naturalteethand necessary treatment requires that dentaltreatment for that Il!iury must be postponed to a date more
than 52 weeks after the dateof the injurydue to, but not limited to, the physiological changes occurr:ing to an
insured who is a growing child, we will paythe lesserofthe maximum bene:fitof $1 ,500 .00 or1he reasonab1e
expense incurred ror the deferred dentaltreatment Reasonable expenses incurred for de:ferred dentaltreatment are
on]y covered ifthey areincurred on or before the insured's 23rd birthday. Reasonable Expenses incurred for
de:ferred root canaltherapy are on]y covered if they are incurred within I04 weeks after the date the Iiymyis
sustained.
CHECKLIST FOR PREPARING CLAIM FORM
1. Print or type all inrormation
2. Complete all portions of the claim form berore ma.iliog to our office.
3. Be sure1n include league name and league ID mmiber.
PART I - CLAIMANT, OR PARENT(S)/GUARDIAN(S), IF CIAIMANT IS A MINOR
1. The aduh c1aimaot or parent(s)/guardians(s) must signthis section, if the claimant is a minor.
2. Give the name and address of the Il!iured person, a1ong withthe name and address of the
parent(s)/guardian(s), if claimant is a minor.
3. Fillout all secti>ns, including check marks in the appropriate boxes ror all categories. Do not leave any
section blank. This will cause a delay in processing your claim and a copy of the claim form will be
returned to you for completion.
4. It is mandatory to forward inrormation on other insurance. Without that information there willbe a deJay in
processingyour claim If no insurance, written verification fromeach parent/spouse employer must be
submitted.
5. Be certainallnecessarypapersare attached 1n the cJaim.ronn. (See instruction3.) Only :itemized bills are
acceptab1e.
6. On dental claims, it is necessary to submit charges 1n the major medicaland dentalinsurance company of
the cJaimant, or parent(s)/guardian(s) if claimant is a minor. "Accident-relatedtreatment to whoJe, solllld, naturalteeth as a direct and independent result of an accident" must be stated on the form and bills. Please
forward a copy of the insurance company's response to Litt1e League International. Include the claimant ' s
name, Jeague ID, and year of the Il!iury on the rorm.
PART II - LEAGUE STATEMENT
1. This section must be fiUed out, signed and dated by the league official.
2. Fill out all section, s including check marks in the appropriate boxes for allcategories. Do not leave any
section blank. This will cause a delay in processing your claim and a copy of the claim form will be
returned to you for completion.
IMPORTANT: Noti:fication ofa claim shoul:I be filed withLittle League International within20 days ofthe incident for the current season

Applicable in Arizona
For your protection, Arizona law requires the following statement to appear on this form. Any person who knowingly
presents a false or fraudulent claim for payment of a loss is subject to criminal and civil penalties.
Applicable in Arkansas, Delaware, District of Columbia, Kentucky, Louisiana,
Maine, Michigan, New Jersey, New Mexico, New York, North Dakota, Pennsylvania,
South Dakota, Tennessee, Texas, Virginia and West Virginia
Any person who knowingly and with intent to defraud any insurance company or another person, files a statement of
claim containing any materially false information, or conceals for the purpose of misleading, information concerning
any fact, material thereto, commits a fraudulent insurance act, which is a crime, subject to criminal prosecution and
[NY: substantial] civil penalties. In DC, LA, ME, TN and VA, insurance benefits may also be denied.
Applicable in California
For your protection, California law requires the following to appear on this form: Any person who knowingly presents a false or fraudulent claim for payment of a loss is guilty of a crime and may be subject to fines and confinement in state prison.
Applicable in Colorado
It is unlawful to knowingly provide false, incomplete, or misleading facts or information to an insurance company for the purpose of defrauding or attempting to defraud the company. Penalties may include imprisonment, fines, denial of insurance, and civil damages. Any insurance company or agent of an insurance company who knowingly provides false, incomplete, or misleading facts or information to a policy holder or claimant for the purpose of defrauding or
attempting to defraud the policy holder or claimant with regard to a settlement or award payable from insurance proceeds shall be reported to the Colorado Division of Insurance within the Department of Regulatory Agencies.
Applicable in Florida and Idaho
Any person who Knowingly and with the intent to injure, Defraud, or Deceive any Insurance Company Files a
Statement of Claim Containing any False, Incomplete or Misleading information is Guilty of a Felony.*
* In Florida - Third Degree Felony
Applicable in Hawaii
For your protection, Hawaii law requires you to be informed that presenting a fraudulent claim for payment of a loss or benefit is a crime punishable by fines or imprisonment, or both.
Applicable in Indiana
A person who knowingly and with intent to defraud an insurer files a statement of claim containing any false, incomplete, or misleading information commits a felony.
Applicable in Minnesota
A person who files a claim with intent to defraud or helps commit a fraud against an insurer is guilty of a crime.
Applicable in Nevada
Pursuant to NRS 686A.291, any person who knowingly and willfully files a statement of claim that contains any false,
incomplete or misleading information concerning a material fact is guilty of a felony.
Applicable in New Hampshire
Any person who, with purpose to injure, defraud or deceive any insurance company, files a statement of claim containing any false, incomplete or misleading information is subject to prosecution and punishment for insurance fraud, as provided in RSA 638:20.
Applicable in Ohio
Any person who, with intent to defraud or knowing that he/she is facilitating a fraud against an insurer, submits an application or files a claim containing a false or deceptive statement is guilty of insurance fraud.
Applicable in Oklahoma
WARNING: Any person who knowingly and with intent to injure, defraud or deceive any insurer, makes any claim for
the proceeds of an insurance policy containing any false, incomplete or misleading information is guilty of a felony.
ACORD 3 (2006/02)
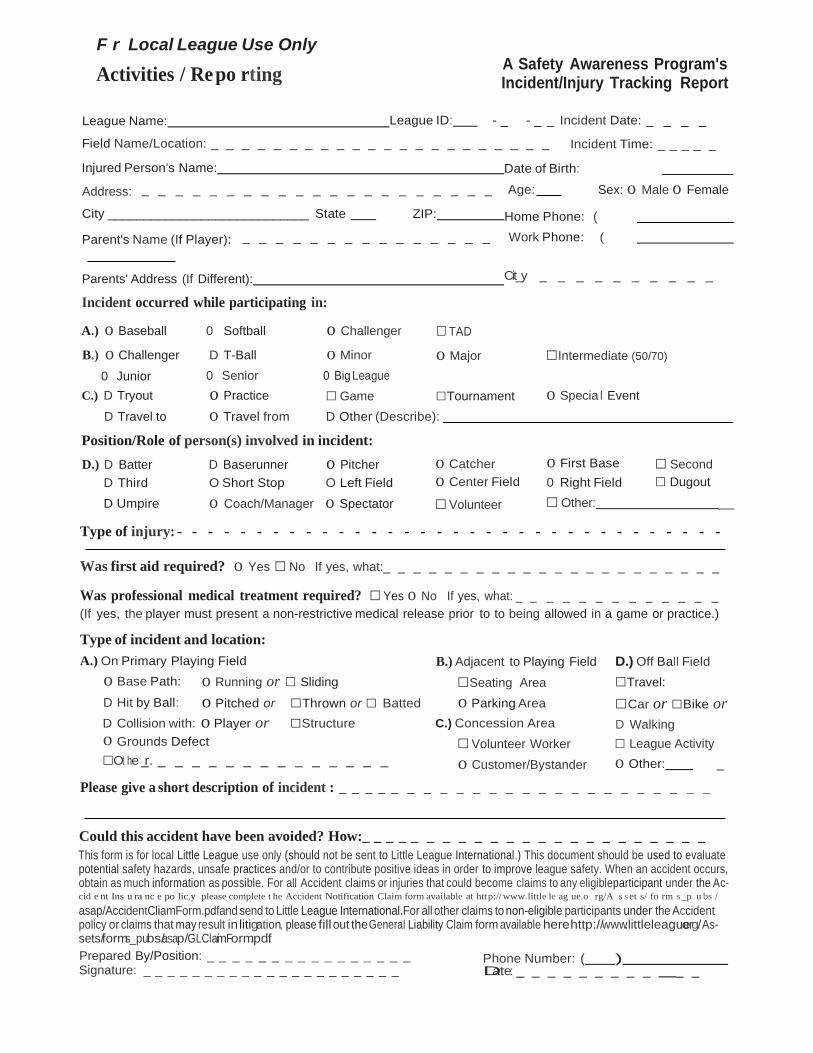
F r Local League Use Only A Safety Awareness Program's Incident/Injury Tracking Report
League Name: League ID: - _ - _ _ Incident Date: _ _ _ _
Field Name/Location: _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Incident Time: _ _ _ _ _
Injured Person's Name: Date of Birth:
Address: _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Age: Sex: o Male o Female
City ____________________________ State ZIP: Home Phone: (
Parent's Name (If Player): _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Work Phone: (
Parents' Address (If Different): Cit_y
Incident occurred while participating in:
A.) o Baseball 0 Softball o Challenger □ TAD
_ _ _ _ _ _ _ _ _ _
B.) o Challenger D T-Ball o Minor o Major □Intermediate (50/70)
0 Junior 0 Senior 0 Big League
C.) D Tryout o Practice □ Game □Tournament o Specia l Event
D Travel to o Travel from D Other (Describe):
Position/Role of person(s) involved in incident:
D.) D Batter D Baserunner o Pitcher
D Third O Short Stop O Left Field
o Catcher
o Center Field
o First Base
0 Right Field
□ Second
□ Dugout
D Umpire o Coach/Manager o Spectator □ Volunteer □ Other: _
Type of injury: - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
Was first aid required? o Yes □ No If yes, what:_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
Was professional medical treatment required? □ Yes o No If yes, what: _ _ _ _ _ _ _ _ _ _ _ _ _
(If yes, the player must present a non-restrictive medical release prior to to being allowed in a game or practice.)
Type of incident and location:
A.) On Primary Playing Field B.) Adjacent to Playing Field D.) Off Ball Field
o Base Path: o Running or □ Sliding
D Hit by Ball: o Pitched or □Thrown or □ Batted
D Collision with: o Player or □Structure
o Grounds Defect
□Ot he _r. _ _ _ _ _ _ _ _ _ _ _ _ _ _
□Seating Area
o Parking Area
C.) Concession Area
□ Volunteer Worker
o Customer/Bystander
□Travel:
□Car or □Bike or
D Walking
□ League Activity
o Other: _
Please give a short description of incident : _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
Could this accident have been avoided? How:_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
This form is for local Little League use only (should not be sent to Little League International.) This document should be used to evaluate potential safety hazards, unsafe practices and/or to contribute positive ideas in order to improve league safety. When an accident occurs, obtain as much information as possible. For all Accident claims or injuries that could become claims to any eligibleparticipant under the Ac cid e nt Ins u ra nc e po lic,y please complete t he Accident Notification Claim form available at htt p:// www.little le ag ue.o rg/A s s et s/ fo rm s _p u bs /
asap/AccidentCliamForm.pdfand send to Little League International.For all other claims to non-eligible participants under the Accident policy or claims that may result in litigation, please fillout theGeneral Liability Claim form available here: http://www.littleleagu.oerg/As sets/forms_pubs/asap/GLClami Form.pd.f
Prepared By/Position: _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Signature: _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
Phone Number: ( ) Date: _ _ _ _ _ _ _ _ _ _ _
Activities / Re po rting
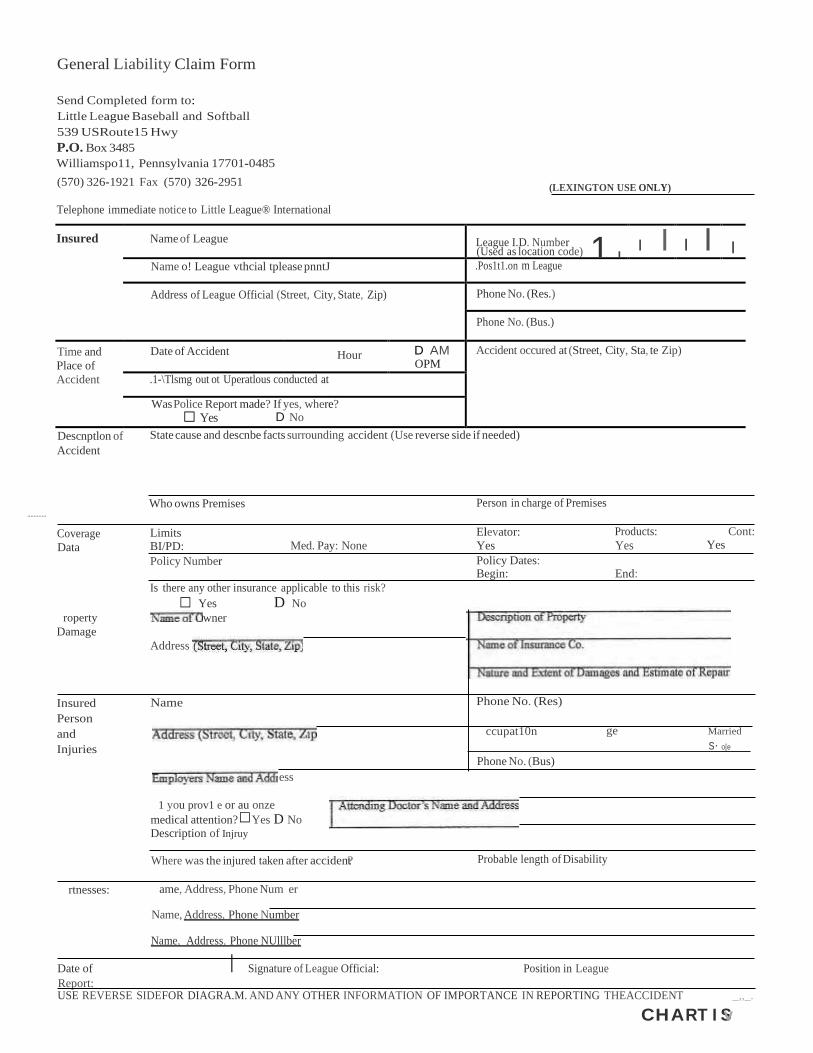
□
□
General Liability Claim Form
Send Completed form to:
Little League Baseball and Softball
539 USRoute15 Hwy
P.O. Box 3485
Williamspo11, Pennsylvania 17701-0485
(570) 326-1921 Fax (570) 326-2951 (LEXINGTON USE ONLY)
Telephone immediate notice to Little League® International
Insured Name of League League I.D. Number 1 I
(Used as location code) I I I I I Name o! League vthcial tplease pnntJ .Pos1t1.on m League
Address of League Official (Street, City, State, Zip) Phone No. (Res.)
Phone No. (Bus.)
Time and
Place of
Accident
Date of Accident Hour D AM OPM
Accident occured at (Street, City, Sta, te Zip)
.1-\Tlsmg out ot Uperatlous conducted at
Was Police Report made? If yes, where?
□ Yes D No
............
Descnptlon of
Accident
State cause and descnbe facts surrounding accident (Use reverse side if needed)
Who owns Premises Person in charge of Premises
Coverage
Data
Limits BI/PD: Med. Pay: None
Elevator:
Yes
Products:
Yes
Yes
Cont:
Policy Number Policy Dates: Begin: End:
roperty
Damage
Is there any other insurance applicable to this risk?
Yes D No
wner
Address
Insured
Person
and
Injuries
Name
ess
Phone No. (Res)
ccupat10n ge Married
s· o[e
Phone No. (Bus)
1 you prov1 e or au onze
medical attention? Yes D No Description of Injruy
Where was the injured taken after acciden?t
Probable length of Disability
rtnesses: ame, Address, Phone Num er
Name, Address, Phone Number
Name, Address, Phone NUlllber
Date of I Signature of League Official: Position in League
Report: USE REVERSE SIDEFOR DIAGRA.M. AND ANY OTHER INFORMATION OF IMPORTANCE IN REPORTING THEACCIDENT _,,_.
CHART I Sv

Little League. Baseball and Softball MEDICAL RELEASE
NOTE: To be carried by any Regular Season or Tournament
Team Manager together with team roster or International Tournament affidavit.
Player: _ Date of Birth: Gender (M/F):. _
Parent (s)/Guardian Name: Relationship: _
Parent {s)/Guardian Name: Relationship: _
Player's Address: City:. State/Country: Zip: _
Home Phone:. Work Phone.: Mobile Phone:. _
PARENT OR GUARDIAN AUTHORIZATION:
In case of emergencyr if family physician cannot be reached, I hereby authorize my child to be treated by Certified
Emergency Personnel. (i.e. EMT, First Responder, E.R. Physician)
Family Physician: _ Phone:
Address: City:. State/Country:. _
Hospital Preference:
Parent Insurance Co: Policy No.: Group ID#:
League Insurance Co.: Policy No.: League/Group ID#:. _
Ifparent(s)/guardian cannot be reached in case of emergency, contact:
Name Phone Relationship to Player
Name Phone Relationship to Player
Please list any allergies/medical problems'
including those requiring maintenance medication (i.e. Diabetic Asthma Seizure Disorder) ' '
Date of last Tetanus Toxoid Booster ----------------------------------------
Tpurpose of the above listed information is to ensure that medical personnel have details of any medical problem which may interfere with or alter treatment
Mr./Mrs./Ms.
Authorized Parent/Guardian Signature Date:
FOR LEAGUE USE ONLY:
league Name:. league ID.:
Division:. Team·.. Date:.
WARNING: PROTECTIVE EQUIPMENT CANNOT PREVENT ALL INJURIES A PLAYER MIGHT RECEIVE WHILE PARTICIPATING IN BASEBALL/SOFTBALL. Little League does not limit participation in its activities on the basis of dio;;;bi!ity, race, color; creed, natioria! origin, gender, sexu;;I preference or religious preference.
Medical Diagnosis Medication Dosage Frequency of Dosage

.........._
WARNING: Protective equipment cannot prevent all injuries a player might recejve while participating in
Baseball / Softball.
WHAT PARENTS SHOULD KNOW ABOUT LITTLE LEAGUE® INSURANCE
The Little League Insurance Program is designed to afford protection to all participants at the most economical
cost to the local league. The Little League Player Accident Policy is an excess coverage, accident only plan, to be used
as a supplement to other insurance carried under a family policy or insurance provided by an employer. If there is
no primary coverage, Little League insurance will provide benefits for eligible charges, up to Usual and Customary
allowances for your area. A $50 deductible applies for all claims, up to the maximum stated benefits.
This plan makes it possible to offer exceptional, affordable protection with assurance to parents that adequate
coverage is in force for all chartered and insured Little League approved programs and events.
If your child sustains a covered injury while taking part in a scheduled Little League Baseball or Softball game or
practice, here is how the insurance works:
1. The Little League Baseball and Softball accident notification form must be completed by parents (if the
claimant is under 19 years of age) and a league official and forwarded directly to Little League Headquarters
within 20 days after the accident. A photocopy of the form should be made and kept by the parent/claimant.
Initial medical/dental treatment must be rendered within 30 days of the Little League accident.
2. Itemized bills, including description of service, date of service, procedure and diagnosis codes for medical
---. services/ supplies and/or other documentation related to a claim for benefits are to be provided within 90 days
after the accident. In no event shall such proof be furnished later than 12 months from the date the initial
medical expense was incurred.
3. When other insurance is present, parents or claimant must forward copies of the Explanation of Benefits or
Notice/ Letter of Denial for each charge directly to Little League International, even if the charges do not
exceed the deductible of the primary insurance program.
4. Policy provides benefits for eligible medical expenses incurred within 52 weeks of the accident, subject to
Excess Coverage and Exclusion provisions of the plan.
5. Limited deferred medical/dentalbenefits maybe available for necessary treatment after the 52-week time limit when;
(a) Deferred medical benefits apply when necessary treatment requiring the removal of a pin /plate, applied to
transfix a bone in the year of injury, or scar tissue removal, after the 52-week time limit is required. The
Company will pay the Reasonable Expense incurred, subject to the Policy's maximum limit of $100,000 for any
one injury to any one Insured. However, in no event will any benefit be paid under this provision for any
expenses incurred more than 24 months from the date the injury was sustained.
(b) If the Insured incurs Injury, to sound, natural teeth and Necessary Treatment requires treatment for that
Injury be postponed to a date more than 52 weeks after the injury due to, but not limited to, the physiological
changes of a growing child, the Company will pay the lesser of: 1. A maximum of $1,500 or 2. Reasonable
Expenses incurred for the deferred dental treatment.
Reasonable Expenses incurred for deferred dental treatment are only covered if they are incurred on or before
the Insured's 23rd birthday. Reasonable Expenses incurred for deferred root canal therapy are only covered if
they are incurred within 104 weeks after the date the Injury occurs.
No payment will be made for deferred treatment unless the Physician submits wrinen certification, within 52
weeks after the accident, that the treatment must be postponed for the above stated reasons.
Benefits are payable subject to the Excess Coverage and the Exclusions provisions of the Policy.
We hope this brief summary has been helpful in providing a better understanding of the operation of the Little
League insurance program.
It is suggested this memo should be reproduced onyour league's letterhead over the signature of
your president or safety officer and distributed to the parents of allparticipants at registration time.
WEATHER
Rain: If it begins to rain: 1. Evaluate the strength of the rain. Is it a light drizzle or is it
pouring? 2. Determine the direction the storm is moving. 3. Evaluate the playing field as it becomes more and more saturated. 4. Stop practice if the playing conditions become unsafe -- use
common sense. If playing a game, consult with the other manager and the umpire to formulate a decision. ·
Lightning: The average lightning stroke is 6-8 miles long with up to 30 million volts at 100,000 amps flow in less than a tenth of a second. The average thunderstorm is 6-10 miles wide and moves at a rate of 25 miles per hour.
Once the leading edge of a thunderstorm approaches to within 10 miles, you are at immediate risk due to the possibility of lightning strokes coming from the storm's overhanging anvil cloud. This fact is the reason that many lightning deaths and injuries occur with clear skies overhead. On average, the thunder from a lightning stroke can only be heard over a distance of 3-4 miles, depending on terrain, humidity and background noise around you. By the time you can hear the thunder, the storm has already approached to within 3-4 miles!
The sudden cold wind that many people use to gauge the approach of a thunderstorm is the result of down drafts and usually extends
· less than 3 miles from the storm's leading edge. By the time you feel the wind, the storm can be less than 3 miles away!

If you can HEAR, SEE OR FEEL a THUNDERSTORM:
1. Suspend all games and practices immediately.
2. Stay away from metal including fencing and bleachers. 3. Do not hold metal bats.
4. Get players to walk, not run to their parent's or designated driver's cars and wait for your decision on whether or not to continue the game or practice.
First Aid
A person who has been struck by lightning does not carry an electrical charge that can shock other people. I fthe victim is burned, provide first and call emergency medical assistance immediately. Look for burns where lightning both entered and exited the body. If the strike has caused the victim's heart or breathing to stop, give cardiopulmonary resuscitation (CPR) until medical professionals arrive and take over.
Hot Weather:
Precautions must be taken in order to make sure the players on your team do not dehydrate or hyperventilate.
1. Suggest players take drinks of water when coming on and going off the field between innings.
2. If a player looks distressed while standing in the hot sun, substitute that player and get him/her into the shade of the dugout A.S.A.P.
3. If a player should collapse as a result of heat exhaustion, call 9-1-1
immediately. Get the player to drink water and use the instant ice bags supplied in your First-Aid Kit to cool him/her down until the emergency medical team arrives. (See section on Hydration)

Sometimes, the most important nutrient.children need is water
especially when they're physically active, their muscles generate
heat thereby increasing their body temperature. As their body
temperature rises, their cooling mechanism - sweat - kicks
in. When sweat evaporates, the body is cooled.
Unfortunately, children get hotter than adults during physical
activity and their body's cooling mechanism is not as efficient as
adults. If fluids aren't replaced, children can become overheated.
Thirst is not the only indicator of fluid needs. Therefore,
children must be encouraged to drink fluids even when
they don't feel thirsty. Managers and coaches should schedule
drink breaks every 15 to 30 minutes during practices on hot days,
and should encourage players to drink between every inning.
During any activity water is an excellent fluid to keep the body
well hydrated. Beverages high in carbohydrates like undiluted
fruit juice may cause stomach cramps, nausea and diarrhea when
the child becomes active. Caffeinated beverages {tea, coffee,
Colas} should be avoided because they are diuretics and can
dehydrate the body further. Avoid carbonated drinks, which
can cause gastrointestinal distress and may decrease fluid
volume.
WBliN111 5 HO'f, DIINK8ff0U YOU'RITHIRSff.

CONDITIONING & STRETCHING
Conditioning is an intricate part of accident prevention. Extensive studies on the effect of conditioning, commonly known as "warm
up, " have demonstrated that:
► The stretching and contracting of muscles just before an athletic activity improves general control of movements, coordination and alertness.
► Such drills also help develop the strength and stamina needed by the average youngster to compete with minimum accident exposure.
The purpose of stretching is to increase flexibility within the various muscle groups and prevent tearing from overexertion. Stretching should never be done forcefully, but rather in a gradual manner to encourage looseness and flexibility.
Hin
►ts on Stretching
Stretch necks, backs, arms, thighs, legs and calves.
Don't ask the child to stretch more that he or she
is capable of.
Hold the stretch for at least 10 seconds.
Don't allow bouncing while stretching. This tears down the muscle rather than stretching it.
Have one of the players lead the stretching exercises.
►Hints on Calisthenics
Repetitions of at least 10.
Have kids synchronize their movements.
Vary upper body with lower body.
Keep the pace up for a good cardio-vascular workout.
►
► ►
►
► ► ►

Suggestions for Warrr1- P Drills
Heel Cord Stretc.lie.s Lean up against a .wall.·Reach one teg behind you. Keep the knee $!Jajght, heel on the ground, and toes pointed forward. Slightly bend the leg that's closer to the wall. Lean forwar.d You should feel the stretch along the back of your calf. Repeat with the other1eg.
Shoulder Stretches # 1 Stand or sit. holding your throwing arm at the
wrist with your other hand. Put your arm over your head and pullgently, feeling your upper arm against your head. You should feel the stretch inside your shoulder.
Head and Neck Circles Make a circle with your head, going around first in one direction five times. Then reverse and make five circles inthe opposite direction.
Shoulder Stretches #2 Stand or sit, holding onto the elbow of your throwing arm with your other hand. Gently pull your throwing arm across yQur chest Youshould feelthe stretch inside your shoulder, especially at the back.
Low BQtk .$tretches Lie on your ba.ck,bnni{bt'ie !{nee up,and pullthe knee slowly toward your chest Hold and repeat three times. SWitch legs and repeat
Shoulder Stretches #3 Stand or sitwithyourpitching arm out tothe side and your elbow b;;nt, Move your arm back until you feel the stretch inthe front of your shoulder.
Thigh Stre tches # 1 Sit on the floor. Stretch both legs out in front of y.ou. Reach forwar,d touching your toes. Eventually, you want to lean forward far enough to put your head on you knees. You should feel the stretch along the backs of your legs.
Thigh Stretches #2 Siton tile floor with one legstretched out in front of you. Bend the other knee and put your foot behindyou. leanbackwards. You should feel the stretch along the front of your thigh.

Allergic Reactions Instruction Sheet Page I of I
/ ,.---..
'._(\ ) '-- · -- /
Signs and Symptoms: A-1itdJ..eactwn ♦ ik hlne-ss
• mild skin rednes$ or swelling
• sf\flfy, rvnny no:!!e
♦ sneet'mg
• itchy, watery ey,:,s
• red bumps {hiVesJ that occur anywhere on the bOdy
Severe Reaction • swelling of fh& foce ormoutll
• difficulty swoilo-wing or speaking
• whee.ting or difficulty breathing
• qb<fQll'linol paio, nqlJSeO, or vomiting
• diizlness or k.linmg
1. Contad a doet<>r If a child h<is <'.111 <'.>lletgie re<icllon that is more than mi1d oz ihe r.:,aellon eoncems you.
.2. II the child hos symptoms of a m.1d
reoclion, give an oral onlihlstamfne
such as dlphenhydramlne.
3. I! the child hossymptoms of <1 severe ollerglc re<lctton ond you hove injectable epinephrine, immedlotely use It os directed and eoll for eniergency help.
• h<ls any symptoms of o sever<> ol!.,rgie reaction
• was "xposed lo a food or subslonc,;· that hos higgered a severe reaciion in the past
• wasgiven lnjeclob!e epinephrine
··.:;r;,;.;::z:;_:}.<Sdikii;,}L t:!ii isiJ?ilff:-:(,J:6; i;;:;;:,-;;.0x:::, >;,;,·<iff
Think Prevention!
©1995-2005 The Nemours Foundation. All rights reserved.
KidsHealth www.KidsHeaith.org
http://kidshealth.org/parent/fustaid_safe/sheets/allergic_reaction_sheet.html 2/6/2005

=
Animal Bites Instruction Sheet Page I of I
/'//---,
\'·'\.. ) '
,; .·ti • nti•·$¢tQR tr1m break fue skin eon cau•lnfedion.
,11mely, animal bites(pollicula!ly from
wildanimals) con cause rabies, a ·.. dangerous, lite-threatening disease.
Bats, mccoons, skunks, and foxes transmit most
coses of mbles.
What to Do: l. Wash the area will! soop and water. ond <:1ppiy r.m,·ssvre wi!h sterile
gauze or a c: on cloth ii the ch d ls bleeding. (Do not <:1ppty on
antiseptic or onythTng else to the wound,)
.2. Cover any broken skln with a bQndoge or sterile gauze.
Seek emergency medical care if the child: • hos o bite !hat punctvred or broke the skin
• was biften by a wild or stray aru1nat or any animal that hasn't recently hod rabies shots or is acting slrangely
• was bitten on the face. neck. or hand, or near a joint
• has a blfe or scwkh !hat's becoming red, hot, swollen. or increasingly poinfol
• is behind on immunizations (Shots} or hasn't nod a recent t-etanus snot
When seeking t'reat'ment, have the following information on hand: • the k!nd of animal tllat bit thechild
• the dote of!he onllr.oi', last robies vacclnalion, If known
• any reeeni unu a! b-ehaviof' b*f th4;¼ animal
• !he <1nlma!'s bcolion {address, if known}
• iffhe animal w<:as wi1d or 1;1 sfroy, or w<1s coplured by a local <1nimal ;;;onirol service
• lhe chik:l's lmmuniz1;11lon (shois) record
··.· 'Many anlrnal biles am preventabk>. Always sl.lp(,!Vise young t:hlldren around dnlmals, even ,:,;::::;::!°"'them.Abo :: r,.::.·.i,..;,.:•····'..'.·.-.:•.·...·.'..",'·,·"······· ; ::, Id:; :V'!:
tostay
t,,._".,
·;·
.;'.
'Nole-: All lnformallon Islot &dui::aflcnol i,ucpooes emy.Foupei::ille -diealadvke; dlagnoset;· and ir<!<llmenl, consult a doctor. Re-view !his will, a doctor p,lorto us&.
teviewe-d by: Kato Cronan MD Dffle- t&vfewedi Nove:mbt!r 2003
P::fr,;1°:·_v11-.:;:;::<-1r/6:: <,): xer::s;:x:>k:,:.;r\11%1?@2%As+t.4;;½fiiS.J' ©1995-2005 The Nemours Foundation. All rights reserved.
KidsHealth
www.KidsHealth.org
http://kidshealth.org/parent/firstaid_safe/sheets/animal_bites_sheet.html 2/6/2005

Broken Bones Instruction Sheet Page 1 of 1
WhattoOo:
The chifd may have a broken a bone if:
• you QI' the child heard ,:i
"'snap" or o gt!ndlng noise during !he
lnli.ll'Y
• !here is swl;'ffing, bruising, lendemess. v1·
a le;;llng ol "pins <1nd needies"
• it's p,::=inM lo beot weigh! en !he inj,;,ed
&ea "" to move l!
1. Remove clolhing from lhe 1niur;;d part.
2:. Awly a cold compress« Ice pack wrapped in cloth.
3. l'kx<> a spfint on the injured p<nt by:
• keeping the injured limb in the poSiffon you !Ind ii
• placing soft poddlr,g around lhe injured part
• pl<1Cing: something firm {like <1 b0<1rd or rolled-up newsPQpers) next lo theinjured
port. rno:ldng sure H's long enoogh to go past the joints <:1bove <Ind below lhe Injury
• keeping the spUnl in place wilh first-aid tape
4. Seek medical eare, and don:'! ollow the child to eat. in case surgexy 1s needed.
Oo not move the ahild - and aa!! for e.mer1ency meg'fr;al care - lf:
• th& child m,:;y hO\le se1fously injured!he head. neck. 'OJ back
• a broken bone comes lhrough the skin (apply constant pte$$tlre with a clean gaU%e
pad or thick doth, ondkeep the child lyingdown until he[p amves; do not wash
the wound or pushIn any part of the bonelh<>t IS slicking aut)
©1995-2005 The Nemours Foundation. All rights reserved.
KidsHealth www.KidsHealth.org
http://kidshealth.org/parenUfirstaid_safe/sheets/broken_bones_sheet.html 2/6/2005

Bums Instruction Sheet Page 1 of 1
. Types of Burns
. • f!r$f degte bt1rns, uwe11fy eouse.d by brief <:onkrct withh t.cttn causer dn(!ss. p<tin,. ctnd sotne swel!tng.
. • Second Ad t ee . bo .tnsare m¢ t e se\fefe and ullyre:sult in bllsfe-rs and more
intense redness.
• Third-degree burns are fh de-epesl'<lild
may be pain! due to nerve damage..
What to Do: If you c m• f get the chil<i to o hospifo"f right dW<lY or must W'<ltit for on
o:mbvlonce. begin this treatment
i Remove c.fofhfng from the burned areas, except clothing stuck to the skin.
2. Run c oof {not cold} water over the burn uniil the pain. lessens.
3. Lightly ap ply o gauze bandage if ifs o small fwsf..-degree bum.
Seek emergency medi al care i:f:
• it's a second.. or third degree burn
• the bumed areo is large (cover the area with a clean, soft cloth or towel)
• the bvm come from a fire, an electrical wire or socket, or chemic als
• the bum is on the face, scalp, hands, or genitals
• the bum rooks infected {with swelling, pus, or increasing redness or red streaking of me skin near the wound)
©1995-2005 The Nemours Foundation. All rights reserved.
,......._ KidsHealth www.KidsHealth.org
http://kidshealth.org/parent/firstaid_safe/sheets/bums_sheet.html 2/6/2005

,· · '.,
- . .
Cuts Instruction Sheet Page 1 of 1
Vein Of
Artery?· , Bleeding from ofi otfory fl.ows quickly
and in spurts. and the bk>iXl isbrigh t red. <aeding ffom o vein flows 8Veruy,
· <1nd the b!o<>dIs dr::!rk red.
WhattoOo: lf the cut ts severe and youcan't getthe<:Md to o hospital tlghf away or
must wail for on ambu la nce. begin this lte<:1hn en t
i Rinse the wo1.ind and oppl;y pteswre to fhe cot with ste:tife govxe. a bondoge, or a
deanelofh.
2.. tf bloodsoaks throug,h
pressure. pface another b<1ndczge over the first and cotitin applying
3. Roise fhe injured body part fo stow bleeding. but don't opl)tV a tourniquet.
When bteeding stops. cover the wound withanew. c.4ean bat1dage.
4. To minitnite scaning, apply sunblock dorfy onee the wotJr.id has tony heated.
Gontact a doctof if the cut: • seems deep or thee<Jgas of the cot etre widely sepcr:oted
• is on the Up ond <:tosses th e pink border onto the foce
• continves to ooz.e <:ind bleeti ev,;;,n oUer applying pressure
• ls from Q bite(-artfmol or human)
Seek e..tru.ir11ency medfcal oafe if the child: • t'k:ls o body port lhat is pottio!Jy or rutty umputcrted
• hcu o cvt and the blood issporting out cmd difficult to c ontrol
• i:s ble-ed1ng :so much that bondages ore be(;omir1g sooked with blood
. :: ' ":-· '.·:.'; - - .
·:mmkPrevtitt! . . . .· . , . . . ,
. '
·. - . ·. Cru1d?r◊ : ftlflinfi<in.d' fo dl ' ore- $$ Jjk_ly t Jme tnjur ·<>ri ()bf rn s - - •'.:.:-
·. :wt ctW_s.or._do or. l hctfmay slamshi.Jt. ttr ee safefy 9cf ( Jhe',6_1?-s:..o d o, orn of staJrs or _ . .-·,
·-dt dt®rn.d QCts; · ' . . . . ' ·. :,. ..·;· • .' :·. · .
.. N'.;t ; .At}j atl Tsfof ducai<>r. taf' Pll'qu>! Soiify.. r ip e1ijc- dl;at, : ; -aia i, ,· :atiid tt e<.1t j c9nsuit a dc (:jo.r R 'vlawiMs'i'<iltlu sdo-c: t pi lor.t&u . , · ., - -· · · .·
. . R ..f. w. e r"by. Job·ns i:nriidLoo;·t2nd:Kolt!Ci mm,MQ: :0 1; re¥i ,-d;' AU9cUi l 2 ··:. . . -
KidsHealth
©1995-2 005 The Nemours Foundation. All rights reserved.
www.KidsHealth.org 1111111 http://kidshealth.org/parent/firstaid_safe/sheets/cuts_sheet.html 2/6/2005

Falls Instruction Sheet Page 1 of 1
Do not move, the chlld and eoll for emergency help (nl)if the child:
.. mqy OOV'/il Se'rlllusly illjlJfed the h,;,Qd, neek, back, h!pbo!le$, orl:hlghs • is vneons.::lous, or W<ls briefly vneoo,:cic:ivs • is hewing difficolly bre<:tlh!ng • l$<1't brooll!ing (siari Cl'!?) " has a s.elzure • hos clear f!uld or bloodco.ming from!he nose, eQrs, or mouth
Calla dodor or seek medical attention if the chttd: • won't stop eryiltg
• becomes very sleepy ond is <fdficuff to wake up • becomes lrril:abie and diffleull to eonoole • vomits more!hanIwo or three limes • complains of neck or back pain • complains of lllcreasing pain • Isn't walldng notmally • doesn't seem to be focusing his or her eyes normnlly • hos ony behavior or symptoms !hot worry you
If you think !j'ssafe to move fue child;
t.Hold the ehild c:mdcomfort him or he< until erylng stops.
2. l'laeG a coldcompress or ice pack on ,mybumps or bruises. 3. Give <1eeltlminophe11 foe pain. 4. let th·e ehi!drest, at needed, for the next few h<>vrs. 5. Watch the childclosely fer the next 24hOV<s for any tmosual symp-!oms or behavior.
1 i ,
\\_,I
KidsHealth www.KidsHealth.org
©1995-2005 The Nemours Foundation. Al! rights reserved.
http://kidshealth.org/parent/firstaid_safe/sheets/falls_sheet.html 2/6/2005

..-
l", ',: .,.·•
. .
Heat Exhaustion and Heatstroke Instruction Sheet Page 1 of 1
,.gn·
' -s-· - . a·n.-- -. :
bunng:hot.humldW-edther.
- the body"$int-emaf
temperafore con dse<nrd c<2n·
t ult inhectf eXhaustton <.lnd he<1tsttoke-. ff · notquickly treated. hectt exhdustion -cctfl
F)f ogre ss toheatstroke. whichrequite:s immed - ! ofe emergency medlcal CQre and
c<m be fntol.
. .. .
Jttptoms:
i; / e
, i1,.1ft' , ,
,. ·
.-, ·.•i:mvs
• ,:da• . :e
•we
• 'akn $s
- -hcUseo, someflrnes vomiting
• fest, shdllow breafhh1g • rrlifQbility • h.ett(klche
• lnereos.ed swe-ctfing • coot, ctornmy skin
• e-!eV-<.itkm of body te-mperafvre to tes$ than 10'4 c:f gtees rdhrenheit {40 · degree$ Celstos)
Heatm oke: • se-vere, fhrobb!-ng heodoche
• weukness, ditt,ness. or eotlfusiot1 • difficulty bteothing
• decreased responsivenessQf toss of consciousness
• litffe or no sweatin • flushed. hot,dry skin • elevcllonpf body ternperofw'.e io 1'04
degrees f o.hrenheit (40 degrees Celsius) orhighet
.. KidsHealth
If the <.:Mild hcts <:1
temperature of 104 degrees Fohrenheif
{40 deg1t?es Celsius) or t'l'lOre, ot shows l;ji'l\f $Ytnpfoms 6f hetdstrokE!:, s-eek
, eme rge ncy tne-dk:olCate fmme<iiately. In eo:se,$ ot heQt exhcu..istlonond white
ow O"it ing helpfor o childwflh possibfe h e<:itsfrok e:
1:. Sling the chHd indoors or into the
sht:Jde im medi a t ly.
2. Undress the- child.
3. Have the child lie down; -ele-v<1te feet sftghfly.
4. ff the chlf-d ls c:tlert. pf ace in CQol (not co1 bathwcter. or sponge bathe
the child r pe ate d ly. If ovtside. sprqy
the child wJthd gardenh05e.
5. if the c:hildisalert, giv-e frequent sii::>s of coot clear fluids.{clear Juicesor
spor ts. drinks dre best). t .1f the childis vomiting. tumihis or her
body fo the side to prevent choking.
1. Monlfor the child's tempe,atute..
©1995-2005 The Nemours Foundatfon. All rights reserved_
,L\ www.KidsHealth.org l!litrill
http://ki dshealth.org / parent/ firstaid safe/sheets/heat exhaustion heatstroke sheet.html 2/6/2005

\f .
:·_: ·.: .:.·-
1
Insect Stings Instruction Sheet Page 1 of 1
.. ,,.
WhattoOo: • • ,,. - ....-., 1R.emove the clufd from the -oreo where he or sheYl<Jt. st.ung.
2. If the child wos stung by a.honeybee, wasp. homet. or yellow jacket, and the- stinger is visible, remove if by gently scraping the skinhoti%onk1Uy withihe edge of a credit c:crd or yoot finge1n0ll
3. Wei.sh the reo with soap and water.
4. AppfY fo·e or a coolwet cloth to the ¢reo torelfevepatnandswelling.
5. If the area isi tchy, Qpp ty a paste of bol<.ittg S()da ('.fhd V!R1t . or cofamln t<:>tion {do not dpply calnmin,e to the child's faceorgenlkds}.
CaUthe child's doctor it • there's swelling <>r redness beyond the sting site
e the site looks infected (inereosing redness, war:mth. swef!ing, pain.or pu-s oce vrring . several hoofs o:t tonger offer the strng)
Seek emergency medical care if: • the- childshows symptoms of o se-vere ollerglc reaction
• the stingis anywhere in the mouth e the chfldhcts o knownse-vere allergy to o stinging insect
• inj fe epine-pMne wos used
,.·-
• 0 : :Tff,.;k,Prev.effti on·! . . . :··· .-_·_;:- .--·: ...:. . -, · , ·. · ·. -' .. .Jyr te; ho: - t&- <::.h ifc:l Voidw.. i:ilfqt.19 bmetoot Whtie- h gia,it{Osif!lgst mt!!d 9: f .;, ' '
··,··.<It h oir:.sproy:.: ssb'!g ih brightc= lot:s.o'f flow rid s;<:tt sw.,:h re Jh ets n .or ongregate; ··· end d kftt.-g fromsod-<_ll c QtlS. 'A. lso rnqkesure J6dt o lskfe:· bag e'·.cc.ns h. t-l'1hM .i ngn .
.· ther-e(:fl'e n,f:Stctgnanf poo'ls ti:f v, er{in rain gutters, noy.,e-r . blrdbcth1, etc.j;•and -foodi-t ., · ·, :C(')Verect w.h fi.e ng_.o v stde. · '' · · · -.·. · - · ·
Nof•: i,.i T tormaHon is.fOJ e uc<allormf pVIP¢ $¢; .F r'$pe ffic &dk;otcd leo,oiag ;. :
· (ffl(l.f tm1) •f .<:-omulf adoctor. RevfewJn,s wtth·o docf r pri.6rt9 use.· ·. · :·. ··· . :· . · • , ' H •• < • : . - • : < • ,_ •:, - - •., , .. . H ; • .. • • ' J "( .-, •
Revt we: by. J6hn B tnatdt MO'.<:i:nd Deb-oich Mulllga n Smllh.MO· . Date i w we:d: Apill2004
KidsHealth
' ' . . ' -
©1995 -2 005 The Nemours Foundation. All rights reserved.
www.KidsHealth.org
http://kidshealth.org/parent/firstaid_safe/sheets/insect_stings_sheet.html 2/6/2005
..• ..--.....
_.: ...: ,.. .
_
·n. '-
Knocked-Out Tooth Instruction Sheet Page 1 of 1
What to Oo:
.'. ,
l . ffndthe- knoc ked - out permanent tooth. tf you·t'e not sore whether ifs <iboby or permctnent tooth{d bdby toothhasa smooth edge}. edll<:r dentist or doctor ot
your foe.QI emergency room immed!dt ly.
-2. Handfelhe tooth only by as crown(the top part). neve"r by the root.
3. Gently rinse(d os,' t s<;rJJb} fhe tc)Qth immediately with sctline solution or milk. (top water sl'loold<)tdy be used <xs o kist resort it <:orltaln$ chfoJine, whichrnoy damage the root.)
4. Keep thetoothfrom dtying,outunli1 yo.u see the -cf'e,cntist by.
o i.n:se,rtlng the tooth b(;tck info its socket in the chlld'smouthlf be or she ts old nol.lghto hc>ld if in pfa e
o stoiingthe tooth in milk {not wmer}, or
o pfacing the tooth between y¢ur eheek and lower gum
5. See the chlld'sdentistor gQ to yotJr local emetgen-cy roomright a:wdy.
. y 1..,• . ; .d t till r , - .- .... ' -.,--._.,." --, ... ,_ ·: -. _.:. ·_ .._._,.·: - ,. D . . .f\ ·.r l • w , '¥ ! • .· · ·.·· . ··, ... · - .. .- · · ..
... · Chifdr.c:iffen e. te,ef.}) fr<irti plC1yina e ·oiildct.sports sucb :<tt fcoffxtJI·orfc hGC.l«-y; ftom·
·rlc:f!mg \bike$,-'<:w- rnbeipg.hri:t Jffl)¢_ r' v e )i 1¢i c rasJ( '.Cf'llldr-elt ¥Jfd e<r, MO'!Jih '9Ua:rd<i . -. ridprot¢eJiJ,,e g.ecltwhert ptaying conkl<:t spor-t, rt,tey $J'l: da ·s ebuckled!llP
: .' foon-o <:>p ri_al e,p _r: -l o.o t-se<it, ors (!>Jf wh♦n-1t\-a. or v l:'ijpf4!: • ' • • • ' . -. ' •. . • ,, , • • •, . ' ' • .. .,_ ' • .• • · : • ' , •• I 1
No'fe.i Allhifo(mciH<. >n fs ft>l' t{o:- o_f p umos d·n.Jy. F,ot e Jije, .dica f a e.dlag J. J
altld-tt: ont n,syr o fC>'-I':-
' Re r w d:-b :t Cf hti M
KidsHealth www.KidsHealth.org
w tt1Js,Wit _ d el _pf'for.-to us.. •
t f Vi wed( s t ' '; '•
\Sl1 995-2005The Nemours Foundation. All rightsreserved.
http://kidshealth.org/parent/fu staid_safe/sheets/tooth_sheet.html 2/6/2005

---
Nosebleeds Instruction Sheet Page 1 of 1
--
Most childhood nosebleeds are- caused by dryness and nose picking. To hetp eombof dryness, use• saHne ($aft wQt r} Ms0:t spr-ay or drops («putpefrofeum jelly on the inside edges of fhe child's nostrils} and osea humidltier in the-child s room. To help prevent damage from n0$e pld dng,. keep the child's ffn moils short.
Nof&r AUrntoimolion ls fot edttcoli<inaf pu 1pQs&s cm!y. f or speeiftc medical adVfce, diagnoses, and fteohn nl co1m.1U-a dodot. vf w this.witha doctor ptit>t fo use.
R vtewedby: Kol e Crort0n,MD. ond Maryl ond ut MSN. R,N CPNP Do rtw fe dt N:ov ber:2003
©1 995-2005The Nemours Foundation. All rights reserved.
KidsHealth www.KidsHealth.org
http://kidshealth.org/parent/firstaid safe/sheets/nosebleeds sheet.html 2/6/?.00')
• ff a e hi fd'5 bed is near a
heater ...fn1.he wJnt&rlime- e specially - the rnem'branes inside th.e nose can become driedorrdik hy, causing th child to piekat his <>r her noseend
• f'urlher irritate- the nasot iissue.
l. Havethe efu1d S'lt up with his. or her headiifted sUghtly fOIWard. Do not have the child te<fn ba.¢k (this may <;aV's 9ogSfn9, ¢ooghing:, or v◊miftns).
.2. Pinch the soft part of thenose(Just befow the bony pad) forat feast. 10 minutes.
con a doctor if the c hild : • ha$ frequent nosebl ds • moyhave pl1i something in his ◊T her nose • tendsto bruise ea sily. or hes heavy bleeding fromminor wounds
• reeently started a new medtc tion,
Seek emergency med.feat core or can the child's doctor if bleeding: • fs heavy, or is aecompanted bydizziness or weakne$$
• confinu s otter1w1> :attempts. of <1pptyin9 pr&$SUre tot 10 minutes aeh • is1here-wlt of a blow to tile head- or-a fa .11
. ., \ .-- .. -

· · • Think.Pnvendom
·. ..
Seizures Instruction Sheet Page 1 of 1
- ((1 ) '<·" -·" Febrile Seizures
hese ore o type ol ,eil:ure
ilh a !evl!'l, Febrile seil'.11tes
n yoonge, childre,, and l!SIJ
. OU$ or eouse an ·· laslin
What to Do: U y-01; ¢(Jn;f ge-f" tt1e chi!d k a: hospiktf rlghi tt,V y
atnbuionce, -beg!n fhis tre{ltmen:t
1 Gentty place the child on /he Boor or ground, and remove cmy nearby objeds,
2. Loosen any clothing qrotmd lh<> head or nwk.
3. Do nol try to prevent the ch!!d !!om sha!dng-thls ,,ill 1'1¢f stop !he sei,vre ond may incteo e !he child's dlscomfo,!.
4, Do not puf anylhlng in lhe child's mouth, The c:hifd will notswallow his •or her
tongo.e, and forcing teeth apart could cavse injuries.
5. Roll !he chi1d onto his or her sJde. ii the eh!!d vomits, keep him or
her on lhe slde ooo cleat out lne mouth wilh yow finger.
6. Do not give !fl,,. chffd arrylhing to drink tmtll ne or She ls /u!ly olert.
1. Coll !he chikfs doctor,
Seek emergency medical care if the child: • hos o selwre los!lt1g more !hem 5 mim,tes or ls h,:wlng r<>peoled s.el,ores
• hos difficul!y bteothing
• lutns d blvish color on !he ps, tongue, o, !ace
• r-ema-ins uneo-nsc:ious or unresponsive for more than -a few minutes ofter a seizure
• fails or hlls hls or her head during o seizlJTe
• hos o known heart condltkm
• seems ill
• ho,; any symptom !hot concems yov
.. •• ::!':er;':io;nseimrecondltkm,1:>e sure lltcilseii!it;i1'ildr6qj!ijnisibR n as
·.· · N<>f l i\lilnk!trn lwn It fur edOCllliOMf p11f!X)Se$ onty; F¢t $pii.i!li8' i. dv! i;i;$:lgn<>. ,·
dild em, <:1:>ll IJ i;, d<>elor, l«\lllewlhh. wilh <I d Of pd!liil!);. i!!f..••
Rii)it i!lly;Johri l3@mtm:il 00 Ocie rovl<iwild:1,toy200. .··· . ' . . '
.· ..·. < •.· . • .·....••.•
KidsHealth www.KidsHeaith.org
©1995-2005 The Nemours Foundation. All rights reserved.
http://kidshealth.org/parent/firstaid safe/sheets/seizures sheet.html ?/6/?fl()

Most spider bites r,G!Yse on!y milcl reo:-a!ions ln children and ron be safely lreoied ctt home. O,:;co:skm<:.1lly, !hov,;1h, o: severe a!!eraie rem:llon lo pitier bites wn be life-threatening lf left untrMted, Arid
some spkler bltes (s.ieh <:>S those from the pol,soi:ous block !dow tt:><i bro\'in
Signs of o Severe Allergic Rencfion:
• swei!ing of!he face or mouth . i dlffkully swallowing or spe«kins
recluse sp1deri} m,ect tmmedm e care.
I breothing
• dizziness or fainting , obdcminol p,;iln, nousoo, or vomiting
':ii! • 'l!Hlh1Ht <i'HIHI <!HHlH!H:i' 11 ,iH,li
♦ chest tlghtness, wl'leezing, or difficulty
Spider Bites Instruction Sheet Page I of I
Stuns and SY!DDloms of Brown 8ooluse orBlnck Widow Spider Biles:
• deep ra,,rple or blue ote,;i otound the bite,
:;-ort¢t1nded byq whltlsh ril'lg and ci forger
ouier red ring
• swelllng or redness arciund !he bite
• JoW $1iffne,s or pain
• rnvscle .pasms, lightness, and stiffness
• body@sh
• lever I> hoodtlche
• abdominal pain
• pink or reddish urine
• general feeHng of si<::kn
• laek of oppeli!e
II the.ehfkl was bllfen by a ,pider (oiha lh<:lrl o brown re,<:Wse or block widow) and doesn't seem to be having on aUergic reat:tlan:
1, W<:ISh !he bitten ,;i,ei:, will! socip cm<l WQ!er.
2 Apply an ice pack or a coo! wetciofh lo !he bile lo refieve pain andswe!ffng.
3. E!ev,:lle !he area to siow !he Spread of venom.
Seek em1;rgency medlcQ! ccire ii;
• lhe chlld hosany signs of an allergic re<1ctton
• !he ehffd develops any .Jctnd of rash ciffer a bile
• !heoreo begins to look ink,eled (increasing redness. pain, swelling, warmlh, or pus}
• YClU lhink !he child was bitten by a brownrecluse or blt.t<:k widow spider
Think Prevention! Insect repellents are useful, but use one coruainlng 10%lo 30% 01:ET, Make sure !hat garage:;-,
offlcs, and woodpiles me free of spideS' webs, ond that children wear longsleeves ond pants
when playing<ttOlltidlhe:1e areas.
Note: Allmformaffoo It for <!duc<lllo11alP<l'I"''""' only. For ip,;.:llle medlea! advlc;i,. di<1gnos<>.s, and lre<rlm<>nt, c<>MUlt yo>1r ebnd'• doetm. Revl<iw tl!ls with o <loclor pllor toUS<!.
R<>vleW<><I by. John 8ert1ar<f• MD, ond O"boralt MlJ!li<1on•Smllh.MO Oafe revl..wed! Apia 2004
©1995-2005 The Nemours Foundation. All rights reserved.
KidsHealth www.KidsHealth.org
http://kidshealth.org/parent/firstaid safe/sheets/spider bites sheet.html

7--:-i ._- · , ::; : ·· fi'' ":,: ,
, ••
; T tkff o
Strains and Sprains Instruction Sheet Page 1 of 1
What to Expect:. •pdin
• difficulty moving the injured part
• deerea-s d tb'ehgth
• swefliti9
... What to Do:
Stop activity tight away.
2. Think IU.c.e. tor the first 48 boors o ff-e r the inj\J1y:
Rest: Rest lhe injured part UhtH it's less pal.nfut.
lee: Wrap dll ice J:)dck or c o-l d comp,::ess in d lowet andptaee over- the injury immec.iia.teJy. Col'ltilnu e tot 15 rnlnofes at a time, six to eignt times u day.
Compr -slon: Support the- injury with on lasfic <:ornptessfon banddge for ot
leost 2 days.
Elevation: Raise the injured ;pent ,obove he-ort level to decrecse sw lling.
3. Give the c.hild i'bupro-fen for l)Oin ond to reduce swelling.
-4. After 48 hovrs, c,pply <1heating pad or moist hedt fhree to·four times a ddy.
Seel<. emergency medical care if the child has: • stgnrficant pi::rin when the injured pent ls toudted or moved
• trooble bearlns;J weight ofter cm injury
• increasing bruising
• numbness or o feeling of "'plhs and needles" in the ihjured dtea
• o limb that looks ..bent" or missh.apeh
• ·sign s of infection (incredslng warmth. redness, swelllt\g, an'ti palri)
• a sfraln ot sprain that' doesn't seem lo be Improving<lfter 5 Jo 7 days
'..:- ··.. -_ ,: .... , , : 1 -;. ,:,-- ··:i: ··· ! .r :· : -t.' :i..-. i!i:.
r -" ToiriR PreventlonL}··· : ..;. ► _:...;
, :::'.!, a chi! ·,_ fo - r p· ifp " ' n : rr t<;h be fc .P. !c •R g 1 y'sp -,aevtty;.
-··• end.make w:r ·fhey ul way .'W..e(:ir.!:ppprgprk,!h -·prot jy 'eqUir, .me nt . · . -
.. -.. - - - .. -- c· . ·:. , ... _ . =---," :!.' ._1, ..:..- · ,.. ?.;:::.. • • ,
'·,.;· Not / AU,foformof <>n is f tlr·t-du"t i a fp1fiPo f orijy, F f' pg fUc me4lcaradli:kt :;.dia 9)'1qs1n; .. ,·,: :,,ond fr.ea ,trl e!)h$U)f'cidoi:t • .R' rew thi$ W1'th "t1<loct ptJ?lf0t-td: !1$i / ' ,' .:· '· ,: ' :rt ,, • "
:..-. _' Ra'!ltQWe.ci by:(K<ftc, C onon,M[)<Dalo G ll ll\be-r2003- .. · •. .. . . .
..1 • - • •I • :,_, i!-
KidsHealth www.KidsHealth.org
; \• • t -: :;: •;•..--;, - ; \..-• - r I
,• • •: L, 4" ,- • . _,
© 19 95-2005 The Nemours Foundation. All rights reserved.
http://kidshealth.org/parent/firstaid_safe/sheets/str_sprains_sheet.html 2/6/2005

Coaches,
Attached is the Medical Release Form. You
are required to distribute these to each of
your players' parents and collect back a
completed and signed form from all.
Once you have completed Medical Release
Forms from all players, a full set should be
turned in to your League Commissioner/Player
Agent. In addition, a full set should be kept
by you in your Coach's book and taken with
you to all games and practices as a reference
in cases of emergency.
Thanks,
Bryan Ennis
NLL Safety Officer
Little League. Baseball and Softball MEDICAL RELEASE
NOTE: To be carried by any Regular Season or Tournament
Team Manager together with team roste r or International Tournament affidavit.
Player: Date of Bi rth: ______________ Gender ( M/ F): _
Parent (s)/ Gu ardian Name:_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Rel ationsh ip:_ _ _ _ _ _ _ _ _ _ _ _
Parent (s)/ Guard ian Na me :_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Re lations hi p:_ _ _ _ _ _ _ _ _ _ _ _
Player's Address :_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ City:_ _ _ _ _ _ _ State/ Count ry: ________ Zi p: _
Home Phone :._ _ _ _ _ _ _ _ _ _ Work Phone: ______________________ Mobile Phone: _
PARENT OR GUARDIAN AUTHORIZATION:
In case of emergency , if fam ily physician cannot be reached , t hereby aut ho rize my child to be treated by Certified
Emergency Pers onne l. (i.e . EMT, First Re s ponder, E. R. Phys ician)
Family Phys icia n: _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Phon_e:_ _ _ _ _ _ _ _ _ _ _ _ _ _
Address: Cit y:_ _ _ _ _ _ _ State/Country: _
Hos pit al Preference : - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
Parent Insurance Co:_ _ _ _ _ _ _ _ _ _ _ _ Polic y No. :_ _ _ _ _ _ _ _ Group I D#:_ _ _ _ _ _ _ _ _ _
Le ague Insurance Co:_ _ _ _ _ _ _ _ _ _ _ _ Policy No .: _ _ _ _ _ _ _ _ League/Group I D# :_ _ _ _ _ _ _
If parent(s)/guardian cannot be reached in case of emergency, contact:
Name Phone Relationship to Player
Name Phone Re latio ns hip to Player
Pleas e list any alle rgies / medic al prob le ms, includ ing those requiring mainte nance medication. (Le . Diabetic, Asthm a, Seizure Dis order)
Medica l Diag nos is Medication Dosage Frequency of Dosage
Date of last Tetanus Toxoid Booste r ----------------------------------------------------------------------------------------------------------------------
The pur pose of th e above listed information is to ensure that medical personnel have detai ls of any medical proble m which may inte rfe re wit h or alt er t reatmen t.
Mr./Mrs./Ms. _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
Authorized Parent/Guardian Signature Date:
FOR LEAGUE USE ONLY:
League Name:_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ League ID: _
Dvi
is oi
n_ : __________________________________ Team: Date : _
WARNI NG: PROT ECT IV E EQ UIPME NT CANNOT PREVENT ALL INJUR I ES A P LAYER MIGHT RECEI VE WHILE PAR TICI PATING IN BASE BALL/SO FT BALL. Litt le Le ag ue do es not limit pa rticipa tion in its activiti es on th e basis of d isa b ility, race, colo r, c;reed natio nal origin. gender, sexual prefer ence o r re lig iou s prefere nce.

Little League Baseball Norwalk Little League Medical Re/ease Form
NOTE: To be carried by any regular season or tournament team manager together with team
roster or eligibility affidavit
Player: Date of Birth: _
In case of emergency, if a family member can not be reached, I hereby authorize my child to be treated by certified Emergency Personnel. (I.e. EMT, First Responder. ER Physician)
Family Physician:. _ Address: _
In case of emergency please contact:
Phone: _ Hosp Preference: _
Name Phone Relationship ID Player
Name Phone Relationship ID Player
Please list any allergies/Medical problems, including those requiring maintenance medications (i.e. Diabetic,. Asthma, Seizure Disorder, etc...)
Medical Diagnosis Medical Medication Dosage Frequency
"'The Purpose of the above listed information is only to insure that medical personnel have details of any medical problem which may interfere with or alter medical treatment.
Date of last tetanus Toxoid Booster: _
Parent/Guardian Signature:. _
Warning: Protective equipment can not protect au injuries and a player may receive while participating in Baseball.
Little League does not limit participation in activities on the basis of disabilities, race, creed, color, national origin, gender, sexual , or religious
preference.

r,0111
( l
SdtJumor
Ncrcr (I >
U uu Uy
(])
AIWM)'$
(3)
Many a fine child has been led into almost unbelievable behavior by peers, In this
situation a youth leader - a YMCA physical direc tor, a Sunday School teacher, a Scout
RELATJONS WTIH OTHERS · ThcMllHc orn mnn11gc·r s work brings him inlo close conlnc:l wilh
many i,coplc.
A. Wllh Pllrcnlt. Do you...
I. Seek their coopcrotiou imd uudcrslanding
in trying 10 achieve lhc gonls orthc Liulc Lcnauc progm111........................ .,_.., _ _ _ _
2. Show consiclcuHion for lhcir opinions n,1d feelings .......................... -, ................. _
3. Disploy rricl\cllincss and co,,rkJy.......... .... _
0. Wilh Collcnguu . Ate 011...
I . f rlcndlf ................................- ................ _ l. Coopcrnlh-c ...............- ........... _ ..............._ _ _ l . Courteous ............. ,
4. Considcrolc............................ _ ................_ _ _
C. Wilh G.imc Ontd ulJ. Do you••
l. Displn)' .:ouncs)'.................._", ................_ _ _ 2. Rcsµccl lhclr decisions nnd ilct.:pl
leader, or a Little League manager can win the confidence of (he peers and divert their
energies into constsructi\lc channels. Parents have A difficult time controlling their
children at tliis stage of their development and when their child becomes influenced
by an adult whose ideals and aspsirataions are similar to theirs, it is a godsend. Parents
desparatcly need help and Little League managers can provide it.
IDOLIZE THE MANAGER
Because baseball means so much in the lives of American youth, they idolize
those who arc their managers. The influence of these leaders upon lhese impressionable
youngster·s is very great - so great, in fact. that no community can afford to have
anylhing short of the finest type of leadersh ip. TlvouHh tlie medium of baseball, the manager can reach these children and profoundly affect their future behavior, It is
through the manager thot all our hopes and amb itions for the players will or will not be realized. \Vhate ver good comes out of Lillle League will be the result of the manager's
leadership. ln other words, the program is as good as the manager.
As important as the manager is to the program. how much attention do we give to
his selection. orienlalion and !raining? ls !here nol, in mosl leagues, a naive assumplion
LITTLE LEAGUE®'S
GREATEST
CHALLENGE
!hem grncc n1llf .........- ....... ..- ................ .. _
3. A,'Oirl blckcrinc 1111d .. 11n1pirc b1.i lin y........ _
MANAGERIAL OUTIRS -The mnnn, cr should lm,c n knowlc,lyc of lhc gnmc of b1tscbnll of ils
C\:tndnmcnlnls nnd Its 1lrn1c10·.
C. Cunchinj! Prnctdurcs. Arc...
I. Practice sessions well plonncd 110d co nd uc led or conching nod lc.irning silu111lons
a. 11 rocticc sessions sn pp)':
that any volunteer will suffice. A district representative related tlie followiny incidcn( to
me: A lengue president was presiding at an organizationi\l meelin g, He said: " We need six
managers. Who will volunteer?" The six who volunlc:crcd first were selected, even though the. president had never seen four of U,em previously.
We make a lol of claims about the wonderful benefits of this prograin for the
pai1icipants. When managers arc selected as in dicated in the above example, the
chances are 50-50 that the children will be benefited adversely - that the program c\'e:ryonc b11sr ...................................... _
b. rlnycrs properly 1nugh1 rul'lllnmcnlnl
skills nnd gftmo strnlcgy lhrou gh th e
use of various drills ....,····- - ····-..,... c. lnst01ctio11sgivcnol l'1c pb)'c11·
leve l ol'unctcrstnnding ..... ...... ............... _
2. Prnctlcc sessions ended before du: plnycrs become bored or clisin lcfcstcd ...... _
3. Prncl icc sessions spnccd so the} do nol
bc,omc o chore for players nnd
moli:JJ;.Cl'S ,11,llkc.. .. ... .................................... _
4,. Adcqu111c prcc,mtions lnkcn to prc \'c,nl
nGcillcnl or injury
n. Items of prolceli\·c cenr ·nrc used nnd
nrc in good rcp11ir... " .. ·.. ·-··--· .. ··- ·..····- - - IJ.
will have undesirable effects upon th em. Women who volunteer as troop leaders for
Brownies must take 16 hours of !raining •· preferably before they unde11ake their
responsibility. Al each successive stage in the Girl Scout programs, volunteer leaders
must participate in a !raining program. Similarly, lhc non-professional leaders in the
Boy Scout program are required in some Councils and expected in others lo unde1)lo
training and indoctrination for their assignments. The Boy Seoul program has found
from bitter experience lhat their adult volunteers do not provide the desired le adership
unless they have been train ed. Even volunteer workers in the Red Cross gel more
indoctrin3tion and training than most Little League manAgers.
Utile League has had many managers of the finest caliber. It is oflcn surpr isi ng
lhat we have had as many exccllcn( manag ers as we have had. l3ut despite our good
managers, we are all forced to admit that we have had too niany poor ones. Many
managers have done h1mn to !heir players and have given crhlcs an opportunity to blast
by
Dr. Arthur A. Esslinger
A penetrating study and currcnl anRlysjs of the manager's role, responsibility
and position of leadership in LitUe Leai:ue. The late Dr. Essli nger, who for
many years was recognized as one of the m1.tion's foremost authorities in
his field , was Past Presid ent, Amcrical\ Associatioll for Hea llh, Physical
Educalion and Recreation and n long-t ime l\1e111ber of the Board of Directors
of Lillie League Baseba ll.
li11,ils of ph)'Sica l nud c1no ilimol
rn1ig11c ...............-.............- ....., .......... _ 5. Plnycrt continunll)" cncourng cd .............. ... _
D. Dcrclo11mcn111r Dcsircnhlc H:1t,11r In Plu,·c rs. Do yo11...
I. encoucogc µcomptucss ..........._................ _ 2. Encourage clean li\'illt nud i;,ood
hcolth habits ........................._._,............... _
J. Ern::unrngc rcsponsil,ilil)' nmJ lcn1lcrship... _
our program. They constitute the greatest threat to our program. Our procedures in
regard to managers is the Achilles' Heel of Lillie League Baseball.
We have stimula lcd lhe imaginations of J million children lo come into this
program. Yet for their leadership we have largely trusted to the luck of(he, d ·aw · to
mere ncccidcnl. The least we CAI\ do for all of the youngsters is to try to find lham a
good manager end, once selected, provide the mana er with some indoctrination and in
service training . This, it seems to me, is a solemn obligatiolL The quality of leadership represents our biggest problem, and until we solve it, we can never realize the full
Little ltc\guc 81,scbi\ll docs not li1nit pftfticipation in ils activities on the basis ordisability, racG, color, creed, national origin, gender,
sexual preference or religious preference.
4. Encourngc s110rlsmnnsh lp nnd folr 11lnr nl ftll limes n. Tcnchh1£ good mnnncr; and cour lcsy . _
b. Concrot11lnli111: oppOL\Cllls ,ncr cac.11 t;nme ........... ................- ....." ........ .. _
c. Accepting dcfcnt grnecrnllJ-- ............. _
d. Acccptinu ,i clory hum bly .-................ _
potential we have.
Access Lillie League Baseball ond Softball on the Internet at:
hllp://W\\," . lit tleleague.ors
,ny ih-c:.1+mcnli k i:111: s upph s·l U,U( U. 0 1fa 1"1 Ch lh:n "'
www.li C tlele ug u e.org
Plo)'ers kept rcnchi ngc xtrc1nc

) '
II has always been dist\\rbing to me that when Little League people get together
they spend thei r limo discussi11g evetything about the program except what is mosl
impot1ant. The usual topics of discussion at Little League Congresses, as well as
smaller local meetings, arc rules interpretations. baseball techniques, duties of district
representatives, tournam ent pfay, financial malters, insurance, player se le ction, etc,
Little consideration is given in these discussions to the Little Leal:!uer - how the
program can belier help them, what mistakes we are making , the best methods of
handling, children, the criteria ofn good manoger, selecting and training the mannger,
huw to eliminate factors detrim enta l to Little Leaguers, and the like.
In U1e final analysis, what happens to the Little Leaguer himself is the major
objective of this huge operation called Little League Bascb i\ll. The ultimate criterion
or Little League is: ls the youngster a belier person as a result of experience in lhe
program? Have the children le arned some lessons end acquired some habits and
ellitud es which will make them more effective in foture work, better parents and finer
citizens? Beside such a criterion such factors as the number of games won anti los the
leading hitter and pitche r, the league championship, toumament play, etc., are all very
If Little League is to become qualitative, lhcn we must do something positive
about improving the quality of leadet hip in its day lo day operation. This assignment
is made more difficult by two factors. The first of these is that we lose many of our
experienced personnel every year. Many parents shly in the program as long as their
children are in it. Then , when they have gained invaluable ex perience and acquired
some of the ideals of the program, we lose them. What would be the quality of
teaching in our schools if our teachers twm:d over as rapidly as ow· managers?
As president of yotu· league, the second handicapping factor is that many
managers arc untrained in youth leadership. Experienced youth leaders (in physical
education or recreation) receive a four year college program of preparation. There is
a vasl amount to be learned before a person can become an excellent Little League
manager. Just because an individual is willing to devote the time to mrurnging is not
enough of a criterion upon which lo base se lec tion. Just because he or she knows
something about baseball is like wise a11 inadequate basis for selection. Even a person
of int egrity, sincerity and high idealism needs other qualifications. All of these
considerations are important but there is far more involved in being a successful Little
A CHECKLIST FOR LITTLE LEAGUE MANAGERS
The follo)Ning checklist is proposed as an aid to Little League managers so
they can personally evaluate themselves with respect to those attributes regarded as
important to a youth leader.
By the thoughtful use of this tool, the individual manager can gel a rather clear
picture of hims elf /h rself as a coach and as n person. ff the Inspection indicates certain
weaknesses, then concenh'Rle upon removing them to the bcUenncnt of service lo the
children and the program.
You can obtain an estimate of your rating by checking the most appropriate bla11k
lo the right of the question, then totaling up your score at the end of the checklist.
If your answer is ''se ldom ornever," give yourself I point, ''usually," 2 points and
"always," 3 point s.
Excellent is 1 30 and over, above avera8e is I:!O to 129, average is 90 to 119, bolow average is 80 to 89. and u11satisfactory is 79 and below.
minor considerations.
As I see it, the real challen ge of Little Leagtte is nol lo create more leagues, larger
loumaments, develop belier players, make more money, etc., but lo make the program
League manager. Your manager needs to know the purposes of the progrnm and how
to evaluate progress toward allaining them. The manager should be acquainted with
the best ways of imparting to the players what he/she knows about baseba ll. TI1en too,
Sch.lum u1·
Nc\'c.1· (1t
Usui.ally
12)
AIWR )'li
(l)
more qunlilative -- lo make it n better, inore wholesome and enriching experience for
1hc youngs ters. This ol>jectjvc js exceedingly difficult lo alLai n. Merely to involve over
J n1illio11 children in a program is 1101 en ough . Mosl people believe thal participation
in baseball is a fine lhing for youngst ers. Yet nothing could be further from lhe truth.
Baseball is not automatically a desirable e><pcrience for youngsters. It might be under
some c ircum sta11ces, bul under other conditions it could be positively detrimental. \ le
have all seen Little League teams where children learned more undesirable habits and
ellitu des Uian desirable.
A TWO-EDGED SWORD
Whether or not baseball is good for children who participate depends upon
the total effect of the game upon th em. Ce1·Lainly, all children will benefit from the
vigorous ouldool' exerc ise . Ho wever,they derive more than ex ercise from baseball .
Their minds and emotions are invol ved in the game, as well as their muscles . l'rom
the manager, teammate s, opponents, officials , and spectatot they learn many things.
While they are acquiring the sk ills of the game, they a1·e also learning many habits
and attitudes in rel;ard to themselves and other people which arc extremely important
to their future success and happiness, They can lenm lo win and lo lose grnciously
or ungraciously, lo be loyal or disloyal, cooperative or uncooperative, courteous
or discourteous10 opponents and umpires , prejudiced or u11prejudiced to those of
different color, mcc or creed, to swear or not to swcnr, lo be considerate of those with
lesser abili ty, lo develop self disciplin e and lo subjugate lh eir own selfish desires for
the good of the team. Baseball is a two-edged sword, As a resolt of tho experience, a
child may acquire positive attributes.
Baseball ls like a package of TNT with its potentialities for constructiv eness
or dostmctiveness - fo11 good or for evil. The crucial factor in the situi\tion is the
leadership which is available. The heart of Little League Baseball is what happens
bclween manager anct player. It is your manager more than any othet' single inc.Hvidual
who makes your program a success or fail ure. He controls the situation in which
the players may be benefited or harm ed. We have all seen managers who excited a
wondetful influence upon their players - an influence which was as fine an educational
experience as any child might undergo. Unfortunately, we have also observed a few
managers who were a menace to children.
there is the critically important matter of understanding chil dren and how to reln lc lo
them most effectively. Finally. there is the mailer of exemptifyiny all the desirable
things in Little League.
My contention is th.\t from the league president's point of view, your manager is
the most impot1ant person in the Little League program. A variety of reasons support
this contention. A very im pot1 ant factor is that a child of Little Laague age wants
to en1ancipale from his primary identification with his/her parents. Up to this time
he/she has lived in submission and obedience to tl1etn. Although not in a slate of hostile rebellion, U1c child is nonetheless experiencing pangs of doubt about the all•
encompassing wisdom or his/her parents. As doubts continue, Rn increasing distance
between parent and child develops and the child lurns toward those of his/her own age
as the ultimate dete rminers of their society.
Mohr and Despres expres it this way: 1'The t:hild seeks tu dist·m•t:r meani11g.r uhcmt hlmst1. /f cmd othe 1 • thl'ough
experiences //,u/ luri:c v exclttd• his1><11 11/ s. 71,/s is 11 111< y'ur p.,ydwlugict1l
/eatwv: oftha p1't! o doll!sn mt. Up to thi.r limt!, idtmtifi,:alitm 11'1/h the pa,.en/ ,\·
uud tlepeudrnc,: t1pt111 thl!ir «pproval aml .mJJ port luwe he1•. 11 purumouut.
Nt1w, lmw,e1 er. otht:t t begin to play llllll't! 1 flg 11{ /it1<mt mlu.,· uml .serve In
importo11/ ways lo ilif/mmr.·.1t t/111 outlnnk.ft!ttli11s:s and va/111t.f act.• f!plt1d by
th< child. "'
The child now seeks for other persons lo typify the ideals and vi1tuc s that once used
to be represented by the parents. This is an age of hero worship. If the child chooses as
a model an adult who represents the high est ideals of gentlemanly behavior and clean
livin g, both the child and his parents arc fortunate. Children of the Little League ages
are strongly inHuenced by their peers. It is a tragic fact th at peer standards frequently are
1Mohr, Gcor c and Despres, Marian Tlw .\.·1or m_1• Dt1t.:adi!: Adul sr.·.,mcl!. Random House.
New York, 1958
PERSONAL ATTRIBUTES -The nu1Mgc·r s pcrsounlil)' is nit imporl;inl (nclor in the sm:ccn or LiUlc Lcoguc Bnscliiill.
A. ApJ'lcllntnct. Do you...
I . Orcss: 11uilnll ly........._................................. .. _
2. Oroom prolJcrly.......- .............................. .. _
B. Dls1u11dliun. Do you displiiy...
I . Plcasa.11l11css .. .... . .. , ... ........... .......... .. .......... _
2. A senseofhu11\ot.......................-···-······ ····- - - J. E,·cn lcntpcr ............... ... ....... ......... ............. _
4. Courtesy ........ - .. ............ - ................- ........ _
5. Sympnlhy ................ .. .......- ......... ....... ...... _
6, Enlhnsi:lsm .................................- ............. _
C. Poise. Do )'OU...
I . Hft\ c s:cl(.co111,ol.. ......................- ......._. __ _ _
2. 8ch11,-c in rm ridull mnnncr........·-····- ....- . _
0 , ChllfRClcr. Arc you... I. Sincere...... ................................................
l , Trulhful,..................................................... _ J. An csnmptc of Linlc Lcngt1c idcnls .......... _
E. Lc.indcr.-hl v. Do rou...
I. Accept responsibilit}•.......................... ....... _ l . H.i,·c lhc nbilitr lo pl.>n and orgooi;,.e ........ _
J. H11tc a good 11ndcrs1anding of the
cmo1tont1l ""ti psycho louicnl chnrnctoristios or prc-ndclcst:cnls (9 lhhl 12 ycnrs ofngc)
:,,-c good i.1pporl wilh each pleycr ......... _
S. Try lo undcrsl;1nd U1c. pcrsonol 11ccds :ind
pro\Jlcms of players And ndj11sl accordin, lr
11,·c discipline suited 10 lhc nae lerel
of lhc plii;-crs .............. .........................;..... _
7. Discipline foirl)· :md in1p1:uti.1II}'
.....

Dear Volunteer,
In an effort to ensure you have complied with all necessary requirements to be able to volunteer this
season, please complete the rorm below and submlt lt to Bryan Ennis @ [email protected]
Volunteer Name:
I have read the safety manual Norwalk Little League has put in place for the 2021
season.
I understand and will comply with said policies, rules & suggestions in manual.
I have completed a background check and have submitted the volunteer
application and photo id to Norwalk Little League.
I have taken the required concussion course and have submitted it to Norwalk
Little League.
I understand that if any injury arises I am to contact the Safety Officer Bryan
Ennis to report incident.
Volunteer signature