Embed Size (px)
Citation preview

Northumberland Hills HospitalUpdate, Coaching ReviewLinda Davis, President and CEO
Presentation to Central East LHIN Board, January 28, 2015
1

Context• In the seven fiscal years since the Central East LHIN assumed
funding responsibility for NHH (2007/08), NHH has incurred four deficits and three surpluses in its operation.
• For the fiscal year ending March 31st, 2015, NHH was (as of late September, 2014) again projecting a significant operating shortfall (approximately 2 per cent, or $1.45 M against a budget of $65 M).
• Continued pressures creating financial challenges: – Increase in service activity and acuity (ED visits have increased 8.9% and
admits have increased by 7.9% from Q1 2013/14);– Increase in ALC cases and patient days due to lack of resources in the
community;– Surge costs of 4.6% + over last fiscal year; – Increase patient transportation costs; and– Increased sick‐time expenses.
2

Context• Demographic trends from Intellihealth Ontario for Northumberland show:
– projected population growth of 11% between 2011 and 2030 – growth in over‐65 age group by 37% by 2020 and a further 40.6% by
2030 – almost double the current population of seniors• While the NHH Board and Senior Management Team understood that
some efficiencies may be possible in the short‐term, the long‐term viability of the organization would be in jeopardy if a sustainable solution could not be found.
• The purpose of the coaching review was, per the LHIN Board’s October 22nd motion: …”the NHH Board approve NHH to obtain a coach to review its current situation and provide the hospital with an accurate depiction of its current financial position, including any suggested actions to address financial pressures, which ensure sustainability of the organization going forward.”
3

Coaching Team Members • JD & Associates
– Janice Dusek• Team Lead • Vast experience in hospital operations • Nursing background and held a number of senior leader positions in hospitals in Ontario
– Norman Rees • Financial Lead • Extensive experience in hospital finances
– Zenita Hirji• HBAM and Quality Based Procedure Lead • Extensive Ministry of Health experience with new funding formula and impact on medium‐sized hospitals
4

Scope of the Coaching Team’s Work
• Identify an accurate picture of NHH’s financial position and potential forecasts for the next 3 years
• Identify and examine NHH’s cost drivers• Conduct a detailed review of the past three years of Health System
Funding Reform (HSFR) funding allocations looking specifically at the Health Based Allocation Model (HBAM) funding allocation and key drivers
• Identify/quantify further opportunities for efficiencies/cost savings and revenue generation
• Identify/quantify barriers preventing NHH from achieving a balanced operating position, recommend mitigation strategies
• Identify opportunities for further integration with partners within the Central East LHIN and in alignment with the Local Health Integration Act
• Develop recommendations including: • a 100‐day implementation plan • actions for long‐term sustainability
5

Process• Review by JD & Associates began December 1st, 2014
– Coordination and Guidance • Steering Committee established to coordinate and guide the work of the
Coaching Team • Membership included representatives from the NHH Board of Directors,
Medical Staff, Senior Management and a Central East LHIN representative – Research
• Relevant information reviewed and analyzed • Comparisons made to 13 peer hospitals in Ontario (see Appendix A)
– Consultation • Interviewed 22 members of the NHH team including Board members,
physicians and staff • Met with senior staff at the Central East LHIN
– Presentation• Findings and recommendations presented to NHH Board January 16th
6

Parameters• Constraints
– Tight timeline – December 1st to January 16th
• Key Resources – Results of benchmarking exercise conducted in Summer 2014
– Ministry of Health data (multiple sources, e.g. funding allocations, activity reports, etc.)
– Hospital’s Annual Audited Financial Statements and detailed supporting documentation
– Hospital’s Preliminary 2015/16 Operating Plan and 5‐Year Capital Plan
– A broad range of other relevant planning documents
7

Assessment of Work Completed
• Scope of the work was met • Good depth of information brought forward regarding HBAM and QBP performance
• Some areas addressed at high level only –designed as Coaching Review not full Operational Review
8

Current Financial Status, 2014/15
Forecast Operating Surplus (Deficit)
Working Funds Requirement
Total Forecasted Shortfall
Q2 Operating Forecast
$(800,000) $(650,000) $(1,450,000)
Additional Operational Efficiencies
$340,000
One‐time Funding (re: Dialysis)
$420,000
Q3 REVISED Operating Forecast
$40,000 $(650,000) $(610,000)
9

Current Financial Status, 2014/15
• Now anticipating balanced operating position at year‐end– Work has continued since end of 2nd quarter to reduce costs
– One‐time funding (re: dialysis) received
• Year‐end forecast based on 3rd quarter results• Assumes pressures do not increase in 4th quarter • Very unlikely to reach $650k surplus to meet full Y2 Working Funds Deficit Initiative requirement
10

Coaching Review –Key Insights/Observations – HSFR
HBAM • Growth is forecasted in every service module • NHH approximately $200 below expected unit cost (‐4.4%)• Majority of peer group hospitals have actual unit costs
below HBAM expected and a number are lower than NHH • NHH’s 2012/13 Base Funded Expenses ratio is lower than
peer and provincial median (contributing factors include Quality Based Procedures (QBPs) carve out and increase in net expenses)
• NHH has had a significant portion of “non‐base” MOH/LHIN revenue
11

Source – MOH HSMI 2014

Source – NHH 15/16 Operating Plan, Nov. 2014

Coaching Review –Key Insights/Observations – HSFR
Quality Based Procedures (QBPs)• NHH has higher volumes of COPD, pneumonia, tonsillectomy and cataracts than peer median
• Inpatient QBP ALOS comparable to peers in most and shorter than peers for stroke
• Opportunities to maximize funding in some QBPs and better align with clinical best practice to ensure cost effectiveness
14

Source – HSFR Impact Analysis 14/15, CE LHIN 15

Coaching Review –Key Insights/Observations – Data Quality
• Capture of flagged interventions in coded data appears to be robust and comparable (if not slightly higher) than peer hospitals
• Audit of ICU days in comparison to peer group hospitals shows no major issues
• Frequency of “discharge to homecare” also aligned with peer group experience
• No major data quality issues in Inpatient Discharge Abstract Database
16

Coaching Review –Key Insights/Observations – Clinical Activity/Costs
• Preliminary review of clinical activity suggests NHH has a less acute profile than peers
• Relatively high volume of non‐acute activity i.e. palliative care, convalescence, dementia
• Relatively high inpatient cost per patient day in comparison to peers
• Units are small and require innovative approaches to integrate services between units to gain efficiencies
17
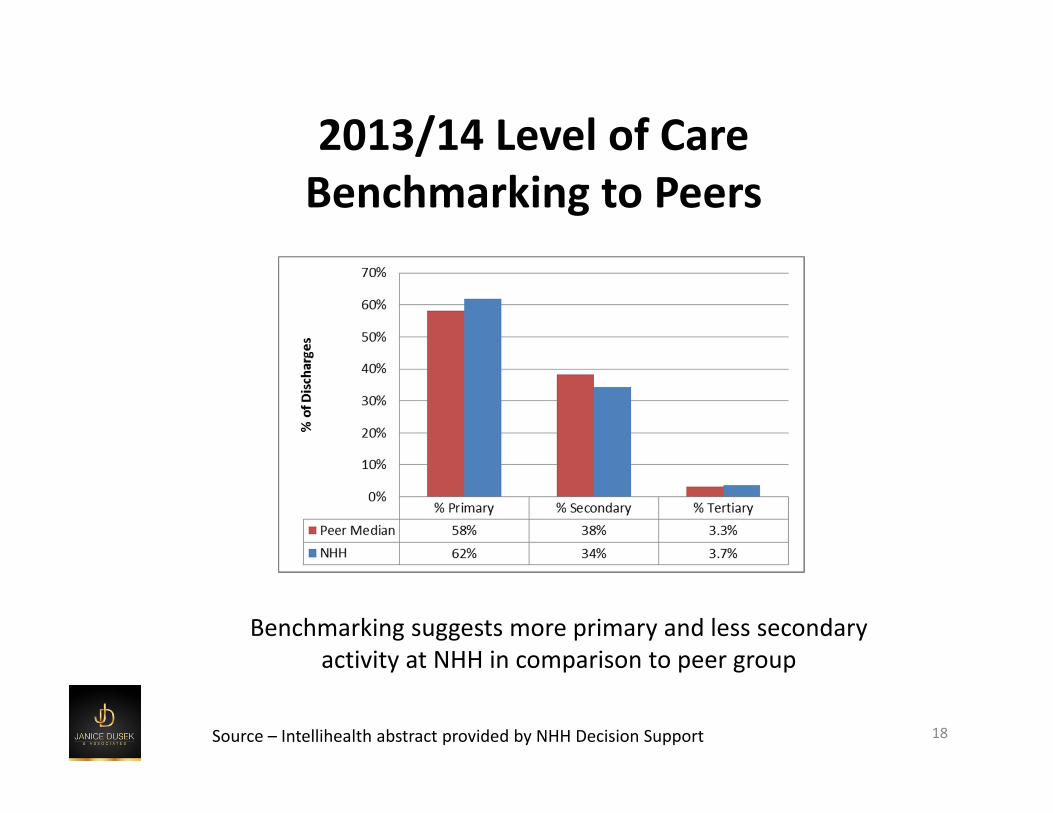
2013/14 Level of Care Benchmarking to Peers
Benchmarking suggests more primary and less secondary activity at NHH in comparison to peer group
18Source – Intellihealth abstract provided by NHH Decision Support

2013/14 Year‐End Top 20 HIGs – by LOSNo. HIG HIG Descriptions IP Cases Acute LOS ALC LOS Total LOS
1 810 Palliative Care 212 1934 3 19372 670 Dementia 49 487 476 9633 139b COPD 125 905 17 9224 196 Heart Failure wo Cor Angio 104 762 19 7815 138 Viral/Unspecified Pneumonia 128 723 18 7416 139a Chronic Bronchitis 108 625 6 6317 806 Convalescence 99 349 156 5058 487 Lower Urinary Tract Infect 78 432 2 4349 202 Arrhythmia wo Cor Angio 92 407 5 41210 576 Normal Newborn Sing Vag Deliv 249 395 0 39511 405 Cellulitis 49 369 25 39412 26 Ischemic Event of CNS 63 321 30 35113 248 Severe Enteritis 44 335 14 34914 254 Gastrointestinal Hemorrhage 58 256 86 34215 577 Normal NB Mult/C‐Sect Deliv 127 323 0 32316 477 Renal Failure 46 315 6 32117 255 Gastrointestinal Obstruction 61 281 6 28718 221 Colostomy/Enterostomy 20 272 11 28319 654 Other/Unspecified Sepsis 40 268 5 27320 257 Symptom/Sign Digestive System 63 256 2 258
Grand Total 4,200 19,735 1,296 21,035
19
HIG = HBAM Inpatient Grouper – Source: 2013/14 Year‐End Inpatient DAD abstract, NHH Decision Support

Coaching Review –Key Insights/Observations – Financial
• Opportunity for further efficiencies of $ 1 – 2 M based on recent benchmarking results
• Even with efficiencies, projected cumulative operating deficit for next 3 years (2015‐18) still estimated at $3 – 5 M
• Future sustainability will require significant clinical and financial operational changes (may take 2 – 3 years to complete)
• Short‐term financial position may require cash infusion or temporary bank line extension
20

Next Steps
NHH Board • Received the Coaching Team’s findings and recommendations January 16th
• Endorsed the findings in principle• No decisions taken at this time regarding recommendations
• Recommendations to be reviewed by Board sub‐committee and decisions taken to full Board
• Recognize need to work with partners and Central East LHIN
21

Review Recommendations, Develop Short‐Term Improvement Plan• February 2015 ‐ In‐depth Board review of each
recommendation • March 2015 ‐ Develop Short‐Term Improvement Plan
• Develop time lines and implementation plans for those recommendations approved by Board:
• Immediate efficiency opportunities to inform 2015/16 budget planning
• Recommendations that can begin with internal discussion/support• Recommendations which require discussion/support with partners and Central East LHIN
• Options for short‐term funding to sustain operations in 2015/16 • Seek Central East LHIN support for Short‐Term
Improvement Plan by March 27th, 2015 • Short‐Term Plan – to be implemented over next 2 years
22

Goals of Short‐Term Improvement Plan
• Reduce costs • Increase internal capability to capture HBAM and QBP funding • Right care, right place, right time ‐With partners, develop
community options for patients with “primary care needs” • Do the work that’s ours to do, as an acute care hospital, to
meet growing demographic pressures• Understand full opportunities for partnerships and integration
with preliminary implementation underway in order to reduce costs and increase acute patient flow
These strategies combined will lay the foundation for long‐term plan and sustainability
23

Long‐Term Goal
Through partnerships and integration, develop a refined vision as a sustainable acute care
hospital providing the services required by the population of west Northumberland
24

Challenges
• Organizational pressures (day‐to‐day responsibilities)• Staff fatigue• System pressures, community capacity, demographics
• Internal capacity to drive/implement significant change
• Threat to much‐needed donor/volunteer support• Community concerns re: change/loss of service• Costs to support transition
25
Transparency, Engagement and Consultation Required Throughout
• Achievement of short‐term and longer‐term goals dependent upon effective engagement
• Input from internal and external stakeholders will be essential
• Work on community engagement plan to commence immediately
26

Summary• Some capacity for further efficiencies/cost reduction within NHH but not
enough to “ensure sustainability of the organization going forward”• NHH continues to be an efficient hospital, but we’re not as efficient as
some of our peers and, coupled with increasing expenses, this is reducing our relative share of the base HBAM funding available
• Patient volumes are expected to continue to grow BUT NHH has a less acute patient profile than its peers and a relatively high volume of non‐acute activity
• Need for further community capacity to support primary care requirements of complex patient population
• Greater partnership, integration and clinical change required to continue to provide local acute care services
• Engagement with LHIN, partners and community required• Need for both short‐term Improvement Plan and long‐term re‐vision
27





























