Embed Size (px)
Citation preview

1
North Trent Cancer Network
North Trent Cancer Network
NSSG Constitution for the Acute Oncology Service Group 2011
Agreements / Cover Sheet This NSSG Constitution was reviewed by Dr David Hughes, Network Lead Clinician, Consultant Histopathologist, Sheffield Teaching Hospital NHS Foundation Trust, Chair of the Acute Oncology Service Task Group, on 9th September 2011 This NSSG Constitution was agreed by Annette Laban Chief Executive, NHS Doncaster Chair of the Network Board on 9th September 2011
This NSSG Constitution was agreed by the Acute Oncology Service Task Group members on 20th October 2011 Agreement for this Constitution was sought from Trust Chief Executives, Trust Lead Cancer Clinicians, Chair of Network Chemotherapy Group, Chair of Network Radiotherapy Group, Specialist Commissioner and Trust Acute Oncology Leads
Also agreed by Network Leads for MSCC Mr Neil Chiverton and Dr David Brooks PCT Cancer Leads Lead Clinicians of the MDT’s The NSSG Constitution was developed in accordance with the NTCN Terms of Reference. NSSG Constitution Review Date: July 2012 Produced by the North Trent Cancer Network Acute Oncology Network Group
July 2011

2
The North Trent Cancer Network (NTCN) serves a population of approximately 1.8 million who live in the South Yorkshire, Bassetlaw and North Derbyshire area. The North Trent Cancer Network includes large areas of deprivation and as the map below shows. The GP practices across the network are highlighted by blue dots and are concentrated in high population areas.
The Network Acute Oncology Group is:-
• the network's primary source of advice on issues relating to acute oncology in the network; • the group with corporate responsibility, delegated by the Network Board for ensuring co-ordination and consistency across the network for implementing the acute oncology measures and for ensuring co-ordination and consistency across the network for the acute oncology practice in hospitals. • the group for consulting with the NSSGs and the Network chemotherapy and radiotherapy groups on the acute oncology treatment and referral guidelines.

3
Network Configuration Acute trust provision is provided in the following organisations Designated Lead AOS Clinician/Team
Hospital Host Organisation
Referring PCT
Population (not weighted)
Dr Julian Humphrey Consultant in Emergency Medicine
Barnsley District General Hospital
Barnsley Hospital NHS Foundation Trust
Barnsley Primary Care Trust
234,397
Dr Mansur Reza Consultant in General Medicine
Chesterfield Royal Hospital
Chesterfield Royal Hospital NHS Foundation Trust
Derbyshire County Primary Care Trust
320,000
Doncaster Primary Care Trust
Dr Joe Joseph Consultant Haematologist
Doncaster Royal Infirmary and Bassetlaw Hospital
Doncaster & Bassetlaw NHS Foundation Trust
Bassetlaw Primary Care Trust
291,624 106,691
Dr Ahmed Arefin, Consultant Physician
Rotherham Hospital
Rotherham Hospital NHS Foundation Trust
Rotherham Primary Care Trust
243,151
Dr Matthew Winter Consultant Medical Oncologist Dr Peter Kirkbride Consultant Clinical Oncologist
Sheffield Teaching Hospitals
Sheffield Teaching Hospitals NHS Foundation Trust
Sheffield Primary Care Trust
550,513

4
NETWORK CONFIGURATION 11-1A-301Y
Weston Park HospitalNo A+E
No Acute medicine beds
Northern General •A & E•Palliative Care Unit•Acute Medical Beds
•No OP Chemo
Royal Hallamshire
•No A+E •No Acute Medicine beds•Haem beds•OP Chemo
Hospice Palliative care
beds
Barnsley •A+E
•Acute medical beds•OP Chemo (Onc)•Haem Beds
Hospice Palliative care
beds
Bassetlaw •A & E•No OP chemo
Doncaster•Haem beds•OP Chemo (Haem + Onc)•A & E
HospicePalliative care
beds
Chesterfield Royal •A+E•Haem beds
•OP Chemo•Acute medical beds
Rotherham•A+E•OP Chemo•Haem beds•Acute medical beds
Hospice
Palliative care beds
NTCN Acute Oncology Service
STHFT
HospicePalliative care
beds
There is a Specialist stand alone cancer hospital, Weston Park Hospital (Group2) based within Sheffield Teaching Hospital trust and based at the South Campus. Weston Park Hospital has
• Oncology beds
• Out patient chemotherapy
• Radiotherapy
• Oncology Acute assessment unit The Royal Hallamshire Hospital also falls into Group 2. All other hospital trusts in NTCN are categorised as Group 1. Haematological services are locality based but participate in a centralised weekly MDT

5
All trusts are in the process of developing acute oncology pathways within their localities and developing plans to investigate a sustainable acute oncology service.
11-1A-301y Agreed named adult Clinical Chemotherapy Services and oncology-pharmacies within the Network and the hospitals designated to treat MSCC Hospital Trust and Head of Service
“Sub-specialty” and Hospital(s) covered
Associated Oncology-pharmacy and Hospitals covered and Lead pharmacist
Designated to Treat MSCC
Barnsley Hospital NHS Foundation Trust Keira Hall
CCS for haematology-oncology As left The trust hosts an outreach service from the WPH CCS.
Trust’s own (single) pharmacy service Hospital as left Keira Hall
No
Chesterfield Royal Hospital NHS Foundation Trust Martin Shepherd
CCS for haematology-oncology As left The trust hosts an outreach service from the WPH CCS.
Trust’s own (single) pharmacy service Hospital as left Rebecca Hill
No

6
Hospital Trust and Head of Service
“Sub-specialty” and Hospital(s) covered
Associated Oncology-pharmacy and Hospitals covered and Lead pharmacist
Designated to Treat MSCC
Doncaster and Bassetlaw Hospitals NHS Foundation Trust Dr G Majumdar
CCS for haematology-oncology Doncaster Royal Infirmary Bassetlaw DGH The trust hosts an outreach service from the WPH CCS.
Trust’s own (single) pharmacy service Hospitals as left Ben East
No
Rotherham Hospital NHS Foundation Trust Dr Peter Taylor
CCS for haematology-oncology As left The trust hosts an outreach service from the WPH CCS.
Trust’s own (single) pharmacy service Hospital as left Susan Gibbons
No
Sheffield Teaching Hospitals NHS Foundation Trust Dr Nick Morley Dr Linda Evans
CCS for haematology-oncology Royal Hallamshire Weston Park Hospital (level II) CCS for solid tumour oncology Weston Park
STH oncology pharmacy service Onco-pharmacy at Royal Hallamshire (part of trust’s own pharmacy service) Hospitals as left Graham Marsh Onco-pharmacy at Royal Hallamshire (part of trust’s own
Yes – Sheffield Teaching Hospitals is the only Trust in the Network to definitively treat MSCC. Surgery at Northern General Hospital or Radiotherapy at Weston

7
Hospital Trust and Head of Service
“Sub-specialty” and Hospital(s) covered
Associated Oncology-pharmacy and Hospitals covered and Lead pharmacist
Designated to Treat MSCC
Hospital The WPH CCS provides an outreach service at the 4 hospital trusts above.
pharmacy service) Hospital as left Graham Marsh
Park Hospital
11-1A-303y Each Hospital will diagnose and treat with appropriate consultation with the cancer centre the following caused by the systemic treatment of cancer in line with NTCN agreed guidelines. Weston Park Hospital does not manage either Pleural or Pericardial effusions
The following caused by chemotherapy Neutropaenic sepsis *
Uncontrolled nausea and vomiting
Extravasations injury
Acute hypersensitivity reactions including anaphylactic shock
Complications associated with venous access devices
Uncontrolled diarrhoea
Uncontrolled mucositis Thrombocytopenia induced haemorrhage not requiring surgical intervention
Hypomagnesaemia
The following caused by radiotherapy
Acute skin reactions

8
Uncontrolled nausea
Uncontrolled diarrhoea
Uncontrolled mucositis Acute radiation pneumonitis Acute cerebral/other CNS oedema
*The current network policy is that the all patients receiving chemotherapy treatment for solid tumours contact Weston Park Hospital directly and are admitted to WPH for treatment. However, in view of the fact that some patients will present locally despite this, all units need to have processes in place to ensure that patients who present directly to them via A&E are promptly assessed and treated in discussion with WPH. When patients are stable they should then be transferred to WPH at the earliest opportunity. Each hospital within the Network undertakes to be responsible to diagnose and manage patients presenting with the following conditions, referring to specialists were appropriate. Conditions presenting as an urgent acute problem Patients with a known malignancy or patients with a previously unknown malignancy Pleural effusion Pericardial effusion Lymphangitits carcinomatosa Superior mediastinal obstruction syndrome including superior vena cava obstruction
Abdominal ascites Hypercalcaemia Spinal cord compression including MSCC Cerebral space occupying lesions Any other cases where A&E staff or acute medical firm decide an urgent oncology assessment needed

9
11-1E-110y (see page 43) Metastatic spinal cord compression All trusts within the Network may diagnose patients with MSCC but treatment interventions are only carried out in Sheffield Teaching Hospitals Trust at either Northern General Hospital site for surgical intervention or Weston Park hospital site for Radiotherapy treatment. This takes place after the relevant discussion with appropriate personnel. See MSCC Referral Proforma Appendix 2 The MSCC Referral Guidelines are attached as Appendix 3 to the NTCN Acute Oncology Annual Report document. All Patients with the potential to develop MSCC should be provided with suitable agreed information see examples Appendix 1(Both Sheffield and Doncaster and Bassetlaw Hospitals have been Beacon sites for the Information Prescriptions project) All organisations provide information to patients at risk. At the time of information provision clear advice is given on the relevant person to contact if they have concerns. This method of providing information has been agreed at the appropriate NSSG’s Hard copies of agreed local information is available These key actions should be undertaken for any suspicion of MSCC Contact MSCC Co coordinator urgently (within 24hours) to discuss the care of the patients with cancer and any of the following symptoms suggestive of spinal metastases
• Pain in the middle (thoracic) or upper (cervical) spine
• Progressive lower (lumbar) spinal pain
• Severe un remitting lower spinal pain
• Spinal pain aggravated by straining (e.g. coughing sneezing)
• Localised spinal tenderness
• Nocturnal spinal pain preventing sleep Contact the MSCC co coordinator immediately to discuss the care of patients with cancer and symptoms or signs suggestive of MSCC and view them as an oncological emergency
• Neurological symptoms including radicular pain
• Any limb weakness
• Difficulty in walking
• Sensory loss or bladder or bowel dysfunction
• Neurological signs of spinal cord or cauda equine compression

10
11-1A-302Y Review the provision of chemotherapy, oncology pharmacy and acute oncology services across the Network
NORTH TRENT CANCER NETWORK BOARD
Friday 11th February 2011
Update on Acute Oncology Service implementation
1 Introduction
The National Chemotherapy Advisory Group Report (Chemotherapy Services in England; ensuring quality and safety) published in August 2009 was a response to the concerns identified through the NCEPOD report and the cancer peer review process regarding the safety and quality of chemotherapy services.
One aspect of the report drew specific attention to the provision of emergency care not only for patients developing complications following chemotherapy, but also for those patients known to have cancer, suffering from acute symptoms of their disease. This includes actions to support the management of patients not yet known to have cancer, but who are suffering from symptoms which may be cancer-related.
In a response to the issues identified above the report recommends that all hospitals with an Accident and Emergency department establish an “acute oncology service” (AOS), which requires that the relevant staff from A&E, general medicine, haematology and clinical/medical oncology, oncology nursing and oncology pharmacy work together as a single acute oncology team.
The draft AOS Cancer Peer review measures are currently out for national consultation and it is expected that Trusts will have to perform a Self assessment against the measures when they are finally issued in time for August 2011. Internal Validation will take place in September
The issue of Acute Oncology has been discussed previously at Cancer Board and this paper summarises the approach that the North Trent Cancer Network has taken and the progress to date.
2 Progress to date
A meeting was held in January (that had been delayed from December) with trust representatives in order to:
a) Agree a set of network wide working principles
b) Acknowledge that there may be a range of clinical models of delivery as models will be developed locally shaped by existing clinical arrangements and specialist input

11
c) Identify the patient groups the acute oncology service clinical model will
address
d) Agree next steps
3 Local Progress
The trusts within the North Trent Cancer Network have local implementation groups in place and are currently working on plans for delivery and making progress in a range of areas.
At the workshop progress in a number of areas was noted including:
a) Rapid alert systems were under development or in the implementation phase in a number of the trusts
b) Data on the number of emergency admissions and length of stay was being collected but that more standardisation and learning from others could support this
c) Patient pathways were under development at most trusts
d) There was a shared understanding that ”oncologist” could include haematologists and therefore service models were being developed with that possibility in mind. However differing views were expressed on the possible role of Haematologists in solid tumour acute oncology.
4 Challenges
Although some good progress has been made locally there is still a considerable amount of work to do, some of which requires significant change both at service level and at a professional level. For the acute oncology service and team to work well a number of issues will be challenging including:
a) Developing appropriate clinical models relevant to each local trust and resourcing it appropriately in order to fulfil the anticipated cancer peer review requirements.
b) The roles of the individuals comprising the acute oncology team will be critical and this will inevitably require that oncologists, haematologists, palliative care consultants and the specialist nursing staff will be affected.
c) More network and local protocols and pathways will be required particularly for the management of metastatic spinal cord compression and cancer of unknown primary both of which have either a NICE clinical guideline available or under development as part of AOS measures.
d) The clinical local pathways, policies and escalation process ensuring timely connectivity to the Oncologist either locally or at Weston Park are crucial, therefore ensuring that the impact on Oncology time is co-ordinated. Determination of “front door” policy is a key factor.
e) Robust data is required to understand the current position so that the changes can be quantified, in particularly reductions in length of stay at

12
trust level
f) Optimising existing resources and developing cost effective “new” ways of working
5 Next Steps
As outlined within this paper there remain many challenges to developing an Acute Oncology Service within each hospital in North Trent. Some progress has been achieved already but in order to meet the expected national milestone it is now necessary to take this work forward quickly and this will require that:
a) The Task subgroup will be set up as soon as possible ( first meeting end of February) and will report to Chemotherapy Strategy Group and Cancer Board on progress
b) The Group take forward the development of protocols, generic pathways and provision of 24/7 advice both in and out of hours.
c) The Group will work to develop a consistent Network education package to support the services.
d) Investigation should take place about the numbers of patients involved and whether emergency and neutropaenic pathways could possibly be delivered locally.
e) The group will ensure that work is coordinated across the network, and with changes already planned/underway on reduction of Follow Up and how this might support AOS.
f) Support should be given to the work underway to develop Health Care Professional assessment of chemotherapy patients to potentially release oncologists’ time for the AOS. The work of this group should be prioritised.
6 Recommendations
The Cancer Board is asked to note the progress to date, the challenges identified and to support the view that a high priority must be given to this work by the trusts and the network team for this work.
Kim Fell David Hughes Cancer Director Network Lead Clinician

13
North Trent Cancer Network Work Plan 2010-2012
Measure 11-1A-303y
Aim To ensure that there is an Acute Oncology Service in every hospital with an A+E department and acute admission wards.
1. Safe – ensuring that the services are as safe as they should be – Robust Governance 2. Effective – focused on delivering best outcomes for patients 3. Personalised – meets the needs of individuals providing access to services at the time and place of their choice 4. Fair – available to all, taking account of personal circumstances and diversity 5. Cost Effective – value for money
Objectives and Requirements Commissioners working with providers will determine the appropriate balance of services across a network at both cancer centre and DGH or at a Community Hospital or in a patients’ home.
Different models will suit different trusts and services but the following key components will need to be met
1. A minimum of two Oncologists are responsible for providing acute oncology (haematologists and oncologists) input 2. The oncologists provide 5 day service for acute oncology 3. The oncologists is likely to provide site specialised services in the same unit 4. Two specialist oncology nurses to provide rapid input into the care of patients suffering from complications of chemotherapy 5. There is an acute oncology team office with part time secretarial support to take referrals and provide a physical focus 6. Oncologists will not usually have their own beds but will be available in the hospital Monday to Friday 7. The extended acute oncology management team is defined as the acute oncologists, the acute oncology nurses, the lead
haematologist, the lead haematology nurse, the lead A&E physician, the lead general physician, the hospital cancer manager / lead nurse, and the palliative care lead.
8. An information system that automatically flags up to the AOT when known cancer patients are seen or admitted 9. The oncologists and specialist oncology nurses will be fully integrated within the trust pathways and protocols, clinical meetings etc

14
10. The AOT will be a service integrated into the hospital’s portfolio of cancer services Patient Groups Included
• Chemotherapy (and radiotherapy) patients currently on treatment (and within 30 days of treatment)
• Treatment of acute symptoms in patients known to have cancer but not currently on active treatment
• Treatment of patients who have not yet been diagnosed with cancer, but who have acute symptoms which might be cancer
• Management of patients with spinal cord compression
• Management of patients with cancer of unknown primary

15
Outcome Theme Action Lead 2010 2011 2012
Accountability i. Subgroup of the Chemotherapy Strategy Group (NCAG Implementation oversight group)
ii. Agree membership iii. Leads to be identified by each Trust iv. Formalise terms of reference
Kim Fell AOS Working group
April 2011
Principles 1. Principles defined 2. Local clinical models to be determined
based on the NCAG recommendations and network principles
3. On call / 7 day cover arrangements
Dec 2010
Clinical Models
Local Implementation Group
Each Trust to identify a project team Each trust to develop local proposals for discussion at the Subgroup meetings
Cancer Managers Identified Lead
May 2010 Sept 2010
Roles and Responsibilities
• Role of Oncologists
• Role of Haematologists
• CNS
KF / PF
December 2010
Testing new clinical models Examples
Each Trust is working on a number of areas including
• Data collection – Length of stay
• Patient flagging/ rapid alert systems
• Emergency Admission process
Workshop
December 2010

16
Outcome Theme Action Lead 2010 2011 2012
Existing protocols
Review Network protocols e.g. neutropaenic sepsis, extravasations Review locality protocols to ensure they meet Network policy Ensure these are embedded into the organisation - audit
Chemo nurses group Chemotherapy Strategy Group Trust Oncology / Haematology Governance leads
Ongoing Pilot in Haematology
On website August 2011 Sept 2011
Monitor and support localities to develop Acute Oncology Team Define principles relating to safe pathways
Workshop
December 2010
Governance
Agree lead arrangements in each trust to support:
• Pathways reviews
• Mortality reviews
• Adherence to policies/procedures
• Defining standards – door to needle time
Haematology and Oncology leads in each Trust Subgroup
December 2010
June 2011
Safe Service Robust Governance
Ensure effective communication
Work with cancer managers Links to Information systems Escalation to Weston park defined – triage – practitioners
Workshop
December 2010
Implement the agreed principles relating to good service level
Trusts to develop plans in line with network principles and the nationally described key components Implementation of the plans
Agree action plan
November 2010
December 2011
Develop links with Engage with primary care once models Primary care lead

17
Outcome Theme Action Lead 2010 2011 2012
primary care
agreed
Optimising resources
Reduce length of stay – need figures Reduce follow-up appointments to free up oncologist time Phone triage Capacity in clinic – urgent clinic appointments?
Discuss with Zoe NSSGs/ SILs
Ongoing work
Work on service Improvement with AOS Nurse group
• Conference Call to establish locality position
• Monthly reporting from Doncaster AOS pilot
• Capture baseline for all localities
• Support lead nurses re retrospective and prospective audit data collection
• Identify with NTCN Info Team if dataset can be sourced from HES or CCT
Karen Leivers Judith Bird Karen Leivers Karen Leivers
31August Sept – Dec 30 November 30 November 31 August
Monitor and support localities to develop Acute Oncology Team
Policy Development
• Define policy for managing complications of
a. chemotherapy b. radiotherapy
• acute symptom management for cancer patients
• Define policy for managing patients not yet diagnosed with cancer
• Define policies for managing spinal cord compression
• Define policies for managing cancer of
Review Network protocols – NSSG guidelines Review locality protocols to ensure they meet Network policy

18
Outcome Theme Action Lead 2010 2011 2012
unknown primary
Ensure that the Network protocols in line with NICE guidance Ensure that the locality protocols to ensure they meet Network policy
ALL
Implementation Phase
Obtain patient and carer views from across on their experience
AOS Nurses 2012
Information Technology
Plans for: Flags on hospital systems – Learning across the network Alert systems with connections to MDT’s within 24hours
Trust leads
December 2010
Effective Time and Place
Ensure effective communication
Robust communication processes in place in each Trust
Trust Leads

19
Outcome Theme Action Lead 2010 2011 2012
Cost Effectiveness
Optimising resources by reducing length of stay and follow up
• Data by cancer diagnosis
• Admissions by cancer diagnosis
• Quantify the financial value and potential savings
• Quantify additional workforce required as part of the AOS
• Develop a fully costed proposal for each trust
• Detail an audit programme post implementation
Cancer Managers / Service Improvement Lead
Ongoing work December 2010
2012

20
NORTH TRENT CANCER NETWORK
Local Chemotherapy Work Programme 2009/2011 1. Strategic Aims
• Deliver services locally where possible creating easier access and reducing inequalities in areas of greater deprivation
• Reducing Death rates / improving survival rates for a number of cancers
• Greater access to Oncologists in areas of greater need
• Local access to research trials – improve survival rates
• Equal access to chemotherapy by reducing travelling to the tertiary centre 2. Change Management tasks to ensure that the objectives are met
• Identify key stakeholders and benefits
• User / Public involvement at all levels and all stages
• Executive leadership at a network and local level to ensure integrated, co-ordinated care through a single integrated team approach but separate management arrangements
• Local Implementation teams with a designated local manager lead.
• Network implementation (Project Board) with regular updates via Director to Cancer Board
• Contracting arrangements, reporting and data management / outcomes to be developed and agreed.
• Links to national tariff arrangements / cost / activity changes – demonstrate value for money. – QUALITY improvement

21
3. Service Issues Desired Outcome Objective Action
Monitoring Measurement
People with cancer will have an improved health outcome
To ensure the people with cancer and their family members will have access to local treatments where possible
Facilitated Sessions User Engagement Clinical Engagement Local Engagement Oncology buy-in Haematology buy-in Identifying Risks / Benefits
Timescales met Strategic Aims agreed Objectives agreed Business plans produced LDP Submission
Board papers presented Papers supported and agreed Funding agreed COMPLETE
Safe and consistent working practices.
Develop, agree and implement clinical pathways Oncology leads in place – July 08
Out of hours cover in place Training complete Staff recruited
Timed pathways monitored Adverse events monitored COMPLETE
Practice meets national standards and Cancer Peer Review measures
Develop services in line with Peer Review measures
Network Chemotherapy Lead clinician will develop Operational policies (clerical activities/treatment options/ clinical trials) in place
Self assessments complete
Ensure oral chemotherapy guidance (NSPA) in place.
Local policies implemented by local teams
Comparable data reports
Chemotherapy data set Data collection points agreed Recruitment complete audits take place
Activity data / drug usage /
Clinical activities and checking point
Each locality working up with oncology leads as part of operational policies
Operational policies in place Adverse events reported Comparable data / network reports
Each locality working up with oncology leads as part of operational policies
Critical assessment points/ trigger points for onward referral to WPH agreed
Audit of the process available
Each locality working up with oncology leads as part of operational policies
Referral back to DGH asap
Audit
People with cancer will receive safe care Delivery in line with NCAG recommendations Co-ordination and Integration of patient Care
Develop processes for sharing clinical information Joint access to clinic booking
Explore and develop locally held clinical records Develop a patient satisfaction survey for
Communication pathway Manual systems in place in the
Patient experience survey Adverse events reported

22
Desired Outcome Objective Action
Monitoring Measurement
arrangements using web technology
use per and post change short term
Define the standards all parties will work towards. Clinical Leadership & Governance
Oncologist lead to develop local governance arrangements
Network lead clinician agreed all arrangements Clinical leadership development requirements for new leads
chemotherapy contracting framework defining Peer review and safety measures - monitored Practices are audited and benchmarked at network and national level
Peer Review All sites visited once. Starting second round of visits
Start preparation for 2011/12. Compliance with Peer review measures at the visits
Waiting times met Audit against JCCO/ RCR Guidelines Include within peer review Waiting time Data – Breaches comparative nationally
2. People with cancer will receive safe care
National Chemotherapy Advisory Group report issues Integrated governance arrangements (Oncology and Haematology) are in place at each local DGH.
Network Lead identified Lead Oncologist sessions identified and funded Joint working in place
In place In Place Recruitment of staff at DGH
Incident reports Adverse events Planned activity transfers have taken place
Funding agreed at all sites. Engaged with STH IT and meeting held across all sites. Phase 1 and 2/3 identified. To proceed with individual procurement for PH1 urgently.
E prescribing implemented Explore potential for phase 2 – haematology and interfacing 2009/10
Audit of protocols used by tumour type and Consultant Use of NICE drugs
To ensure people with cancer are able to access cost effective care
Capacity and Demand studies Implement C Port WPH close to completion of baseline.
Implement CRF – integration and co-ordination of care a. capacity and demand – C-PORT complete
Comparative costs for day case activity Utilisation of resources
3. Patients with cancer will receive NICE approved cancer drugs
Reduce bed utilisation – in patient and WPH development of short stay LoS

23
Desired Outcome Objective Action
Monitoring Measurement
chemotherapy complications unit
More self management Work with the Primary care Group to develop proposals
Links/protocols with primary care to reduce need for admission
Adverse events Emergency admissions Readmission rates
Ensure people have access to trials locally
Clinical Trials – increase recruitment, develop trained workforce
Bid agreed for pharmacist for a. STH haematology and b. cross locality liaison/oversight
% patients entering trials Patient feedback
Ongoing nursing and pharmacy Planned staff recruited in DGHs (nursing, pharmacy) complete
Activity versus capacity
Sufficient, trained staff to deliver a local service
Nursing – package in place. Implemented with support from WPH. Pharmacy – standard training package being developed.
All staff trained and recruited complete
Comparable quality – adverse events – peer review
4. Improved survival
Less centralisation Increasing the rollout of local chemotherapy - nursing subgroup
Assessment of implications of reduced activity in WPH Review the additional regimens for local delivery Work with NCAT to develop effective clinical outcome measures
Access the Impact at the tertiary centre Assess capacity, efficiency and working practices Pilot to be done in WPH over 1 year period and then results used in other sites
Activity / costs and comparable data Funding to match activity To be agreed
Contract for Quality Determine Data requirements Patient outcomes agreed and defined across the pathway
Increases local delivery - activity
Include pathway measures in contracts
Review Service Level Agreements
Access improved Patient satisfaction / feedback
5. Achieve positive patient outcomes through contracting
Demonstrate value for money Review activity – day case Drug costs/usage
Clear links to pathway performance
Comparable costs in all Trusts or defined quality benefit
a) Chemotherapy (and Network to support the development of: Local meetings
24
Desired Outcome Objective Action
Monitoring Measurement
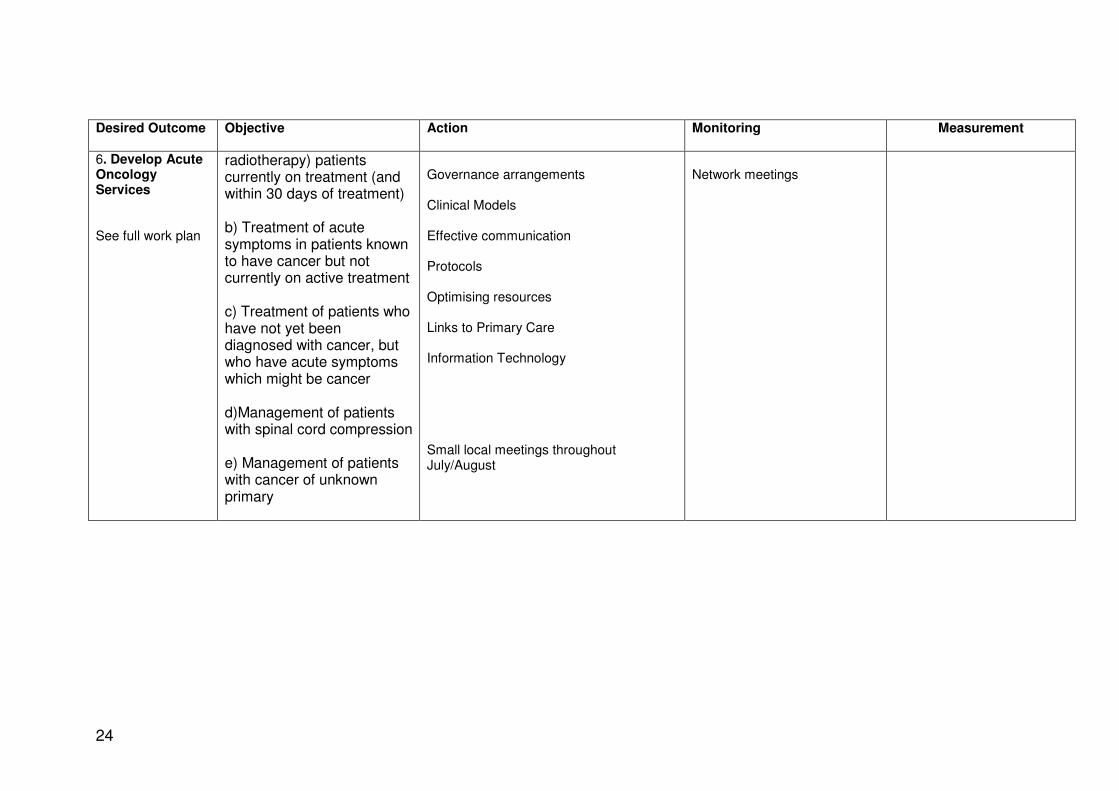
6. Develop Acute Oncology Services See full work plan
radiotherapy) patients currently on treatment (and within 30 days of treatment) b) Treatment of acute symptoms in patients known to have cancer but not currently on active treatment c) Treatment of patients who have not yet been diagnosed with cancer, but who have acute symptoms which might be cancer d)Management of patients with spinal cord compression e) Management of patients with cancer of unknown primary
Governance arrangements Clinical Models Effective communication Protocols Optimising resources Links to Primary Care Information Technology Small local meetings throughout July/August
Network meetings

25
11-1A-304y MEMBERSHIP OF ACUTE ONCOLOGY TASK GROUP CORE MEMBERS CHAIR
Dr David Hughes AOS lead - Network Lead Clinician
Sheffield
CLINICAL LEAD
Dr Patricia Fisher Consultant Clinical Oncologist Sheffield (WPH )
Dr Ahmed Arefin Consultant Physician Rotherham
Lesley Barnett Lead Cancer Nurse Doncaster
Judith Bird Network Lead Nurse NTCN
Janine Birley Lead Cancer Nurse Rotherham
Dr Linda Evans Consultant Medical Oncologist Network Chemotherapy Deputy Chair
Sheffield (WPH)
Kim Fell Network Director Current Network Chemotherapy Chair
NTCN
Mark Gilmore Lead Cancer Nurse Barnsley
Nicky James Lead Nurse Chesterfield
Dr Joe Joseph Consultant Haematologist Doncaster
Graham Marsh Pharmacist - Oncology Sheffield
Dr Simon Pledge Consultant Clinical Oncologist Chair of the Network Radiotherapy Group
Sheffield (WPH)
Pauline Pledge Matron Outpatient and Chemotherapy Day case Services Nurse member of AOAS service
Sheffield (WPH)
Dr Mansur Reza
Consultant Physician Chesterfield
Martin Salt
Lead Nurse Sheffield
Michel Thompson
Matron Rotherham
Sue Tonge Senior Sister, Chemo Day Unit Doncaster
Lucy Walkington Medical Oncology SpR Sheffield
Dr Emma Welch
Consultant Haematologist Chesterfield

26
Dr Matthew Winter From August 2011
AOS Lead Sheffield
Alison Morton Patient Representative *
Dr David Brooks From September 2011
Macmillan Consultant in Palliative Medicine
Chesterfield
Jane Harding From August 2011
AHP Lead Lymphoedema specialist - Physiotherapist
NTCN
Dr Christopher Dalley From August 2011
Haemato-oncologist
Sheffield
*The agreed mechanism for obtaining further user advice if necessary, is via the Network Macmillan User Facilitator and the Network Patient Partnership Group
Terms of Reference
The Network Acute Oncology Group is a Network Cross Cutting Group (CCG) and the Terms of Reference for the group are the Network generic terms of reference used for both NSSGs and CCGs. A list of responsibilities included in list of responsibilities identified in Network CCG Terms of Reference

27
NAME OF GROUP: Network Site Specific Group (NSSG)
Cross Cutting Group (CCG)
ACCOUNTABLE TO:
The North Trent Cancer Network Board The NSSG/CCG Chair is a member of the Network Lead Clinician Forum and as such is responsible for ensuring risks associated with the delivery of services across the relevant pathway are fed into the network planning process.
PURPOSE: The NSSG/CCG has responsibility, delegated by the Board, for ensuring the co-ordination of the cancer pathway and the consistency of care for the relevant client group within the cancer network. This includes:
• Service planning
• Service Improvement / Redesign
• Service Quality Monitoring and evaluation including clinical performance and outcomes
• Workforce Development
• Research and Development The Network tumour-site specific groups should have the active engagement of all MDT leads from the relevant constituent organisations in the network. NSSGs should ensure that all agreed operational changes are discussed with local managers to ensure that changes are integrated into constituent organisational structures and processes. Discussions to explore other changes to existing patient pathways may be initiated by commissioners including Primary Care. NSSG provides advice in respect of all significant service changes (e.g. IOG) particularly if there are financial consequences, and will make recommendations to the Cancer Board. The NSSG has a key role in: Developing plans to implement Improving Outcomes Guidance Monitoring the implementation of the agreed Improving Outcomes guidance action plans. Raising concerns and areas of risk to the Board via the agreed governance arrangements.
COMPOSITION OF NSSG:
• Chair of the NSSG
• The MDT lead clinician from each MDT in the network
• Nominated Oncologist
• Pathologist
NORTH TRENT CANCER NETWORK (NTCN)
NETWORK SITE SPECIFIC / CROSS CUTTING GROUP(s) COMMON TERMS OF REFERENCE 1
February 2011

28
• Specialist Surgeons / Physicians
• At least one nurse core member of a MDT
• A service improvement staff representative
• Two user representatives* All the above are core members common to every NSSG . The following members are optional: As many other members of those MDTs e.g. Physiotherapy, Speech and Language therapy as appropriate
• A representative of palliative care
• A Primary Care Cancer Lead
• A manager representative (from a PCT, provider or NORCOM HQ)
• As a minimum, involve users in their service planning and review * For any one NSSG, the network partnership group can agree an alternative mechanism for obtaining user advice.
Each NSSG will list all its members. COMPOSITION OF CCG:
The composition of each cross cutting group includes a representative from each locality of each specific cross cutting group, and where appropriate wider membership will reflect National Guidance. All groups will review membership annually, and record attendance as per National Guidance.
CHAIR: The NSSG/CCG will select its own chair and deputy. Tenure in each role should be reviewed after 3 years. The Chair should have an annual appraisal.
CHAIR’S EXTRA-MEETINGS ROLE
The Chair will: -
• Ensure engagement of constituent members.
• Attend development programmes organised for the Lead Clinicians
• Facilitate the identification and agreement of the service priorities for the NSSG/CCG
• Recommend priorities to the Network Board.
• Ensure an annual report of the NSSG’s work is written
• Have an annual (review) meeting with the Network Lead Clinician and the outcomes agreed by the Network Chair.
• Be an ambassador for service improvement locally and the NSSG/CCG, regionally and nationally.
INDIVIDUAL ROLES:
Each core member should attend 50% or more of the NSSG/CCG meetings. It is assumed that their employers will protect the time commitment entailed. One of the NHS-employed NSSG members will be named as having specific responsibility for users' issues. One of the NHS-employed NSSG members will be named as having specific responsibility on information for patients and carers. One of the NHS-employed NSSG members will be named as having specific responsibility on service improvement* ie being a champion for it.

29
None of the above three roles are mutually exclusive. Members should ensure that all decisions become integrated into constituent organisational structures and processes * but not the member of service improvement staff.
DECISION MAKING PROCESS:
All attendees at the NSSG meeting will have a vote. Recommendations to the Board will normally be achieved through consensus; however, when a vote is required it is essential that the split of votes is recorded to aid the understanding of the Board in the decision making process
QUORUM: The meeting is quorate when 50% of the constituent core members are represented at the meeting, but the chair can declare a larger meeting non-quorate if key members are not present.
RESPONSIBILITIES:
NB this (long) list of responsibilities assumes the regular input of provider managers and network officers. Service Planning is in line with: 1 National guidelines and advising commissioners and provider
trusts of the implications of that guidance for the whole network. 2 Identifying any risks within the service and developing a network-
wide service delivery plan to deliver the NHS Cancer Plan. 3 Responding to Improving Outcomes Guidance recommendations
and advising commissioners on appropriate patient pathway (or model options) developments within North Trent, which will deliver patient care within those recommendations. Developing efficient working models aligned to good practice guidance and national policy drivers.
4 Agreeing common standards including referral pathways, revised
in light of national policy or guidance, patient care pathways (from primary care, both into and out of tertiary services). This includes updating and revising referral guidelines as appropriate. In time a service specification will be generated.
5 Agree on priorities for data collection, produce audit data and
participate in open review including the user experience and service user evaluation
6 Monitor progress on meeting national cancer measures, trial entry
and ensure action plans agreed at Peer Review are implemented. 7 Reviewing approved clinical trials, and other research, once a year.
Agreeing a single list of clinical trials and studies into which the network’s MDTs should give priority for patient entry.
8 Develop clear cancer workforce recommendations that foster new
30
ways of working so that services are robust in the face of recruitment difficulties and emergent technologies.
9 Foster strong working relationships to develop network-wide
resolution to workforce issues 10 Liaising and consulting with the relevant "cross cutting" network
groups to identify issues that have wider implications and consequent knock on effects. This includes chemotherapy; imaging; histopathology (and other laboratory investigations); specialist palliative care, with the Head of Service for radiotherapy, Children and Young People and Primary Care.
FREQUENCY OF MEETINGS:
At least once every 6 months to a maximum of 4 times per year. Additional meetings may be necessary for short term task and finish projects e.g Peer Review preparation, IOG implementation
SERVICED BY: Cancer Network Office (2 days per meeting, but 9 days pa max) 2
COMMUNICATIONS:
Outward – NSSG/CCG lead to give feedback to the Lead Clinicians Forum and present findings, with recommendations, to Cancer Board
- MDT leads to share items of news with fellow MDT members and with local managers
- NSSG (lead) to write an annual report - NSSG to write an annual work programme for Board endorsement
News can be placed on the network’s website
http://www.northtrentcancernetwork.nhs.uk Agreed guidelines will be downloadable from there.
MINUTES CIRCULATED TO:
NSSG members Network Lead Clinician
Cross-Cutting Groups Leads Primary Care Cancer Leads
REVIEW DATE: July 2012 11-1E-101y The Network AOS Group holds quarterly two hour meetings. Details of these meetings are outlined in the Annual Report. The meeting has administrative support to record the details of the discussions and those in attendance. 11-1E-103y There is a 24/7 on call consultant oncologist via the on call rota at Weston Park Hospital 9.00am to 5.00 pm 7 days per week they are contactable via the hot mobile telephone 07949 021449 or the on call bleep, out of hours contacted via the hospital ( WPH) switchboard, Please see extract from specimen rota below

31

32

33
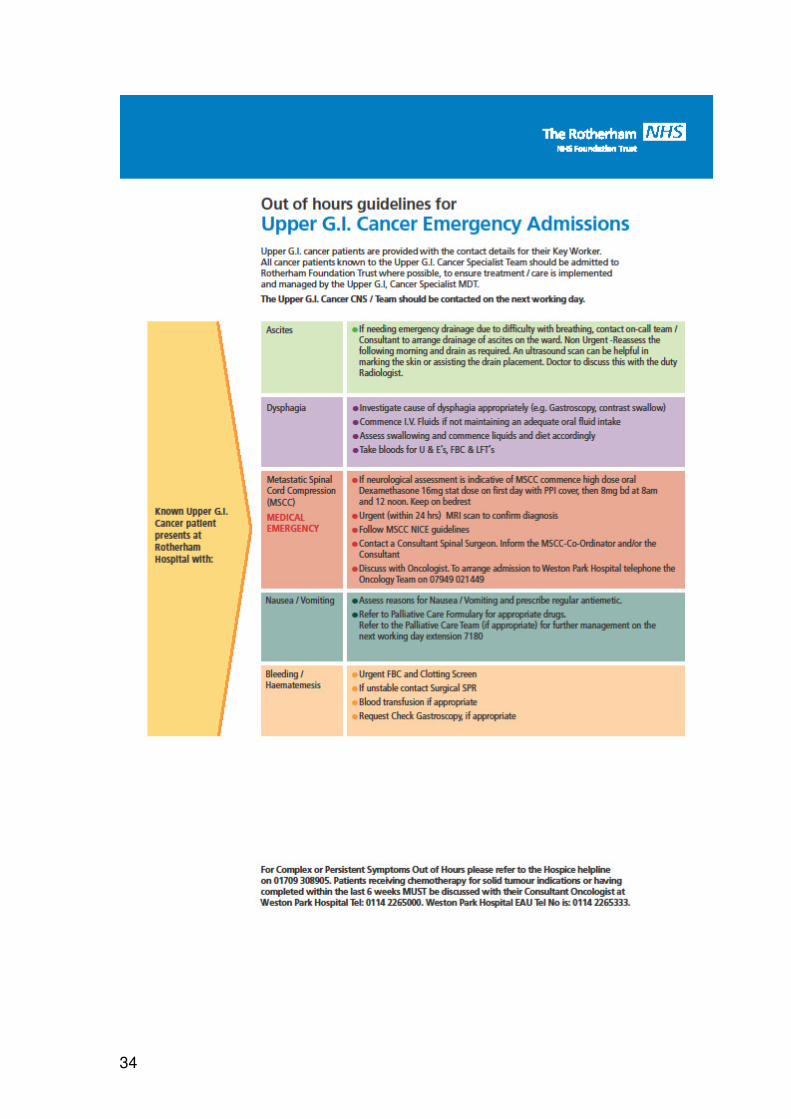
11-1E-104y Guidelines for Emergency Admissions – Page 34 The example used in Rotherham (developed by Doncaster from work done by the Sherwood Forest Foundation Trust) has to been adapted for each trust and used across the network. All trust may have slightly different formats but all contain the same criteria. Treatment protocols have been adapted into a generic form for use across the Network (see the example for anaphylaxis below page 36.) Guidelines for referral for MSCC are included in Appendix 3 Annual Report Other protocols included are:-
Radiotherapy induced mucositis.doc
Radiotherapy induced nausea.doc
Radiotherapy induced oesophagitis.doc
Radiotherapy induced nausea.doc
Radiotherapy induced mucositis.doc
Radiotherapy induced diarrhoea.doc
Radiotherapy induced cerebral oedema.doc
Radiotherapy induced acute skin reaction.doc
Radiotherapy induced acute skin reaction.doc
Radiation induced pneumonitis.doc
Thrombocytopenia Induced Bleeding.doc
SOL AOS.ppt Neutropenic Sepsis Policy network.doc
lymphangitis carcinomatosis AOS.ppt
hypomagnesaemia AOS.ppt
extravasation2AOS.doc
extravasation1AOS.doc
ascites AOS.ppt AOS SCC.pdf AOS CVAD.ppt
Chemotherapy induced nausea and vomiting.doc
Chemotherapy induced mucositis.doc
Chemotherapy induced diarrhoea.doc
Emergency management of Spinal Cord Compression (SCC.ppt
Pleural Aspiration.doc
Hypercalcaemia pathway comments.doc
Hypercalcaemia pathway 2.doc
SUPERIOR VENA CAVA OBSTRUCTION.doc
34

35

36
Example of a protocol for AOS - anaphylaxis Action to be taken if patient presents with anaphylaxis Action Rationale
1. Stop infusion/ treatment. The hypersensitivity reaction is affected by the quantity of the trigger
2. Assess airway, breathing, circulation To determine extent of reaction and help required
3. Call for immediate emergency help – stay with the patient and provide reassurance
Patients condition may deteriorate very quickly
4. Place the patient in a reclined position of comfort
Lying flat may help hypotension but breathing difficulties also need to be supported
5. Start oxygen at high flow rate (10 to 15 litres per minute)
To increase oxygen saturation levels
6. If the patient has stridor, wheeze, respiratory distress or clinical signs of shock administer adrenaline (epinephrine) 1:1000 solution 0.5 ml (500 micrograms)* IM
To reverse peripheral vasodilatation and reduce oedema. The IM route is more effective and associated with less complications than other routes of administration
7. Change IV giving set and administer rapid infusion of IV 0.9% sodium chloride
To increase circulating volume of blood. A crystalloid may be safer than a colloid
8. Check vital signs – BP, pulse, respirations, oxygen saturations
To aid assessment of the patients’ condition
9. Repeat adrenaline (epinephrine) 1:1000 solution 0.5 ml (500 micrograms)* IM if there are no signs of clinical improvement
To reverse peripheral vasodilatation and reduce oedema.
10. Administer chlorphenarimine 10 - 20 mg by slow IV injection or IM injection
To counteract histamine mediated vasodilatation
11. If severe anaphylactic reaction administer hydrocortisone 100 mg IV
Plays a role in preventing late effects of the reaction
12. If hypotension does not respond to drug treatment administer rapid infusion of 1-2 litres IV 0.9% sodium chloride
To increase circulating volume of blood. A crystalloid may be safer than a colloid
13. If patient has bronchospasm consider giving nebulised salbutamol
To treat bronchospasm
14. Discuss with the doctor the need to monitor the patient post anaphylaxis event. If the patient is discharged from hospital warn them of the possibility of recurrence of symptoms and the need to seek urgent medical attention if they do occur
To ensure appropriate post anaphylaxis care. Anaphylaxis reactions can recur in some cases 8 - 24 hours after the initial reaction.
15. Document the episode in the medical and nursing notes. Inform the patients’ general practitioner of the event. Advise the patient that they need to try and avoid future exposure to the suspected allergen trigger.
To try and prevent repeat anaphylaxis reactions.

37
The Network agrees that all localities will adhere to common agreed best practice guidelines specifying
• Where a patient will be managed
• Referral processes
• Treatment guidelines / indications for each tumour site
• Oncological emergencies 11-1E-105y Network information on early detection of MSCC Patient Information MSCC, examples from Sheffield and Chesterfield are included in Appendix 1 It is expected that all patients at risk of this condition are advised of their risk and provided with appropriate information. Information leaflets are available from all relevant MDT teams. Leaflets are available on NTCN website Local contact points are via patients GP’s and links to acute oncology services available for primary care. All patients and advised of their local contact points The referral process is outlined in NTCN Referral guidelines Appendix 3 of the Annual Report document and Appendix 3 for 2WW pathway in this document.

38
11-1E-106y/107 Acute Oncology Training in the use of services. Each locality within the Network should provide induction training to inform all their staff of Acute Oncology services and how to access them. There should be a local plan to ensure that it is given to all new starters to organisations and particularly to all staff working on Medical admissions units, A&E and junior doctors. The training should include and cover at least the following:-
1. A description of the network configuration of the acute oncology service and where they are based in each of the localities
2. An awareness and understanding of the acute oncology referral guidelines and how individual patients should be managed
3. The protocols associated with the acute oncology service 4. The roles and responsibilities and relevant contact points for the
following:-
a) The Network Acute Oncology Group b) The Hospital Acute Oncology Teams
c) The Acute oncology assessment service in their area d) How to access the North Trent 24/7ChemotherapyPatientAdvice service e) The process to access Fast Track referrals for patients to attend the appropriate Outpatients clinics in their organisations f) Awareness of The Consultant ‘On Call’ service and how to access this g) How to contact the MSCC Hospital Coordinators h) How to contact the MSCC Clinical Advisors for both surgery/radiotherapy
It is important that the information should contain locally specific information. It is expected that this training will be individual to each locality and will be delivered locally due to understanding of their own geographical location and processes. All organisations will have different emergency access configurations so requiring this approach There is a requirement for localities to keep written records of the training completion The training itself maybe delivered in a variety of formats i.e. face to face, e learning. Within North Trent cancer network, all organisations have developed their own individual training packages, which incorporate the above requirements. As example of training already undertaken, the South Yorkshire Programmes for Education in cancer care have developed a programme to
39
cover issues around Acute Oncology services and will continue to be delivered. Please see full Training Policy in Appendix 4 Training for MSCC Co-ordinators. Within North Trent we operate a system where Clinical advisors act as the coordinators for this emergency condition. The Clinical advisors are Consultant surgeons, Oncologists and Radiologists Please see MSCC Referral Guidelines (Appendix 3 Annual Report)
11-1E-108y There is a separate Network MSCC subgroup The Network Metastatic Spinal Cord Group
Core Group
Joint Chairs Mr N Chiverton Spinal Surgeon Sheffield Teaching Hospitals Dr D Brooks Consultant in Palliative Medicine Chesterfield Royal Hospital Medical Members Dr A.Cheema Consultant in Acute Medicine Sheffield Teaching Hospitals Dr M. Fernando Consultant in Palliative Medicine Doncaster & Bassetlaw Dr B Foran Consultant Clinical Oncologist Sheffield Teaching Hospitals Dr C Ingram Consultant Radiologist Sheffield Teaching Hospitals Dr O Purohit Consultant Clinical Oncologist Sheffield Teaching Hospitals Dr A Arefin Consultant Physician Rotherham Hospital(June 2012) AHP Members Suzanne Hodson Physiotherapist Sheffield Teaching Hospitals Sarah Nichol Occupational Therapist Ashgate Hospice
Roles Assigned to Core Members
Imaging Lead Dr C Ingram Consultant Radiologist Sheffield
Non Core members
Management Support Judith Bird Network Lead Nurse NTCN
Administrative Support
Lin Jameson Groups & Projects Support Officer NTCN

40
Interested Practitioners Who Receive Minutes Dr P M Fisher Clinical Director
Weston Park Hospital Sheffield Teaching
Hospitals Dr Kevin Bolster Speciality Doctor in
Palliative Care Rotherham Hospice
Dr R Cullen
Primary Care Cancer Lead NTCN
D Hughes Lead Cancer Clinician Sheffield Teaching Hospitals
N James Lead Cancer Nurse Chesterfield Royal Hospital
41
NAME OF GROUP: Network Site Specific Group (NSSG)
Cross Cutting Group (CCG)
ACCOUNTABLE TO:
The North Trent Cancer Network Board (including clinical and corporate governance). The MSCC CCG Chair is a member of the Network Lead Clinicians Group and as such is responsible for ensuring risks associated with the delivery of services are fed into the network planning process.
PURPOSE: The MSCC CCG has responsibility, delegated by the Board, for ensuring the co-ordination of the cancer pathway and the consistency of care for the relevant client group within the cancer network. This includes:
• Service planning
• Service Improvement / Redesign
• Service Quality Monitoring and evaluation including clinical performance and outcomes
• Workforce Development
• Research and Development The Network tumour-site specific groups should have the active engagement of all MSCC leads from all the relevant constituent organisations in the network. MSCC should ensure that all agreed operational changes are discussed with local managers to ensure that changes are integrated into constituent organisational structures and processes. Discussions to explore other changes to existing patient pathways may be initiated by commissioners including Primary Care. MSCC provides advice in respect of all significant service changes (e.g. IOG) particularly if there are financial consequences, and will make recommendations to the Cancer Board. The MSCC has a key role in: Developing plans to implement Improving Outcomes Guidance Monitoring the implementation of the agreed Improving Outcomes guidance action plans. Raising concerns and areas of risk to the Board via the agreed governance arrangements.
COMPOSITION OF • Chair of the MSCC CCG
NORTH TRENT CANCER NETWORK (NTCN)
NETWORK Metastatic Spinal Cord Compression Cross Cutting Group TERMS OF REFERENCE
April 2010

42
MSCC CCG: • The MSCC lead clinician from each organisation in the network
• Nominated Oncologist
• Radiologist
• Specialist Surgeons /Emergency Physicians
• At least one nurse core member of a MDT
• A service improvement staff representative
• Palliative care lead
• Two user representatives* * For any one NSSG, the network partnership group can agree an alternative mechanism for obtaining user advice.
The following members are optional: As many other members of those MDTs e.g. Physiotherapy, Speech and Language therapy as appropriate
• A Primary Care Cancer Lead
• A manager representative (from a PCT, provider or NORCOM HQ)
• As a minimum, involve users in their service planning and review
Each CCG will list all its members.
COMPOSITION OF CCG:
The composition of each cross cutting group includes a representative from each locality of each specific cross cutting group, and where appropriate wider membership will reflect National Guidance. All groups will review membership annually, and record attendance as per National Guidance.
CHAIR: The MSCC CCG will select its own chair and deputy. Tenure in each role should be reviewed after 3 years. The Chair should have an annual appraisal.
CHAIR’S EXTRA-MEETINGS ROLE
The Chair will: -
• Ensure engagement of constituent members.
• Attend development programmes organised for the Lead Clinicians
• Facilitate the identification and agreement of the service priorities for the CCG
• Recommend priorities to the Network Board.
• Ensure an annual report of the CCGs work is written
• Have an annual (review) meeting with the Network Lead Clinician and the outcomes agreed by the Network Chair.
• Be an ambassador for service improvement locally and the CCG, regionally and nationally.
INDIVIDUAL ROLES:
Each core member should attend 50% or more of the CCG meetings. It is assumed that their employers will protect the time commitment entailed. One of the NHS-employed CCG members will be named as having specific responsibility for users' issues. One of the NHS-employed CCG members will be named as having specific responsibility on information for patients and carers. One of the NHS-employed CCG members will be named as having

43
specific responsibility on service improvement* ie being a champion for it. None of the above three roles are mutually exclusive. Members should ensure that all decisions become integrated into constituent organisational structures and processes * but not the member of service improvement staff.
DECISION MAKING PROCESS:
All attendees at the CCG meeting will have a vote. Recommendations to the Board will normally be achieved through consensus; however, when a vote is required it is essential that the split of votes is recorded to aid the understanding of the Board in the decision making process
QUORUM: The meeting is quorate when 50% of the constituent core members are represented at the meeting, but the chair can declare a larger meeting non-quorate if key members are not present.
RESPONSIBILITIES:
NB this (long) list of responsibilities assumes the regular input of provider managers and network officers. Service Planning is in line with: 1 National guidelines and advising commissioners and provider
trusts of the implications of that guidance for the whole network. 2 Identifying any risks within the service and developing a network-
wide service delivery plan to deliver the NHS Cancer Plan. 3 Responding to Improving Outcomes Guidance recommendations
and advising commissioners on appropriate patient pathway (or model options) developments within North Trent, which will deliver patient care within those recommendations. Developing efficient working models aligned to good practice guidance and national policy drivers.
4. Agreeing common standards including referral pathways, revised
in light of national policy or guidance, patient care pathways (from primary care, both into and out of tertiary services). This includes updating and revising referral guidelines as appropriate. In time a service specification will be generated.
5. Agree on priorities for data collection, produce audit data and
participate in open review including the user experience and service user evaluation
6. Monitor progress on meeting national cancer measures, trial entry
and ensure action plans agreed at Peer Review are implemented.
7. Reviewing approved clinical trials, and other research, once a year. Agreeing a single list of clinical trials and studies into which the network’s MDTs should give priority for patient entry.

44
8. Develop clear cancer workforce recommendations that foster new ways of working so that services are robust in the face of recruitment difficulties and emergent technologies.
9. Foster strong working relationships to develop network-wide
resolution to workforce issues
10. Liaising and consulting with the relevant "cross cutting" network groups to identify issues that have wider implications and consequent knock on effects. This includes chemotherapy; imaging; histopathology (and other laboratory investigations); specialist palliative care, with the Head of Service for radiotherapy, Children and Young People and Primary Care.
FREQUENCY OF MEETINGS:
At least once every 6 months. Additional meetings may be necessary for short term task and finish projects e.g Peer Review preparation, IOG implementation
SERVICED BY: Cancer Network Office (2 days per meeting, but 9 days pa max) 3
COMMUNICATIONS:
Outward – NSSG/CCG lead to give feedback to the Lead Clinicians Forum and present findings, with recommendations, to the Network Strategy Group
- MDT leads to share items of news with fellow MDT members and with local managers
- NSSG (lead) to write an annual report - NSSG to write an annual work programme for Board endorsement
News can be placed on the network’s website
http://www.northtrentcancernetwork.nhs.uk Agreed guidelines will be downloadable from there.
MINUTES CIRCULATED TO:
CCG members Network Lead Clinician
Cross-Cutting Groups Leads Primary Care Cancer Leads
REVIEW DATE: July 2012

45
11-1E-109y MSCC Clinical Advisor service - See Algorithm Appendix B in the MSCC Guidelines (extract below) In Annual Report document 11-1E-110y MSCC Case discussion policy - See Algorithm Appendix B in the MSCC Guidelines particularly the information in the extract below “URGENT Referral/opinion- Spinal surgical team (Northern General Hospital-Sheffield) for decompression and spinal stabilization-Tel:0114 2715244 (08:00 17:00) Out of hours-Spinal Surgeon on call via Northern General hospital switch board ( 0114 2434343) Referral proforma to be completed ( internet link) North Trent Cancer Network-guidance notes ( internet link)
Note: Need Consultant to Consultant discussion
Referral to Oncology team for Radiotherapy at Weston Park Hospital-Sheffield as appropriate depending on the outcome from discussion with the Spinal surgical team “ 11-1E-103y Consultant Oncologist Telephone ‘On Call’ Service The detail required of this service is contained in the Cancer chemotherapy specification (full copy available).The specification was approved at the Chemotherapy Strategy group meeting on the 6th September 2011 Minutes in hard copy evidence. Relevant extract from service specification below and Triage tool for calls to the service included:- 3.3 Pathways
All providers are required to follow the generic network chemotherapy pathways and locally customised developed pathways, and to set up planned audit against the pathway. Outcomes (including morbidity and mortality, waiting times) will be monitored as part of the quarterly review. Where local pathways exist for solid tumour oncology they should be designed to show clearly the links with the Oncology Centre, including how a patient enters, is managed and discharged from the service. All pathways should include timelines and alert mechanisms for potential breaches, audit processes to ensure standards are met, and specification of provider and commissioner responsibilities. The provider(s) should meet standards for prescribing, adhere to the required competency checks and should foster a responsive and participative approach to including patients’ views about their care in the design of care pathways, and should collaborate with other organisations involved in the patient pathway to provide a seamless patient journey. At entry to pathway, the provider must have systems and processes in place to

46
• register patients
• collect relevant clinical and administrative data
• manage the appointment process, (reappointment and DNA process, if appropriate)
• provide information to patients
• undertake initial assessment in the appropriate location At point of intervention, the provider must have systems and processes in place to ensure that:
• the intervention is conducted safely and in accordance with accepted quality standards and good clinical practice.
• the patient receives appropriate care during the intervention(s), including on treatment review and support, in accordance with best clinical practice
• where clinical emergencies or complications do occur they are managed in accordance with best clinical practice
• the intervention is carried out in a facility which provides a safe environment of care and minimises risk to patients, staff and visitors
• the intervention is undertaken by staff with the necessary qualifications, skills, experience and competence
• There are arrangements for the management of out of hours care according to best clinical practice
• There is communication with primary care At exit from pathway, the provider must have systems and processes, which are agreed with all parties and networks, in place to:
• undertake telephone triage
• make urgent onward referrals where life-threatening conditions or serious unexpected event occur during an intervention/assessment
• ensure that patients receive discharge information relevant to their intervention including arrangements for contacting the provider and follow up if required
• provide timely feedback to the referrer re intervention, complications and proposed follow up
• ensure that the patient receives required drugs/dressings/aids
• ensure that support is in place with other care agencies as appropriate 3.4 Treatment Protocols and Interventions
All providers are required to follow evidence-based treatment protocols and interventions as agreed with the North Trent Cancer Network and adherence to the external accreditation and / or internal quality assurance processes for chemotherapy. Treatment protocols/interventions
Include all individual treatment protocols in place within the service or planned to be used including: • Individual systemic therapies

47
• Drug reconstitution and handling • Drug spillage • Cytotoxic disposal • Other, e.g. management of emergencies (anaphylaxis, cardiac arrest,
extravasation etc), complications of systemic therapy, febrile neutropenia etc
• Information on how to contact clinical staff throughout the 24 hour period
Services should ensure that patients do not have to wait longer than one hour before start of treatment where an appointment time has been given for chemotherapy to be administered on a subsequent day. Where chemotherapy is to be given on the same day as the assessment/consultation, any delays should be communicated to the patient immediately.

48

49

50

51

52

53
54

55

56
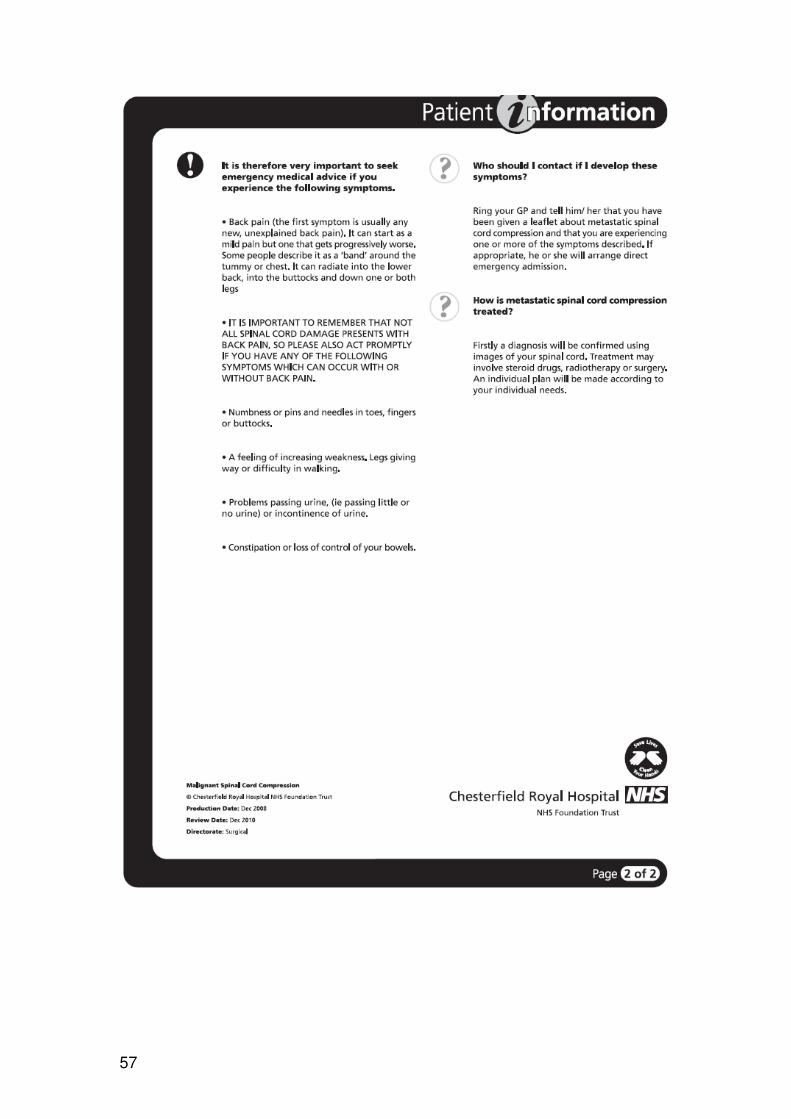
Appendix 1 11-1E-105y Examples of Patient information – 1.Chesterfield
57

58
2. - Sheffield

59

60

61

62
Appendix 2
Acute oncology triage and assessment (Held 29th September and 31st October 2011)
Programme 9. 15 Coffee and Registration 9 .25 Welcome and introductions Kam Singh 9. 30 Acute oncology including renal
failure, dehydration and tumour lysis syndrome
Dr Kate Shankland
10. 30 Tea 10. 55 Telephone assessment review Kam Singh 12. 00 Lunch 12. 45 Telephone assessment guidelines
and reporting forms Clare Warnock/ Charlie Osguthorpe
14.00 Acute oncology – complications of
cancer treatment Dr Matt Winter
• Nausea and Vomiting • Infection and use of growth
factor support
• Thrombosis • Hypercalcaemia • Management of hypotensive
cancer patient
14. 45 Tea 15.00 Scenarios and workshops 16. 15 Evaluations and close

63
Target audience: CNS / triage nurses / allied health professionals / junior doctors Introduction to Acute Oncology at STH
• Background / Need for Acute Oncology service NCEPOD etc
• Service structure (Central campus vs. Northern Campus)
• How to contact us
• Patients we want to know about (This session will cover some of the peer review requirements of induction training for acute oncology. For people who could not attend could be available electronically with read receipt etc) Morning session
• To cover early recognition, evaluation and immediate management of o Acute oncology presentations caused by disease o Complications of systemic treatment of cancer o Complications / Adverse effects of radiotherapy o Triage Assessment tools (Clare Warnock)
Afternoon session could include
• Malignant Spinal Cord Compression
• Palliative Care and Acute Oncology
• Update on specific areas e.g. cardiology in oncology, site specific updates
• Problem based scenarios and discussion e.g. off legs, nausea and vomiting, Fever, SOB (Group working)

64
Appendix 3
Proforma for Metastatic Spinal Referrals Emergency Referral (phone call already made) / Referral for urgent opinion* Delete as appropriate
Please complete as fully as possible and fax to: 0114 2266796
Patient details Referrer details
Surname: Hospital:
Forename: Ward:
Gender: Direct dial number:
D.O.B.: Consultant i/c:
Address: Contact number:
Date of admission:
: Time of admission:
Date of referral:
Telephone no: Time of referral:
Current co-morbidities Is patient's Oncologist aware of referral? Y / N / NA
1) Is the patient anticoagulated? Y / N
2) Patient understanding
3) Has diagnosis been discussed with the patient? Y / N
4) Does the patient wish to consider surgery? Y / N
Tumour presentation Available Imaging
Known primary Whole spine MRI Y / N
Unknown primary (investigations complete) (Date and time of MRI):
Unknown primary (Investigations incomplete) CT chest / abdo / pelvis Y / N
Prognosis >3 months Y / N / ? Bone scan Y / N
PLEASE ENSURE ALL IMAGING IS UPLOADED TO NGH PACS SYSTEM
Performance status (prior to onset of spinal symptoms) (tick)
0 Fully active
1 Fully ambulant. Restricted with strenous activities only
2 Fully self caring.
3 Limited with self care. Resting for >50% of waking hours
4 Completely disabled. Totally confined to bed or chair
PLEASE COMPLETE THE NEXT PAGE

65
Patient name: D.O.B.:
Primary tumour site Pain Symptoms
Breast Prostate Renal Pain Y / N since (date):
Lung Myeloma Lymphoma Level / location:
Thyroid GIT Urothelial Type Non-specific Mechanical Neuralgic
Uterine/Cx Melanoma Pattern Nocturnal Diurnal Constant
Other (specify): Analgesia Minor Major
Date of diagnosis: VAS Score: __ / 10
Primary treatment: Neurological symptoms
Describe:
Adjuvant treatment Current walking status
1) XRT to spinal met Y / N Normal
2) Unsteady since (date):
3) Non-ambulant since (date):
Metastases Continence
Extra spinal bone mets Y / N Urinary incontinence Y / N since (date):
Visceral mets Y / N Faecal incontinence Y / N since (date):
Liver Lung Anal tone Normal Reduced Absent
Brain Adrenal Perineal sensation Normal Reduced Absent
Lymph nodes Other Catheter tug Felt Not felt N/A
Power
Most distal myotome with normal power
MRC grade of weakest muscle(s)
Details of clinician to be responsible for ongoing care of the patient following surgery
Name: Contact number:
If you wish to discuss a referral please contact the on-call spinal surgeon on 0114 2715244 during office hours or otherwise via the NGH switchboard (0114 2434343)
Sensation
Normal Reduced Absent
Most distal dermatome with normal sensation:
Other relevant Information:

66
Appendix 4
Network Training in Acute Oncology Services Measure 11-1E-106y/107 Review Date April 2013

67
NTCN Acute Oncology Training in the use of acute oncology services. Introduction It is the networks view that all localities should provide training to all relevant staff as outlined in the Acute Oncology National Cancer Peer Review Measure1within their organisations about Acute Oncology services and provide regular awareness sessions and updates to existing staff in their organisations This policy is intended to introduce the concept of Acute Oncology and to provide guidance on the Acute Oncology process for all medical and nursing staff involved directly in the assessment and admission of known cancer patients presenting as unscheduled attendances. Background An Acute oncology service is designed to be a process to meet the needs of cancer patients who become acutely unwell or develop a new problem associated with their treatment and/or their disease and which needs urgent care, often by presentation to an emergency department. Some problems e.g. neutropenic sepsis following chemotherapy can be life threatening conditions unless treated promptly and correctly. Others such as spinal cord compression may lead to permanent disability and subsequent poor quality of life. Sometimes the development of a new, urgent medical problem is the presentation of an underlying undiagnosed cancer. Acute Oncology as a service is a relatively new development in Cancer Services. The development of an acute oncology infrastructure came from recommendations of the National Chemotherapy Advisory Group (NCAG): Chemotherapy Services in England: Ensuring Quality and Safety in 2009 and the NCEPOD Report: For Better, For Worse in 2008 which examined the incidence of deaths within 30 days of systemic anti-cancer treatment (SACT). These reports concluded that there were patient deaths due to complications of treatment that could have been avoided and that there was a need for better communication and coordination between services. Which patients does Acute Oncology apply to?
Any patient with an existing cancer diagnosis (solid tumour or haematological) who has an urgent problem related to:
• A complication of recent cancer treatment (acute side effects during treatment or within 6 weeks of administration). Late effects of treatment
1 National Cancer Peer Review Programme
Manual for Cancer Services: Acute Oncology - Including Metastatic Spinal Cord Compression Measures Version 1.0 April 2011
68
can develop months and years after treatment but are less likely to present as an emergency
• A new problem caused by the cancer itself or a consequence of the cancer illness. e.g. a bleed from a tumour, a fit caused by a brain metastases or systemic infections. Some of these are extreme oncological emergencies and staff should to be familiar with the common causes and how to manage them.
• A new acute problem that might be the first sign of a recurrent cancer – in patients who have had previous treatment e.g. surgery
• A presentation of a previously undiagnosed cancer – particularly when there is evidence of widespread metastases and no known primary site of origin (cancers of unknown origin)
The emphasis of the Acute Oncology Service is non-surgical management since guidelines and care pathways concerning acute post-operative emergencies are normally well established and would supercede any others. The noticeable exception to this is the initial surgical management of patients presenting with Metastatic Spinal Cord Compression (M.S.C.C) Cancer patients may also present to emergency departments with problems that are considered to be unrelated to their cancer and which are a manifestation of co-morbidity. In general these presentations will not be referred to the Acute Oncology team although it might be appropriate to seek their advice if the patient is on current treatment or there is uncertainty as to whether the presenting problem is a consequence of the cancer and/or its treatment. Advantages of an Acute Oncology service For Staff Cancer management is becoming increasingly complex. All staff that sees these acute patients needs to have prompt access to up to date clinical information about a patients cancer, treatment details, aims and prognosis. There should also be easy access to specialist oncology advice, both during the working day and outside of working hours for members of the Acute Oncology team including non-surgical oncologists who may be sited at the Cancer Centre. For Patients The aim of Acute Oncology is to improve both the safety and quality of care:
• Safer cancer treatments – with side effects managed promptly and correctly

69
• Management of cancer problems – co-ordination of expertise in emergency care, non-surgical oncology, haemato-oncology and palliative care
• More efficient pathway management with fewer, potentially avoidable admissions, unnecessary tests and investigations and shorter lengths of stay
• Greater confidence for patients and carers in teams that have access to up to date clinical information, who understand the concept of acute oncology and who communicate effectively with each other
Locality Training Requirements Each locality within the Network should provide induction training to inform all relevant health care professionals according to the Acute Oncology Cancer Peer Review Measures (2011)2 and how to access them. There should be a local plan to ensure that it is given to all new starters to organisations and particularly to all staff working on Medical admissions units, A&E and junior doctors. It is important that the information should contain locally specific information. It is expected that this training will be individual to each locality and will be delivered locally due to an understanding of their geographical location and processes. All organisations will have different emergency access configurations so requiring this approach. In addition to this, training is provided by South Yorkshire Programme Education in cancer care, around oncology issues and this can also be accessed from other areas. Any local training in the use of the acute oncology service is expected to apply to Consultant Oncologists and to the hospital acute oncology assessment rota staff in all the hospitals who take part in such a rota (Measure11-3Y-403) It should also be part of the training for the staff who take part in the Consultant oncologist 24/7 on call rota and the 24/7 chemotherapy advice service rota should be trained in the use of an acute oncology service if that hospital provides such a service. (Measure 11-3Y-305) It also expected that the training should include an assessment process which ascertains the treatment intent and addresses Palliative and End of life issues The education policy should be developed in conjunction with existing policies already developed by NTCN for example
2 National Cancer Peer Review Programme
Manual for Cancer Services: Acute Oncology - Including Metastatic Spinal Cord Compression Measures Version 1.0 April 2011

70
http://www.northtrentcancernetwork.nhs.uk/Downloads/Chemotherapy-Guidelines/Microsoft%20Word%20-%20chemo%20ed%20v3.pdf There is a requirement that the training should include at least the following 5. A description of the network configuration of the acute oncology service
and where they are based in each of the localities 6. The roles and responsibilities and relevant contact points of key personnel
in oncology services by locality and network wide including
• The Network Acute Oncology Group
• The Hospital Acute Oncology teams,
• The Acute Oncology Assessment service,
• The 24/7chemotherapy patient advice service
• How to fast track referral to out patient clinics
• How to access the consultant on call service
• How to access the MSCC co coordinators
• How to access the MSCC clinical advisors
3. An awareness and understanding of the acute oncology referral guidelines and how individual patients should be managed 4 The protocols and pathways associated with the acute oncology service 5. Contain locally specific information 6. Confirmation of completion of this training as part of induction should be kept and regularly updated.

71
1. A description of the network configuration of the acute oncology service and where they are based in each of the localities
Weston Park HospitalNo A+E
No Acute medicine beds
Northern General •A & E•Palliative Care Unit•Acute Medical Beds
•No OP Chemo
Royal Hallamshire
•No A+E •No Acute Medicine beds•Haem beds•OP Chemo
Hospice Palliative care
beds
Barnsley •A+E
•Acute medical beds•OP Chemo (Onc)•Haem Beds
Hospice Palliative care
beds
Bassetlaw •A & E•No OP chemo
Doncaster•Haem beds•OP Chemo (Haem + Onc)•A & E
HospicePalliative care
beds
Chesterfield Royal •A+E•Haem beds
•OP Chemo•Acute medical beds
Rotherham•A+E•OP Chemo•Haem beds•Acute medical beds
Hospice
Palliative care beds
NTCN Acute Oncology Service
STHFT
HospicePalliative care
beds

72
2. The roles and responsibilities and relevant contact points
HOSPITALS PROVIDING ACUTE CARE IN NORTH TRENT CANCER NETWORK AND THE HOSPITAL ACUTE ONCOLOGY TEAMS CONTACT DETAILS ARE AVAILABLE LOCALLY FOR ALL SERVICES
Designated Lead AOS Clinician/Team
Hospital Host Organisation
Referring PCT
Population (not weighted)
MSCC treated
Dr Julian Humphrey Consultant in Emergency Medicine
Barnsley District General Hospital
Barnsley Hospital NHS Foundation Trust
Barnsley Primary Care Trust
234,397
No
Dr Mansur Reza Consultant in General Medicine
Chesterfield Royal Hospital
Chesterfield Royal Hospital NHS Foundation Trust
Derbyshire County Primary Care Trust
320,000
No
Doncaster Primary Care Trust
No Dr Joe Joseph Consultant Haematologist
Doncaster Royal Infirmary and Bassetlaw Hospital
Doncaster & Bassetlaw NHS Foundation Trust
Bassetlaw Primary Care Trust
291,624 106,691 No
Dr Ahmed Arefin, Consultant Physician
Rotherham Hospital
Rotherham Hospital NHS Foundation Trust
Rotherham Primary Care Trust
243,151 No
Dr Matthew Winter Consultant Medical Oncologist
Yes Surgery at NGH
Dr Peter Kirkbride Consultant Clinical Oncologist
Sheffield Teaching Hospitals
Sheffield Teaching Hospitals NHS Foundation Trust
Sheffield Primary Care Trust
550,513
DXR at WPH

73
Network Acute Oncology Group The Network Acute Oncology Group is a subgroup of the Network Chemotherapy Strategy Group and reports into this group Details of the members and activities of the group are available in the Network Acute Oncology Group Constitution document and on the NTCN website. All localities from the Network are represented on this group and contact details should be available locally.
In addition it is expected that the training should provide
3. Awareness and understanding of the acute oncology referral guidelines and how individual patients should be managed and the purpose of the Acute Oncology team.
Acute Oncology Presentations
Each Hospital will diagnose and treat with appropriate consultation with the cancer centre the following caused by the systemic treatment of cancer in line with NTCN agreed guidelines. Weston Park Hospital does not manage either Pleural or Pericardial effusions
The current network policy is that the all patients receiving chemotherapy treatment for solid tumours contact Weston Park Hospital directly and are admitted to WPH for treatment. However, in view of the fact that some patients will present locally despite this, all units need to have processes in place to ensure that patients who present directly to them via A&E are promptly assessed and treated in discussion with WPH. When patients are stable they should then be transferred to WPH at the earliest opportunity. The following, as caused by systemic anti-cancer treatment:
• Neutropaenic sepsis
• Uncontrolled nausea and vomiting
• Extravasation injury
• Acute hypersensitivity reactions including anaphylactic shock
• Complications associated with venous access devices
• Uncontrolled diarrhoea
• Uncontrolled mucositis
• Hypomagnesaemia The following, as caused by radiotherapy:

74
• Acute skin reactions
• Uncontrolled nausea and vomiting
• Uncontrolled diarrhoea
• Uncontrolled mucositis
• Acute radiation pneumonitis
• Acute cerebral/other CNS oedema The following, caused directly by malignant disease and presenting as an acute problem. This section may refer to patients with known malignant disease, whether they are picked up by the hospitals ‘flagging system’ or not, or patients with previously unknown malignant disease:
• Pleural effusion
• Pericardial effusion
• Lymphangitis carcinomatosa
• Superior mediastinal obstruction syndrome, including superior vena cava obstruction
• Abdominal ascites
• Hypercalcaemia
• Spinal cord compression including M.S.C.C
• Cerebral space occupying lesion(s) Any other cases where the A&E staff and acute medical firm decide an urgent oncology assessment is needed. Assessing the Cancer Patient in the Emergency Department When a known cancer patient attends the emergency department an Acute Oncology Assessment Proforma should be completed. The documentation is designed to assist clinicians with the assessment and to help determine the need for admission (Appendix 1) This documentation maybe different in each locality but should take account of at least the following factors. Patient assessment Type of cancer and sites of disease

75
Name of oncologist (haematologist) with overall management, hospital where seen for treatment/follow-up, key worker name Names contact details, hospital number Are they currently on chemotherapy/radiotherapy treatment or completed in the last 6 weeks Date of last treatment When last seen Current medication Prognosis and treatment intent Currently on treatment /not started Is the problem related to cancer treatment/Infection/EOL/Unrelated to cancer Patients and carers understanding and expectations The Acute Oncology Team The Acute oncology team is not an MDT. This team’s role is not intended to be one of dealing with the care of individual patients although individual members may be involved with Acute Oncology problems in the course of their everyday practice. The team is organisational, dealing with Acute Oncology policies, protocols and procedures. The team will have the designated responsibility from the hospital management to:
• Act as the coordinating body for matters relating to acute oncology between the hospitals directorates and departments and between the hospital and other hospitals in the Network.
• Ensure the implementation and compliance with the Acute Oncology Cancer Peer Review measures for the hospital
• Report to the N.A.O.G and the hospital management team Metastatic Spinal Cord Compression It is recommended that any training that is delivered should pay particular attention to raising awareness of Metastatic Spinal Cord Compression and understanding of the local pathways and appropriate referrals to the MSCC service based at the Northern General Hospital In Sheffield. This will require an understanding of:- 1. Metastatic Spinal Cord Compression: early signs and symptoms Contact MSCC co-ordinator urgently within 24 hours to discuss care of patients with cancer and any of the following symptoms suggestive of spinal metastases:
• Pain in the middle (thoracic) or upper (cervical) spine
• Progressive lower (lumbar) spinal pain
• Severe unremitting lower spinal pain

76
• Spinal pain aggravated by straining (for example, at stool, or when coughing or sneezing)
• Localised spinal tenderness
• Nocturnal spinal pain preventing sleep N.B Most patients who are felt to be particularly at risk of this condition occurring should have already been provided with appropriate information to raise the patients awareness of this risk. This information should include relevant local contact details as felt appropriate Contact the MSCC coordinator immediately to discuss the care of patients with cancer and symptoms suggestive of spinal metastases who have any of the following neurological symptoms or signs suggestive of MSCC, and to view them as an oncological emergency: This is for either Surgery or Radiotherapy
• Neurological symptoms including radicular pain, any limb weakness, difficulty walking, sensory loss or bladder and bowel dysfunction
• Neurological signs of spinal cord or corda equina compression. Referral forms and contact details for this condition are included in NTCN Constitution document and should be part of all organisations local information and training and are on NTCN website. www.northtrentcancernetwork.nhs.uk Training for MSCC Co-ordinators. Measure 11-1E-107y
Within North Trent we operate a system where Clinical advisors act as the coordinators for this emergency condition. The Clinical advisors are Consultant surgeons, Oncologists and Radiologists and have highly specialist knowledge of this condition.
4. The protocols associated with the acute oncology service Network oncology pathways have been developed and cover all the main tumour groups. These have been developed in conjunction with all localities but they may be produced in a slightly different format in each area.
77
In addition there are more comprehensive policies available via the NTCN website e.g. neutropaenic sepsis which has been developed across the network and links into the education and training process. http://www.northtrentcancernetwork.nhs.uk/Chemotherapy-Guidelines/Microsoft%20Word%20-%20Neutropenic%20Sepsis%20revised%202007%20minus%20answers%20ratified%202010%204.pdf Treatment protocols and guidelines for acute oncology presentations should be available electronically and hard copies will also be available prominently in clinical areas. These again should not detract from the need to seek specialist advice from the MDT members/oncologist/Haematologist managing the patient’s cancer. Within NTCN there is a requirement for all ‘solid tumour’ patients being treated or having been treated with chemotherapy in the last 6 weeks and presenting with signs and/or symptoms of neutropenia to be ‘treated and transferred’ to Weston Park Hospital. Assessing clinicians/Health Care Professionals must liaise with the patients own oncologist or the oncologist on call at W.P.H for advice and to arrange the transfer. In the event that Weston Park Hospital does not have any beds available the transfer should be facilitated at the earliest opportunity Contact details included in Appendix 2 and available on NTCN website Fast track Access to OP Clinics The training should address the process of how to access Fast Track referrals for patients to attend the appropriate Outpatients clinics in their organisations. This will require an understanding of a locality Oncologist timetable and services/ specialities provided. Access to Advice and information Training should inform staff on how they can access the North Trent 24/7Chemotherapy Patient Advice service as per flyer Appendix 2 and in addition an awareness of The Consultant ‘On Call’ service and how to access this Training Compliance There is a requirement for localities to keep written records of the training completion There is no specification as to how the training itself should be delivered and can be done in a variety of formats i.e. face to face, e learning.
78
In the future it is planned to develop an e-learning package in conjunction with East Midlands Cancer Network which may support and enhance this work
Within North Trent Cancer Network, all organisations have developed their own individual training packages, which incorporate the above requirements. There is a requirement that localities will provide reassurance to the NAOG that this process is being undertaking on a regular basis and that a list on training completion is kept and updated locally. This will be a regular agenda item of the group. As an example of training already undertaken, the South Yorkshire Programmes for Education in cancer care have developed a programme to cover issues around Acute Oncology services and will continue to be delivered.
Programme included in Appendix 3

79
Appendix 1 AOS Assessment Proforma

80

81
Appendix 3 Example of training programme
Acute oncology triage and assessment
(held 29th September and 31st October 2011 )
Programme 9. 15 Coffee and Registration 9 .25 Welcome and introductions Kam Singh 9. 30 Acute oncology including renal
failure, dehydration and tumour lysis syndrome
Dr Kate Shankland
10. 30 Tea 10. 55 Telephone assessment review Kam Singh 12. 00 Lunch 12. 45 Telephone assessment guidelines
and reporting forms Clare Warnock/ Charlie Osguthorpe
14.00 Acute oncology – complications of
cancer treatment Dr Matt Winter
• Nausea and Vomiting • Infection and use of growth
factor support
• Thrombosis • Hypercalcaemia • Management of hypotensive
cancer patient
14. 45 Tea 15.00 Scenarios and workshops 16. 15 Evaluations and close
82
Target audience: CNS / triage nurses / allied health professionals / junior doctors Introduction to Acute Oncology at STH
• Background / Need for Acute Oncology service NCEPOD etc
• Service structure (Central campus vs. Northern Campus)
• How to contact us
• Patients we want to know about (This session will cover some of the peer review requirements of induction training for acute oncology. For people who could not attend could be available electronically with read receipt etc) Morning session
• To cover early recognition, evaluation and immediate management of o Acute oncology presentations caused by disease o Complications of systemic treatment of cancer o Complications / Adverse effects of radiotherapy o Triage Assessment tools (Clare Warnock)
Afternoon session could include
• Malignant Spinal Cord Compression
• Palliative Care and Acute Oncology
• Update on specific areas e.g. cardiology in oncology, site specific updates
• Problem based scenarios and discussion e.g. off legs, nausea and vomiting, Fever, SOB (Group working)