Embed Size (px)
Citation preview

(WEB: The Eyes have it)
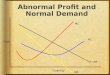
Normal Optic Disc
The optic disc is shaped like a doughnut with a pink neuroretinal rim and a central white
depression called the physiologic cup.
Check out the color of the neuroretinal rim, which carries the axons of the retinal ganglion
cells. It should be orange-pink. If its axons die, the rim will turn white. Inflammation,
infarction, and compression are common causes.
Inspect the external margins of the neuroretinal rim. Are they distinct? Some fuzziness of
the nasal margin is acceptable. Otherwise, the optic nerve may be pathologically swollen,
particularly if the rim rises well above the retinal surface. Common causes of disc edema are
increased intracranial pressure and optic nerve inflammation and infarction.
Inspect the physiologic cup. Its horizontal diameter should not exceed 1/2 the horizontal
diameter of the entire disc (the "cup-to-disc ratio"). Otherwise, suspect pathologic optic disc
cupping. Glaucoma is the commonest cause.
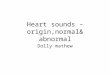
Arteries and Veins of the Normal Optic Fundus

The retinal arteries and veins emerge from the nasal side (left) of the optic disc. Vessels
directed temporally have an arching course; those directed nasally have a radial course.
Arteries are brighter red and narrower than veins. Actually, the retinal arteries lack a
muscular coat, so they are more correctly called arterioles. The vessels you see here supply
and drain the inner retina, including the retinal ganglion cells and their axons and the
bipolar cells. The outer retina, including the rods and cones and retinal pigment epithelium,
is supplied by the choroidal circulation.
The fovea is a 2.5 mm-diameter area that looks slightly darker than the surrounding retina
because of increased pigment. It is centered about 2 1/2 disc diameters temporal to the
optic disc. The fovea lies in the center of the macular region.
Made up exclusively of cones, the fovea processes high-contrast discriminative vision (visual
acuity) and color vision. Without it, you could not see fine detail. The most common disorder

of the macular region in the elderly is age-related macular degeneration, an idiopathic
disorder of the retinal pigment epithelium. Other important macular disorders are diabetic
macular edema, toxoplasmosis, and cherry-red spot.
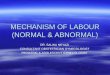
Pathologic Optic Disc Cupping
In this eye, the disc neuroretinal rim is much thinner than in the normal optic disc. The cup-to-disc ratio here is about 0.8—much greater than the physiologic limit of 0.5! When the cup-to-disc ratio exceeds 0.5, optic disc cupping is probably pathologic. This patient has glaucoma. To find out more about glaucoma, click here.
Optic Disc Pallor

In this eye, the neuroretinal rim is much whiter than in the normal optic disc. The pallor
reflects replacement of dead axons by glial tissue. The loss of the small capillaries within the
nerve accounts for the shift from orange-pink to white.
Be careful about judging optic nerve function by its color. First, the color change may be
very subtle. Second, it takes many weeks of optic nerve damage before pallor appears.
Third, a cataract may make a pale disc look orange.
Congenital Optic Disc Anomaly
In this eye, the optic disc is pathologically elevated above the retinal surface. It lacks a
physiologic cup, and its margins are slightly blurred. The signs depicted here are caused by
a congenital optic disc anomaly, leading to overcrowding of axons as they exit the eye.
It is often difficult to tell the difference between a congenital optic disc anomaly and optic
disc edema, an acquired swelling of optic nerve axons caused by increased intracranial
pressure, infarction, or inflammation of the optic nerve.
Acute Optic Disc Edema

The optic disc is elevated and its surface is covered by cotton wool spots and flame
hemorrhages. The cotton wool spots reflect explosion of damaged axons; the flame
hemorrhages reflect explosion of vessels under pressure.
Although blurred optic disc margins and disc elevation can also be caused by a congenital
optic disc anomaly, the cotton wool spots and hemorrhages tell you the disorder is acquired.
Optic disc edema is commonly caused by the four "I's":
increased intracranial pressure (papilledema)
infarction
inflammation
infiltration (by cancer)
Compression and toxins are other causes. You cannot differentiate one cause of optic disc
edema from another on the basis of its ophthalmoscopic appearance! You must use non-
ophthalmoscopic information, such as visual acuity or visual field defect, to make that
distinction.
Subtle Optic Disc Edema

This is an example of subtle optic disc edema. The temporal margin appears quite distinct,
but the nasal, superior, and inferior margins are not. Blurred nasal margins are acceptable in
the normal optic disc, but its upper and lower poles should have discrete borders.
Chronic Optic Disc Edema
This optic disc is elevated and its surface is turning white. The edema tells us that
axoplasmic flow is backed up in some axons. The pallor tells us that other axons have died—
from the effects of axoplasmic stasis!
Patients with this sign have constricted visual fields. The usual cause is chronic elevated
intracranial pressure. At this stage, vision may not improve even if the pressure is relieved
and the optic disc edema disappears. The disc will then be flat but pale.
Arteriovenous Nicking

Chronic hypertension has stiffened the arteries. At arteriovenous crossing points, they
indent and displace the more pliant veins. Called arteriovenous nicking, this phenomenon
does not occur in the normal fundus.
Increased Light Reflection in Chronic Hypertension
Chronic hypertension also thickens the arterioles. Intimal and subintimal fibrosis
narrows their lumina, and gives the red reflection from their blood columns a
shiny appearance (increased light reflection). At first, the light reflection has a
bronze sheen ("copper-wiring"); with continued hypertension, it develops a
whitish glint ("silver-wiring").
Obliterative Retinal Vasculopathy

The white, string-like vessel has been completely occluded by an old thrombus.
Longstanding occlusion of arterioles gives them a thready, white appearance, like a pipe
cleaner.
This patient, who has lupus erythematosus, has visual field loss corresponding to the area of
infarcted retina around this obliterated arteriole.
Hollenhorst Plaque
The yellow fleck trapped at the bifurcation of retinal arterioles is probably a platelet-fibrin-
cholesterol embolus. Called a Hollenhorst plaque, it originated in an atheroma of the cervical
carotid bifurcation.

Most retinal emboli arrive at their stopping points without infarcting the retina, as shown
here. But if they plug an important proximal feeder vessel, they may cause a segmental
retinal infarct and a disturbing visual field defect.
Segmental Retinal Infarct from Embolus
This refractile, yellow fleck is a platelet-fibrin-cholesterol retinal embolus called a
Hollenhorst plaque. It has lodged at a critical bifurcation near the fovea and
caused a moderate-sized branch retinal artery occlusion and a segmental retinal
infarct. The patient would report an area of cloudy vision just above fixation.
Calcific Intraluminal Plaque

l
This white fleck is a calcific embolus that came from the aortic valve. Somehow it did not
cause a retinal infarct!
Retinal Vasculitis
The white cuff that looks like frosting along the vessels is a perivenous lymphocytic
infiltration. Sometimes called "sheathing," it betokens a vasculitis.
Retinal vasculitis occurs in sarcoidosis, Behçet's Disease, multiple sclerosis, and in idiopathic
conditions. But contrary to popular opinion, it is extremely rare in connective tissue
disorders such as lupus. Instead, connective tissue diseases produce multiple bland

occlusions appearing as cotton wool spots, branch retinal artery occlusions, and obliterative
vasculopathy.
Myelinated Nerve Fibers
The white clouds that surround the optic disc represent a congenital anomaly called
myelinated retinal nerve fibers. Myelination does not normally extend onto the retina. When
it does, these clouds appear permanently adjacent to the optic disc. They do not interfere
with vision.
Did you mistake these myelinated nerve fibers for cotton wool spots or retinal infiltrates?
Many people do. They are whiter, larger and denser than cotton wool spots and are almost
always connected to the optic disc. They are unlike retinal infiltrates in having no overlying
vitreous haze.
To review the many other yellow-white things in the retina with which you could confuse
myelinated nerve fibers, check out Yellow-White Things in the Retina.
Cotton Wool Spots

These yellow-white spots are called cotton wool spots. They are caused by retinal nerve fiber
layer microinfarcts. Exploded retinal ganglion cell axons extrude their axoplasm like
toothpaste. Expect to find cotton wool spots arrayed around the optic disc and along the
temporal vascular arcades.
Cotton wool spots have a myriad of causes. Any process that occludes small retinal
arterioles will do this: hypertension, diabetes, HIV, severe anemia or thrombocytopenia,
hypercoagulable states, connective tissue disorders, viruses, lues, Behçet's and many
others.
To review the many other yellow-white things in the retina with which you could confuse
cotton wool spots, check out Yellow-White Things in the Retina.
Roth Spot
The Roth Spot is a white-centered hemorrhage. Actually, it is a cotton wool spot surrounded
by hemorrhage. The cotton wool comes from ischemic bursting of axons; the small
hemorrhage comes from ischemic bursting of a pre-capillary arteriole. Many, many
conditions may cause this. It is not, as often supposed, specific to bacterial endocarditis!

Hard Exudates
These yellow flecks are called hard exudates. They are the lipid residues of serous leakage
from damaged capillaries. The commonest cause is diabetes. Other causes are retinal vein
occlusion, angiomas (Von Hippel-Lindau Disease), other vascular dysplasias, and radiation-
induced retinal vasculopathy.
If you think you could confuse hard exudates with other yellow-white things in the retina
(yes, easily), check out Yellow-White Things in the Retina.
Retinal Drusen
The yellow-white flecks scattered around the macular region are little mounds beneath the
retinal pigment epithelium. They are tombstones of dead retinal pigment epithelial cells. The
commonest cause is age-related macular degeneration, a common but poorly understood
disorder of the elderly.

At this stage, visual acuity may be only slightly abnormal. If the retinal pigment epithelium
dies further, vision will fail as the foveal region turns into a confluent yellow-white area. The
greatest threat to vision, however, is the development of submacular neovascularization,
which can cause bleeding in the retina.
Retinal Infiltrate
The yellow-white area with fuzzy edges is a retinal infiltrate. It consists of inflammatory cells,
dead retinal tissue, and perhaps micro-organisms. Its indistinct margins and overlying
vitreous haze distinguish it from other yellow-white things in the retina.
This patient has retinal toxoplasmosis. In immunocompromised hosts, such as this patient
with HIV disease, the toxoplasmosis is usually acquired, and no old scars are seen. In
immunocompentent hosts, this condition usually represents satellite reactivation of a
congenital lesion, evident as an adjacent healed chorioretinal scar.
Dot, Flame, Boat Retinal Hemorrhages
This slide of a patient with acute lymphocytic leukemia shows three types of retinal
hemorrhages.

The dot hemorrhages, lying deep within the retina, reflect leakage of capillaries or venules.
They are common in diabetes.
The flame hemorrhages, lying within the superficial nerve fiber layer, reflect ischemic
leakage from arterioles or veins that are ischemic or, in the case of veins, under high
pressure.
The boat hemorrhage (pre-retinal), lying at the interface between retina and vitreous,
reflects leakage under enough pressure to burst through the internal liminiting membrane of
the retina.
Blood can also escape into the vitreous cavity to cause a vitreous hemorrhage.
To learn more about retinal hemorrhages and their causes, check out Retinal Hemorrhages.
Submacular Hemorrhage
This patient has developed bleeding in the macula. The cause of the bleeding is choroidal
neovascularization, that is, a net of new blood vessels that have burrowed from the choroid
under the retina.
The gray portion lies under the retinal pigment epithelium. Surrounding the gray
hemorrhage is a ring of red blood that has escaped into the retina. This patient has age-
related macular degeneration, the commonest cause of choroidal neovascularization and
submacular hemorrhage.
To learn more about retinal hemorrhages and their causes, check out Retinal Hemorrhages.
Retinal Neovascularization

This tangle of blood vessels on the retinal surface is a crude attempt at vascularizing
ischemic tissue. Retinal neovascularization lacks the bifurcating pattern of normal vessels.
Poorly and hastily built, they bleed spontaneously or with minimal trauma. The blood pours
into the retina and into the interface between retina and vitreous, where it attracts fibroglial
elements which form fibrovascular stalks. The stalks induce vitreous contraction which pulls
them farther away from the retina. Eventually the retina detaches. The combination of
hemorrhage and retinal detachment spells blindness.
The common causes of retinal neovascularization on or near the optic disc are diabetes,
retinal vein occlusion, and radiation. Neovascularization in the peripheral retina (out of view
of the direct ophthalmoscope) is most commonly caused by sickle cell disease and
retinopathy of prematurity.
Retinal Pigment Epitheliopathy
Diffuse damage to the retinal pigment epithelium (RPE), which anchors the photoreceptors,
occurs in many hereditary, intra-uterine inflammatory, and acquired toxic-metabolic

disorders. Two retinal areas are most vulnerable: the mid-peripheral (equatorial) and the
perifoveal regions.
Notice that the retinal arterioles are very thin compared to those of the normal fundus. This
arteriolar narrowing is particularly common in advanced hereditary disorders of the RPE.
Damage to the RPE causes the RPE to migrate into the superficial retina. The black pigment
flecks are particularly evident in the retinal mid-periphery.
The combination of RPE loss and migration produces the "salt and pepper" fundus. The
pepper may be clumpy ("bone spicular"), as in the hereditary degenerations, or very fine, as
in the intra-uterine inflammations like rubella. Depending on the degree of damage, the
patient with peripheral retinal pigment epitheliopathy may be asymptomatic or have
profound loss of night vision and construction of the visual field.
In the perifoveal region, you will sometimes see a grayish-brown halo that looks like a bull's
eye. Patients may notice blurred vision just off center. Eventually the foveal region itself
becomes damaged and visual acuity falls.