Embed Size (px)
Citation preview

Nonsteroidal Anti-Inflammatory Drug Prescribing:Past, Present, and Future
Roger Jones, DM, FRCP, FRCGP, FMedSci, FFPHM
Nonsteroidal anti-inflammatory drugs, including as-pirin, are now among the most widely prescribedmedications in the world. They have a long and fas-cinating history, with the use of aspirin derived fromwillow bark stretching back into the Assyrian culture.In the twenty-first century we are faced with both thechallenge of balancing the benefits and side effectsof these drugs and the exciting prospect of new,safer agents with comparable efficacy. Am J Med.2001;110(1A):4S–7S. © 2001 by Excerpta Medica, Inc.
The history of nonsteroidal anti-inflammatorydrugs (NSAIDs) stretches back to the use of ex-tracts of willow bark in prehistory and extends for-
ward to an exciting frontier of technological advancesand new indications for the use of aspirin and the non-aspirin NSAIDs.
PREHISTORY
Stone tablets from the Sumerian period confirmed thatthe Assyrians used the extract of willow leaves for painfulmusculoskeletal conditions and that the Egyptians used adecoction of myrtle and willow leaves for joint pain andfor the relief of pain and inflammation associated withwounds. At the height of the Greek empire there was con-troversy about the most appropriate treatment for painand inflammation, with Dioscorides favoring the use ofcoriander and Hippocrates prescribing, in the shade ofhis plane tree at Kos, extract of willow bark.1
ST. KEVIN OF GLENDALOUGH
One of the most intriguing characters involved in the useof willow bark extract for therapeutic purposes was St.Kevin of Glendalough, who used this medicament to treatpainful musculoskeletal conditions in southern Ireland.St. Kevin was a Catholic monk who, awakening onemorning in his cell, was so overwhelmed by the beauty ofthe countryside around him that he stretched his armsout in praise and thanks to God. His right hand extendedbeyond the bars of his cell and, while he was holdinghimself in his reverie, a dove fluttered down and landedon Kevin’s arm. The monk noticed that the dove wascarrying a twig in its beak and wondered, correctly as ittranspired, whether it was going to build a nest. He didnot move his hand, and the dove returned time and timeagain with further twigs and began building its nest. Sup-ported, fed, and watered by his brethren, St. Kevin re-mained in his cruciform posture until the nest was com-pleted, the eggs laid and hatched, the chicks fed, and thefledglings had flown the nest. He was canonized for thisact of great kindness and patience.
THE EIGHTEENTH CENTURY
The first quasiscientific description of the use of willowbark as an anti-inflammatory agent is attributed to theReverend Edmund Stone from Chipping Norton, Ox-fordshire, United Kingdom, in 1763. He wrote to the then
From the Guy’s, King’s & St. Thomas’ School of Medicine, London,United Kingdom.
Requests for reprints should be addressed to Roger Jones, DM, Guy’s,King’s & St. Thomas’ School of Medicine, 5 Lambeth Walk, LondonSE11 6SP, United Kingdom.
4S © 2001 by Excerpta Medica, Inc. 0002-9343/01/$20.00All rights reserved. PII S0002-9343(00)00627-6

President of the Royal Society, the Earl of Macclesfield, aletter describing successful treatment of patients with fe-ver, possibly malaria, with about 1 g (20 grains) of pow-dered willow bark, taken in a “dram” of water every 4hours. Stone was operating in an almost homeopathic(rather than allopathic) mode, writing of the willow: “Asthis tree delights in a moist or wet soil, where agues chieflyabound, the general maxim that many natural maladiescarry their cures along with them, or that their remedieslie not far from their causes, was so very apposite to thisparticular case.”2
The first clinical trial of the use of aspirin is credited toDr. Thomas MacLagan, a Scottish physician, who tried2 g of salicin on himself and then gave it to patients withacute rheumatism, resulting in complete remission of fe-ver and joint inflammation.3 MacLagan seemed to shareStone’s homeopathic tendencies: “A remedy for that dis-ease would most hopefully be looked for among thoseplants and trees whose favourite habitat presented condi-tions analogueous to those under which the rheumaticmiasma seemed most to prevail. A low-lying damp local-ity, with a cold rather than warm climate gives the condi-tions under which rheumatic fever is most readily pro-duced.”3
THE NINETEENTH AND EARLYTWENTIETH CENTURIES
In the early nineteenth century, Peruvian willow bark wasfavored until Napoleon’s blockade of British trade shiftedthe focus to the use of European willow bark. In 1828,Johann Buchner, professor of pharmacy at Munich, ex-tracted salicin from willow bark. The following year,Henri Leroux obtained crystalline salicin.4 Salicylic acidwas first derived from salicin by the Italian chemist Raf-faele Piria; its chemical structure was identified in Mar-burg, Germany, by Hermann Kolbe, who synthesized sal-icylic acid in 1859. By 1874 industrial production was wellunder way.
Bayer and CompanyGastric irritation and the unpleasant taste of salicylic acidwere, however, problematic side effects. The search for abetter-tolerated compound was led by Felix Hoffmann, achemist with Bayer and Company in Germany, whosefather had tried to take salicylic acid and experienced un-pleasant, unwanted effects. Hoffmann succeeded in syn-thesizing acetylsalicylic acid in 1897. Heinrich Dreser,head of pharmacology at Bayer, immediately experi-mented on himself with this new compound and begananimal experiments, demonstrating the anti-inflamma-tory and analgesic effects of acetylsalicylic acid.5 Thetrade name “Aspirin” was registered in 1899 ( “A” fromacetyl and “spir” from the first part of Spirea ulmania, theplant from which salicylic acid had originally been isolat-
ed). Bayer began to promote the drug to more than30,000 doctors, the first example of mass marketing of apharmaceutical product. Aspirin was, however, refused apatent by the German patent office, which considered theindustrial process insufficiently novel. This meant thatHoffmann received no royalties on the sale of aspirin,because his contract stipulated that royalties were payableonly on patentable products, whereas Dreser’s contractpaid him a royalty on any product introduced, enablinghim to retire a wealthy man.
William OslerNot everyone was an enthusiastic prescriber of salicylate.The great William Osler, in his Principles and Practice ofMedicine, published in 1892, was unimpressed by itsvalue in the treatment of rheumatoid arthritis: “The bestthat can be hoped for is a gradual arrest. It is useless tosaturate the patient with iodide of potassium, salicylatesor quinine. Arsenic seems to do good as a general tonic.”6
The rest is history. Sales of Bayer Aspirin rose fromaround 100 million Deutschmarks in the 1940s to morethan 800 million annually in the mid-1990s, with pro-jected sales approaching 2 billion Deutschmarks per an-num in the twenty-first century.
Winston ChurchillInterestingly, Winston Churchill provides an early casestudy of the changing pattern of the use of aspirin.Churchill’s physician was Lord Moran (whom Churchilldid not particularly like, regarding him as a pill pusher).Moran had the unenviable task of providing medical sup-port to someone who started the day with half a bottle ofchampagne and finished it with half a bottle of brandy,and the medications prescribed for Churchill were corre-spondingly robust. Concoctions known as “Moran’s ma-jors” included barbiturates and amphetamines. Moran’s“minors” also contained stimulants and sedatives, withthe addition of 160 mg of aspirin daily. These medica-tions were prescribed to Churchill after his first stroke in1955, so that Moran may have unwittingly prolongedChurchill’s life by prescribing low-dose aspirin, with itscardiovascular protective properties.7
NONASPIRIN NONSTEROIDALANTI-INFLAMMATORY DRUGS
Compared with aspirin, the nonaspirin NSAIDs(NANSAIDs) have enjoyed a much shorter, although noless fascinating, history. Ibuprofen, the first of theNANSAIDs, was identified from hundreds of candidatecompounds by the Boots Company in the early 1950s,and by the 1970s it was being widely prescribed for thetreatment of painful musculoskeletal anti-inflammatoryconditions. Over the subsequent years, new classes ofNANSAIDs were identified and a series of novel agentswas brought to market. These drugs are now among the
A Symposium: Nonsteroidal Anti-Inflammatory Drug Prescribing/Jones
January 8, 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 110 (1A) 5S
most widely prescribed of all therapeutic agents, but alsohave a significant history of serious toxicity and adverseeffects.
The NSAIDs exert their anti-inflammatory effect byinhibition of the enzyme cyclooxygenase (COX); thismechanism is the basis for their therapeutic effect as wellas their toxicity. Gastrointestinal irritation, ulceration,and hemorrhage; fluid retention and exacerbation of hy-pertension; and exacerbation of bronchospasm and ana-phylaxis are their most serious adverse effects, althoughmany others have been recorded. Approaches to manag-ing the risks and benefits of these important agents forma major part of this supplement.
In recent years, however, it has become clear that COXexists in two isoforms, constitutive COX-1 and inducibleCOX-2. Drugs that selectively inhibit the COX-2 isoformare much less likely to cause the adverse effects of COX-1inhibition. These agents offer the promise of efficacywithout toxicity. Their place in future treatment is alsodiscussed in detail elsewhere in this supplement.
PRESCRIBING NONSTEROIDALANTI-INFLAMMATORY DRUGS
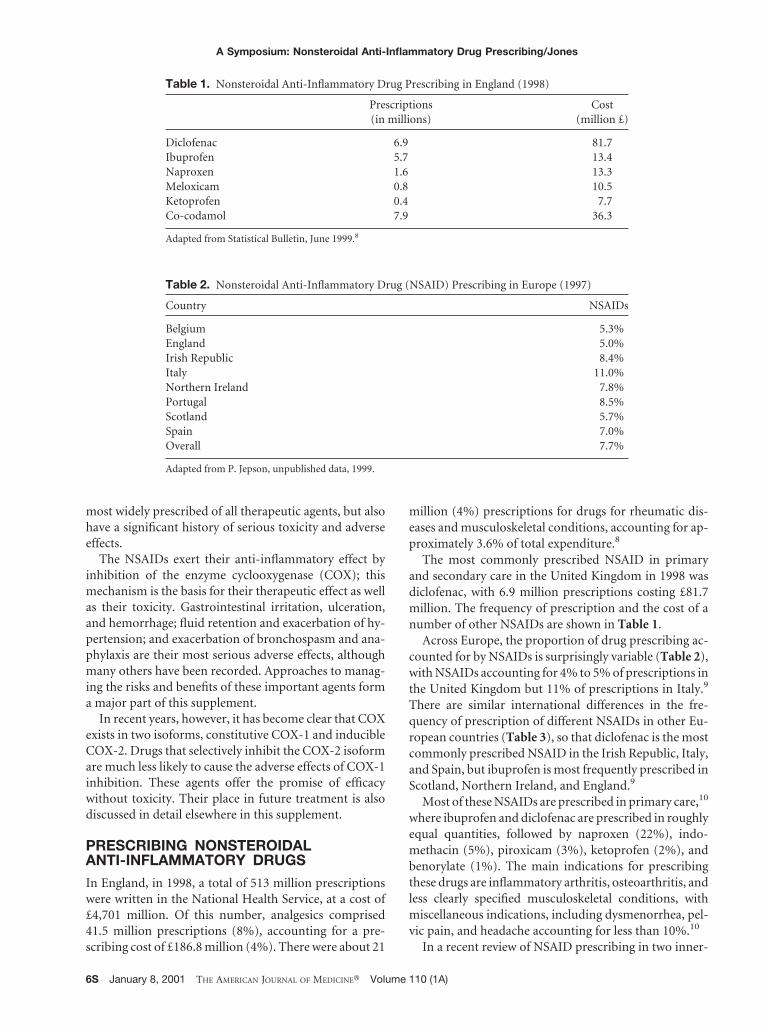
In England, in 1998, a total of 513 million prescriptionswere written in the National Health Service, at a cost of£4,701 million. Of this number, analgesics comprised41.5 million prescriptions (8%), accounting for a pre-scribing cost of £186.8 million (4%). There were about 21
million (4%) prescriptions for drugs for rheumatic dis-eases and musculoskeletal conditions, accounting for ap-proximately 3.6% of total expenditure.8
The most commonly prescribed NSAID in primaryand secondary care in the United Kingdom in 1998 wasdiclofenac, with 6.9 million prescriptions costing £81.7million. The frequency of prescription and the cost of anumber of other NSAIDs are shown in Table 1.
Across Europe, the proportion of drug prescribing ac-counted for by NSAIDs is surprisingly variable (Table 2),with NSAIDs accounting for 4% to 5% of prescriptions inthe United Kingdom but 11% of prescriptions in Italy.9
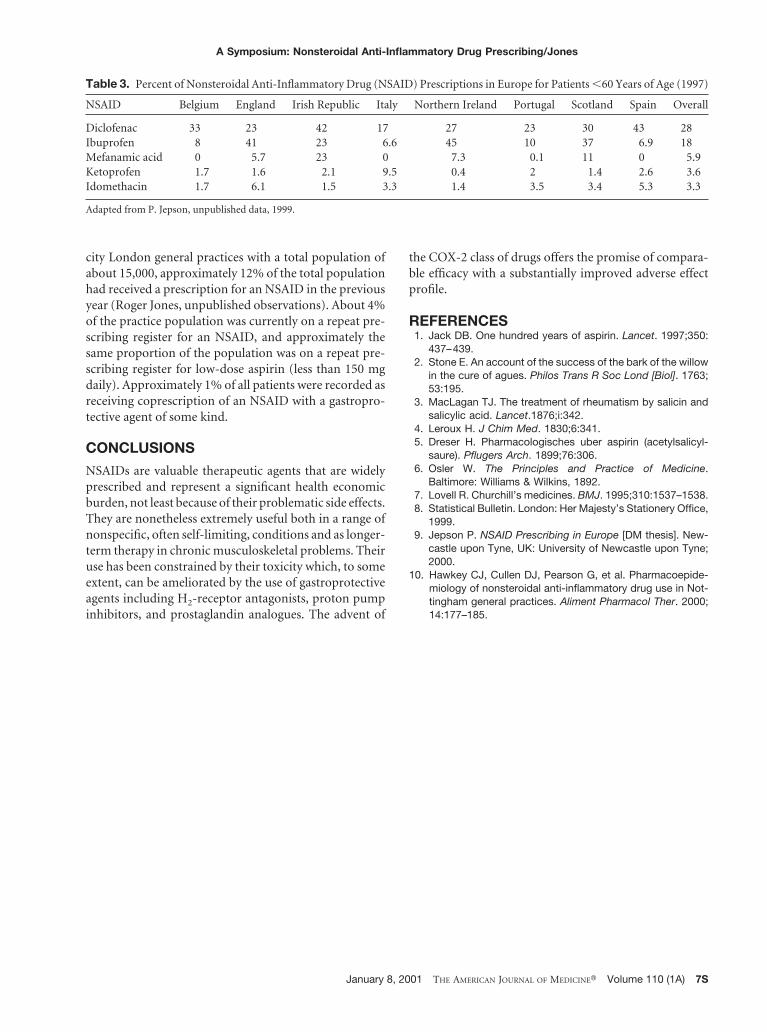
There are similar international differences in the fre-quency of prescription of different NSAIDs in other Eu-ropean countries (Table 3), so that diclofenac is the mostcommonly prescribed NSAID in the Irish Republic, Italy,and Spain, but ibuprofen is most frequently prescribed inScotland, Northern Ireland, and England.9
Most of these NSAIDs are prescribed in primary care,10
where ibuprofen and diclofenac are prescribed in roughlyequal quantities, followed by naproxen (22%), indo-methacin (5%), piroxicam (3%), ketoprofen (2%), andbenorylate (1%). The main indications for prescribingthese drugs are inflammatory arthritis, osteoarthritis, andless clearly specified musculoskeletal conditions, withmiscellaneous indications, including dysmenorrhea, pel-vic pain, and headache accounting for less than 10%.10
In a recent review of NSAID prescribing in two inner-
Table 1. Nonsteroidal Anti-Inflammatory Drug Prescribing in England (1998)
Prescriptions(in millions)
Cost(million £)
Diclofenac 6.9 81.7Ibuprofen 5.7 13.4Naproxen 1.6 13.3Meloxicam 0.8 10.5Ketoprofen 0.4 7.7Co-codamol 7.9 36.3
Adapted from Statistical Bulletin, June 1999.8
Table 2. Nonsteroidal Anti-Inflammatory Drug (NSAID) Prescribing in Europe (1997)
Country NSAIDs
Belgium 5.3%England 5.0%Irish Republic 8.4%Italy 11.0%Northern Ireland 7.8%Portugal 8.5%Scotland 5.7%Spain 7.0%Overall 7.7%
Adapted from P. Jepson, unpublished data, 1999.
A Symposium: Nonsteroidal Anti-Inflammatory Drug Prescribing/Jones
6S January 8, 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 110 (1A)
city London general practices with a total population ofabout 15,000, approximately 12% of the total populationhad received a prescription for an NSAID in the previousyear (Roger Jones, unpublished observations). About 4%of the practice population was currently on a repeat pre-scribing register for an NSAID, and approximately thesame proportion of the population was on a repeat pre-scribing register for low-dose aspirin (less than 150 mgdaily). Approximately 1% of all patients were recorded asreceiving coprescription of an NSAID with a gastropro-tective agent of some kind.
CONCLUSIONS
NSAIDs are valuable therapeutic agents that are widelyprescribed and represent a significant health economicburden, not least because of their problematic side effects.They are nonetheless extremely useful both in a range ofnonspecific, often self-limiting, conditions and as longer-term therapy in chronic musculoskeletal problems. Theiruse has been constrained by their toxicity which, to someextent, can be ameliorated by the use of gastroprotectiveagents including H2-receptor antagonists, proton pumpinhibitors, and prostaglandin analogues. The advent of
the COX-2 class of drugs offers the promise of compara-ble efficacy with a substantially improved adverse effectprofile.
REFERENCES1. Jack DB. One hundred years of aspirin. Lancet. 1997;350:
437–439.2. Stone E. An account of the success of the bark of the willow
in the cure of agues. Philos Trans R Soc Lond [Biol]. 1763;53:195.
3. MacLagan TJ. The treatment of rheumatism by salicin andsalicylic acid. Lancet.1876;i:342.
4. Leroux H. J Chim Med. 1830;6:341.5. Dreser H. Pharmacologisches uber aspirin (acetylsalicyl-
saure). Pflugers Arch. 1899;76:306.6. Osler W. The Principles and Practice of Medicine.
Baltimore: Williams & Wilkins, 1892.7. Lovell R. Churchill’s medicines. BMJ. 1995;310:1537–1538.8. Statistical Bulletin. London: Her Majesty’s Stationery Office,
1999.9. Jepson P. NSAID Prescribing in Europe [DM thesis]. New-
castle upon Tyne, UK: University of Newcastle upon Tyne;2000.
10. Hawkey CJ, Cullen DJ, Pearson G, et al. Pharmacoepide-miology of nonsteroidal anti-inflammatory drug use in Not-tingham general practices. Aliment Pharmacol Ther. 2000;14:177–185.
Table 3. Percent of Nonsteroidal Anti-Inflammatory Drug (NSAID) Prescriptions in Europe for Patients ,60 Years of Age (1997)
NSAID Belgium England Irish Republic Italy Northern Ireland Portugal Scotland Spain Overall
Diclofenac 33 23 42 17 27 23 30 43 28Ibuprofen 8 41 23 6.6 45 10 37 6.9 18Mefanamic acid 0 5.7 23 0 7.3 0.1 11 0 5.9Ketoprofen 1.7 1.6 2.1 9.5 0.4 2 1.4 2.6 3.6Idomethacin 1.7 6.1 1.5 3.3 1.4 3.5 3.4 5.3 3.3
Adapted from P. Jepson, unpublished data, 1999.
A Symposium: Nonsteroidal Anti-Inflammatory Drug Prescribing/Jones
January 8, 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 110 (1A) 7S





























